Mauro PapottiM. Volante, F.
Maletta, J. Metovic
University of TurinItaly
POORLY DIFFERENTIATED
THYROID CARCINOMA
Veenendaal, April 13, 2018

WHO CLASSIFICATION OF ENDOCRINE TUMORS
June 2017

WHO 2017
Hobnail var.

PD thyroid carcinoma definition
2004 2017
Follicular-cell neoplasm that show limited evidence of structural follicular cell differen-tiation and is both morphologically and beha-viorally an intermediate position between differentiated (follicular & papillary cancers) and undifferentiated (anaplastic) carcinomas.

YES !!
AGGRESSIVE THYROID CARCINOMAS
What are wetalking about?

AGGRESSIVE THYROID CARCINOMAS
-Histotype: PDTC, tall cell, columnar, solid, hobnail PTCs, Hurthle ca…. -High tumor stage: ETE (pT4 vs pT3) -Role of early RAI therapy-Prognostic markers any reliable ? PDGFRa & p-mTor may predict resistanceto RAI -Molecular profiles BRAF mutations, TERT promoter mutations, STRN/ALK fusion, p53
Lopez-Campistrous EBioMed 2016;12:86-97 Tavares. Surgery 2016 Aug

FTC
PTC
Good
ATCClassic
Follicular
Minimallyinvasive
Widelyinvasive POORLY
DIFFERENTIATED CA.
Well diff. Undiff.
Poor
DIFFERENTIATION
PROGNOSIS
Angiosarcoma
AGGRESSIVE THYROID CANCERS
Aggressive variants

TG
•Poorly differentiated carcinoma (1963)
•Insular carcinoma (1984)
•Primordial cell carcinoma (1993)
•Solid / Trabecular carcinoma•Intermediate type carcinoma•Less-well differentiated carcinoma
including extra thyroid ovary locations
Does PD carcinoma exist?
YES, since the WHO 2004 scheme
Proposednames

PD ca • Wuchernde struma
1907 1988
Bern Turin

Any associated condition?
YES (association or transition)
1- Nodular goiter (easy distinction)2- WD carcinoma
PTC (difficult if solid variant PTC) FTC (difficult if solid & few mitoses)
1% US 2% South East Asia6% Italy (Alpine area)
PD ca - Incidence
Varallo Sesia, Italy
Yu. Endocr Metab Seoul 2017 Win. Indian J Pathol Microb 2017

> growth pattern (solid/trabecular/insular)?
PD ca: Diagnostic controversy since 1983
1984
1983
1993
High grade features (mitoses >5 & necrosis) are similarly prognostic as the Turin proposalGnemmi, Aubert. PD thyroid carcinomas: application of the Turin proposal provides prognostic results similar to those from the assessment of high-grade features. Histopathol 2014;64:263-73
2006
> Or high grade features?
> Or both??

PD carcinoma
SOLID
INSULAR
TRABECULAR
Ki67 ≥ 4% predicts survival Histopathology 2014;64:263-73

MIXED
Mitoses & Necrosis

PD ca - Diagnostic clues
NO
A malignant solid trabecular tumor with non-PTC nuclei and mitoticindex >3/10HPF or necrosis, or convoluted (raisin-like) nuclei
Different patterns in different Countries
March 2006The Turinproposal
83 cases x 10 experts

Day 2
PDca
AC & others
FTC
PTC, any variant
EU USA JAP
The Turin proposal
Day 1
Dr Rosai, Turin 2006

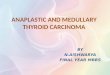
Diagnostic algorithm “Turin proposal”

The Turin proposal for PD caclassification was endorsed by
WHO 2017, page 102

PD carcinoma: high grade features

PD carcinoma PDC DM GET EVI
GET: gross extensionbeyond thyroid
Bin Xu et al.

PD carcinoma, oncocytic variant

Oncocytic PDca (“Turin proposal”) made of small/medium size cells follows a more aggressive behavior Asioli. Human Pathol 2014;45:1489
PD carcinoma, oncocytic variant
Worseprognosis

associated components

Hobnail features in AC and PDca
“Hobnail” is a rare variant of PTC associated to a more aggressive behavior. Hobnail features >10% were identified in-PD ca (4/18 cases, 22%), -anaplastic ca (1/26, 3.8%) -only 6 of 478 (1.3%) of PTC (all clinically aggressive variants).Hobnail features may be a manifestation of higher-gradetransformation.
Teng L. Hobnail variant of PTC. Oncotarget 2017;8:22023. Different molecular profile compared to classical PTC, and also to PD ca and ATC.

A- High grade features (atypias, necrosisand mitoses in S/T tumor clusters of cellblock or smears) may point to PDca, if IHC is concordant (TG dots) THY4 (or even 5).
B- A S/T growth of follicular (TG+) cellsleaves several options open
indeterminate category, as for follicularneoplasms THY 3b
Can PDca be diagnosedby FNA cytology?
depending on each case
YES/NO

-High cellularity (solid/trabecular clusters)-Discohesive, small/intermediate size cells
-Rare microfollicles and scant colloid-High mitotic activity -Mild atypia
-Necrosis
PD ca – Main features in FNA cytology
Saglietti … Bongiovanni. FNA diagnosis of PDTC. A review of the recent literature. Cytopathology 2017;28:467-474
Bongiovanni. Cancer Cytopathol 2009;117:185-194

Other solid/trabecular tumors in the thyroid
Is IHC confirmation mandatory? YES
Fetal (follicular) adenomaMedullary carcinomaThyroid ParagangliomaMetastatic NE tumorsTG
Ki67
PDca
HTT/HTASolid trabecularPTC
Parathyroidtumor

How much “poorly differentiated” needed?
Relevance of PDca diagnosis

Relevance of PDca diagnosis
In an independent series, the Turin consensus criteria reliably stratified PDCa cases, with similar overall survival compared to other series. [IMP3 was a further adverse prognostic factor in such PDCa series].
The “Turin proposal” helps to identify thyroid PDca associated to the worst survival.
Ito. World J Surg 2008;32:1535-43
Dettmer. AJSP 2011;35:1866-72 Bongiovanni. Int J Surg Path 2014
Asioli. Mod Pathol 2010;23:1269-78
10%
Rossi, Fadda. AIMM 2015;23:196-201
A minor PDC component (10%) is associated to poor prognosis as cases with extensive PDCa areas.

PD Sakam. PD WHO PD Turin
_______________________________________________
# cases 189 15 5
10 yrs DFS 77% 53.8% 25%
10 yrs survival 94.2% 80% 60%
- Aggressive clinical behavior ++

-Surgery 1st choice then early radio
iodine therapy to obtain persistent results; uptake retained in 80% of PDC. Refractory tumors increasing.
Why is an accurate PDca dx needed?
-Adverse prognostic factors: age >45, size, extrathyroidal extension, distant mets, no post-operative radioiodine therapy.
Hannallah. Int J Endocrinol2013;2013:317487
Asioli. Mod Pathol 2010;23:1269-78 Ibrahimpasic. Thyroid 2013;23:997-1002
-5-yr OS: 60-85%Kazaure. Cancer 2012;118:3260-7Ibrahimpasic. JCEM 2014;99:1245-52
-New therapies? eg somatostatin receptors SSTR5 truncated variant is highlyexpressed in PDca SSA efficacy?
Puig-Domingo. PLoS One 2014;9:e85527

Follicular adenomaRASTSH r, αGTPbp(hyperfunctioning)
HTT: RET/PTC, other?
Follicular carcinomaRAS, PAX8/PPARγ, PI3K, TSHR
Papillary carcinomaRET/PTC, TRK, BRAF, RAS, (APC, CTNNB1)
Anaplastic carcinomaBRAF, PTEN, p16, TP53
BENIGN
MALIGNANT
Molecular alterations in the spectrumof follicular cell-derived tumors
PD carcinomaRAS, PI3K, TP53 (BRAF, RET)

Genetics

Molecular data on 65 PDca classified
according to the Turinproposal
YE NIKIFOROV M VOLANTE
23%

NGS demonstrated mutations in up to 30% of PDCa, mostly in BRAF & RAS (+ PIK3CA, TP53, TSHR & others). Nikiforova. JCEM 2013;98:E1852-60
Genetics in PDca
-Mutually exclusive mutations are found in TP53 (AC: 42%; PDCa: 27%) and RAS(AC: 31%; PDCa: 18%) (p= 0.035). -PIK3CA, PTEN, & CDKI mutations in 14%-20% of PDCa and in 10%-14% of AC. -BRAF, CTNNB1, AXIN1 mutations were rare.
Pita. JCEM 2014;99:E497-507
RET/PTC rearrangements & BRAF mutations in PDca are mostlyassociated with PTC features

Using miR-23b and miR-150 as a separator, 73-79% accuracy was found in taking PDCaapart from WD thyroid cancers.
Dettmer. J Mol Endocrinol 2014;52:181-9
Some miRNAs are down regulated in PDca & AC
Horm Metab Res 2009;41:475-81
Analysis of deregulated miRNAs is helpful to distinguish
poorly differentiated thyroid carcinoma from papillary
thyroid carcinoma.
Schwertheim S, Sheu SY, Worm K, Grabellus F, Schmid KW.
Genetics / epigenetic changes
Dysregulated epigenetic candidates include the Aurora group, KMT2D, PTEN, RASSF1A, multiple non-coding RNAs (ncRNA), and the SWI/SNF chromatin-remodeling complex
Sasanakietkul T. Mol Cell Endocrinol 2017

Genetics

Genetics
From WDCa to ATC: BRAF & RAS + p53, mTor, TERT promoter, PI3K, EIF1AX, SWI/ SNF, mismatch repair, ….
PDCa
ATC

Phenotypic, molecular & prognostic features of PD ca
WHO 2017

In other tumor models predictive biomarkers of response to chemotherapy were identified, such as:-Thymid. synthase (TS) response to antifolates-ERCC1 response to cisplatin-RRM1 response to gemcitabine-Topoisomer. 2A response to etoposide (& doxo)
Therapeutic issuesCrouzeix G et al. Unusual short-term complete response to two regimens of
cytotoxic chemotherapy in a patient with PDTC. JCEM 2012;97:3046-50
Rosenbaum MW,… Faquin WC. PD-L1 and IDO1 Are Expressed in Poorly
Differentiated Thyroid Carcinoma. Endocr Pathol 2018;29:59-67.
25% PDTC were PDL1 positive. Almost one third of these also co-expressed IDO1 (indoleamine 2,3-dioxygenase). Immunocheckpoint inhibitors (+ IDO1 inhibitor) should be explored as a novel treatment modality of PDTC.

-53 PD carcinomas (Turin criteria)
-20 anaplastic carcinomas
-BRAF, NRAS and HRAS mutations-TS, ERCC1, RRM1, TOPO2A, VEGFR 1,2,3, PDGF-Rβ gene expression
Predictive gene expressionG
E l
eve
ls
TS ERCC1
PDCAAC PDCAAC
p=0.0092 p=0.0003
p=0.00002
p=0.0055
PDCAAC
PDCAACPD
GFR
βV
EG
FR
2

Gene expressionand genotype
TS RRM1
BR
AF
p=0.088R
AS wt
TOPO2A
BR
AF
RA
S wt
BR
AF
RA
S wt
p=0.087 p=0.115
BRAF: 3/73, all AC, all V600E
RAS: 14/73 (4/20 AC & 10/73
PDca), all N-RAS61
Gen
e e
xp
ress
ion
levels
COMMENTS: 1) genotype (BRAF vs RAS/wt) was associated to specific gene profiles.2) GEP of DNA synthesis/repair enzymes and vasculogenic receptors was different in PDca vs AC different responsiveness to CT & targeted tx ??

Sobrinho- Simoes M, 1990?
FOLLICULARCARCINOMA
PAPILLARYCARCINOMA
POORLYDIFFERENTIATED
CARCINOMA
UNDIFFERENTIATED
CARCINOMA
Rosai J, USCAP 2004
PDca
PTC
FTC
AC
THE STORY OF PD CA

University of Turin
Medical School
Marco Volante
Luisella Righi
Ida Rapa
Simona Vatrano
Federica Massa
Arianna Votta
Jessica Giorcelli
Stefania Izzo
Massimo DiMaio
Silvia Novello
Giorgio Scagliotti
Thank you!!
Luisa Delsedime
Francesca Maletta
Luca Molinaro
Carla Pecchioni
Chiara Musuraca
Francesca Veneziano
Jasna Metovic
Recommended