
OUTPATIENT PHYSICAL THERAPY FOR A PATIENT WITH TRANSLOCATION
DOWN SYNDROME
A Doctoral Project A Comprehensive Case Analysis
Presented to the faculty of the Department of Physical Therapy
California State University, Sacramento
Submitted in partial satisfaction of the requirements for the degree of
DOCTOR OF PHYSICAL THERAPY
by
Cynthia G. Rivera
SUMMER 2015

ii
© 2015
Cynthia G. Rivera
ALL RIGHTS RESERVED

iii
OUTPATIENT PHYSICAL THERAPY FOR A PATIENT WITH TRANSLOCATION
DOWN SYNDROME
A Doctoral Project
by
Cynthia G. Rivera
Approved by: __________________________________, Committee Chair Dr. Katrin Mattern-Baxter __________________________________, First Reader Dr. Toran MacLeod __________________________________, Second Reader Dr. Edward Barakatt ____________________________ Date

iv
Student: Cynthia G. Rivera
I certify that this student has met the requirements for format contained in the University
format manual, and that this project is suitable for shelving in the Library and credit is to
be awarded for the project.
__________________________________, Graduate Coordinator ____________ Edward Barakatt, PT, PhD Date Department of Physical Therapy

v
Abstract
of
OUTPATIENT PHYSICAL THERAPY FOR A PATIENT WITH TRANSLOCATION
DOWN SYNDROME
by
Cynthia G. Rivera
A patient with translocation Down Syndrome was seen for physical therapy
treatment for ten sessions from 03/21/2014 – 05/23/2014 in an outpatient clinic under the
supervision of a licensed physical therapist.
The patient was evaluated at the initial encounter with Gross Motor Function
Measure-88, Peabody Developmental Motor Scales II, Pediatric Evaluation of Disability
Inventory, Functional Mobility Scale and 10 meter walk test and a plan of care was
established. Main goals for the patient were independent ambulation and improvement in
gross motor skills. Main interventions used were intensive, task-specific training and
home exercise program. The patient achieved the following goals: improvements in gross
motor function and improvements in functional ambulation. The patient was discharged
to home with parents as primary caregivers.
_______________________, Committee Chair Katrin Mattern-Baxter PT, PhD _______________________ Date

vi
ACKNOWLEDGEMENTS
I would like to thank my husband for being patient, supportive and understanding
throughout my educational endeavors.
I would like to express my deep gratitude to my parents who encouraged my pursuit of
higher learning. Me gustaría expresar mi profunda gratitud a mis padres que alentaron mi
búsqueda de la educación superior.
I would also like to thank my friends/future colleagues and faculty at California State
University, Sacramento’s Department of Physical Therapy for their patient guidance,
encouragement and critiques of this doctoral project.

vii
TABLE OF CONTENTS Page
Acknowledgements ............................................................................................... vi
List of Tables ...................................................................................................... viii
Chapter
1. GENERAL BACKGROUND ...................................................................................... 1
2. CASE BACKGROUND DATA .................................................................................. 3
3. EXAMINATION – TESTS AND MEASURES ......................................................... 6
4. EVALUATION ......................................................................................................... 16
5. PLAN OF CARE – GOALS AND INTERVENTIONS ............................................ 17
6. OUTCOMES ............................................................................................................. 29
7. DISCUSSION ............................................................................................................ 36
References ....................................................................................................................... 40

viii
LIST OF TABLES Tables Page
1. Examination Data……………………………….… ...... ……………………………. 13
2. Evaluation and Plan of Care……… ...... ………….…………………………………. 17
3. Outcomes……………………………….……… .............. …………………………. 29

1
Chapter 1
General Background
Down syndrome (DS) is a genetic condition that results in cognitive and motor
delays and is estimated to occur in 1 out of 800 live births.1-3 Cases of DS can be
categorized as complete trisomy 21, mosaicism of trisomy 21, and translocations
involving chromosome 21.1,4 Complete trisomy 21 is the presence of 3 copies of
chromosome 21 and accounts for 95% of DS cases, whereas moscaicism of trisomy 21
and translocation involving chromosome 21 occur at a rate of 1-3%.1 In translocations, all
or part of one of the duplicated chromosome 21 will attach to a nearby chromosome.2
Common translocation attachment sites include chromosome 13, 14, 15, 18, and 22.2
In neonates, trisomy 21 and translocations involving chromosome 21 present with
similar physical appearance and complications such as cognitive delays, gastrointestinal
malformations, severe visual impairment, congenital heart defects and display similar
prenatal screening test abnormalities.1 In general, characteristics among individuals with
complete trisomy or non-disjunction and translocation are not remarkably different,
whereas individuals with mosaicism may only demonstrate a few characteristics of DS
because not every cell possesses additional genetic material.4 Pathology of mosaicism DS
is attributed to an error in cell division and not the result of inherited risk. Approximately
two-thirds of individuals with translocation DS are attributed to an error in cell division
and approximately one-third of individuals with translocation DS are due to a parent
being a carrier for the translocation. A high recurrence rate of translocation DS in

2
subsequent pregnancies exists when a parent is a carrier for the translocation. While non-
disjunction DS is reported to occur as an error in cell division, some families may be
prone to error of non-disjunction and may have a higher risk of having a child with DS.2,4
Increased maternal and paternal age has been associated with an increased risk of non-
disjunction DS, whereas risk of translocation DS occurs equally among maternal and
paternal ages.1,2 Infants and young children diagnosed with DS typically present with low
muscle tone, poor postural control, ligamentous laxity, and poor balance, which may
negatively impact the acquisition of motor skills.3,5-7 Individuals with non-disjunction and
translocation DS have increased risk of cognitive delays, congenital heart defects,
gastrointestinal malformations, severe visual impairments, thyroid disorders, epilepsy and
hearing loss.1,2 On average, children with DS will walk independently at approximately 2
years of age, one year later than a typically developing child.3,6,8 The variable
development in children with DS is attributed to the number and severity of medical
complications.7 The lifespan of 61% of individuals with DS is 50 years of age, and 50%
of that group will survive beyond 57 years of age.1

3
Chapter 2
Case Background Data
Examination - History
The patient was a 2 year, 2 month old active Hispanic female with gross motor
delays. The patient was born to a 34 year old mother and the child was given a diagnosis
of translocation DS a few days after birth. Her older sibling was typically developing.
The patient had a medical history of premature birth, neonatal jaundice and weight loss.
She was born at 36 weeks and weighed 5 pounds 2 ounces. There were no reported
complications during pregnancy. The patient’s mother was unaware of the DS diagnosis
during pregnancy as prenatal testing to assess risk of DS was not assessed. The patient
received phototherapy to treat neonatal jaundice in the hospital during the initial hospital
stay immediately after birth and again at 6 days old. Jaundice was determined to be
resolved at 1 week following discharge from the hospital. The patient’s parents were
referred to a lactation specialist when the patient was 6 days old. Per parent report,
patient’s weight gain was no longer a concern of her primary care physician.
Transthoracic Echocardiography (TTE) was performed when patient was 2 weeks old to
rule out congenital heart disease. Findings from TTE revealed a small secundum atrial
septal defect measuring up to 3 mm with a left to right shunt, also known as a heart
murmur. Per parent report, the atrial septal defect was determined to be closed at 1 year
of age by the cardiologist. It was recommended that she follow up with a cardiologist at 3
years of age. The patient was not followed by any other specialists. The patient had

4
pneumonia in January 2013 and was hospitalized for 5 days and treated with albuterol
breathing treatments only during the hospital stay.
The patient received services from the county services including specialized
instruction with infant educator twice a month, nursing consultation six times per year,
speech therapy six times per year and physical therapy once a month. Per parent report,
the infant educator and physical therapist focused therapeutic services on improving the
patient’s fine motor skills.
The patient lived in single family home with her mother, father, and older brother.
The patient’s grandparents were supportive and lived nearby. Patient had one small step
at the front and rear entrances. The patient used crawling as her preferred method of
ambulation and was able to crawl distances up to 150 feet. The patient had not yet begun
to walk independently but was able to walk up to 80 feet with two hand held assistance.
The parent’s chief complaint was inability of the child to walk independently. Patient’s
parents expressed a goal for the patient to walk independently without assistance.
The patient was recruited from a supported treadmill exercise program to
participate in this case report. The patient was given approval by her primary care
physician to participate and noted no past medical history other than her DS diagnosis,
precautions or contraindications applicable to the patient. The patient did not take any
medications, herbal remedies, vitamins or supplements throughout the duration of
treatment for this case report. Systems affected by DS include the musculoskeletal

5
system, neuromuscular system and cognitive system delays. Other systems have been
checked and cleared.
Examination – Medications
Patient did not take any medications, herbal remedies, vitamins or supplements.

6
Chapter 3
Examination – Tests and Measures
The outcome measures utilized for this patient assessed the patient at the levels of
“Body Structure and Function,” “Activity” and “Participation” using the International
Classification of Function – Children and Youth (ICF-CY) model. The primary outcome
measure utilized at the level of “Body Structure and Function” was the 10 meter walk test
(10MWT). Primary outcome measures for assessing improvement at the level of
“Activity” were the Gross Motor Function Measure-88 (GMFM-88) , the Gross Motor
subscales of the Peabody Developmental Motor Scales, second edition (PDMS-2) and the
Functional Mobility Scale (FMS) The “Mobility, Caregiver Assistance and Modification”
domains of the Pediatric Evaluation of Disability Inventory (PEDI) were used as primary
outcome measures for assessing improvement at the level of “Participation,” although it
is important to note that the PEDI assesses changes at both the “Activity” and
“Participation” levels.
The 10MWT was originally designed to assess walking speed in adults post-
stroke. The 10MWT has demonstrated good test-retest reliability with intraclass
correlation coefficient (ICC) of 0.81with a 95% confidence interval (CI) between 0.75-
0.90 in adults. A modified version of the 10MWT, the 10 meter fast walk test (10mFWT)
uses a fast walking pace instead of a self-selected pace for the test. In children with CP, a
change of 107% is defined as the minimal detectable change (MDC).9 An MDC95 for the
10mFWT in children with CP of 12.2 seconds has been reported. Test-retest reliability

7
cited for the 10mFWT with ICC of 0.81 and 95% CI between 0.65-0.90.10 Unfortunately
MDC data pertaining to young children with DS was not found in the literature.
The FMS is a performance measure and was developed for children with CP to
assess functional mobility in the home, school and community settings corresponding to
distances of 5 meters, 50 meters and 500 meters, respectively. The FMS was designed to
assess individuals with CP between the ages of 4 years of age to 18 years of age. Inter-
rater reliability is reported for surgeons as the FMS and ICC for 5 meters is 0.95 with
95% CI between 0.88-0.98, ICC for 50 meters is 0.94 with 95% CI between 0.88-0.97
and ICC for 500 meters is 0.95 with 95% CI between 0.89-0.99.11 MDC values are not
available for the FMS as the ratings are based on an ordinal scale.12 Values for
responsiveness were assessed in children with spastic CP utilizing mean change between
pre-surgical intervention and three months post-surgical intervention. A statistically
significant mean change in FMS ratings is cited as 1.8 for 5 meters, 1.1 for 50 meters and
for 500 meters. Construct validity has been established for the FMS in children with CP11
Psychometric data for the FMS and DS were not found in the literature.
The GMFM-88 is a criterion-referenced measure and evaluates gross motor
abilities in children with cerebral palsy (CP), DS and acquired brain injury in their
abilities to perform activities in 5 dimensions: A) Lying/rolling, B) Sitting, C) Crawling,
D) Standing and E) Walking, Running and Jumping.13 The GMFM-88 was used to
develop the Gross Motor Function Classification System (GMFCS) and is used
throughout all GMFCS levels I through V in children with CP. The GMFCS was

8
originally developed to classify children with CP in terms of functional limitations.14
Scoring for the GMFM-88 is based on individual items scored on a 4 point scale
“completes” (3 points), “partial completion” (2 points), “initiates” (1 point) and “does not
initiate” (0 points).6,15 The GMFM-88 was originally assessed in children aged 5 months
to 16 years of age but may be used in children with gross motor skills at or below a
typically developing child of five years of age.15 High internal consistency has been
reported for the GMFM-88 in populations with CP demonstrated by Cronbach’s alpha of
0.99.9 High inter-rater and test-retest reliability have been reported in children with DS
with ICCs cited as 0.98 and 0.96, respectively.13 Face, content and construct validity have
been established for the GMFM-88 in populations with CP.9,13 A statistical significant
difference in change scores has been reported as 11% in children with DS.13 The
calculated SEM (SEM=SD√1-ICC)16 was determined to be 5.2. The SEM was calculated
using the total ICC of 0.96 and standard deviation (SD) of 26.13 The MDC95 (MDC95 =
1.96*SEM*√2)16 for the GMFM-88 was calculated to be 15%. The GMFM-88 has been
shown to be reliable, valid and responsive in children with CP17 and DS.6,13 Children with
DS usually obtain developmental quotient scores two standard deviations below their
typically developing peers when assessed using norm-referenced gross motor
development outcome measures. Developmental quotient scores express the development
of a child by relating their performance on a measure to their chronological age.13 Motor
growth curves for children with DS were developed to account for differences in motor
development compared to typically developing children. The motor growth curves for

9
children with DS are based on the GMFM-88 and provide an estimate of probability of
gross motor functions at different ages.6 The motor growth curves have been validated in
children with DS to assess prognosis of future gross motor development.6 The GMFM-88
was utilized as a prognostic tool and outcome measure for this case report.
The PDMS-2 is a standardized, norm-referenced measure comprised of six
subtests that assess the motor skills in children from birth to 6 years of age. The PDMS-2
is comprised of two scales, a Gross Motor Scale and a Fine Motor Scale. The six subtests
of the PDMS-2 include the Reflexes, Stationary, Locomotion, Object Manipulation,
Grasping, and Visual-motor Integration. The gross motor section of the PDMS-2 includes
Reflexes, Stationary, Locomotion and Object Manipulation subtests. The fine motor
section includes Grasping and Visual-motor Integration subtests. Scoring for the PDMS-2
is based on individual items scored on a 3 point scale categorized as “mastery of the
skill” (2 points), “partial mastery of the skill” (1 point), and “unable to demonstrate the
item or makes an attempt without demonstrating mastery of the skill” (0 points).18
According to the PDMS-2 manual, the Cronbach’s coefficient alpha for content of the
PDMS-2 subtest scores for the 24-25 month age range are 0.95 for Stationary, 0.96 for
Locomotion and 0.84 for Object Manipulation. The average Cronbach coefficient alphas
for content of the Stationary, Locomotion, and Object Manipulation subtests are 0.89,
0.96 and 0.90, respectively, demonstrating internal consistency reliability of the PDMS-2.
The PDMS-2 has a small standard error of measurement (SEM) of 1 for the 24-35 month
age group and an average across all age groups for the three subtests of the gross motor

10
section. Scoring for the PDMS-2 is available as raw scores, standard scores, age
equivalents and quotient scores. The low SEM with a range of PDMS-2 Gross Motor
Quotient percentile scores between 0-100 indicates confidence with the accuracy of
PDMS-2 scores.19 The calculated MDC95 (MDC=z*SEM*√2)16 is 3 standard score points
using the reported SEM. According to the PDMS-2 manual, test-retest reliability for the
PDMS-2 Gross Motor Quotient was measured as 0.84 for ages 2-11 months and 0.93 for
ages 12-17 months. The PDMS-2 is a valid measure for assessing motor abilities of a
child. The PDMS-2 possesses content validity, which indicates that the items on the
PDMS-2 provide a representative sample of the domains being measured. Criterion
validity has been established for the PDMS-2 and denotes that the PDMS-2 parallels
results from other tests that measure motor development in children.19,20 The PDMS-2
demonstrates construct validity as the test demonstrates the ability to differentiate across
age groups in a normative sample. The correlation coefficients across ages range between
0.80- 0.93 for the subtests. The ability of the PDMS-2 to differentiate between groups is
another facet of construct validity. Raw PDMS-2 scores and percentage scores can be
used to determine the effect of an intervention.19 The gross motor quotient and percentage
scores may be used to assess severity of developmental delay.18,19 The PDMS-2
demonstrates 98% diagnostic accuracy in distinguishing children with motor
disabilities.18 Psychometric data of the PDMS-2 specifically for children with DS were
not found in the literature. The high validity, reliability and diagnostic accuracy support

11
the use of the PDMS-2 to assess gross motor development. The PDMS-2 was utilized as a
diagnostic tool and outcome measure for this case report.
The PEDI was utilized as an outcome measure to assess changes at the levels of
“Activity” and “Participation.”21 The PEDI was designed to assess limitations in
functional activities and evaluate change over time in children between the ages of 6
months and 7.5 years and older children that are functioning at less than 7 years of age. It
is comprised of 3 domains: Functional Skills scale, Caregiver Assistance scale and
Modifications scale.21-24 The PEDI assesses items such as car transfers, indoor and
outdoor locomotion and the level of caregiver assistance or use of assistive devices. The
Functional Skills scale assesses ability to perform a task, the Caregiver Assistance scale
assesses performance and the Modifications scale accounts for the use of assistance and
assistive devices to support activities of daily living.21 The PEDI is typically completed
by the primary caregiver to assess their child’s performance of functional skills.25 The
PEDI has shown to be responsive to change in children with disabilities over a six month
period. Normative and scaled scores are available for the PEDI. Normative standard
scores are adjusted for age with the mean set at 50 and a standard deviation of 10 and
scaled scores are non-age adjusted scores from 0-100 with a score of 100 indicating that
the child is able to achieve all the items on the PEDI.23 The inter-rater reliability ICC for
the PEDI has been documented between 0.74-0.95.25 Values for inter-rater reliability are
greater for typically developing children, reported between 0.95-0.99.9,21,24 The PEDI
possesses construct validity as it is able to differentiate children with and without

12
disabilities. The PEDI has shown to be responsive to change.9,17,22,23 Effect size and
standard response means for the PEDI have been reported to be 0.8 in populations with
CP, 17 which demonstrates the responsiveness. A minimal clinically important difference
(MCID) of 11% on a 0-100 percent scale has been cited for the PEDI for inpatient
populations of children with CP.22

13
Table 1
Examination Data
BODY FUNCTION OR STRUCTURE IMPAIRMENTS Measurement Category
Test/Measure Used
Test/Measure Results
Gait Observation Wide base of support, requires two hand held assistance to take forward steps, hyperextension of 10° at knees was noted bilaterally during stance. Unable to take independent steps.
Balance GMFM-88 Item #56 “Standing: Maintains arms free, 20 seconds”
Stands independently and maintains standing, arms free for 1-2 seconds
PDMS-2 Stationary Item #20: “Stands on 1 foot with hands on hips for 3 seconds”
Patient requires two hand held assistance to stand on 1 foot with right/left foot
Range of Motion (ROM)
Observation Patient presents with no impairments in range of motion. Range of motion is excessive in trunk and extremities.
Muscle Tone Modified Ashworth Scale (MAS)
Patient was assessed to have low muscle tone in trunk and extremities. Patient does not demonstrate any signs of spasticity.
ACTIVITY LIMITATIONS Measurement Category
Test/Measure Used
Test/Measure Results
Walking Speed 10MWT Note: Scores are averages of 2 trials
One hand held assistance: 0.17 m/s
Two hand held assistance: 0.55 m/s
Delayed gross motor skills
GMFM-88 (A-E) A. Lying and Rolling – Raw Score 51/51; Percentage: 100% B. Sitting – Raw Score: 33/60; Percentage: 55%

14
C. Crawling and Kneeling – Raw Score: 32/42;
Percentage: 76% D. Standing – Raw Score: 18/39; Percentage: 46% E. Walking, Running and Jumping – Raw
score:13/72; Percentage: 18% Total GMFM-88 (Raw Percentage Scores divided by total number of dimensions, 5): Raw Percentage Score: 295 Total GMFM-88 Percentage: 59%
PDMS-2 Gross Motor
Stationary Subscale: 9th percentile; below average 11 month age equivalent Locomotion Subscale: <1 percentile; very poor 10 month age equivalent Object Manipulation Subscale: 1 percentile Standard score: 3 12 month age equivalent Total Gross Motor Subtest Total: 10 < 1 percentile PDMS-2 Gross Motor Quotient: 57; very poor
Patient’s functional mobility to access toys is limited.
FMS Walking distance 5 meters – Rating: C (Crawling) Walking distance 50 meters – Rating: C (Crawling) Walking distance 500 meters – Rating: N (Does not apply)
Patient’s functional mobility to access toys and keep up with her peers to participate in play activities are limited
PEDI Mobility – Raw Score: 26/65; Percentile: 40%
Modification Scale – Raw Score: 1/21 Percentile: 5%

15
Patient’s indoor/outdoor locomotion is limited to 150 feet with moderate assistance from the caregiver through two hand held assistance.
PARTICIPATION RESTRICTIONS Measurement Category
Test/Measure Used
Test/Measure Results
Patient’s functional mobility keep up with her peers to participate in play activities are limited
PEDI Caregiver Assistance – Raw Score: 11/35; Percentile: 31%
10MWT, 10 Meter Walk Test; FMS, Functional Mobility Scale, GMFM-88, Gross Motor Function Measure-88, PDMS-2, Peabody Developmental Motor Scales, second edition, Pediatric Evaluation of Disability Inventory, PEDI.

16
Chapter 4
Evaluation
Evaluation Summary
The patient was a pre-ambulatory 2 year old female that presented with delayed
gross motor skills as determined by the GMFM-88 and PDMS-2, muscle hypotonia as
measured by MAS and delayed cognition per parent report, which was consistent with
her medical diagnosis of translocation DS.
Diagnostic Impression
The patient presented with gross motor delays consistent with DS, which caused
restrictions in the levels of “Activity” and “Participation.”
Physical Therapy Guide Practice Pattern
Patient’s presentation fits practice pattern 5B, impaired neuromotor development.
G-Code/s
G8978 CK (57%) – Mobility: Walking + Moving Around; Modifier CK. The
modifier is based on the average PDMS-2 age equivalents divided by the patient’s age.

17
Chapter 5
Plan of Care – Goals and Interventions
Table 2
Evaluation and Plan of Care
PROBLEM PLAN OF CARE Short Term Goals (Anticipated Goals) (4 Weeks)
Long Term Goals (Expected Outcomes) (9 Weeks)
Planned Interventions Interventions are Direct or Procedural unless they are marked: (C) = Coordination of care intervention (E) = Educational intervention [HEP] = denotes the addition of exercise to patient’s home exercise program.
BODY FUNCTION OR STRUCTURE IMPAIRMENTS Gait
Patient will take 6 independent steps without support demonstrating a decreased base of support.
Patient will take 10 independent steps without support demonstrating a decreased base of support.
(E) Patient and parent instructed on decreasing hand held support from two hand held assistance to two hand held assistance and increasing walking practice opportunities. (C) Communicated with parent about speaking with physical therapist from to obtain a Kaye walker for patient. (C) Communicated need for reverse walker with clinical instructor.

18
Kaye walker was loaned to patient to improve independent mobility and increase walking practice at home Treadmill training on a pediatric treadmill to promote task specificity and overload principle to improve walking and over ground training (parameters listed below)
Balance Patient demonstrates limited balance in single and double leg stance. GMFM-88 #56 Stands independently and maintains standing, arms free for 1-2 seconds PDMS-2 Stationary #20 Patient requires two hand held assistance to stand on 1 foot with right/left foot
GMFM-88 #56 Stands independently and maintains standing, arms free for 10 seconds PDMS-2 Stationary #20 Patient will be able to stand on 1 foot with hands on hips for 1-2 seconds
Stands independently and maintains standing arms free for 20 seconds Patient will be able to stand on 1 foot with hands on hips for 3 seconds.
Standing at white board to draw using one arm to draw on white board and other arm for support Ascending and descending pediatric stairs progressing to utilizing 6 inch stairs (4 steps) with two hand held assistance, then one hand held assistance from therapist or parent Kicking a ball with one hand held assistance for a period of 5 minutes, 5 days per week progression to

19
kicking a ball with patient holding onto one finger from parent/student therapist [HEP]
ACTIVITY LIMITATIONS Walking Speed Measured by 10MWT Note: Scores are the average of 2 trials
One hand held assistance 0.17 m/s to 0.18 m/s
One hand held assistance 0.18m/s to 0.21 m/s
Treadmill training Speed parameters ranged from 0.2 to 0.3 mph, progressed to using a 4 inch incline, replacing rails with tabletop surface in front of treadmill and 1 pound ankle weights bilaterally. Goal of progressing time to tolerance of 30 minutes of treadmill training. Over-ground walking with hula hoop and later a reverse Kaye walker with swivel wheels locked and unlocked were used when patient was not interested in engaging in treadmill training activities to promote task-specificity and work on walking practice (E) Walking with walker Walking 10 minutes per day, 5 times a week and progress by increasing the time spent walking each session/day up to 30
Two hand held assistance 0.55 m/s to 0.63 m/s
Two hand held assistance 0.63 m/s to 0.70 m/s

20
minutes per day. [HEP]
Gross motor delays were noted using the GMFM-88 and PDMS-2. Improvements in the GMFM-88 by 15% (MDC95) and PDMS-2 by 3 points (MDC95) through attainment of long-term goals will demonstrate gross motor improvements. GMFM-88 # 59 Patient does not initiate standing from sitting on a small bench
Patient initiates will be able to initiate standing from a small bench
Patient will be able to attain standing from without using arms
Crossing midline and overhead to reach toys in sitting position without back support [HEP] Sit to stand from small bench while reaching for ball repetitions 5 times per set, with goal to attain 10 repetitions per set. Sit to stand exercise progressed by reducing assistance from one hand held assistance to stand by assistance. The exercise was further progressed by decreasing bench height from 10 inches to 7 inches [HEP]
GMFM-88 # 69 Patient initiates taking a forward step but results in a loss of balance
Patient will be able to walk 6 forward steps, independently
Patient will be able to walk10 forward steps, independently
Over-ground walking and treadmill training, which are detailed in above sections

21
PDMS-2 Object Manipulation #2 Patient attempts to catch a ball that is rolled to her. She catches the ball with her arms while sitting with her legs spread out in front of her but loses balance
Patient is able to catch a ball that is rolled from to her by corralling a ball with her arms while sitting with legs spread apart without a loss of balance in 1/3 trials
Patient is able to catch a ball that is rolled from 3 feet away by corralling a ball with her arms while sitting with legs spread apart without a loss of balance in 3 out of 3 trials
Weight shifts (forward, back and side to side) on a large Swiss ball (SB) with parent/student physical therapist (SPT) stabilizing the pelvis to improve trunk control [HEP]
Patient’s functional mobility to access toys and keep up with her peers to participate in play activities are limited Patient’s preferred method of functional mobility is crawling. Patient can crawl up to a distance of 50 meters (150 feet) Measured by the FMS
Patient will be able to walk 25 meters (75 feet) with the use of a reverse Kaye walker
Patient will be able to walk 50 meters (150 feet) with the use of a reverse Kaye walker
Over ground walking practice with reverse Kaye walker, Treadmill, and functional strength training activities detailed in above sections will lead to improvements in functional mobility
Patient’s functional mobility to access toys and keep up with her peers to participate in play activities
Patient will be able to take 6 independent steps between furniture or mom and dad to access toys
Patient will be able to take 10 independent steps to access toys and participate in play activities with peers
Functional strength training activities including over-ground walking with support, which will be reduced progressively from two hand held to unstable hula-hoop and

22
are limited Patient’s indoor/outdoor locomotion is limited to 150 feet with moderate assistance from the caregiver through two hand held assistance. Measured by the Mobility and Modification scale of PEDI
Patient was able to walk 150 feet indoor/outdoor with one hand held assistance 50% of the time and two hand held assistance for the remaining 50%. Modification scale: No expected change short term
Patient was able to walk 150 feet indoor/outdoor with a reverse Kaye walker and independent of caregiver assistance. +11% change in Modification Scale (MCID95=11%)
treadmill training. Treadmill training on a pediatric treadmill to promote task specificity and overload principle to improve walking (parameters listed above)
PARTICIPATION RESTRICTIONS Patient’s functional mobility keep up with her peers to participate in play activities are limited Measured by the Caregiver Assistance scale of the PEDI
+ 5.5% change in Caregiver Assistance scale (MCID95=11%)
+11% change in Caregiver Assistance scale
Treadmill, over-ground walking with varied support (hand held assistance, hula hoop and reverse Kaye walker) and functional strength training activities detailed in above sections will lead to improvement in Caregiver Assistance scale. (E) Patient will demonstrate assisted independence on a home exercise program [HEP]
10MWT, 10 Meter Walk Test; FMS, Functional Mobility Scale, GMFM-88, Gross Motor Function Measure-88, PDMS-2, Peabody Developmental Motor Scales, second edition, Pediatric Evaluation of Disability Inventory, PEDI, MDC95 minimal detectable change

23
95% confidence interval, MCID95, minimal clinically important difference 95% confidence interval.

24
Prognostic Considerations
Positive prognostic indicators included ongoing early intervention services that
began at the age of 2 months and strong social support. The literature suggested that
incorporating early intervention programs assist in the development of a child with a
genetic disorder.2 Early intervention programs have been shown to encourage more
efficient walking in children with health problems and moderate to severe motor
impairments.6 Implementation of early intervention programs in children with DS have
been demonstrated to be a critical component to yield positive changes in motor and
cognitive development.5,6,13 Critical periods of brain development during the early years
of life warranted the implementation of early intervention programs to impart plastic
changes to a developing child’s brain.26 The patient had an ideal social and living
environment. She had strong social support from her mother, father and paternal
grandparents. Treatment plans that included goal directed training, functional training and
home exercise programs have been demonstrated to improve function at the “Activity”
level have been studied most in children with CP.27 Negative prognostic indicators that
impacted mental and motor development in children with DS included comorbidities,
such as heart, gastrointestinal, central nervous system (CNS) and pulmonary disease,
hospitalizations and use of prescription medications.28 This patient did not have any
negative prognostic indicators. Children with DS require additional time and practice to
learn movements, especially as the complexity of movements was increased. Children
with DS acquire gross motor skills at twice the mean age of typically developing

25
children.6,13 One study found the probability of walking in a child with DS by 30 months
of age was 74% and probability of walking by 36 months is 92%.6 The presence of
multiple positive prognostic indicators created an expectation that the patient would
achieve therapy goals resulting in improved gross motor skills and independent walking.
Plan of Care- Interventions
See Table 2.
Overall Approach
The treatment approach for the patient was based on functional strength training,
family-centered goals, treadmill training and intensive, task-specific training through
application of the overload principle. The patient was provided a HEP to encourage
improvements in functional mobility through the overload principle. Family-centered
goals are important and should be incorporated into early intervention services.29
Incorporation of family centered goals leads to improved collaboration between therapist
and parent of the child.27,29 Expectations of a parent may influence the child’s ability to
perform self-care tasks and additional attention from the parent may yield increased
motivation in the child to perform a task.24 This further highlights the need to incorporate
the family’s goals as the family is more likely to incorporate goals into the child’s
routine. The uses of functional training goals and home exercise program have been
shown to improve function at the level of “Activity” in children with CP.27 Specific
functional strength training data on children with DS was not found in a review of the
literature. Reporting on children with CP is the best available evidence found to comment

26
on the use of functional training. Treadmill training was used as a task specific, intensive
intervention and has been shown to promote earlier walking in young pre-ambulatory
children.5,8 Treadmill training offers pre-ambulatory children with DS the opportunity to
practice walking, improve balance, improve lower extremity strength and stimulate the
CNS connections necessary for the development and emergence of independent walking.8
The patient’s goals were achieved through physical therapy visits and parent assisted
independence in the HEP.
PICO Question
For a 2 year old female patient with DS (P) is a combined functional
strengthening and treadmill training program a more effective treatment compared to a
treadmill training only (C) to improve mobility and walking function (O)?
The first study of interest that addressed this PICO question was a single-blinded,
randomized controlled trial with pre-training and post-training assessments (Level of
evidence: 1b; PEDro Score 6/10).30 Participants in the study were ten children, 5 males
and 5 females, with a diagnosis of cerebral palsy with GMFCS level I-III. Five children
were randomly allocated to the experimental group and another five children were
randomly allocated to the control group. The mean age for the participants in the study
was 6.5 years of age. The experimental group underwent strengthening exercises of the
lower extremities using task-oriented training and practicing functional activities. Task
oriented training included walking activities, walking up and down ramps, stepping onto
blocks, standing balance activities, standing up from a chair, ability to perform a single

27
leg stance and kicking a ball. The control group received conventional physical therapy
with goals to improve walking and balance. The experimental group in this study yielded
statistically significant change scores compared to the control group at 5 weeks post-
training period in the Timed up and Go (p=0.017) and the GMFM dimension D: Standing
(p=0.009), and dimension E: Walking, Running and Jumping (p=0.009).30 Quality
intervention studies for strengthening in young children with DS was lacking in the
literature. As a result, this intervention study of older children with CP was utilized as the
best available evidence to support interventions used for this case report.
The second study of interest that addressed this PICO question was a randomized
controlled trial with pre and post training assessments (Level of evidence: 1b, PEDro
Score 5/10).8 Participants in the study were thirty pre-ambulatory children with a
diagnosis of DS with a mean age of 307.4 days (10.1 months) at entry to the study. The
control group, which received pediatric physical therapy services twice a week and an
experimental group, which included treadmill training and pediatric physical therapy
services twice a week. The children in the experimental group walked independently 101
days sooner when compared to the children in the control group (p=0.02) demonstrating
statistically significant results in two of the selected items from the Bayley Scales of
Infant Development, Second Edition (BSID-II), which included walking with help
(p=0.03) and walking independently (p=0.02). Independent walking was achieved at a
mean age of 21.9 months across both groups. Children in the experimental group walked

28
on average at 19.9 months, whereas the children in the control group on average walked
at 23.9 months.8
It is difficult to compare CP and DS populations to address the PICO question.
Several distinctions in development of motor skill acquisition exist between children with
DS and children with CP. Unfortunately, limited evidence for children with DS and
interventions warrants exploration of interventions in other populations with
developmental delays. Motor delays are present in populations of children with CP and
DS and motor milestone attainment in high-functioning children with CP have been
shown to be similar to children with DS.31 The limited evidence for young children with
DS and the moderate evidence for the interventions presented in this PICO question led
to a decision to incorporate a combined functional strength training and treadmill training
into the plan of care for this patient.
29
Chapter 6
Outcomes
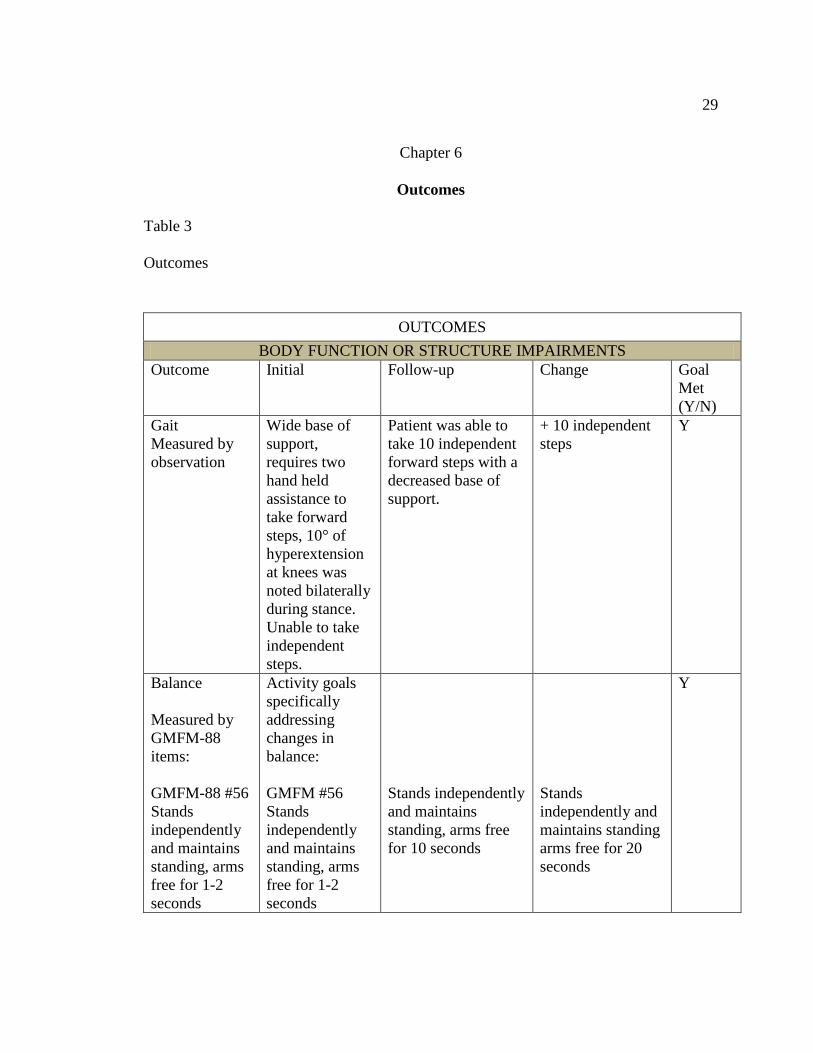
Table 3
Outcomes
OUTCOMES BODY FUNCTION OR STRUCTURE IMPAIRMENTS
Outcome Initial Follow-up Change Goal Met (Y/N)
Gait Measured by observation
Wide base of support, requires two hand held assistance to take forward steps, 10° of hyperextension at knees was noted bilaterally during stance. Unable to take independent steps.
Patient was able to take 10 independent forward steps with a decreased base of support.
+ 10 independent steps
Y
Balance Measured by GMFM-88 items: GMFM-88 #56 Stands independently and maintains standing, arms free for 1-2 seconds
Activity goals specifically addressing changes in balance: GMFM #56 Stands independently and maintains standing, arms free for 1-2 seconds
Stands independently and maintains standing, arms free for 10 seconds
Stands independently and maintains standing arms free for 20 seconds
Y

30
PDMS-2 Stationary #20 Patient requires two hand held assistance to stand on 1 foot with right/left foot
PDMS-2 Stationary #20 Patient requires two hand held assistance to stand on 1 foot with right/left foot
Patient was able to stand on 1 foot (left/right) with hands on hips for 1 second
Patient was able to stand on 1 foot with hands on hips for 3 seconds on the right and 2 seconds on the left balance in 3 out of 3 trials
ACTIVITY LIMITATIONS Outcome Initial Follow-up Change Goal
Met (Y/N)
10MWT Ave of 2 trials (MDC95=107% change)
One hand held assistance 60.5 seconds; 0.17 m/s Two hand held assistance 18 seconds ; 0.55 m/s
One hand held assistance 29.35 seconds; 0.34m/s Two hand held assistance 14.8 seconds; 0.68 m/s With reverse Kaye Walker: 15.47 seconds; 0.64 m/s
- 0.17m/s - 0.13 m/s Change with reverse walker cannot be assessed as 10MWT with Kaye reverse walker was only assessed at discharge
N
GMFM-88 Total Score (MDC95=15%)
59% Activity goals specifically addressing changes in GMFM-88 Score: GMFM # 59 Patient does not
72% Patient was able to initiate standing from
+13% Patient was able to attain standing
N

31
initiate standing from sitting on a small bench GMFM # 69 Patient initiates taking a forward step but results in a loss of balance
a small bench Patient was able to walk 3 forward steps, independently
from without using arms Patient was able to walk10 forward steps, independently
PDMS-2 Gross Motor Section (MDC95 = 3 points)
Gross motor subtest total: 10 < 1 percentile Gross Motor Quotient 57; very poor Activity goals specifically addressing changes in the PDMS-2 Score: PDMS-2 Object Manipulation #2 Patient is attempts to catch a ball that is rolled from to her by corralling a ball with her arms while sitting with legs spread apart but loses balance
Gross motor subtest total: 18 4th percentile Gross Motor Quotient 74; poor Patient was able to catch a ball that is rolled from to her by corralling a ball with her arms while sitting with legs spread apart without a loss of balance in 1/3 trials
+8 points Gross Motor Subtest + 17 points Gross Motor Quotient Patient was able to catch a ball that is rolled from 3 feet away by corralling a ball with her arms while sitting with legs spread apart without a loss of balance in 3 out of 3 trials
Y

32
Stationary: 9th percentile, Standard score: 6; below average 11 month age equivalent
Stationary: 63th percentile, Standard score: 11; average 33 month age equivalent
+54% + 22 month age equivalent
Locomotion: <1 percentile, Standard score: 1; very poor 8 month age equivalent
Locomotion: <1 percentile, Standard score: 1; very poor 9 month age equivalent
No change in percentile +1 month age equivalent
Object Manipulation: 1 percentile Standard score: 3 12 month age equivalent
Object Manipulation: 1 percentile Standard score: 3 12 month age equivalent
No change
FMS (No MDC/MCID reported. Statistically significant mean change in FMS ratings are cited as 1.8 for 5 meters, 1 for 50 meters and1.1 for 500 meters.)
Activity goals contributing to increase in FMS Rating: Patient’s preferred method of functional mobility is crawling. Patient can crawl up to a distance of 50 meters (150 feet)
Patient will be able to walk 25 meters (75 feet) with the use of a reverse Walking Distance 5
Kaye walker Patient will be able to walk 50 meters (150 feet) with the use of a reverse Kaye walker Walking Distance
Y

33
Walking Distance 5 meters – Rating: C (crawling)
meters – Rating: C (crawling)
5 meters – Rating: 2 (Uses walker or frame: Without help from another person )
Walking Distance 50 meters – Rating: C (crawling)
Walking Distance 50 meters – Rating: C (crawling)
Walking Distance 50 meters – Rating: 2 (Uses walker or frame: Without help from another person )
Walking Distance 500 meters – Rating: N (Not applicable)
Walking Distance 500 meters – Rating: N (Not applicable)
Walking Distance 500 meters – Rating: N (Not applicable)
Pediatric Evaluation of Disability Inventory (PEDI) (MCID95=11%)
Mobility Raw Score:26/65 Percentile: 40% Activity goals contributing to increase in PEDI Mobility and Modification Score: Patient’s functional mobility to access toys and
Raw Score:40/65 Percentile: 62% Patient was able to take 6 steps between furniture or mom and dad to access toys
+14 points (+22%) Patient was able to take 10 independent steps to access toys and
Y

34
10MWT, 10 Meter Walk Test; FMS, Functional Mobility Scale, GMFM-88, Gross Motor Function Measure-88, PDMS-2, Peabody Developmental Motor Scales, second edition, Pediatric Evaluation of Disability Inventory, PEDI, MDC95 minimal detectable change 95% confidence interval, MCID95, minimal clinically important difference 95% confidence interval.
keep up with her peers to participate in play activities are limited Patient’s indoor/outdoor locomotion is limited to 150 feet with moderate assistance from the caregiver through two hand held assistance.
Patient was able to walk 150 feet indoor/outdoor with one hand held assistance 50% of the time and two hand held assistance for the remaining 50%.
participate in play activities with peers Patient was able to walk 150 feet indoor/outdoor with a reverse Kaye walker and independent of caregiver assistance.
Modification Raw Score:1/21 Percentile: 5%
Raw Score:5/21 Percentile: 24%
+ 4 points (+19%)
Y
PARTICIPATION RESTRICTIONS Outcome Initial Follow-up
Change Goal
Met (Y/N)
Pediatric Evaluation of Disability Inventory (PEDI) (MCID95=11%)
Caregiver Assistance Raw Score: 11/35 Percentile: 31%
Raw Score:19/35 Percentile: 54%
+ 8 points (+23%)
Y

35
Discharge Statement
Patient received an evaluation and 10 visits of physical therapy intervention over
the course of 9 weeks. The original plan of care involved a frequency of visits of one time
per week for 8 weeks. The patient missed 3 consecutive appointments toward the
beginning of plan of care due to patient illness and a scheduled family vacation.
Frequency of visits was changed from one time per week to two times per week in week
6 for visits 4 through 10 and an additional week was added to enable additional treatment
and outcome measurements prior to discharge. The patient met 7 out of 9 goals set. The
patient met goals in improved gait and gross motor function as measured by the GMFM-
88 and PDMS-2. The patient also made improvements at the “Participation” level as
measured by the PEDI. The patient was able to take up to 10 independent steps at the
time of discharge and was able to walk up to 25 continuous minutes while walking with a
reverse Kaye walker with the wheels unlocked. She was loaned a Kaye walker for use
during the period of care. The patient had a supportive and motivated mother, father and
paternal grandparents. The patient was discharged to current living situation with a HEP
after 10 sessions of physical therapy intervention over 9 weeks.
G-Code/s at discharge:
G8978 CJ (31%) – Mobility: Walking + Moving Around; Modifier CJ. The
modifier is based on the average PDMS-2 age equivalents divided by the patient’s age.

36
Chapter 7
Discussion
The patient was able to take ten independent steps by discharge. The parent’s
primary goal for the patient was to achieve independent ambulation. While attainment of
ten independent steps does not equate functional independent ambulation, the patient’s
ability to complete ten independent steps helped improve her functional mobility, access
to toys and peers. Experience working with pediatric patients in a physical therapy
context is recommended for treating pre-ambulatory children DS presenting with gross
motor delays. Addressing the parent’s goal for the child to walk was important for the
plan of care for the patient as research supported the use of family-centered goals to
improve motor skills.
Combining a functional strength training exercises in conjunction with treadmill
training was a good choice for this patient. Incorporating functional strength training
exercises was an important component that could be practiced outside of the physical
therapy treatment setting especially since a pediatric treadmill for use at home was not
available during the intervention period. The patient’s and parent compliance to the HEP
promoted positive outcomes. Maturity of the patient during the treatment period may
have positively influenced outcomes measured. If I had the opportunity to treat this
patient again, I would utilize a similar approach. However, I would have treated the
patient for additional treatment sessions. Nine weeks was a relatively short intervention
period when considering the patient missed three scheduled visits. The frequency of visits

37
was changed from once a week to two times per week to accommodate for the missed
visits in week 6. In addition, the length of treatment was altered from eight weeks to nine
weeks to accommodate for additional treatment time and time needed to assess outcome
measurements at discharge. Ideally, I would have preferred to treat this patient for a
longer duration to help the patient continue to improve independent ambulation. If I
would treat this patient again, I would incorporate the use of a reverse Kaye walker
sooner in the treatment period, incorporate in-home pediatric treadmill training as part of
the HEP and progressively increase the one pound bilateral ankle weights during
treadmill walking to increase frequency of intensive, task-specific practice. Additional
pediatric experience in the context of physical therapy session would be helpful in my
treatment approach if I had the opportunity to treat this patient again. Additional
experience working with the pediatric population would improve my ability to attend to
the child’s cues of fatigue, disinterest and/or frustration. At the start of care, I struggled to
instruct the patient to focus on the activity I wanted her to perform but I learned that
children are motivated by interest and fun. Learning the activities and toys the she
enjoyed, such as bubbles and playing with a ball, and understanding when to take a break
or redirect her to another activity became a key to making the treatment successful.
Interestingly, a greater amount of participation in functional strengthening, over-ground
walking and treadmill training occurred when the patient’s father was present in
comparison when the patient’s mother was present during the session. There was not an
occasion when both parents were present for the treatment session. The father was more

38
engaged with the child during treatment sessions, which may account for increased
participation of the patient for visits when the father was present during sessions.
Incorporation of gait analysis software could have been used to help assess the
quality of gait and provide quantitative data to supplement qualitative descriptions of gait
in the “Body Structure and Function” level of the ICF model. For the 10MWT, the time
was averaged across 2 trials instead of the three trials as typically cited in the literature
because the child was unwilling to perform a third trial. Data at discharge was collected
for the 10MWT using a reverse Kaye walker but unfortunately data was not collected
during the evaluation as it was not expected that the patient would be loaned a temporary
reverse Kaye walker. The goal of increasing walking speed as measured by the 10MWT
and increasing gross motor function measured by the GMFM-88 were goals that were not
met; however, the patient did achieve 7 of the remaining 9 goals. The patient was able to
complete the 10MWT with hand held assistance. The patient improved the 10MWT time
by completing the test in half the time at discharge compared to the initial evaluation but
did not reach the established MDC for the 10MWT in populations with CP.
Unfortunately, the MDC for populations with CP is the only available evidence found in
the literature as data for this outcome measure is lacking in young populations with DS.
The use of the reverse Kaye walker is only represented in the PEDI and pre and post data
collection for all other outcome measures used in this study were performed without the
walker. The use of the reverse Kaye walker is reflected in the Modifications Assistance
Scale of the PEDI reflecting a 19% increase, which reflects an increased need in

39
assistance to complete tasks. However, it is important to note that the scores in the
Caregiver Assistance scale reflects that the child was able to travel a greater distance
independently with the use of an assistive device compared to the initial assessment,
which was performed without an assistive device. Changes in functional ambulation as
measured by the FMS illustrate this change in functional mobility through a change in the
child’s rating from the ability of the child to crawl distances up to 50 meters to the ability
of the child to walk distances up to 50 meters with the use of a reverse Kaye walker.
The patient presented with typical features of DS, such as low muscle tone,
delayed gross motor skills and delayed cognition; however, the patient did not present
with other common comorbidities that typically accompany a diagnosis of DS, such as a
heart condition. The patient had a heart murmur at birth that resolved within the first year
and did not receive any treatment. The use of the GMFM-88 as a prognostic tool and
PDMS-2 as a diagnostic tool were appropriate for use in the DS population and
ultimately for this patient to determine the presence of gross motor delays and to predict
changes over time. The use of the PEDI provided further insight into the child’s
functional mobility and level of caregiver assistance needed to perform activities of daily
living. The specific interventions used for this patient may not be appropriate for broad
application. Better evidence specific to children with DS may have improved my ability
to treat this patient as the evidence available for children with DS and interventions is
limited. Additional research is warranted to determine effective interventions in children
with DS.

40
References
1. Bornstein E, Lenchner E, Donnenfeld A, et al. Complete trisomy 21 vs
translocation Down syndrome: a comparison of modes of ascertainment. Am J
Obstet Gynecol. 2010; 203:e391- e395.
2. Pastva M, Corwin EJ, Morin K. Down syndrome with an unusual etiology: case
report and review. J Am Acad Nurse Pract. 2004; 16:244-250.
3. Lloyd M, Burghardt A, Ulrich DA, Angulo-Barroso R. Physical activity and
walking onset in infants with Down syndrome. Adapt Phys Activ Q. 2010; 27:1-
16.
4. Hartway S. A parent's guide to the genetics of Down syndrome. Adv Neonatal
Care. 2009; 9:27-30.
5. Ulrich DA, Lloyd MC, Tiernan CW, Looper JE, Angulo-Barroso RM. Effects of
intensity of treadmill training on developmental outcomes and stepping in infants
with Down syndrome: a randomized trial. Phys Ther. 2008; 88:114-122.
6. Palisano RJ, Walter SD, Russell DJ, et al. Gross motor function of children with
Down syndrome: creation of Motor Growth Curves. Arch Phys Med Rehabil.
2001; 82:494-500.
7. Rahman SAA, Shaheen A. Efficacy of weight bearing exercises on balance in
children with Down syndrome. Egypt J Neurol Psychiat Neurosurg. 2010; 47:37-
46.

41
8. Ulrich DA, Ulrich BD, Angulo-Kinzler RM, Yun J. Treadmill training of infants
with Down syndrome: evidence-based developmental outcomes. Pediatrics. 2001;
108:E84.
9. Majnemer A, ed. Measures for Children with Developmental Disabilties: An ICF-
CY Approach. London, UK: Mac Keith Press; 2012.
10. Thompson P, Beath T, Bell J, et al. Test-retest reliability of the 10-Metre Fast
Walk Test and 6-Minute Walk Test in ambulatory school-aged children with
cerebral palsy. Dev Med Child Neurol. 2008; 50:370-376.
11. Graham HK, Harvey A, Rodda J, Nattrass GR, Pirpiris M. The Functional
Mobility Scale (FMS). J Pediatr Orthop. 2004; 24:514-520.
12. Harvey A, Robin J, Morris ME, Graham HK, Baker R. A systematic review of
measures of activity limitation for children with cerebral palsy. Dev Med Child
Neurol. 2008; 50:190-198.
13. Russell D, Palisano R, Walter S, et al. Evaluating motor function in children with
Down syndrome: validity of the GMFM. Dev Med Child Neurol. 1998; 40:693-
701.
14. Bodkin AW, Robinson C, Perales FP. Reliability and validity of the gross motor
function classification system for cerebral palsy. Pediatr Phys Ther. 2003;
15:247-252.

42
15. Russell DJ, Rosenbaum PL, Wright M, Avery LM. Gross Motor Function
Measure (GMFM-66 & GMFM-88) User's Manual. 2nd ed. Ontario, Canada: Mac
Keith Press; 2013.
16. Portney LG, Watkins MP. Foundations of Clinical Research: Applications to
Practice. 2nd ed. Upper Saddle River, NJ: Prentice Hall Health; 2000.
17. Vos-Vromans DC, Ketelaar M, Gorter JW. Responsiveness of evaluative
measures for children with cerebral palsy: the Gross Motor Function Measure and
the Pediatric Evaluation of Disability Inventory. Disabil Rehabil. 2005; 27:1245-
1252.
18. Wang HH, Liao HF, Hsieh CL. Reliability, sensitivity to change, and
responsiveness of the Peabody Developmental Motor Scales-second edition for
children with cerebral palsy. Phys Ther. 2006; 86:1351-1359.
19. Folio MR, Fewell RR. Peabody Developmental Motor Scales: Examiner's
Manual. 2nd ed. San Antonio, TX: Pearson; 2000.
20. Palisano RJ, Kolobe TH, Haley SM, Lowes LP, Jones SL. Validity of the
Peabody Developmental Gross Motor Scale as an evaluative measure of infants
receiving physical therapy. Phys Ther. 1995;75: 939-948.
21. Østensjø S, Bjorbækmo W, Carlberg EB, Vøllestad NK. Assessment of everyday
functioning in young children with disabilities: an ICF-based analysis of concepts
and content of the Pediatric Evaluation of Disability Inventory (PEDI). Disabil
Rehabil. 2006; 28:489-504.

43
22. Iyer LV, Haley SM, Watkins MP, Dumas HM. Establishing minimal clinically
important differences for scores on the Pediatric Evaluation of Disability
Inventory for inpatient rehabilitation. Phys Ther. 2003; 83:888-898.
23. Haley SM, Coster W, Ludlow LH, Haltiwanger JT, Andrellos PJ. Pediatric
Evaluation of Disability Inventory (PEDI). Version 1.0: Development,
Standardization and Administration Manual. Boston, MA: New England Medical
Center Hospitals Inc; 1992.
24. Berg M, Jahnsen R, Froslie KF, Hussain A. Reliability of the Pediatric Evaluation
of Disability Inventory (PEDI). Phys Occupational Ther Pediatr. 2004; 24:61-77.
25. Nichols DS, Case-Smith J. Reliability and Validity of the Pediatric Evaluation of
Disability Inventory. Pediatr Phys Ther. 1996; 8:15-24.
26. Hadders-Algra M. Challenges and limitations in early intervention. Dev Med
Child Neurol. 2011; 53:52-55.
27. Novak I, McIntyre S, Morgan C, et al. A systematic review of interventions for
children with cerebral palsy: state of the evidence. Dev Med Child Neurol. 2013;
55:885-910.
28. van Trotsenburg AS, Heymans HS, Tijssen JG, de Vijlder JJ, Vulsma T.
Comorbidity, hospitalization, and medication use and their influence on mental
and motor development of young infants with Down syndrome. Pediatrics. 2006;
118:1633-1639.

44
29. Dirks T, Hadders-Algra M. The role of the family in intervention of infants at
high risk of cerebral palsy: a systematic analysis. Dev Med Child Neurol. 2011;
53:62-67.
30. Salem Y, Godwin EM. Effects of task-oriented training on mobility function in
children with cerebral palsy. NeuroRehabilitation. 2009; 24:307-313.
31. Horovitz M, Matson JL. Developmental milestones in toddlers with atypical
development. Res Dev Disabil. 2011; 32:2278-2282.
Recommended

















