SAGE meeting – April 2014
Dr Sir Andrew Hall
Senior visiting Scientist
IARC
Optimizing Human
Papilloma Virus
immunization
schedules
Why are we reviewing the evidence
on schedules for HPV vaccines?
Emerging evidence on effect of < 3-dose
schedules
Opportunities to facilitate delivery and increase
coverage
Potential to reduce costs (vaccine and delivery)
Sources of DATA
1. Data presented during the Ad hoc Expert Consultation on Human
Papilloma Virus Vaccine schedules organized in Geneva, November
18, 2013.
2. Results from a systematic review conducted by an independent team
of Investigators.
HPV vaccines: review of alternative vaccination schedules
(D’Addario M et al 2014)1.
3. Results from non-systematic review of the data from observational
studies.
4. EMA- Report: The bivalent vaccine received approval for a pre-
adolescent and adolescent indication to allow for administration of the
vaccine according to an alternative 2-dose schedule (0, 6 months) in
females aged 9-14 years old.
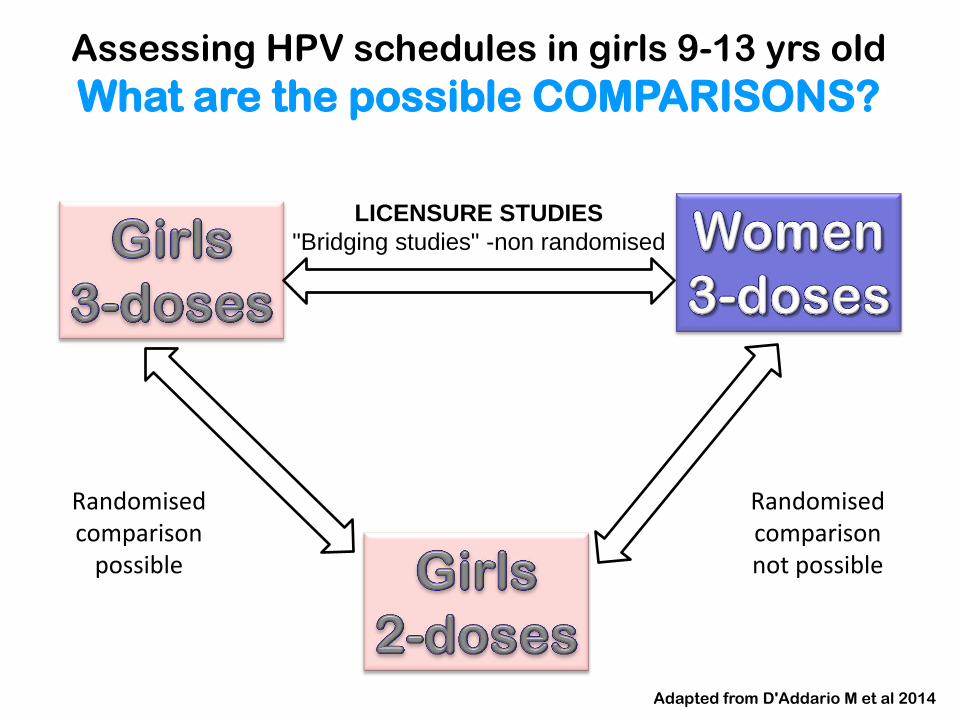
Assessing HPV schedules in girls 9-13 yrs old
What are the possible COMPARISONS?
LICENSURE STUDIES
"Bridging studies" -non randomised
Randomised comparison
possible
Randomised comparison not possible
Adapted from D'Addario M et al 2014
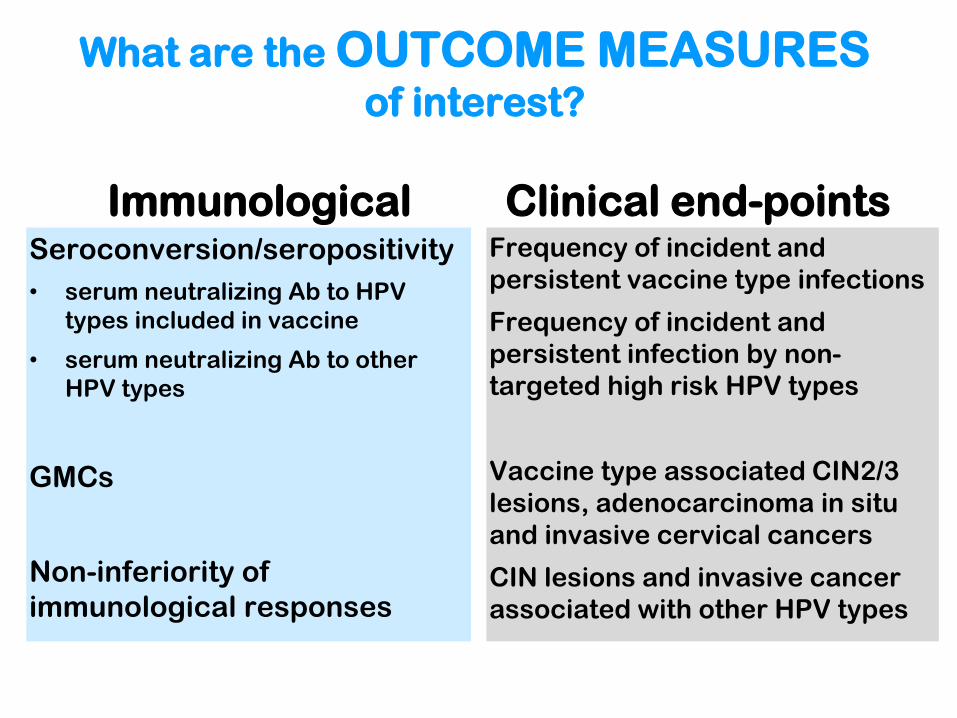
What are the OUTCOME MEASURES of interest?
Immunological Seroconversion/seropositivity
• serum neutralizing Ab to HPV
types included in vaccine
• serum neutralizing Ab to other
HPV types
GMCs
Non-inferiority of
immunological responses
Clinical end-points Frequency of incident and
persistent vaccine type infections
Frequency of incident and
persistent infection by non-
targeted high risk HPV types
Vaccine type associated CIN2/3
lesions, adenocarcinoma in situ
and invasive cervical cancers
CIN lesions and invasive cancer
associated with other HPV types
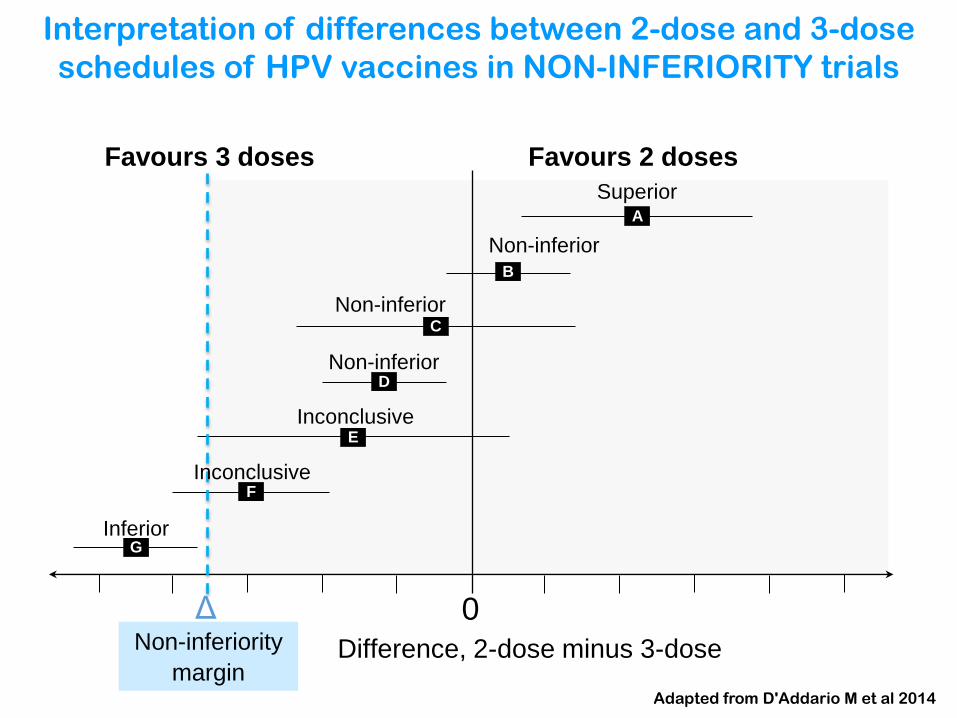
Favours 3 doses Favours 2 doses
A
B
C
D
E
F
G
Superior
Non-inferior
Non-inferior
Non-inferior
Inferior
Inconclusive
Inconclusive
Δ
Difference, 2-dose minus 3-dose Non-inferiority
margin
0
Interpretation of differences between 2-dose and 3-dose
schedules of HPV vaccines in NON-INFERIORITY trials
Adapted from D'Addario M et al 2014
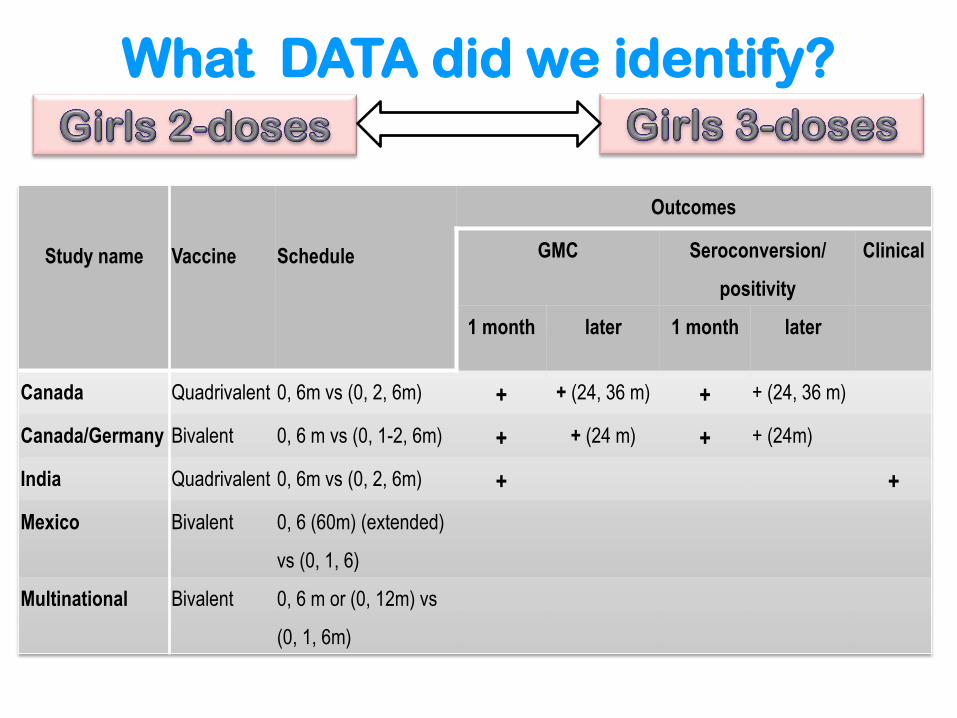
What DATA did we identify?
Study name
Vaccine
Schedule
Outcomes
GMC Seroconversion/
positivity
Clinical
1 month later 1 month later
Canada Quadrivalent 0, 6m vs (0, 2, 6m) + + (24, 36 m) + + (24, 36 m)
Canada/Germany Bivalent 0, 6 m vs (0, 1-2, 6m) + + (24 m) + + (24m)
India Quadrivalent 0, 6m vs (0, 2, 6m) + +
Mexico Bivalent 0, 6 (60m) (extended)
vs (0, 1, 6)
Multinational Bivalent 0, 6 m or (0, 12m) vs
(0, 1, 6m)
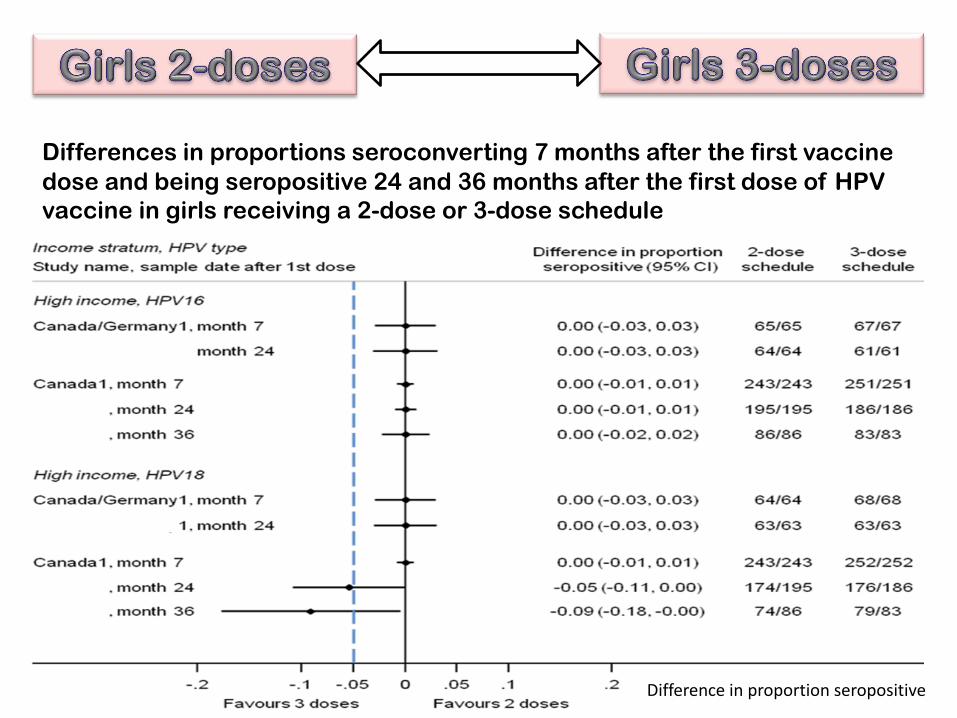
Differences in proportions seroconverting 7 months after the first vaccine
dose and being seropositive 24 and 36 months after the first dose of HPV
vaccine in girls receiving a 2-dose or 3-dose schedule
Difference in proportion seropositive
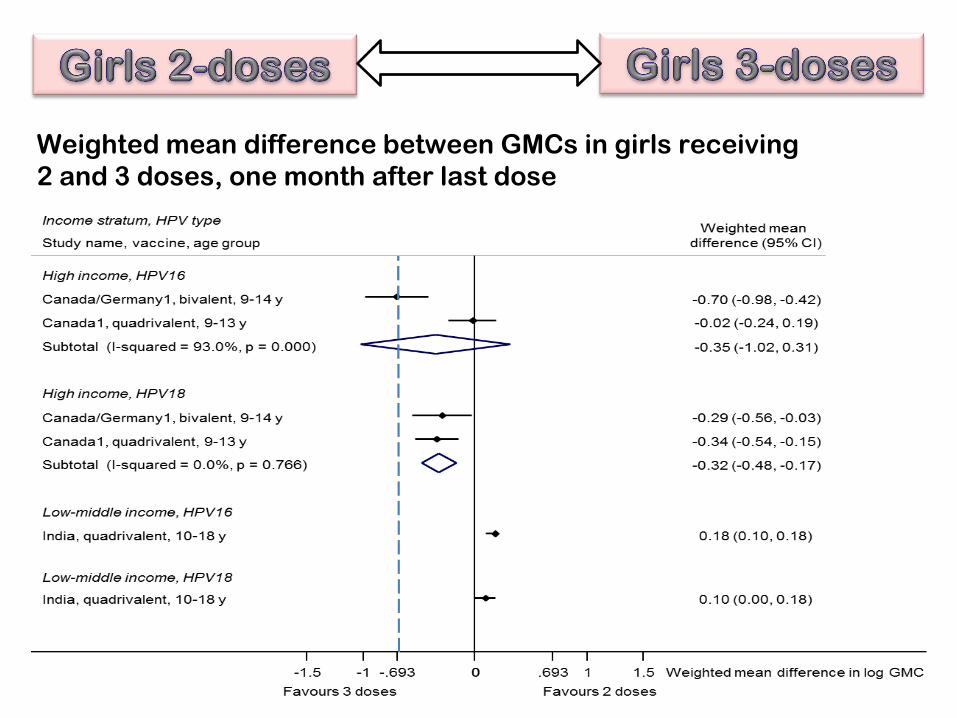
Weighted mean difference between GMCs in girls receiving
2 and 3 doses, one month after last dose
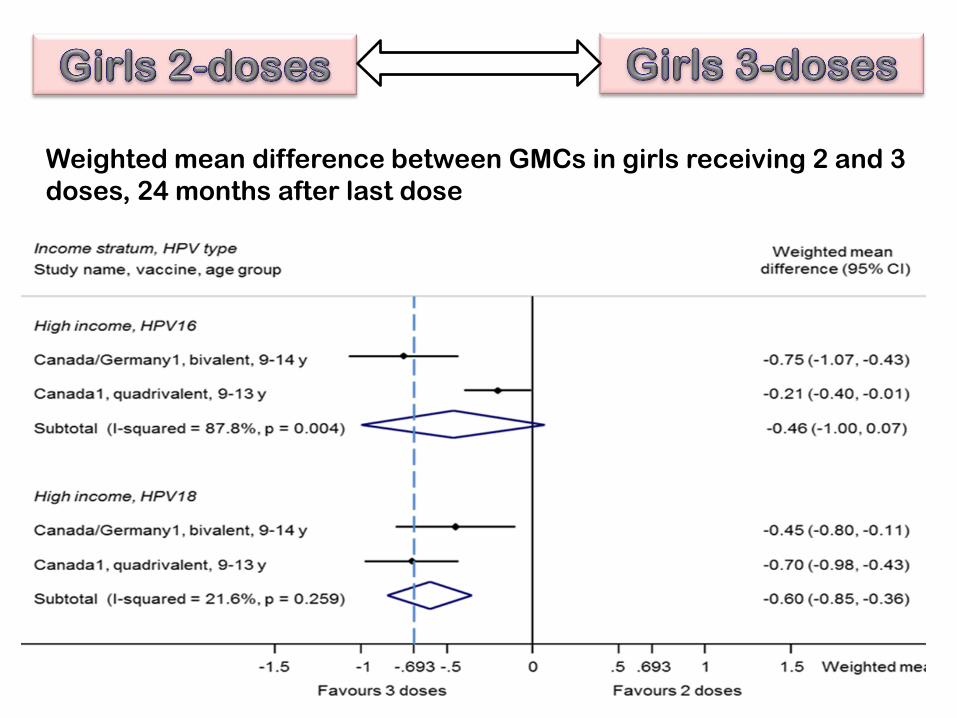
Weighted mean difference between GMCs in girls receiving 2 and 3
doses, 24 months after last dose
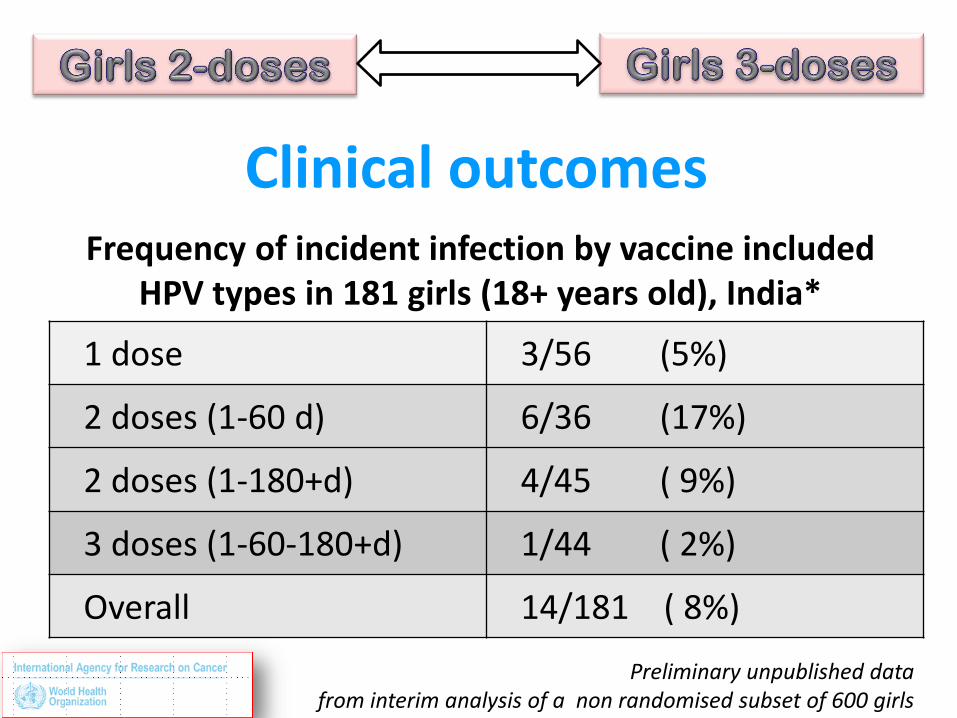
Clinical outcomes
1 dose 3/56 (5%)
2 doses (1-60 d) 6/36 (17%)
2 doses (1-180+d) 4/45 ( 9%)
3 doses (1-60-180+d) 1/44 ( 2%)
Overall 14/181 ( 8%)
Frequency of incident infection by vaccine included HPV types in 181 girls (18+ years old), India*
Preliminary unpublished data from interim analysis of a non randomised subset of 600 girls
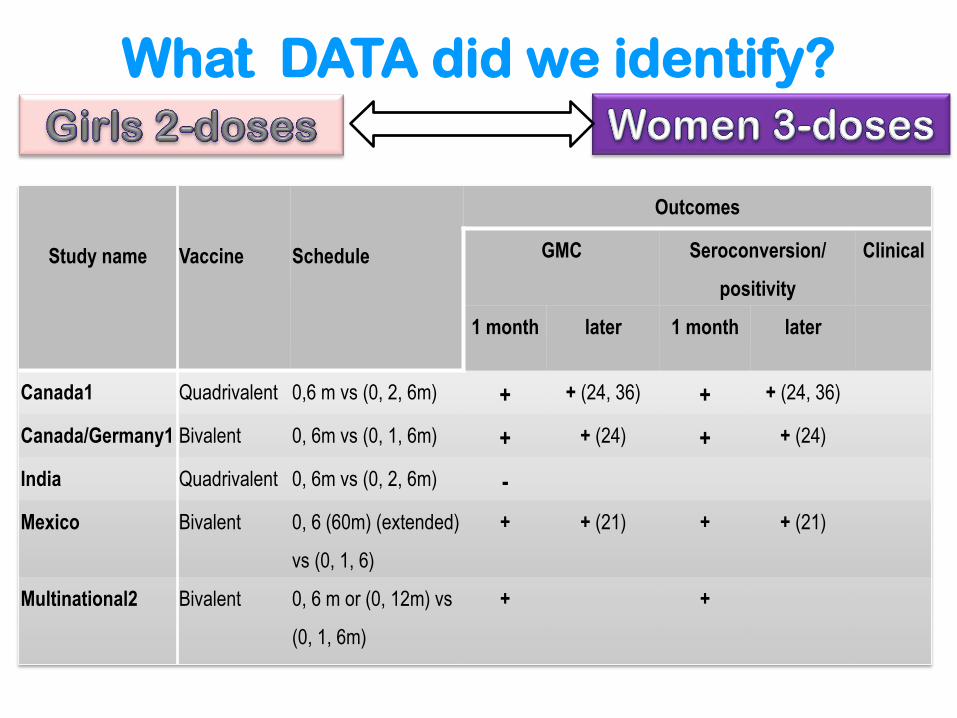
What DATA did we identify?
Study name
Vaccine
Schedule
Outcomes
GMC Seroconversion/
positivity
Clinical
1 month later 1 month later
Canada1 Quadrivalent 0,6 m vs (0, 2, 6m) + + (24, 36) + + (24, 36)
Canada/Germany1 Bivalent 0, 6m vs (0, 1, 6m) + + (24) + + (24)
India Quadrivalent 0, 6m vs (0, 2, 6m) -
Mexico Bivalent 0, 6 (60m) (extended)
vs (0, 1, 6)
+ + (21) + + (21)
Multinational2 Bivalent
0, 6 m or (0, 12m) vs
(0, 1, 6m)
+ +
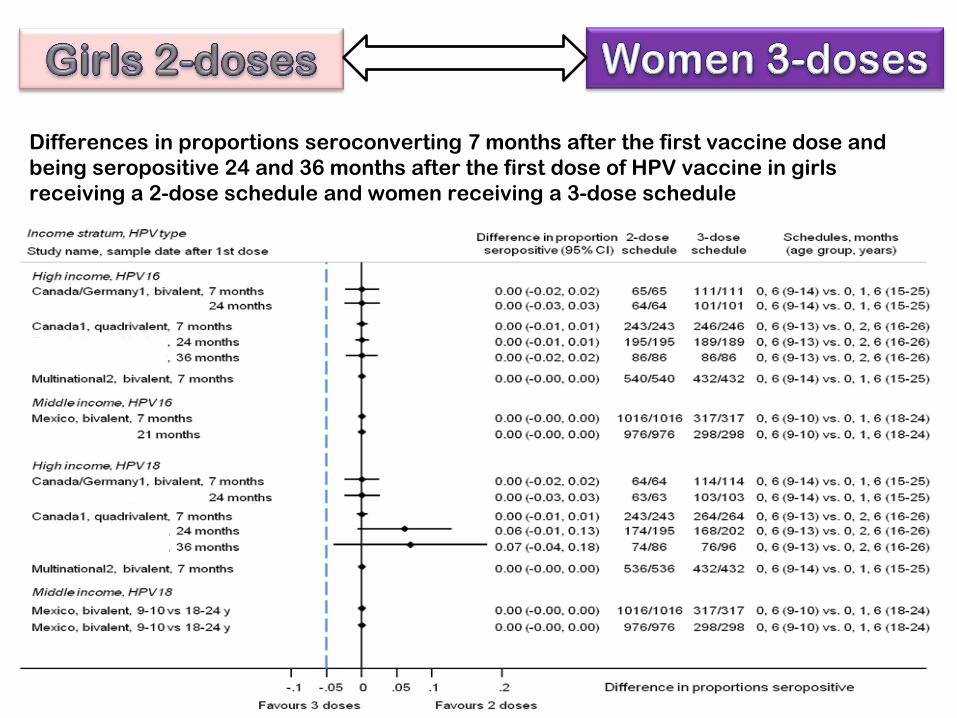
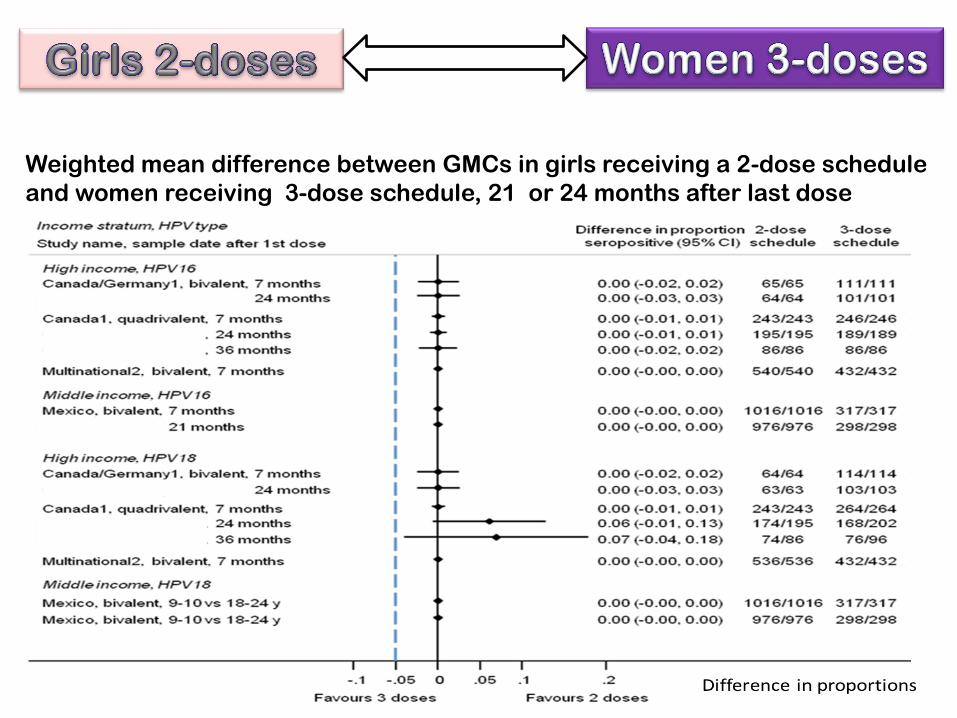
Differences in proportions seroconverting 7 months after the first vaccine dose and
being seropositive 24 and 36 months after the first dose of HPV vaccine in girls
receiving a 2-dose schedule and women receiving a 3-dose schedule
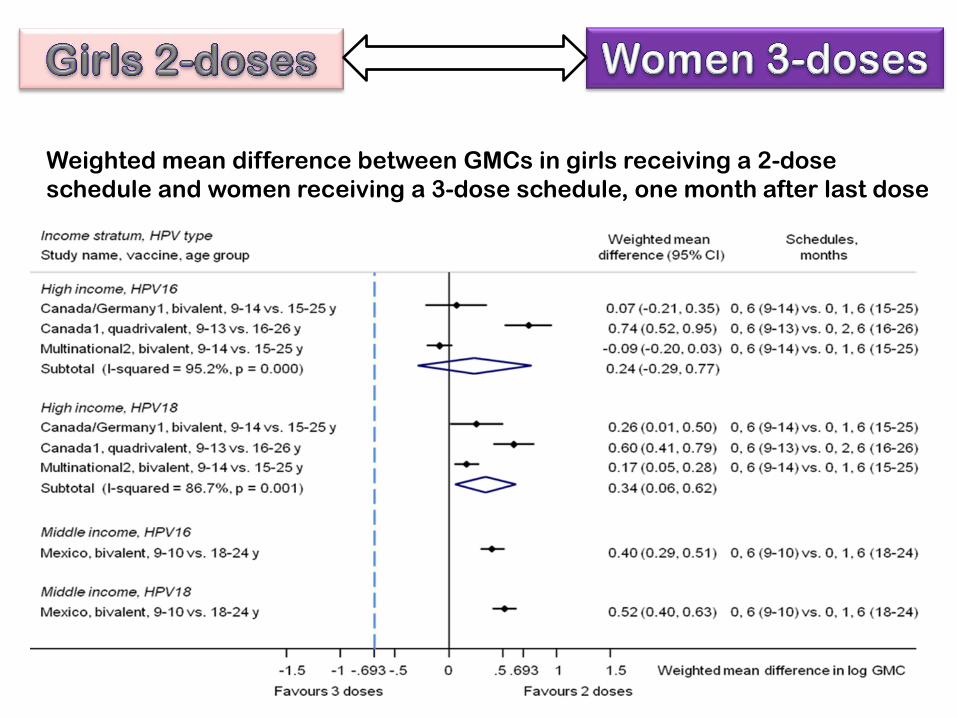
Weighted mean difference between GMCs in girls receiving a 2-dose
schedule and women receiving a 3-dose schedule, one month after last dose
Weighted mean difference between GMCs in girls receiving a 2-dose schedule
and women receiving 3-dose schedule, 21 or 24 months after last dose
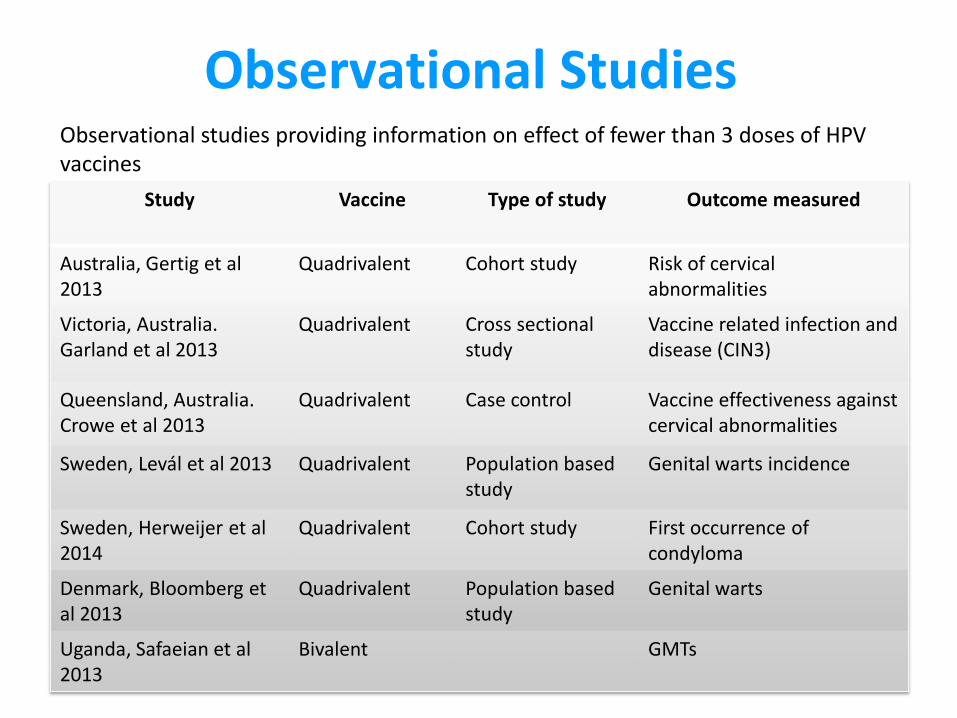
Observational Studies Observational studies providing information on effect of fewer than 3 doses of HPV vaccines
Study
Vaccine
Type of study Outcome measured
Australia, Gertig et al 2013
Quadrivalent Cohort study Risk of cervical abnormalities
Victoria, Australia. Garland et al 2013
Quadrivalent Cross sectional study
Vaccine related infection and disease (CIN3)
Queensland, Australia. Crowe et al 2013
Quadrivalent Case control Vaccine effectiveness against cervical abnormalities
Sweden, Levál et al 2013 Quadrivalent Population based study
Genital warts incidence
Sweden, Herweijer et al 2014
Quadrivalent Cohort study First occurrence of condyloma
Denmark, Bloomberg et al 2013
Quadrivalent Population based study
Genital warts
Uganda, Safaeian et al 2013
Bivalent GMTs
Observational Studies
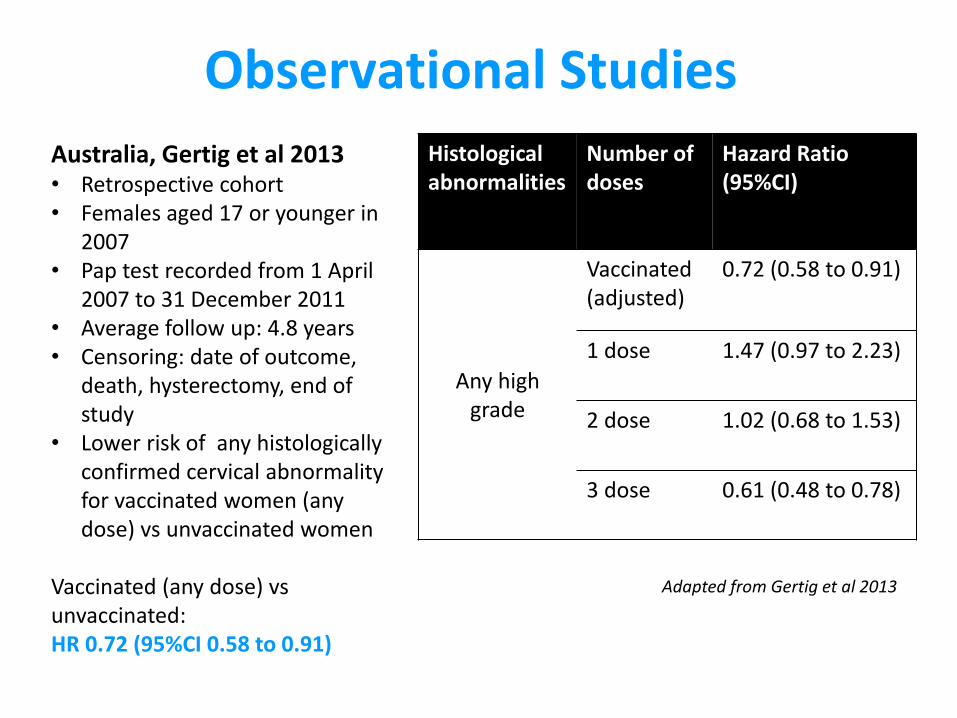
Australia, Gertig et al 2013 • Retrospective cohort • Females aged 17 or younger in
2007 • Pap test recorded from 1 April
2007 to 31 December 2011 • Average follow up: 4.8 years • Censoring: date of outcome,
death, hysterectomy, end of study
• Lower risk of any histologically confirmed cervical abnormality for vaccinated women (any dose) vs unvaccinated women
Vaccinated (any dose) vs unvaccinated: HR 0.72 (95%CI 0.58 to 0.91)
Histological abnormalities
Number of doses
Hazard Ratio (95%CI)
Any high grade
Vaccinated (adjusted)
0.72 (0.58 to 0.91)
1 dose 1.47 (0.97 to 2.23)
2 dose 1.02 (0.68 to 1.53)
3 dose 0.61 (0.48 to 0.78)
Adapted from Gertig et al 2013
Observational Studies Victoria, Australia, Garland et al 2013
• Cross sectional study
Sub study A
• Women 18-25 years (81% fully vaccinated)
• Questionnaire and Self collected vaginal swab
• HPV vaccine-related infection and disease (CIN3)
• Prevalence (interim analysis)
• HPV 16 was 1.6% (95 CI 0.6 to 3.5)
• Any high risk type 14.4% (95 CI 11 to 18.4)
• No HPV 18 detected
Observational Studies Queensland, Australia, Crowe et al 2014
• Case control study
• Females aged 12-26 years in 2007
• First cervical smear test between April 2007 and March 2011
• 3 doses vs no vaccination
• VE 3 doses High grade cases 46% (33-67) Other 34% (30-38)
• VE 2 doses High grade cases 21% (2-36) Other 21% (5-26)
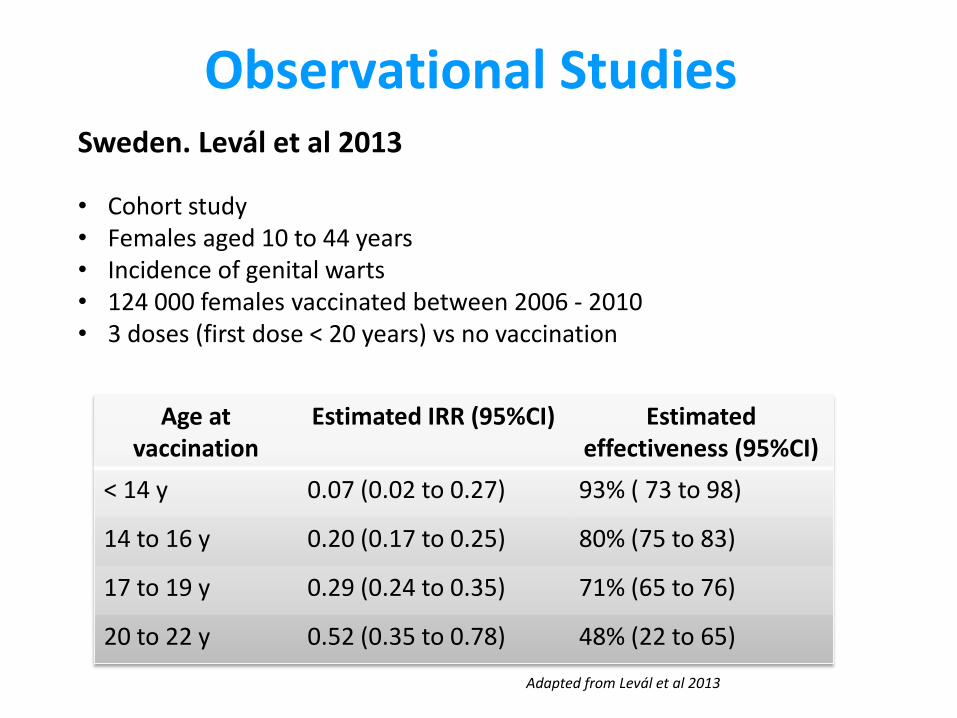
Observational Studies Sweden. Levál et al 2013
• Cohort study • Females aged 10 to 44 years • Incidence of genital warts • 124 000 females vaccinated between 2006 - 2010 • 3 doses (first dose < 20 years) vs no vaccination
Age at vaccination
Estimated IRR (95%CI) Estimated effectiveness (95%CI)
< 14 y 0.07 (0.02 to 0.27) 93% ( 73 to 98)
14 to 16 y 0.20 (0.17 to 0.25) 80% (75 to 83)
17 to 19 y 0.29 (0.24 to 0.35) 71% (65 to 76)
20 to 22 y 0.52 (0.35 to 0.78) 48% (22 to 65)
Adapted from Levál et al 2013
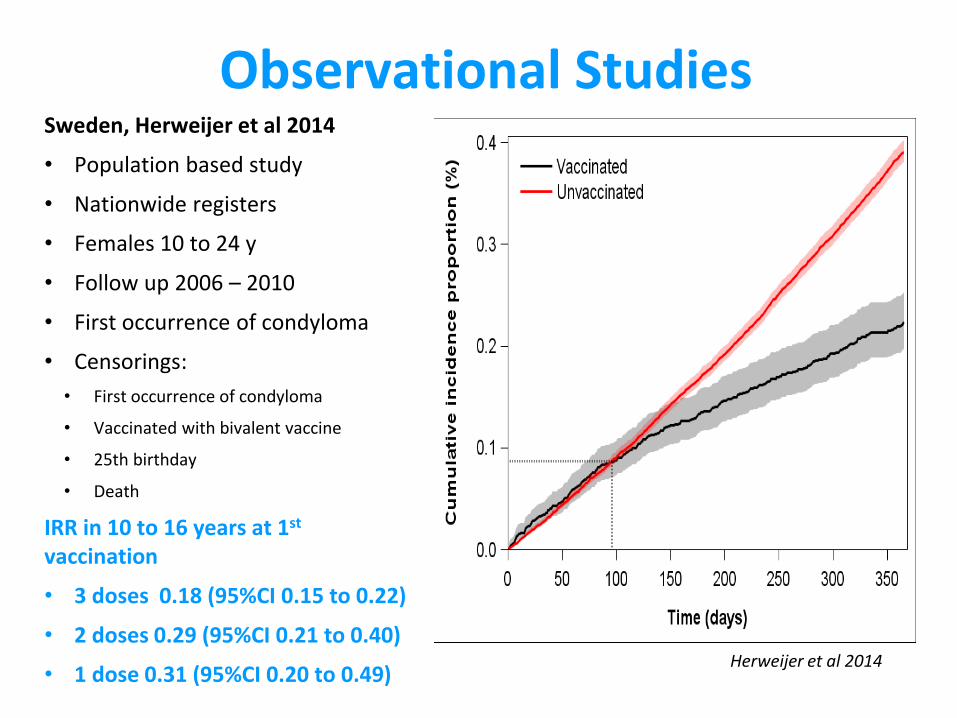
Observational Studies Sweden, Herweijer et al 2014
• Population based study
• Nationwide registers
• Females 10 to 24 y
• Follow up 2006 – 2010
• First occurrence of condyloma
• Censorings:
• First occurrence of condyloma
• Vaccinated with bivalent vaccine
• 25th birthday
• Death
IRR in 10 to 16 years at 1st vaccination
• 3 doses 0.18 (95%CI 0.15 to 0.22)
• 2 doses 0.29 (95%CI 0.21 to 0.40)
• 1 dose 0.31 (95%CI 0.20 to 0.49) Herweijer et al 2014
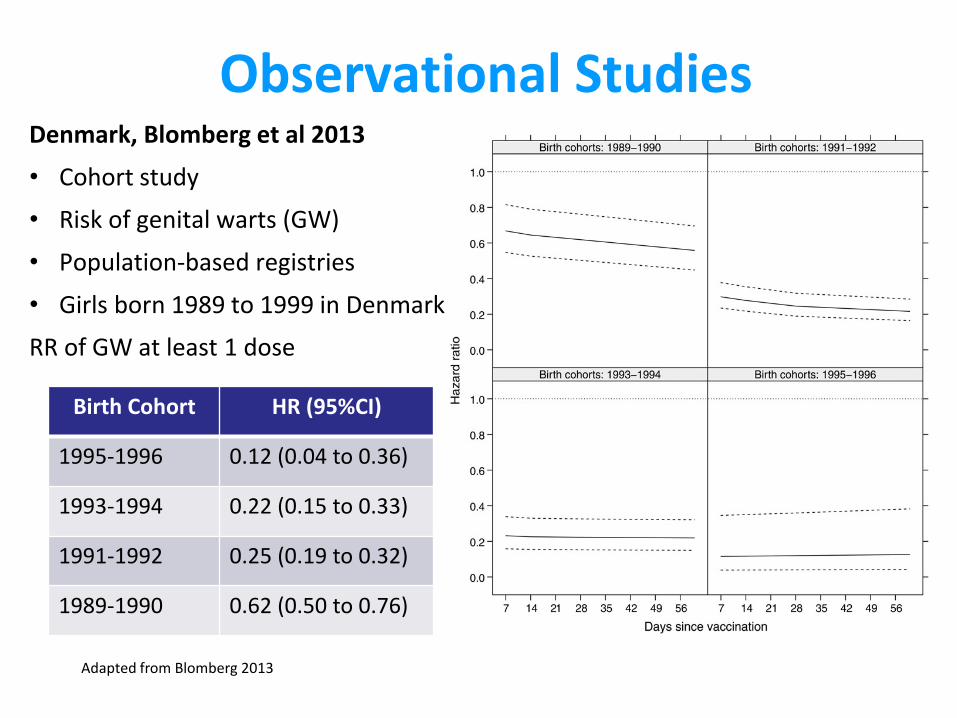
Observational Studies Denmark, Blomberg et al 2013
• Cohort study
• Risk of genital warts (GW)
• Population-based registries
• Girls born 1989 to 1999 in Denmark
RR of GW at least 1 dose
Birth Cohort HR (95%CI)
1995-1996 0.12 (0.04 to 0.36)
1993-1994 0.22 (0.15 to 0.33)
1991-1992 0.25 (0.19 to 0.32)
1989-1990 0.62 (0.50 to 0.76)
Adapted from Blomberg 2013
Observational Studies Uganda, Safaeian et al 2013
• HPV demonstration project in Uganda (2008-2009)
• Girls who received 1, 2 or 3 doses
• In addition: 24 months since vaccination
• ELISA: HPV-16 and HPV-18 specific antibody levels
• 2 vs 3 doses
• GMT ratios
HPV-16 0.51 (97.5%CI 0.37 to 0.69)
HPV-18 0.69 (97.5%CI 0.50 to 0.96)
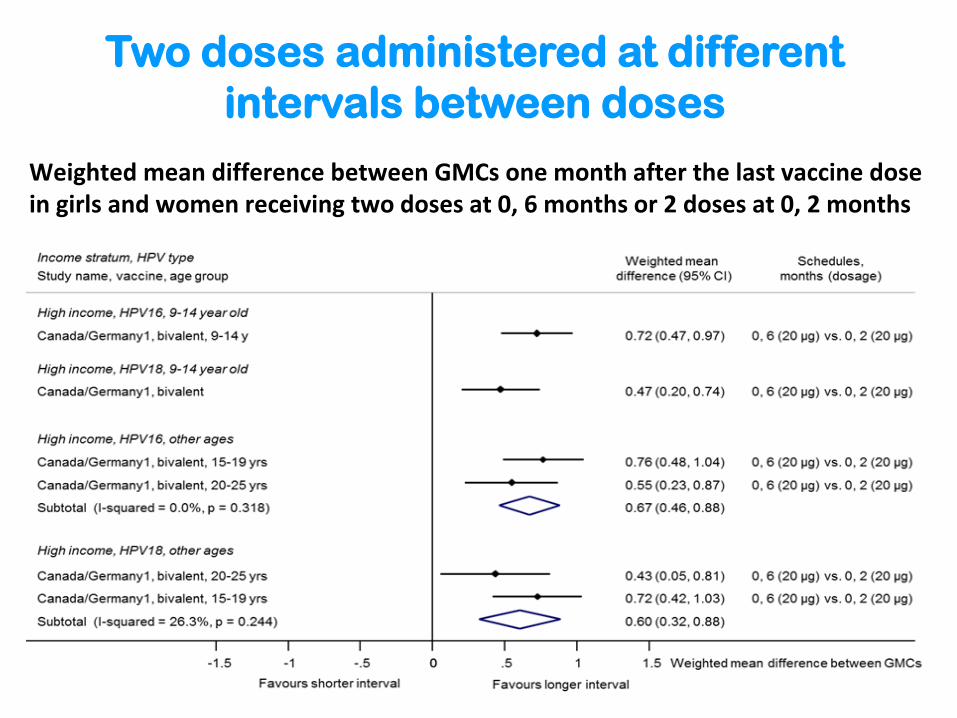
Weighted mean difference between GMCs one month after the last vaccine dose in girls and women receiving two doses at 0, 6 months or 2 doses at 0, 2 months
Two doses administered at different
intervals between doses
Special populations
HIV infected individuals
Although the immunogenicity and efficacy of HPV
vaccines may be reduced in HIV-infected females,
the potential benefit of vaccination in this group is
particularly great owing to their increased risk of
HPV-related disease, including cervical cancer.
There are limited data from HIV-infected
individuals receiving a 3-dose schedule and, no
data from HIV-infected individuals receiving a 2-
dose schedule.
Summary of Findings 2-dose schedule versus 3-dose schedules
In randomised comparisons,
Seroconversion and seropositivity were non-inferior or inconclusive at all time points.
Geometric mean concentrations (GMCs), 1 month after the last dose, in the 2-dose group were lower but non-inferior or inconclusive compared with the 3-dose group.
Summary of Findings 2-dose schedule versus 3-dose schedules
In non-randomised comparisons,
All available data for seroconversion and seropositivity showed non-inferiority of the 2-dose compared with the 3-dose schedule.
GMCs were non-inferior or superior in girls receiving the 2-dose schedule compared with women receiving the 3-dose schedule at all time points assessed, up to 36 months after vaccination.
Summary of Findings 2-dose schedule versus 3-dose schedules
Limited data about clinical outcomes.
The efficacy against virological endpoints in initially HPV-naïve subjects who received 2 doses of bivalent vaccine at month 48 indicates that the two-dose schedule prevents HPV-16/18 infection in subjects who did not receive a complete 3-dose vaccination course.
In the randomized comparisons, in one study, incident infections with any of the vaccine types in the quadrivalent vaccine were more common in the 2-dose than the 3-dose group.
Summary of Findings 2-dose schedule versus 3-dose schedules
Observational data overall support the
findings from the trials.
However it should be noted that
girls or women receiving 2 doses probably differ from those receiving 3, in particular they may have different exposure to infection, adjustment for confounding is unlikely to remove all of this difference
Summary of Findings 2-dose schedule versus 3-dose schedules
Interval between doses
Two RCTs compared two 2-dose schedules with different intervals (0, 6 and 0, 12 months).
Data from one of them reported that the 6-month interval resulted in superior GMCs compared with the 2-month interval one month after the last vaccine dose in all age groups enrolled (9-14, 15-19, 20-25 years).
Mathematical models
UK and Canadian models:
under the hypothetical assumption that a female-only two dose schedule has a
duration of protection of at least 20 years, then there will be few additional cases
prevented by adding a third dose
EMEA assessment
…as the immune responses are comparable between the reduced
dose schedule in the target population (9-14 years old girls) and
the standard schedule in the population where clinical protection
was demonstrated…..
CHMP endorsed the introduction of a two dose (0,6 months) schedule in
girls aged 9-14 years
Research Priorities 1
o Follow up of the cohorts under study in India and duplicate similar studies especially in LMICs.
o Definition of end points for second generation vaccines to
provide additional guidance for the evaluation of alternative schedules, different intervals between doses in different epidemiological settings.
o Head to head comparisons of the two licensed vaccines of
various alternative schedules. o Longer-term clinical effectiveness studies to define the duration
of protection after a 3-dose or 2-dose schedules, and whether a booster may be needed.
Research Priorities 2 o Studies in regions where high rates of vaccination have not yet
occurred because of high herd protection conferred by the 3-dose regimen.
o Multicenter studies in LICs in healthy adolescent girls and special
populations to provide additional evidence. o Systematically review and assess the available (and limited) data on
the impact of various schedules among HIV-infected individuals. o Explore the impact of cost-effectiveness of 2-dose vs. 3-dose in LMICs. o The US National Cancer Institute (NCI) is considering an RCT to assess
the effect on persistence of DNA and immunogenicity of HPV vaccines after 1 or 2 doses in an area with low to moderate vaccine uptake.
Support?
Recommended