PEDICLED FLAPS IN HEAD AND
NECK SURGERY Dr . Rama raju

MYOCUTANEOUS FLAPS
• Commonest reconstructive option for head and neck defects include:
1. Pectoralis major myocutaneous flap2. Latissimus dorsi flap3. Trapezius flap4. Stenomastoid flap5. Platysma flap• PMMC flap and latissimus dorsi flaps still represent the
workhorses for some head and neck reconstructive surgeons around the world

Blood supply to the muscles • Random• AxialRandom : perforators enters the
belly and immediately break up in to branches (round muscles like SCM)
Axial : major artery runs the entire length of muscle giving perforators (flat muscles like PM,LD)

PECTORALIS MAJOR FLAP
ANATOMY :• Orgin -clavicle, sternum, upper
seven ribs• Insertion – bicipital groove of
humerus• Blood supply –Acromiothoracic artery branches1) Superior clavicular branch2) Main pectoral branch a)Inferior thoracoacromial branch
b) Lateral thoracic trunk

ADVANTAGES OF PMMC FLAP
1. Large skin territory with rich vascular supply2. Large arc of rotation 3. Can be harvested in supine position4. Either muscle only or skin and muscle paddle can be
used5. Primary donor site closure is easily achieved

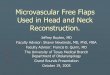
TECHNIQUE SURFACE MARKING:• A dotted line is marked from
acromion to xiphoid process and another dotted line is drawn perpendicular to first line from sternal notch , this point represents the location of vascular pedicle( acromiothoracic artery)
• Skin island is drawn over distal part of artery
• The border of skin island is stenum medially and the nipple laterally

STEPS OF PMMC FLAP ELEVATION
Skin paddle has been marked over the caudal , medial portion of the chest wall

The lateral margin of the pectoralis major is identified through wide undermining of the skin of lateral chest wall

A circumferential incision around the skin paddle has been completed, along with exposure of entire pectoralis major muscle.

• Pectoralis major muscle is elevated off the chest wall by sharp and blunt dissection

• Medial attachments of the muscle are transected till the level of clavicle.
• Careful attention should to paid to stay lateral to perforators of internal mammary artery at the level of 2nd and 3rd intercoastal spaces to preserve blood supply to deltopectoral flap

• Plane between pectoralis major and minor is usually avascular ,so blunt dissection with finger is done.
• Pectoral branch of thoracoacromial artery is easily visualised in the undersurface PM muscle
• Vascular pedicle is usually located medial to pectoralis minor

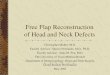
Muscular attachments to humerus are transected keeping vascular pedicle in full view to prevent injury to nutrient supply

• Tunnel is created for the passage of PM flap in to the neck
• Adequate underming is required to prevent compression of vascular pedicle

• Flap has been transferred to the neck superficial to the clavicle , it is important to avoid twisting or placing excess tension to the pedicle in this manoeuvre

Donor site closure should be done by wide undermining of chest wall skin

LATISSIMUS DORSI FLAP• Large and triangular muscle• ORGIN : sacrum, lumbar
vertebrae, thoracolumbar fascia, posterior iliac crest , lower six thoracic vertebrae
• INSERTION: intertubercular groove of humerus
• Forms posterior wall of axilla

Blood supply:• Major vascular supply-
thoracodorsal vessels• It enters latissimus dorsi 10cm
from its humeral insertion• Within LD muscle ,
thoracodorsal vessels divide in to superior and lateral branches which allow muscle to split in to two.

• ADVANTAGES OF LD FLAP1. Large amounts of tissue
can be transferred 2. Pedicled or free tissue
transfer3. Cosmetic
advantage ,especially in females
4. Versatile: may be tubed/multiple/osseous components
5. When pedicled , it can reach upper face and scalp
• DISADVANTAGES OF LD FLAP
1. It is very bulky2. There is occasional
donor site dehiscence3. There is reduction in
upper limb power4. May require moving of
patient to harvest

STEPS OF HARVESTING LD FLAP
• Important landmarks – axilla , scapular tip, iliac crest
• Dotted line drawn from midpoint of axilla to midpoint b/w anterior and posteior iliac spine represent anterior border of LD
• 8 to 10 cm below the midpoint of axilla the thoracodorsal artery and vein enters the undersurface of LD muscle
• Divides into horizontal and vertical branch

Initial incision is made at mid point of axilla and runs along the dashed line superiorly and anterior edges of cutaneous paddle inferiorly

• Anteior border of LD retracted and branches of thoracodorsal artery supplying serratus anterior are exposed and these are used to find thoracodorsal vessels.
• Division of serratus anterior branches allow near complete mobilization of thoracodorsal pedicle.

• An incision is made circumferentially along postero-medial portion of skin paddle .
• This incision is made to the level of fascia overlying muscle

• Elevation of back skin off the muscle provides exposure of LD to posterior midline.

• LD is mobilised by blunt and sharp dissection off the chest wall ,external oblique , serratus anterior muscle
• The muscle and aponeurotic attachment to iliac crest , vertebrae and ribs are sharply transected

As the dissection proceeds distally to proximally , the vascular hilum identified , careful dissection along the thoracodorsal vascular pedicle requires division of muscular and angular branches.

• Passage of pedicled flap requires preparation of tunnel b/w pectoralis major and minor
• The lateral edge of these muscles are identified in anterior axilla

• An incision parallel and inferior to clavicle is required to complete the tunnel . The pectoralis major muscle attachments to the clavicle are incised
• A good tunnel must accomdate atleast four of surgeon’s fingers.

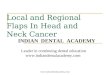
Under vision ,LD should be passed through the tunnel while being certain not to twist the pedicle or to cause shearing forces between skin and the muscle.

Latissimus dorsi has been to transferred to temporal region without tension on vascular leash

PLATYSMA FLAP
An island myocutaneous flap based on the platysma muscle is ideal for reconstructing the superficial lining defects of oral cavity
DISADVANTAGES OF PLATYSMA FLAP:1) Blood supply can be unreliable.2) Prior neck dissection or any neck surgeries precludes
the use of this flap3) A proper neck dissection may damage the blood supply
to the flap4) Removal of the platysma interferes with the blood
supply to the overlying skin and can lead to necrosis of skin.
5) Platysma flap is not advisable in patients with prior irradiation to neck.

STERNOMASTOID FLAP
Advantages The skin paddle of superiorly based sternomastoid
flap is hairless and thin and is an ideal reconstructive option for medium sized cheek defects.
It does not produce excessive bulk in the face or mouth
Disadvantages A proper neck dissection is likely to cause damage to
the vascular pedicle. Hence a previous neck surgery or concurrent lymphadenectomy preclude the use of this flap

Thank you
Recommended