Dave McClure, Ellen Paddock, Rayanne Hawkins, and Mayookha Mitra-Majumdar URBAN INSTITUTE
with contributions from
Andre Bethea Gillian Caplan Carl Filler BUREAU OF JUSTICE ASSISTANCE JOHNS HOPKINS UNIVERSITY ST. LOUIS MAYOR’S OFFICE
Kate Lawson Mark Munetz Mike Prado PIMA COUNTY ATTORNEY’S OFFICE OHIO CRIMINAL JUSTICE
COORDINATING CENTER FOR EXCELLENCE
INTERNATIONAL ASSOCIATION OF CHIEFS OF POLICE (VISITING LAW ENFORCEMENT FELLOW)
Mark Slater Amy Watson Jason Winsky BALTIMORE BEHAVIORAL HEALTH SYSTEMS
UNIVERSITY OF ILLINOIS AT CHICAGO
TUSCON POLICE DEPARTMENT
November 2017
Policymakers and community stakeholders across the US are increasingly recognizing
the crisis intervention team (CIT) model as a valuable approach for improving law
enforcement’s interactions with people with mental health issues. Though costs of initial
training and partnerships are low, successfully integrating CIT into a jurisdiction’s day-
to-day activities requires investment from health systems and law enforcement that can
be expensive. Pay for success (PFS) has strong potential for funding these critical CIT
enhancements; however, both CIT and PFS require culture shifts and strong
partnerships to be sustained.
This brief is intended to help stakeholders determine whether and how their jurisdiction might
create or expand its CIT program, and to guide their assessment of how PFS might support those efforts.
J U S T I C E P O L I C Y C E N T E R
Pay for Success and the Crisis Intervention Team Model Insights from the PFS-CIT Learning Community

2 P A Y F O R S U C C E S S A N D T H E C R I S I S I N T E R V E N T I O N T E A M M O D E L
To do this, this brief begins with primers on PFS and CIT. The next section describes overlap between
starting a new CIT program and starting a PFS project. Then, the brief describes ways PFS could be used
to support expansion of a jurisdiction’s CIT program in a manner that suits the jurisdiction’s specific
needs. The final section provides a framework and considerations for determining whether PFS is the
right approach for funding the jurisdiction’s expansion of its CIT program.
The insights contained in this brief are based on CIT and PFS reference materials, as well as the
experiences and expertise of a multidisciplinary stakeholder learning community convened over three
months in summer 2017. The learning community members shared their perspectives, experiences, and
understanding on specific issue areas through an in-person meeting and virtual workgroup meeting,
email discussions, and several working group conference calls. These stakeholders were so invaluable in
developing the content contained in this brief that they have been included as authors, rather than in
the acknowledgments.
Primer on PFS: What Is Pay for Success?
Ordinarily, government-funded services are provided through activity- and output-focused programs or
single agency contracts with an outside organization. Though this approach enables governments to
offer services, it rarely assesses whether the sponsored activities achieve the intended results or
outcomes. Moreover, payment is based on delivering predefined services or outputs (e.g., number of
formerly incarcerated people receiving education and workforce development services) rather than
outcomes (e.g., reduced rates of recidivism among people receiving that training).
Pay for success, sometimes referred to as social impact bonds, is an innovative financing mechanism
for evidence-based interventions that changes the ordinary government-funded services model. PFS
shifts the focus to results, using data and evaluation to determine whether a program is successful and
will be paid for by government. Thus, the risk of paying for programs that might not work is also shifted
away from the government.
In a pay-for-success project, an investor, typically a private investor or philanthropic
organization, commits up-front capital for a proven social intervention with the potential to
achieve better outcomes. If the service provider delivering that intervention achieves
predetermined outcomes for the target population, as assessed by an independent evaluator,
the government repays the investor with interest. If that intervention does not successfully
achieve the predetermined outcomes, the government does not pay for the services delivered.
The finances of the project are often managed by an intermediary, an organization that
specializes in structuring and managing PFS projects.1
As described above, PFS projects involve active collaboration and management among
stakeholders focused on achieving measurable social outcomes. This shift toward outcomes invites new
stakeholders to the table (investors and intermediaries) and refocuses the roles of current players, such
as service providers and the government, on the quality of services provided and their ability to be
measured in real time by the evaluator.

P A Y F O R S U C C E S S A N D T H E C R I S I S I N T E R V E N T I O N T E A M M O D E L 3
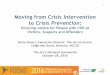
FIGURE 1
Roles and Relationships in a PFS Deal
Typically, a PFS project involves several key roles:
Intermediary: Organization that coordinates among partners to assess feasibility, structure the
transaction, and manage payments
Investor: Philanthropy or private firm that provides up-front capital
Government: Agency or agencies that will pay if the program is successful (sometimes referred
to as the “end payer”)
Service provider: Organization that provides direct services to the target population
Evaluator: Independent organization that determines if the program met its goals
In the PFS model, the process of delivering government-funded services is driven by whether the
outcome is achieved, rather than whether a service provider or government program simply performed
the activities it was funded to perform. As a result, the most crucial element of a PFS project is the social
outcome the funded project is meant to achieve.
The critical social outcome for a PFS project is a specific desired change or result, around which
every aspect revolves. Typically, this result is an improvement in outcomes related to an issue or
condition affecting the target population. This result is what the government is trying to achieve with
the funding resources they have allocated to the issue. The service provider is trying to produce this
result, and the investors are betting that they will be able to achieve this result. Ultimately, the
evaluator is measuring how successfully they achieved this result. The outcome is the lynchpin of the
entire PFS project. For the project to work, all the relevant project components must appropriately fit
together.

4 P A Y F O R S U C C E S S A N D T H E C R I S I S I N T E R V E N T I O N T E A M M O D E L
Structure of PFS
Not all projects are suitable for PFS financing. For instance, in programs without prior evaluations, the
ability of the program to achieve the desired outcome may be too uncertain for investors to take the
risk or evaluating whether the outcome was achieved could take too long. Several factors help to
determine whether PFS is an appropriate funding mechanism, as summarized in table 1.
TABLE 1
When Is PFS Appropriate?
Appropriate for PFS Not appropriate for PFS
Clearly defined problem Poorly defined or unmeasurable problem
Evidenced-based and/or promising interventions Untested programs or core services (e.g., ambulances, emergency shelters) provided regardless of outcomes
Strong and effective provider capacity Insufficient provider capacity
Committed support from relevant government agencies
Weak government support
Strong data capacity Limited or poor-quality data capacity
Willingness and ability to participate in a rigorous evaluation
Unwillingness or inability to participate in an evaluation
Note: This table presents only some of the highest-level criteria for a PFS deal to occur. Urban’s Project Assessment Tool provides
a much more in-depth and concrete scoring guide for jurisdictions seeking to assess the suitability of potential PFS deals (Milner
et al. 2016).
PFS transactions are executed in four phases. During the initial feasibility phase, intermediaries
coordinate with other stakeholders to assess whether a project is suitable for PFS based on program
strength, local capacity, and other factors. If deemed feasible, projects proceed to transaction
structuring, in which PFS partners develop the PFS contract and agree upon which outcomes will
determine payment. Only after a contract is signed does the project launch and enter implementation,
in which the service provider begins delivering program services and all stakeholders engage in active
project management. Finally, though evaluation considerations are built in throughout the project, in
the evaluation phase, evaluators determine if the program hit outcomes targets, and investors are
repaid by government.
Examples of PFS in the United States
Between 2012 and 2017, 17 PFS projects were fully launched in the United States2 and nearly 60
feasibility studies were funded by the Corporation for National and Community Service’s Social
Innovation Fund.3 Though Urban researchers could not identify any examples of PFS being applied to

P A Y F O R S U C C E S S A N D T H E C R I S I S I N T E R V E N T I O N T E A M M O D E L 5
CIT programs to date, many PFS projects have focused on outcomes similarly related to recidivism and
behavioral health. More information about how PFS can be applied in a criminal justice context may be
found in Urban’s forthcoming “Using Pay for Success to Address Criminal Justice Issues” brief.
To help illustrate how PFS works, the following tables describe two real PFS projects and key
lessons learned for the field.
TABLE 2
Case Study 1: Santa Clara Project Welcome Home
Location: Santa Clara, CA
Size of investment: $6.9 million (maximum success payments possible: $8 million)
Partners:
Intermediary: None (Third Sector as transaction coordinator, government advisor)
Service Provider: Abode Services
Outcome Payer: Santa Clara County
Investors: Reinvestment Fund, Corporation for Supportive Housing, Sobrato Family Foundation, the California Endowment, Health Trust, the James Irvine Foundation, Google.org, Laura and John Arnold Foundation (evaluation), Abode Services (service fees)
Technology Partner: Palantir Technologies
Evaluator: University of California San Francisco School of Medicine
Payment Outcome: Number of months in continuous stable housing
Status: Implementation (ongoing)
This project provides permanent supportive housing to 150–200 individuals experiencing chronic homelessness defined as high-cost users of county services. A strong evidence base suggests that permanent supportive housing can increase housing tenure and reduce homelessness, emergency room visits, and hospitalizations.a
Project Welcome Home officially launched on July 1, 2015, with the goal of helping over 80 percent of participants achieve 12 months of continuous stable tenancy.b Over the six-year service delivery period, the University of California San Francisco School of Medicine will evaluate payment outcomes using a randomized controlled trial and “intent to treat” analysis. The evaluation will also track other outcomes of interest (e.g., use of county services), but these will not determine payments. In December 2016, the county’s primary PFS legal advisor reported that the project was so far achieving its outcomes.c
Key Lessons: Project Welcome Home built data capacity and partnerships that enabled the county to enter a new PFS project providing assertive community treatment to adults with severe mental health conditions and frequent emergency room usage.d
Source: “Project Welcome Home,” PFS project fact sheet, Urban Institute, http://pfs.urban.org/pfs-project-fact-
sheets/content/project-welcome-home. a Debra J. Rog, Tina Marshall, Richard H. Dougherty, Preethy George, Allen S. Daniels, Sushmita Shoma Ghose, and Miriam E.
Delphin-Rittmon, “Permanent Supportive Housing: Assessing the Evidence,” Psychiatric Services 65, no. 3 (2014): 287–94. b Third Sector Capital Partners, “Project Welcome Home Fact Sheet,” 2015, http://www.thirdsectorcap.org/wp-
content/uploads/2015/08/150811_SCC-CH-PFS_Fact-Sheet.pdf. c Greta Hansen, “Getting More Than You Pay For with Pay-For-Success,” Stanford Social Innovation Review, December 1, 2016,
https://ssir.org/articles/entry/getting_more_than_you_pay_for_with_pay-for-success. d Hansen, “Getting More Than You Pay For”; “Santa Clara County Partners in Wellness,” Nonprofit Finance Fund, last updated
May 31, 2017, http://www.payforsuccess.org/project/santa-clara-county-partners-wellness.

6 P A Y F O R S U C C E S S A N D T H E C R I S I S I N T E R V E N T I O N T E A M M O D E L
TABLE 3
Case Study 2: The NYC ABLE Project for Incarcerated Youth
Location: New York, NY
Size of investment: $9.6 million (maximum success payments possible: $11.7 million)
Partners:
Intermediary: MDRC Service Provider: Osborne Association,
Friends of Island Academy Outcome Payer: NYC Department of
Corrections Investors: Goldman Sachs Urban Investment
Group, Bloomberg Philanthropies Evaluator: The Vera Institute of Justice
Payment Outcome: Recidivism, based on days avoided
Status: Terminated, outcomes not achieved
In February 2013, the NYC Adolescent Behavioral Learning Experience (ABLE) project became the first PFS deal to launch in the United States. Using a cognitive behavioral therapy called moral reconation therapy, ABLE sought to reduce recidivism among 16- to 18-year-old youth incarcerated in NYC’s Rikers Island jail. Earlier studies provided moderate evidence of the effectiveness of moral reconation therapy in reducing recidivism,a and stronger evidence for cognitive behavioral therapy generally.b
Using a quasi-experimental design, the Vera Institute evaluated whether participation in ABLE was associated with reduced recidivism in bed days, with success payments contingent upon a 10 percent reduction. However, the project was halted one year early for failing to meet this benchmark.c
Key Lessons: Suggested reasons for the ABLE project’s results include high turnover that made fidelity to program implementation more challenging;d lack of prior evaluation of moral reconation therapy with the target population and within a correctional setting; and the service provider’s lack of experience with this intervention.e However, the project succeeded in applying the PFS model and promoting an outcomes-based culture.f
Source: “The NYC ABLE Project for Incarcerated Youth,” PFS project fact sheet, Urban Institute, http://pfs.urban.org/pfs-project-
fact-sheets/content/nyc-able-project-incarcerated-youth. a Gregory L. Little, “Meta-Analysis of Moral Reconation Therapy Recidivism Results from Probation and Parole Implementations,”
Cognitive-Behavioral Treatment Review 14, no. 1/2 (2005): 14–16. b Mark W. Lipsey, Nana A. Landenberger, and Sandra J. Wilson, “Effects of Cognitive-Behavioral Programs for Criminal
Offenders,” Campbell Systematic Reviews 6, no. 1 (2007): 27. c Vera Institute of Justice, Impact Evaluation of the Adolescent Behavioral Learning Experience (ABLE) Program at Rikers Island:
Summary of Findings (New York: Vera Institute of Justice, 2015). d Megan Golden and Joe Waters, “What Does NYC Mean for the Pay for Success Field?” Institute for Child Success, July 8, 2015,
https://www.instituteforchildsuccess.org/what-does-nyc-mean-for-the-pay-for-success-field/. e “The NYC ABLE Project for Incarcerated Youth,” Urban Institute. f Justin Milner, Erika C. Poethig, John Roman, and Kelly Walsh, “Putting Evidence First: Learning from the Rikers Island Social
Impact Bond,” Urban Wire, Urban Institute, July 5, 2015, https://www.urban.org/urban-wire/putting-evidence-first-learning-
rikers-island-social-impact-bond; James Anderson and Andrea Phillips, “What We Learned From the Nation’s First Social Impact
Bond,” The Huffington Post, July 2, 2015/6, http://www.huffingtonpost.com/james-anderson/what-we-learned-from-the-
_1_b_7710272.html.

P A Y F O R S U C C E S S A N D T H E C R I S I S I N T E R V E N T I O N T E A M M O D E L 7
Advantages of PFS over Traditional Funding Approaches
Lessons learned from PFS projects implemented to date suggest PFS has impacts that go beyond the
project itself and may contribute to a larger shift in culture toward prioritizing evidence, outcomes,
collaborative and active performance management, and the strategic deployment of resources.
Emphasizing performance based on outcomes, rather than activities, provides agencies and service
providers with greater flexibility. Because their performance is no longer assessed based on adherence
to predefined activities or outputs, they have more flexibility to take actions they deem necessary and
appropriate to achieve the desired outcomes. At the same time, PFS establishes structures, such as
integrated data systems, that can make services more data-driven and streamlined in the future. PFS
can also address “wrong pockets” problems where government agencies may be unwilling to invest in
projects whose benefits will be reaped all or partially by other agencies.
Finally, because the PFS model requires rigorous evaluation to determine whether the funded
intervention has led to the desired outcome, PFS projects can also contribute to the larger evidence
base on when and how interventions are successful.
BOX 1
Common Questions about Pay for Success When you talk about government, what does that mean (city, county, state)?
Government payers vary by intervention and context. It is also important to distinguish between the level of the end payer and the scope of program implementation. For example, the end payer may be a state because that is where the project may produce cost savings, yet the actual project could be implemented at the county level within a few counties. State, county, and city governments have all served as end payers in PFS projects to date, but there have also been projects with federal payers (e.g., the Department of Labor).
Who establishes the performance and/or outcome metrics for PFS?
Partners collaborate to define the metrics, but typically the government end payer(s) and agencies that own the data have particularly strong influence. Moreover, the following are key considerations: the data available, the quality of the data, and the outcomes of interest to the paying agency.
Who sets the interest rate in a PFS deal?
All players involved negotiate this as part of the contract development process. Some reports show that interest rates have typically been fairly low or less than market averages.a One benefit of PFS deals is that they (and the interest rates) are less vulnerable to market forces than other investments because they are fully agreed upon in advance.
What role does the investor play in shaping how the program will be developed?
The investor’s role varies by project. For example, in a Cuyahoga County project, foundation investors were involved early on and had more input on developing the project.b In other deals, investors have less or later involvement. Typically, governments play the larger role in defining the outcomes.
a For example, the Improving Elementary School Student Performance in Utah had a 5 percent interest rate (Monitor Deloitte, The
Many Ways to Pay for Results: Funding Options for Innovation and Success [New York: Deloitte, 2015]). b See Enterprise Community Partners and Third Sector Capital Partners, Developing the Cuyahoga Partnering for Family Success
Program: Partner Perspectives and Lessons Learned (Boston: Third Sector Capital Partners, 2016).

8 P A Y F O R S U C C E S S A N D T H E C R I S I S I N T E R V E N T I O N T E A M M O D E L
Additional Resources
Several resources are available to learn more about pay for success:
The Urban Institute’s Pay for Success Initiative has developed a suite of resources at
pfs.urban.org to support a wide range of stakeholders interested in PFS.
The Brookings Institution has published a comprehensive report on social impact bonds
worldwide (Emily Gustafsson-Wright, Sophie Gardiner, and Vidya Putcha, The Potential and
Limitations of Impact Bonds: Lessons from the First Five Years of Experience Worldwide [Washington,
DC: Brookings Institution Press, 2015]).
The Nonprofit Finance Fund, a PFS funder and intermediary, has developed a website
(www.payforsuccess.org) with resources on PFS. NFF’s First Generation Report, which
provides detailed information on the first 10 PFS projects, has been a key resource for the field
(Dana Archer-Rosenthal, Pay for Success: The First Generation [New York: Nonprofit Finance
Fund, 2016]).
Primer on CIT: What Is the Crisis Intervention Team Model?
Sworn to protect and serve, law enforcement officers are often first responders to challenging
situations that do not necessarily involve criminal activity. Some of the more challenging interactions
officers can face involve people in mental health, behavioral, or emotional crisis. Without the
information or training to recognize the mental or emotional issues that may be at play, such
interactions have demonstrated potential to escalate dangerously, resulting in use of force, officer
injuries, or even fatalities (Fuller et al. 2015). In many cases, officers might repeatedly encounter the
same person.
The Crisis Intervention Team (CIT) model was designed to break that cycle by training first responders
how to diffuse volatile crisis situations and connect people with services. Originally developed in Memphis
in the late 1980s, the CIT model partners law enforcement, behavioral health providers, hospitals, families,
people with mental health conditions, and other key stakeholders to respond appropriately in situations
involving apparent mental or emotional distress. Core components of a CIT program include training for
key local stakeholders (including law enforcement and other first responders, hospitals, and treatment
providers) and coordination with other health and crisis response systems.
CIT in Practice
Traditionally, law enforcement is alerted to a potential crisis situation through a call for service. The call
goes to dispatch, which sends an officer to assess the scene and determine next steps. For most
resource-constrained law enforcement agencies, the goal is then to uphold the law while resolving the

P A Y F O R S U C C E S S A N D T H E C R I S I S I N T E R V E N T I O N T E A M M O D E L 9
situation in the safest and fastest manner possible, enabling officers to quickly return to the street.
Historically, the typical way to resolve such a situation would be a nonresponse, informal response, or
arrest. If fully implemented and operating as intended, CIT provides alternative response options that
minimize inappropriate arrests and increase connection to services.
The CIT model requires several core components for these alternative response options to be viable:
CIT coordinator(s) and coordinating body to drive CIT efforts forward and ensure continued
coordination between law enforcement and behavioral health professionals.
Training for law enforcement, other first responders, and health services partners. For law
enforcement, this includes the intensive 40-hour standard CIT curriculum, as well as potential
enhancements such as basic mental health awareness training for all officers and/or ongoing
training refreshers.
Coordination with health service providers, including drop-off locations where officers can
bring people to receive assistance when the situation requires. Optimally, this may be a crisis
triage center that specializes in linking people to appropriate services. However, existing
practice has often been to use emergency rooms. Other aspects of this coordination may
include information sharing and referrals.
Partnership with core stakeholders, including
» Law enforcement, including leadership, dispatch, CIT officers, and regular patrol officers
» Other first responders, such as the fire department or emergency medical services (EMS),
who may also encounter crisis situations
» Health services providers, including behavioral health clinicians and case workers, to help
coordinate response options and treat the person experiencing distress
» Families of people with mental or behavioral disorders, who may seek the help of CIT
professionals and have an important perspective for shaping response options
» People living with mental health conditions and/or directly exposed to CIT, who may provide
valuable insights about how CIT is experienced and may be involved in training in some
cases
In addition to these core components, some jurisdictions have implemented further program
enhancements such as information sharing tools or applications,4 hiring full-time clinicians into the law
enforcement agency, conducting more preventive outreach with vulnerable individuals, and using
secure communication apps or a “warm line” (as opposed to a hotline)5 to contact clinicians in the field.
Learning-community participants also emphasized the importance of culture change in law
enforcement to actively recognize and search for signs of behavioral health issues in calls for service
and to value and use CIT and alternatives to arrest.

1 0 P A Y F O R S U C C E S S A N D T H E C R I S I S I N T E R V E N T I O N T E A M M O D E L
Evidence for CIT
In a 2008 literature review, Compton and colleagues found 12 empirical reports examining officer-level
outcomes of CIT programs; in 2017, this number has doubled to roughly 24 pre-post and quasi-
experimental studies. Of these, a majority have examined CIT’s effects on officer attitudes and
knowledge,6 and a smaller body of research has examined more direct impacts on behavior in the form
of transportation to treatment,7 rates of arrest,8 use of force,9 longer-term engagement with
treatment,10 and cost savings.11 Generally, these studies have shown that CIT officers have greater
knowledge of mental health conditions,12 improved confidence in their ability to respond, improved
confidence in the perceived effectiveness of CIT,13 reduced stigmatization of mental health
conditions,14 and more positive attitudes toward treatment and health systems.15 These critical outputs
show that CIT training has been received as intended. Findings on arrests and transportation to
treatment are similarly positive, with multiple studies suggesting that CIT reduces rates of
inappropriate or unnecessary arrest of people with mental health conditions16 and increases connection
to treatment.17 Only one cost-benefit analysis has been conducted to date, finding evidence of modest
cost savings from a reduction in the average length of stay after arrest.18
Though these results are promising, several methodological issues suggest the need to further
strengthen this evidence base. Researchers have struggled with devising a feasible approach to more
rigorously test CIT using the commonly recognized “gold standard” randomized controlled trial (Watson
2010), which presents significant ethical issues in this setting (i.e., randomly assigning how officers
respond to a crisis situation). Few studies have used rigorous comparison methods to assess the effects
of CIT training relative to a matched sample of non-CIT-trained officers. Furthermore, evaluations of
CIT have focused almost exclusively on police officer training, with little empirical examination of the
larger model or of the impact of other elements (e.g., reliable drop-off locations) on effectiveness. The
question of program fidelity has also been largely absent from CIT research, despite findings that
sustained adherence to the model faces several implementation challenges (Addy 2005; Compton et al.
2010; Dupont and Cochran 2000). According to learning-community participants, part of the challenge
in assessing fidelity is the lack of clarity about what fidelity means and/or the lack of a concrete tool with
which to assess it. Nevertheless, the current consensus is that CIT is a “promising practice,” which
means it does not yet rise to the level of evidence-based but could reach this status with further, more
rigorous research (Thompson and Borum 2006; Watson and Fulambarker 2012).

P A Y F O R S U C C E S S A N D T H E C R I S I S I N T E R V E N T I O N T E A M M O D E L 1 1
BOX 2
Common Myths about CIT
CIT is a police intervention. Though officers are often the first responders, partnership and coordination with health services is integral to the CIT model and essential for success.
CIT is just training. CIT requires sustained partnership across agencies and should be embedded in law enforcement and health operations to be successful. Training without drop-off locations or clinician support leaves officers without the tools to successfully resolve situations.
CIT is expensive. Law enforcement agencies often think they can’t afford CIT at all. However, the national curriculum is freely available for local adoption; thus, the main costs of starting a CIT program are time or in-kind contributions (e.g., printing materials) for training and coordination meetings. Higher costs come through enhancements such as crisis triage centers.
CIT is only for crisis situations. CIT officers are trained to be mental health specialists in the department and are best equipped to respond to any calls involving a person showing symptoms of mental health conditions, even if they are not currently in crisis. Bringing in a CIT officer who knows how to handle the situation appropriately can also prevent a situation from escalating to a crisis.
“Crisis” always means mental illness. Very often, mental health and substance use disorders are co-occurring. CIT trains officers to recognize a potential behavioral health crisis, but not to diagnose. Asking officers to distinguish why someone is in crisis—because of a mental health conditions, drugs or alcohol, or another cause—is impractical and may invite biased decision-making. The skills taught in CIT, including de-escalation, apply to a variety of crisis situations.
Arrest is always the wrong answer. The ultimate goal of CIT is to ensure the safety of people in crisis, people around them, the responding officer, and the public. Though CIT generally promotes responses other than arrest, there may be some instances where arrest becomes necessary to ensure public safety.
Departments should always aim to train 20 percent of officers in CIT. Based on recommendations from the original Memphis CIT developers (Dupont, Cochran, Pillsbury 2007; Watson and Fulambarker 2012), customary practice among law enforcement agencies is to seek to train 20 percent of patrol officers in CIT.a However, there is little evidence to support this threshold for all agencies in all cases (Watson and Fulambarker 2012); instead, learning-community participants said that it is essential to ensure that all shifts and patrol districts have at least one CIT-trained officer available.
CIT training should be mandatory for law enforcement officers. Though some departments have made CIT mandatory, learning-community participants emphasized that this approach can be detrimental. Mandating CIT can undercut officer buy-in and place officers who are neither interested nor appropriate to become CIT officers in the position of responding to sensitive crisis situations. Instead, learning-community members suggested emphasizing the value of CIT to officers as a tool to protect officer safety and liability and employing credible messengers (i.e., well-respected and experienced officers) to deliver this message.
Sources: Myths derived from learning-community discussions and supplemented with external resources where pertinent. a See examples in Spokane, New York City, Georgia and New Orleans

1 2 P A Y F O R S U C C E S S A N D T H E C R I S I S I N T E R V E N T I O N T E A M M O D E L
Starting a New CIT Program: Parallels with PFS
Both CIT and PFS have their own explicit goals: CIT seeks to improve the way law enforcement
responds in situations involving mental health, and PFS pays for programs based on the outcomes they
achieve. A subtle but significant part of both models is that for their goals to be achieved, organizations
must change their culture so that the norms and processes contribute to the overall goal.
For PFS, an integral part of the process is shifting a jurisdiction’s culture to focus on delivering
government services that improve the outcomes of the population being served. After all, achieving the
predefined outcome is the linchpin of a PFS project. Similarly, CIT requires shifts in thinking (e.g., for
officers to consistently think of mental health referral as an option, or for dispatchers to consistently
think to call CIT officers) that will improve the outcomes of people with mental and behavioral health
issues who interact with law enforcement. Though this type of culture change can often be a byproduct
of meaningful reform, thinking of it as a discrete goal from the beginning can help to sustain efforts.
However, culture change is also challenging and requires true buy-in from partners, rather than a desire
to “check the box” or only minimally invest in solving a problem.
As an example, a common misperception about CIT is that a police department could create a
program by simply mandating all officers take 40 hours of CIT training from a certified trainer. Learning-
community participants described this as counterproductive in several ways. First, mandating CIT can
create resentment toward the program that undermines culture change. Second, this forces officers
who may be unwilling and not open to CIT to take the training, which would yield suboptimal results.
Furthermore, the process of training itself is not sufficient to improve outcomes; CIT requires a
partnership with health response systems. Where would officers take people who have been identified
as having mental health needs and have been safely taken into custody? When implemented correctly,
CIT is well integrated across law enforcement and health response systems with input and coordination
from other key stakeholders, such as people with mental health conditions and their families.
Ultimately, voluntary training is a necessary but insufficient component of building a CIT program;
however, a common and necessary first step for both CIT and PFS toward culture change is
coordination across agencies and other stakeholder organizations.
Coordination across Agencies and Stakeholder Organizations
CIT requires active coordination across law enforcement, behavioral health agencies, and other
community partners. Multiagency coordination is also a central component of a PFS deal. Learning-
community participants agreed that the first step in launching a CIT program is to get key partners
together to define the problem, reach consensus on what is needed, and start to build key partnerships.
Specifically, there must be strong buy-in and involvement from leadership of agencies whose
investment is most central to the model (i.e., law enforcement and behavioral health). To illustrate this
point, participants offered several examples of how partnership helped drive CIT in jurisdictions they
were familiar with:

P A Y F O R S U C C E S S A N D T H E C R I S I S I N T E R V E N T I O N T E A M M O D E L 1 3
Baltimore, Maryland: Police leadership was critical in bringing other city stakeholders on board
because they are respected and taken more seriously by other first responders such as Fire and
EMS. Community input to the CIT partnership was added later but has been critical; in
retrospect, participants said they would have added community input earlier.
Chicago, Illinois: CIT was initially driven by a group called the Criminal Justice Task Force that
was organized by the area mental health director. This committee had been laying the
groundwork and advocating for training for years, but it wasn’t until a critical incident (officer-
involved shooting with a mental health component) that the mayor agreed and began moving
CIT forward. Subsequent pressure from the Kennedy Forum and the Department of Justice
investigation has helped continue to move things forward.
Pima County, Arizona (program redesign, not original launch): The first step in revamping CIT was
putting together a “coalition of the willing,” including high-level agency leaders willing to put
their support behind growing the program. Though there were advocates outside of law
enforcement pushing to move forward, progress was made only when the police department
leadership bought into the concept.
Summit County, Ohio: The county mental health authority learned about CIT during an annual
conference. The Ohio Department of Mental Health approached the director of training for the
Akron Police Department about visiting a model CIT jurisdiction to observe the program with a
mental health clinician, followed by a walkthrough of the CIT training. The two returned from
the visit believing in the program, and the training director got buy-in from the chief of police.
The mental health authority served as the lead in organizing the training and program
development, which over the subsequent years involved all law enforcement jurisdictions in the
county.
STAKEHOLDERS
Law enforcement agencies. CIT is often misconstrued as solely a law enforcement initiative. This is
misleading and fails to account for the role that health systems and other stakeholders must play, but
law enforcement agencies are inarguably central to CIT. As the primary first responders to people in
mental health crisis and the focus of CIT training, law enforcement agencies must be essential partners
for CIT to be viable. Often, law enforcement leadership takes the lead in driving CIT forward; though
this is not always necessary, clear demonstration of commitment from law enforcement leadership is
essential for effecting culture change at all levels of the law enforcement agency.
Though departments often focus on training specialized CIT officers, employees across a variety of
roles in the agency have the potential to contribute to or hinder the goals of CIT.
Agency leadership plays a critical role in setting the vision for the agency, investing resources
in CIT, and strengthening partnerships.
Dispatchers are often the first to receive calls and thus should be able to recognize a potential
CIT-related situation and determine which CIT-trained officers to send.

1 4 P A Y F O R S U C C E S S A N D T H E C R I S I S I N T E R V E N T I O N T E A M M O D E L
Patrol officers may be the first to encounter a person in crisis and should have enough baseline
knowledge to recognize the need to call a CIT officer.
Line-level supervisors (i.e., lieutenants and sergeants) are particularly influential and should
understand what CIT means for their role—for example, allowing officers to take time to
resolve a situation when needed, rather than pressuring or criticizing them for taking time in a
way that counteracts the message of CIT.
Nearby agencies may also need to become collaborators for some jurisdictions to develop a
successful CIT program. For example, county-level programs are unlikely to be very successful
if constituent municipal agencies are not trained.
Behavioral health agencies. Even if officers receive excellent training and an agency is fully on board with
CIT, the model risks failure without necessary health services and support. Optimally, this includes a
dedicated drop-off location such as a crisis triage center, where police can drop off an individual in crisis
to receive immediate assistance and linkage to further care. Crisis triage centers are interdisciplinary
crisis response centers staffed by nurses, behavioral health clinicians, and social service providers. In
the context of CIT, the goal of these centers is often speed—a location where officers can quickly drop
someone off after diffusing a situation and then return to the street. Ideally, staff at the crisis triage
center then help to connect a person with longer-term services that can help address any underlying
problems and prevent future problematic encounters.
However, challenges can emerge when health services are insufficient or not easily accessible. In
jurisdictions where crisis centers do not exist, law enforcement agencies may rely on emergency
departments as drop-off locations, which presents significant problems for hospitals attempting to
quickly triage and treat high volumes of life-threatening health issues. Having strong partnerships with
stakeholders in local health systems can help manage expectations and mitigate challenges even when
resources are not available for more dedicated drop-off options.
CATALYSTS FOR COORDINATION
Achieving coordination across agencies can be difficult, but several factors can catalyze or renew
support for CIT across agencies. This includes critical incidents such as publicized use of force, as well as
more diffuse motivators. For example, learning-community participants highlighted that the current
climate surrounding police-community relations, enhanced by media attention,19 has increased the
appeal of CIT for many departments. Others recalled departments taking interest in implementing CIT
after nearby agencies had done so. However, these types of catalysts are external to any deliberate
government actions to crystalize multiagency support. For both PFS and CIT, developing and sustaining
multiagency support for efforts that will change the jurisdiction’s culture is the role of a coordinator or
policy champion.
CRYSTALLIZING COORDINATION: ROLE OF A COORDINATOR AND CHAMPION
As CIT programs develop, partnerships benefit from formalizing into a collaborative oversight body
that continues to meet, monitor, and drive implementation and identify any implementation issues.

P A Y F O R S U C C E S S A N D T H E C R I S I S I N T E R V E N T I O N T E A M M O D E L 1 5
Having a CIT “champion” and/or CIT coordinator (who may or may not be the same person) is central to
maintaining the commitment and consistent communication of this group. This role is comparable to
that of the intermediary in PFS—a central figure or body whose role is to drive efforts forward.
Learning-community members suggested that where possible, programs should have dual CIT
coordinators from both law enforcement and behavioral health agencies. These coordinators would
have a better understanding of how CIT works in their respective contexts and can communicate this in
ways that others in their field understand. Additionally, having a champion outside the law enforcement
agency (in addition to one inside) can help insulate efforts from turnover in police leadership.
INFORMATION EXCHANGE AND DATA INTEGRATION
Coordinating effectively across multiple agencies and stakeholder organizations requires sharing
information. However, information sharing can also help to institutionalize cross-agency perspectives
by placing agency-specific information within the larger context of the jurisdiction’s entire processes
and interactions on a given activity, issue, or person. For CIT, this can be an important way to refer
people to the most appropriate services, call on family members for assistance, or share information
among officers so that they are aware a person is living with a mental health condition. Data sharing is
required at every stage of PFS, from the initial process of identifying a program’s target population and
outcomes to the ongoing evaluation and performance monitoring that determine success payments.
Data sharing can take a variety of forms, from individual communication between people at an
agency, to fully integrated platforms that retrieve and combine datasets from various sources. Though
privacy and legal concerns can make the latter difficult, finding ways to reliably and regularly exchange
information in some form is essential.
These aspects of developing coordination create a critical and often informal foundation for a CIT
program. Training often represents the first formal step toward establishing these programs.
Training
Though coordination is a prerequisite for launching both CIT programs and PFS projects, CIT programs
also typically require specialized stakeholder training. CIT training is often the first concrete component
of the model to be implemented, and one of the most standardized pieces of the curriculum. Though
some law enforcement agencies may pay direct costs for external trainers to provide CIT, more often
the true costs of CIT training are the time and personnel required to modify the curriculum to local
context and bring officers off the street for training while ensuring continued coverage across patrol
districts. Departments may need to provide overtime pay for officers to either attend training or work
additional hours to cover others attending training. Learning-community participants noted that though
this arrangement and reliance on volunteer work is challenging, this way of providing training can be
more sustainable than applying for grants.
CIT training varies most when it comes to how departments train their employees. Some
jurisdictions opt to train the department, but others aim to sustain the principles of CIT by incorporating

1 6 P A Y F O R S U C C E S S A N D T H E C R I S I S I N T E R V E N T I O N T E A M M O D E L
it into academy training, Learning-community participants expressed caution about both
implementation strategies. First, making CIT voluntary and conveying its value to officers helps to
ensure that those who are willing and open to CIT self-select into the program, and those who are not
ready or do not want to change do not become bad CIT officers and “poison the well.” Similarly,
learning-community participants agreed that providing the full 40-hour CIT training in the academy is
ineffective at best and risky at worst. New officers lack the experience in which to ground CIT or fully
understand its implications. They are seeking to rapidly learn a variety of skills and may be more
immediately preoccupied with their own survival than more experienced officers. That said, basic
awareness training on mental health conditions and the circumstances that justify calling a CIT officer
can lay a foundation for continued changes in practice and culture.
Developing an Outcome-Oriented Perspective
A foundation of cross-agency coordination and collaboration is necessary to begin either PFS or CIT.
This perspective and capacity is a prerequisite for PFS to work, and jurisdictions have reported that just
preparing to support a PFS project was beneficial—whether or not the intervention was eventually
financed by PFS—because it provided outcome-oriented perspective and cross-agency coordination.
After training, the effects are similar for jurisdictions starting CIT.
CIT is far from a “plug and play” intervention. One jurisdiction could not simply copy a fully
developed CIT program from another jurisdiction. Developing a CIT program is an iterative process that
involves cultivating partnerships, providing training, setting up structures for ongoing coordination and
information sharing, putting in place key infrastructure such as crisis triage centers, and more. Each of
these steps takes time, and time itself is an important resource that allows necessary culture change to
occur. CIT is also very specific to the characteristics of each jurisdiction, which can affect how and why a
program develops. Some agencies may need to train more or different partners; others may need better
data integration systems, more proactive follow-up services, a tool for police and clinicians to
communicate, or other supports. Though there are unique considerations for each CIT component, this
layered nature provides multiple points at which PFS financing could help to build or enhance a CIT
program in a jurisdiction-specific manner.
Enhancing an Existing CIT Program with a PFS Project: Facilitating Jurisdiction-Specific Progress
CIT programs do not get up and running overnight. The process of developing a CIT program (and
related culture change) is different for every jurisdiction. However, once the seeds of change are
present for cross-agency collaboration and outcome-oriented thinking, PFS can provide a financing
option for taking the next step. to improve a CIT program’s ability to provide responsive, coordinated,
and comprehensive engagement with people expressing their mental health needs in a crisis.

P A Y F O R S U C C E S S A N D T H E C R I S I S I N T E R V E N T I O N T E A M M O D E L 1 7
One of the most consistent themes discussed by the learning community was that CIT is a
multilayered intervention that is built up over time. Though training and partnership are consistent
core components, there can be greater variation in how jurisdictions coordinate with health agencies
and further enhance programs. Learning-community members also noted that allowing sufficient time
to build CIT into local operations is essential for cultivating the culture change and partnerships
necessary for CIT to be successful.
Whether they stem from grant funding or another source, efforts to implement CIT are very closely
tied to the conditions and needs within the jurisdiction. A CIT program is developed slowly and
incrementally to allow the culture to change along with the jurisdiction’s new capacities that support
CIT. PFS should be considered a potential solution to fund those specific increments, whatever the
jurisdiction determines them to be.
This section provides some examples of common incremental CIT program enhancements
described by members of the learning community. This is certainly not a comprehensive list, nor are all
these incremental components appropriate for every jurisdiction. Rather, these examples are meant to
solidify the concept of how PFS could be used to support a jurisdiction’s efforts to incrementally expand
and enhance its CIT program.
It is important to note that some of the foundational components of CIT often come at little or no
budget cost. For example, trainings are often provided through volunteer trainers and in-kind
contributions that cover backfill time for officers attending CIT training and minimize costs for agencies.
At the same time, greater coordination across agencies can help realize savings for one agency based on
costless changes in another agency. For example, limited evidence suggests that CIT may lead to cost
savings in the form of deferred hospitalizations, reduced inpatient referrals from jail, and reduced jail
bed usage (El-Mallach, Kiran, and El-Mallach 2014).
In determining how PFS might make sense, it is important to first ask what the direct costs are—what
would “pay for success” actually pay for? Though specific CIT components vary, learning-community
participants identified three core “big ticket” costs associated with a well-functioning CIT program:
Formal CIT Coordinator(s): Having a funded coordinator whose primary responsibility is to
ensure that CIT efforts move forward can be critical to success. However, funding a full position
requires a substantial investment that may be challenging to provide, especially for smaller
jurisdictions or those with particularly limited resources.
Crisis Triage Center: Crisis triage centers are integral to CIT but represent a substantial
investment because they should operate 24 hours and require coverage from clinical staff. In
many cases, police that do not have access to a crisis triage center rely instead on emergency
departments, which further strains already stretched hospital capacity.
Enhancements: Learning-community members described a number of ways that CIT could be
further enhanced, including improved data integration infrastructure, greater involvement
and/or direct hiring of clinicians, and more proactive outreach to people who frequently

1 8 P A Y F O R S U C C E S S A N D T H E C R I S I S I N T E R V E N T I O N T E A M M O D E L
encounter CIT officers. Though not included in the core CIT model, these enhancements
represent investments that may help to increase success.
The payers of these costs vary. Learning-community participants cited CIT programs that received
funding from city police departments, mental health agencies, county governments, and foundations.
Each of these costs represents an opportunity where PFS could help to finance an enhancement to CIT,
though some may be more appropriate than others. Crisis triage centers may have operating costs that
are more definable but much harder for jurisdictions to pay up front. Program leaders must assess
whether alternative funding can be obtained and whether the costs are clearly definable. Training, for
example, may not be an appropriate avenue for PFS financing because many opportunity costs of
training are unpredictable (e.g., how much overtime a department must pay to ensure patrol coverage).
Further, departments have found other ways to fund training, whether through agency budgets or grant
funding, though this may not be the case in all jurisdictions.
A jurisdiction could many steps take to enhance its existing CIT program. The following examples
model how a jurisdiction might expand its program through a PFS project.
HYPOTHETICAL PFS-CIT PROJECT: CRISIS TRIAGE CENTER
Problem: One of the largest and most important investments in enhancing a CIT program is building a crisis triage center, where officers can transport a person who is in crisis or needs treatment and then quickly return to duty. However, crisis triage centers are often an underdeveloped component of CIT because of their up-front costs. Instead, CIT officers often bring people to local hospitals or emergency departments, which can strain these resources particularly in jurisdictions already lacking robust health care infrastructure.
Current Funding Sources: Learning-community participants said that crisis triage centers are often difficult to fund, though they cited examples of jurisdictions that did so. Illinois has been operating a state-funded crisis triage center and recently opened a new county-funded center. In Portland, a crisis triage center was funded through a collaboration of different health care and hospital systems and with philanthropic contributions. In some parts of Ohio, crisis triage centers are funded by local mental health providers. These examples suggest that there is momentum for governments to invest in crisis triage centers, even if the up-front costs are a deterrent in many places.
Program Strength: Bringing people in crisis to hospital emergency rooms is costly to hospitals (Alakeson, Pande, and Ludwig 2010) and can worsen symptoms and heighten distress for the person in crisis (Clarke et al 2000; Clarke, Dusome, and Hughes 2007). Early research has found that by providing a safer, more homelike environment and access to clinical staff (Action Alliance 2016), crisis triage or stabilization centers are effective at avoiding unnecessary hospitalizations (Action Alliance 2016; SAMHSA 2014) and may help to reduce hospital costs (Bengelsdorf 1993). Little research at this time examines how crisis triage centers may impact law enforcement operations.
Provider Capacity: Locally specific.
Public System Partners and Political Will: Learning-community members agreed that having a well-connected group of stakeholders is the first step to building a crisis triage center, and the array of funders above indicates that many agencies may take interest.
First Step to Build: Having a strong, well-connected partnership of stakeholders who can identify and agree on the gaps and the solutions to fix them; then, determining who pays.
Outcomes/Problems Likely to Motivate Investment: Demonstrating cost savings from reduced jail and hospital stays.

P A Y F O R S U C C E S S A N D T H E C R I S I S I N T E R V E N T I O N T E A M M O D E L 1 9
HYPOTHETICAL PFS-CIT PROJECT: HIGH USERS OUTREACH AND DATA
Problem: Many jurisdictions have noted that a small number of people with high behavioral health and other needs often have repeated interactions with hospitals, law enforcement, and public service systems (Chambers et al. 2013). The basic CIT model is often reactive, but proactively identifying and reaching out to so-called high users (people who have high rates of contact with criminal justice, health, and/or other public services systems) has the potential to help prevent crises and reduce costs. In Chicago, a partnership of stakeholders decided that outreach groups that include a CIT officer and clinicians will help to ensure safety, based on either the individual’s history or because of the neighborhood. (Though some private providers have provided outreach to this group in the past, their capacity is too low; also, providers tend to avoid the most vulnerable areas because of safety concerns.) However, systematically identifying high users has proven challenging, and such a strategy will require resources, flexible support from the city, and a strengthened partnership between law enforcement, EMS, and other stakeholders.
Program Strength: Growing evidence supports targeting services at people with the highest needs to reduce costs and minimize inefficient or inappropriate service use (Culhane, Metraux, and Hadley 2002; Simon et al. 2001). Potential enhancements could include installing data infrastructure or other tools to identify high users and building outreach teams. This could also bring value to other city projects.
Provider Capacity: In Chicago, learning-community participants perceived that outreach teams will be most effective if the police department can hire clinicians. This is predicated on having the funding and infrastructure in place to support their work.
Public System Partners and Political Landscape: An interagency group has been meeting and has demonstrated interest in moving forward; however, one challenge is determining who pays for this type of intervention because it would require resources from different systems.
Project Alignment: Multiple agencies, including law enforcement and hospitals, are likely to benefit, making this a promising potential opportunity for PFS. In Chicago, one potential payer may be the state of Illinois, which funds mental health services. However, though some PFS projects have successfully entered contracts with state payers, both Chicago and Illinois currently have significant financial troubles (e.g., Illinois had no state budget for two years).a
Project Evaluability: Chicago has data from the Criminal Justice and Mental Health Coordinating Team, which has led CIT efforts, and data from a class-action lawsuit about putting people in nursing homes. The University of Chicago has also begun efforts to obtain and integrate data to identify high users. However, data sharing and privacy concerns are presenting early challenges and likely to complicate evaluation efforts.
A randomized controlled trial is also likely to generate significant pushback from partners who want to serve everyone who asks for services or has a need. Emphasizing that the need is so high that providers can’t serve everyone, and using a list of people with the highest needs or highest use as a naturalistic waiting list may help to alleviate some of these concerns. However, collecting control group data will likely remain a challenge.
a Jessica D’Onofrio, Sarah Schulte, and Craig Wall, “Illinois Misses Budget Deadline, House will Reconvene Saturday,” ABC 7, July
1, 2017, http://abc7chicago.com/politics/no-budget-deal-friday-house-will-reconvene-saturday/2167095/.

2 0 P A Y F O R S U C C E S S A N D T H E C R I S I S I N T E R V E N T I O N T E A M M O D E L
Assessing CIT Program Elements through the PFS Framework: Determining Whether PFS Is Appropriate
As the previous sections have explained, the path of developing organizational culture and responses is
different for every jurisdiction. After cross-agency coordination and trainings, the next steps for
incrementally growing a jurisdiction’s CIT program will vary across jurisdictions because of their unique
characteristics, conditions, and needs. As jurisdictions consider their next incremental step to improve
their CIT program, they should also consider whether that step could be financed through PFS. This
section provides a framework for considering whether a given incremental improvement in a
jurisdiction’s CIT program is suitable for financing through PFS. (More information on this framework is
available in Urban’s PFS Project Assessment Tool; see Milner et al. 2016.)
TABLE 4
PFS and CIT: Who Are the Main Players?
Key CIT partners and their PFS roles
PFS role Potential CIT partners
Intermediary: coordinates among partners to assess feasibility, structure the transaction, and manage payments
Locally specific. Should be a neutral third party able to coordinate across groups, ideally with experience in each stage of the PFS process (feasibility, structuring, and implementation). For CIT, the intermediary could be a local chapter of the National Alliance on Mental Illness, for example. PFS projects may also bring in a “financial intermediary” whose specific expertise lies in navigating the PFS contracting process.
Investor: provides up-front capital for a project and gets paid back with interest if it succeeds
Foundations Insurance companies that cover jurisdictions in use-of-force settlement cases
End Payer: pays for the program if it is successful
Potential end payers may include: Mental/behavioral health agencies Jails/correctional agencies (e.g., if jail usage is measured and reduced) Hospitals (may be interested in reducing emergency department visits and/or frequent
follow-up visits)
Service Providers: delivers the actual intervention
Police and sheriff’s departments Crisis triage centers Hospitals Other mental/behavioral health service providers
Evaluator: determines if a program achieved successful outcomes
Variable; should have experience conducting rigorous program evaluations

P A Y F O R S U C C E S S A N D T H E C R I S I S I N T E R V E N T I O N T E A M M O D E L 2 1
Public System Partners and Political Landscape: How strong is political and
bureaucratic support from the public partner (government) for the proposed project and
financing structure?
Strong partnerships and the committed support of agencies—including law enforcement and behavioral
health—are prerequisites for CIT and enable information sharing that is critical to program success. PFS
requires partners to be actively engaged, invested in program implementation, and willing to share data
to measure performance. Though actual commitment from agencies varies by jurisdiction, the centrality
of partnership to each model is promising.
CHALLENGES
Collaboration failures. Collaboration can be challenging to maintain, and learning-community
participants identified several specific concerns for CIT. In jurisdictions without designated drop-off
locations, it can be challenging to secure the buy-in of local hospitals, which may have concerns about
security or accommodating CIT users. Like any collaborative venture, CIT may also face waning support
from individual partners or vulnerability from changes in leadership.
Local government resources. Though PFS provides up-front investment in projects to offset the risks of
potential failure, governments still must pay for programs if they are successful. If a jurisdiction does not
have the resources to do so, then a PFS deal will not be viable.
Problem Definition: How clearly defined and understood is the problem?
CIT tends to be presented as a solution to two primary problems. First, in the short term, CIT seeks to
ensure the safety of people with mental/behavioral health conditions, the people around them, and
officers. In the longer term, CIT seeks to reduce unnecessary contact with the criminal justice system
for people with behavioral health issues. Both problems can be measured using data such as police call
dispositions and jail admissions.
Identifying the problem begs the question of what a successful solution to that problem looks like.
The solution should not be broad or general, such as “improve responsiveness to the target population.”
Instead, it should be a specific objective of the incremental next step a jurisdiction is considering to
advance their CIT program. This requires special attention to properly defining a measurable and
appropriate form of success.
DEFINING A MEASURABLE AND APPROPRIATE FORM OF SUCCESS
One of the most important and challenging aspects of a PFS deal is determining which outcomes will
decide whether a project was successful (and whether the investor gets repaid). Often, PFS projects will
measure payment outcomes (which determine payment) and nonpayment outcomes (which may be of
interest as performance metrics but do not determine payment).
For CIT, outcomes may depend on what specific goal jurisdictions are most interested in achieving.
For example, a jurisdiction primarily interested in diverting people with behavioral health issues from

2 2 P A Y F O R S U C C E S S A N D T H E C R I S I S I N T E R V E N T I O N T E A M M O D E L
the criminal justice system and/or emergency departments may think about outcomes in a different way
than a jurisdiction primarily interested in officer safety and liability. CIT may also have secondary goals,
such as changing agency culture or law enforcement awareness of mental health. Drawing on earlier
evaluations and practical experience, the learning-community members proposed outputs (measures
that show a CIT program is doing what it should be to reach its goals) and outcomes (measures that
show CIT is achieving its goals). These are presented in figure 2.
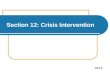
FIGURE 2
Measuring CIT
Examples of measurable outputs and outcomes related to CIT
CIT Components
Training
Partnership
Coordination with health service providers
Outputs
Training appropriate number of CIT officers
Successfully identifying calls as CIT-related (911/dispatch)
Percentage of calls with an identified mental/behavioral health where CIT officer responded
Officer awareness of CIT
Crisis triage center use
Service referrals and/or connections to case management
Outcomes
Reduced percentage of calls with a mental health component that result in arrest
Reduced use of force
Reduced officer injuries
Reduced inappropriate emergency department usage
Improved quality of interactions between law enforcement and people with mental health problems
Increased linkage to appropriate mental health services
Decline in mental health crisis calls
Cost savings (e.g., from connecting high users to more sustainable treatment services or reducing use of force, use of sick leave, loss of capacity because of injury or suspension, and lawsuits)
Culture change
Improved police-community trust
Learning community participants also described several challenges with measuring the success of
CIT. There is little information on the prevalence of police encounters with people with mental health
conditions, partly because it can be challenging to determine whether calls have a mental health
component. Emergency operators and dispatchers responding to 911 calls may not have the
information or training to ask and affirm that a situation may involve a person with a mental health
condition, and officers may have trouble assessing this on the street. These challenges extend to
reporting; for example, officers may be inconsistent in noting whether an interaction involved a mental
health component, compared with simply listing it under another crime or incident code (e.g., labeling a

P A Y F O R S U C C E S S A N D T H E C R I S I S I N T E R V E N T I O N T E A M M O D E L 2 3
behavioral health–related situation as an assault). Police data systems may not have an easy way to
identify such incidents in aggregate.
The learning community also identified some measures to avoid. For example, officer time spent on
a call is a problematic performance measure in the context of CIT. Ideally, a CIT operation would allow
officers to quickly address a situation and move on to their next call. However, part of a CIT officer’s
training is to know when to take time to resolve a situation; using time as a performance metric may
exacerbate these competing priorities. Learning-community members also emphasized that metrics
related to insurance coverage (e.g., treating people with insurance coverage) were inappropriate
because first responders are required to respond regardless of insurance status.
Another problem is that success for one agency may raise challenges for another. For example, if
law enforcement successfully diverts someone away from the criminal justice system, this may transfer
a greater burden to behavioral health treatment providers. CIT may also cause some outcomes to
increase initially, then decline: one participant said that when they first launched CIT, there was a spike
in mental health calls for service as people became aware of the program’s existence. It was only after
this initial reaction stabilized that it became possible to rely on this metric.
Program Strength: How strong is the proposed solution to address the problem?
Though existing research is insufficient to place CIT in the realm of “evidence-based practice,” (Watson
and Fulambarker 2012) it is generally considered a promising or “best practice” in law enforcement
(Thompson and Borum 2006; Watson and Fulambarker 2012), with examples of success in several
jurisdictions (see Compton et al. 2008). The evaluation component of a PFS deal has the potential to
strengthen this body of research.
Given the variation across jurisdictions, many different program components or increments could
be required to enhance a jurisdiction’s ability to provide responsive and coordinated services to people
with mental health needs. Some of the reasonable next steps for a jurisdiction will be supported by an
evidence base, but others will not, providing limited insight on the selected program component’s
effectiveness.
Project Evaluability: Does the proposed project have a clear, rigorous, and feasible
evaluation plan?
CIT has been evaluated, though few studies have met the level of rigor necessary for a PFS evaluation.
Drawing on the literature and practical experience, learning-community members identified potential
outcomes and data sources that could be used to measure the success of CIT (see figure 2). Where there
is no evidence base for a specific program component but all the PFS stakeholders agree the program
component is reasonable, PFS can actually be used to help create the evidence base because evaluation
is part of the PFS process.

2 4 P A Y F O R S U C C E S S A N D T H E C R I S I S I N T E R V E N T I O N T E A M M O D E L
Provider Capacity: Is the service provider capable of effectively delivering the program?
PFS requires ample provider capacity and data capacity, which vary greatly across jurisdictions. Current
trends lay a promising foundation for PFS data capacity: a growing number of jurisdictions are seeking
to link health and criminal justice systems, often to reduce costs and provide more targeted outreach
and support to high users. Such efforts not only increase data linkage across agencies, but also help to
cultivate a culture of information sharing.
SPECIFIC CONSIDERATIONS AND CHALLENGES RELATED TO PROVIDER CAPACITY
Weak health infrastructure. One of the most common challenges identified by the learning community
was the weakness of local health infrastructure. If officers have nowhere to take individuals after
addressing a crisis, they may feel compelled to arrest people they do not feel are safe to leave on the
street because they don’t see an alternative. Participants noted that many officers view jail as the only
way to get someone into treatment because of the lack of community-based options.
Limited law enforcement capacity. Prioritizing CIT takes a great deal of commitment from law
enforcement agencies, which can be challenging to balance with their high volume of work and limited
budgets. Ensuring that leadership is willing to prioritize CIT in this way is essential to success but also a
vulnerability of CIT partnerships.
Culture change. Shifting culture in any way, shape, or form is often challenging. Though officers are
accustomed to calling for specific types of backup (e.g., a CIT officer), learning to look for signs of
mental/behavioral health issues, as opposed to criminal activity, requires a shift in thinking that can be
difficult and contradictory to prior training.
Project Alignment: How well do all the key components of the proposed project fit together
in a specific jurisdiction?
The resources and capacity of each jurisdiction will differ, so it’s difficult to predict how PFS-CIT project
components would fit together. For example, local health care providers may be initially reluctant to
work with police or to accept people after a crisis situation. In another jurisdiction, a stakeholder agency
may be unwilling to provide data or depart from their standard procedures and protocols, even if it is
necessary for the PFS project to succeed. It is critical that all the stakeholders understand and agree on
the key components of the PFS project, and that they fit together in a manner that will allow the project
to function properly.
SPECIFIC CONSIDERATIONS AND CHALLENGES REATED TO PROJECT ALLIGNMENT
Data sharing. Exchanging information between law enforcement and health agencies can be greatly
beneficial to CIT, but also raises challenges related to patient privacy. The ability to work out a solution
to these issues reflects how well stakeholder agencies are aligned with common objectives for the CIT
program they are attempting to support through PFS.

P A Y F O R S U C C E S S A N D T H E C R I S I S I N T E R V E N T I O N T E A M M O D E L 2 5
Large versus small jurisdictions. Learning-community participants noted that though CIT is discussed
most often in large urban contexts, it may require special considerations for small and/or rural
departments. Small departments may have some advantages because dispatchers are more likely to
know the CIT-trained officers to call. However, small departments often have limited budgets with less
flexibility. In some cases, it may be appropriate for small jurisdictions to be part of a larger regional CIT
effort (e.g., multicounty programs), which requires considering the priorities of all the relevant
stakeholder agencies within that regional unit.
Summary Insights and Considerations for Policymakers
The pay for success model is focused on financing government programs, and the Crisis Intervention
Team model is focused on responses to metal health issues in the community. Though these two models
deal with different aspects of public administration, they both emphasize achieving certain outcomes,
rather than simply performing certain actions or producing certain outputs. This shared emphasis
represents these models’ departure from common approaches to public administration.
Similarities between the PFS and CIT models create a natural opportunity for PFS to support the
development and growth of CIT. The elements necessary to start a new CIT program (cross-agency
coordination on improving responses to mental health in the community, followed by training) have a lot
in common with the elements necessary to start a new PFS project (cross-agency collaboration on
defining and attempting to solve a specific social problem). Though PFS may not be the most
appropriate means of starting a new CIT program, the emphasis and infrastructure involved in starting a
CIT program does appear to lay the foundation for PFS to support expanding an existing CIT program.
The expert stakeholders who contributed to this brief explained that a CIT program can be different
for every jurisdiction based on its specific needs, circumstances, and culture. Though every CIT program
begins with cross-agency coordination and stakeholder training, there does not appear to be a standard
next step or specific program element for enhancing the program. Each jurisdiction needs to consider its
own circumstances, determine the specific outcomes to be improved, and decide on the best approach
for achieving those outcomes. These considerations are a natural fit for many elements of the PFS
model. Whether the jurisdiction’s plans fit within the rest of the PFS model will determine whether PFS
is a suitable means of financing the jurisdiction’s expansion of its CIT program.
Providing guidance on developing and growing CIT programs through PFS projects is the primary
objective of this brief, but a second objective is to highlight how both models necessitate an important
shift in a jurisdiction’s public administration priorities. Rather than following specific actions or
producing specific outputs, an important emphasis on achieving specific outcomes is shared by Pay for
Success and the Crisis Intervention Team model.

2 6 P A Y F O R S U C C E S S A N D T H E C R I S I S I N T E R V E N T I O N T E A M M O D E L
Notes
1 This synopsis draws heavily from Milner (2016).
2 Includes projects categorized as “in progress” or “finished” as of August 2017 on payforsuccess.org, operated by the Nonprofit Finance Fund. See “Projects,” Nonprofit Finance Fund, accessed September 22, 2017, http://www.payforsuccess.org/projects/?sort=recent.
3 Cecilia Muñoz and Shaun Donovan, “Administration Nearly Doubles Number of ‘Pay for Success’ Feasibility Studies,” White House Blog, April 19, 2016, https://obamawhitehouse.archives.gov/blog/2016/04/19/administration-nearly-doubles-number-pay-success-feasibility-studies.
4 Such as the Ridealong app, which provides first responders with key background information about people with mental health conditions to help officers more effectively de-escalate situations.
5 A warm line serves as a resource for people struggling with mental health issues. Unlike hotlines, warm lines hope to help people before they reach a point of crisis.
6 See Bahora and colleagues (2008); Borum and colleagues (1998), Broussard and colleagues (2011); Canada, Angell, and Watson (2012); Compton and colleagues (2006, 2009, 2014a, 2015); Demir and colleagues (2009); Ellis (2014); Hanafi and colleagues (2008); Ritter and colleagues (2006, 2010); Wells and Schafer (2006).
7 See Compton and colleagues (2014b); Steadman and colleagues (2000); Teller and colleagues (2006); Watson and colleagues (2010).
8 See Franz and Borum (2011); Morabito and colleagues (2012); Skeem and Bibeau (2008); Steadman and colleagues (2000).
9 See Morabito and colleagues (2012) and Skeem and Bibeau (2008).
10 See Broner and colleagues (2004).
11 See El-Mallakh, Kiran, and El-Mallakh (2014).
12 See Canada, Angell, and Watson (2012); Compton and colleagues (2006, 2014a); and Ellis (2014).
13 See Borum and colleagues (1998); Compton and colleagues (2014a); Hanafi and colleagues (2008); Wells and Schafer (2006).
14 See Bahora and colleagues (2008); Broussard and colleagues (2011); and Ritter and colleagues (2006, 2010).
15 See Borum and colleagues (1998).
16 See Franz and Borum (2011); Morabito and colleagues (2012); Skeem and Bibeau (2008); and Steadman and colleagues (2000).
17 See Compton and colleagues (2014b); Steadman and colleagues (2000); Teller and colleagues (2006); and Watson and colleagues (2010).
18 See El-Mallakh, Kiran, and El-Mallakh (2014).
19 Examples include the Washington Post’s finding that a quarter of officer-involved shootings in the first half of 2015 killed someone in mental or emotional crisis. See Wesley Lowery, Kimberly Kindy, Keith L. Alexander, Julie Tate, Jennifer Jenkins, Steven Rich, “Distraught People, Deadly Results,” Washington Post, June 30, 2015, http://www.washingtonpost.com/sf/investigative/2015/06/30/distraught-people-deadly-results/?utm_term=.4052cadf7730.

P A Y F O R S U C C E S S A N D T H E C R I S I S I N T E R V E N T I O N T E A M M O D E L 2 7
References Action Alliance (National Action Alliance for Suicide Prevention). 2016. Crisis Now: Transforming Services Is within
Our Reach. Washington, DC: Education Development Center.
Addy, Catherine. 2005. “An Examination of the Development of Standardized Training Protocols for Law Enforcement Crisis Intervention Teams for the Mental Health Consumer.” PhD thesis, University of Memphis.
Alakeson, Vidhya, Nalini Pande, and Michael Ludwig. 2010. "A Plan to Reduce Emergency Room ‘Boarding’ Of Psychiatric Patients.” Health Affairs 29 (9):1637–42.
Bahora, Masuma, Sonya Hanafi, Victoria H. Chien, and Michael T. Compton. 2008. “Preliminary Evidence of Effects of Crisis Intervention Team Training on Self-Efficacy and Social Distance.” Administration and Policy in Mental Health and Mental Health Services Research 35 (3): 159–67.
Bengelsdorf, Herbert, John O. Church, Richard A. Kaye, Barbara Orlowski, and Diane C. Alden. 1993. “The Cost Effectiveness of Crisis Intervention: Admission Diversion Savings Can Offset the High Cost of Service.” Journal of Nervous and Mental Disease 181 (12): 757–62.
Borum, Randy, Martha Williams Deane, Henry J. Steadman, and Joseph Morissey. 1998. “Police Perspectives on Responding to Mentally Ill People in Crisis: Perceptions of Program Effectiveness.” Behavioral Sciences and the Law 16 (4): 393–405.
Broner, Nahama, Pamela K. Lattimore, Alexander J. Cowell, and William E. Schlenger. 2004. “Effects of Diversion on Adults with Co-occurring Mental Illness and Substance Use: Outcomes from a National Multi�Site Study.” Behavioral Sciences & the Law 22 (4): 519–41.
Broussard, Beth, Shaily Krishan, Dana Hankerson-Dyson, Letheshia Husbands, Tarianna Stewart-Hutto, and Michael T. Compton. 2011. “Development and Initial Reliability and Validity of Four Self-Report Measures Used in Research on Interactions between Police Officers and Individuals with Mental Illnesses.” Psychiatry Research 189 (3): 458–62.
Canada, Kelli E., Beth Angell, and Amy C. Watson. 2012. “Intervening at the Entry Point: Differences in How CIT Trained and Non-CIT Trained Officers Describe Responding to Mental Health-Related Calls.” Community Mental Health Journal 48 (6): 746–55.
Chambers, Catharine, Shirley Chiu, Marko Katic, Alex Kiss, Donald A. Redelmeier, Wendy Levinson, and Stephen W. Hwang. 2013. “High Utilizers of Emergency Health Services in a Population-Based Cohort of Homeless Adults.” American Journal of Public Health 103 (S2): S302–10.
Clarke, Gregory N., Heidi A. Herinckx, Ronald F. Kinney, Robert I. Paulson, David L. Cutler, Karen Lewis, and Evie Oxman. 2000. “Psychiatric Hospitalizations, Arrests, Emergency Room Visits, and Homelessness of Clients with Serious and Persistent Mental Illness: Findings from a Randomized Trial of Two ACT Programs vs. Usual Care.” Mental Health Services Research 2 (3): 155–64.
Clarke, Diane E., Debra Dusome, and Linda Hughes. 2007. “Emergency Department from the Mental Health Client’s Perspective.” International Journal of Mental Health Nursing 16 (2): 126–31.
Compton, Michael T., Masuma Bahora, Amy C. Watson, and Janet R. Oliva. 2008. “A Comprehensive Review of Extant Research on Crisis Intervention Team (CIT) Programs.” Journal of the American Academy of Psychiatry and the Law Online 36 (1): 47–55.
Compton, Michael T., Roger Bakeman, Beth Broussard, Dana Hankerson-Dyson, Letheshia Husbands, Shaily Krishan, et al. 2014a. “The Police-based Crisis Intervention Team (CIT) Model: I. Effects on Officers’ Knowledge, Attitudes, and Skills.” Psychiatric Services 65 (4): 517–22.
———. 2014b. "The Police-Based Crisis Intervention Team (CIT) Model: II. Effects on Level of Force and Resolution, Referral, and Arrest.” Psychiatric Services 65 (4): 523–29.
Compton, Michael T., Beth Broussard, Dana Hankerson-Dyson, Shaily Krishan, Tarianna Stewart, Janet R. Oliva, and Amy C. Watson. 2010. “System-and Policy-level Challenges to Full Implementation of the Crisis Intervention Team (CIT) Model.” Journal of Police Crisis Negotiations 10 (1-2): 72–85.

2 8 P A Y F O R S U C C E S S A N D T H E C R I S I S I N T E R V E N T I O N T E A M M O D E L
Compton, Michael T., Beth Broussard, Thomas A. Reed, Anthony Crisafio, and Amy C. Watson. 2015. "Surveys of Police Chiefs and Sheriffs and of Police Officers About CIT Programs.” Psychiatric Services 66 (7): 760–63.
Compton, Michael T., Berivan N. Demir Neubert, Beth Broussard, Joanne A. McGriff, Rhiannon Morgan, and Janet R. Oliva. 2009. “Use of Force Preferences and Perceived Effectiveness of Actions Among Crisis Intervention Team (CIT) Police Officers and Non-CIT Officers in an Escalating Psychiatric Crisis Involving a Subject with Schizophrenia.” Schizophrenia Bulletin 37 (4): 737–45.
Compton, Michael T., Michelle L. Esterberg, Robin McGee, Raymond J. Kotwicki, and Janet R. Oliva. 2006. “Crisis Intervention Team Training: Changes in Knowledge, Attitudes, and Stigma Related to Schizophrenia.” Psychiatric Services 57 (8): 1199–202.
Culhane, Dennis P., Stephen Metraux, and Trevor Hadley. 2002. "Public Service Reductions Associated with Placement of Homeless Persons with Severe Mental Illness in Supportive Housing.” Housing Policy Debate 13 (1): 107–63.
Demir, Berivan, Beth Broussard, Sandra M. Goulding, and Michael T. Compton. 2009. “Beliefs about Causes of Schizophrenia among Police Officers Before and After Crisis Intervention Team Training.” Community Mental Health Journal 45 (5): 385–92.
Dupont, Randolph, and Sam Cochran. 2000. “Police Response to Mental Health Emergencies: Barriers to Change.” Journal of the American Academy of Psychiatry and the Law 28 (3): 338–44.
Dupont Randolph, Sam Cochran, and Sarah Pillsbury. 2007. Crisis Intervention Team: Core Elements. Memphis, TN: University of Memphis, School of Urban Affairs and Public Policy.
El-Mallakh, Peggy L., Kranti Kiran, and Rif S. El-Mallakh. 2014. “Costs and Savings Associated with Implementation of a Police Crisis Intervention Team.” Southern Medical Journal 107 (6): 391–5.
Ellis, Horace A. 2014. "Effects of a Crisis Intervention Team (CIT) Training Program Upon Police Officers Before and After Crisis Intervention Team Training.” Archives of Psychiatric Nursing 28 (1): 10–16.
Franz, Stephanie, and Randy Borum. 2011. “Crisis Intervention Teams May Prevent Arrests of People with Mental Illnesses.” Police Practice and Research: An International Journal 12 (3): 265–72.
Fuller, Doris A., H. Richard Lamb, Michael Biasotti, and John Snook. 2015. Overlooked in the Undercounted: The Role of Mental Illness in Fatal Law Enforcement Encounters. Arlington, VA: Treatment Advocacy Center.
Hanafi, Sonya, Masuma Bahora, Berivan N. Demir, and Michael T. Compton. 2008. “Incorporating Crisis Intervention Team (CIT) Knowledge and Skills into the Daily Work of Police Officers: A Focus Group Study.” Community Mental Health Journal 44 (6): 427–32.
Milner, Justin. 2016. “Pay for Success.” Washington, DC: Evidence-Based Policymaking Collaborative.
Milner, Justin, Matthew Eldridge, Kelly Walsh, and John K. Roman. 2016. Pay for Success Project Assessment Tool. Washington, DC: Urban Institute.
Morabito, Melissa S., Amy N. Kerr, Amy C. Watson, Jeffrey Draine, Victor C. Ottati, and Beth Angell. 2012. “Crisis Intervention Teams and People with Mental Illness Exploring the Factors that Influence the Use of Force.” Crime & Delinquency 58 (1): 57–77.
Ritter Christian, Jennifer L. S. Teller, Mark R. Munetz, et al. 2006. “The Quality of Life of People with Mental Illness: Consequences of Pre-arrest and Post-arrest Diversion Programs.” Presented at Second National CIT Conference, Orlando, FL, September.
Ritter, Christian, Jennifer L. S. Teller, Mark R. Munetz, and Natalie Bonfine. 2010. “Crisis Intervention Team (CIT) Training: Selection Effects and Long-Term Changes in Perceptions of Mental Illness and Community Preparedness.” Journal of Police Crisis Negotiations 10 (1-2): 133–52.
SAMHSA (Substance Abuse and Mental Health Services Administration). 2014. Crisis Services: Effectiveness, Cost-Effectiveness, and Funding Strategies. Rockville, MD: SAMHSA.
Simon, Gregory E., Willard G. Manning, David J. Katzelnick, Steven D. Pearson, Henry J. Henk, and Cindy P. Helstad. 2001. “Cost-effectiveness of Systematic Depression Treatment for High Utilizers of General Medical Care.” Archives of General Psychiatry 58 (2): 181–87.

P A Y F O R S U C C E S S A N D T H E C R I S I S I N T E R V E N T I O N T E A M M O D E L 2 9
Skeem, Jennifer, and Lynne Bibeau. 2008. “How Does Violence Potential Relate to Crisis Intervention Team Responses to Emergencies?” Psychiatric Services 59 (2): 201–4.
Steadman, Henry J., Martha Williams Deane, Randy Borum, and Joseph P. Morissey. 2000. “Comparing Outcomes of Major Models of Police Responses to Mental Health Emergencies.” Psychiatric Services 51 (5): 645–49.
Teller, Jennifer L. S., Mark R. Munetz, Karen M. Gil, and Christian Ritter. 2006. "Crisis Intervention Team Training for Police Officers Responding to Mental Disturbance Calls.” Psychiatric Services 57 (2): 232–37.
Thompson, Larry E., and Randy Borum. 2006. “Crisis Intervention Teams (CIT): Considerations for Knowledge Transfer.” Law Enforcement Executive Forum 6 (3): 25–36.
Watson, Amy C. 2010. “Research in the Real World: Studying Chicago Police Department’s Crisis Intervention Team (CIT) Program.” Research on Social Work Practice 20 (5): 536–43.
Watson, Amy C., and Anjali J. Fulambarker. 2012. “The Crisis Intervention Team Model of Police Response to Mental Health Crises.” Best Practices in Mental Health 8 (2): 71–81.
Watson, Amy C., Victor C. Ottati, Melissa Morabito, Jeffrey Draine, Amy N. Kerr, and Beth Angell. 2010. "Outcomes of Police Contacts with Persons with Mental Illness: The impact of CIT.” Administration and Policy in Mental Health and Mental Health Services Research 37 (4): 302–17.
Wells, William, and Joseph A. Schafer. 2006. “Officer Perceptions of Police Responses to Persons with a Mental Illness.” Policing: An International Journal of Police Strategies & Management 29 (4): 578–601.

3 0 P A Y F O R S U C C E S S A N D T H E C R I S I S I N T E R V E N T I O N T E A M M O D E L
About the Authors
David McClure is a research associate in the Justice Policy Center at the Urban
Institute. His work focuses on improving the efficiency and effectiveness of
government through science and technology, particularly in the justice system.
McClure holds bachelor’s degrees from the University of Georgia and a MA and a PhD
from George Mason University.
Ellen Paddock is a research associate in the Justice Policy Center at the Urban
Institute. Her work focuses on the overlap between public health and criminal justice
and on public safety strategies that effectively reduce crime while minimizing collateral
damage to vulnerable communities. Before joining Urban, Paddock completed
internships with a youth gang intervention program, a reentry job training program,
and an interagency criminal justice resource center. She graduated from Duke
University in May 2014 with a BA in public policy and Arabic.
Rayanne Hawkins is the business operations manager for the Pay for Success Initiative
in the Policy Advisory Group at the Urban Institute. She works on the help desk for Pay
for Success training and technical assistance, and she tracks initiative goals and
milestones. She received her MBA from Georgetown University’s McDonough School
of Business, where she studied alternative financing for social programs.
Mayookha Mitra-Majumdar is a research assistant with the Policy Advisory Group at
the Urban Institute, where she works on the Pay for Success Initiative. Before joining
the Policy Advisory Group, Mitra-Majumdar interned with Urban’s Health Policy
Center, where she supported the second-year evaluation of the Strong Start for
Mothers and Newborns Initiative. Her research at the University of Pennsylvania’s
Center for Mental Health Policy and Services Research focused on underserved
communities’ access to health and social services. Mitra-Majumdar has also worked
with issues around global health justice. Mitra-Majumdar graduated from the
University of Pennsylvania, where she received a BA in biology.

P A Y F O R S U C C E S S A N D T H E C R I S I S I N T E R V E N T I O N T E A M M O D E L 3 1
Acknowledgments
This project was supported by Grant No. 2012-DJ-BX-K001 awarded by the Bureau of Justice
Assistance. The Bureau of Justice Assistance is a component of the Department of Justice's Office of
Justice Programs, which also includes the Bureau of Justice Statistics, the National Institute of Justice,
the Office of Juvenile Justice and Delinquency Prevention, the Office for Victims of Crime, and the
SMART Office. Points of view or opinions in this document are those of the authors and do not
necessarily represent the official position or policies of the US Department of Justice.
We are grateful to them and to all our funders, who make it possible for Urban to advance its
mission.
The views expressed are those of the authors and should not be attributed to the Urban Institute,
its trustees, or its funders. Funders do not determine research findings or the insights and
recommendations of Urban experts. Further information on the Urban Institute’s funding principles is
available at www.urban.org/support.
ABOUT THE URBAN INSTIT UTE The nonprofit Urban Institute is dedicated to elevating the debate on social and economic policy. For nearly five decades, Urban scholars have conducted research and offered evidence-based solutions that improve lives and strengthen communities across a rapidly urbanizing world. Their objective research helps expand opportunities for all, reduce hardship among the most vulnerable, and strengthen the effectiveness of the public sector.
Copyright © November 2017. Urban Institute. Permission is granted for reproduction of this file, with attribution to the Urban Institute.
2100 M Street NW Washington, DC 20037
www.urban.org
Recommended