8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 1/106
Interventions for Clientswith Pituitary and AdrenalGland Problems

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 2/106
Hormones secreted from the anterior pituitary glandregulate growth, metabolism, and sexualdevelopment. These functions are affected when thepituitary gland secretes too much or too little of one
or more hormones
The posterior pituitary gland secretes vasopressin(antidiuretic hormone [ADH]). Dysfunction of theposterior pituitary gland results in fluid and electrolyteimbalance
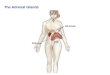
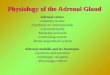
The adrenal gland produces and secretes hormonesthat influence homeostasis and are life sustaining

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 3/106
DISORDERS OF THE PITUITARY GLAND
The anterior pituitary gland(adenohypophysis) controls growth,metabolic activity, and sexual developmentthrough the actions of the following hormones:
Growth hormone (GH; somatotropin) Prolactin (PRL) Thyrotropin (thyroid-stimulating hormone [TSH]) Corticotropin (adrenocorticotropic hormone [ACTH]) Follicle-stimulating hormone (FSH) Luteinizing hormone (LH) Melanocyte-stimulating hormone (MSH)

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 4/106
DISORDERS OF THE PITUITARY GLAND
Disorders of hormones secreted by the anteriorpituitary gland can result from problems arisingwithin the anterior pituitary gland itself(primary pituitary dysfunction) or from
problems in the hypothalamus that changeanterior pituitary function (secondarypituitary dysfunction)
In either case, one or more hormones may be
undersecreted (pituitary hypofunction) oroversecreted (pituitary hyperfunction)

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 5/106
DISORDERS OF THE PITUITARY GLAND.Hypopituitarism
Pathophysiology A person with hypopituitarism has a deficiency of one
or more anterior pituitary hormones, resulting inmetabolic abnormalities and sexual dysfunction
Decreased production of all of the anterior pituitaryhormones is an extremely rare condition known aspanhypopituitarism
Deficiencies of adrenocorticotropic hormone (ACTH)
and thyroid-stimulating hormone (TSH) are the mostlife threatening because they result in a correspondingdecrease in the secretion of vital hormones from theadrenal and thyroid glands

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 6/106
DISORDERS OF THE PITUITARY GLAND.Hypopituitarism
Deficiency of the gonadotropins (luteinizing hormone[LH] and follicle-stimulating hormone [FSH]—hormonesthat stimulate the ovaries and testes to produce sexhormones) changes sexual function in both men andwomen
In males, gonadotropin deficiency results in testicularfailure, with decreased testosterone production from theLeydig cells and decreased or absent spermatogenesisfrom the seminiferous tubules. Decreased testosteronelevels in males cause delayed onset of puberty and
sterility
In females, gonadotropin deficiency results in ovarianfailure, amenorrhea, and infertility

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 7/106
DISORDERS OF THE PITUITARY GLAND.Hypopituitarism
Growth hormone (GH) deficiency changes tissuegrowth patterns indirectly. GH itself has little effecton tissues and cells. Rather, the presence of GHstimulates the liver to produce substances knownas somatomedins
These somatomedins, especially somatomedin С(insulin-like growth factor-1 [IGF-1]), then enhancegrowth activities in cells and tissues. SomatomedinС is responsible for bone and cartilage growth and
maintenance

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 8/106
DISORDERS OF THE ANTERIOR PITUITARY GLAND.Hypopituitarism
GH deficiency may be a result of insufficientproduction of GH, failure of the liver to producesomatomedins, or a failure of the cells or tissues torespond to the presence of the somatomedins
GH deficiency in children leads to short stature andother manifestations of growth retardation
GH deficiency in adults produces no obviousanatomic changes but does increase the rate of
bone destructive activity, leading to thinner, morefragile bones

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 9/106
DISORDERS OF THE ANTERIOR PITUITARY GLAND.Hypopituitarism
Etiology The cause of hypopituitarism varies
Benign or malignant pituitary tumors can compressand destroy pituitary tissue.
Pituitary function can be impaired by severemalnutrition or rapid loss of body fat, such as inpeople with anorexia nervosa (a disorder in whichpeople see themselves as overweight and eat so littlethat excessive weight loss and starvation result)
Poor circulation to the pituitary gland can causehypoxia and infarction
Idiopathic hypopituitarism may result in anisolated hormone deficiency, and often the cause isunknown

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 10/106
DISORDERS OF THE ANTERIOR PITUITARY GLAND.Hypopituitarism
Postpartum hemorrhage is the most common causeof pituitary infarction, which results in decreasedhormone secretion. This clinical problem is knownas Sheehan's syndrome
The pituitary gland normally enlarges duringpregnancy, and when hypotension results fromhemorrhage, ischemia and necrosis of the glandoccur
Usually this condition develops immediatelypostpartum, although some cases have occurredseveral years after delivery

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 11/106
DISORDERS OF THE PITUITARY GLAND.Hypopituitarism

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 12/106
DISORDERS OF THE PITUITARY GLAND.Hypopituitarism
AssessmentAnterior Pituitary Hormones Growth hormone (GH) Decreased bone density
Pathologic fracturesDecreased muscle strength
Increased serum cholesterol levels
Gonadotropins Women:(luteinizing • Amenorrheahormone [LH], • Anovulation folliclestimulating • Low circulating estrogen levels hormone [FSH]) • Breast atrophy
• Loss of bone density • Decreased axillary and pubic hair • Decreased libido • Fine facial wrinkles

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 13/106
DISORDERS OF THE PITUITARY GLAND.Hypopituitarism
Men:• Decreased facial hair • Decreased ejaculate volume
• Reduced muscle mass • Loss of bone density • Decreased body hair • Decreased libido
• Impotence • Fine facial wrinkles

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 14/106
DISORDERS OF THE PITUITARY GLAND.Hypopituitarism
Thyrotropin Decreased circulating TSH levels
(Thyroid-stimulating Decreased circulating thyroid
hormone [TSH]) hormone levels
Weight gain
Intolerance to cold
Scalp alopecia
Hirsuitism
Menstrual abnormalities
Decreased libido
Slowed cognition
Lethargy

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 15/106
DISORDERS OF THE PITUITARY GLAND.Hypopituitarism
Adrenocorticotropic Decreased serum cortisol levels
hormone (ACTH) Pale, sallow complexion
Malaise and lethargy
Anorexia
Postural hypotension
Headache
Hypoglycemia
Hyponatremia
Decreased axillary and pubichair (women)

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 16/106
DISORDERS OF THE GLAND.Hypopituitarism
Posterior Pituitary Hormones Vasopressin (antidi- Diabetes insipidus
uretic hormone • Greatly increased [ADH]) urine output
• Low urine specific gravity (< 1.005)• Hypovolemia
HypotensionDehydration
• Increased plasma osmolarity • Increased thirst • Output does not decrease when fluid intake decreases

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 17/106
DISORDERS OF THE PITUITARY GLAND.Hypopituitarism
Neurologic manifestations ofhypopituitarism due to tumor growth oftenfirst occur as changes in visual perception
The nurse evaluates the client's visualacuity, particularly peripheral vision, forchanges or loss
Bilateral temporal headaches are a commonfinding
Other manifestations may include diplopia(double vision) and ocular muscle paralysis,limiting eye movement

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 18/106

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 19/106
DISORDERS OF THE ANTERIOR PITUITARY GLAND.Hypopituitarism
Pituitary abnormalities may cause changesin the sella turcica (the bony nest wherethe pituitary gland rests) that can be seenwith skull x-ray studies
Such changes may include enlargement,erosion, and calcifications in the area of the sellaturcica as a result of pituitary tumors
An angiogram may be indicated to rule out
the presence of an aneurysm or congenitalvascular malformations, especially beforeany surgical intervention

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 20/106
DISORDERS OF THE PITUITARY GLAND.Hypopituitarism
Interventions Management of the adult with hypopituitarism focuses on
replacement of deficient hormones Men who have gonadotropin deficiency are treated with
androgens (testosterone). The most widely used and most
effective route of administration is intramuscular (IM),although use of transdermal testosterone patches isincreasing
Therapy isusually initiated with high-dose testosterone andis continued until virilization (presence of male secondarysex characteristics) is achieved. The dose may then bedecreased, but therapy continues throughout life
Androgen therapy is avoided in men with prostate cancer. Side effects of testosterone therapy include gynecomastia
(the development of breast tissue in men), baldness, andprostatic hypertrophy

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 21/106
DISORDERS OF THE PITUITARY GLAND.Hypopituitarism
Women who have gonadotropin deficiency receivehormone replacement with a combination of estrogenand progesterone administered at their menstrualcycle, which causes withdrawal bleeding
The risk for hypertension or thrombosis (formationof blood clots in deep veins) is increased withestrogen therapy, especially among women whosmoke
For women who wish to become pregnant, clomiphenecitrate (Clomid) may be given to induce ovulation.Menotropins in conjunction with human chorionicgonadotropin (hCG) are used to stimulate ovulationwhen therapy with clomiphene citrate has failed

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 22/106
DISORDERS OF THE PITUITARY GLAND.Hyperpituitarism
Hyperpituitarism is a condition ofhormone oversecretion that occurs when aclient has pituitary tumors or hyperplasias
PRL-secreting tumors are the most commonof the pituitary adenomas. Excessive PRLsecretion inhibits the secretion of gonadalsteroids and gonadotropins in men and
women, resulting in galactorrhea(production of breast milk), amenorrhea,and infertility

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 23/106
DISORDERS OF THE PITUITARY GLAND.Hyperpituitarism
Overproduction of GH results in gigantismor acromegaly
In the client with gigantism, the onset of
GH hypersecretion occurs before puberty,which causes rapid proportional growth inthe length of all bones
In the client with acromegaly, excessive GHsecretion occurs after puberty and producesincreased skeletal thickness, hypertrophy ofthe skin, and enlargement of many visceralorgans, such as the liver and heart

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 24/106
DISORDERS OF THE PITUITARY GLAND.Hyperpituitarism

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 25/106
DISORDERS OF THE PITUITARY GLAND.Hyperpituitarism
History The nurse obtains data about the client's age, gender, and
family history The client is asked about any change in hat, glove, ring, or
shoe size
Fatigue and lethargy are common The client with excessively high GH levels may have backache
and arthralgias (joint pain) in response to bone changes He or she is asked specifically about the presence of headaches
and changes in vision The client with hypersecretion of PRL (hyperprolactinemia)
often reports difficulties in sexual functioning
The nurse asks women about menstrual changes (e.g.,amenorrhea, irregular menses, and difficulty in achievingpregnancy) and about decreased libido or dyspareunia(painful intercourse)
Men may report decreased libido and impotence

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 26/106
DISORDERS OF THE PITUITARY GLAND.Hyperpituitarism
History The nurse obtains data about the client's age, gender, and
family history The client is asked about any change in hat, glove, ring, or
shoe size
Fatigue and lethargy are common The client with excessively high GH levels may have backache
and arthralgias (joint pain) in response to bone changes He or she is asked specifically about the presence of headaches
and changes in vision The client with hypersecretion of PRL (hyperprolactinemia)
often reports difficulties in sexual functioning
The nurse asks women about menstrual changes (e.g.,amenorrhea, irregular menses, and difficulty in achievingpregnancy) and about decreased libido or dyspareunia(painful intercourse)
Men may report decreased libido and impotence

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 27/106

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 28/106
DISORDERS OF THE PITUITARY GLAND.Hyperpituitarism

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 29/106
DISORDERS OF THE PITUITARY GLAND.Hyperpituitarism
Suppression tests High circulating levels of glucose have a suppressive
effect on the release of GH. In a suppression test, 100g of oral glucose or 0.5 g/kg of body weight is givenintravenously. GH levels are measured serially for up
to 120 minutes. GH levels that do not fall below 5ng/mL indicate a positive (abnormal) result
Administration of intravenous (IV) cortisol in the formof dexamethasone (Decadron). This agent shouldresult in suppression of ACTH. When ACTH productioncontinues in the presence of dexamethasoneadministration, the client may have pituitaryCushing's disease

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 30/106
DISORDERS OF THE PITUITARY GLAND.Hyperpituitarism
Interventions
NONSURGICAL MANAGEMENT DRUG THERAPY bromocriptine mesylate (Parlodel) 7.5
mg/day - stimulates dopamine receptors inthe brain and inhibits the release of manypituitary hormones, most specifically GHand PRL
RADIATION THERAPY
SURGICAL MANAGEMENT

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 31/106
DISORDERS OF THE PITUITARY GLAND.Hyperpituitarism

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 32/106
DISORDERS OF THE POSTERIORPITUITARY GLAND
Disorders of the posterior pituitary(neurohypophysis) are directly related toa deficiency or excess of the hormone
vasopressin (antidiuretic hormone[ADH])
Two disorders associated with ADHdeficiency or excess are diabetes insipidus
and the syndrome of inappropriateantidiuretic hormone (SIADH)

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 33/106
DISORDERS OF THE POSTERIORPITUITARY GLAND
Diabetes Insipidus
Diabetes insipidus is a disorder of water metabolismcaused by a deficiency of ADH—either a decrease inADH synthesis or an inability of the kidneys to
respond appropriately to ADH ADH deficiency results in the excretion of large
volumes of dilute urine. Without the presence of ADH,the distal tubules and collecting ducts of the kidneyremain impermeable to water. Thus water is excretedas urine rather than being absorbed in these areas,
which leads to polyuria (excessive urination with lossof free water)

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 34/106
DISORDERS OF THE POSTERIORPITUITARY GLAND
ADH deficiency can be classified as nephrogenic,drugrelated, primary, or secondary
Nephrogenic diabetes insipidus is an inherited
disorder. The renal tubules do not respond to theactions of ADH, which results in inadequate waterreabsorption by the kidney. The actual amount ofhormone produced is not deficient.
Primary diabetes insipidus is caused by a defect in thehypothalamus or pituitary gland, resulting in a lack ofADH production or release

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 35/106
DISORDERS OF THE POSTERIORPITUITARY GLAND
Secondary diabetes insipidus results from tumorswithin or adjacent to the hypothalamus or pituitarygland, head trauma, infectious processes, surgicalprocedures (hypophysectomy), or metastatic tumors,usually from the lung or the breast. Less commonly, itis caused by brain hemorrhage, brain disease, orcerebral aneurysm
Drug-related diabetes insipidus is caused by theadministration of lithium carbonate (Eskalith, Lithobid,
Carbolith) and demeclocycline (Declomycin). Thesedrags can interfere with the kidneys' response to ADH

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 36/106
DISORDERS OF THE POSTERIORPITUITARY GLAND
Assessment
Most of the clinical manifestations of diabetesinsipidus are related to dehydration
The nurse notes the key symptoms of an increase in
the frequency of urination and excessive thirst The client is asked about a history of any known
etiologic factors, such as recent surgery, headtrauma, or medication use (e.g., lithium)
Although increased fluid intake usually prevents
serious dehydration and volume depletion, the clientwho is deprived of fluids or who cannot increase oralfluid intake may experience shock caused by fluid lossand plasma hyperosmolality

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 37/106
DISORDERS OF THE POSTERIORPITUITARY GLAND
Signs of dehydration, such aspoor skin turgor and dry orcracked mucous membranesor skin, may be present in
varying degrees
*Occurs when access to water islimited and rapid dehydration results

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 38/106
DISORDERS OF THE POSTERIORPITUITARY GLAND
Loss of free water produces expected changes inblood and urine tests. The initial step in diagnosis is tomeasure a 24-hour fluid intake and output. Theamount of the client's food and fluid is not restrictedduring this measurement. Urine output must be morethan 4 L during this period for diabetes insipidus to bediagnosed. The amount of urine excreted in 24 hoursmay vary from 4 to 30 L/day. Urine is dilute andtherefore has a low specific gravity (less than 1.005)and low osmolality (50 to 200 mOsm/kg)
Fluid deprivation and hypertonic saline tests are alsoused for diagnosis of the disorder

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 39/106
DISORDERS OF THE POSTERIORPITUITARY GLAND

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 40/106
DISORDERS OF THE POSTERIORPITUITARY GLAND
Interventions Medical management is aimed at controlling the
symptoms of the disease through drag therapy.
If only a partial deficit of ADH is present, effective
control can be achieved with oral chlorpropamide orclofibrate.
These drags increase the action of existing ADH andpossibly have a direct stimulating effect on theproduction of ADH in the hypothalamus. They have
some undesirable side effects, however, and are notused as often as synthetic vasopressin
When ADH deficiency is severe, ADH is replaced inamounts sufficient to maintain water balance

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 41/106
DISORDERS OF THE POSTERIORPITUITARY GLAND

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 42/106
DISORDERS OF THE POSTERIORPITUITARY GLAND
Syndrome of Inappropriate Antidiuretic Hormone The syndrome of inappropriate antidiuretic
hormone (SIADH) occurs when vasopressin(antidiuretic hormone [ADH]) is secreted even whenplasma osmolality is low or normal
SIADH is also known as the Schwartz-Bartter syndrome
ADH continues to be released even when plasma ishyposmolar. Water is retained, which results in dilutionalhyponatremia (a decreased serum sodium level due todilution) and expansion of the extracellular fluid volume.
The increase in plasma volume causes an increase in theglomerular filtration rate and inhibits the release of reninand aldosterone. The combined effect is an increasedsodium loss in urine, further contributing tohyponatremia

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 43/106
DISORDERS OF THE POSTERIORPITUITARY GLAND

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 44/106
DISORDERS OF THE POSTERIORPITUITARY GLAND
HISTORY
The nurse pays particular attention toa history of the following:
Recent trauma
Cerebrovascular disease
Tuberculosis or other pulmonary disease
Cancer
All past and current medication use

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 45/106
DISORDERS OF THE POSTERIORPITUITARY GLAND
Assessment Initially, the symptoms of SIADH are related to water retention. Gastrointestinal (GI) disturbances may occur first:
loss of appetite nausea and vomiting
The nurse weighs the client and documents any recent weight gain
The client may experience lethargy, headaches, hostility, anddisorientation. A change in level of consciousness is an early signof SIADH. Neurologic symptoms can progress from lethargy andheadaches to decreased responsiveness, seizures, and coma.
The nurse assesses deep tendon reflexes, which are often
decreased or sluggish. Vital sign changes include tachycardia (caused by the increasedfluid volume) and hypothermia (caused by central nervous systemdisturbance)

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 46/106
DISORDERS OF THE POSTERIORPITUITARY GLAND
Diagnostic assessment Water retention changes both plasma and urine osmolality. Urine volume decreases, and urine osmolarity increases. Plasma volume increases, and plasma osmolarity
decreases.
Elevated urine sodium levels and elevated specific gravityreflect increased urine concentration.
Serum sodium levels are decreased, often as low as 110mEq/L, because of volume expansion and sodium excretion.
Radioimmunoassay of ADH can diagnose SIADH when ADH
levels are inappropriately elevated in relation to plasma osmolality. (When plasma osmolality is normal or ecreased,
ADH levels should be low)

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 47/106
DISORDERS OF THE POSTERIORPITUITARY GLAND
Interventions
Interventions to treat SIADH focus onrestricting fluid intake, promoting the
excretion of water, replacing lost sodium,interfering with the action of ADH, andpreventing injury if the client experiencesincreased cranial pressure or seizures.
FLUID RESTRICTION (500 to 600 mL/24 hr)
DRUG THERAPY. Diuretics, Hypertonicsaline (3% sodium chloride [3% NaCl])

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 48/106
DISORDERS OF THE ADRENAL GLANDADRENAL GLAND HYPOFUNCTION
Insufficiency of adrenocortical steroids causes problemsthrough the loss of mineralocorticoid (aldosterone) andglucocorticoid (cortisol) action
Impaired secretion of cortisol results in decreased
gluconeogenesis, leading to hypoglycemia. Theglomerular filtration rate and gastric acid productiondecrease, leading to a reduction in urea nitrogen excretion,causing anorexia and weight loss
Reduced aldosterone secretion causes potassium, sodium,and water imbalances. Potassium excretion is
decreased,causing hyperkalemia; sodium and waterexcretion is increased, causing hyponatremia andhypovolemia. Potassium retention also promotesreabsorption of hydrogen ions, which can ultimately lead toacidosis

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 49/106
DISORDERS OF THE ADRENAL GLANDADRENAL GLAND HYPOFUNCTION
Acute adrenal insufficiency, or Addisoniancrisis, is a ifethreatening event in whichthe physiologic need for glucocorticoid andmineralocorticoid hormones is greater thanthe available supply
In most cases, acute adrenal insufficiencyoccurs in response to a stressful event
(e.g., surgery, trauma, or severe infection),especially when the adrenal hormoneoutput is already compromised

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 50/106
DISORDERS OF THE ADRENAL GLANDADRENAL GLAND HYPOFUNCTION

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 51/106
DISORDERS OF THE ADRENAL GLANDADRENAL GLAND HYPOFUNCTION
HISTORY The client is asked about any change in activity level, because
lethargy, fatigue, and muscle weakness are often present Questions about salt intake are included because salt craving is
often a symptom of adrenal hypofunction Gastrointestinal (GI) problems, such as anorexia, nausea,
vomiting, diarrhea, and abdominal pain, often occur. The nurseasks about weight loss during the past weeks or months
Female clients report menstrual changes related to weight loss,and male clients may report impotence
The nurse asks whether the client has had radiation to the abdomen or head.
Significant medical problems (e.g., tuberculosis or previousintracranial surgery) and all past and current medications,especially steroids, anticoagulants, or cytotoxic drugs, aredocumented

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 52/106
DISORDERS OF THE ADRENAL GLANDADRENAL GLAND HYPOFUNCTION
HISTORY The client is asked about any change in activity level, because
lethargy, fatigue, and muscle weakness are often present Questions about salt intake are included because salt craving is
often a symptom of adrenal hypofunction Gastrointestinal (GI) problems, such as anorexia, nausea,
vomiting, diarrhea, and abdominal pain, often occur. The nurseasks about weight loss during the past weeks or months
Female clients report menstrual changes related to weight loss,and male clients may report impotence
The nurse asks whether the client has had radiation to the abdomen or head.
Significant medical problems (e.g., tuberculosis or previousintracranial surgery) and all past and current medications,especially steroids, anticoagulants, or cytotoxic drugs, aredocumented

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 53/106
DISORDERS OF THE ADRENAL GLANDADRENAL GLAND HYPOFUNCTION
PHYSICAL ASSESSMENT/CLINICAL MANIFESTATIONS
The clinical manifestations of adrenal hypofunction vary,and the severity of symptoms is related to the degree ofhormone deficiency
In clients with primary adrenal hypofunction, plasma ACTHand melanocyte-stimulating hormone (MSH) levels areelevated because of the loss of the adrenal-hypothalamic-pituitary feedback system. Elevated MSH levels result inareas of increased pigmentation
In primary autoimmune disease, areas of decreasedpigmentation may occur because of destruction of
pigmentproducing cells in the skin (melanocytes). Body hairmay also be decreased
In secondary disease, there is no increase in skinpigmentation

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 54/106
DISORDERS OF THE ADRENAL GLANDADRENAL GLAND HYPOFUNCTION

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 55/106
DISORDERS OF THE ADRENAL GLANDADRENAL GLAND HYPOFUNCTION

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 56/106
DISORDERS OF THE ADRENAL GLANDADRENAL GLAND HYPOFUNCTION
The nurse assesses the client for symptomsof hypoglycemia (e.g., sweating,headaches, tachycardia, and tremors) and
volume depletion (postural hypotension anddehydration)
Hyperkalemia (elevated blood levels ofpotassium) can cause dysrhythmias with an
irregular heart rate and result in cardiacarrest

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 57/106
DISORDERS OF THE ADRENAL GLANDADRENAL GLAND HYPOFUNCTION
PSYCHOSOCIAL ASSESSMENT
Depending on the degree of metabolicimbalance, clients may appear lethargic,
apathetic, depressed, confused, and evenpsychotic. The nurse observes the clientand checks his or her orientation to person,place, and time. Families may report that
the client has a decreased energy level,experiences wide mood swings, and isforgetful

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 58/106
DISORDERS OF THE ADRENAL GLANDADRENAL GLAND HYPOFUNCTION

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 59/106
DISORDERS OF THE ADRENAL GLANDADRENAL GLAND HYPOFUNCTION
Plasma cortisol levels fail to rise during stimulationtests
Urinary 17-hydroxycorticosteroids are theglucocorticoid metabolites, and 17-ketosteroid levelsreflect the adrenal androgen metabolites. Both levels
are in the low or low-normal range in adrenalhypofunction Skull x-ray films, computed tomography (CT),
magnetic resonance imaging (MRI), and arteriographymay aid in the search for a cause of pituitaryproblems leading to adrenal insufficiency
Noninvasive procedures of the adrenal gland, such asCT scans without dye, may occasionally show atrophyof the gland. CT scans may help determine adrenalhypofunction

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 60/106
DISORDERS OF THE ADRENAL GLANDADRENAL GLAND HYPOFUNCTION
A rapid ACTH stimulation test may be administered on anoutpatient basis. Cosyntropin 0.25 to 1 mg is givenintramuscularly or intravenously, and plasma cortisol levelsare obtained at 30-minute and 1-hour intervals after thebaseline value is established. In primary insufficiency, thecortisol response is absent or markedly decreased; in
secondary insufficiency, it is decreased
A longer ACTH stimulation test uses a continuous infusion of50 units of ACTH in saline for 24 hours or an 8-hourinfusion daily for 4 to 5 days, with simultaneously collected24-hour urine samples. Levels of urinary 17-hydroxycorticosteroids and urinary free cortisol are alsomeasured. In clients with primary adrenal insufficiency, theresponse is low or absent; in those with secondaryinsufficiency, the value for 17-hydroxycorticosteroids failsto rise above 20 mg per total volume

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 61/106
DISORDERS OF THE ADRENAL GLANDADRENAL GLAND HYPOFUNCTION
Interventions Nursing interventions are aimed at
promoting fluid balance and monitoring forfluid deficit
The nurse or assistive nursing personnelweighs the client daily and records intakeand output. Vital signs are assessed every1 to 4 hours, depending on the client'scondition and the occurrence of
dysrhythmias or postural hypotension.Laboratory values are monitored to identifyhemoconcentrations

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 62/106
DISORDERS OF THE ADRENAL GLANDADRENAL GLAND HYPOFUNCTION
Glucocorticoid and mineralocorticoid deficiencies arecompletely corrected by replacement therapy.Hydrocortisone corrects glucocorticoid deficiency
An additional mineralocorticoid hormone, such as
fludrocortisone (Florinef), may be needed to maintaincorrect electrolyte balance (especially sodium andpotassium). Adjustments in dosage may be necessaryin hot weather, when additional sodium is lostbecause of excessive perspiration
Salt restriction or diuretic therapy should not bestarted without considering whether it mightprecipitate an adrenal crisis

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 63/106
DISORDERS OF THE ADRENAL GLANDADRENAL GLAND HYPERFUNCTION
Hypersecretion by the adrenal cortex may result inexcessive amounts of glucocorticoids, leading tohypercortisolism (e.g., Cushing's syndrome),hyperaldosteronism (excessive mineralocorticoidproduction), or excessive androgen production
Hypersecretion of the adrenal medulla caused by atumor (pheochromocytoma) results in excessivesecretion of catecholamines, of which 80% is
epinephrine and the remainder is norepinephrine

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 64/106
DISORDERS OF THE ADRENAL GLANDADRENAL GLAND HYPERFUNCTION
Hypercortisolism (Cushing's Syndrome) Excessive stimulation of adrenocorticotropic
hormone (ACTH) of either pituitary orectopic origin causes adrenocortical
hyperplasia, which results in loss of normalhormone secretion rhythms
The client's endocrine tissues havedecreased responsiveness to releasinghormones, especially prolactin (PRL),thyrotropin, and gonadotropin. Many clientsalso experience abnormal sleep patterns

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 65/106
DISORDERS OF THE ADRENAL GLANDADRENAL GLAND HYPERFUNCTION
The client with Cushing's syndrome has alterations ofnitrogen, carbohydrate, and mineral metabolism. Anincrease in total body fat results from slow turnover ofplasma fatty acids, and a redistribution of fatproduces the typical body pattern of trancal obesity,"buffalo hump," and "moon face“
Increases in the breakdown of tissue protein and anincrease in urine nitrogen excretion also occur,resulting in decreased muscle mass, atrophic (thin)skin, and bone density loss
High levels of corticosteroids kill lymphocytes and
shrink organs containing lymphocytes, such as theliver, the spleen, and the lymph nodes. Thusprotection of the inflammatory and immune responsesis reduced

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 66/106
DISORDERS OF THE ADRENAL GLANDADRENAL GLAND HYPERFUNCTION
In most cases, increased androgenproduction causes acne, hirsutism(increased hair growth), and occasionally,
clitoral hypertrophy Increased androgen production can also
interrupt the normal hormone feedbackmechanism for the ovary, decreasing the
ovary's production of estrogens andprogesterone. Oligomenorrhea (scant orinfrequent menses) occurs as a result

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 67/106

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 68/106
DISORDERS OF THE ADRENAL GLANDADRENAL GLAND HYPERFUNCTION

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 69/106
DISORDERS OF THE ADRENAL GLANDADRENAL GLAND HYPERFUNCTION
HISTORY The nurse asks about changes in activity or sleep
patterns, fatigue, and muscle weakness. Osteoporosisis common in hypercortisolism, and the client is askedabout bone pain or a history of fractures. The nurse
also questions the client about a history of frequentinfections and easy bruising, which suggesthypercortisolism. Women may report a cessation ofmenses
Gastrointestinal (GI) complaints may indicate ulcerformation from increased hydrochloric acid secretion
The nurse also refers to the client's medical history.Steroid or alcohol abuse can produce the clinical andbiochemical features of Cushing's syndrome

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 70/106
DISORDERS OF THE ADRENAL GLANDADRENAL GLAND HYPERFUNCTION
PHYSICAL ASSESSMENT/CLINICAL MANIFESTATIONS The client with hypercortisolism has characteristic physical
changes. The general appearance of the client is observed.Changes in fat distribution may result in fat pads on theneck, back, and shoulders ("buffalo hump"); an enlargedtrunk with thin arms and legs; and a round face ("moon
face"). Other characteristics include generalized musclewasting and weakness
The nurse also inspects the client for skin changes resultingfrom increased blood vessel fragility, such as bruises, thinor translucent skin, and wounds that have not healed
properly
Reddish purple striae ("stretch marks") are often presenton the abdomen, upper thighs, and upper arms because ofthe degradative effect of cortisol on collagen

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 71/106
DISORDERS OF THE ADRENAL GLANDADRENAL GLAND HYPERFUNCTION

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 72/106
DISORDERS OF THE ADRENAL GLANDADRENAL GLAND HYPERFUNCTION
Excessive cortisol secretion may result in afine coating of hair over the face and bodyand in acne. In the female client, the nurse
looks for the presence of hirsutism, clitoralhypertrophy, and male pattern baldingrelated to androgen excess
Elevations in blood glucose levels are also a
frequent finding Hypertension from water and sodium
retention is common

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 73/106
DISORDERS OF THE ADRENAL GLANDADRENAL GLAND HYPERFUNCTION
PSYCHOSOCIAL ASSESSMENT
Hypercortisolism can result inemotional lability, and the nurse asks
about mood swings, irritability,confusion, or depression
The client may become neurotic orpsychotic as a result of changes inblood cortisol levels

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 74/106
DISORDERS OF THE ADRENAL GLANDADRENAL GLAND HYPERFUNCTION
DIAGNOSTIC ASSESSMENT
Plasma cortisol levels are elevated in clients withhypercortisolism.
Blood for cortisol assays is obtained at the same time
of day because levels vary throughout the day. Plasma ACTH levels vary, depending on the cause of
hypercortisolism
In ectopic (ACTHproducing) syndromes, ACTH levelsare elevated.
In Cushing's syndrome (primary disease of theadrenal gland), ACTH levels are low to immeasurable

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 75/106
DISORDERS OF THE ADRENAL GLANDADRENAL GLAND HYPERFUNCTION
Additional laboratory findings mayinclude the following:
Increased blood glucose level
Elevated white blood cell count
Elevated lymphocyte count
Increased sodium level
Decreased serum calcium level Decreased serum potassium level

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 76/106

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 77/106
DISORDERS OF THE ADRENAL GLANDADRENAL GLAND HYPERFUNCTION
Radiographic studies, computedtomography (CT) scans, magneticresonance imaging (MRI), and
arteriography may identify lesions ofthe adrenal or pituitary glands, lung,GI tract, or pancreas in a client with
clinical manifestations of cortisolhypersecretion

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 78/106
DISORDERS OF THE ADRENAL GLANDADRENAL GLAND HYPERFUNCTION
The overnight dexamethasonesuppression test is an initial screeningtest for Cushing's syndrome. The client is
instructed not to take medications,especially phenytoin (Dilantin) orphenobarbital, for at least 2 days beforethe test. Normally, plasma cortisol levelsare lower than 5 (xg/dL). Higher levelsindicate that further, definitive testing isnecessary

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 79/106
DISORDERS OF THE ADRENAL GLANDADRENAL GLAND HYPERFUNCTION
For the 3-day, low-dose dexamethasone suppression test,the client must take no medications for at least 2 daysbefore the test (if possible) and have no stressfulprocedures (e.g., barium enema, myelogram, or an intensephysical therapy session) performed during the test
A baseline 24-hour urine sample is collected on day 1.
Dexamethasone 0.5 mg is administered every 6 hours ondays 2 and 3, during which time 24-hour urine collectionsare taken
The 24-hour urine collections are tested for 17-ketosteroids, 17-hydroxycorticosteroids, creatinine, andurinary free cortisol
Normally, urinary 17-hydroxycorticosteroid excretion andfree cortisol levels are suppressed by dexamethasone, andCushing's syndrome is ruled out. If these levels are notsuppressed, a higher-dose dexamethasone test isperformed

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 80/106
DISORDERS OF THE ADRENAL GLANDADRENAL GLAND HYPERFUNCTION
The high-dose (8-mg) dexamethasone suppressiontest distinguishes between bilateral adrenocorticalhyperplasia (e.g., Cushing's syndrome) and anadrenocortical neoplasm as the cause ofhypercortisolism
This test can be performed as an overnight test or a2-day test and is similar to the tests previouslydiscussed but uses higher doses of dexamethasone
In the overnight high-dose test, the client with
Cushing's disease will have a reduced plasma cortisollevel that is less than 50% of baseline. This test ismore reliable than the 2-day high-dose test

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 81/106
DISORDERS OF THE ADRENAL GLANDADRENAL GLAND HYPERFUNCTION
Interventions
Goals of treatment for hypercortisolism includereduction of plasma cortisol levels, removal oftumors, prevention of complications, and
restoration of normal or acceptable bodyappearance
Preoperative and postoperative nursing care is anintegral part of the management of the client with
endogenous hypercortisolism because surgicalintervention is usually necessary for the relief ofsymptoms

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 82/106
DISORDERS OF THE ADRENAL GLANDADRENAL GLAND HYPERFUNCTION
NONSURGICAL MANAGEMENT. The nurse weighs theclient daily and monitors intake and output to assesshydration status. Restriction of fluid intake issometimes necessary to maintain fluid balance
DRUG THERAPY. Most clients with endogenoushypercortisolism undergo surgery. Drugs thatinterfere with adrenocorticotropic hormone (ACTH)production or adrenal hormone synthesis, however,may be used for palliation. Mitotane (Lysodren) is an adrenal cytotoxic agent
used for inoperable adrenal tumors Aminoglutethimide (Elipten, Cytadren) is an adrenal
enzyme inhibitor that decreases cortisol production

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 83/106
DISORDERS OF THE ADRENAL GLANDADRENAL GLAND HYPERFUNCTION
Trilostane (Modrastane), also an enzymeinhibitor, has not always been effective
Cyproheptadine (Periactin) is less commonlyused to treat clients with adrenal hyperfunction
resulting from pituitary-related Cushing'sdisease because it interferes with ACTHproduction
During all drug therapy, the nurse assesses
the client for therapy effectiveness and sideeffects or symptoms of toxicity

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 84/106
DISORDERS OF THE ADRENAL GLANDADRENAL GLAND HYPERFUNCTION
RADIATION THERAPY. Radiation, applied internally orexternally, may be used to treat hypercortisolismcaused by pituitary adenomas. However, radiation isnot always effective and also may destroy normaltissue
The nurse observes for any changes in the client'sneurologic status, such as headache, elevated bloodpressure or pulse, disorientation, or changes in pupilsize or reaction
The client may experience skin dryness, redness,
flushing, or alopecia at the radiation site The nurse reviews these possible side effects with the
client

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 85/106
DISORDERS OF THE ADRENAL GLANDADRENAL GLAND HYPERFUNCTION
SURGICAL MANAGEMENT. The surgical treatment ofadrenocortical hypersecretion depends on the causeof the disease
When adrenal hyperfunction is due to increasedpituitary secretion of ACTH, transsphenoidal removal
of an adenoma may be attempted. In many instances,small adenomas cannot be localized andhypophysectomy is needed. Hypophysectomy isperformed via the transsphenoidal or transfrontalcraniotomy route
If hypercortisolism is caused by adrenal adenomas orcarcinomas, a partial or complete adrenalectomy(removal of the adrenal gland) may be needed
DISORDERS OF THE ADRENAL GLAND

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 86/106
DISORDERS OF THE ADRENAL GLANDADRENAL GLAND HYPERFUNCTION
PREOPERATIVE CARE. Electrolyte imbalances arecorrected before surgery, and the nurse monitorspotassium, sodium, and chloride values.Dysrhythmias from potassium imbalance may occur,and cardiac monitoring may be indicated.
Hyperglycemia, if present, is controlled beforesurgery, and the nurse monitors blood glucose levels.
The nurse and assistive nursing personnel attempt toprevent infection with handwashing and aseptictechnique.
DISORDERS OF THE ADRENAL GLAND

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 87/106
DISORDERS OF THE ADRENAL GLANDADRENAL GLAND HYPERFUNCTION
The risk for falls is decreased by raising the siderailsof the bed and encouraging the client to ask forassistance when getting out of bed.
Glucocorticoid preparations are administeredpreoperatively as ordered. The client continues toreceive glucocorticoids throughout the operativeprocedure to prevent adrenal crisis. The removal ofthe tumor results in a sudden drop in cortisol levels.
The nurse discusses postoperative care and long-termmedication therapy during preoperative teaching
DISORDERS OF THE ADRENAL GLAND

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 88/106
DISORDERS OF THE ADRENAL GLANDADRENAL GLAND HYPERFUNCTION
OPERATIVE PROCEDURES. A unilateraladrenalectomy is performed when one gland isinvolved. A bilateral adrenalectomy is necessarywhen ectopic ACTH-producing tumors cannot betreated by other means or when both adrenal glands
are diseased
Surgery can be abdominal or through the lateralflank. Abdominal surgery causes a higher degree ofillness and risk. In the flank approach (the preferred
approach), the abdominal cavity is not entered, andthe morbidity and mortality rates are reduced. A newapproach, laparoscopic adrenalectomy, may reducethe incidence of some postoperative complications
DISORDERS OF THE ADRENAL GLAND

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 89/106
DISORDERS OF THE ADRENAL GLANDADRENAL GLAND HYPERFUNCTION
POSTOPERATIVE CARE. After an adrenalectomy, the client isusually sent to a critical care unit.
In the immediate postoperative period, the nurse assesses theclient every 15 minutes to identify symptoms of cardiovascularcollapse or shock (e.g., hypotension, a rapid, weak pulse, anda decreasing urine output) due to possible insufficient
glucocorticoid replacement. The nurse monitors ongoing vital signs and otherhemodynamic variables (central venous pressure, pulmonarywedge pressure), intake and output, daily weights, and serumelectrolyte levels.
After a bilateral adrenalectomy, clients require lifelongglucocorticoid and mineralocorticoid replacement. The nurse
administers glucocorticoid preparations as ordered. In unilateral adrenalectomy, glucocorticoid replacement
continues until the remaining gland increases hormoneproduction. This therapy may be required for up to 2 yearsafter surgery
DISORDERS OF THE ADRENAL GLAND

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 90/106
DISORDERS OF THE ADRENAL GLANDADRENAL GLAND HYPERFUNCTION
PREVENTING COMPLICATIONS.The client who has hypercortisolism isprone to injury from skin breakdown,
pathologic bone fractures, andgastrointestinal (GI) bleeding.
Prevention of such injuries is a majornursing care focus
DISORDERS OF THE ADRENAL GLAND

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 91/106
DISORDERS OF THE ADRENAL GLANDADRENAL GLAND HYPERFUNCTION
Gastrointestinal Bleeding. Interventions areaimed at minimizing gastric irritation,usually through drug therapy
Drug therapy involves two different typesof agents: those that protect the GI mucosa(antacids) and those that decrease the
secretion of hydrochloric acid (H2-blockers,inhibitors of gastric proton pump)
DISORDERS OF THE ADRENAL GLAND

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 92/106
DISORDERS OF THE ADRENAL GLANDADRENAL GLAND HYPERFUNCTION
Hyperaldosteronism In clients with hyperaldosteronism, increased
secretion of aldosterone results in mineralocorticoidexcess.
Primary hyperaldosteronism (Conn's syndrome) is due
to excessive secretion of aldosterone from one or bothadrenal glands, which is most commonly caused by anadenoma.
In a person with secondary hyperaldosteronism, thecontinuous excessive secretion of aldosterone iscaused by high levels of angiotensin II that are due to
high plasma renin activity. Causes of this reninactivation include renal hypoxemia and the use ofthiazide diuretics.
DISORDERS OF THE ADRENAL GLAND

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 93/106
DISORDERS OF THE ADRENAL GLANDADRENAL GLAND HYPERFUNCTION
Increased aldosterone levels affect the renal tubules andcause sodium retention with potassium and hydrogen ionexcretion.
Hypernatremia, hypokalemia, and metabolic alkalosisresult.
Sodium retention increases blood and interstitial fluidvolume, which elevates blood pressure and suppressesrenin production. The elevated blood pressure may causestrokes and renal damage.
Peripheral edema rarely occurs because of the "renalescape mechanism," in which the proximal tubule decreasessodium reabsorption. However, no compensatorymechanism exists to stop or reverse the loss of potassium
DISORDERS OF THE ADRENAL GLAND

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 94/106
DISORDERS OF THE ADRENAL GLANDADRENAL GLAND HYPERFUNCTION
Assessment
Symptoms related to hypokalemia and elevated bloodpressure are the most common problems of the clientwith hyperaldosteronism.
The history may reveal nonspecific findings, such asheadache, fatigue, muscle weakness, nocturia(excessive urination at night), and loss of stamina.
Polydipsia (excessive fluid intake) and polyuria(excessive urine output) occur less frequently.
Paresthesias (sensations of numbness and tingling)
may occur if potassium depletion is severe. The clientmay have visual changes related to hypertension
DISORDERS OF THE ADRENAL GLAND

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 95/106
DISORDERS OF THE ADRENAL GLANDADRENAL GLAND HYPERFUNCTION
The diagnosis of primary hyperaldosteronism is madeon the basis of laboratory studies and x-ray findings.
Serum potassium levels are decreased, and sodiumlevels are elevated.
Plasma renin levels are low; aldosterone levels areelevated.
Increased hydrogen ion secretion results in metabolicalkalemia (elevated blood pH).
Urine studies show low specific gravity and elevatedaldosterone levels.
Computed tomography (CT) scans reveal thepresence and location of adrenal adenomas
DISORDERS OF THE ADRENAL GLAND

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 96/106
DISORDERS OF THE ADRENAL GLANDADRENAL GLAND HYPERFUNCTION
Interventions Surgery is the treatment of choice for
hyperaldosteronism if the problem is identified in itsearly stages.
Adrenalectomy may be unilateral or bilateral. Surgeryis not performed, however, until the client'spotassium levels are normal.
The physician orders spironolactone (Aldactone,Novospiroton, Sincomen), a potassium-sparing
diuretic and aldosterone antagonist, to promote fluidbalance. Potassium supplements may be ordered toincrease potassium levels before surgery.
DISORDERS OF THE ADRENAL GLAND

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 97/106
DISORDERS OF THE ADRENAL GLANDADRENAL GLAND HYPERFUNCTION
The client may also benefit from a low-sodiumpreoperative diet, but no dietary restrictions areneeded after surgery because aldosterone levelsshould return to normal.
The client who has undergone a unilateraladrenalectomy may require temporary glucocorticoidreplacement, and the client who has undergone abilateral adrenalectomy needs lifelong replacement.Glucocorticoids are administered before surgery to
prevent adrenal hypofunction. The client receivinglong-term replacement therapy should wear a medicalalert bracelet
DISORDERS OF THE ADRENAL GLAND

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 98/106
DISORDERS OF THE ADRENAL GLANDADRENAL GLAND HYPERFUNCTION
When surgery is inadvisable, spironolactonetherapy is continued to control the symptomsof hypokalemia and hypertension.
Because spironolactone is a potassium-sparingdiuretic, hyperkalemia can occur in clients whohave impaired renal function or excessivepotassium intake.
The nurse advises the client to avoid potassiumsupplements and foods rich in potassium.
DISORDERS OF THE ADRENAL GLAND

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 99/106
DISORDERS OF THE ADRENAL GLANDADRENAL GLAND HYPERFUNCTION
Because hyponatremia can occur withspironolactone therapy, the client may requireincreased dietary sodium. He or she is instructed toreport symptoms of hyponatremia, such as drynessof the mouth, thirst, lethargy, or drowsiness.
The nurse alerts clients to report any additional sideeffects of spironolactone therapy, includinggynecomastia, diarrhea, drowsiness, headache,rash, urticaria (hives), confusion, inability tomaintain an erection, hirsutism, and amenorrhea
DISORDERS OF THE ADRENAL GLAND

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 100/106
DISORDERS OF THE ADRENAL GLANDADRENAL GLAND HYPERFUNCTION
Pheochromocytoma Pheochromocytoma is a catecholamine-
producing tumor that arises in chromaffincells
Pheochromocytomas release thecatecholamines epinephrine andnorepinephrine (NE). Excessive epinephrineand NE stimulate alpha receptors and betareceptors and can have wide-ranging
adverse effects mimicking stimulation ofthe sympathetic division of the autonomicnervous system
DISORDERS OF THE ADRENAL GLAND

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 101/106
DISORDERS OF THE ADRENAL GLANDADRENAL GLAND HYPERFUNCTION
Assessment The history may include intermittent hypertensive
episodes or attacks that vary in length from a fewminutes to several hours.
During these episodes, the client experiences severe
headaches, palpitations, profuse diaphoresis, flushing,apprehension, or a feeling of impending doom. Pain inthe chest or abdomen, with nausea and vomiting, canalso occur.
Certain stimuli, such as increased abdominalpressure, urination, and vigorous abdominal
palpation, can provoke a hypertensive crisis. The client may also report heat intolerance, weight
loss, and tremors.
DISORDERS OF THE ADRENAL GLAND

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 102/106
DISORDERS OF THE ADRENAL GLANDADRENAL GLAND HYPERFUNCTION
Diagnostic tests include 24-hour urine collections forvanillylmandelic acid (VMA) (a product ofcatecholamine metabolism), metanephrine, and freecatecholamines, all of which are elevated in thepresence of a pheochromocytoma.
Basal plasma catecholamine levels are elevated afterthe client has been at rest for at least 30 minutes.
The clonidine suppression test is used in the diagnosisof a pheochromocytoma. When oral clonidinehydrochloride (Catapres, Dixarit) is given to a personwho does not have a pheochromocytoma, theclonidine suppresses catecholamine release andreduces the serum catecholamine levels. Theresponse is not seen in the client who has apheochromocytoma.
DISORDERS OF THE ADRENAL GLAND

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 103/106
DISORDERS OF THE ADRENAL GLANDADRENAL GLAND HYPERFUNCTION
When the client suspected of having apheochromocytoma has severe hypertension, testingfor the disorder may include alpha-adrenergicblockade with phentolamine.
Phentolamine (Regitine, Rogitine) is administeredintravenously at a dose of 5 mg, and blood pressure ismeasured every 30 seconds for 3 minutes, then everyminute for 7 minutes.
When a rapid drop of at least 35 mm Hg systolicpressure and 25 mm Hg diastolic pressure results, thetest is considered positive
DISORDERS OF THE ADRENAL GLAND

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 104/106
DISORDERS OF THE ADRENAL GLANDADRENAL GLAND HYPERFUNCTION
After diagnosis, computedtomography (CT) scans of the adrenalglands locate intra-adrenal tumors.
Chest x-ray films and tomograms canlocate tumors in the thoracic area;
arteriograms can locate intra-abdominal tumors
DISORDERS OF THE ADRENAL GLAND

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 105/106
DISORDERS OF THE ADRENAL GLANDADRENAL GLAND HYPERFUNCTION
Interventions Surgery is the treatment of choice for a
pheochromocytoma. One or both adrenal glands areremoved (depending on whether the tumor is bilateral).
Preoperatively, the nurse focuses on adequate tissueperfusion, nutritional needs, and comfort measures.
The nurse monitors the blood pressure regularly andplaces the cuff consistently on the same arm, with theclient in lying and standing positions.
The nurse also identifies stressors that may precede ahypertensive crisis and attempts to minimize them. Theclient is instructed not to smoke, drink caffeine-containing beverages, or change position suddenly.
The abdomen should not be palpated . A diet rich incalories, vitamins, and minerals is provided.
DISORDERS OF THE ADRENAL GLAND

8/10/2019 Pituitary and Adrenal Glands
http://slidepdf.com/reader/full/pituitary-and-adrenal-glands 106/106
DISORDERS OF THE ADRENAL GLANDADRENAL GLAND HYPERFUNCTION
Postoperative nursing care is similar to that for theclient who has undergone an adrenalectomy
The nurse closely monitors the client for hypotensionrelated to the sudden decrease in catecholamine leveland for hypovolemia, especially when the client was
inadequately prepared for surgery. Hemorrhage and shock are possible, and the nurse
administers plasma expanders and fluids asprescribed.
Vital signs, as well as fluid intake and output, are
monitored. If opioids are administered, the nurseobserves their effect on blood pressure
Recommended