PopulationandAssayThresholdsforthePredictiveValueofLipoprotein(a)
forCoronaryArteryDisease:TheEPIC-NorfolkProspectivePopulationStudy
RutgerVerbeek1,S.MatthijsBoekholdt2,RobertM.Stoekenbroek1,G.KeesHovingh1,JosephL.
Witztum,3NicholasJ.Wareham4,ManjinderS.Sandhu5,6,Kay-TeeKhaw5,SotiriosTsimikas7
1.DepartmentofVascularMedicine,AcademicMedicalCenter,theNetherlands
2.DepartmentofCardiology,AcademicMedicalCenter,theNetherlands
3.DivisionofEndocrinology,DepartmentofMedicine,UniversityofCaliforniaSanDiego,La
Jolla,California,USA
4.MedicalResearchCouncilEpidemiologyUnit,Cambridge,UnitedKingdom
5.DepartmentofPublicHealthandPrimaryCare,UniversityofCambridge,Cambridge,United
Kingdom
6.GeneticEpidemiologyGroup,WellcomeTrustSangerInstitute,Hinxton,UnitedKingdom
7.VascularMedicineProgram,SulpizioCardiovascularCenter,UniversityofCaliforniaSan
Diego,LaJolla,California,USA
Correspondingauthor:Sotirios Tsimikas, MD, Vascular Medicine Program, Sulpizio
CardiovascularCenter, University of California San Diego, 9500 Gilman Drive, BSB 1080,
La Jolla, CA 92093-0682. E-mail [email protected]
by guest, on March 23, 2019
ww
w.jlr.org
Dow
nloaded from
2
Abstract
VariableagreementexistsbetweendifferentLp(a)measurementmethods,buttheirclinical
relevanceremainsunclear.ThepredictivevalueofLp(a)measuredbytwodifferentassays
(RandoxandUCSD)wasdeterminedin623CADcasesand948controlsinacase-controlstudy
withintheEPIC-Norfolkprospectivepopulationstudy.Participantsweredividedintosex-
specificquintiles,andbyLp(a)<50versus>50mg/dL,whichrepresentsthe80thpercentilein
northernEuropeansubjects.RandoxandUCSDLp(a)levelswerestronglycorrelated,with
Spearman’scorrelationcoefficientsformen,womenandsexescombinedwere0.905,0.915
and0.909,respectively(p<0.001foreach).The>80thpercentilecut-offvalues,however,were
36mg/dLand24mg/dLfortheRandoxandUCSDassays,respectively.Despitethis,Lp(a)levels
weresignificantlyassociatedwithCADrisk,withoddsratiosof2.18(1.58-3.01)and2.35(1.70-
3.26)forpeopleinthetopversusbottomLp(a)quintilefortheRandoxandUCSDassays,
respectively.ThisstudydemonstratesthatCADriskispresentatlowerLp(a)levelsthanthe
currentlysuggestedoptimalLp(a)levelof<50mg/dL.Appropriatethresholdsmayneedtobe
populationandassayspecificuntilLp(a)assaysarestandardizedandLp(a)thresholdsare
evaluatedbroadlyacrossallpopulationsatriskforCVDandaorticstenosis.
by guest, on March 23, 2019
ww
w.jlr.org
Dow
nloaded from
3
Introduction
Elevatedlevelsoflipoprotein(a)[Lp(a)]areagenetic,independentriskfactorforthe
developmentofcardiovasculardisease(CVD)(1).TheEuropeanAtherosclerosisSociety(EAS)
ConsensusPanelhasrecommendedthatLp(a)levelsshouldbemeasuredinpatientswithan
intermediateorhighCVDriskandthatdesirableLp(a)levelsarebelowthe80thpercentileof
thepopulationdistribution,whichroughlycorrespondedto50mg/dLinaCopenhagen
populationof6000subjects(2).Preciseandreliablemeasurementmethodsaretherefore
essentialtoguideclinicaldecision-making.Yet,previousstudieshaveindicatedsubstantial
differencesinLp(a)valuesasmeasuredbyvariousassaysandamongdifferentracialgroups(3,
4).Animportantlimitationintheinconsistencyofmeasurementsisthefactthatmanyassays
areaffectedbythesizeofapolipoprotein(a)[apo(a)],themajorproteincomponentofLp(a),
andthatantibodiesandcalibratorsvaryacrossplatforms.Basedongeneticvariantsofthis
protein,largeinter-individualdifferencesinapo(a)isoformsizeexist.
Previousstudieshaveattemptedtoelucidatetheclinicalrelevanceofthepoorinter-
assayagreementintermsofcardiovascularriskclassification.Marcovinaetal.assessedthe
concordanceinLp(a)resultsamong22differentLp(a)assays(3).Considerableheterogeneity
wasobserved,inparticularbetweenapo(a)size-sensitiveassays.Theauthorsalsospeculated
thatthisinaccuracymighttranslateintoinaccurateriskassessment.Adirectcomparisonof
threeLp(a)assaysinasubsetoftheFraminghamOffspringcohortdemonstratedlargeinter-
assaydifferencesinLp(a)valuesandconsequentlyinthe80thpercentilecut-offvalues,which
waslargelydeterminedbydifferencesinapo(a)isoformsize(4).However,thenumberof
coronaryarterydisease(CAD)eventsinthatstudywaslimited.Arecentmeta-analysis
by guest, on March 23, 2019
ww
w.jlr.org
Dow
nloaded from
4
evaluatedtheCVDpredictivevaluebetweenpooledisoform-sensitiveandisoform-insensitive
assays(5)andobservedasubstantialheterogeneitybetweenthedifferentstudies.However,no
formalassaycomparisonsweremadeandassayswereperformedindifferentstudy
populations,makingitimpossibletodirectlycomparethepredictivevalueofdifferentassays.
Understandingappropriateassayandpopulationthresholdsforriskareessentialas
noveltherapies,includingantisenseoligonucleotides,PCSK9inhibitorsandCETPinhibitorsand
mipomersen(6-10),lowerLp(a).Therefore,ourobjectivesweretwofold:firsttodetermineif
thepopulationthresholdspreviouslysuggestedforoptimallevelsapplybroadlytoothergroups
ofpatients;andsecondtodeterminetheconcordancebetweenaclinically-availableand
commonlyusedimmonoturbidimetricLp(a)assaycomparedtoaresearch-basedenzyme-linked
immunosorbentassay(ELISA)inpredictingCADrisk.Weaddressedthisobjectiveinacase-
controlstudynestedintheEPIC-Norfolkprospectivepopulationstudy.
Methods
Studydesign
TheEuropeanProspectiveInvestigationofCancer(EPIC)-Norfolkprospectivepopulation
studyhasbeendescribedindetailpreviously(11).Inbrief,theEPIC-Norfolkprospective
populationstudyincluded25,663menandwomenagedbetween45and79yearsold,and
livinginNorfolk,UnitedKingdom.Thestudywasdesignedtodeterminetheeffectsofdietand
otherlifestylefactorsontheriskofdevelopingcancer,andadditionaldatawereobtainedto
studydeterminantsofotherdiseases.Participantswererecruitedusingregistersfromgeneral
practicesandwereincludedafterwritteninvitation.Allsubjectshavebeenflaggedfordeath
by guest, on March 23, 2019
ww
w.jlr.org
Dow
nloaded from
5
certificationattheUnitedKingdomOfficeofNationalStatistics,withvitalstatusascertainedfor
theentirecohort.Inaddition,allhospitalizationsforstudyparticipantswererecordedusing
theiruniqueNationalHealthServicenumberbydatalinkagewithENCORE,theEastNorfolk
HealthAuthoritydatabase,whichidentifiesallhospitalcontactsthroughoutEnglandandWales
forNorfolkresidents.Trainednosologistscodedtheunderlyingcauseofhospitaladmissionor
deathaccordingtothe10threvision(ICD-10)oftheInternationalClassificationofDiseases.
FatalCADduringfollow-upwasdefinedasdeathwiththeunderlyingcausecodedasICD-10
codesI20toI25.NonfatalCADwasdefinedashospitalizationwiththeunderlyingcausecoded
asI20toI25.
Participants
Forthisspecificstudy,weanalyzedthedataofacase-controlstudyoriginallydescribed
byBoekholdtetal(12).Briefly,participantsweremarkedasacaseiftheywereapparently
healthyatbaseline,andhaddiedorbeenhospitalizedwithCADastheunderlyingcauseduring
follow-up.Controlsweredefinedasstudyparticipantswhowereapparentlyhealthyatbaseline
anddidnotdevelopanyCVDduringfollow-up.Intheoriginalstudydesign,weattemptedto
matchtwocontrolstoeachcase,bysex,age(within5years),anddateofbaselinevisit(within
3months).Inthisstudyset,Lp(a)levelsweremeasuredin2160participantsattheUniversityof
CaliforniaSanDiego,aspreviouslydescribed(13).Severalyearslater,itwasdecidedto
measureLp(a)levelsintheentireEPIC-NorfolkcohortattheUniversityofCambridge,
dependingonsampleavailability,aspreviouslydescribed(14).Theseincludedsamplesfrom
thecase-controlstudy.Duetoinsufficientsamplematerialhowever,notallsampleswere
by guest, on March 23, 2019
ww
w.jlr.org
Dow
nloaded from
6
measuredwithbothassays.Thereforethecurrentanalysisisbasedontheoverlapbetween
thesetworoundsofLp(a)measurements.
Biochemicalanalysis
Atthebaselinestudyvisit,bloodwasdrawnfromstudyparticipants,aspreviously
described(11).Totalcholesterol,high-densitylipoprotein(HDL)cholesterolandtriglycerides
weredeterminedwiththeRA1000(BayerDiagnostics,Basingstoke,UnitedKingdom).The
Friedewaldformulawasusedforthecalculationoflow-densitylipoprotein(LDL)cholesterol
levels.Laterintime,Lp(a)levelsweredeterminedinnon-fastingbaselinesampleswhichhad
beenstoredat-80°C.
IntheRandoxassay,Lp(a)levelsweredeterminedonaOlymposAU640analyserwithan
immunoturbidimetricmethod(RandoxlaboratoriesLtd.Crumlin,CountyAntrim,United
Kingdom)(14).Thisassayuseslatexparticlescontainingrabbitanti-humanLp(a)polyclonal
antibodyasareagent(licensedfromDenkaSeikenCo.,Ltd.,Niigata,Japan)andRandox'sown
calibratorsandcontrolsfromscreenedplasmadonatedbyvolunteers.Therabbitanti-human
Lp(a)polyclonalantibodyistechnicallyisoformsensitivebyvirtueoftheantiserabindingto
multiplesitesofKIV2repeats,buttheassayistheoreticallymadenearlyisoformindependent
bythecalibratorsystem.Thisassayformat,likemostcommercialassays,bindstobothfree
apo(a)andtrueLp(a)(i.e.apo(a)covalentlyboundtoapolipoproteinB-100),thereforeitisbest
describedasmeasuring"totalapo(a)"ratherthan"Lp(a)".
IntheUCSDassay,designedandconductedattheUniversityofCaliforniaSanDiego,
Lp(a)levelswerealsodeterminedwithanLp(a)assaydesignedbyTsimikasetal(15),which
by guest, on March 23, 2019
ww
w.jlr.org
Dow
nloaded from
7
incorporatesthemurinemonoclonalantibodyLPA4withachemiluminescentELISA(13).LPA4
isamurinemonoclonalIgGantibodytoapo(a)thatwasgeneratedbyimmunizingmicewiththe
apo(a)sequenceTRNYCRNPDAEIRP.ThissequenceispresentasonecopyonKIV5,KIV7,and
KIV8ofapolipoprotein(a),anddoesnotcross-reactwithplasminogen.LPA4doesnotbindto
KIV2,andthereforeitisisoformindependent.Thisassayisalsoatrue“Lp(a)”assayasitusesa
captureantibodytoapolipoproteinB-100anddetectsapo(a)withbiotinylatedLPA4.Free
apo(a)isnotdetectedwiththisassay,butitisusuallynotpresenttoanysignificantamountin
humansingeneralpopulations.BecauseLPA4bindsto3identicalsitesonapo(a),whichare
presentinallpatientsandallisoformstothesameextent,thisassayhashighsensitivityanda
broadlinearrangefrom0.5-180mg/dL.Thisassayuses9calibrators,rangingfrom6-168mg/dL
tocaptureawiderangeofvalues,identifiedfromindividualhumanplasmasamples.Thevalues
assignedtothecalibratorswerevalidatedbyboththeDiasorin(Stillwater,Mn)and
Technoclone(Vienna,Austria)calibrators.Thisassaycorrelateswellwithcommercially
availableLp(a)assays,hasacoefficientofvariabilityof3-5%,andhasbeenusedinover20
studiesand20,000patients(13,16-19).
Statisticalanalysis
ThecurrentanalysisisbasedonavailabilityofbothLp(a)measurementsinthecohort
database.TheselectionofcasesandcontrolsisthereforebasedontheoverlapbetweenLp(a)
measurementsperformedinanestedcase-controlsetasdescribedabove,andtheentireEPIC-
Norfolkcohort.Byvirtueofthisselectionprocedure,theoriginal1:2matchingbysex,ageand
enrollmenttimewaspartiallylost.
by guest, on March 23, 2019
ww
w.jlr.org
Dow
nloaded from
8
Baselinecharacteristicswerecalculatedforcasesandcontrolsseparately,stratifiedby
sex.ThecorrelationbetweenLp(a)levelsasmeasuredbytheRandoxandUCSDassaywas
quantifiedusingSpearmancorrelationcoefficients.BecausetheEASConsensusPanel
recommendedusingthe80thpercentileasthecut-offvalueforanelevatedLp(a)level(2),we
performedanalysesusingbothsex-specificandpooledLp(a)quintiles.Inaddition,becausethe
80thpercentileinDanishpopulationsisthoughttocorrespondroughlytoanLp(a)levelof50
mg/dL,wealsoperformedanalyseswhereparticipantswerestratifiedusingtheLp(a)threshold
of50mg/dL.ToassesstheassociationbetweenLp(a)levelsandtheriskofdevelopingCAD,
logisticregressionanalyseswereperformedtodeterminetheoddsratiosandcorresponding
95%confidenceintervalsperLp(a)quintile,usingthelowestquintileasreferencecategory.
Furthermore,oddsratiosweredeterminedforparticipantswithLp(a)levels>50mg/dL,using
those<50mg/dLasreferencecategory.Analyseswereperformedseparatelyformenand
womenusingsex-specificcut-offs,andalsoformenandwomencombinedusingpooledcut-
offs.Inaddition,weassessedtheconcordancebetweentheassaysinclassifyingstudy
participantsas<50mg/dLversus>50mg/dL.AllstatisticalanalyseswereperformedwithSPSS
statisticalsoftware(Version21.0,IBMCorporation,Armonk,NY).
RESULTS
Atotalof1571studyparticipantshadLp(a)measurementsdonebyboththeRandox
andUCSDassays.Thissetcomprised623CADcasesand948matchedcontrols.Baseline
characteristicsareshowninTable1.Asexpected,caseshadhigherlevelsofLDL-cholesterol,
by guest, on March 23, 2019
ww
w.jlr.org
Dow
nloaded from
9
higherbloodpressureandhigherbodymassindex,andweremorelikelytosmokeandhave
diabetesmellitus,comparedtocontrols.Median(interquartilerange)Lp(a)levelsmeasuredby
theRandoxassaywere14.3(7.2-35.9)mg/dLformalecases,11.2(6.1-23.2)mg/dLformale
controls,15.5(8.5-37.9)mg/dLforfemalecasesand11.4(6.8-21.9)mg/dLforfemalecontrols.
MedianLp(a)levelsmeasuredbytheUCSDassaywere9.3(6.8–23.9)mg/dLformalecases,
8.1(6.4-13.4)mg/dLformalecontrols,10.4(7.4-29.8)mg/dLforfemalecasesand8.5(6.5-12.9)
mg/dLforfemalecontrols.
Lp(a)levelsasquantifiedbytheRandoxandUCSDassayswerestronglycorrelated.
Spearman’scorrelationcoefficientsformen,womenandsexescombinedwere0.905,0.915
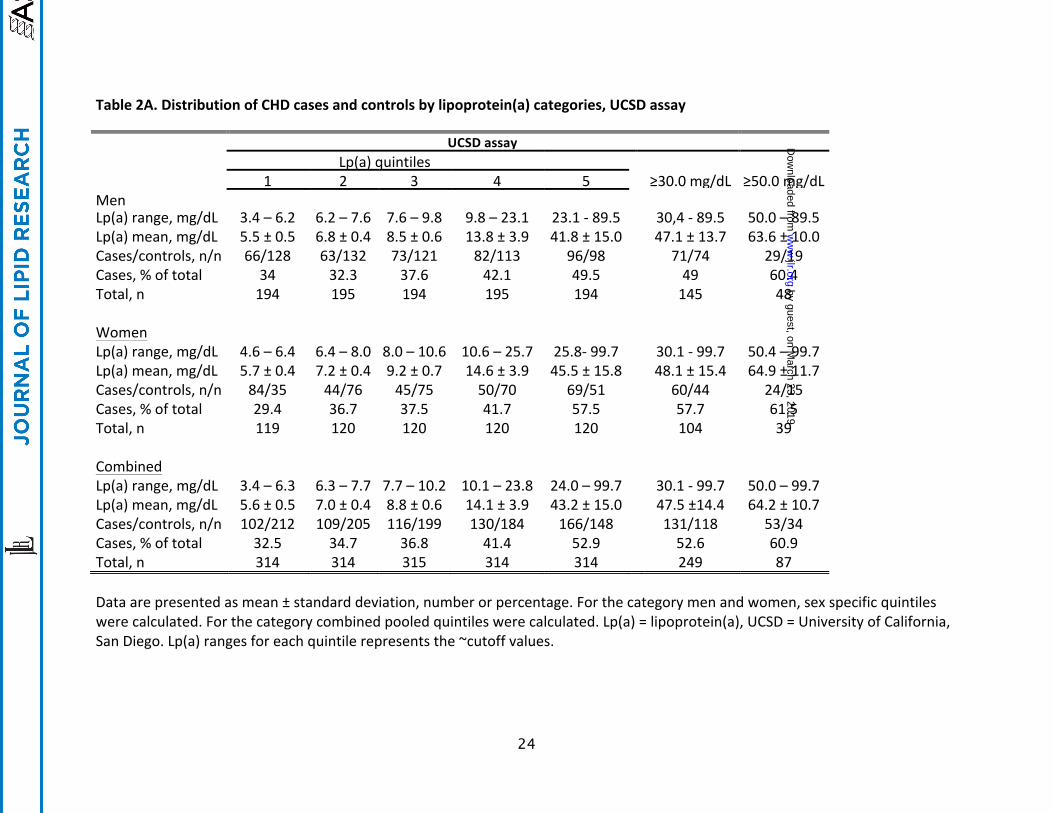
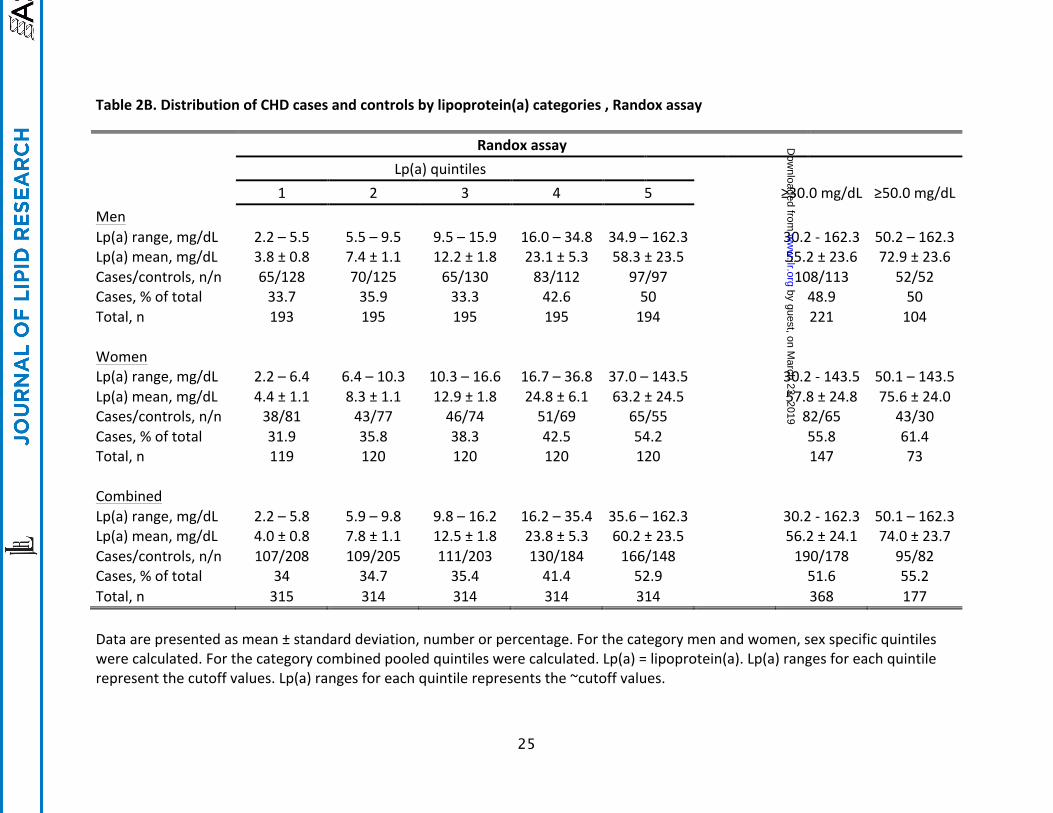
and0.909,respectively(p<0.001foreach).ThedifferencesinLp(a)levelsmeasuredbythe
RandoxandUCSDassaysweremostprominentinthehighestquintiles,withtheRandoxassay
yieldinghigherLp(a)levelsthantheUCSDassay,asshowninTable2.The80thpercentile
thresholdswerealsodifferent.TheRandoxassayyielded80thpercentilethresholdvaluesof35
mg/dL,37mg/dLand36mg/dLformen,womenandsexescombined,respectively.The
corresponding80thpercentilethresholdsaccordingtotheUCSDassaywere23mg/dL,26mg/dL
and24mg/dLformen,womenandsexescombined,respectively.Importantly,withboth
assays,the80thpercentilethresholdswerewellbelow50mg/dL.UsingtheRandoxassay,the
distributionofcasesversuscontrolsamongthepooledsexesrangedfrom107/208(34.0%)in
thelowestquintileto166/148(52.9%)inthehighestquintile.UsingtheUCSDassaythe
correspondingnumberswere102/212(32.5%)inthelowestquintileand166/148(52.9%)in
thehighestquintile.Inthegroup≥50mg/dL,thenumbersofcasesversuscontrolswere95/82
(55.2%)fortheRandoxassay,and53/34(60.9%)fortheUCSDassay.
by guest, on March 23, 2019
ww
w.jlr.org
Dow
nloaded from
10
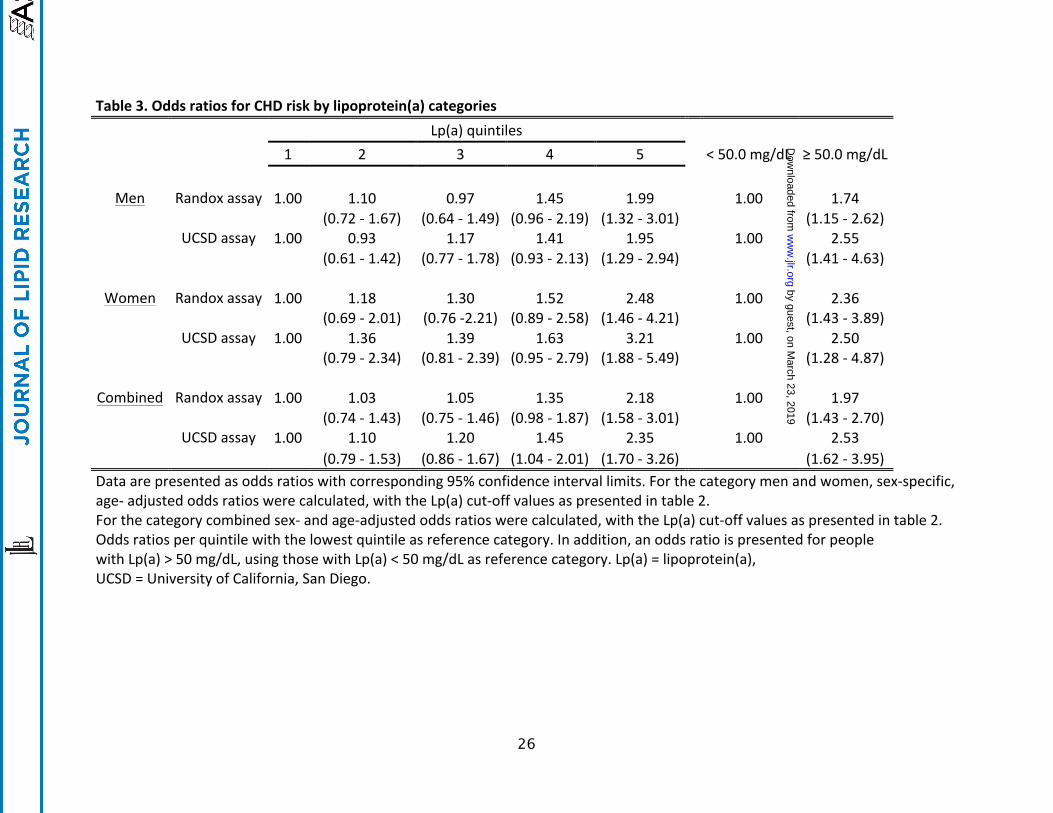
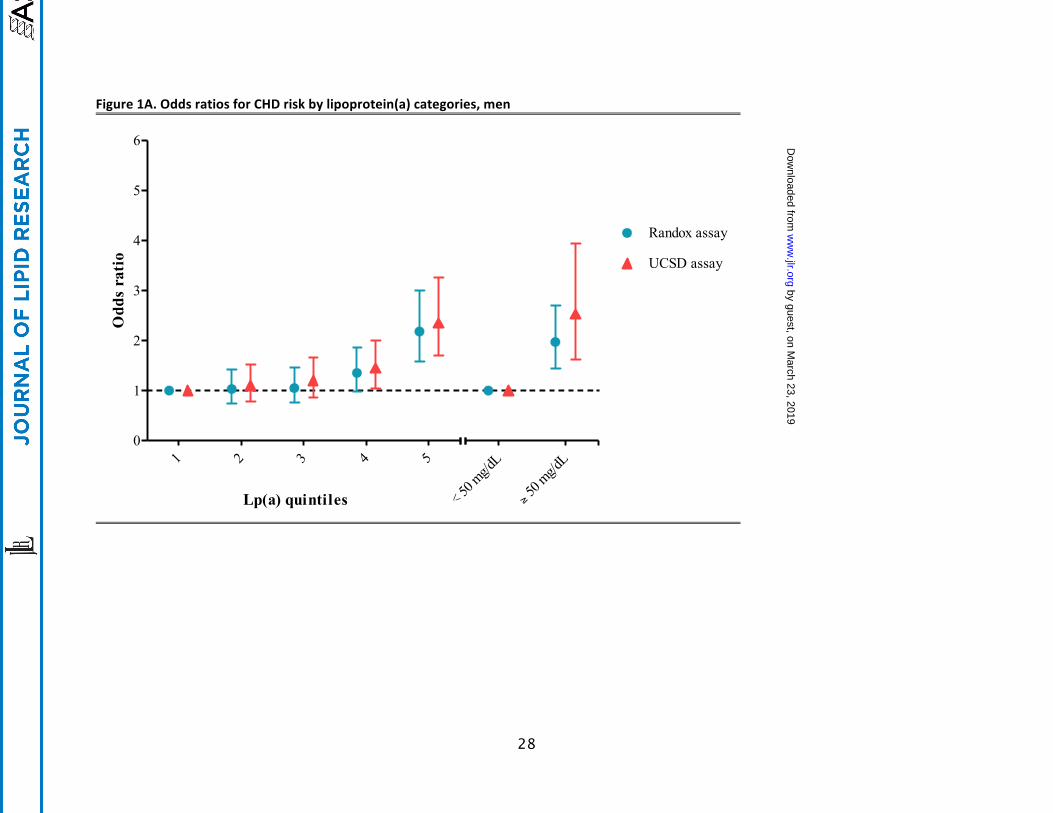
OddsratiosfortheriskofCADbyLp(a)quintiles,aswellasforthecomparison≥versus
<50mg/mlareshowninTable3andFigure1.Oddsratiosforpeopleinthetopquintile(i.e.
>80thpercentile)comparedtothoseinthelowestquintilewere2.18(95%CI1.58–3.01)using
theRandoxassayand2.35(95%CI1.70–3.26)usingtheUCSDassay.Oddsratiosforpeople
withLp(a)≥50mg/dLversus<50mg/dLwere2.29(95%CI1.56–3.36)fortheRandoxassay
and2.85(95%CI1.66–4.90)fortheUCSDassay.
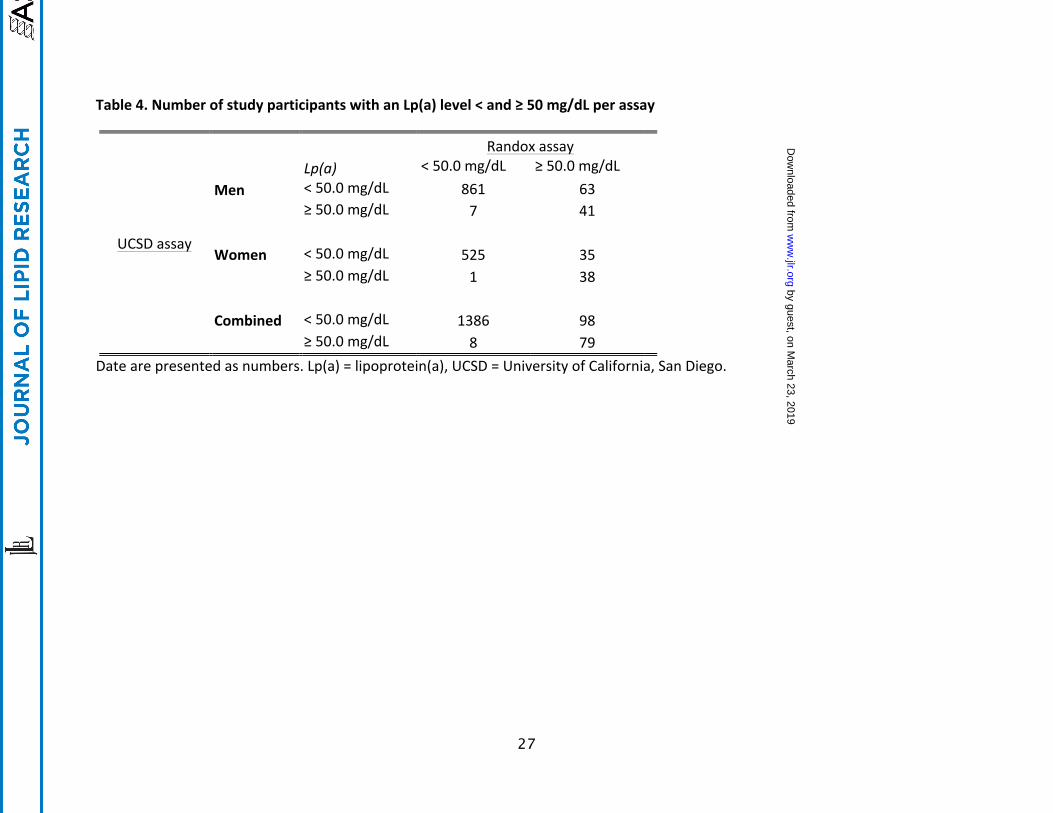
Theconcordance/discordancebetweenthetwoassaysinclassifyingstudyparticipants
accordingtoanLp(a)levelaboveorbelow50mg/dLareshowninTable4.Atotalof1465study
participantshadconcordantresultsforbothassays.Discordantresultswereobservedin106
studyparticipants(6.9%oftotalsubjects),with8havingLp(a)<50mg/dLontheRandoxassay
butLp(a)≥50mg/dLontheUCSDassay,whereas98havingLp(a)≥50mg/dLontheRandox
assaybutLp(a)<50mg/dLontheUCSDassay.
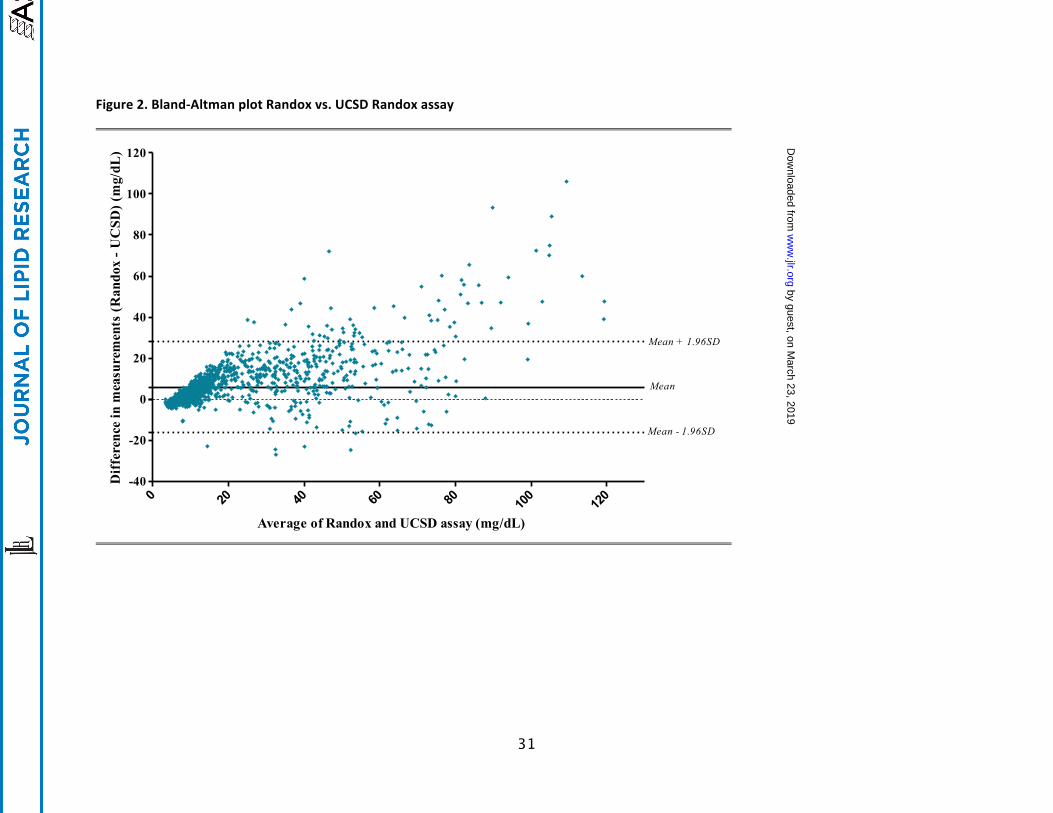
ABland-Altmananalysiswasperformedtodeterminethelevelofagreementbetween
theUCSDandtheRandoxassay(Figure2).Themeanaveragewas-5.9mg/dL,thelower95%
limitofagreementwas-16.3mg/dLandtheupper95%limitofagreementwas-28.2mg/dL.At
lowaverageconcentrations,thelevelofagreementwasgood,butwithincreasing
concentrations,thelevelofagreementdiminished.
DISCUSSION
ThisstudyevaluatedpopulationandassaythresholdsforthepredictivevalueofLp(a)
fortheriskofcoronaryarterydiseasewith2differentassaysmeasuredinthesamesubjects.
Interestingly,nearlyidenticalpredictivevalueforidentifyingsubjectswithorwithoutCADwas
by guest, on March 23, 2019
ww
w.jlr.org
Dow
nloaded from
11
evidentbutthiswastruewhenexaminedinthecontextofthewholepopulationstudiedforthe
givenassay,e.g.intermsofquintiles,butnotwhencomparingabsoluteLp(a)levelsand80th
percentilecut-offvalues.Finally,forbothassaysthe80thpercentilecut-offsweresignificantly
lowerthan50mg/dL,theEASproposedthreshold,whichwasbasedontheCopenhagen
GeneraPopulationStudy(2,20,21).ThisthresholdwasbasedonprevalenceofLp(a)valuesin
thegeneralpopulationandnotnecessarilybasedonwhenriskofLp(a)begins.Epidemiological
andgeneticstudiessuggesttheriskthresholdsstartat25-30mg/dLinprimarycarepopulations
(1,14,20),but>50mg/dLinsecondarypreventionpopulationsthathavebeentreatedwith
severalsecondarypreventionmeasuressuchasaspirin,clopidogrel,statinsandanti-
hypertensivemedications(22,23).Ourfindingssuggestthatthethresholdsfordetermining
whatisahighlevelandwhoisatriskshouldbereportedasassayspecificthresholdsuntil
assaysfromallmanufacturersaresufficientlystandardizedeachassayprovidesthesame
absolutevaluesforagivenplasmasample.Preferably,asetofinternationallyaccepted
standardsandcalibratorsshouldbeagreeduponandimplementedacrossallassayplatforms.
Lp(a)consistsofanLDL-likeparticle,inwhichapoB-100iscovalentlyboundtoapo(a).
Apo(a)consistsofseveralkringledomains,inwhichthenumberofkringledomainIVtype2
(KIV2)repeatsisthedominantsize-determiningdomainofapo(a);eachapo(a)isoformcan
containfrom3upto>40KIV2repeats(24,25).ThenumberofKIV2repeatsisinverselyrelated
withtheplasmalevelofLp(a),andexplains25-50%ofplasmaLp(a)levels(20,26).Additional
geneticdeterminantsofvariabilityarepresentintheLPAgeneandincluderegulatoryelements
andsinglenucleotidepolymorphismsthatmediateeitherhighorlowLp(a)levels(27-31).These
by guest, on March 23, 2019
ww
w.jlr.org
Dow
nloaded from
12
uniquepropertiesofLp(a)greatlycontributetothedifficultyofestablishingcommonstandards
foritsclinicalmeasurement.
Lp(a)measurementmethodsarebasedonavarietyoftechniques,including
immunonephelometry,immunoturbidometry,andELISA’s(32).Incontrasttootherprotein
quantificationassays,Lp(a)assaysarenotoriouslychallengingbecauseofthelargevariationin
sizeandstructureoftheapo(a)proteinsize,whichismediatedbytheallelicheterogeneityin
thenumberofKIV2repeats.Additionally,eachindividualgenerallyhastwoexpressedalleles
thatusuallycodefortwodifferentsizedapo(a)proteinsinplasma.Over40differentsized
isoformsofapo(a)havebeenreportedandapproximately80%ofindividualshavetwodifferent
sizedapo(a)isoformsinplasma(29).Furthermore,althoughthemolecularweightofapoB-100
isfixed,differencesbesidesvariabilityofKIV2repeatsmayexistinadditionalcomponentsof
Lp(a),suchasthecarbohydratecontentonapolipoprotein(a)andthelipidcompositionofthe
LDL,whichmayfurthercomplicatetheaccuratequantificationofLp(a)levelsbymass(33).
Otheraspectsthatimpactprecisionandreproducibilityaretheuseofdifferentdetection
antibodiesandimportantly,thelackofcommonstandardsandparticularlyuniformcalibrators.
Almostallcommerciallyavailablemethodsusepolyclonalantibodies,whichare,by
definition,isoformdependentsincepolyclonalantibodypreparationscontainheterogeneous
mixtureofantibodiesthatbindtodifferentsitesonapo(a)protein.SinceKIV2repeatsarethe
generallythemostprevalentkringles,itisexpectedthatamajorityofbindingsitesofsuch
polyclonalantibodieswillbeatKIV2repeats.Theonlyisoformindependentantibodiesusedin
recentlypublishedassays,asdefinedbyvirtueofnotbindingtoKIV2repeats,aremonoclonal
antibodya6fromtheNorthwestLipidMetabolismandDiabetesResearchLaboratoriesthat
by guest, on March 23, 2019
ww
w.jlr.org
Dow
nloaded from
13
bindstoKIV9andmonoclonalantibodyLPA4fromUCSD.Itisalsoimportanttoemphasizethat
mostcommerciallyavailableassaysmeasure“totalapo(a)”ratherthanLp(a).Sinceall
polyclonalantibodieswilllikelybindtoKIV2,ideallymonoclonalantibodiesnotbindingKIV2
shouldbeusedtoavoidtheissueofisoformsensitivity.Althoughtheissueofisoformsensitivity
hasbeenaddressedtosomeextentbycarefulselectionofcalibrators,itisquitelikelythatuse
ofpolyclonalantibodieswillalwayshavesomeisoformsensitivityifcarefullyanalyzed.
Althoughmanufacturersdonotusuallypublicallyreporttheprocessofgenerating
appropriatecalibrators,theygenerallyusepooledplasmasamplesfrommanydonorstoisolate
Lp(a).Often,suchcalibratorsetsresultfromserialdilutionsofconcentratedLp(a)values,but
canalsobeseparatepoolsofplasmathathaveameanvaluesrangingfromlowtohigh.Itis
importantthatthecalibratorsusedreflectthepresenceofthewholerangeofdifferentsized
allelesbothbetweenandwithinindividuals,andthatsuchallelesarepresentinthesample
beingmeasured.Afurtherdisadvantageofusinghumanpooledplasmaforcalibratorsisthat
eachbatchchangesaccordingtotheavailabilityofdonorsovermonthsandyears,and
therefore,theremaybevariationeachtimeanewbatchismade.Thisissuewillbecome
increasinglyimportantasthemeasurementofLp(a)ispredictedtoincreasesubstantiallywith
availabletherapiestolowerlevelsandthemeasurementofLp(a)levelsincreasesglobally.
IdeallycalibratorsshouldbelinkedtothereferencematerialfromtheWorldHealth
Organizationtoensurerelativeisoformindependence.
Toaddressthelimitationofinter-assayvariation,manyinvestigatorssuggesttheuseof
apolipoprotein(a)isoform-independentassayscorrectedwithinternationalsecondaryLp(a)
references.AlsotheproposalhasbeenmadetodeterminetheconcentrationofLp(a)as
by guest, on March 23, 2019
ww
w.jlr.org
Dow
nloaded from
14
particlenumberreportedinnmol/L,preferablyusingthereferencestandardofthe
InternationalFederationofClinicalChemistryasawaytominimizetheissuesrelatedto
variabilityinLp(a)mass(33,34).ThisWorldHealthOrganizationapprovedstandard,withan
Lp(a)concentrationof107nmol/Land21KIVrepeats,ensuresafixedandapo(a)isoform
independentmeasurementofthemolarconcentrationsofLp(a)(3).Althoughonecanroughly
convertmg/dLtonmol/Lwitharatioof~2.4,inreality,thisisnotappropriateandshouldnot
becarriedoutasitdependsonknowingtheunderlyingisoformnumbersaswellashavinga
fixedconcentrationofthelipidandcarbohydratecontentoftheLp(a),whichareusuallynot
known(35).Ultimately,theuseofmolar-basedmeasurescoupledwithadvancesinappropriate
gold-standardcalibratorswithouttheneedofpooledplasma,willpavethewaytofully
standardizetheseassays,improveclinicaldecision-making,aswellasoptimizeclinicaltrial
designwithnewtherapeuticapproaches.
AswehavepreviouslyshownintheEPIC-Norfolkcohort,highLp(a)levelswerestrongly
associatedwithanincreasedriskofCAD(13,14).Theseobservationsareconsistentwiththe
EASconsensusstatement,andmultiplestudiesandmeta-analysesconsistentlydemonstratinga
curvilinearcorrelationbetweenLp(a)levelsandincreasedriskofcardiovasculardisease(2,5,
13).Inthecurrentstudy,independentofthetypeofassayorthesexofthestudyparticipants,
bothLp(a)levelsinexcessof50mg/dlorabovethe5thquintile(or80thpercentile)were
correlatedwithincreasedCADrisk.The80thpercentilecut-offvalues,inapopulationenriched
inCADcases,of36mg/dlfortheRandoxassayand24mg/dlfortheUCSDassaywere
considerablylowerthantheEASproposedthresholdof50mg/dl,butareconsistentwith
epidemiologicalandtrialdata(2,5,20,21).Thisdiscrepancyisrelevantbecauseclinical
by guest, on March 23, 2019
ww
w.jlr.org
Dow
nloaded from
15
decision-makingissuggestedtobemadeonthe50mg/dlthresholdinEurope,althoughmost
USlaboratoriesuse>30mg/dLaselevatedrisk(36).Asshownbymendelianrandomization
studiesattheprimarycarelevel(20),thatCVDriskassociatedwithLp(a)beginsatmuchlower
levelsthan50mg/dLandimpliesthatthelevelof50mg/dLisarbitrarybasedonpopulation
cutoffsandnotevidencebasedonCVDrisk.Anotherwaytobypassspecificthresholdsisto
determineassayspecific80thpercentilethresholds.Inthisway,theeffectofinter-assay
variationisminimized,becauseeachassayhasitsowncut-offvalue.Forthistowork,itisvital
todetermineLp(a)levelsofabroadrangeofpersons.Althoughlessfavorablethanamethod
basedoninternationalstandardsandcalibratorsitcanbeagoodinterimsolution.Finally,it
wasrecentlyshownintheMESAstudythatrace-specificlevelsofLp(a)mayalsoneedtobe
institutedduetodifferencesinthethresholdsandpredictivevaluesforCHDacrossraces(37).
However,hewaslimitedbylownumberofcardiovasculareventsandwideconfidenceintervals
inthePointestimates,suggestinganeedforconfirmationofthesefindings.Futurestudies,as
wellasclinicaltrialswithnoveldrugs,(6-10)willhavetotakeintoaccountwhattheappropriate
riskthresholdistotestthehypothesisthatLp(a)loweringpreventsCVDevents.
Limitationsofthisstudyarethatitonlyincludedoneepidemiologicalcohort,whichwas
primarilyCaucasian,andalsoonlycomparedtwoassays.Furtherstudiescomparingavarietyof
assaysindiversepopulationswillbeneededtoconfirmtheseresults
Inconclusion,theseresultsdemonstratethatevenlowercut-offvaluesofLp(a)couldbe
clinicallysignificantandtheuseofdifferentassayscouldhavelargeimpactonclinicaldecision
making.WiththearrivalofpotentdrugstolowerLp(a)to“normal”levels,fullstandardization
by guest, on March 23, 2019
ww
w.jlr.org
Dow
nloaded from
16
ofassaymethodologieswillbeneededtoultimatelyoptimizeclinicaldecision-makingforthe
estimated>1billionpeoplewithpotentiallyatherogenicLp(a)levels(38).
Funding
ThisworkwassupportedbytheEPIC-NorfolkStudyisfundedbyCancerResearchUK
grantnumber14136andtheMedicalResearchCouncilgrantnumberG1000143.Thefunders
hadnoroleinthestudydesign,datacollection,analysis,decisiontopublishorpreparationof
themanuscript.DrsTsimikasandWitztumaresupportedbyNIHR01grantsHL119828,P01-
HL088093,P01HL055798,R01-HL106579,R01-HL078610,andR01-HL124174.
Disclosures
Drs.TsimikasandWitztumareco-inventorsandreceiveroyaltiesfrompatentsowned
bytheUniversityofCaliforniaSanDiegoonoxidation-specificantibodiesandofbiomarkers
relatedtooxidizedlipoproteins.Dr.WitztumisaconsultanttoIonisPharmaceuticalsand
InterceptPharmaceuticals.Dr.TsimikascurrentlyholdsadualappointmentatUCSDandIonis
Pharmaceuticals.Theotherauthorshavenopotentialconflictstodeclare.
Acknowledgements
TheauthorswishtothanktheparticipantsandstaffoftheEPIC-Norfolkprospective
populationstudy.
by guest, on March 23, 2019
ww
w.jlr.org
Dow
nloaded from

17
References
1. Erqou,S.,S.Kaptoge,P.L.Perry,E.DiAngelantonio,A.Thompson,I.R.White,S.M.
Marcovina,R.Collins,S.G.Thompson,andJ.Danesh.2009.Lipoprotein(a)concentrationand
theriskofcoronaryheartdisease,stroke,andnonvascularmortality.JAMA302:412-423.
2. Nordestgaard,B.G.,M.J.Chapman,K.Ray,J.Boren,F.Andreotti,G.F.Watts,H.
Ginsberg,P.Amarenco,A.Catapano,O.S.Descamps,E.Fisher,P.T.Kovanen,J.A.
Kuivenhoven,P.Lesnik,L.Masana,Z.Reiner,M.R.Taskinen,L.Tokgozoglu,A.Tybjaerg-Hansen,
andP.EuropeanAtherosclerosisSocietyConsensus.2010.Lipoprotein(a)asacardiovascular
riskfactor:currentstatus.EurHeartJ31:2844-2853.
3. Marcovina,S.M.,J.J.Albers,A.M.Scanu,H.Kennedy,F.Giaculli,K.Berg,R.Couderc,F.
Dati,N.Rifai,I.Sakurabayashi,J.R.Tate,andA.Steinmetz.2000.Useofareferencematerial
proposedbytheInternationalFederationofClinicalChemistryandLaboratoryMedicineto
evaluateanalyticalmethodsforthedeterminationofplasmalipoprotein(a).ClinChem46:
1956-1967.
4. Lamon-Fava,S.,S.M.Marcovina,J.J.Albers,H.Kennedy,C.Deluca,C.C.White,L.A.
Cupples,J.R.McNamara,L.J.Seman,V.Bongard,andE.J.Schaefer.2011.Lipoprotein(a)levels,
apo(a)isoformsize,andcoronaryheartdiseaseriskintheFraminghamOffspringStudy.JLipid
Res52:1181-1187.
5. Erqou,S.,A.Thompson,E.DiAngelantonio,D.Saleheen,S.Kaptoge,S.Marcovina,andJ.
Danesh.2010.Apolipoprotein(a)isoformsandtheriskofvasculardisease:Systematicreviewof
40studiesinvolving58,000participants.JAmCollCardiol55:2160-2167.
6. Handa,J.T.,M.Tagami,K.Ebrahimi,G.Leibundgut,A.Janiak,J.L.Witztum,andS.
Tsimikas.2015.Lipoprotein(A)withAnIntactLysineBindingSiteProtectstheRetinaFroman
Age-RelatedMacularDegenerationPhenotypeinMice(AnAmericanOphthalmologicalSociety
Thesis).TransAmOphthalmolSoc113:T51-T522.
7. Gaudet,D.,D.J.Kereiakes,J.M.McKenney,E.M.Roth,C.Hanotin,D.Gipe,Y.Du,A.C.
Ferrand,H.N.Ginsberg,andE.A.Stein.2014.Effectofalirocumab,amonoclonalproprotein
convertasesubtilisin/kexin9antibody,onlipoprotein(a)concentrations(apooledanalysisof
150mgeverytwoweeksdosingfromphase2trials).AmJCardiol114:711-715.
by guest, on March 23, 2019
ww
w.jlr.org
Dow
nloaded from
18
8. Raal,F.J.,R.P.Giugliano,M.S.Sabatine,M.J.Koren,G.Langslet,H.Bays,D.Blom,M.
Eriksson,R.Dent,S.M.Wasserman,F.Huang,A.Xue,M.Albizem,R.Scott,andE.A.Stein.
2014.Reductioninlipoprotein(a)withPCSK9monoclonalantibodyevolocumab(AMG145):a
pooledanalysisofmorethan1,300patientsin4phaseIItrials.JAmCollCardiol63:1278-1288.
9. Cannon,C.P.,S.Shah,H.M.Dansky,M.Davidson,E.A.Brinton,A.M.Gotto,M.
Stepanavage,S.X.Liu,P.Gibbons,T.B.Ashraf,J.Zafarino,Y.Mitchel,P.Barter,E.Determining
the,andI.Tolerability.2010.Safetyofanacetrapibinpatientswithorathighriskforcoronary
heartdisease.NEnglJMed363:2406-2415.
10. Santos,R.D.,F.J.Raal,A.L.Catapano,J.L.Witztum,E.Steinhagen-Thiessen,andS.
Tsimikas.2015.Mipomersen,anantisenseoligonucleotidetoapolipoproteinB-100,reduces
lipoprotein(a)invariouspopulationswithhypercholesterolemia:resultsof4phaseIIItrials.
ArteriosclerThrombVascBiol35:689-699.
11. Day,N.,S.Oakes,R.Luben,K.T.Khaw,S.Bingham,A.Welch,andN.Wareham.1999.
EPIC-Norfolk:studydesignandcharacteristicsofthecohort.EuropeanProspectiveInvestigation
ofCancer.BrJCancer80Suppl1:95-103.
12. Boekholdt,S.M.,R.J.Peters,N.E.Day,R.Luben,S.A.Bingham,N.J.Wareham,C.E.
Hack,P.H.Reitsma,andK.T.Khaw.2004.Macrophagemigrationinhibitoryfactorandtherisk
ofmyocardialinfarctionordeathduetocoronaryarterydiseaseinadultswithoutprior
myocardialinfarctionorstroke:theEPIC-NorfolkProspectivePopulationstudy.AmJMed117:
390-397.
13. Tsimikas,S.,Z.Mallat,P.J.Talmud,J.J.Kastelein,N.J.Wareham,M.S.Sandhu,E.R.
Miller,J.Benessiano,A.Tedgui,J.L.Witztum,K.T.Khaw,andS.M.Boekholdt.2010.Oxidation-
specificbiomarkers,lipoprotein(a),andriskoffatalandnonfatalcoronaryevents.JAmColl
Cardiol56:946-955.
14. Gurdasani,D.,B.Sjouke,S.Tsimikas,G.K.Hovingh,R.N.Luben,N.W.Wainwright,C.
Pomilla,N.J.Wareham,K.T.Khaw,S.M.Boekholdt,andM.S.Sandhu.2012.Lipoprotein(a)
andriskofcoronary,cerebrovascular,andperipheralarterydisease:TheEPIC-Norfolk
ProspectivePopulationStudy.ArteriosclerThrombVascBiol32:3058-3065.
by guest, on March 23, 2019
ww
w.jlr.org
Dow
nloaded from
19
15. Tsimikas,S.,H.K.Lau,K.R.Han,B.Shortal,E.R.Miller,A.Segev,L.K.Curtiss,J.L.
Witztum,andB.H.Strauss.2004.Percutaneouscoronaryinterventionresultsinacuteincreases
inoxidizedphospholipidsandlipoprotein(a):short-termandlong-termimmunologicresponses
tooxidizedlow-densitylipoprotein.Circulation109:3164-3170.
16. Taleb,A.,J.L.Witztum,andS.Tsimikas.2011.Oxidizedphospholipidsonapolipoprotein
B-100(OxPL/apoB)containinglipoproteins:Abiomarkerpredictingcardiovasculardiseaseand
cardiovascularevents.BiomarkersMed5:673-694.
17. Tsimikas,S.,J.L.Witztum,E.R.Miller,W.J.Sasiela,M.Szarek,A.G.Olsson,andG.G.
Schwartz.2004.High-doseatorvastatinreducestotalplasmalevelsofoxidizedphospholipids
andimmunecomplexespresentonapolipoproteinB-100inpatientswithacutecoronary
syndromesintheMIRACLtrial.Circulation110:1406-1412.
18. Willeit,P.,S.Kiechl,F.Kronenberg,J.L.Witztum,P.Santer,M.Mayr,Q.Xu,A.Mayr,J.
Willeit,andS.Tsimikas.2014.Discriminationandnetreclassificationofcardiovascularriskwith
lipoprotein(a):Prospective15-yearoutcomesintheBruneckStudy.JAmCollCardiol64:851-
860.
19. Leibundgut,G.,C.Scipione,H.Yin,M.Schneider,M.B.Boffa,S.Green,X.Yang,E.A.
Dennis,J.L.Witztum,M.L.Koschinsky,andS.Tsimikas.2013.Determinantsofbindingof
oxidizedphospholipidsonapolipoprotein(a)andlipoprotein(a).JLipidRes54:2815-2830.
20. Kamstrup,P.R.,M.Benn,A.Tybjaerg-Hansen,andB.G.Nordestgaard.2008.Extreme
lipoprotein(a)levelsandriskofmyocardialinfarctioninthegeneralpopulation:the
CopenhagenCityHeartStudy.Circulation117:176-184.
21. Kamstrup,P.R.,A.Tybjaerg-Hansen,andB.G.Nordestgaard.2013.Extreme
lipoprotein(a)levelsandimprovedcardiovascularriskprediction.JAmCollCardiol61:1146-
1156.
22. Albers,J.J.,A.Slee,K.D.O'Brien,J.G.Robinson,M.L.Kashyap,P.O.Kwiterovich,Jr.,P.
Xu,andS.M.Marcovina.2013.RelationshipofapolipoproteinsA-1andB,andlipoprotein(a)to
cardiovascularoutcomes:theAIM-HIGHtrial(AtherothrombosisInterventioninMetabolic
SyndromewithLowHDL/HighTriglycerideandImpactonGlobalHealthOutcomes).JAmColl
Cardiol62:1575-1579.
by guest, on March 23, 2019
ww
w.jlr.org
Dow
nloaded from

20
23. Nestel,P.J.,E.H.Barnes,A.M.Tonkin,J.Simes,M.Fournier,H.D.White,D.M.
Colquhoun,S.Blankenberg,andD.R.Sullivan.2013.Plasmalipoprotein(a)concentration
predictsfuturecoronaryandcardiovasculareventsinpatientswithstablecoronaryheart
disease.ArteriosclerThrombVascBiol33:2902-2908.
24. Kraft,H.G.,C.Sandholzer,H.J.Menzel,andG.Utermann.1992.Apolipoprotein(a)
allelesdeterminelipoprotein(a)particledensityandconcentrationinplasma.Arterioscler
Thromb12:302-306.
25. Marcovina,S.M.,H.H.Hobbs,andJ.J.Albers.1996.Relationbetweennumberof
apolipoprotein(a)kringle4repeatsandmobilityofisoformsinagarosegel:basisfora
standardizedisoformnomenclature.ClinicalChemistry42:436-439.
26. Clarke,R.,J.F.Peden,J.C.Hopewell,T.Kyriakou,A.Goel,S.C.Heath,S.Parish,S.
Barlera,M.G.Franzosi,S.Rust,D.Bennett,A.Silveira,A.Malarstig,F.R.Green,M.Lathrop,B.
Gigante,K.Leander,U.deFaire,U.Seedorf,A.Hamsten,R.Collins,H.Watkins,M.Farrall,and
P.C.the.2009.GeneticvariantsassociatedwithLp(a)lipoproteinlevelandcoronarydisease.N
EnglJMed361:2518-2528.
27. Luke,M.M.,J.P.Kane,D.M.Liu,C.M.Rowland,D.Shiffman,J.Cassano,J.J.Catanese,
C.R.Pullinger,D.U.Leong,A.R.Arellano,C.H.Tong,I.Movsesyan,J.Naya-Vigne,C.Noordhof,
N.T.Feric,M.J.Malloy,E.J.Topol,M.L.Koschinsky,J.J.Devlin,andS.G.Ellis.2007.A
polymorphismintheprotease-likedomainofapolipoprotein(a)isassociatedwithsevere
coronaryarterydisease.ArteriosclerThrombVascBiol27:2030-2036.
28. Chasman,D.I.,D.Shiffman,R.Y.Zee,J.Z.Louie,M.M.Luke,C.M.Rowland,J.J.
Catanese,J.E.Buring,J.J.Devlin,andP.M.Ridker.2009.Polymorphisminthe
apolipoprotein(a)gene,plasmalipoprotein(a),cardiovasculardisease,andlow-doseaspirin
therapy.Atherosclerosis203:371-376.
29. Boerwinkle,E.,C.C.Leffert,J.Lin,C.Lackner,G.Chiesa,andH.H.Hobbs.1992.
Apolipoprotein(a)geneaccountsforgreaterthan90%ofthevariationinplasmalipoprotein(a)
concentrations.JClinInvest90:52-60.
30. Kronenberg,F.,andG.Utermann.2013.Lipoprotein(a):resurrectedbygenetics.JInt
Med273:6-30.
by guest, on March 23, 2019
ww
w.jlr.org
Dow
nloaded from

21
31. Hoover-Plow,J.,andM.Huang.2013.Lipoprotein(a)metabolism:potentialsitesfor
therapeutictargets.Metabolism:ClinExper62:479-491.
32. Marcovina,S.M.,J.J.Albers,B.Gabel,M.L.Koschinsky,andV.P.Gaur.1995.Effectof
thenumberofapolipoprotein(a)kringle4domainsonimmunochemicalmeasurementsof
lipoprotein(a).Clinicalchemistry41:246-255.
33. Marcovina,S.M.,M.L.Koschinsky,J.J.Albers,andS.Skarlatos.2003.Reportofthe
NationalHeart,Lung,andBloodInstituteworkshoponlipoprotein(a)andcardiovascular
disease:Recentadvancesandfuturedirections.ClinChem49:1785-1796.
34. Dati,F.,J.R.Tate,S.M.Marcovina,A.Steinmetz,C.InternationalFederationofClinical,
M.Laboratory,andI.W.G.f.L.A.Standardization.2004.FirstWHO/IFCCIinternational
referencereagentforlipoprotein(a)forimmunoassay--Lp(a)SRM2B.ClinChemLabMed42:
670-676.
35. Brown,W.V.,C.M.Ballantyne,P.H.Jones,andS.Marcovina.2010.Managementof
Lp(a).JClinLipidol4:240-247.
36. Kostner,G.M.,P.Avogaro,G.Cazzolato,E.Marth,G.Bittolo-Bon,andG.B.Qunici.
1981.LipoproteinLp(a)andtheriskformyocardialinfarction.Atherosclerosis38:51-61.
37. Guan,W.,J.Cao,B.T.Steffen,W.S.Post,J.H.Stein,M.C.Tattersall,J.D.Kaufman,J.P.
McConnell,D.M.Hoefner,R.Warnick,andM.Y.Tsai.2015.Raceisakeyvariableinassigning
lipoprotein(a)cutoffvaluesforcoronaryheartdiseaseriskassessment:theMulti-EthnicStudy
ofAtherosclerosis.ArteriosclerThrombVascBiol35:996-1001.
38. Tsimikas,S.,andJ.H.Hall.2012.Lipoprotein(a)asapotentialcausalgeneticriskfactor
ofcardiovasculardisease:Arationaleforincreasedeffortstounderstanditspathophysiology
anddeveloptargetedtherapies.JAmCollCardiol60:716-721.
by guest, on March 23, 2019
ww
w.jlr.org
Dow
nloaded from
22
FIGURELEGENDS
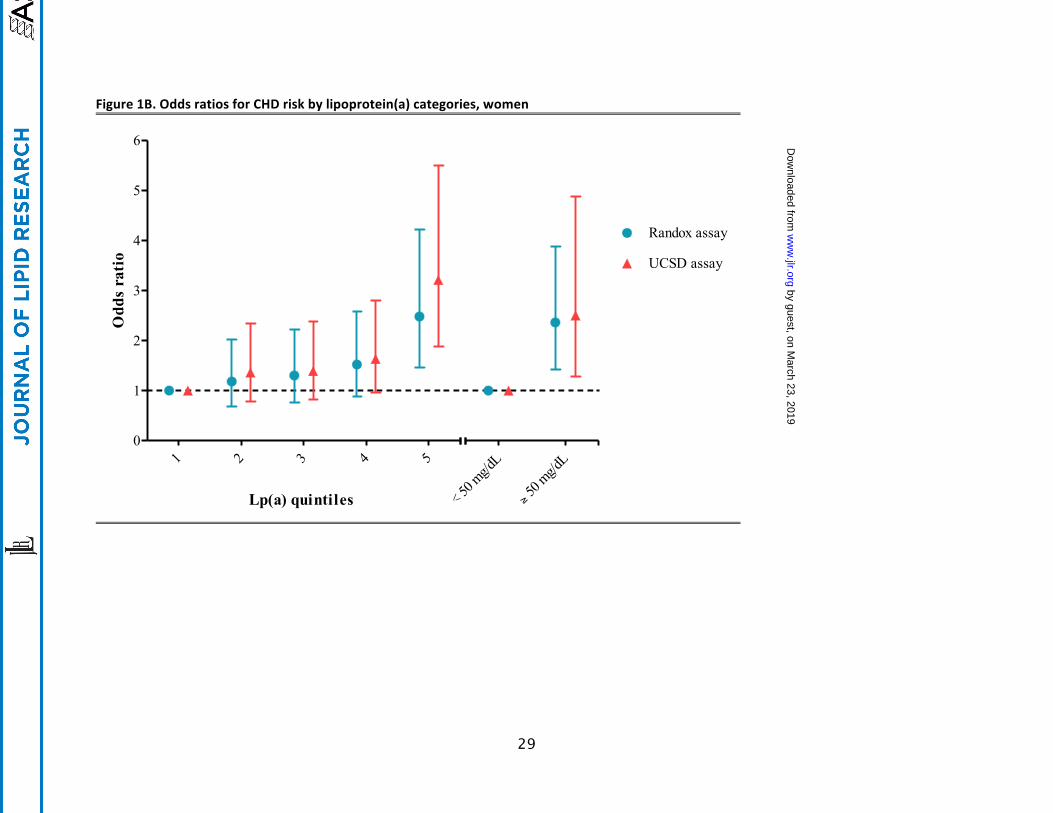
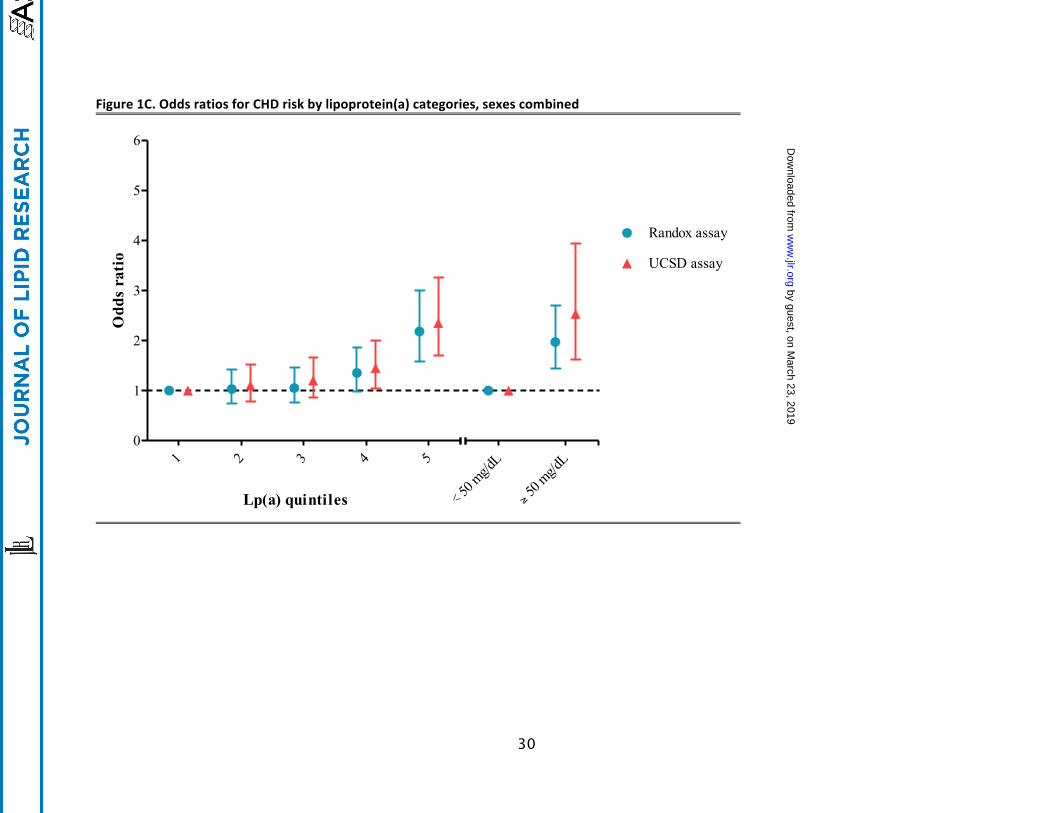
Figure1.OddsratiosforCHDriskbylipoprotein(a)categoriesformen(A),women(B)andboth
sexescombined(C).Dataarepresentedassex-specific,age-adjustedoddsratioswith
corresponding95%confidenceintervallimits.Oddsratiosperquintilewiththelowestquintile
asreferencecategory.Inaddition,anoddsratioispresentedforpeoplewithLp(a)>50mg/dL,
usingthosewithLp(a)<50mg/dLasreferencecategory.Lp(a)=lipoprotein(a),UCSD=
UniversityofCalifornia,SanDiego.
Figure2.Bland-AltmananalysisoftheaverageoftheUCSDandRandoxassaysplottedagainst
themeandifference.Dataarepresentedasdifferenceinmeasurements(Randox-UCSD)in
mg/dL,mean,lower95%limitofagreement(mean-1.96SD)andupper95%limitofagreement
(mean+1.96SD).AverageofRandoxandUCSDassaywerecalculated.UCSD=UniversityofSan
Diego.
by guest, on March 23, 2019
ww
w.jlr.org
Dow
nloaded from
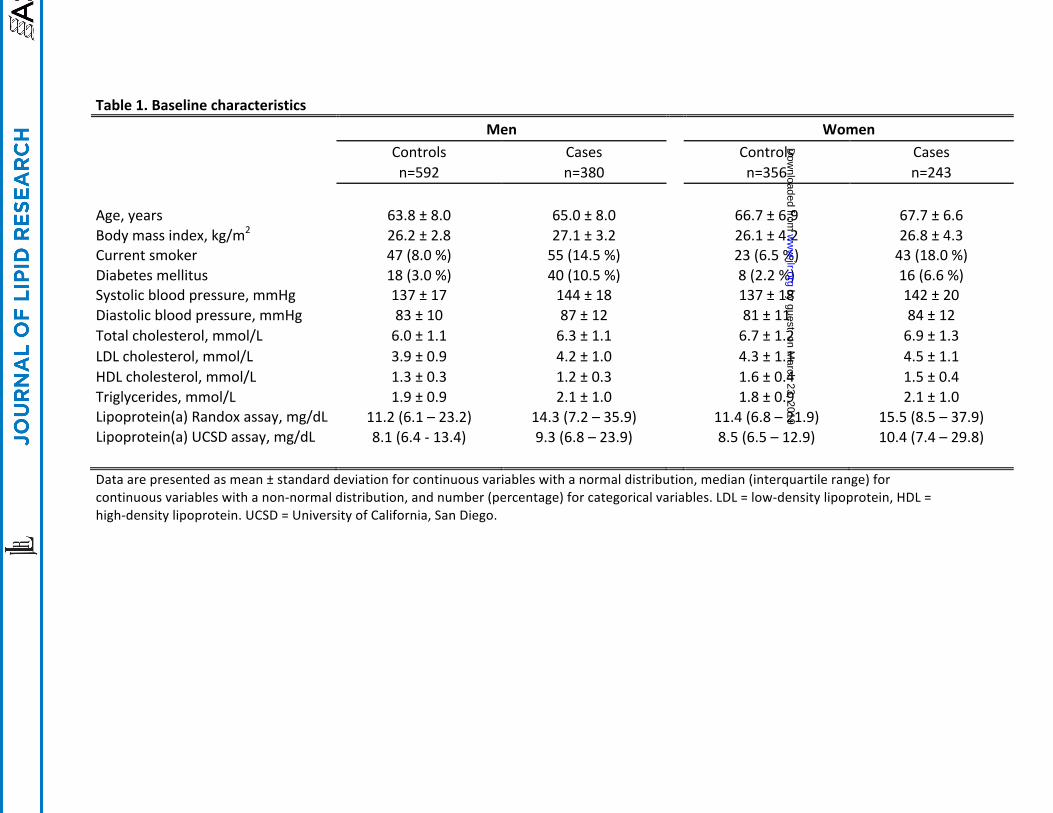
Table1.Baselinecharacteristics
Men Women
Controls Cases Controls Cases
n=592 n=380 n=356 n=243
Age,years 63.8±8.0 65.0±8.0 66.7±6.9 67.7±6.6Bodymassindex,kg/m2 26.2±2.8 27.1±3.2 26.1±4.2 26.8±4.3Currentsmoker 47(8.0%) 55(14.5%) 23(6.5%) 43(18.0%)Diabetesmellitus 18(3.0%) 40(10.5%) 8(2.2%) 16(6.6%)Systolicbloodpressure,mmHg 137±17 144±18 137±18 142±20Diastolicbloodpressure,mmHg 83±10 87±12 81±11 84±12Totalcholesterol,mmol/L 6.0±1.1 6.3±1.1 6.7±1.2 6.9±1.3LDLcholesterol,mmol/L 3.9±0.9 4.2±1.0 4.3±1.1 4.5±1.1HDLcholesterol,mmol/L 1.3±0.3 1.2±0.3 1.6±0.4 1.5±0.4Triglycerides,mmol/L 1.9±0.9 2.1±1.0 1.8±0.9 2.1±1.0Lipoprotein(a)Randoxassay,mg/dL 11.2(6.1–23.2) 14.3(7.2–35.9) 11.4(6.8–21.9) 15.5(8.5–37.9)Lipoprotein(a)UCSDassay,mg/dL 8.1(6.4-13.4) 9.3(6.8–23.9) 8.5(6.5–12.9) 10.4(7.4–29.8) Dataarepresentedasmean±standarddeviationforcontinuousvariableswithanormaldistribution,median(interquartilerange)forcontinuousvariableswithanon-normaldistribution,andnumber(percentage)forcategoricalvariables.LDL=low-densitylipoprotein,HDL=high-densitylipoprotein.UCSD=UniversityofCalifornia,SanDiego.
by guest, on March 23, 2019
ww
w.jlr.org
Dow
nloaded from
24
Table2A.DistributionofCHDcasesandcontrolsbylipoprotein(a)categories,UCSDassay
UCSDassay
Lp(a)quintiles
1 2 3 4 5 ≥30.0mg/dL ≥50.0mg/dL
Men Lp(a)range,mg/dL 3.4–6.2 6.2–7.6 7.6–9.8 9.8–23.1 23.1-89.5 30,4-89.5 50.0–89.5
Lp(a)mean,mg/dL 5.5±0.5 6.8±0.4 8.5±0.6 13.8±3.9 41.8±15.0 47.1±13.7 63.6±10.0Cases/controls,n/n 66/128 63/132 73/121 82/113 96/98 71/74 29/19Cases,%oftotal 34 32.3 37.6 42.1 49.5 49 60.4Total,n 194 195 194 195 194 145 48
Women Lp(a)range,mg/dL 4.6–6.4 6.4–8.0 8.0–10.6 10.6–25.7 25.8-99.7 30.1-99.7 50.4–99.7
Lp(a)mean,mg/dL 5.7±0.4 7.2±0.4 9.2±0.7 14.6±3.9 45.5±15.8 48.1±15.4 64.9±11.7Cases/controls,n/n 84/35 44/76 45/75 50/70 69/51 60/44 24/15Cases,%oftotal 29.4 36.7 37.5 41.7 57.5 57.7 61.5Total,n 119 120 120 120 120 104 39
Combined Lp(a)range,mg/dL 3.4–6.3 6.3–7.7 7.7–10.2 10.1–23.8 24.0–99.7 30.1-99.7 50.0–99.7
Lp(a)mean,mg/dL 5.6±0.5 7.0±0.4 8.8±0.6 14.1±3.9 43.2±15.0 47.5±14.4 64.2±10.7Cases/controls,n/n 102/212 109/205 116/199 130/184 166/148 131/118 53/34Cases,%oftotal 32.5 34.7 36.8 41.4 52.9 52.6 60.9Total,n 314 314 315 314 314 249 87Dataarepresentedasmean±standarddeviation,numberorpercentage.Forthecategorymenandwomen,sexspecificquintileswerecalculated.Forthecategorycombinedpooledquintileswerecalculated.Lp(a)=lipoprotein(a),UCSD=UniversityofCalifornia,SanDiego.Lp(a)rangesforeachquintilerepresentsthe~cutoffvalues.
by guest, on March 23, 2019
ww
w.jlr.org
Dow
nloaded from
25
Table2B.DistributionofCHDcasesandcontrolsbylipoprotein(a)categories,Randoxassay
Randoxassay
Lp(a)quintiles
1 2 3 4 5 ≥30.0mg/dL ≥50.0mg/dL
Men Lp(a)range,mg/dL 2.2–5.5 5.5–9.5 9.5–15.9 16.0–34.8 34.9–162.3 30.2-162.3 50.2–162.3
Lp(a)mean,mg/dL 3.8±0.8 7.4±1.1 12.2±1.8 23.1±5.3 58.3±23.5 55.2±23.6 72.9±23.6Cases/controls,n/n 65/128 70/125 65/130 83/112 97/97 108/113 52/52Cases,%oftotal 33.7 35.9 33.3 42.6 50 48.9 50Total,n 193 195 195 195 194 221 104
Women
Lp(a)range,mg/dL 2.2–6.4 6.4–10.3 10.3–16.6 16.7–36.8 37.0–143.5 30.2-143.5 50.1–143.5Lp(a)mean,mg/dL 4.4±1.1 8.3±1.1 12.9±1.8 24.8±6.1 63.2±24.5 57.8±24.8 75.6±24.0Cases/controls,n/n 38/81 43/77 46/74 51/69 65/55 82/65 43/30Cases,%oftotal 31.9 35.8 38.3 42.5 54.2 55.8 61.4Total,n 119 120 120 120 120 147 73
Combined
Lp(a)range,mg/dL 2.2–5.8 5.9–9.8 9.8–16.2 16.2–35.4 35.6–162.3 30.2-162.3 50.1–162.3Lp(a)mean,mg/dL 4.0±0.8 7.8±1.1 12.5±1.8 23.8±5.3 60.2±23.5 56.2±24.1 74.0±23.7Cases/controls,n/n 107/208 109/205 111/203 130/184 166/148 190/178 95/82Cases,%oftotal 34 34.7 35.4 41.4 52.9 51.6 55.2Total,n 315 314 314 314 314 368 177Dataarepresentedasmean±standarddeviation,numberorpercentage.Forthecategorymenandwomen,sexspecificquintileswerecalculated.Forthecategorycombinedpooledquintileswerecalculated.Lp(a)=lipoprotein(a).Lp(a)rangesforeachquintilerepresentthecutoffvalues.Lp(a)rangesforeachquintilerepresentsthe~cutoffvalues.
by guest, on March 23, 2019
ww
w.jlr.org
Dow
nloaded from
26
Table3.OddsratiosforCHDriskbylipoprotein(a)categories Lp(a)quintiles
1 2 3 4 5 <50.0mg/dL ≥50.0mg/dL
Men Randoxassay 1.00 1.10 0.97 1.45 1.99
1.00 1.74
(0.72-1.67) (0.64-1.49) (0.96-2.19) (1.32-3.01)
(1.15-2.62)
UCSDassay 1.00 0.93 1.17 1.41 1.95
1.00 2.55
(0.61-1.42) (0.77-1.78) (0.93-2.13) (1.29-2.94)
(1.41-4.63)
Women Randoxassay 1.00 1.18 1.30 1.52 2.48
1.00 2.36
(0.69-2.01) (0.76-2.21) (0.89-2.58) (1.46-4.21)
(1.43-3.89) UCSDassay 1.00 1.36 1.39 1.63 3.21
1.00 2.50
(0.79-2.34) (0.81-2.39) (0.95-2.79) (1.88-5.49)
(1.28-4.87)
Combined Randoxassay 1.00 1.03 1.05 1.35 2.18
1.00 1.97
(0.74-1.43) (0.75-1.46) (0.98-1.87) (1.58-3.01)
(1.43-2.70) UCSDassay 1.00 1.10 1.20 1.45 2.35
1.00 2.53
(0.79-1.53) (0.86-1.67) (1.04-2.01) (1.70-3.26) (1.62-3.95) Dataarepresentedasoddsratioswithcorresponding95%confidenceintervallimits.Forthecategorymenandwomen,sex-specific,
age-adjustedoddsratioswerecalculated,withtheLp(a)cut-offvaluesaspresentedintable2.Forthecategorycombinedsex-andage-adjustedoddsratioswerecalculated,withtheLp(a)cut-offvaluesaspresentedintable2.Oddsratiosperquintilewiththelowestquintileasreferencecategory.Inaddition,anoddsratioispresentedforpeoplewithLp(a)>50mg/dL,usingthosewithLp(a)<50mg/dLasreferencecategory.Lp(a)=lipoprotein(a),UCSD=UniversityofCalifornia,SanDiego.
by guest, on March 23, 2019
ww
w.jlr.org
Dow
nloaded from
27
Table4.NumberofstudyparticipantswithanLp(a)level<and≥50mg/dLperassay
UCSDassay
Randoxassay
Lp(a) <50.0mg/dL ≥50.0mg/dL
Men <50.0mg/dL 861 63 ≥50.0mg/dL 7 41
Women <50.0mg/dL 525 35 ≥50.0mg/dL 1 38
Combined <50.0mg/dL 1386 98 ≥50.0mg/dL 8 79
Datearepresentedasnumbers.Lp(a)=lipoprotein(a),UCSD=UniversityofCalifornia,SanDiego.
by guest, on March 23, 2019
ww
w.jlr.org
Dow
nloaded from
28
Figure1A.OddsratiosforCHDriskbylipoprotein(a)categories,men
1 2 3 4 50
1
2
3
4
5
6
Randox assay
UCSD assay
< 50 m
g/dL
≥ 50 m
g/dL
Lp(a) quintiles--------------------------
Odd
s ra
tio
by guest, on March 23, 2019
ww
w.jlr.org
Dow
nloaded from
29
Figure1B.OddsratiosforCHDriskbylipoprotein(a)categories,women
1 2 3 4 50
1
2
3
4
5
6
Randox assay
UCSD assay
< 50 m
g/dL
≥ 50 m
g/dL
Lp(a) quintiles------------------------
Odd
s ra
tio
by guest, on March 23, 2019
ww
w.jlr.org
Dow
nloaded from
30
Figure1C.OddsratiosforCHDriskbylipoprotein(a)categories,sexescombined
1 2 3 4 50
1
2
3
4
5
6
Randox assay
UCSD assay
< 50 m
g/dL
≥ 50 m
g/dL
Lp(a) quintiles--------------------------
Odd
s ra
tio
by guest, on March 23, 2019
ww
w.jlr.org
Dow
nloaded from
31
Figure2.Bland-AltmanplotRandoxvs.UCSDRandoxassay
0 20 40 60 80 100
120
-40
-20
0
20
40
60
80
100
120
Mean - 1.96SD
Mean + 1.96SD
Mean
Average of Randox and UCSD assay (mg/dL)
Dif
fere
nce
in m
easu
rem
ents
(Ran
dox
- UC
SD) (
mg/
dL)
by guest, on March 23, 2019
ww
w.jlr.org
Dow
nloaded from
Recommended