
Presentor: Christian Gallardo, MDResource: Dr. Nerissa Reyes (Neurologist) and Dr. Jesus Relos (Hematologist)Moderator: Dr. Ian Dennis FranciscoGuest Speaker: Dr. Rico Lodronio
POLYCYTHEMIA VERA AND CEREBROVASCULAR EVENTS
Objectives
To present a case of Chronic Myeloproliferative Disease such as Polycythemia Vera.
To discuss Janus Kinase 2 and its significance in diagnosing Chronic Myeloproliferative Disorder.
To discuss the relationship of Hypercoagulable State and Acute Cerebral Events such as Ischemic Strokes
General Data
D.C. 56 year old Male Bacoor Cavite Roman Catholic Admitted Jan 12, 2010

Chief Complaint:
Nape Pain
History of Present Illness
1 month
PTA
• Nape pain• (-) Headache, (-) Nausa and
Vomiting, (-) Loss of consciousness
• (-) Fever, (-) easy brusability, (-) no bleeding
• BP Taken = 160/100• ER consult.
Clonidine SL was given. Discharged
Known Hypertensive for 5 years maintained
Felodipine 5mg OD
History of Present Illness
1 weekPTA
• Nape pain• BP= 160/100
• Admitted at a local hospital in Imus, Cavite for control of BP
• Nurses noted to have concentrated blood flow when inserting IVF
• CBC revealed increase in Hgb and Hct
• Advised Hematology Consult as OPD
• Discharged
Home Medications:1. Telmisartan
(Micardis) 40 mg/ tab 1 tab OD
2. Cilostazol (Pletaal) 50mg/tab 1 tab BID
3. Bisoprolol 5mg/ tab 1 tab TID
4. Clonidine (Catapres) 75 ug/tab 1 tab SL for BP>160/100
History of Present Illness
2 daysPTA
•Nape pain•Eye redness•Flushed Face•Gum Bleeding•BP: 150/100•Had consult with AP and advised admission
Admitted

Past Medical History
Hypertension – 5 years HBP:160/100 UBP: 120 – 130/90 Medications:
Telmisartan (Micardis) 80mg/tab 1 tab OD Cilostazol 50mg/tab 1 tab TID Bisoprolol 5mg/tab 1 tab TID
(-) Diabetes Mellitus (-) Bronchial Asthma (-) Allergy (-) Previous Surgeries
Family Medical History
Hypertension – Paternal Side DM – Siblings (-) Cancer (-) Bronchial Asthma (-) Blood Dyscrasia (-) Kidney Disease (-) CVD
Past Medical History
Non-smoker Occasional Alcoholic beverage No exposure to chemicals and
toxic substances Works as a Front Desk Manager
Review of Systems
General: no weight loss, no easy fatigability
EENT: no blurring of vision, no photophobia, no ear discharge, no epistaxis
Respiratory: no colds, no cough, no hemoptysis
Cardiovascular: no chest pain, no orthopnea, no palpitations
Gastrointestinal: no abdominal pain, no diarrhea, no constipation, no hematemesis
Genitourinary: no flank pain, no frequency, no urgency
Musculoskeletal/Extremities: no joint pain
Hematology: no abnormal bleeding, no easy bruising
Physical Examination
General: Conscious, Coherent, Conversant, Not in distress
Vital Signs: BP: 150/100 RR: 18 cpm CR: 86 bpm T: 37C Skin: Warm to touch, No Rashes, No
Lesions, No Petecchiae HEENT: Anicteric Slerae, Slight Conjunctival
Effusion, Pink Palpebral Conjuctivae, (-) Tonsillopharyngeal Congestion, (-) Nasoaural Discharge, Plethoric face, (-) Neck Vein Engorgement, (-) Carotid Bruit
Physical Examination
Chest and Lung Findings: Symmetrical Chest Expansion, No Lagging, No retractions, Clear Breath Sounds
Heart: Adynamic precordium, normal rate, regular rhythm, Normal S1 and S2, (-) S3, PMI at 5th ICS LMCL, no murmur.
Admomen: Flabby, Soft, tympanitic, non-tender, Liver Edge non- palpable, Liver Span: 8 cm at the midclavicular line, Intact Traube Space, No Abdominal Bruit
Extremities: Grossly Normal Pulses, No cyanosis, No Clubbing, Flushed Skin and Palms, No Limitation of motion

Neurological Examination Cerebral:
Oriented to time, person and place Mini Mental status Exam: 30 points (-) dysarthria
Cerebellar: (-) Dysmetria (-) Dysdiadochokenisia (-) Rhomberg Test, (-) apraxia, (-) ataxia
Cranial Nerves: I: Can smell familiar odors in each nostrils II: 2-3mm PERTL, Visual Acuity :20/20, Fundoscopy: (+) ROR, Clear Media,
Distinct Cup borders, CDR: 1:3, AVR: 2:3, No exudates, No Hemorrhage III, IV, VI: Full EOM V: (+) bilateral corneal reflex, good masseter tone VII: (-) facial asymmetry VIII: Weber Test: no lateralization, Rinne‘s Test: AC>BC, (-) Nystagmus IX, X: (+) Gag Reflex XI: Can equally shrug shoulder XII: No tongue deviation
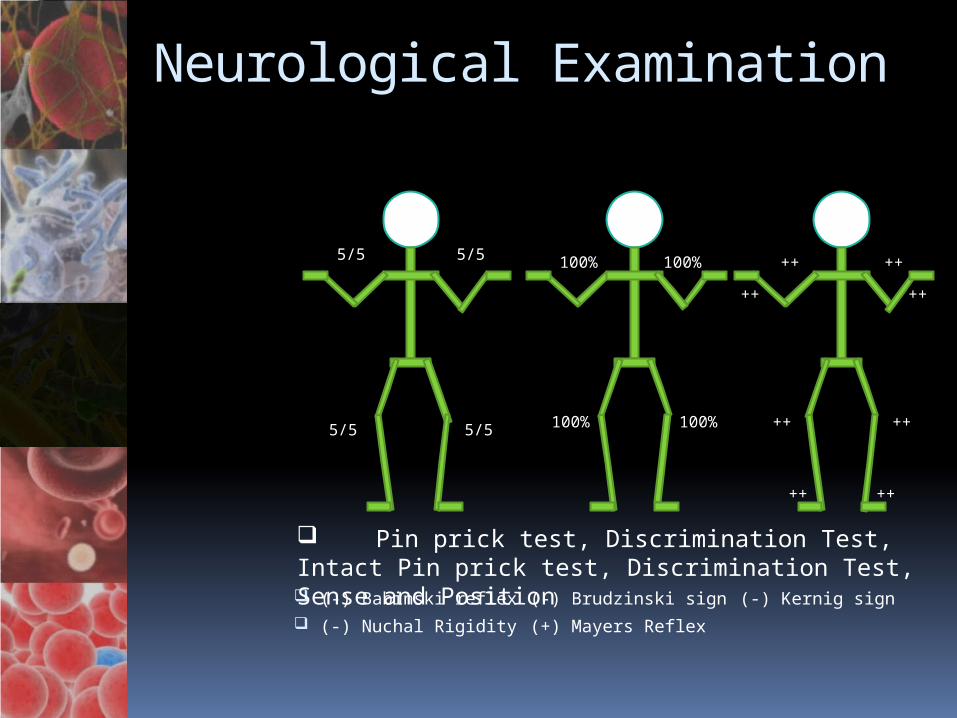
Neurological Examination
(-) Babinski reflex (-) Brudzinski sign (-) Kernig sign (-) Nuchal Rigidity (+) Mayers Reflex
++
5/5 ++5/5 100%
5/55/5
++
++100%
100% 100% ++ ++
++++
Pin prick test, Discrimination Test, Intact Pin prick test, Discrimination Test, Sense and Position

Salient Features
55 year old Male Hypertensive for 5 years History of nape pains Flushed face, palms and hands Eye redness and gum bleeding Findings of Increased Hct and Hgb on
previous admission PE: BP: 150/90, Phletoric face,
conjunctival effusion, flushed palms and soles
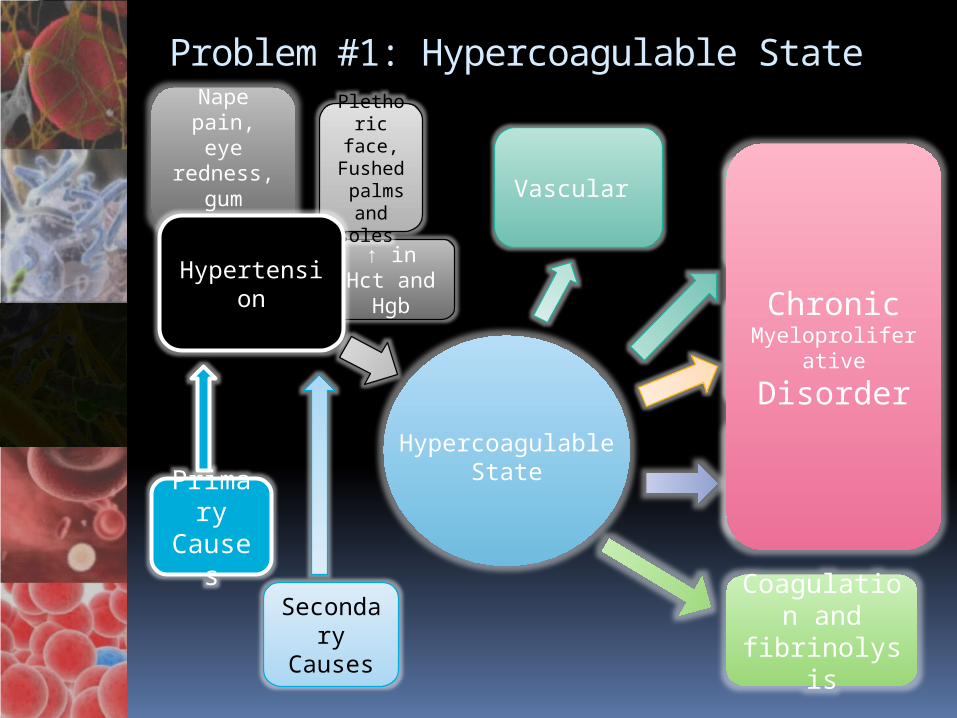
↑ in Hct and Hgb
Plethoric face,Fushed palms and
soles
Nape pain, eye redness,
gum bleeding
Problem #1: Hypercoagulable State
Primary
Causes
Secondary
Causes
Thrombocythemia
Erythrocytosis
Coagulation and
fibrinolysis
Myelofibrosis
Chronic Myeloproliferati
ve Disorder
Hypertension
Vascular
Hypercoagulable State
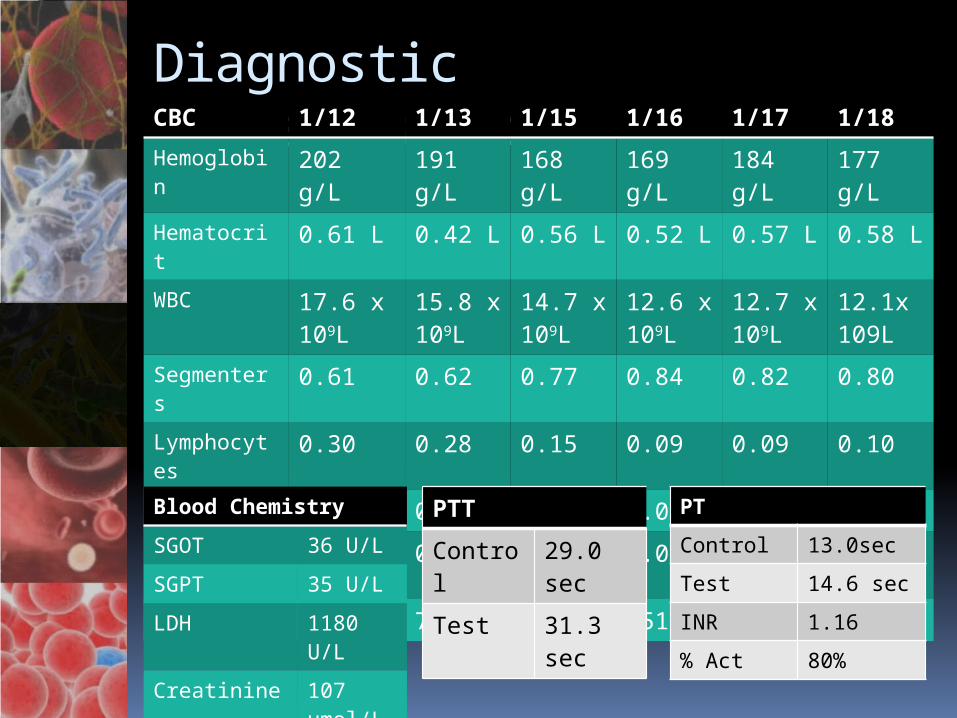
Diagnostic Investigation:CBC 1/12 1/13 1/15 1/16 1/17 1/18
Hemoglobin
202 g/L 191 g/L
168 g/L
169 g/L
184 g/L
177 g/L
Hematocrit 0.61 L 0.42 L 0.56 L 0.52 L 0.57 L 0.58 L
WBC 17.6 x 109L
15.8 x 109L
14.7 x 109L
12.6 x 109L
12.7 x 109L
12.1x 109L
Segmenters
0.61 0.62 0.77 0.84 0.82 0.80
Lymphocytes
0.30 0.28 0.15 0.09 0.09 0.10
Monocytes 0.05 0.08 0.06 0.04 0.03 0.06
Eosinophils 0.01 0.02 0.01 0.03 0.06 0.04
Platelets 758 740 648 651 702 750Blood Chemistry
SGOT 36 U/L
SGPT 35 U/L
LDH 1180 U/L
Creatinine 107 umol/L
PTT
Control 29.0 sec
Test 31.3 sec
PT
Control 13.0sec
Test 14.6 sec
INR 1.16
% Act 80%
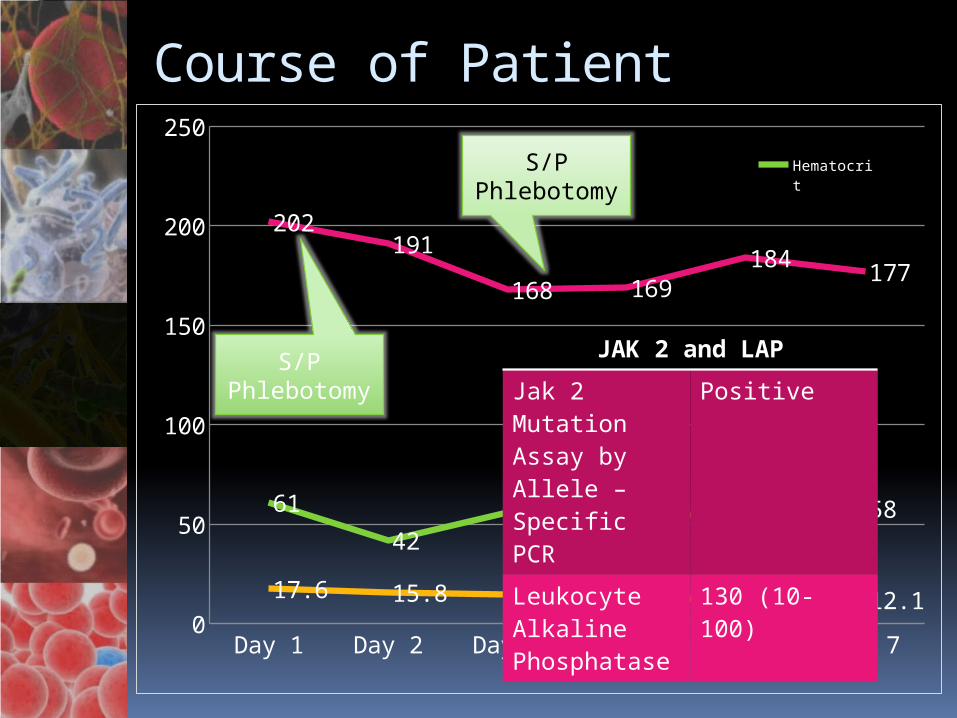
Course of Patient
Day 1 Day 2 Day 4 Day 5 Day 6 Day 70
50
100
150
200
250
61
4256 52 57 58
202191
168 169184
177
17.6 15.8 14.7 12.6 12.7 12.1
Hema-tocritHemo-globin
S/P Phlebotomy
S/P Phlebotomy
JAK 2 and LAP
Jak 2 Mutation Assay by Allele – Specific PCR
Positive
Leukocyte Alkaline Phosphatase
130 (10-100)

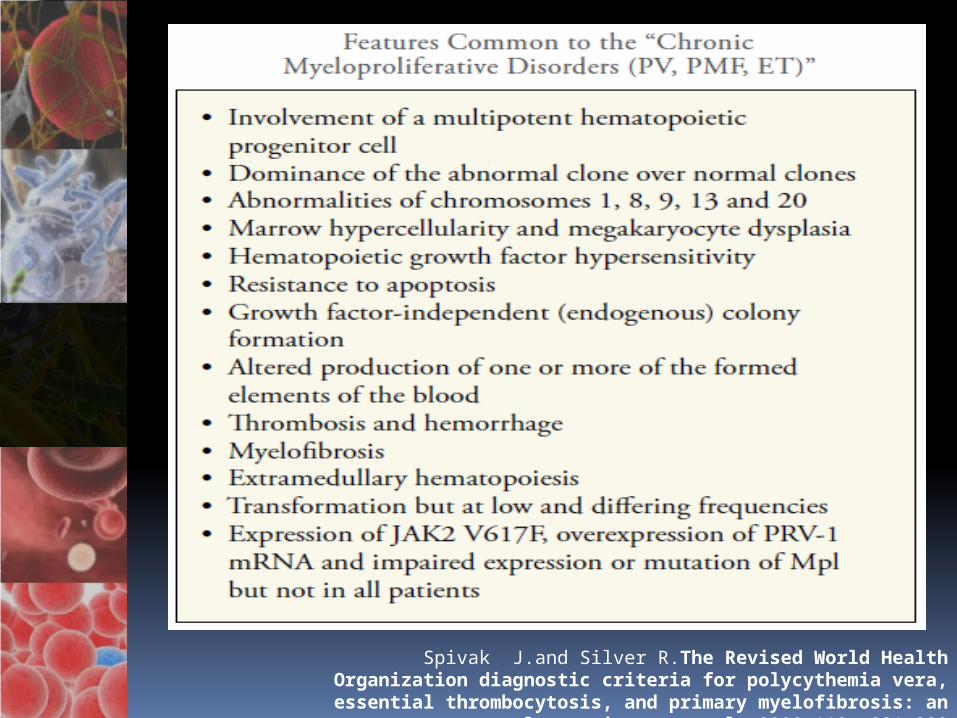
Chronic Myeloproliferative Disorders (MPD) Polycythemia vera (PV) Essential thrombocythemia (ET) Primary myelofibrosis (PMF)
Characterized by clonal hematopoiesis involving a multipotent hematopoietic progenitor cell,
Unregulated production of red cells, white cells, and platelets alone or in combination
Tendency to extramedullary hematopoiesis, and transformation to acute leukemia or myelofibrosis at a variable but low rate. Spivak J.and Silver R.The Revised World Health Organization
diagnostic criteria for polycythemia vera, essential thrombocytosis, and primary myelofibrosis: an alternative
proposal. 2008 112: 231-239
Spivak J.and Silver R.The Revised World Health Organization diagnostic criteria for polycythemia vera, essential
thrombocytosis, and primary myelofibrosis: an alternative proposal. 2008 112: 231-239
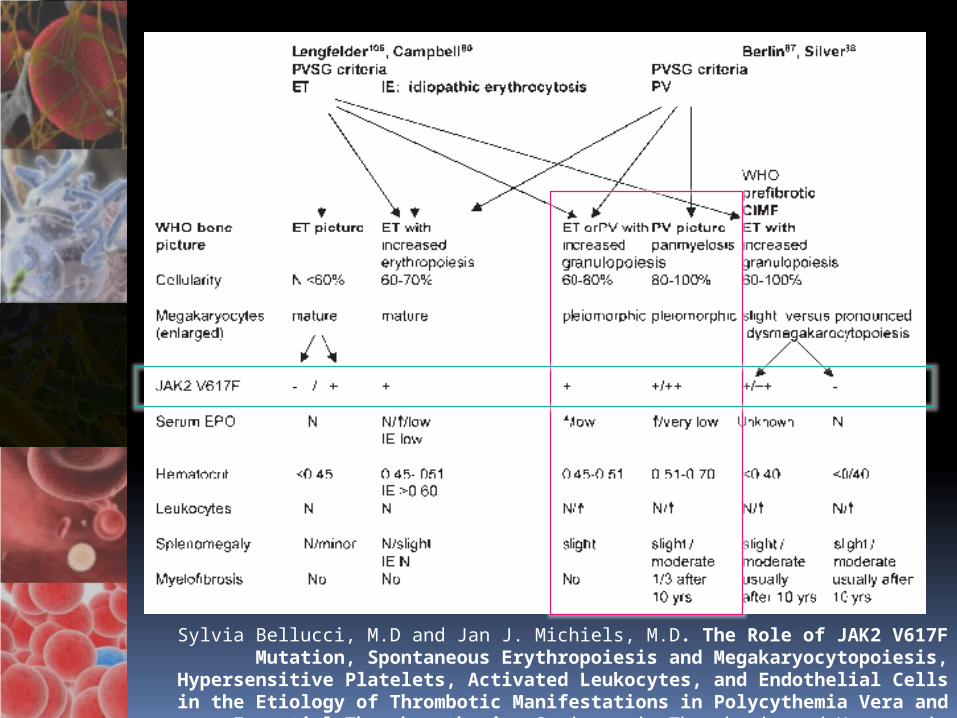
Sylvia Bellucci, M.D and Jan J. Michiels, M.D. The Role of JAK2 V617F Mutation, Spontaneous Erythropoiesis and Megakaryocytopoiesis, Hypersensitive Platelets, Activated Leukocytes, and Endothelial Cells in the Etiology of
Thrombotic Manifestations in Polycythemia Vera and Essential Thrombocythemia. Seminars in Thrombosis and Hemostasis Volume 32, Number
4. 2006

Spivak J.and Silver R.The Revised World Health Organization diagnostic criteria for polycythemia vera, essential
thrombocytosis, and primary myelofibrosis: an alternative proposal. 2008 112: 231-239
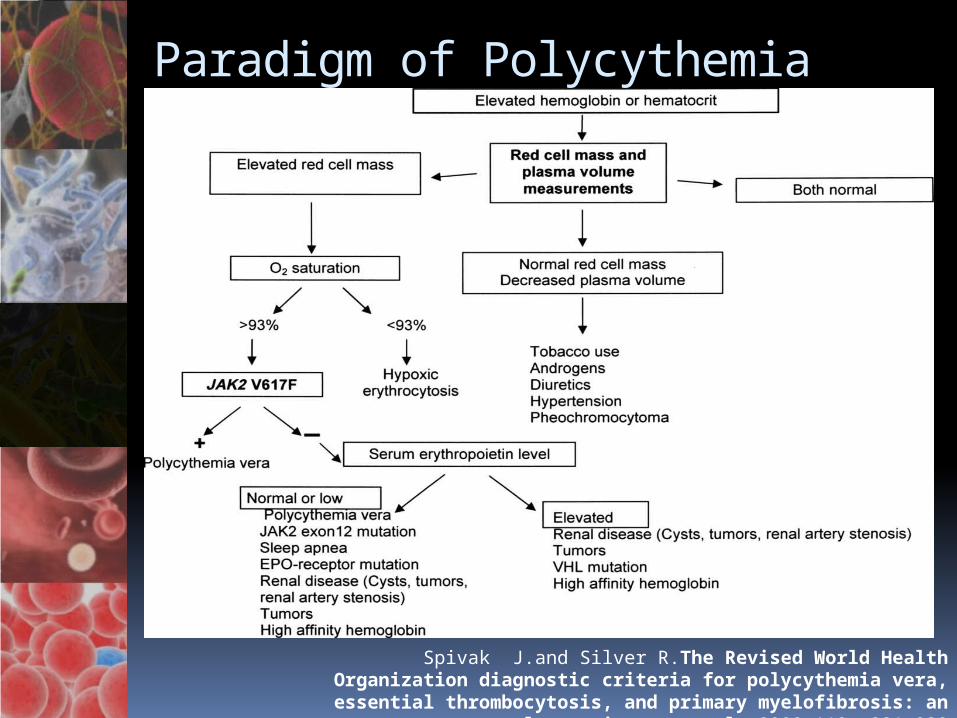
Paradigm of Polycythemia Vera
Spivak J.and Silver R.The Revised World Health Organization diagnostic criteria for polycythemia vera, essential
thrombocytosis, and primary myelofibrosis: an alternative proposal. 2008 112: 231-239

Polycythemia Vera
Malignant Disorder of the hematopoetic stem cells which characterized by Clonal hyperproliferation Low rate of apoptosis
Endogenous Erythroid Colonies Chracteristic biological feature of PV
Erythroid precursor
Spivak J.and Silver R.The Revised World Health Organization diagnostic criteria for polycythemia vera, essential
thrombocytosis, and primary myelofibrosis: an alternative proposal. 2008 112: 231-239
Major Criteria of PV
1) JAK2 mutation2) Absolute erythrocytosis
Hallmark of PV The diagnosis cannot be established,
nor can PV be distinguished
3) Plasma volume expansion, even in the absence of splenomegaly
4) Presentation of PV is sufficiently pleomorphic that all laboratory clues need to be used
Spivak J.and Silver R.The revised World Health Organization diagnostic criteria for polycythemia vera, essential
thrombocytosis, and primary myelofibrosis: an alternative proposal. 2008 112: 231-239
Major Criteria of PV
5) Given practice situation to define pretest probabilities with respect to the frequency with which different forms of erythrocytosis or apparent erythrocytosis are encountered
Spivak J.and Silver R.The revised World Health Organization diagnostic criteria for polycythemia vera, essential
thrombocytosis, and primary myelofibrosis: an alternative proposal. 2008 112: 231-239
Clinical Manifestation of PV
Hypercatabolism and hyperviscosity Resulting from excessive red cell
production Concomitant thrombocytosis and
leukocytosis Lead to headache, fatigue, dizziness,
pruritus (particularly after bathing in hot water), excessive sweating, and erythromelalgia.
Huichun Zhan, MD, and Jerry L. Spivak, MD. The Diagnosis and Management of Polycythemia Vera, Essential Thrombocythemia, and Primary Myelofibrosis
in the JAK2 V617F Era. Clinical Advances in Hematology & Oncology Volume 7, Issue 5 May 2009
Janus Associated Kinase 2
One member of a family of four cytoplasmic tyrosine kinases that also includes JAK1, JAK3 and Tyk2. Signaling by cytokine and growth
factor receptors that lack intrinsic kinase activity
Utilizes some growth factors such as erythropoietin and thrombopoietin
Srdan Verstovsek. Therapeutic potential of JAK2 inhibitors. American Society of Hematology. Hematology 2009
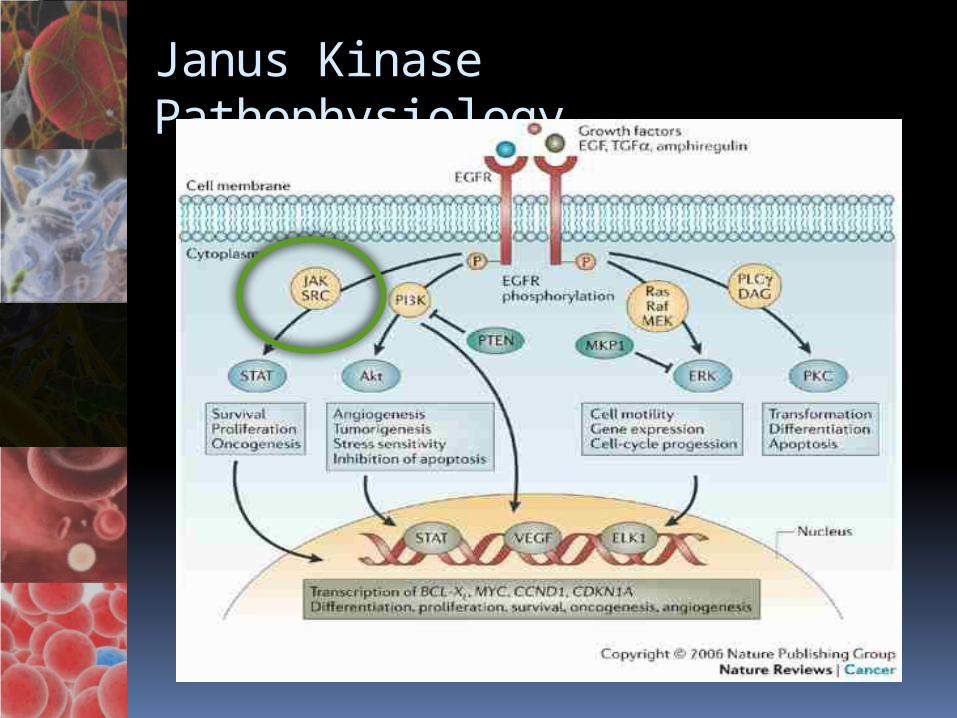
Janus Kinase Pathophysiology
Jak 2 Mutations
JAK2 mutations (with highly sensitive allele-specific polymerase chain reaction assays and blood neutrophils)
95% of Polycythemia vera 50–60% of Essential Thrombocythemia
and Primary Myelofibrosis
The mutation substitutes a valine for a phenylalanine at position 617 within the JAK2 kinase regulatory domain, releasing the JAK2 kinase from regulatory control.
Spivak J.and Silver R.The revised World Health Organization diagnostic criteria for polycythemia vera, essential
thrombocytosis, and primary myelofibrosis: an alternative proposal. 2008 112: 231-239
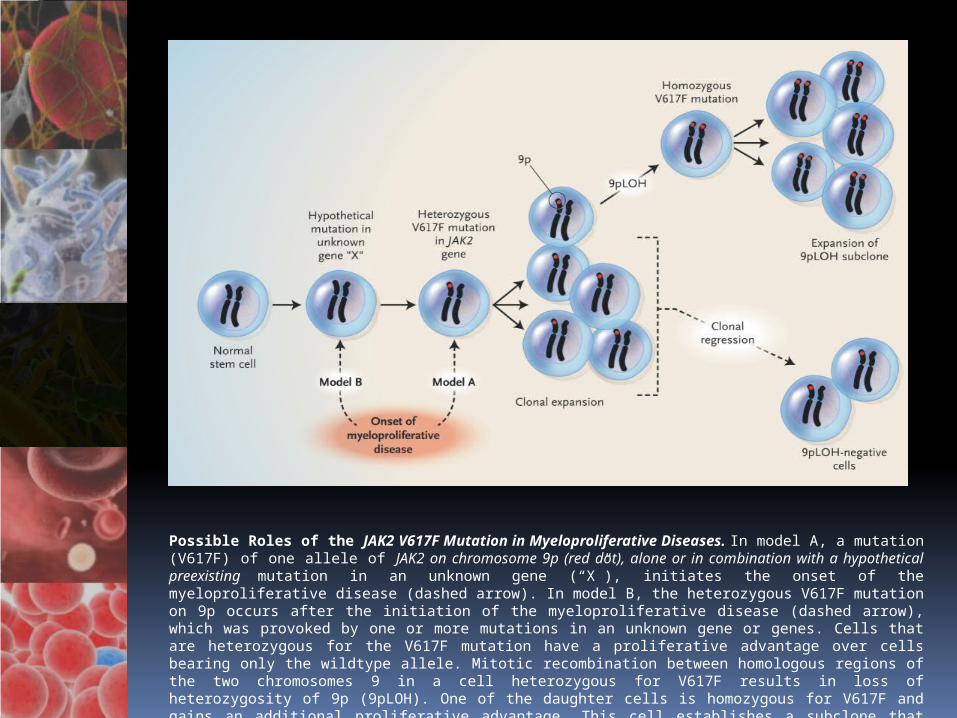
Possible Roles of the JAK2 V617F Mutation in Myeloproliferative Diseases. In model A, a mutation (V617F) of one allele of JAK2 on chromosome 9p (red dot), alone or in combination with a hypothetical preexisting mutation in an unknown gene (“X”), initiates the onset of the myeloproliferative disease (dashed arrow). In model B, the heterozygous V617F mutation on 9p occurs after the initiation of the myeloproliferative disease (dashed arrow), which was provoked by one or more mutations in an unknown gene or genes. Cells that are heterozygous for the V617F mutation have a proliferative advantage over cells bearing only the wildtype allele. Mitotic recombination between homologous regions of the two chromosomes 9 in a cell heterozygous for V617F results in loss of heterozygosity of 9p (9pLOH). One of the daughter cells is homozygous for V617F and gains an additional proliferative advantage. This cell establishes a subclone that outcompetes both cells that are heterozygous for V617F and cells that are homozygous for wild-type JAK2.
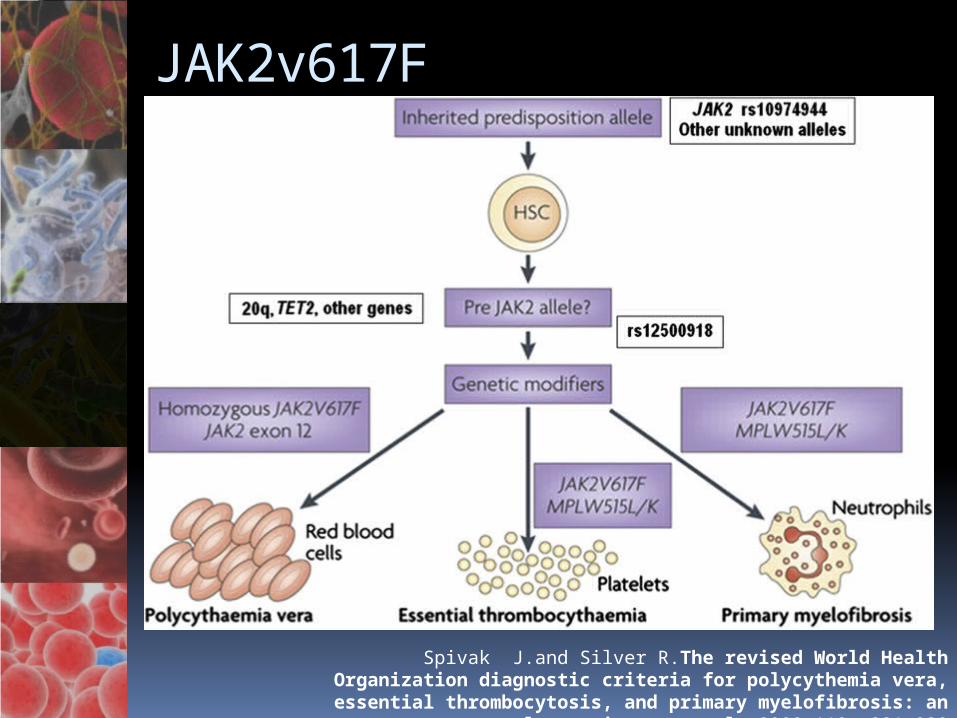
JAK2v617F
Spivak J.and Silver R.The revised World Health Organization diagnostic criteria for polycythemia vera, essential
thrombocytosis, and primary myelofibrosis: an alternative proposal. 2008 112: 231-239
The Role of JAK 2 Tyrosine Kinase
The JAK2 V617F point mutation Makes the normal hematopoietic
progenitor cells hypersensitive Thrombopoietin Erythropoietin Myeloid progenitor cells
leading to Trilinear hematopoietic myeloproliferation
Sylvia Bellucci, M.D and Jan J. Michiels, M.D. The Role of JAK2 V617F Mutation, Spontaneous Erythropoiesis and Megakaryocytopoiesis, Hypersensitive Platelets, Activated Leukocytes, and Endothelial Cells in the Etiology of
Thrombotic Manifestations in Polycythemia Vera and Essential Thrombocythemia. Seminars in Thrombosis and Hemostasis Volume 32, Number
4. 2006

The Role of JAK 2 Tyrosine Kinase
Significant correlation between JAK2 V617F mutational status and hematocrit (Ht), white blood cell and platelet counts in PV patients, and Ht values in ET cases, was observed by ASPCR.
Lucia E., Martino B., Mammi C. The incidence of JAK2 V617F mutation in bcr/abl-negative chronic myeloproliferative disorders:
assessment by two different detection methods. Leukemia & Lymphoma, October 2008; 49(10): 1907–1915

Three main clinical consequences during long-term follow-up (JAK2 V617F point mutation) -1st Spontaneous growth of enlarged
mature megakaryocytes in ET/PV with overproduction of hypersensitive platelets results Found in a broad spectrum of platelet-
mediated microvascular circulatory disturbances
Very sensitive to low-dose aspirin.
Sylvia Bellucci, M.D and Jan J. Michiels, M.D. The Role of JAK2 V617F Mutation, Spontaneous Erythropoiesis and Megakaryocytopoiesis, Hypersensitive Platelets, Activated Leukocytes, and Endothelial Cells in the Etiology of
Thrombotic Manifestations in Polycythemia Vera and Essential Thrombocythemia. Seminars in Thrombosis and Hemostasis Volume 32, Number
4. 2006

Three main clinical consequences during long-term follow-up (JAK2 V617F point mutation) – 2nd Spontaneous growth of
erythropoiesis with the overproduction of erythrocytes Increased hemoglobin, hematocrit,
and red cell mass. Major arterial and venous thrombotic
complications Platelet-mediated microvascular
circulatory disturbances of thrombocythemia.Sylvia Bellucci, M.D and Jan J. Michiels, M.D. The Role of JAK2 V617F Mutation,
Spontaneous Erythropoiesis and Megakaryocytopoiesis, Hypersensitive Platelets, Activated Leukocytes, and Endothelial Cells in the Etiology of
Thrombotic Manifestations in Polycythemia Vera and Essential Thrombocythemia. Seminars in Thrombosis and Hemostasis Volume 32, Number
4. 2006
Three main clinical consequences during long-term follow-up (JAK2 V617F point mutation) – 3rd Slowly progressive myeloid
granulocytic metaplasia in bone marrow and spleen 1/4th to 1/3rd of JAK2 V617F-positive PV
patients after long-term follow-up No tendency of leukemic transformation as long
as they are not treated with myelosuppressive agents.
Sylvia Bellucci, M.D and Jan J. Michiels, M.D. The Role of JAK2 V617F Mutation, Spontaneous Erythropoiesis and Megakaryocytopoiesis, Hypersensitive Platelets, Activated Leukocytes, and Endothelial Cells in the Etiology of
Thrombotic Manifestations in Polycythemia Vera and Essential Thrombocythemia. Seminars in Thrombosis and Hemostasis Volume 32, Number
4. 2006
Leukocyte Alkaline Phosphatase (LAP) Score
In 1955, Kaplow described a cytochemical technique for assessing LAP activity.
Later, a score greater than 100 LAP in granulocytes of peripheral blood was included in the Polycythemia Vera Study Group (PVSG) diagnostic criteria.
Basquiera A, Fassetta F, Soria E et al. Accuracy of leukocyte alkaline phosphatase score to predict JAK2 V617F mutation.
Haematologica 2007; 92:5:704-705
Leukocyte Alkaline Phosphatase (LAP) Score
A LAP score above 100 Sensitivity: 88.2% Specificity: 87.5%
The highest LAP score in patients with PV may be due to a greater prevalence of homozygosity for JAK2 V617F mutation in PV
Basquiera A, Fassetta F, Soria E et al. Accuracy of leukocyte alkaline phosphatase score to predict JAK2 V617F mutation.
Haematologica 2007; 92:5:704-705
Why there is an increase LAP Score in PV?
Polymorphonuclear (PMN) leukocyte hyperactivation Measured by the increased expression
of membrane CD11b Cellular elastase content or
myeloperoxidase levels
Sylvia Bellucci, M.D and Jan J. Michiels, M.D. The Role of JAK2 V617F Mutation, Spontaneous Erythropoiesis and Megakaryocytopoiesis, Hypersensitive Platelets, Activated Leukocytes, and Endothelial Cells in the Etiology of
Thrombotic Manifestations in Polycythemia Vera and Essential Thrombocythemia. Seminars in Thrombosis and Hemostasis Volume 32, Number
4. 2006

Problem # 2: Neuro
Day 1 Day 2 Day 4 Day 5 Day 6 Day 70
50
100
150
200
250
61
4256 52 57 58
202191
168 169184
177
17.6 15.8 14.7 12.6 12.7 12.1
Hema-tocritHemo-globin
S> R Sided Paresthesia Mild Dysarthria (-) HA, (-) Dizziness
O> BP:140/90 CR: 89 Shallow Nasolabial fold L (-) Babinski
Plain Cranial Computed Tomography
Referred to Neurology Service
Transferred to ICU
Medications:1) ASA 300mg
POThe 160 mg OD
PO2) Pantoprazole 40mg/ tab 1 tab
OD PO
MAP: 110-120mmHG
S/P Phlebotomy

OtherDiagnostic Investigation
Diagnostics
ECG LAE and LVH by Voltage
Carotid Doppler Bilateral Normal Duplex ScanBilateral Tortous Common Carotid Artery Othewise Normal Forward FlowBilateral Forward Vertebral Artery Flow

Retrospective cohort study of patients with polycythemia who had been followed for 20 years.
Arterial and venous thrombosis 2/3rd and 1/3rd of thromboses either
before or when PV was diagnosed Ischemic stroke and transient
ischemic attacks 70% of arterial thromboses at
diagnosis and Prevalent as myocardial infarction
(30%) before diagnosis of PV
Polycythemia Vera: The Natural History of 1213 Patients Followed for 20 Years
Gruppo Italiano Studio Policitemia, Ann Intern Med. 1995;123:656-66

Thrombotic Events in PV
Arterial or venous thrombosis can be the presenting manifestation of PV
PV must always be included in the evaluation of a hypercoagulable state
Age (>60 years) and a previous history of thrombosis Major risk factors for recurrent
thrombotic eventsHuichun Zhan, MD, and Jerry L. Spivak, MD. The Diagnosis and Management of Polycythemia Vera, Essential Thrombocythemia, and Primary Myelofibrosis
in the JAK2 V617F Era. Clinical Advances in Hematology & Oncology Volume 7, Issue 5 May 2009
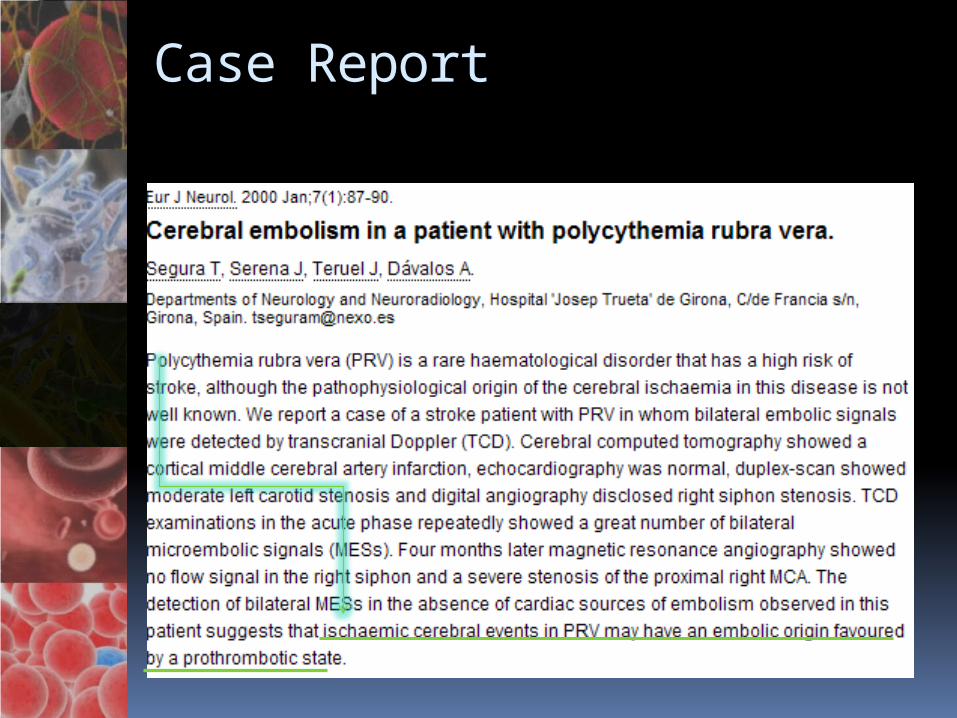
Case Report


Final Diagnosis
CVD, Multiple Ischemic Infarct Secondary to Hypercoagulable State
Polycythemia Vera

Management of Polycythemia Vera
Phlebotomy: Management of PV Mainstay of therapy Target
HCT below 45% in men HCT below42% in women
Reduces the red cell mass Alleviates the symptoms of
hyperviscosity and the threat of thrombosis
Huichun Zhan, MD, and Jerry L. Spivak, MD. The Diagnosis and Management of Polycythemia Vera, Essential Thrombocythemia, and Primary Myelofibrosis
in the JAK2 V617F Era. Clinical Advances in Hematology & Oncology Volume 7, Issue 5 May 2009
Phlebotomy: Management of PV Periodic phlebotomy
To render the patient iron deficient to prevent rapid elevation of the red cell mass
Phlebotomy required only at 3-month intervals. Once an iron-deficient state is
achieved
Huichun Zhan, MD, and Jerry L. Spivak, MD. The Diagnosis and Management of Polycythemia Vera, Essential Thrombocythemia, and Primary Myelofibrosis
in the JAK2 V617F Era. Clinical Advances in Hematology & Oncology Volume 7, Issue 5 May 2009
Phlebotomy:Management of PV Benefits Restoration of systemic and pulmonary
pressures to normal Increase in plasma volume and a reduction
in blood viscosity Reduction in spleen size Improved platelet function Improved cognition Decrease in nitric oxide scavenging by the
elevated red cell mass Contributes to vasoconstriction and
pulmonary hypertensionHuichun Zhan, MD, and Jerry L. Spivak, MD. The Diagnosis and Management of Polycythemia Vera, Essential Thrombocythemia, and Primary Myelofibrosis
in the JAK2 V617F Era. Clinical Advances in Hematology & Oncology Volume 7, Issue 5 May 2009
Management of PV
Pruritus is a unique feature of PV Including phlebotomy H1 and H2 blockers Ataractics such as doxepin Antidepressants such as paroxetine Either UV B directly from sunlight or in
a tanning parlor, or UV A exposure with psoralens (PUVA light therapy)
Cytoreductive therapy with hydroxyurea or alpha interferon
Huichun Zhan, MD, and Jerry L. Spivak, MD. The Diagnosis and Management of Polycythemia Vera, Essential Thrombocythemia, and Primary Myelofibrosis
in the JAK2 V617F Era. Clinical Advances in Hematology & Oncology Volume 7, Issue 5 May 2009
Management of PV
Asymptomatic hyperuricemia (<10 mg%) requires no therapy But allopurinol should be
administered to avoid further elevation of the uric acid when chemotherapy is employed to reduce splenomegaly or leukocytosis or to treat pruritus
Fauci, Braunwald, Kasper et al. Harrison of Internal Medicine. Copyright The McGraw-Hill Companies 2008. Part 5 Sec 1 Chap 103.
Hydroxyurea: Management of PV
Widely used in PV Without any evidence
Prolongs survival Prevents complications of PV, such as
thrombosis or myelofibrosis Should be used judiciously in PV
It is only myelosuppressive Continued uncertainty about its
leukemogenic potential Huichun Zhan, MD, and Jerry L. Spivak, MD. The Diagnosis and Management of Polycythemia Vera, Essential Thrombocythemia, and Primary Myelofibrosis
in the JAK2 V617F Era. Clinical Advances in Hematology & Oncology Volume 7, Issue 5 May 2009
Prognosis
Each independent factors associated with a shortened survival Progressive splenomegaly and
myelofibrosis Anemia (hemoglobin <10g),
thrombocytopenia (<100,000/μL) Leukocytosis (>30,000/μL)
Huichun Zhan, MD, and Jerry L. Spivak, MD. The Diagnosis and Management of Polycythemia Vera, Essential Thrombocythemia, and Primary Myelofibrosis
in the JAK2 V617F Era. Clinical Advances in Hematology & Oncology Volume 7, Issue 5 May 2009
Aspirin: Management of PV
Effective in relieving the microvascular complications of erythromelalgia and ocular migraine in PV
Does not appear to be more effective than anagrelide in preventing other forms of thrombosis, either venous or arterial
Caution: PC is in excess of 1,000,000/μL because it can cause serious bleeding
Huichun Zhan, MD, and Jerry L. Spivak, MD. The Diagnosis and Management of Polycythemia Vera, Essential Thrombocythemia, and Primary Myelofibrosis
in the JAK2 V617F Era. Clinical Advances in Hematology & Oncology Volume 7, Issue 5 May 2009
Aspirin: Management of PV
Whether low-dose aspirin (81 mg daily) is effective in preventing thrombotic complications without increasing the risk of major bleeding has not been definitely proven.
Huichun Zhan, MD, and Jerry L. Spivak, MD. The Diagnosis and Management of Polycythemia Vera, Essential Thrombocythemia, and Primary Myelofibrosis
in the JAK2 V617F Era. Clinical Advances in Hematology & Oncology Volume 7, Issue 5 May 2009
Drugs in Development
There are several compounds targeting the JAK2 mutation in development: INCB018424 (Incyte/Novartis) TG101348 (TargeGen) CEP-701 (Cephalon) AZD1480 (AstraZeneca) XL019 (Exelixis) WP1066 (Calistoga) CYT-387 (Cytopia)
Garber, K. JAK2 Inhibitors: Not the Next Imatinib But Researchers See Other Possibilities. JNCI Journal of the National
Cancer Institute. 2009. 101 (14), 980-982 DOI

JAK 2 Inhibitors
INCB018424 (Incyte/Novartis) First to be evaluated in PMF and post-
PV/ET MF Entered clinical trials in mid-2007 Inhibited hematopoietic progenitor
cell colony formation from CD34+ cells isolated from PV patients Did so more potently than with cells
from normal donors Starting dose of 25 mg twice daily
Srdan Verstovsek. Therapeutic potential of JAK2 inhibitors. American Society of Hematology. Hematology 2009

INCB018424

JAK 2 Inhibitors
CEP-701 (lestaurtinib) (Cephalon) Derivative of the indolocarbazole
K252 (straurosporine analog) Potent inhibitory activity of JAK2, in
addition to a number of other kinases including FLT-3, RET and Trk-A
Dose of 80 mg BID PO Recommended for hematologic
malignancy trialsSrdan Verstovsek. Therapeutic potential of JAK2 inhibitors.
American Society of Hematology. Hematology 2009
JAK 2 Inhibitors
TG101348 (TargeGen) 35- and 334-fold selectivity for JAK2
as compared with JAK3 and JAK1, respectively
Inhibited hematopoietic progenitor colony formation and erythroid engraftment
Twenty-eight patients were treated at 8 dose levels from 30 mg to 800 mg daily
Srdan Verstovsek. Therapeutic potential of JAK2 inhibitors. American Society of Hematology. Hematology 2009
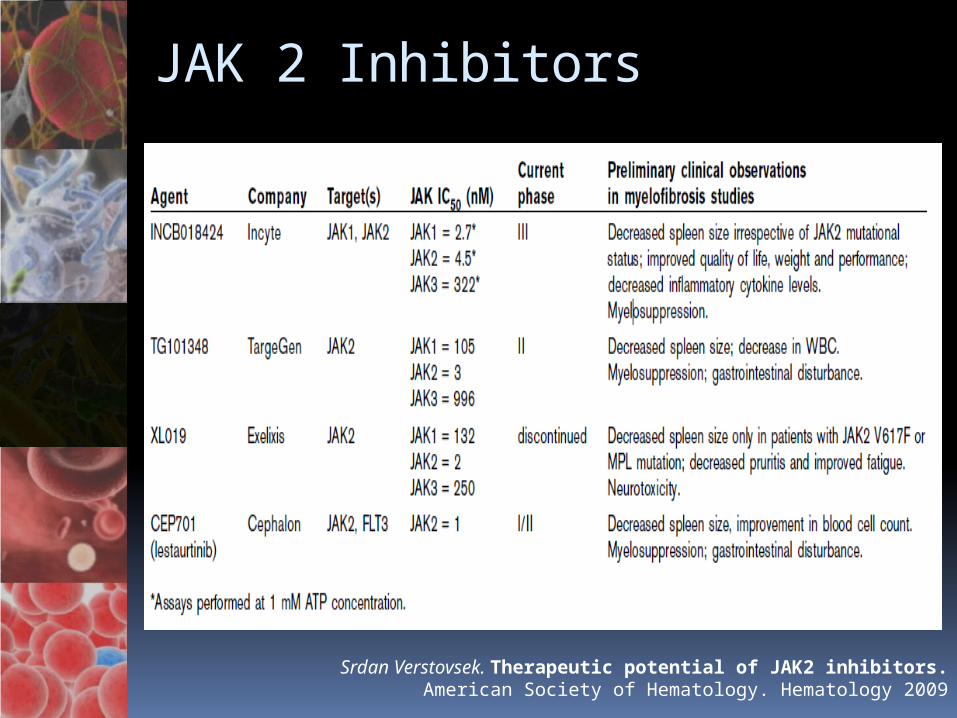
JAK 2 Inhibitors
Srdan Verstovsek. Therapeutic potential of JAK2 inhibitors. American Society of Hematology. Hematology 2009

THANK YOU VERY MUCH!
Recommended






![Is there a gender effect in polycythemia vera? · 2021. 1. 4. · Polycythemia Vera), the CYTO-PV (Cytoreductive therapy in PV) prospective studies [44, 45] (female rate was 40.5%](https://img.pdfslide.us/doc/110x75/60d8fb8169a3c6351e0a476a/is-there-a-gender-effect-in-polycythemia-vera-2021-1-4-polycythemia-vera.jpg)