OSTEOARTHRITISAgus Widiyatmoko
2
INTRODUCTION
• Mostly elderly
• Ageing process???
• Repeated micro trauma to the joint??
ACRFPACRFP
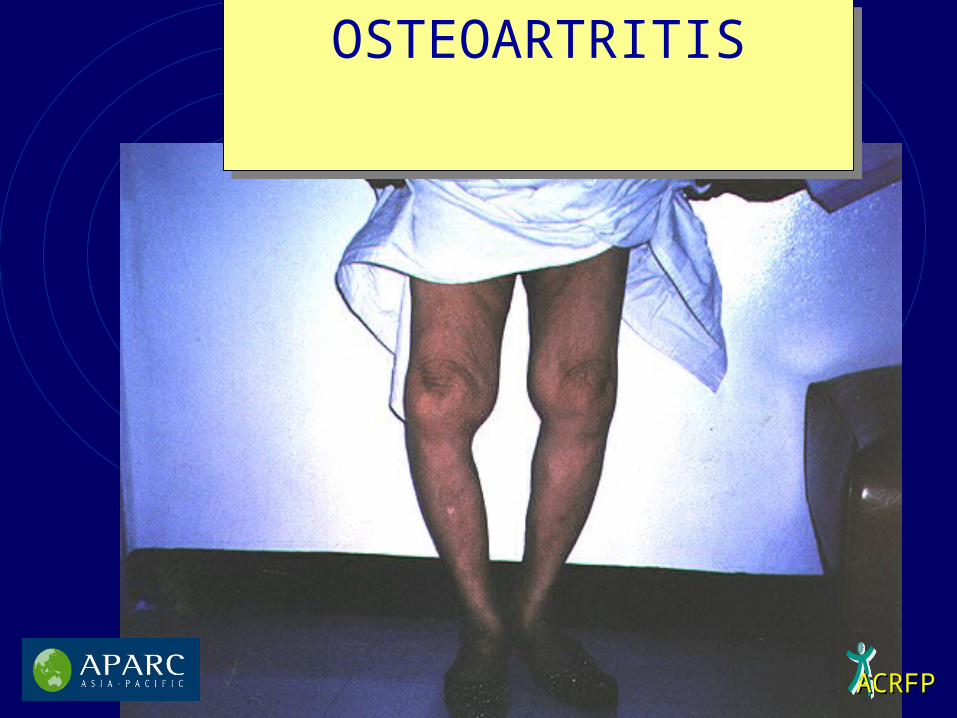
OSTEOARTRITISOSTEOARTRITIS
4
INTRODUCTION
Many theories of etiology and pathogenesis
Start from breakage of cartilage and pathologic condition of the synovium
Definite treatment ???
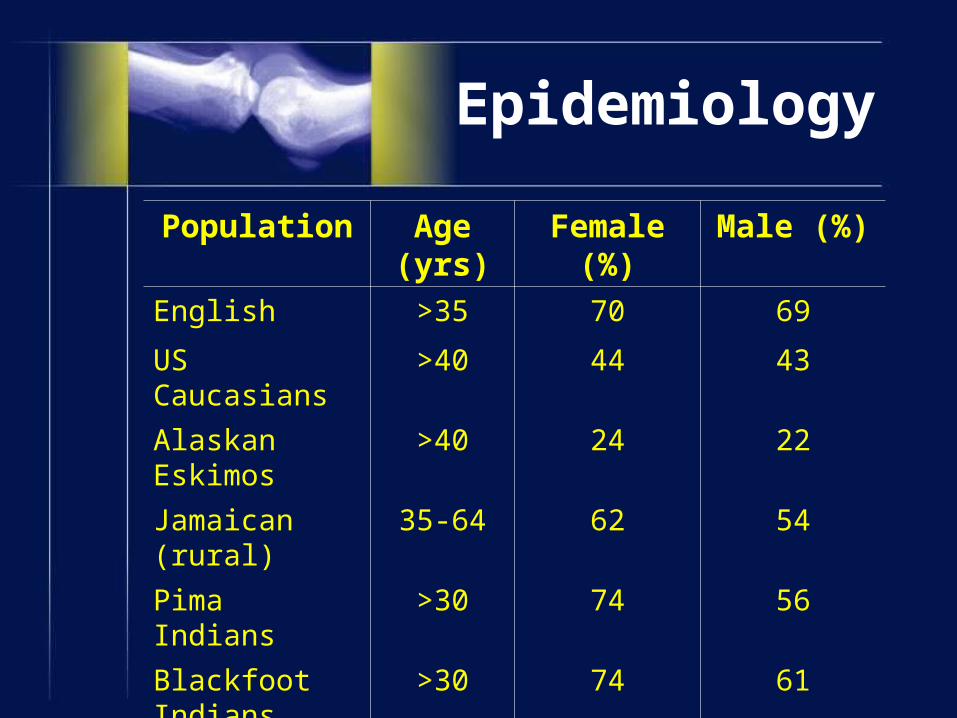
Epidemiology
Population Age (yrs) Female (%) Male (%)
English >35 70 69
US Caucasians >40 44 43
Alaskan Eskimos >40 24 22
Jamaican (rural) 35-64 62 54
Pima Indians >30 74 56
Blackfoot Indians
>30 74 61
South African Black
>35 53 60
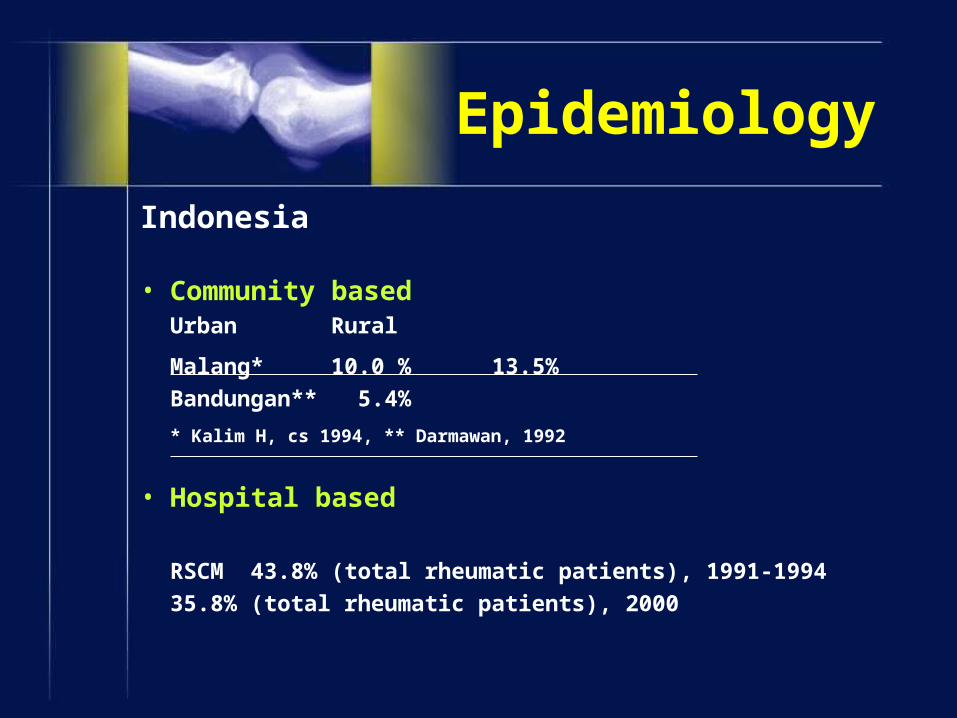
Indonesia
• Community basedUrban Rural
Malang* 10.0 % 13.5%
Bandungan** 5.4%
* Kalim H, cs 1994, ** Darmawan, 1992
• Hospital based
RSCM 43.8% (total rheumatic patients), 1991-1994
35.8% (total rheumatic patients), 2000
Epidemiology
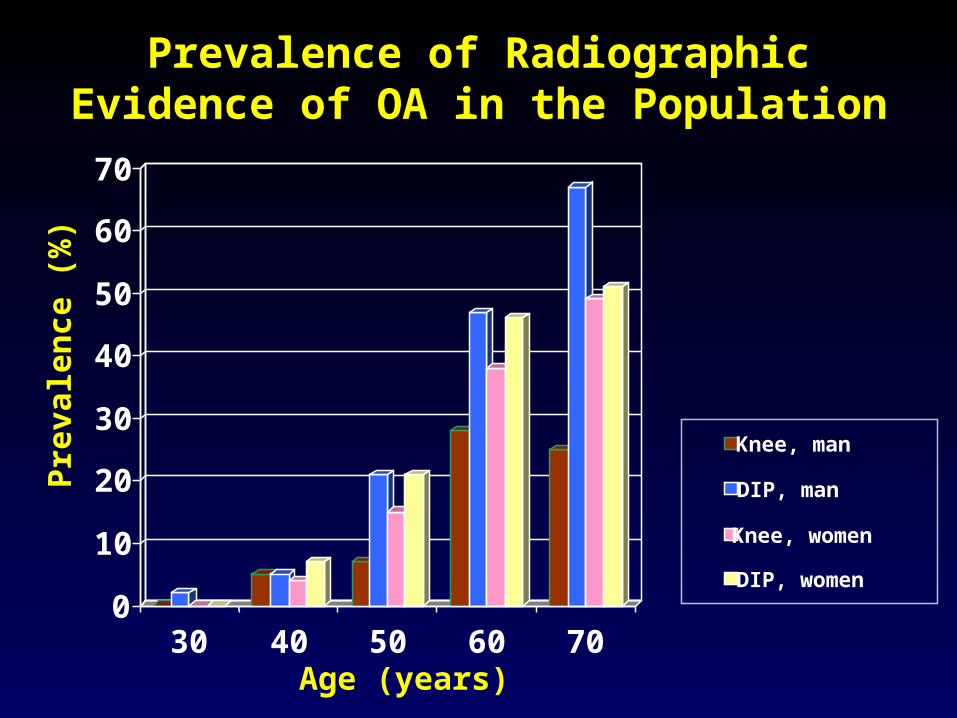
Prevalence of Radiographic Evidence of OA in the Population
Pre
vale
nce
(%
)
Age (years)
0
10
20
30
40
50
60
70
30 40 50 60 70
Knee, man
DIP, man
Knee, women
DIP, women
8
ETIOLOGY
Knowing a normal tissue around the joint
1. Chondrocytes
2. Collagen
3. Proteoglycan
4. Synovial fluid
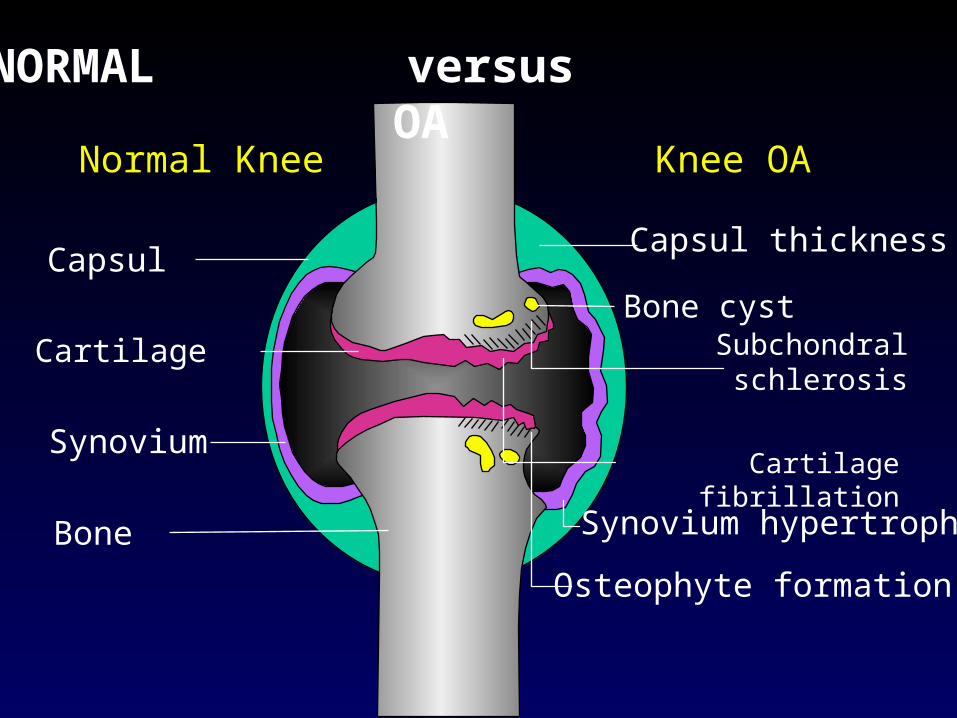
NORMAL versus OA
Capsul thickness
Knee OANormal Knee
Bone cystSubchondral
schlerosis
Cartilage fibrillation
Synovium hypertrophy
Osteophyte formation
Capsul
Cartilage
Synovium
Bone
10
CARTILAGE
1. Hyaline cartilage
2. Fibro cartilage
11
CARTILAGEFibro cartilage : meniscus

ACRFPACRFP
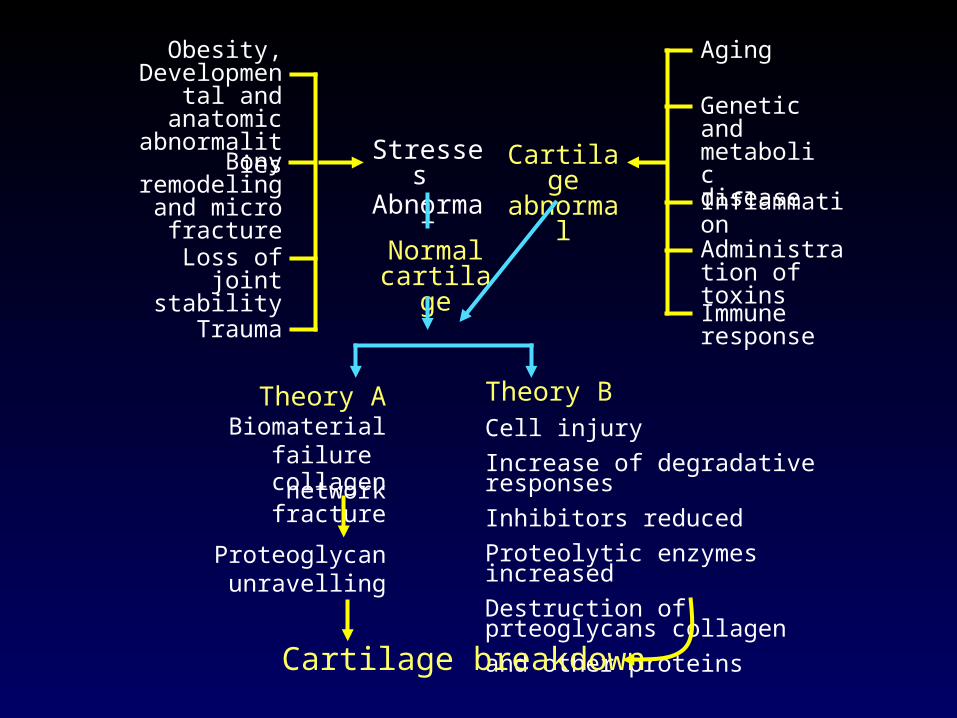
Stresses Abnormal
Normal cartilage
Cartilage abnormal
Aging
Genetic and metabolic disease
Inflammation
Administration of toxins
Immune response
Obesity, Developmental
and anatomic abnormalities
Bony remodeling and micro
fracture
Loss of joint stability
Trauma
Theory A Biomaterial failure
collagen networkfracture
Theory BCell injuryIncrease of degradative responsesInhibitors reducedProteolytic enzymes increasedDestruction of prteoglycans collagenand other proteins
Proteoglycan unravelling
Cartilage breakdown
Degenerative Joint DiseaseDegenerative Joint Disease
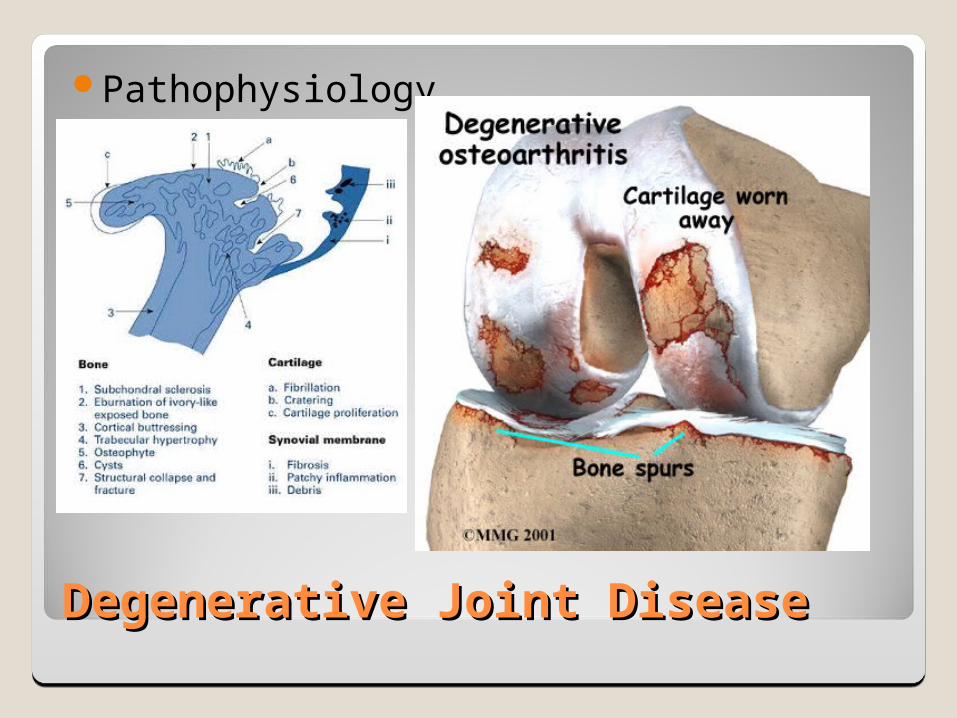
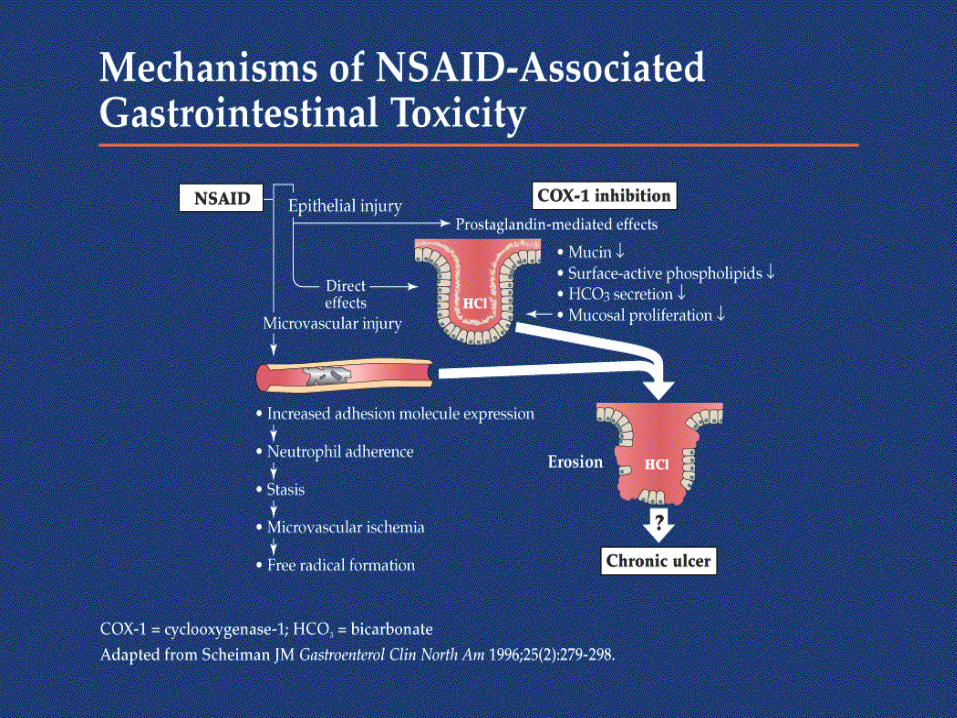
Pathophysiology
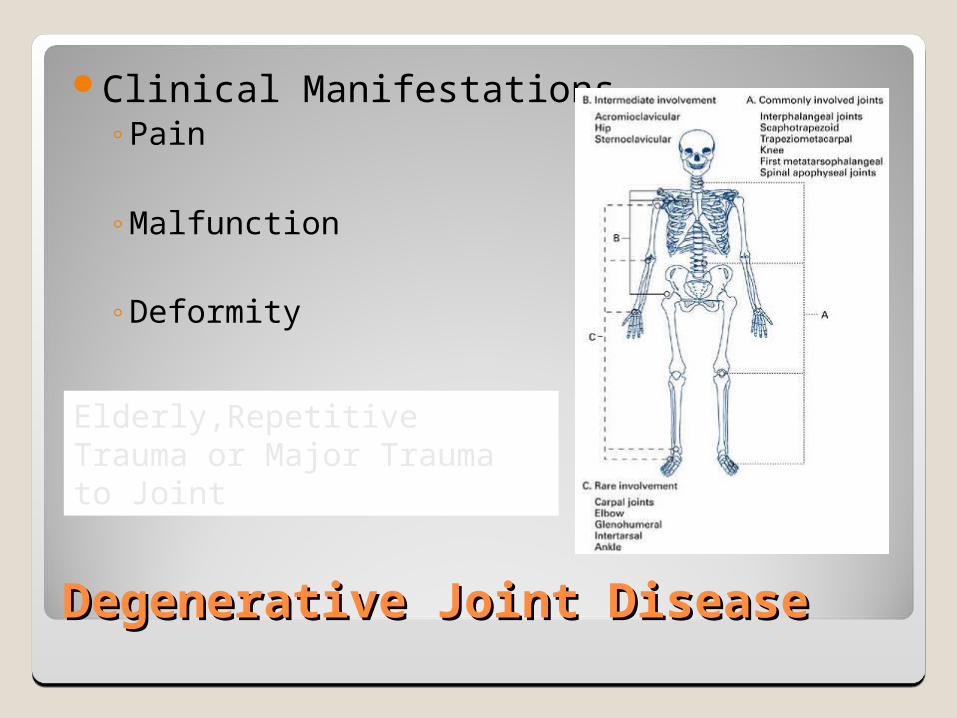
Degenerative Joint DiseaseDegenerative Joint Disease
Clinical Manifestations◦Pain
◦Malfunction
◦Deformity
Elderly,Repetitive Trauma or Major Trauma to Joint
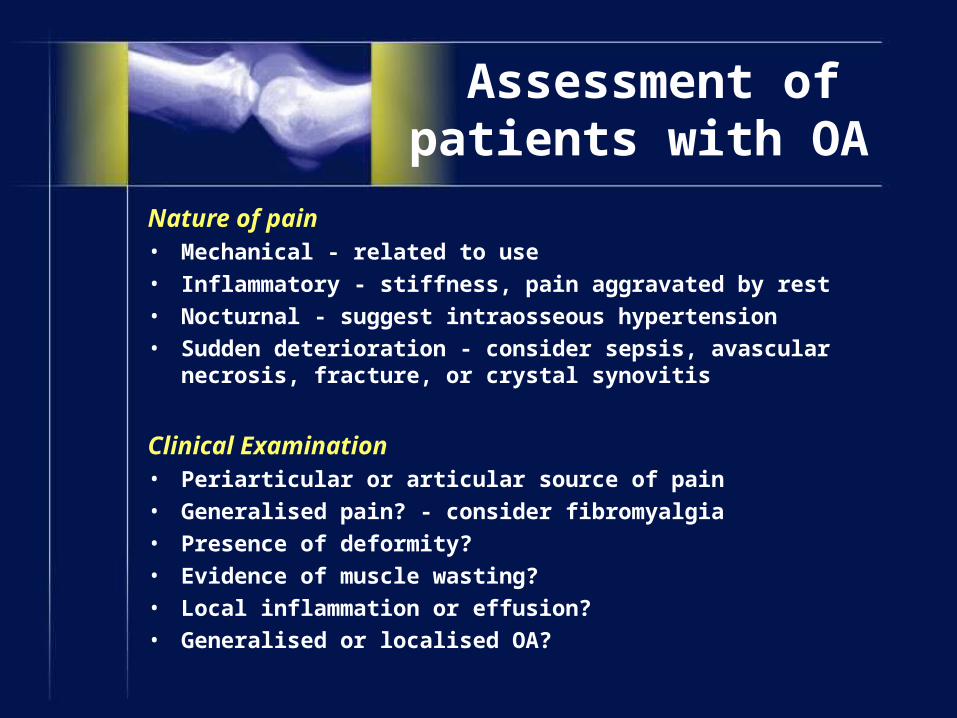
Assessment of patients with OA
Nature of pain• Mechanical - related to use• Inflammatory - stiffness, pain aggravated by rest• Nocturnal - suggest intraosseous hypertension• Sudden deterioration - consider sepsis, avascular necrosis,
fracture, or crystal synovitis
Clinical Examination• Periarticular or articular source of pain• Generalised pain? - consider fibromyalgia• Presence of deformity?• Evidence of muscle wasting?• Local inflammation or effusion?• Generalised or localised OA?
Weight• Potentially modifiable risk factor
Joint locking• Orthopaedic referral probably appropriate
Sleep disturbance• May be associated with fibromyalgia and depression
Comorbid disease
Assessment of patients with Osteoarthritis

19
CLINICAL
1. Altman criteria's
2. Achlback classification
3. Outerbridege grading
4. Kellgreen
20
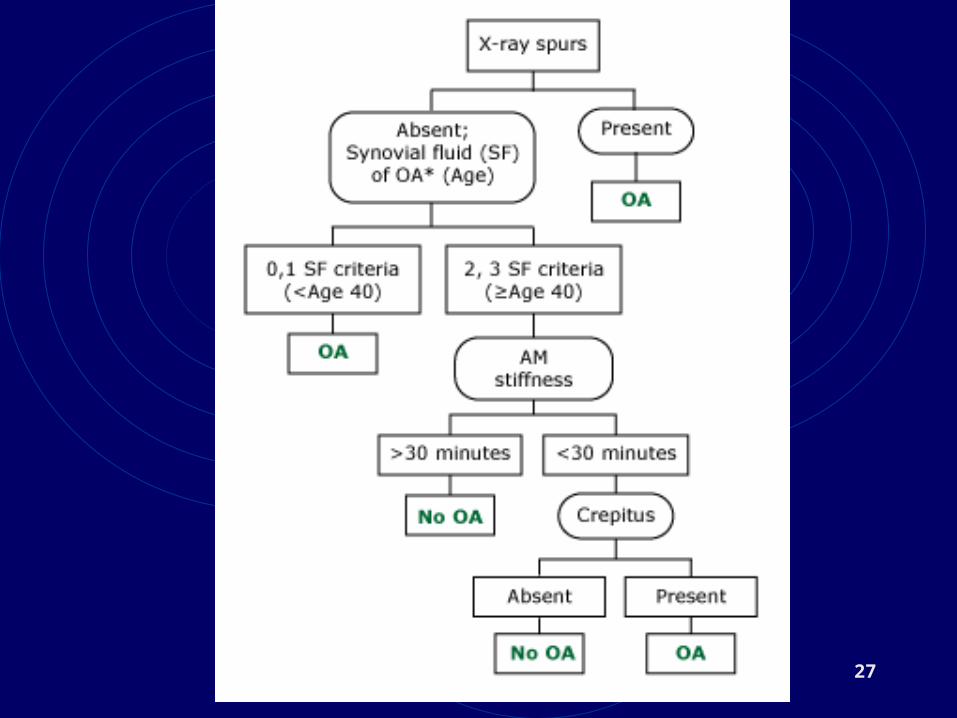
ALTMAN’S CRITERIAS • CLINICAL and LABORATORY Knee pain plus at least 5 of these 9 : 1. Age > 50 years 2. Stiffness < 30 min 3. Crepitus 4. Bony tenderness 5. Bony enlargement 6. No palpable warmth 7. ESR < 40 mm/h 8. RF < 1: 40 ( Rheumatoid Factor ) 9. SF OA ( Synovial Fluid Sign of Osteoarthritis)
21
ALTMAN’S CRITERIAS
• Clinical and Radiographic Knee pain + at least 1 of these 3 :
1. Age > 50 years
2. Stiffness < 30 min
3. Crepitus + osteophytes
22
ALTMAN’S CRITERIAS
• Clinical Knee pain + at least 3 of these 6 : 1. Age > 50 years 2. Stiffness < 30 min 3. Crepitus 4. Bony tenderness 5. Bony enlargement 6. No palpable warmth
23
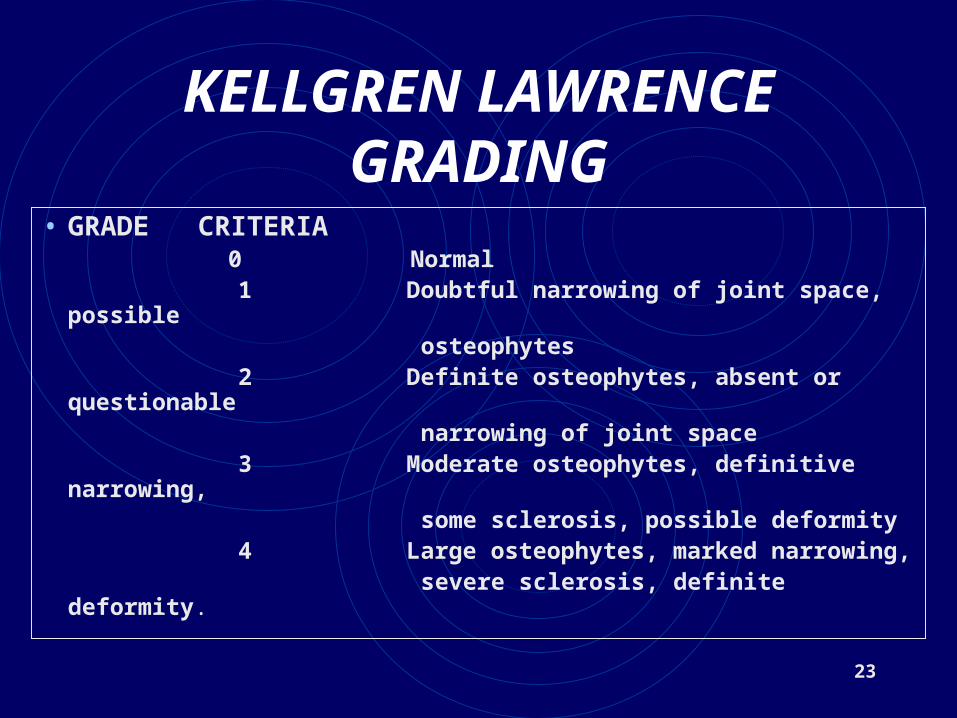
KELLGREN LAWRENCE GRADING
• GRADE CRITERIA 0 Normal 1 Doubtful narrowing of joint space, possible osteophytes 2 Definite osteophytes, absent or questionable narrowing of joint space 3 Moderate osteophytes, definitive narrowing, some sclerosis, possible deformity 4 Large osteophytes, marked narrowing, severe sclerosis, definite deformity.
24
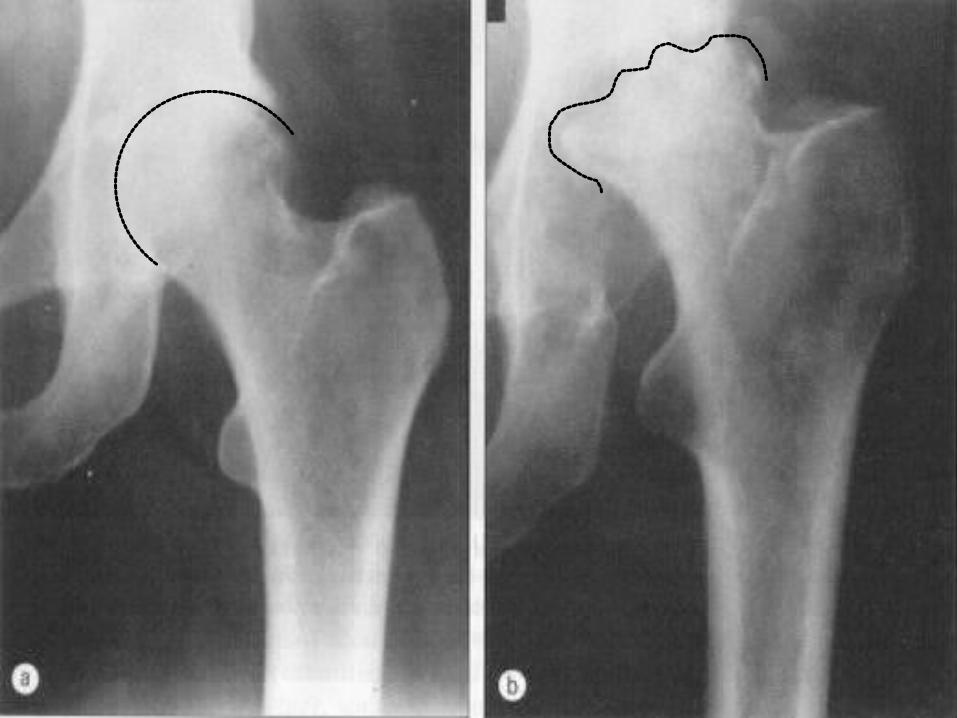
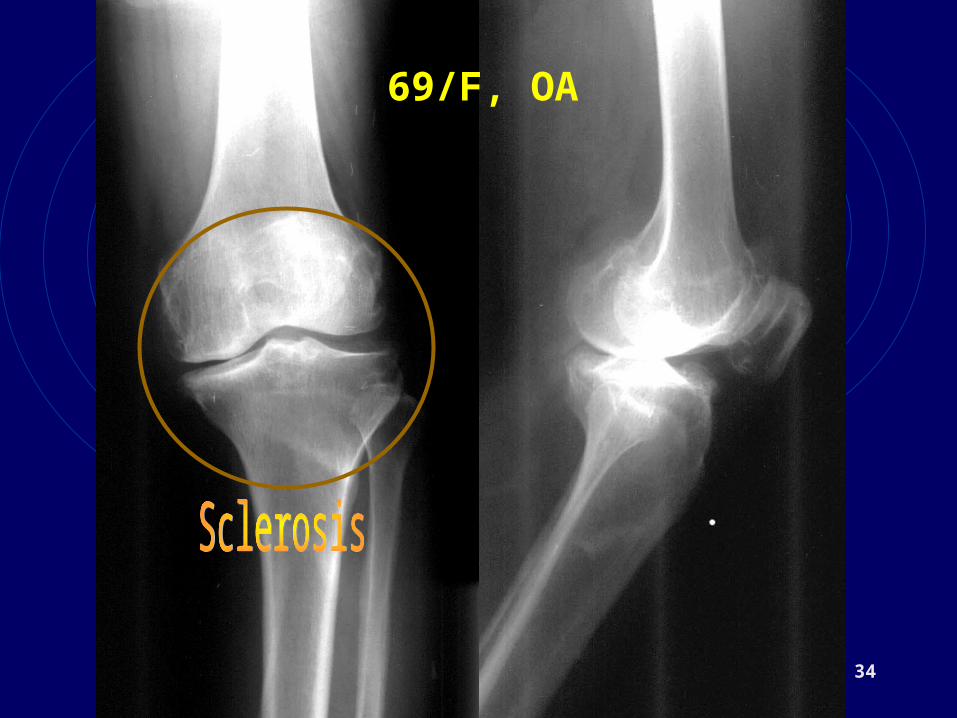
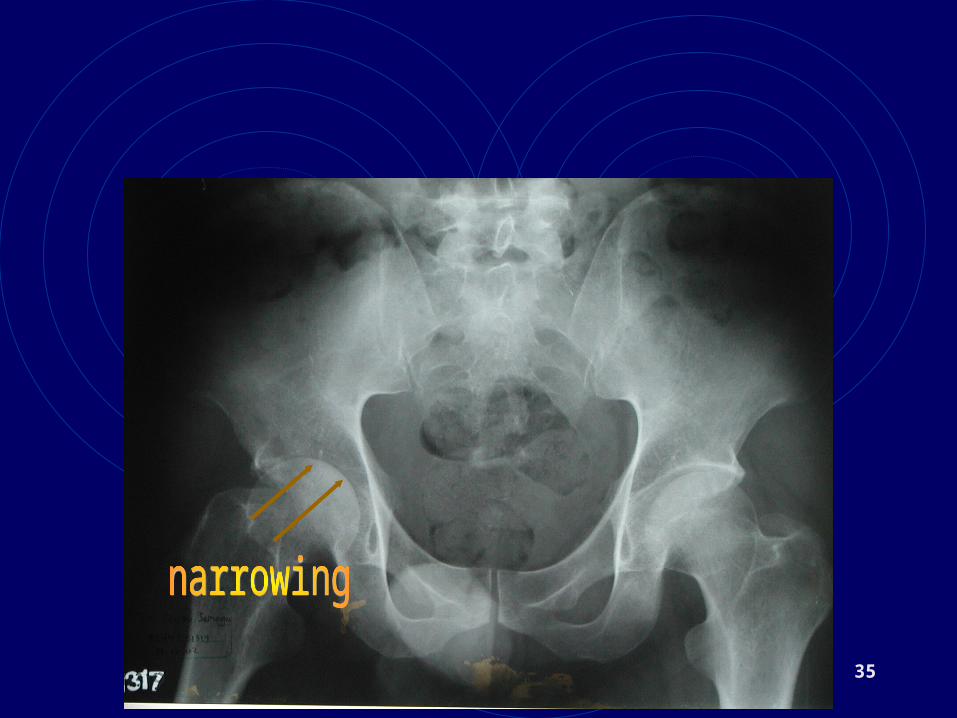
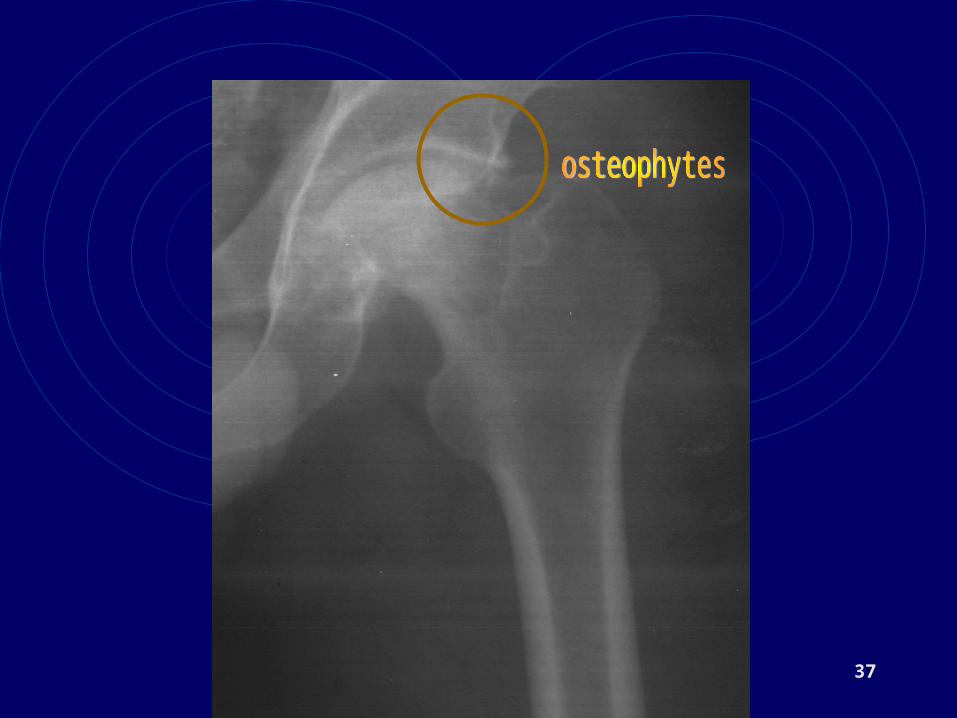
RADIOLOGY
• SOFT TISSUE : ATROPHY
• JOINT SPACE : NARROWING
• BONE : OSTEOPHYTE, SCLEROSING, BONE CYST, MALALIGNMENT (VARUS, VALGUS)
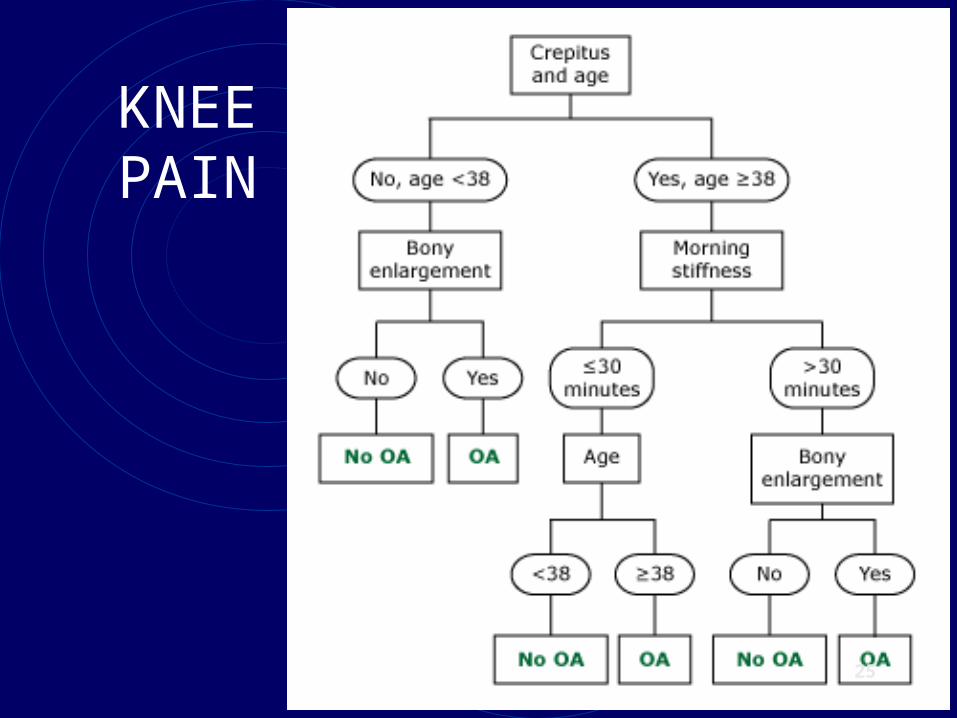
KNEE PAIN
25
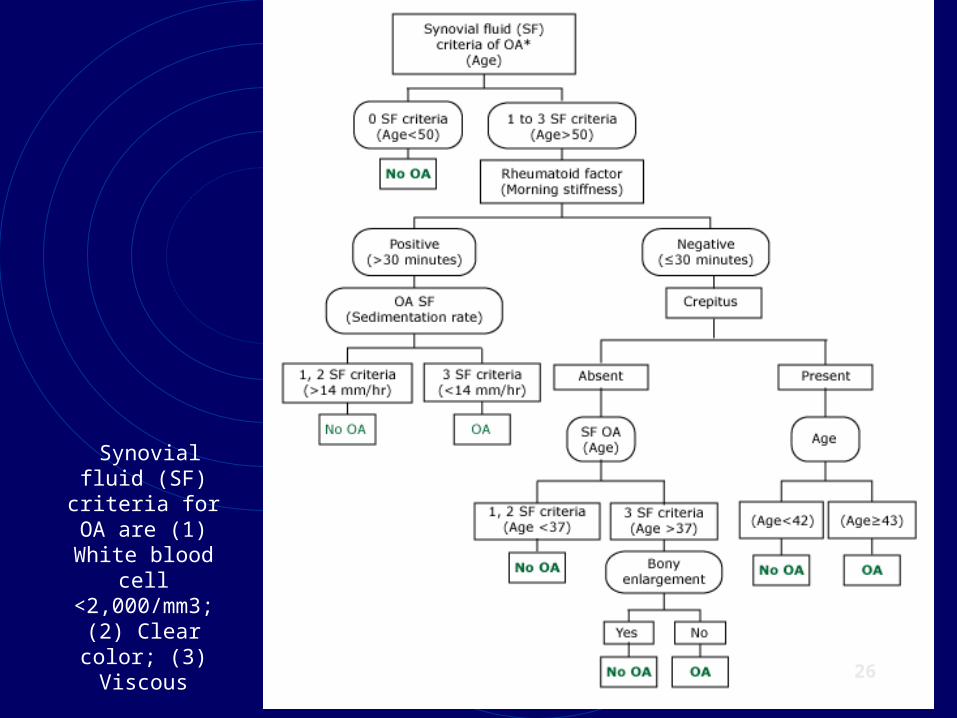
Synovial fluid (SF) criteria for OA are (1)
White blood cell <2,000/mm3; (2) Clear color; (3)
Viscous
26
27
28
29
30
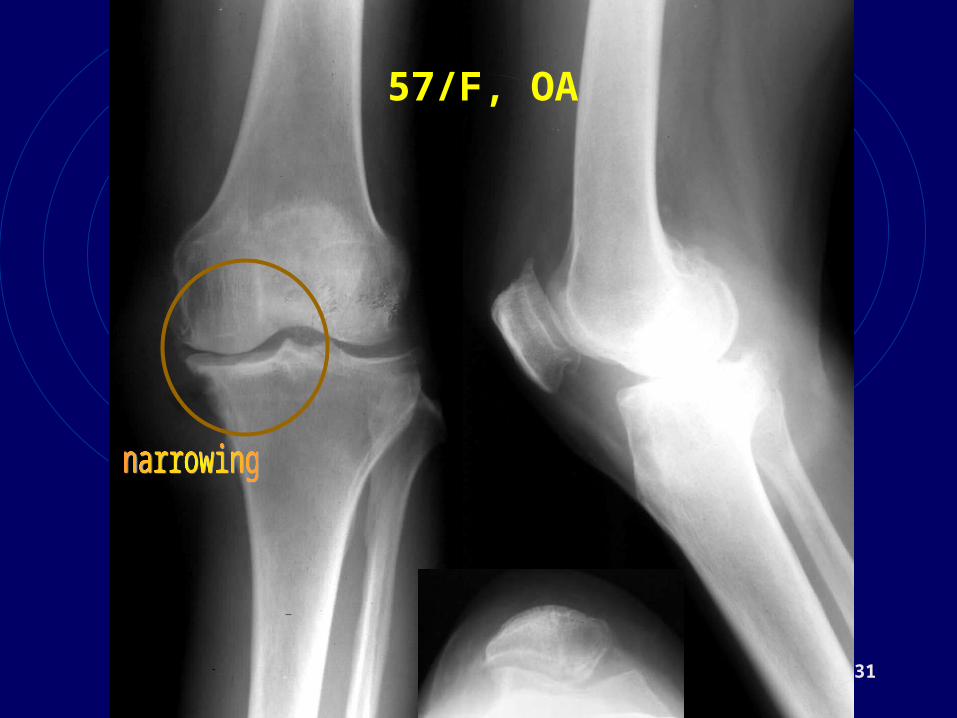
31
57/F, OA
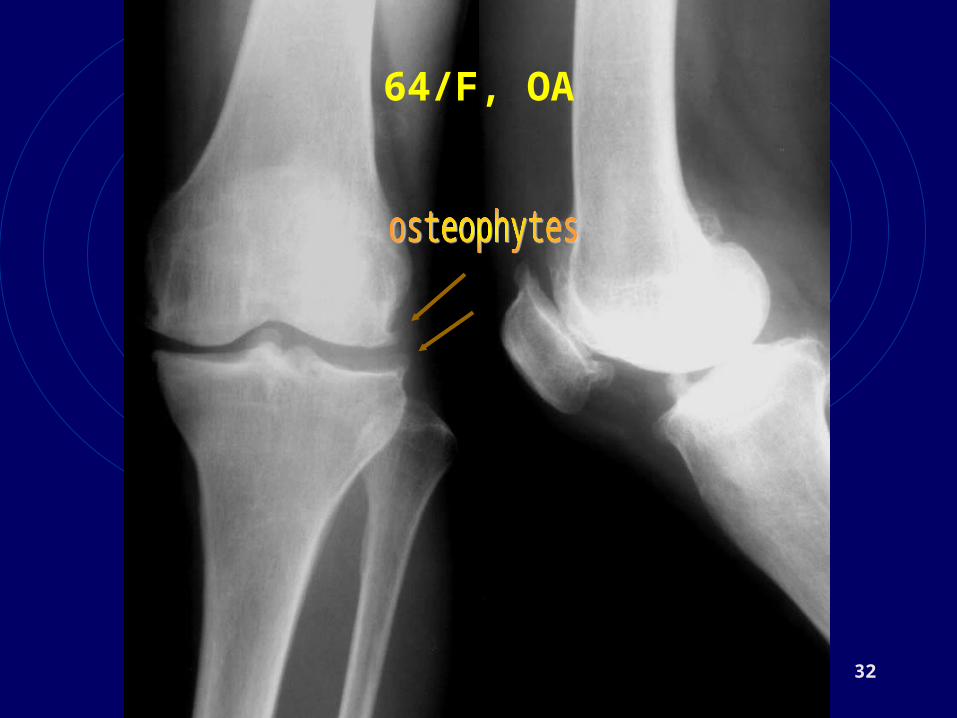
32
64/F, OA
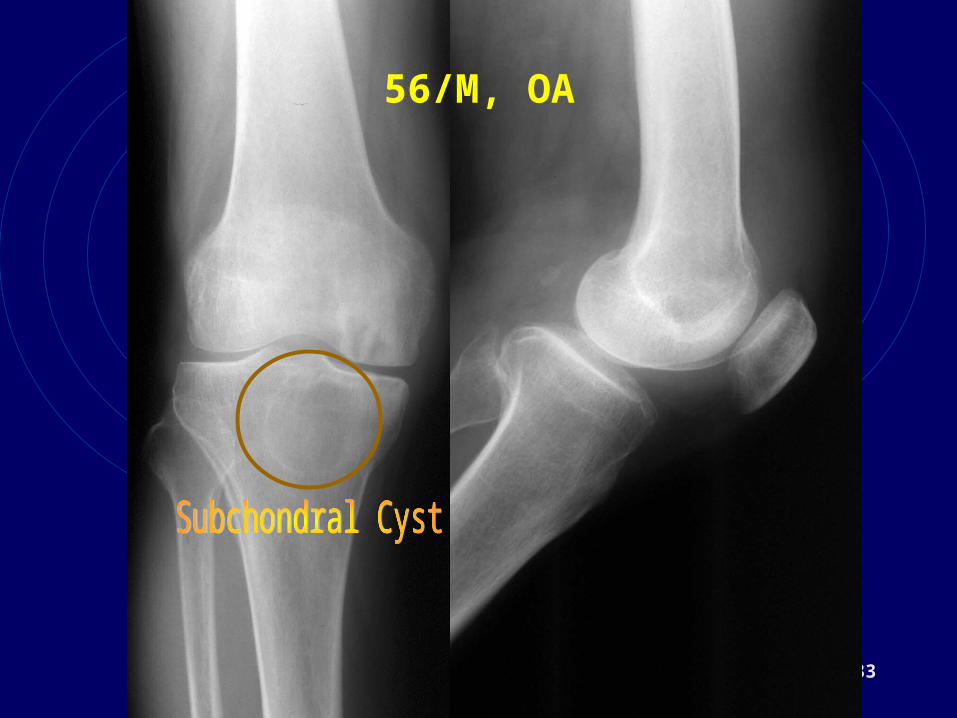
33
56/M, OA
presented at National congress of Indonesian Rheumatology Association. 3rd July 2005.
Jogyakarta
34
69/F, OA
35

36
37
38
CLINICAL
As a whole
• History.
• Atrophy
• Joint Contracture
• Activity daily living
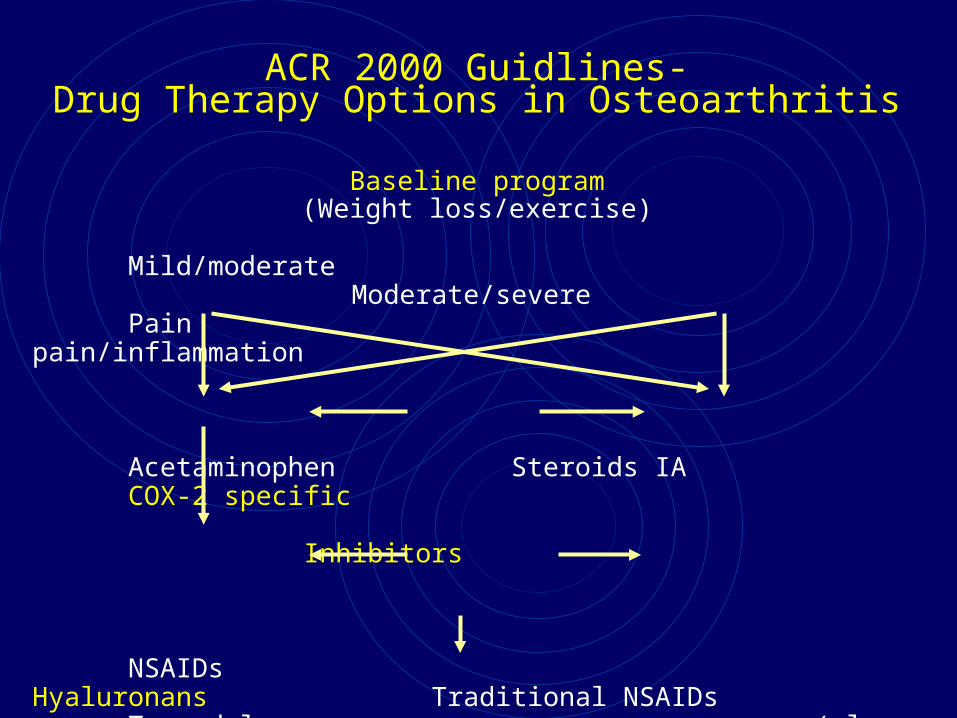
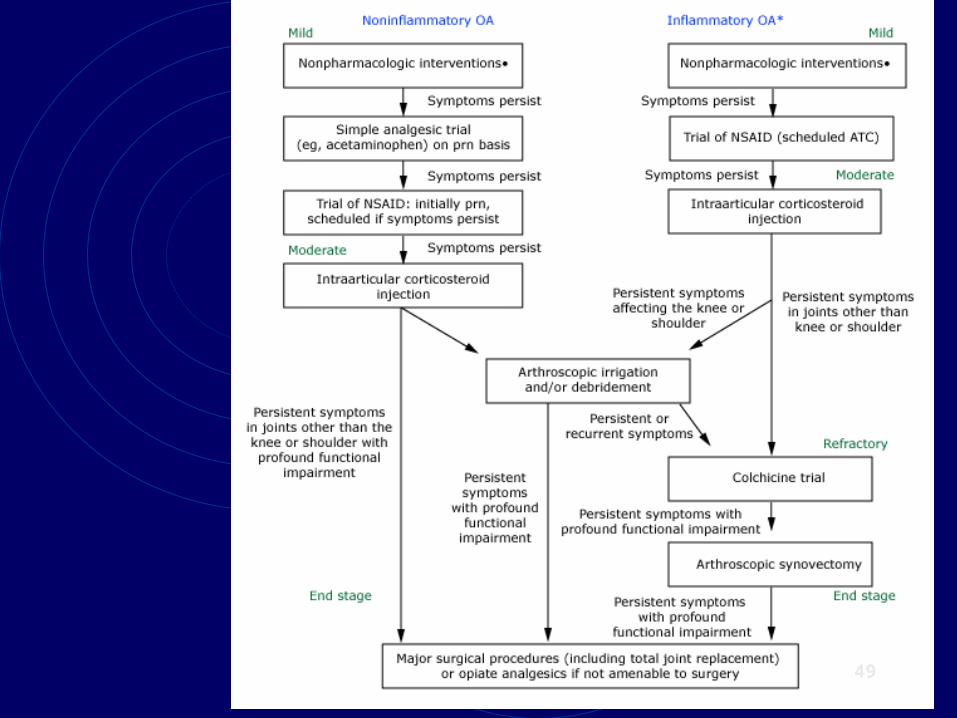
ACR 2000 Guidlines-Drug Therapy Options in Osteoarthritis
Baseline program(Weight loss/exercise)
Mild/moderate Moderate/severePain pain/inflammation
Acetaminophen Steroids IA COX-2 specific Inhibitors
NSAIDs Hyaluronans Traditional NSAIDs Tramadol (plus gastroprotection)
Propoxyphene Opioids
Surgery
40
TREATMENT
1. Conservative
2. Operative.
Reduce the symptoms / pain, improve joint function, reduce the progress, and improve quality of life
41
CONSERVATIVE
Pharmacogenic :
1. NSAID
2. Cox 2 inhibitor
3. Intra articular injection: hyaluronic acid, analgesic. steroid
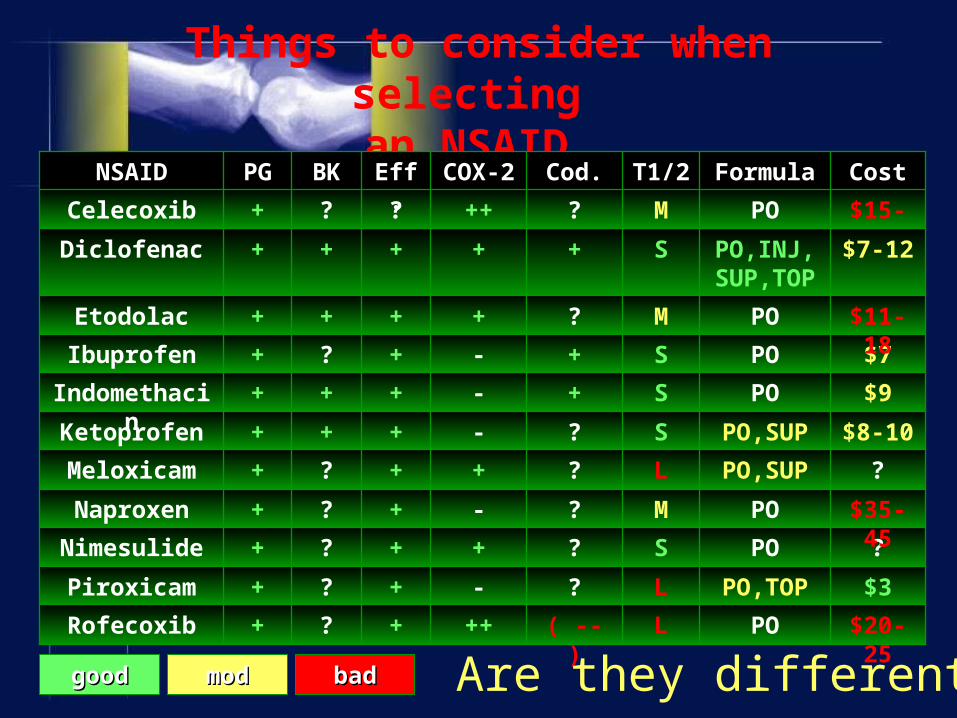
Things to consider when selecting an NSAID
PO
PO,TOP
PO
PO
PO,SUP
PO,SUP
PO
PO
PO
PO,INJ, SUP,TOP
PO
Formula
+
+
+
+
+
+
+
+
+
+
?
Eff.
$15-20M?++?+Celecoxib
$7-12S++++Diclofenac
$20-25L( -- )++?+Rofecoxib
$3L?-?+Piroxicam
?S?+?+Nimesulide
$35-45M?-?+Naproxen
?L?+?+Meloxicam
$8-10S?-++Ketoprofen
$9S+-++Indomethacin
$7S+-?+Ibuprofen
$11-18M?+++Etodolac
CostT1/2Cod.COX-2BKPGNSAID
Are they different?goodgood modmod badbad
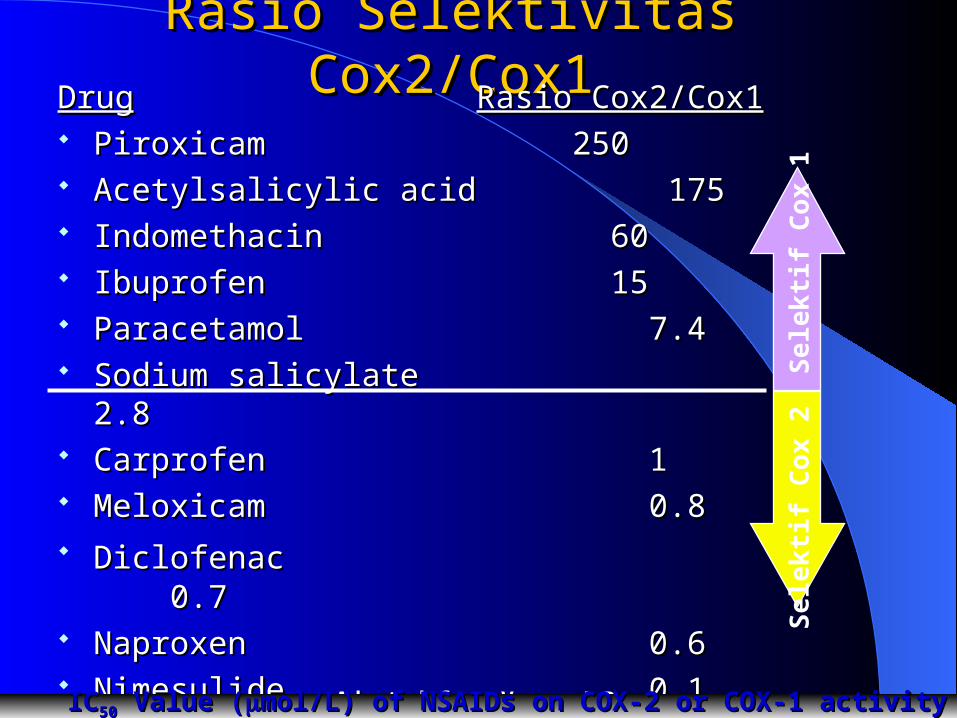
Rasio Selektivitas Rasio Selektivitas Cox2/Cox1Cox2/Cox1DrugDrug Rasio Cox2/Cox1Rasio Cox2/Cox1
PiroxicamPiroxicam 250250 Acetylsalicylic acidAcetylsalicylic acid 175175 IndomethacinIndomethacin 60 60 IbuprofenIbuprofen 15 15 ParacetamolParacetamol 7.4 7.4 Sodium salicylateSodium salicylate 2.8 2.8 CarprofenCarprofen 1 1 MeloxicamMeloxicam 0.8 0.8 DiclofenacDiclofenac 0.70.7 NaproxenNaproxen 0.6 0.6 NimesulideNimesulide 0.1 0.1 ROFECOXIBE ROFECOXIBE 0.020.02
Se
lek
tif
Co
x 2
Se
lek
tif
Co
x 1
Adapted from Vane, J.R.Adapted from Vane, J.R. ICIC5050 Value ( Value (mol/L) of NSAIDs on COX-2 or COX-1 activity in intact cellsmol/L) of NSAIDs on COX-2 or COX-1 activity in intact cells
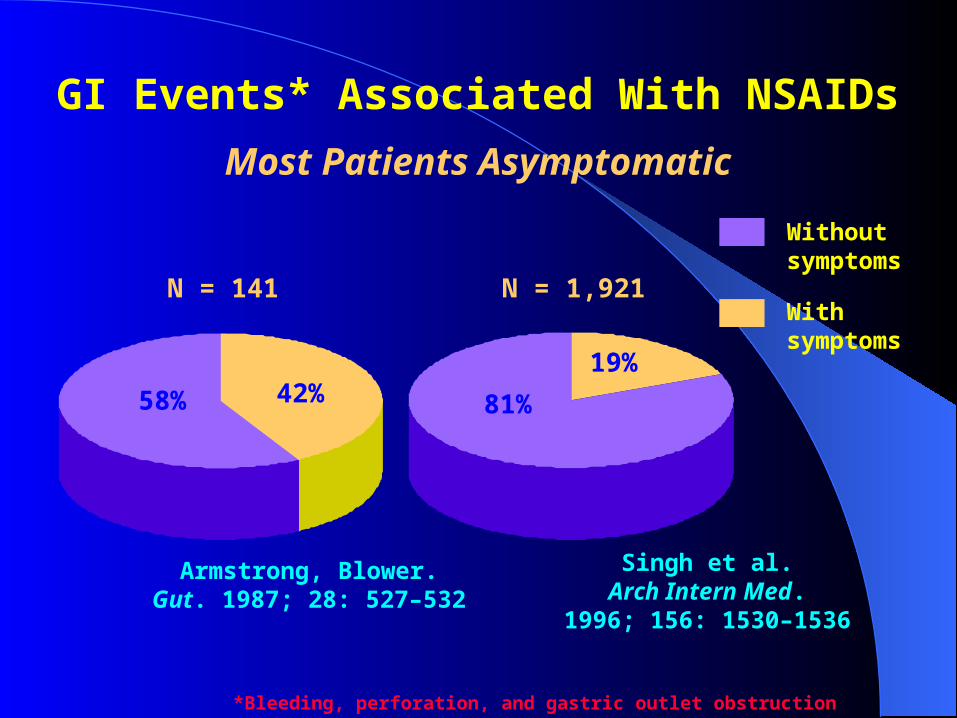
GI Events* Associated With NSAIDs
Most Patients Asymptomatic
N = 141 N = 1,921
Armstrong, Blower.Gut. 1987; 28: 527–532
Singh et al.Arch Intern Med.
1996; 156: 1530–1536
Withoutsymptoms
Withsymptoms
42%58% 81%
19%
*Bleeding, perforation, and gastric outlet obstruction
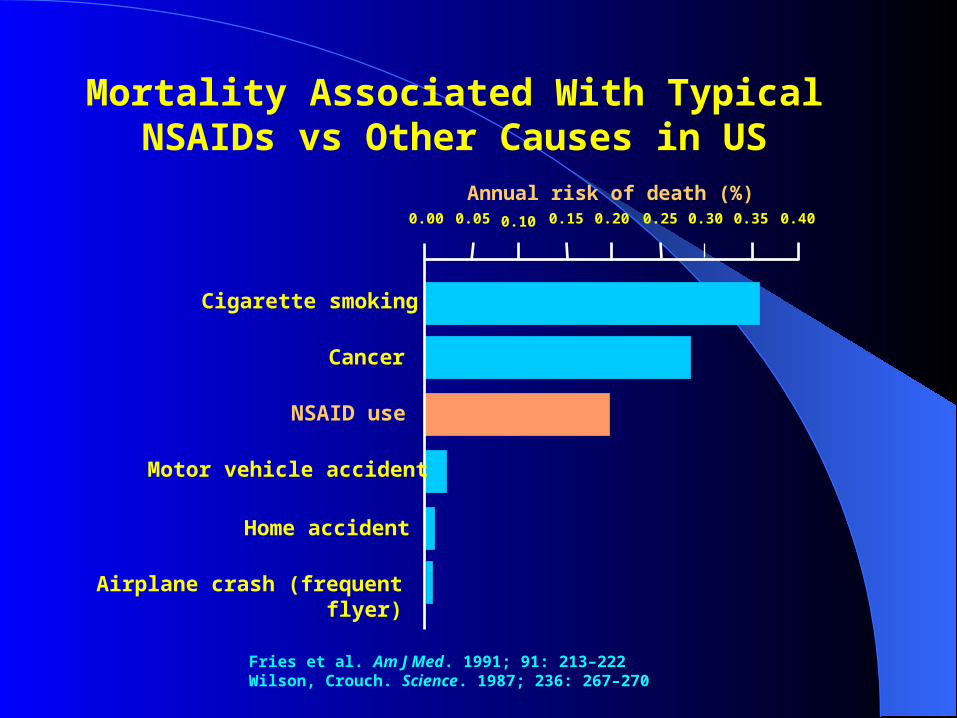
Mortality Associated With TypicalNSAIDs vs Other Causes in US
Fries et al. Am J Med. 1991; 91: 213–222Wilson, Crouch. Science. 1987; 236: 267–270
Annual risk of death (%)0.250.200.150.100.050.00 0.400.350.30
Cigarette smoking
Cancer
NSAID use
Motor vehicle accident
Home accident
Airplane crash (frequent flyer)
49
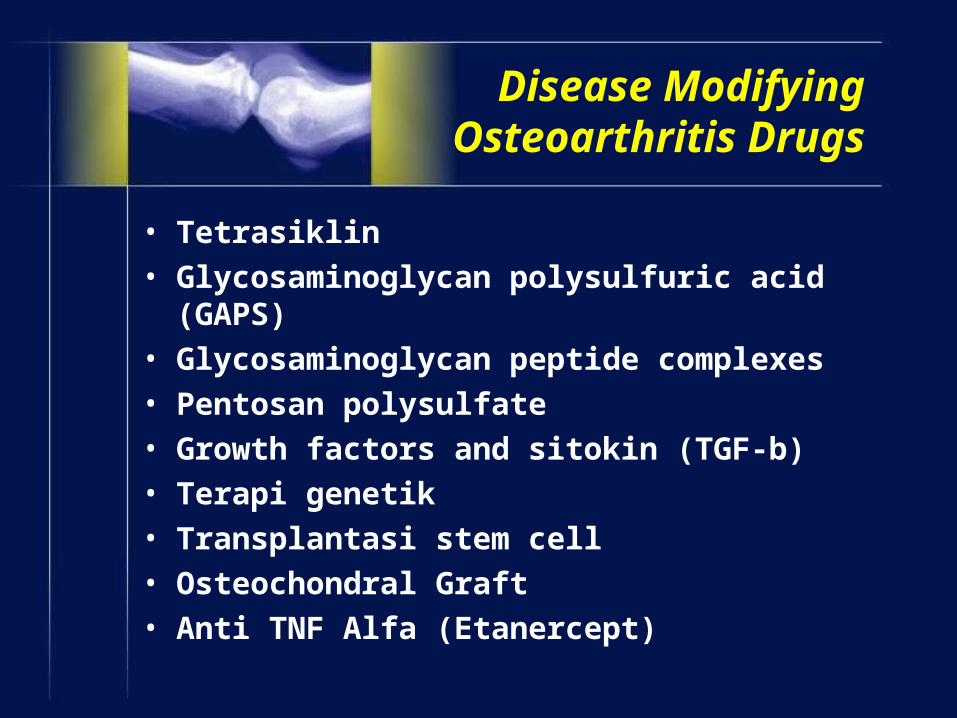
Disease Modifying Osteoarthritis Drugs
• Tetrasiklin
• Glycosaminoglycan polysulfuric acid (GAPS)
• Glycosaminoglycan peptide complexes
• Pentosan polysulfate
• Growth factors and sitokin (TGF-b)
• Terapi genetik
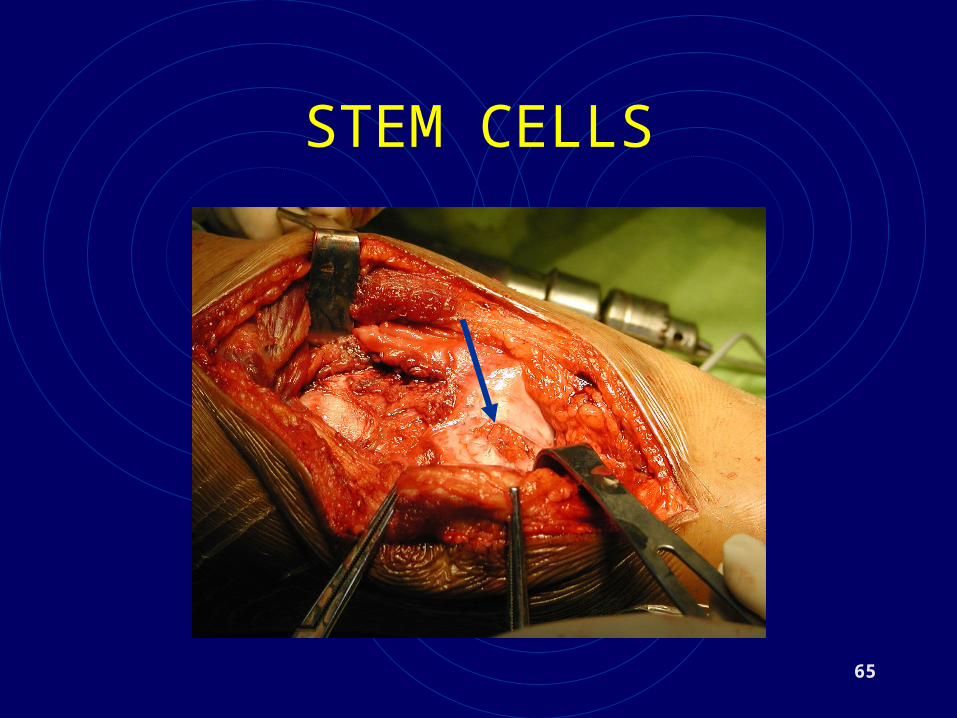
• Transplantasi stem cell
• Osteochondral Graft
• Anti TNF Alfa (Etanercept)
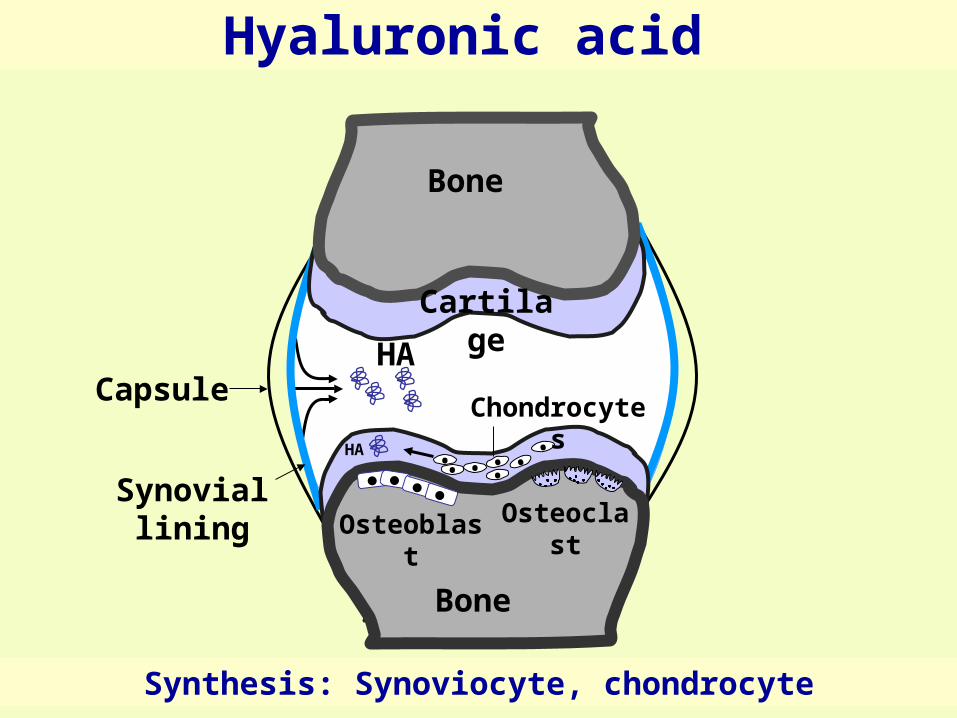
Hyaluronic acid Hyaluronic acid
Bone
Bone
•• • •• •
•
Cartilage
OsteoclastOsteoblast
Chondrocytes
HA
HA
Synovial lining
Capsule
Synthesis: Synoviocyte, chondrocyte
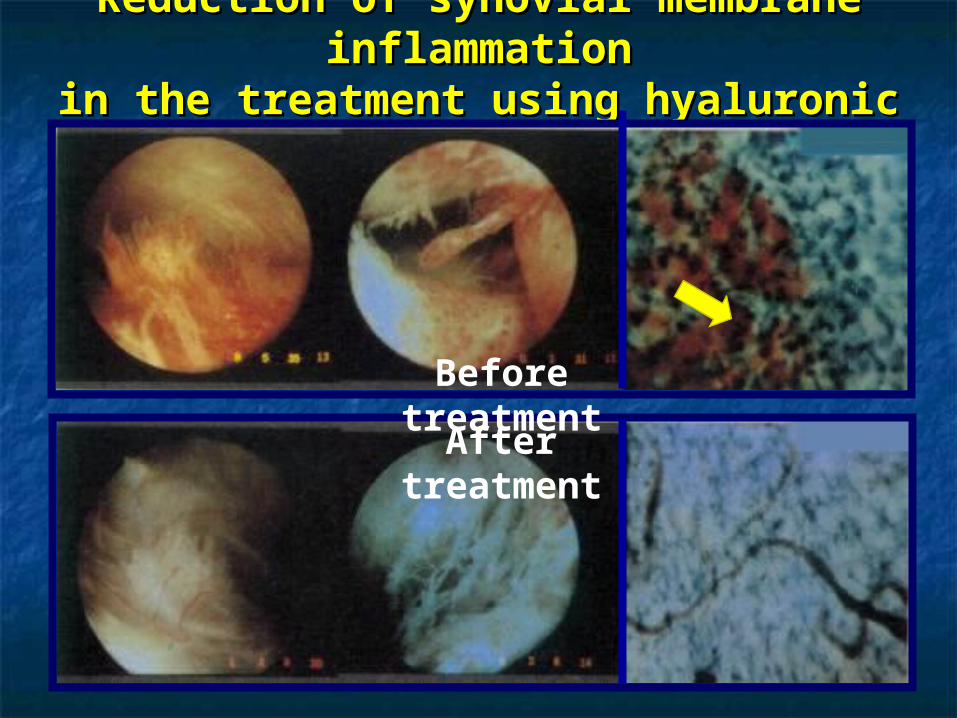
Reduction of synovial membrane inflammationReduction of synovial membrane inflammationin the treatment using hyaluronic acidin the treatment using hyaluronic acid
Before treatment
After treatment
54
OPERATIVE
1. Arthroscopy : lavage, shaving, drilling.
2. Osteotomy
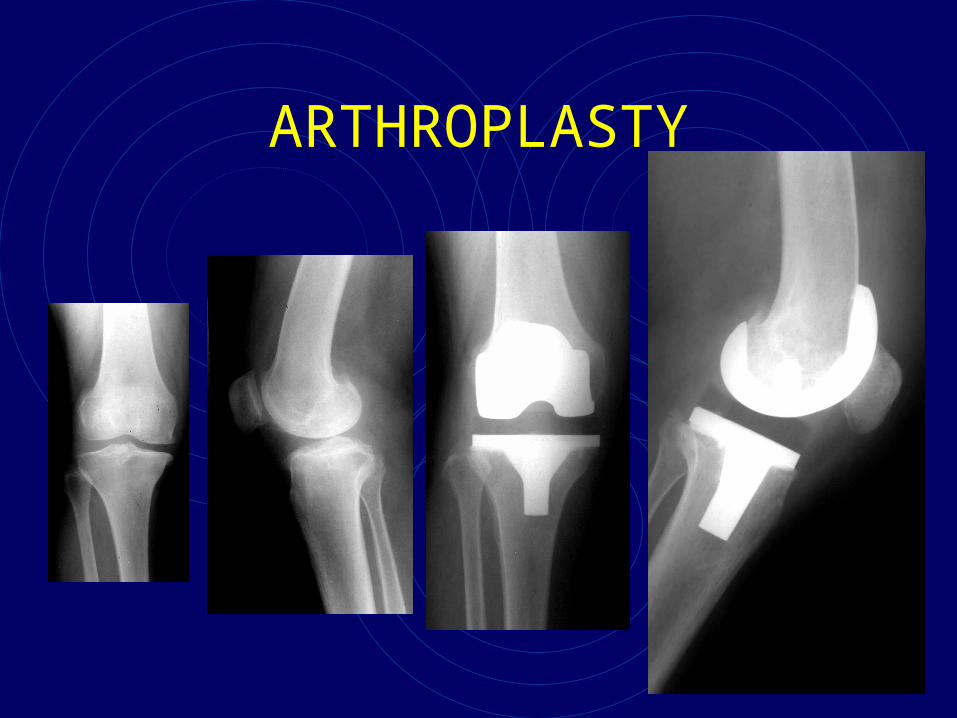
3. Arthroplasty
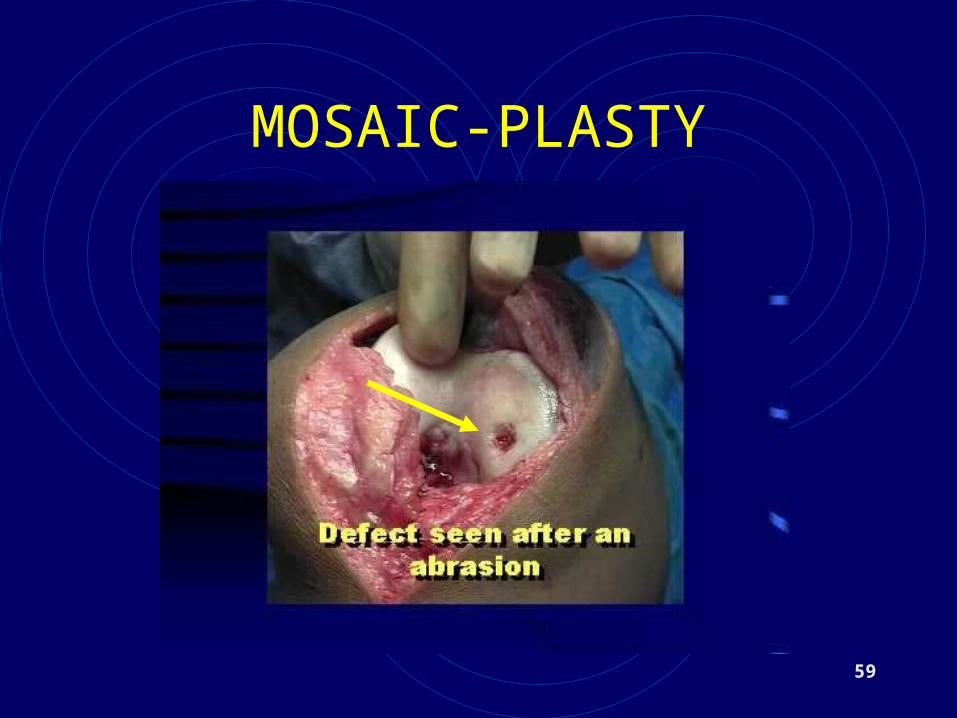
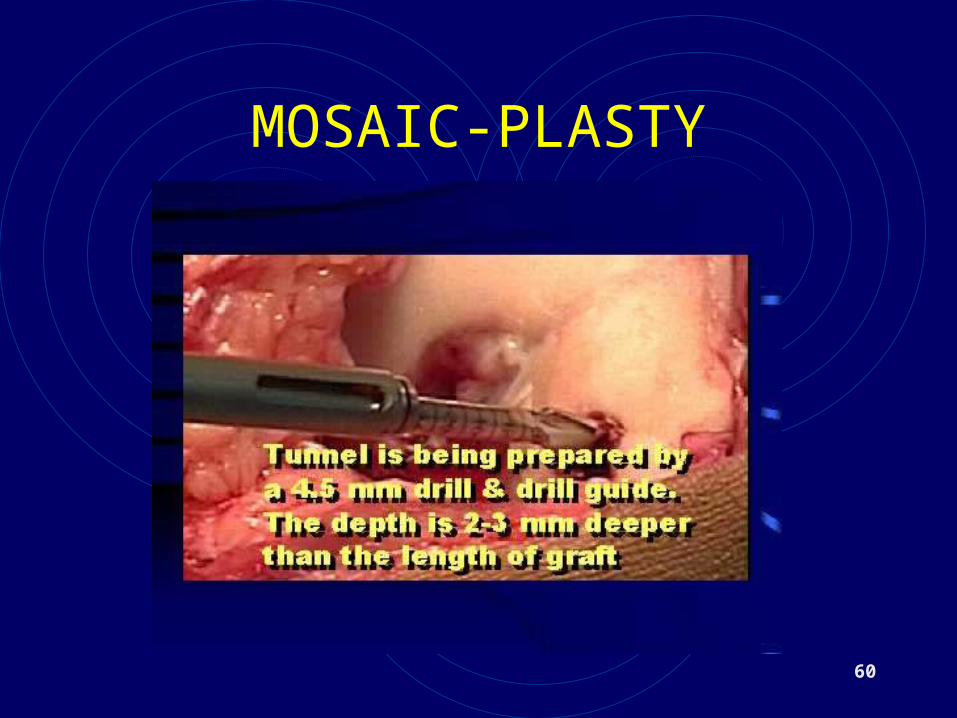
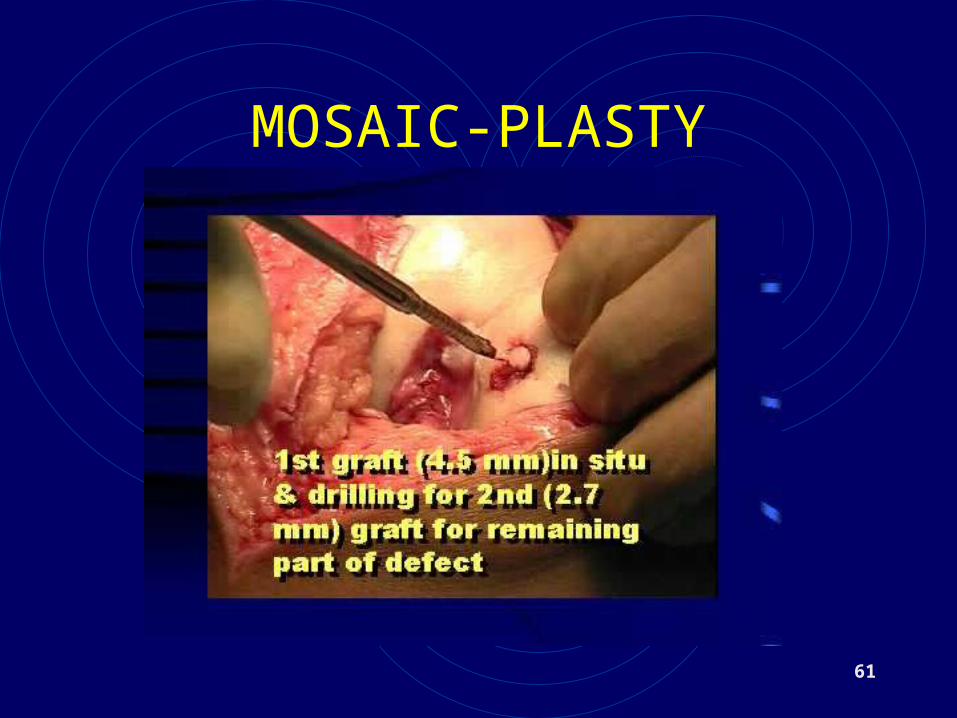
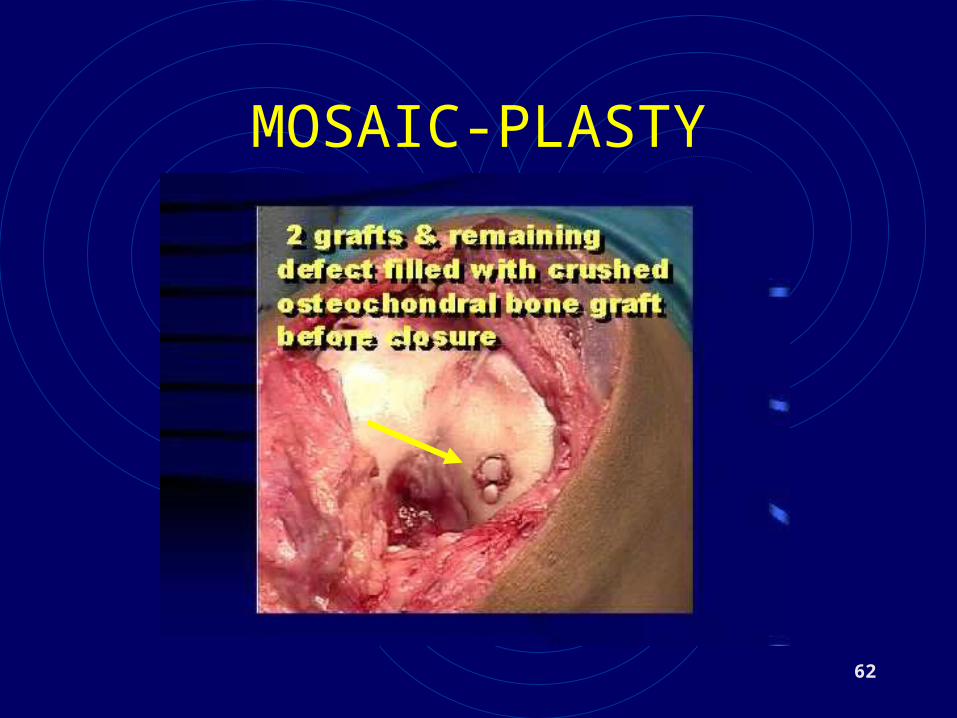
4. Mozaic graft
5. Stem cell graft
55
ARTHROSCOPY
56
ARTHROSCOPY
57
ARTHROSCOPY

58
OSTEOTOMY
59
MOSAIC-PLASTY
60
MOSAIC-PLASTY
61
MOSAIC-PLASTY
62
MOSAIC-PLASTY
63
ARTHROPLASTY

64
ARTHROPLASTY
65
STEM CELLS
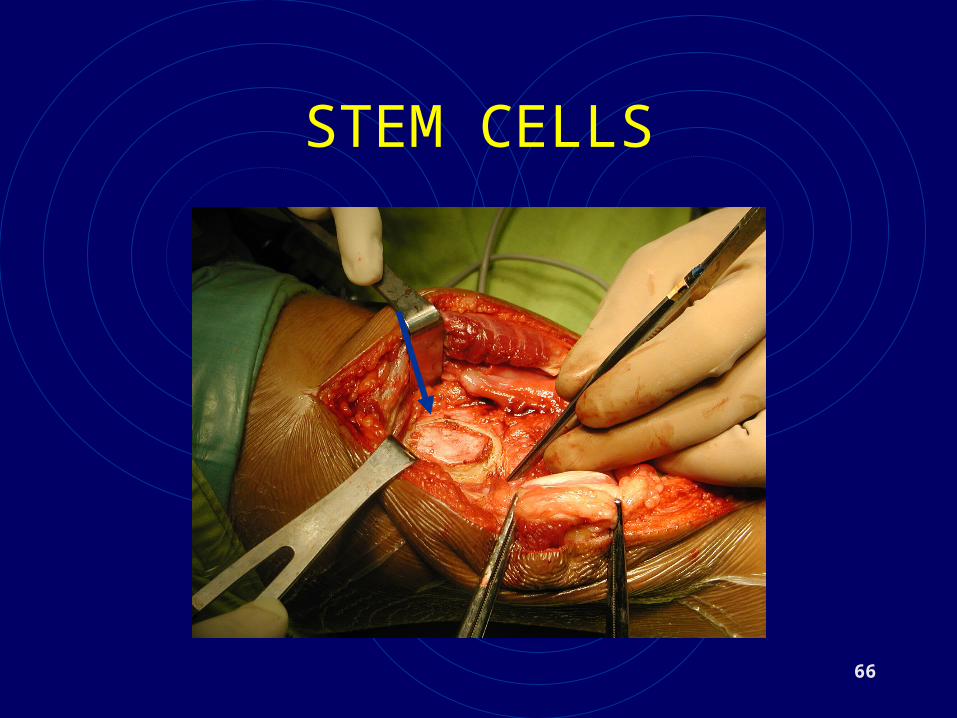
66
STEM CELLS
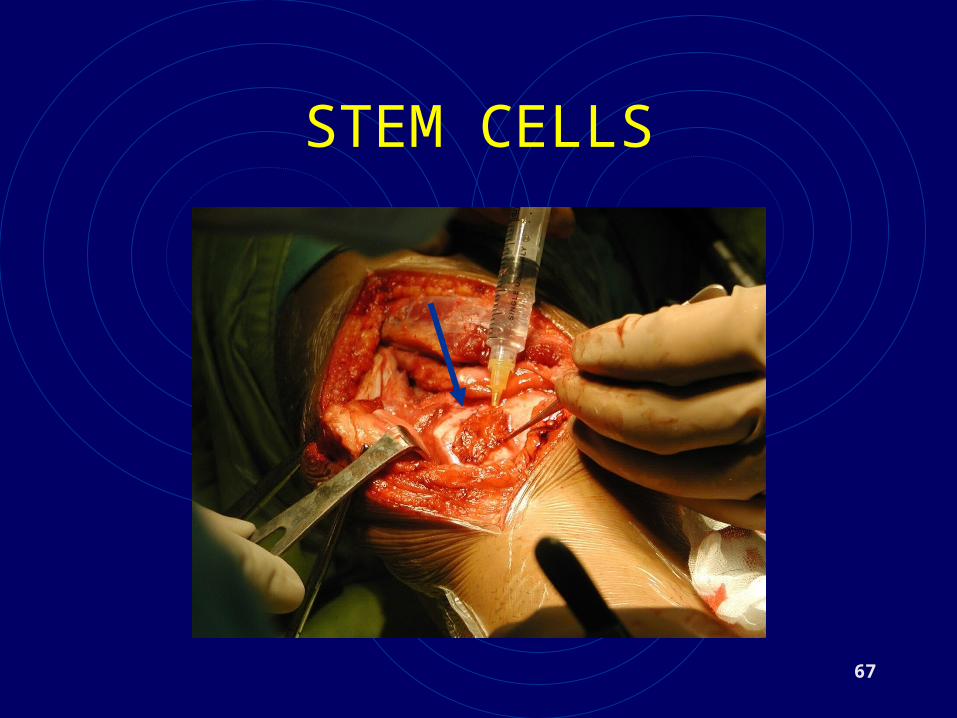
67
STEM CELLS
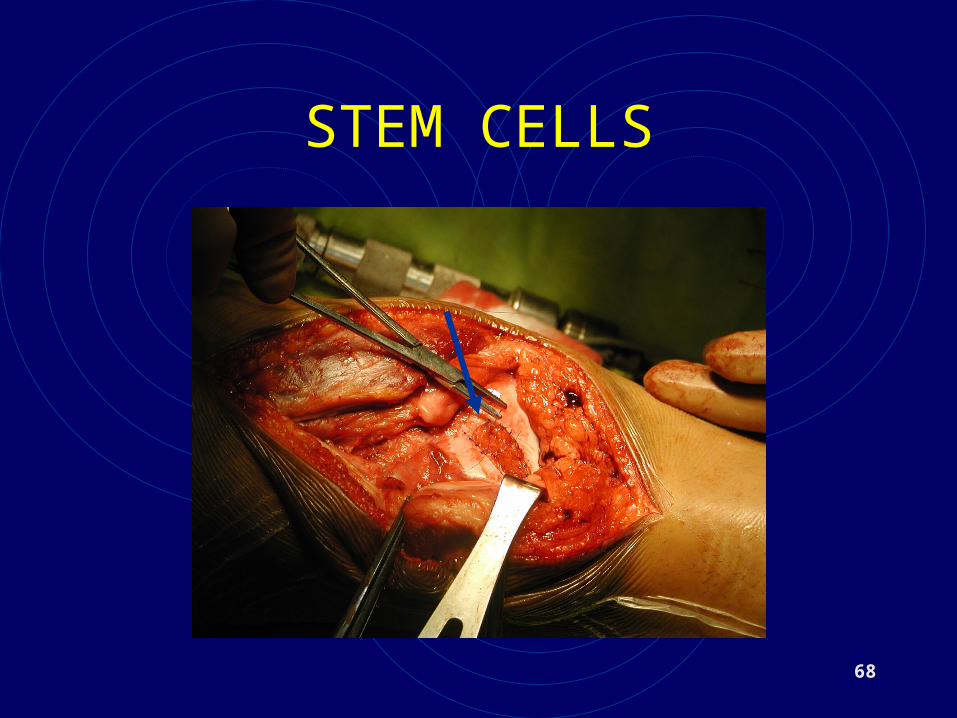
68
STEM CELLS

benefitbenefitriskrisk
Measures the risk and benefit for your patients
ALHAMDULILLAH
TERIMA KASIH
70
Recommended

















