Pharmacogenomic Evaluation of Antihypertensive Responses (PEAR)
KEY INVESTIGATORS
University of Florida
Emory University
Mayo Clinic
Julie Johnson(PI)
Rhonda Cooper-DeHoff
Reggie Frye Yan Gong
Arlene Chapman(Site PI)
Eric Boerwinkle(Site PI)
John Gums
Amber Beitelshees(Site PI)
Wolfgang Sadee,(Site PI)
University of Texas at Houston
University of Maryland Ohio State University
Kent Bailey
BACKGROUND Hypertension (HTN) places over 70 million Americans (1 billion individuals
worldwide) at risk for stroke, coronary heart disease, renal failure, and heart failure, and is the most common chronic disease for which medications are prescribed.
Antihypertensive medications are monitored and adjusted based on their effects on blood pressure and certain metabolic parameters, and are utilized to prevent the long-term complications of HTN.
Genetic variability plays an important role in the effects of antihypertensive drugs, including their BP lowering, and adverse metabolic effects, and their influence on clinical outcomes.
OVERARCHING HYPOTHESIS
Discover, replicate and delineate the mechanistic basis for genetic determinants of the BP lowering and adverse metabolic responses to two commonly prescribed classes of antihypertensive drugs, thiazide diuretics and beta-blockers, and the genetic determinants of clinical outcomes associated with these treatments. Our approach will also provide insight into the drug class effect of the genetic associations we study.
OVERARCHING AIMS
PEAR-1Atenolol and HCTZ
INVEST-GENESAtenolol (+ HCTZ) vs.
Verapamil (+ Trandolapril)
Aim 1: BP response associations
Aim 2: AME associations
Illumina HumanCVD 50K BeadChip
Replication cohorts
Replication cohorts
Aim 3: Adverse CV outcomes
associations
Aim 4: New-onset diabetes
associations
Replication in ASCOT
Illumina HumanCVD 50K BeadChipIllumina Human 1M-DUO BeadChip
Aim 5:Targeted resequencing and functional genomics studies
Replicated, functional polymorphisms identified for potential translation to practice
Abbreviations: AME – adverse metabolic effects; BP – blood pressure, CV – cardiovascular HCTZ - hydrochlorothiazide
SPECIFIC AIMS
Aim 1. Antihypertensive response pharmacogenomics. (Led by Julie Johnson, Stephen Turner, Arlene Chapman, Kent Bailey).
Aim 1 Replication efforts. HCTZ replication analyses will be conducted on four cohorts, from the US, Italy and Finland,
that collectively provide 1,479 participants treated with HCTZ. Replication of the β-blocker associations will also arise from four different cohorts, also from the
US, Italy and Finland, totaling 825 β1-blocker treated individuals (mostly whites). To provide much needed replication data in blacks, extend the replication data in whites, and
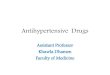
enhance the clinical value of the data, we will conduct a 400 subject clinical study, testing different drugs in the same drug classes, namely metoprolol and chlorthalidone. The flow diagram for the study is shown at the right
Aim 2. Pharmacogenomics of adverse metabolic responses to antihypertensives. (Led by Eric Boerwinkle, Amber Beitelshees, Rhonda Cooper-DeHoff).
Adverse metabolic effects of thiazides and β1-blockers are of increasing concern clinically. Test genetic associations with changes in glucose, triglycerides and uric acid in PEAR.Replication efforts HCTZ replication analyses will be conducted in one US and two Italian cohorts, providing data on 840
whites and 291 blacks. β-blocker replication analyses will arise from two Italian cohorts for a total of 430 whites. There are essentially no data available for replication of β-blocker AMEs in blacks, making the
proposed clinical study particularly important to this aim.
Aims 3 and 4. Pharmacogenomics of protection against adverse cardiovascular (CV) outcomes and new onset diabetes. (Led by Julie Johnson, Rhonda Cooper-DeHoff, Amber Beitelshees, Eric Boerwinkle).
Primary analyses in Aims 3 and 4 arise from data from the International Verapamil SR-Trandolapril Study Genetic Substudy (INVEST-GENES), for which approximately 6,000 genetic samples are available. INVEST randomized hypertensives with coronary artery disease to treatment with a β-blocker (+ HCTZ) or calcium channel blocker (+ ACE inhibitor) treatment strategy.
Aim 3 will focus on genetic associations with adverse outcomes in hypertension, including death, myocardial infarction (MI) and stroke (INVEST primary outcome).
Aim 4 will determine genetic associations with drug-associated new onset diabetes (INVEST secondary outcome). Genetic associations will be conducted on the Illumina Human50K CVD Bead Chip data.
Replication efforts. Findings from INVEST-GENES will be replicated in the Anglo-Scandinavian Cardiac Outcomes Trial (ASCOT), which included 19,257 high risk hypertensive participants, also randomized to a beta-blocker + thiazide or a CCB + ACE inhibitor treatment strategy. Primary and secondary outcomes were similar to INVEST.
Aim 5. Resequencing and molecular functional mechanisms in antihypertensive drug pharmacogenomics. (Led by Wolfgang Sadee, Eric Boerwinkle, Taimour Langaee).
Replicated genetic associations arising from Aims 1-4 will be further investigated to identify the functional polymorphism(s) and define the mechanistic basis for their effects.
Using next-generation sequencing approaches, we will sequence the genomic region of interest in individuals sampled from the extremes of clinical response.
We will also carry out intensive molecular studies focused on potential sources of functional effects, including nonsynonymous variation and differential expression.
POPULATIONS BEING STUDIED AND RESOURCES AVAILABLE
Uncomplicated hypertensives (no cardiovascular, renal, liver disease or diabetes) studied for BP and adverse metabolic responsesEthnically diverse population, approximately
45% minority (42% black)Phenotype data include: home BP, 24 hour
ambulatory BP, office BP, numerous metabolic phenotypes, including glucose, insulin, complete lipid panel, uric acid, plasma renin activity, extensive medical history and clinical/demographic data I including smoking and alcohol history
Biological resources include: DNA, plasma, serum and urine from multiple study time points; lymphocyte RNA from multiple study time points, lymphoblastoid cell lines
High risk hypertensives from large clinical trial
>50 years old, with hypertension + documented coronary artery disease
Extensive medical/demographic informationEthnically diverse population, approximately 47%
white, 42% Hispanic, 11% black
Taimour Langaee
SPECIFIC AIMS
Test genetic associations of BP response to two antihypertensive drug classes, the thiazide diuretics and β1-selective adrenergic receptor blockers, utilizing PEAR data which includes 50K Illumina Cardiovascular Gene Chip data and Illumina 1M Quad GWA data.
Stephen Turner (Site PI)
Clorthalidone 15 mg daily
Metoprolol IR 50 mg bid
HBP, OBP, blood & urinesamples for labs, DNA, RNA
HBP, OBP, blood & urinesamples for labs, DNA, RNA
6 weeks++
2 weeks
Clorthalidone 25 mg daily
Metoprolol IR 100 mg bid
Washout if treated: Minimum 3 weeks;
4 weeks recommended
Eligibility determinationMetoprolol baseline studies:
HBP, OBP, blood & urine samples for labs, DNA, RNA
Chlorthalidone Baseline StudiesHBP, OBP, blood & urine samples for
labs, DNA, RNA
++Patients will have dose up-titrated if BP > 120/70; otherwise continue initial
dose 4 more weeks
Min 3 week washout4 weeks recommended
2 weeks
6 weeks++
Study entry, screening
Clinical study diagram
Recommended