Blood Cells, Molecules and Diseases 53 (2014) 105–109
Contents lists available at ScienceDirect
Blood Cells, Molecules and Diseases
j ourna l homepage: www.e lsev ie r .com/ locate /bcmd
Outcome of early-treated type III Gaucher disease patients
Ni-Chung Lee a, Yin-Hsiu Chien a, Siew-Lee Wong b, Jiunn-Ming Sheen c, Fuu-Jen Tsai d, Shinn-Forng Peng e,Joseph Hang Leung f, Mei-Chyn Chao g, Chia-Tung Shun h, Wuh-Liang Hwu a,⁎a Department of Medical Genetics and Pediatrics, National Taiwan University Hospital and National Taiwan University College of Medicine, Taipei, Taiwanb Department of Pediatrics, Ditmanson Medical Foundation Chia-Yi Christian Hospital, Chia-Yi, Taiwanc Department of Pediatrics, Kaohsiung Chang Gung Memorial Hospital and Chang Gung University College of Medicine, Kaohsiung, Taiwand Department of Pediatrics and Medical Genetics, China Medical University Hospital, Taichung, Taiwane Department of Radiology, National Taiwan University Hospital and National Taiwan University College of Medicine, Taipei, Taiwanf Department of Radiology, Ditmanson Medical Foundation Chia-Yi Christian Hospital, Chia-Yi, Taiwang Department of Pediatrics, Kaohsiung Medical University Hospital and Department of Medical Genetics, Kaohsiung Medical University College of Medicine, Kaohsiung, Taiwanh Department of Pathology, National Taiwan University Hospital and National Taiwan University College of Medicine, Taipei, Taiwan
Abbreviations: GD, Gaucher disease; GBA, acid β-glument therapy.⁎ Corresponding author at: Department of Pediatrics
Taiwan University Hospital, 7 Chung-Shan South Road, T23314518.
E-mail address: [email protected] (W.-L. Hwu).
http://dx.doi.org/10.1016/j.bcmd.2014.05.0071079-9796 © 2014 Elsevier Inc. All rights reserved.
a b s t r a c t
a r t i c l e i n f oArticle history:Submitted 13 December 2013Revised 6 February 2014Accepted 14 May 2014Available online 28 June 2014
Communicated by: Ari Zimran
Keywords:Type IIIB Gaucher diseaseNeuropathicp.L444P mutationEnzyme replacement therapyLymphadenopathyMental retardation
Recombinant human acid β-glucosidase GBA (rhGBA) infusion is an effective therapy for non-neuropathic(type I) Gaucher disease (GD), but its effect on subacute neuropathic (type III) GD is still controversial. Themost common genotype for type III GD is homozygous c.1448TNC (p.L444P) mutation, and in this study, wetreated seven such patients starting from an early age (median 2.1 years; range 1–2.9 years). Before the startof treatment, all patients presented hepatosplenomegaly, anemia, and thrombocytopenia, but with no neurolog-ical signs. Normalization of hemoglobin levels and platelet numbers was achieved in all patients in one year.However, after a median treatment period of 7.6 years (2.2–12.0 years), two patients developed horizontalgazepalsy, onehad seizures, four demonstratedmental retardation, andfive showedkyphosis.Moreover, lymph-adenopathy in the neck, thorax, or abdomenwas observed in four patients. Therefore, the progression of neuro-logical symptoms in these patients probably reflected the neurologic natural history of type III GD. Residualsomatic symptoms, including kyphosis and lymphadenopathy, may be more common than what we thought.An additional treatment will be necessary to improve the outcome of type III GD.
© 2014 Elsevier Inc. All rights reserved.
Introduction
Gaucher disease (GD) is a sphingolipid storage disease, resultingfrom a deficiency in β-glucocerebrosidase (EC 3.2.1.45, acid β-glucosidase, GBA) activity [1]. A deficiency in GBA leads to accumulationof glucocerebroside inmacrophages (Gaucher cell) in the bonemarrow,liver, spleen, and brain. GD can be classified into 3 clinical types: type I,or the non-neuropathic form (MIM #230800); type II or the acute neu-ropathic form(MIM#230900); and type III, or the subacute neuropathicform (MIM #231000) [2]. Patients with type I GD usually manifesthepatosplenomegaly with or without bone deformity/crisis duringadulthood. Enzyme replacement therapy (ERT) with recombinant
cosidase; ERT, enzyme replace-
and Medical Genetics, Nationalaipei 100, Taiwan. Fax: +886 2
human GBA (rhGBA) is an effective treatment for type I GD, which re-duces hepatosplenomegaly, increases hemoglobin levels and plateletcount, and increases bone mineral density [3]. Patients with type II GDtypically exhibit neurodegeneration and hepatosplenomegaly beforeone year of age. ERT does not prevent neurodegeneration [4], andmost type II GD patients die before early childhood.
Type III GD was originally reported from the province ofNorrbotten in Sweden. At that time these patients exhibited bothvisceral and neurological manifestations from childhood to deathwhich commonly occur before they reach adulthood [5], but nowthey respond to ERT with increased well-being [6]. The causativeGBA gene mutation is c.1448TNC (p.L444P) [7]. Type III GD patientswith myoclonic epilepsy and other GBA gene mutations were also re-ported [8]. The p.L444P mutation is the predominant mutation intype III GD [9–11]. Patients with homozygous p.L444P mutation fre-quently manifested severe systemic involvements but only mildneurological abnormalities including supranuclear horizontal gazepalsy and/or other eye symptoms, mental retardation, and seizures.These patients have also been classified as having type IIIB GD [12],

106 N.-C. Lee et al. / Blood Cells, Molecules and Diseases 53 (2014) 105–109
as a means to differentiate them from the earlier recognized type IIIpatients (now defined as type IIIA) and patients with progressiveheart valve calcification (type IIIC) [13].
Although rhGBA infusion is an effective therapy for type I GD,effects of ERT on type III GD patients were variable. The EuropeanTask Force for Neuronopathic GD has reviewed the largest cohort(55 patients) of type III GD (40 with homozygous p.L444P mutation)[14]. However, therewas considerable variation in the dose of ERT, aswell as an uneven distribution of risk factors including age, genotype,and splenectomy.
In this study, we described seven type III GD patients who had ahomogeneous genetic background (homozygous p.L444P mutation).We treated these patients from an early age but found that their neuro-logical symptoms developed gradually. Residual somatic symptoms,including kyphosis and lymphadenopathy, are also common.
Methods
GBA activity was measured by 4-methylunbellyferal substrates, aspreviously described [15]. Genotyping was performed as described inour previous publication [9]. A total of seven GD patients who werehomozygous for the p.L444P mutation were analyzed in this study(Table 1). Patient 2 was born prematurely at gestational age 29 weekswith a birth weight of 1340 g. The median age of the seven patients atdiagnosis was 1.9 years and the median age at the start of ERT withCerezyme® (Imiglucerase) was 2.1 years (Table 1). The dose of ERTused was 60 U/kg/2 weeks, with the exception of patient 2, whosedosage was increased to 120 U/kg/2 weeks when lymphadenopathywas found. The median treatment period was 7.6 years. Follow-up ex-aminations of these patients were performed according to the recom-mendations from the Gaucher Registry, including regular studies forhemogram, chitotriosidase activity, CCL18 levels, the skeletal system,sizes of the visceral organs, andmentality. The degree of thoracic kypho-sis was estimated by the traditional Cobb angle measured on lateralspine radiographs, and the definition of kyphosis was an angle ≧45°.An intelligence quotient (IQ) was obtained by using theWechsler Intel-ligence Scale for Children. Data are presented as the means ± standarddeviations. Statistical analyseswere performed using the SPSS statisticalpackage, version 11.5. The Wilcoxon signed rank test was applied for
Table 1Clinical characteristics of p.L444P/p.L444P Gaucher disease patients.
Patient no. 1 2 3
Gender M M FAge at diagnosis 10 m 1 y, 2 m 2 y, 7 mAge at ERT start 11 m 1 y, 2 m 2 y, 9 mGBA activitya 0.16 1.42 1.43ERT dose (U/kg/2 weeks) 60 60b 60Age at last survey 8 y, 5 m 4 y, 11 m 9 y, 2 mHemoglobin (g/dl)c 12.5 ± 0.6 13.0 ± 0.5 12.6 ± 0.5Platelet (k/cumm) 162.2 ± 31.7 182.6 ± 62.4 213.0 ± 41BMD (age, Z score) 0.581
(8.1 y,−0.1)0.345(5.5 y,−4.1)
0.565(9.6 y,−1
Gaze palsy − + −Seizure − − −Mental retardation − (FIQ 88)d + (FIQ 66) −Kyphosis (degree, age, area) + (48°, 7 y 5 m, thoracic) + (53°, 2 y 2 m,
thoracolumbar)−
Lymphadenopathye + (8 y 3 m,abdomen)
+ (3 y 6 m, neck,thorax, abdomen)
+ (7 y 8 mabdomen)
a GBA activity N N 5.1 nmol/mg/h.b Increased to 120 U/kg/2 weeks when lymphadenopathy occurred.c Hemoglobin and platelet values are mean ± (SD) after 1 year of treatment.d Scores of Verbal Comprehension index (VCI) and Processing Speed Index (PSI) were belowe Lymphadenopathy (age detected, location).
statistical analysis before and after treatment. A p value less than 0.05was considered statistically significant.
Results
Somatic responses to ERT
Hepatosplenomegaly and thrombocytopenia were observed in allpatients at the time of diagnosis, and five patients (except patient 6and 7) showed failure to thrive (Table 1). ThemeanHgB level increasedfrom 8.6 ± 1.6 (g/dl) to 12.4 ± 0.77 (g/dl) after 1 year of treatment(p = 0.028). The platelet count increased from 89.32 ± 31.971.6(k/cumm) to 215.94 ± 33.58 (k/cumm) after 1 year of treatment(p = 0.028). After a median treatment period of 7.6 years (2.2–12.0 years), none of them had an enlargement of the liver or spleen.Chitotriosidase activity decreased adequately in response to ERT,though a transient rise of chitotriosidase activities was noted duringthe period of drug shortage [15]. None of the 7 patients had bone crisisor avascular necrosis of the hip during the follow-up period. Bonemineral density measured using dual-energy X-ray absorptiometry re-vealed osteopenia (Z b 1) only in patient 2 (Z = −4.1) and patient 3(Z = −1.8).
However, at the latest follow up, four (patients 1–4) showed shortstature and three (patiens 2, 3, and 6) had a lowbodyweight.Moreover,five of the seven patients exhibited kyphosis, although none of themcomplained of pain or discomfort (Table 1). Their spines felt rigid duringphysical examination, and patient 2 showed an acute angle over thethoracolumbar junction.
Progression of neurological symptoms
All patients, throughout the following period, had normal musclepower and muscle tone, normal deep tendon reflex, and no cerebel-lar sign. However, horizontal gaze palsy was observed in two pa-tients (patients 2 and 5), although this symptom did not interferewith the daily activity of the patients. Patient 7 exhibited absenceseizures since 10 years of age. Moreover, mild mental retardationwas noted in patient 2 (FIQ 66), patient 5 (FIQ 55), and patient 7(FIQ 70). Patient 1 had a borderline FIQ score (FIQ 88), but scores
4 5 6 7
M F F F1 y, 10 m 1 y, 3 m 1 y, 9 m 2 y, 3 m2 y 2 y, 1 m 2 y, 1 m 2 y, 4 m3.58 0.79 0.91 0.960 60 60 604 y, 2 m 13 y, 5 m 14 y,1 m 13 y, 1 m11.8 ± 0.2 13.1 ± 0.5 11.0 ± 0.6 13.0 ± 0.6
.9 228.0 ± 33.9 226.0 ± 45.9 260.7 ± 57.1 239.8 ± 69.9
.8)0.502(4.6 y, 0.5)
0.826(14 y,−0.7)
1.123(14.5 y, 0.2)
1.005(13.6 y,−0.2)
− + − −− − − +− + (FIQ 55) − + (FIQ 70)− + (54°, 13 y 6 m,
thoracic)+ (45°, 14 y 2 m,thoracic)
+ (56°, 13 y,thoracic)
, thorax, + (2 y, thorax,abdomen)
− − −
the normal ranges.

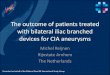
Fig. 1. Lymphadenopathy shown by computed tomography (CT) imaging in patients with Gaucher disease. (A) Lateral view of the head and neck of patient 2 showsmultiple lymph nodeshadows over the posterior cervical triangles (arrows). (B) Anterior–posterior viewof the head and neckof patient 2 one year later showsmultiple lymphnode shadows over the posteriorcervical triangles (arrows). (C) Horizontal view of the chest of patient 2 shows multiple subcarinal and pulmonary hilar lymph nodes (arrows). (D) Horizontal view of the abdomen ofpatient 2 shows enlarged lymph nodes in the mesentery and para-aortic regions (arrow). (E) Horizontal view of the abdomen of patient 4 shows conglomerate mesenteric lymphnodes surrounding the mesenteric vessels (arrow). (F) Horizontal view of the abdomen of patient 5 shows conglomerate mesenteric lymph nodes and enlarged para-aortic lymphnodes (arrow).
107N.-C. Lee et al. / Blood Cells, Molecules and Diseases 53 (2014) 105–109
of Verbal Comprehension index (VCI) and Processing Speed Index(PSI) were below the normal ranges.
Lymphadenopathy
Lymphadenopathy occurred in 4 of the 7 patients (57.1%). Patient 2was found to have enlarged submandibular lymph nodes at 3 years and6 months of age during an upper airway infection. A neck computer to-mography (CT) scan revealed extensive homogeneous soft tissueshadows over both upper, mid, and lower jugular regions, right upperpara-tracheal regions, and axillary regions (Fig. 1). A lymphnode biopsythat was performed on frozen sections and stained for the histiocytemarker CD68 and the tumormarker EBER (EBV-encoded RNA) revealedmassive lymphadenopathy with the infiltration of numerous CD68-positive histiocytes in the lymphoid sinusoid spaces without malig-nancy changes (Fig. 2). Patient 3 was found to have asymptomaticlymphadenopathy over the left para-aortic and juxa-intestinal regionsat the age of 7 years and 8 months. Patient 4 was noted to have lymph-adenopathy (bilateral para-aortic, superior mesenteric, and gastro-omental) at the time of diagnosis. A CT scan performed on patient 1identified calcified lymph nodes extending from the para-aortic to
mesenteric areas, which likely indicates lymphadenopathy. The lymph-adenopathywas stationary in these patients during follow-up analyses.
Discussion
In the current study, we analyzed seven type III GD patients with ahomogeneous genetic background (homozygous p.L444P mutation)and we treated them from an early age. Our results revealed that ERTreverted patients' visceral symptoms rapidly, but neurological symp-toms including horizontal gaze palsy, seizure, and mental retardationstill appeared during the treatment period.
The large variability in the treatment outcome of type III GD mightarise from genetic heterogeneity of the patients and the differences inage to start the treatment. Altarescu et al. treated 21 type III GD patients(13with homozygous p.L444Pmutation) and found that cognitive func-tion remained unchanged or improved over time in 13 patients but de-clined in 8 patients [16]. Tajima et al. described the long-term follow up(9–15 years) of the treatment of ten patients with homozygous p.L444Pmutation, and four had mental retardation [11]. More recently, Kraouaet al. reported ten type III GD patients, and ERT prevented the evolutionof neurological disturbances in the four patients with homozygousp.L444P mutation [17]. In the current study, although we treated the

Fig. 2.Histology and special stains of a lymph node biopsy from patient 2. (A) A 100×magnification view of lymphnodes stainedwith H&E stain reveals intensive infiltration in the lymphnode sinusoid spaces. (B) A higher magnification (400×) view of lymph nodes stained with H&E. The arrows point to a clump of large infiltrating cells with pale cytoplasm (arrows).(C) The infiltrating cells are positive for the macrophage marker CD68 (arrows). (D) The infiltrating cells are negative for the tumor marker EBER.
Table 2Summary of reported Gaucher disease patients with lymphadenopathy.
Case Age/sex Type Ethnics Genotype Time Location of LAPs F/U Outcome Reference
1 3 y/F III NR NR 2 Mesenteric 3 Stationary [26]2 3 y/M III Caucasian p.L444P/K79N 1.3 Mediastinal, hilar,
mesenteric, para-aortic9 Progressive despite dose
increase to 60 IU/kg/wk; died[27,28]
3 5 y/F I/III Turkish p.L444P/? 3.4 Mesenteric 1 Stationary [29]4 4 y/F NR NR NR 1.8 Nasopharyngeal,
mesenteric5 Progressive [30]
5 8 y/F NR NR p.L444P/L444P 7 Mesenteric NR NR [30]6 4.6 y/M III Korean p.L444P/L444P 3.6 Cervical, mediastinal,
mesenteric3 Progressive after increase
dose to 120 IU/kg/qow[18]
7 10 m/M II African-American NR 0 Cervical, axillary, inguinal 0 Died at time of diagnosis [31]8 10 y/F IIIB NR NR 10 Mesenteric
(calcified by CT scan)9 Progressive [32]
9 8.3 y/M IIIB Chinese p.L444P/L444P 7.2 Para-aortic, mesenteric(calcified by CT scan)
1 Stationary Our case 1
10 3.5 y/M IIIB Chinese p.L444P/L444P 3.7 Cervical, subcarinal,hilar, mesenteric, para-aortic
2.3 Stationary after increase indose to 120 IU/kg/qow
Our case 2
11 7.6 y/F IIIB Chinese p.L444P/L444P 5 Para-aortic, juxa-intestinal 2.5 Stationary Our case 312 2 y/M IIIB Chinese p.L444P/L444P 0 Para-aortic, mesenteric,
gastro-omental3 Stationary Our case 4
13 5.5 y/M I Egyptian p.R359Q/R359Q 5 Mesenteric, mediastinal 6.5 Regression after increasein ERT dose to120 IU/kg/qow, deterioratedon dose reduction
[33]
14 4 y/F I Egyptian NR 2.5 Mesenteric, para-aortic,mediastinal
0.25 Progressive [33]
15 NR/F I Egyptian NR NR Mesenteric NR NR [33]16 4.5 y/M 3 Egyptian p.L444P/L444P 3.5 Pelviabdominal,
retroperitoneal, mediastinal(calcified by CT scan)
NR NR [33]
17 6 y/M III Egyptian p.L444P/L444P 5 Mediastinal, hilar,pelviabdominal
NR NR [33]
18 NR/F III Egyptian p.L444P/L444P NR Mesenteric NR NR [33]
CT, computed tomography; F, female; F/U, years of follow up after notice of lymphadenopathy; LAP, lymphadenopathy; M, male; NR, not reported; time, years after enzyme replacementtherapy at the time noticed to have lymphadenopathy.
108 N.-C. Lee et al. / Blood Cells, Molecules and Diseases 53 (2014) 105–109

109N.-C. Lee et al. / Blood Cells, Molecules and Diseases 53 (2014) 105–109
seven patients from an early age (median 2.1 years), neurologicalsymptoms appeared in four of them at a mean age of 11 years (mean9.6 years). Further progression of neurological symptoms in these pa-tients is also possible. Therefore, the progression of neurological symp-toms in these patients probably reflected the neurologic natural historyof type III GD. However, the cognitive decline may not be comparedacross studies because of the differences in ethnicity and start point ofbaseline IQ. The current study also demonstrates the phenotype vari-ability among patients with homozygous p.L444P mutations. Correctprediction of phenotype for GD will be critical before presymptomaticdiagnosis like newborn screening can be effectively applied to GD.
Somatic manifestations may not respond to ERT as well. Lymphade-nopathy was thought to be a rare manifestation of GD. A recentlystudy on lymphadenopathy in GD collected six cases at a young age(3–8 years), and two of them were homozygous for the p.L444P muta-tion [18]. However, this symptomwas found in four of our seven (57%)patients, so the incidence may be higher than what people thought. Al-though the lymphadenopathy in our patients was stationary during thefollow-up period, it progressed and caused protein-losing enteropathyin two previously reported patients [18]. We have reviewed 18 casesof GD with lymphadenopathy, and the most common location for thelymph nodes were abdominal or mesenteric (Table 2). Gaucher cellinfiltration in the lymph nodesmay raise further concerns becausemul-tiple myeloma is the most frequent neoplasm seen in GD [19]. Lymph-adenopathy occurred in patients who underwent ERT and might notrespond to dose adjustment [18]. Patients with homozygous p.L444Pmutation also have an increased risk of pulmonary manifestations[20]. Similarly, pulmonary hypertension in type I GD and Gaucher celllung infiltration in type II and III GDmaynot respond to ERT [21]. Patientwith type III GD also developed kyphosis during ERT [17,22]. Kyphosismay be considered to be of a central nervous system (CNS) etiology,and hence not seen or expected to reverse with or without ERT.
In conclusion, this study describes the neurological natural history ofp.L444P homozygous GD patients who underwent ERT, and also empha-sizes the residual somatic burden in those patients. Because the recombi-nant enzyme is not supposed to cross the blood–brain barrier efficientlyand act on the CNS [23], an additional treatment, like the brain-penetrating substrate reduction therapy [24] or pharmacological chaper-ones [25], will be necessary to improve the outcome of type III GD.
Disclosure
These cases have been submitted to the Gaucher Registry, which issupported by Genzyme, a Sanofi Company. Yin-Hsiu Chien has receiveda grant from Genzyme to operate the registry. Wuh-Liang Hwu hasreceived traveling grants from Genzyme to join the registry meetings.
Acknowledgments
We thank the patients and their families for their cooperation.
References
[1] R.O. Brady, J.N. Kanfer, D. Shapiro, Metabolism of glucocerebrosides. II. Evidence ofan enzymatic deficiency in Gaucher's disease, Biochem. Biophys. Res. Commun. 18(1965) 221-5.
[2] E. Beutler, G. Grabowski, Gaucher disease, in: C. Scriver, A. Beaudet, W. Sly, D. Valle(Eds.), The Metabolic and Molecular Bases of Inherited Diseases, McGraw-Hill, NewYork, 1995, pp. 2641–2670.
[3] N.J. Weinreb, J. Charrow, H.C. Andersson, et al., Effectiveness of enzyme replacementtherapy in 1028 patients with type 1 Gaucher disease after 2 to 5 years of treat-ment: a report from the Gaucher Registry, Am. J. Med. 113 (2002) 112–119.
[4] K.E. Bove, C. Daugherty, G.A. Grabowski, Pathological findings in Gaucher diseasetype 2 patients following enzyme therapy, Hum. Pathol. 26 (1995) 1040–1045.
[5] S. Dreborg, A. Erikson, B. Hagberg, Gaucher disease—Norrbottnian type. I. Generalclinical description, Eur. J. Pediatr. 133 (1980) 107–118.
[6] A. Erikson, M. Astrom, J.E. Mansson, Enzyme infusion therapy of the Norrbottnian(type 3) Gaucher disease, Neuropediatrics 26 (1995) 203–207.
[7] N. Dahl, M. Lagerstrom, A. Erikson, U. Pettersson, Gaucher disease type III(Norrbottnian type) is caused by a single mutation in exon 10 of theglucocerebrosidase gene, Am. J. Hum. Genet. 47 (1990) 275-8.
[8] J.K. Park, E. Orvisky, N. Tayebi, et al.,Myoclonic epilepsy inGaucher disease: genotype–phenotype insights from a rare patient subgroup, Pediatr. Res. 53 (2003) 387–395.
[9] L. Wan, C.M. Hsu, C.H. Tsai, et al., Mutation analysis of Gaucher disease patients inTaiwan: high prevalence of the RecNciI and L444P mutations, Blood Cells Mol. Dis.36 (2006) 422–425.
[10] H. Ida, O.M. Rennert, K. Iwasawa, M. Kobayashi, Y. Eto, Clinical and genetic studies ofJapanese homozygotes for the Gaucher disease L444P mutation, Hum. Genet. 105(1999) 120–126.
[11] A. Tajima, T. Yokoi, M. Ariga, et al., Clinical and genetic study of Japanese patientswith type 3 Gaucher disease, Mol. Genet. Metab. 97 (2009) 272–277.
[12] M.C. Patterson, M. Horowitz, R.B. Abel, et al., Isolated horizontal supranuclear gazepalsy as a marker of severe systemic involvement in Gaucher's disease, Neurology43 (1993) 1993–1997.
[13] A. Abrahamov, D. Elstein, V. Gross-Tsur, et al., Gaucher's disease variantcharacterised by progressive calcification of heart valves and unique genotype,Lancet 346 (1995) 1000–1003.
[14] E.H. Davies, A. Erikson, T. Collin-Histed, et al., Outcome of type III Gaucher disease onenzyme replacement therapy: review of 55 cases, J. Inherit. Metab. Dis. 30 (2007)935–942.
[15] Y.H. Chien, N.C. Lee, F.J. Tsai, M.C. Chao, W.L. Hwu, Reduction in imiglucerase dosagecauses immediate rise of chitotriosidase activity in patients with Gaucher disease,Mol. Genet. Metab. 101 (2010) 90–91.
[16] G. Altarescu, S. Hill, E. Wiggs, et al., The efficacy of enzyme replacement therapy inpatients with chronic neuronopathic Gaucher's disease, J. Pediatr. 138 (2001)539–547.
[17] I. Kraoua, F. Sedel, C. Caillaud, et al., A French experience of type 3 Gaucher disease:phenotypic diversity and neurological outcome of 10 patients, Brain Dev. 33 (2011)131–139.
[18] B.H. Lee, D.Y. Kim, G.H. Kim, et al., Progressive mesenteric lymphadenopathy withprotein-losing enteropathy; a devastating complication in Gaucher disease, Mol.Genet. Metab. 105 (2012) 522–524.
[19] A.A. Tantawy, E.M. Sherif, A.A. Adly, S. Hassanine, A.H. Awad, Evoked potentialsand neurocognitive functions in pediatric Egyptian Gaucher patients on enzymereplacement therapy: a single center experience, J. Inherit. Metab. Dis. 36 (2013)1025–1037.
[20] F. Santamaria, G. Parenti, G. Guidi, et al., Pulmonary manifestations of Gaucher dis-ease: an increased risk for L444P homozygotes? Am. J. Respir. Crit. Care Med. 157(1998) 985–989.
[21] S.M. Lo, J. Liu, F. Chen, et al., Pulmonary vascular disease in Gaucher disease: clinicalspectrum, determinants of phenotype and long-term outcomes of therapy, J. Inherit.Metab. Dis. 34 (2011) 643–650.
[22] P. Suwannarat, S. Keeratichamroen, D.Wattanasirichaigoon, et al., Molecular charac-terization of type 3 (neuronopathic) Gaucher disease in Thai patients, Blood CellsMol. Dis. 39 (2007) 348–352.
[23] A. Vellodi, A. Tylki-Szymanska, E.H. Davies, et al., Management of neuronopathicGaucher disease: revised recommendations, J. Inherit. Metab. Dis. 32 (2009)660–664.
[24] J. Cox-Brinkman, M.J. van Breemen, B.T. van Maldegem, et al., Potential efficacy ofenzyme replacement and substrate reduction therapy in three siblings withGaucher disease type III, J. Inherit. Metab. Dis. 31 (2008) 745–752.
[25] A. Zimran, G. Altarescu, D. Elstein, Pilot study using ambroxol as a pharmacologicalchaperone in type 1 Gaucher disease, Blood Cells Mol. Dis. 50 (2013) 134–137.
[26] A.K. Lim, A. Vellodi, K. McHugh, Mesenteric mass in a young girl—an unusual site forGaucher's disease, Pediatr. Radiol. 32 (2002) 674–676.
[27] T.A. Burrow, M.B. Cohen, R. Bokulic, et al., Gaucher disease: progressive mesentericand mediastinal lymphadenopathy despite enzyme therapy, J. Pediatr. 150 (2007)202–206.
[28] T. Burrow, D. Witte, L. Bailey, et al., Abnormal pathology findings in a patient withGaucher disease type 3 treated with enzyme replacement therapy, Mol. Genet.Metab. 108 (2013) S27-S27.
[29] B. Yagci, O. Salor, B. Yalcin, et al., Giant lymphadenopathy infiltrated by Gaucher cellsmimicking lymphoma, Pediatr. Blood Cancer 52 (2009) 870–871.
[30] D.J. Fowler, M.A. Weber, G. Anderson, et al., Ultrastructural features of Gaucherdisease treated with enzyme replacement therapy presenting as mesenteric masslesions, Fetal Pediatr. Pathol. 25 (2006) 241–248.
[31] J.M. Levy, D.A. Glass, K.H. Rodriguez, An unusual presentation of Gaucher disease inan infant with progressive dyspnea, Ochsner J. 13 (2013) 270–272.
[32] E. Perez-Colon, A. Sanchez-Valle, S. Patel, M. Murphy, Mesenteric Gaucher cellpseudotumor — a rare cause for diarrhea and tetany in a 19 year-old Gaucher'sType 3b patient, in: J. Zschocke, K.M. Gibson (Eds.), 12th International Congressof Inborn Errors of Metabolism, Journal of Inherited Metabolic Disease, 2013,p. S274, (Barcelona, Spain).
[33] M. Abdelwahab,Mesenteric andmediastinal lymphadenopathy in Egyptian childrenwith Gaucher disease: a study of 6 patients: can enzyme replacement therapy (ERT)play a role in improving their condition? in: S.v. Dahl, M. Horowitz, H. Michelakakis,N. Belmatoug (Eds.), 10th EuropeanWorkingGroup onGaucher Disease, 2012, p. 37,(Paris, France).
Recommended