77
Acta Dermatovenerol Croat 2009;17(1):77-83 LETTER TO THE EDITOR
Pediculosis Pubis and Dermoscopy
Pediculosispubis(PP)isinfestationwithpubiclice of the species Phthirus pubis.There are noratial differences in its incidence and the infes-tation isgenerally common (1).Direct contact istheprimarysourceoftransmission.Inadults,PPmost frequentlyoccursasasexually transmitteddisease (STD), commonly associated with otherSTDs(1).However,transmissionmayoccurfromsheetsandclothing. Phthirus pubishabituatesregionsthatarerichin apocrine glands, so predilection sites are pu-bicarea,axillaeandeyelashes.Scalphair,beard,moustache,and inhirsute individualsshorthairsofthethighs,trunkandperianalareamaybein-volved (1). Phthirus pubis in eyelashes and pe-riphery of the scalp is mainly found in children,probablyastheresultofcontactwithaninfectedparent(1). Pubic lice feed and reproduce on the humanhost cementing their nits to the hair shaft 1 cmfromtheskinsurfaceandnitshatchin8to10days(1).Themajorityofpatientscomplainofpruritus.Pruritus is moderate. Typical clinical findings are blue to grey macules (sky-blue spots), maculae ceruleae,sizedfromseveralmillimeterstoseveralcentimeters (1). Excoriations are not commonlyfound. Secondary infection due to excoriationscanleadtolocallymphadenitisandfever.
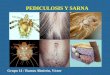
Pubic licecansometimesbemacroscopicallyidentified with the naked eye and with a magnifying lens (1). The diagnosis is confirmed by microscop-icexaminationof thepluckedhair to identify thenitswithvitalnymphsandhatchedemptycases(1). Lice are difficult but possible to see with close inspection or magnification. Additionally, dermos-copyallowstodifferentiatenitswithvitalnymphsfromemptycasesandtoidentifypubiclice(2). We present a 33-year-old male patient withsymptomsofmoderatepubic itch lasting for twoweeks. Clinically, whitish to brownish nits fixed to thehairandfewaliveandmovingliceinthepubicareawereseen.Otherpartsofthebodywerenotinfected. Dermoscopy with a noncontact and contacthandheld dermoscope (DermLite Platinum andDermLiteIIPRO-HR,3Gen,LLC)wasdone.Der-moscopyofaffectedhairshowednitscontainingan unhatched nymphs (Fig. 1) and translucentempty cases. Also, the Phthirus pubis wasvisual-ized(Fig.2). Treatmentwithlindane1%shampoowasdoneintwocyclesfor3weeks,alongwithnitremoval.The response to treatment was good. At control
Figure 2. Alive Phthirus pubis seen under thehandheld dermoscope: typical crab-like appear-ancewithashortovalbodyandprominentclaws(DermLite II PRO-HR, 3Gen, LLC; Sony DSC-P200). (original magnification X10)
Figure 1. A lice egg with nymphs attached to the pubichairshaft(DermLiteIIPRO-HR,3Gen,LLC;Sony DSC-P200. (original magnification X10)

78 ACTA DERMATOVENEROLOGICA CROATICA
visitthepatientwasfreefromanysymptomsandnonitsorlicewereobserved. Dermoscopyisanoninvasivetechniqueusedintheevaluationofpigmentedskinandnonpigment-edskinlesions,particularlyfortheearlydetectionsofmelanoma(3).Furthermore,itisalsoemployedas an adjunct to clinical examination in generaldermatology(4).“Entodermoscopy”isanewtermemployed for dermoscopy of skin infections andinfestations, recently introduced by Zalaudek et al. (5). It isused for thediagnosisand treatmentfollow-upforviralwarts,molluscumcontagiosum,scabies,tineanigra,tungiasis,cutaneouslarvami-grans,tics,andreactionstospiderlegspins(5-9).Furthermore, it iswell established in thediagno-sis and treatment follow-up in pediculosis capitisandpubis(2,10,11). In vivo dermoscopic findings withnoncontacthandhelddermoscopeofpedicu-losiscapitisshowsovoidbrownnitswithnymphs,whileemptycasesaretranslucentwithplaneandfissured free ending (10). Practical technique with examination of the hair on transparent adherenttapewithcontacthandhelddermoscopeforthedi-agnosisofpediculosiscapitishasbeendescribed(11). Alive and moving lice were seen in PP per-formingdigitaldermoscopyinrealtimeprojectiononthemonitor(2). Inourcase,dermoscopywithnoncontactandcontact handhelddermoscopeenabledus toes-tablisharapiddiagnosisvisualizingunhatchedandhatchednitsandlice,andalsotreatmentfollow-up.Therefore, in vivo dermoscopy isa safe, reliableand simple method in diagnosing and treatmentmonitoringofPPthatcanbeusedindailyroutine.
Dragomir Budimčić1, Jasna Lipozenčić1, Zrinjka Paštar2, Ružica Jurakić Tončić1
1UniversityDepartmentofDermatologyandVenereology,ZagrebUniversityHospitalCenter
andSchoolofMedicine;2HealthDepartment,MinistryofDefense,Zagreb,Croatia
Corresponding author: Dragomir Budimčić, MD, MSc
UniversityDepartmentofDermatologyandVenereology
ZagrebUniversityHospitalCenterandSchoolofMedicineŠalata4
HR-10000ZagrebCroatia
Received:March11,2008Accepted: January 20, 2009
References1. StoneSS.Scabiesandpediculosis.In:Free-
dberg IM, Eisen AZ, Wolff K, Austen KF, Goldsmith LA, Katz SI, editors. Fitzpatrick`s DermatologyinGeneralMedicine.6thEd.NewYork(NY):McGrawHill;2003.pp.2283-9.
2. ChuhA,LeeA,WongW,OoiC,ZawarV.Di-agnosisofpediculosispubis:anovelapplica-tionofdigitalepiluminescencedermatoscopy.J Eur Acad Dermatol Venereol 2007;21:837-8.
3. Argenziano G,SoyerHP,ChimentiS,SalaminiR,CoronaR,SeraF,et al.Dermoscopyofpig-mented skin lesions: results of a consensusmeetingvia the Internet. J Am Acad Dermatol 2003;48:679-93.
4. Zalaudek I,Argenziano G,DiStefaniA,Fer-rara G, Marghoob AA, Hofmann-WellenhofR,et al.Dermoscopyingeneraldermatology.Dermatology2006;212:7-18.
5. Zalaudek I, Giacomel J, Cabo H, Di StefaniA, Ferrara G, Hofmann-Wellenhof R, et all. Entodermoscopy: a new tool for diagnosingskin infectionsand infestations.Dermatology2008;216:14-23.
6. Argenziano G, Fabbrocini G, Delfino M. Epilu-minescence microscopy. A new approach to in vivodetectionofSarcoptes scabiei. Arch Der-matol1997;133:751-3.
7. Bauer J, Forschner A, Garbe C, Röcken M. Dermoscopy of tungiasis. Arch Dermatol 2004;140:761-3.
8. Di Stefani A, Rudolph CM, Hofmann-Wel-lenhof R, Müllegger RR. An additional der-moscopic feature of tungiasis. Arch Dermatol 2005;141:1045-6.
9. Elsner E,Thewes M, Worret WI. Cutaneouslarvamigransdetectedbyepiluminescentmi-croscopy. Acta Derm Venereol 1997;77:487-8.
10.DiStefaniA,Hofmann-WellenhofR,ZalaudekI. Dermoscopy for diagnosis and treatmentmonitoring of pediculosis capitis. J Am Acad Dermatol2006;54:909-11.
11.BakosRM,BakosL.Dermoscopyfordiagno-sisofpediculosiscapitis.J Am Acad Dermatol2007;57:727-8.
Acta Dermatovenerol CroatLettertotheeditor 2009;17(1):77-83

79ACTA DERMATOVENEROLOGICA CROATICA
Anaphylactic Shock Caused by a Cosmetic Cream Applied Fourteen Hours Before Manifested on Medical Examination: Case Report
A case of a female patient who sought medical attentionduetoasevere,yetlocalized,dermato-logicallergicreactiontoacosmeticcreamispre-sented. A written informed consent was obtained fromthepatientforpublishingthiscase,withmu-tualunderstandingthatnophotographswouldbetakeninsupport. The patient applied the cream to her face inthe evening before examination. The changeswerestrictlylimitedtotheareaswherethecreamhad been applied. On examination, the patientpresentedthepackagecontainingtherespectivecream but did not open it at any point. A few min-uteslater,whilethenecessarypreparationsweremade to administer appropriate therapy, the pa-tient fell to the floor, presenting the signs of ana-phylacticshock.Immediateinterventionincludingadrenaline administration proved efficient. We still cannot state for sure whether our patient devel-opedanextremelydelayedanaphylacticreaction,ortheanaphylaxiswasprovokedbytouchingtheunopened cream box, probably covered with anon-visiblecreamresidue.Cliniciansarestronglyadvised toexercisecautionwithallpatientspre-sentingwithanacutelocalizedskinallergy,andtoadvisepatientstoavoidanypotentialre-exposure,even to unbroken skin. Patients should also beinstructed toavoid contactwith itemscontainingthedocumentedorsuspectedallergen,duetothepossibilityofthepackagingcontaininganinvisibleresidueofthesubstance. Ithasbeenwidelyrecognizedthatalmostanysubstancemayinduceanallergicreaction,asin-ertsubstancesarerare.Life-threateningreactionssuch as anaphylaxis are only rarely induced bypurecontactwithunbrokenskin.Incaseofdam-aged skin, passive cutaneous anaphylaxis mayalso develop. As a rule, anaphylactic reactions de-velopquickly. There are no previously published cases ofanaphylacticshockbeingcausedbyapresumedinertsubstanceemployedforcosmeticpurposes,causedbypurecontactwithunbrokenskin,anddevelopingsosuddenly,morethan10hoursaftercontact,asinthecasepresented.
Thecasepresentedwasencounteredatagen-eral practitioner office. A young woman, not one of regular patients, asked for help because of asevere, yet localized, allergic skin reaction.Herwholefacewasextremelyedematous,somuchsothatshewasunabletoopenoneeyeandtheotheroneonlybarely,byabout2mm.Theedemawasstrictly limited to the regionof the face towhichthecosmeticcreamhadbeenappliedonthepre-viousevening.Theedematousedgewassoclearthatitsthicknesscouldbesetatabout1-1.5cm,andwasnotoverlappingbeyondthehairline. Inadditiontotheedema,theaffectedskinwasbrightredandcoveredwithsoresdevelopeddur-ingthenight,showingacuteeczematouschang-es, with yellowish serous secretion. The patientcomplainedofitchingandburninginherface.Shegave affirmative answer to the question whether shehadputthecreamontoherfacewithherbarehands. The next logical question was why herhandsshowednoeffectsatall.Inresponse,sheshowedustwolittlepapulesonthedorsalsideofonehand.Shesaid shehadwashedherhandsbefore going to sleep, after putting the creamontoherface.Shehadbeenusingtheverysamecreamregularly. Therewerenootherskinreactions,i.e.noitch-ing, no urticaria, and no erythema on the otherparts of her skin. No systemic reactions wereobserved either; her heart rate and blood pres-surewerenormal;therewasnodyspneaandnodysphagiaintermsofswallowingdisorder,oranybronchialspasmwhatsoever.Shetalkednormally,havinganormalsoundofhervoice,andwasfullyconscious.Onlytheaffectedareasofherfacehadbeenaggressivelyalteredbythesubstance. Onexamination,shetooktheoriginalpackagecontainingthecreamshehadappliedtoherfaceoutofherhandbag,andsimplyshowed it tous,keepingitclosed.Inthenext15-20minutes,whilewewerepreparingher therapy(notyetadminis-teredcorticosteroids), shepresentedwithanewitchingattackandaquicklydevelopingerythemathatprogressedtogeneralizedurticaria.Wewerenotsurewhereitstarted;probablyonherhands,
Acta Dermatovenerol CroatLettertotheeditor 2009;17(1):77-83

80
asshesubsequently claimed,but theonsetwassorapidthatwewereunabletowitnessthestartinglocalization.Shedevelopedtachycardia;herpulsebecame weak and almost impalpable. Strugglingforairandwithobviousfearandrestlessness,shegrasped her chest and finally fell from the chair down to the floor. The pulse over the carotid arteries wasnolongerpalpable,theskinhadturnedgray-ish-blue, her blood pressure became immeasur-able,andshelostconsciousness.Herveinswerealready collapsed, but the standard anti-anaphy-lactic therapy was efficient, starting with adrenaline dilutedwithwaterina1:10ratio.Uponresuscitationandtheexpectedpost-adrenalinereaction(severetremor involving her whole body), she regainedconsciousnessandgraduallybecamestable. Thepatientwasobservedinthesurgeryforthenext8hours,butnoadditionalreactionsoccurred.Sherefusedtobereferredtoahospital.Theonlyproposalsheacceptedwastovisitusonthenextday.Wealsowashedherhandsagaininordertoremoveanypotential(althoughinvisible)residueofthecream,andthrewawaythecreampackagetoprevent any new possible reactions. We decidedagainst washing the patient’s face, as it seemedtoovulnerable. On thenextday,onlyminimal improvement intheconditionoftheskinonherfacewasobserved,however,onthedayafterimprovementbysome30percentwasrecorded.Thecircumstancesdidnotallow appropriate tests to make (patient-traveler,refusinghospital treatment,maybe tooashamed,promisingtomakethetestswhencomingbacktohercountry,creamboxthrownaway,unexpectedsituationatall,etc.).
Thiscaseposedatleastthreeissues: 1) Was there something at the GP surgery that provoked a new severe allergic reaction?- The patient denied any previous allergic mani-festations, so she did not suffer from multipleallergies,reactingtomanydetectedandundetect-edallergens.- Prior to anaphylaxis, she had not taken anymedication whatsoever. We were just preparinghertherapy,butwewereyettoadministerit.- Moreover, we left the patient in the office, sep-aratingher fromotherpatientsdue to theseveredisfiguration of her face. Therefore she was inside, waitingforabout40minutes,inhalingthesameair,andnothinghappeneduntilshetouchedthecreamboxduringorpossibly justafter theexamination.In addition, the reactiondidnot includebroncho-spasm,which isotherwiseverycommon inaller-giescausedbyinhalantsornutritiveallergens.
2) Was it a markedly delayed generalized al-lergic reaction? Eventhoughveryrare,anaphylaxiscausedbysimply touchinganallergenhasbeenpreviouslydocumented.Suchallergicreactionstocontactal-lergens,even to theextentofanaphylaxis,weremost commonly described with latex (1-3), butalso many other allergens, and included cross-reactionsinaddition(1,3,4).Itisalsoknownthatcosmetics,ortheiringredients,maycausecontactallergy(3,5-10).Bothcosmeticsandothercontactallergensmayleadtoananaphylacticreaction,orcausecoexistinglocalandsystemiclife-threaten-ing reactions (1-4,6,7,9-19). According to literature reports, type IVallergic reactions (cell-mediated,local reaction) donot necessarily exclude type Iallergic reaction (anaphylaxis, immunoglobulin-mediated)(3,6,10,13,16,17).Thetwotypesofre-actions,evenonlytocontactallergen,mightoccurinthesamepersonsuccessively,oneafteranoth-er,orsimultaneously, i.e.bothat thesametime.Thepresentedpatienthadacombinationoflocalandsystemicallergic reaction;not triggeredwithphysical activity, as in exercise-induced anaphy-laxis(20).Suchaseverereactionismorelikelytobecausedbyadeclaredallergen(1,6,11),mostlywithoccupationaldailyexposure. The case described is even more intriguingbearinginmindthatthecreamwasclaimedtobedermatologicallytestedandproducedbyaworld-famous manufacturer. The phrase “dermatologi-cally tested” does not mean that the product issafeforeveryone(21,22). Passive cutaneous anaphylaxis also occursrapidly,butonlyiftheallergenpenetratesintotheskin.Theskinonourpatient’shandswas intactandnothingatallwasgiventoherbeforetheon-set of the reaction described. However, classicanaphylactic reaction may develop by virtue ofpurecontactwithunbrokenskin(1,6,7,10-12). By definition, anaphylactic reaction develops quickly. However, in this case, the anaphylacticreactionoccurredabout12-14hoursafterapply-ingthecreamtotheface.Thepatientcamewithanobviousbutlocalizedreaction:severechangeson the skin of her face and two papules on thehand.Thecreamwasonher face for thewholeofthenight,and,asitseems,shecouldwellhavediedatanypointduringthenightorthenextmorn-ing.Onherarrival,withthecreamstillonherun-washed face, she did not show a single sign ofsystemicallergy. Medical literature lacks any documentationconcerning anaphylaxis provoked by a contact
Acta Dermatovenerol CroatLettertotheeditor 2009;17(1):77-83
ACTA DERMATOVENEROLOGICA CROATICA

81
allergen, constitutinga cosmetic preparationap-plied tounbrokenskin, especially not in caseofallergypresentingafterasmanyas12-14hourspost-contact. There is a report on anaphylaxisdue to such an allergen, which developed threehoursaftertheapplication,asareactionfollowingrepeatedcontactinoccupationalsetting(6).Usu-ally, it takes 5-30 minutes from exposure to thereaction.
3) Was it really a re-exposure to the aller-gen? The reaction developed about 15-20 minutesafter touching the cream packet. Nevertheless,thepatientdidnotopenthebox,therewasnovis-ible residue of the cream on the box, and mostimportantly, thecreamhadalreadybeenappliedtothepatient’sfaceandhadnotbeenwashedoff.Byvirtueofastrongtimecorrespondence,andinabsenceofotherconvincingpossibilities,thisop-tionseemstobemostlikely. One possible explanation for this hypothesisis that the cream had some labile components,whichcouldhavebeenslightlychemicallyalteredwith intensive skin secretion over 10 hours. So,touching the cream again could be consideredre-exposure.Thesecondpossibleexplanation isallergytotheperfumecomponent,whichispres-entinalmosteverycosmeticcream.Theperfumecould have evaporated from the skin during 10hoursandnewcontactcouldbere-exposure.Per-fumesarewellknownallergens.Thethirdandthesimplestexplanationisthattheskinabsorbedtheallergenduringthenight. Itmightalsobeusefultoobservepatientspre-senting with only local allergic reactions over aprolongedperiod,andnot just togivethemtheirtherapy as soon as possible and let them walkawaybecausecomplicationsofanunforeseense-verityandnaturemayoccurinthetimetocome.
Vesna Kos
DepartmentofGeneral/FamilyMedicine,SchoolofMedicine,UniversityofZagreb,Zagreb,Croatia
Corresponding author:Vesna Kos, MD, MSc
DepartmentofGeneral/FamilyMedicineUniversityofZagreb
Rockefellerova4HR-10000Zagreb
Received:February28,2008Accepted: February 22, 2009
References1. Anda M, Gomez B, Lasa E, Arroabarren E,
GarridoS,EchechipiaS.Latexallergy.Clini-cal manifestations in the general populationand reactivity crossed with foodstuffs. An Sist SanitNavar2003;26Suppl2:75-80.
2. CogenFC,BeezholdDH.Hair glueanaphy-laxis: a hidden latex allergy. Ann Allergy Asth-maImmunol2002;88:61-3.
3. Fujie S, Yagami A, Suzuki K, Akamatsu H, Matsunaga K. A case of the latex-induced anaphylaxisbycontactwithbariumenemaca-theter. Arerugi 2004;53:38-42.
4. Lipozencić J, Wolf R. Life-threatening severe allergicreactions:urticaria,angioedema,andanaphylaxis.ClinDermatol2005;23:193-205.
5. Blumenfeld O, Nathansohn N, Yeshurun I, As-hkenaziI.Eyecosmetics–thebeautyandthebeast.Harefuah2005;144:357-62,381.
6. Babilas P, Landthaler M, Szeimies RM. Anap-hylacticreactionfollowinghairbleaching.Hau-tarzt2005;56:1152-5.
7. Mozelsio NB, Harris KE, McGrath KG, Gram-merLC. ImmediatesystemichypersensitivityreactionassociatedwithtopicalapplicationofAustralian tea tree oil. Allergy Asthma Proc 2003;24:73-5.
8. Engasser PG. Lip cosmetics. Dermatol Clin2000;18:641-9.
9. HughesTM,StoneNM.Benzophenone4:anemergingallergenincosmeticsandtoiletries?ContactDermatitis2007:56:153-6.
10. Krautheim AB, Jermann TH, Bircher AJ. Chlorhexidine anaphylaxis: case report andreview of the literature. Contact Dermatitis2004;50:113-6.
11.SachsB,Fischer-BarthW,ErdmannS,MerkHF, Seebeck J. Anaphylaxis and toxic epider-mal necrolysis or Stevens-Johnson syndrome afternonmucosaltopicaldrugapplication:factor fiction? Allergy 2007;62:877-83.
12. Autegarden JE, Pecquet C, Huet S, Bayrou O, Leynadier F. Anaphylactic shock after applica-tionofchlorhexidinetounbrokenskin.ContactDermatitis1999;40:215.
13. Potter PC, Mather S, Lockey P, Knottenbelt JD, Paulsen E, Skov PS, et al.Immediateand
Acta Dermatovenerol CroatLettertotheeditor 2009;17(1):77-83
ACTA DERMATOVENEROLOGICA CROATICA

82
delayed contact hypersensitivity to verbenaplants.ContactDermatitis1995;33:343-6.
14.Ebo DG, Verheecke G, Bridts CH, MertensCH, Stevens WJ. Perioperative anaphylaxis fromlocallyappliedrifamycinSVandlatex.BrJ Anaesth 2006;96:738-41.
15. Tan BM, Sher MR, Good RA, Bahna SL. Se-vere food allergies by skin contact. Ann Allergy Asthma Immunol 2001;86:583-6.
16. Lauerna AI. Simultaneous immediate and de-layed hypersensitivity to chlorhexidine diglu-conate.ContactDermatitis2001;44:59.
17. Tabar AI, Alvarez MJ, Echechipía S, Acero S, Garcia BE, Olaguíbel JM. Anaphylaxis from cow’s milk casein. Allergy 1996;51:343-5.
18. Pietroletti R, Navarra L, Simi M. Anaphylactic reactioncausedbyperianalapplicationofgly-ceryl trinitrate ointment. Am J Gastroenterol 1999;94:292-3.
19. Laing ME, Fallis B, Murphy GM. Anaphylactic reaction to intralesional corticosteroid injec-tion.ContactDermatitis2007;57:132-3.
20. Codreanu F, Morisset M, Cordebar V, Kanny G, Moneret-Vautrin DA. Risk of allergy to food proteins in topicalmedicinalagentsandcos-metics. Allerg Immunol (Paris) 2006;38:126-30.
21. Noiesen E, Munk MD, Larsen K, Johansen JD, Agner T. Difficulties in avoiding exposure toallergens incosmetics.ContactDermatitis2007;57:105-9.
22. Timmermans A, De Hertog S, Gladys K, Va-nacker H, Goossens A. ”Dermatologically tested”babytoilettissues:acauseofallergiccontactdermatitisinadults.ContactDermati-tis2007;57:97-9.
Human Dirofiliariasis in Croatia
DearEditor, Ireadwithgreatinterestthearticle“Subcutane-ous dirofilariasis caused by Dirofilaria repensdi-agnosedbyhistopathologicandpolymerasechainreaction analysis”, published in the last issue ofActa Dermatovenerologica Croatica. The authors of the article describe a case of human dirofilaria-siswithtypicalsubcutaneouspresentationoftheparasite.TheycitethiscaseasthefourthreportedcaseofthediseaseinCroatia(1). However, dirofilariasis in Croatia has been reported more frequently than it looks at the first glance.The main reason for this discrepancy isthat somecaseshavebeen reported in journalsandotherpublicationswithpoorornovisibility. The first case reported was the case of con-junctival dirofilariasis described by Bujger et al.in1996,publishedinOphthalmologiaCroatica.Un-awareofthiscase,duetoitsinvisibilityinthemainjournal databases, in 2003 Puizina-Ivić et al. re-ported two cases of the disease as the first cases of human dirofilariasis in Croatia. Actually, these were the first reported cases of the subcutaneous formofthediseaseinourcountry,followedbythecasepresentedassubcutaneousmammarynod-
ule (3,4). All of these subcutaneous cases were fromthesouthernpartofCroatia,whereadditionalcaseswerefrequentlyencounteredandreported(5,6). In 2007, another case of ocular dirofilariasis wasreported, followedby two reportedcasesofthesubcutaneousformofthedisease,allfromtheinlandpartofCroatia(7,8). Inallof the reportedcases,Dirofilaria repenswas identified as the causative agent. Altogether, including the case reported in your journal, at least 10 human cases of this emerg-ingzoonosishavebeenreportedinCroatiasofar,confirming the conclusion by Marušić et al. thatCroatia represents an endemic area, like othercountries in the Mediterranean basin (1). As the majority of cases presented as subcutaneousnodules,dermatologistsanddermatopathologistsshouldfamiliarizethemselveswiththeclinicalandhistologic aspects of the disease, considering itin thedifferentialdiagnosisofsolitarynodules insubcutaneoustissue.
Joško Bezić
Acta Dermatovenerol CroatLettertotheeditor 2009;17(1):77-83
ACTA DERMATOVENEROLOGICA CROATICA

83
Acta Dermatovenerol CroatLettertotheeditor 2009;17(1):77-83
InstituteofPathology,CytologyandForensicMedicine,SplitUniversityHospitalCenter,Split,
Croatia
Correspondending author:Joško Bezić, MD
InstituteofPathology,CytologyandForensicMedicineSplitUniversityHospitalCenter
Spinčićeva 1HR-21000Split
References1. Marušić Z, Slastny T, Kirac I, Stojčević D,
Krušlin B, Tomas D. Subcutaneous dirofila-riasis caused by Dirofilaria repens diagno-sedbyhistopathologicandpolymerasechainreaction analysis. Acta Dermatovenerol Croat 2008;16:222-5.
2. Bujger Z, Ekert M, Tojagić M, Čačić M, Granić J. Dirofilaria conjunctivae. Ophthalmol Croat1996;5:63-6.
3. Puizina-Ivić N, Džakula N, Bezić J, Punda-Polić V, Sardelić S, Kuzmić-Prusac I. First two
cases of human dirofilariasis recorded in Cro-atia.Parasite2003;10:382-4.
4. Bezić J, Vrbičić B, Guberina P, Alfier V, Projić P, Marović Z. A 52-year-old woman with a sub-cutaneous,slightlymovableandpainlessno-dule in the left breast. Subcutaneous breastnodule due to Dirofilaria repens infestation.Ann Saudi Med 2006;26:403-4, 414-6.
5. Bezić J, Kuzmić-Prusac I, Vrbičić B, Njirić Z, Puizina-Ivić N. Subcutaneous dirofilariasis in Dalmatian region of Croatia. Proceedings ofthe Third Croatian Congress on PathologyandForensicMedicine;2005May8-11;Opa-tija,Croatia;p.68.
6. Paić M, Vrbičić B, Stegić M, Reljić D. Case of dirofilariasis infection of epididymis: clinical, ultrasonographical and histopathological fea-tures. Proceedings of the EAU Seventh Cen-tral European Meeting; 2007 Oct 26-27; Za-greb,Croatia;p.52.
7. Juri J, Kuzman T, Stiglmayer N, Tojagić M. A case of lacrimal gland dirofilariasis. Ophthal-mologica2007;221:204-6.
8. Vicković N, Granić J, Desnica B, Makek N, Balen-Topić M. Subcutaneous dirofilariasis – a casereport.Infektoloskiglasnik2007;27:135-7.
CosmeticproductsNobilior;year1929.(FromthecollectionofMt.ZlatkoPuntijar)
ACTA DERMATOVENEROLOGICA CROATICA
Recommended


![Clinical and videodermoscopic look of pediculosis corporis....humanus corporis in detail on all sites infected with lice [3]. Figure 2: Dermoscopy of a louse of Pediculus humanus corporis](https://img.pdfslide.us/doc/110x75/6088caa7aa1079274b4aef57/clinical-and-videodermoscopic-look-of-pediculosis-humanus-corporis-in-detail.jpg)