
Operational Plan for Operational Plan for Comprehensive HIV and AIDS Comprehensive HIV and AIDS
Care, Management and Treatment Care, Management and Treatment for for
South AfricaSouth Africa

Cabinet Mandate
On 8 August 2003 Cabinet requested the Ministry of Health to
“as a matter of urgency, develop a detailed operational plan on an
antiretroviral treatment programme”
by the end of September 2003
Pillars• Ensuring that the uninfected remain HIV negative• Prevention and changing lifestyles and behaviour • Broader context - social programmes of Government
and the wider society that aim to reduce poverty through job creation and social support
• 5.3 million HIV + progress as slowly as possible to developing AIDS
• Appropriate treatment of AIDS-related conditions including the use antiretroviral therapy in patients presenting with low CD4 counts to :– Improve functional health status– Prolong life

Guiding Principles
• Quality of Care
• Universal and Equitable Implementation
• Strengthening the National Health System
• Re-informing Prevention
• Providing a Continuum of Care
Guiding Principles
• Sustainability
• Promotion of healthy lifestyles
• Promotion of individual choice of treatments
• Integration
• Safety of Medicines
• TB

Goals
• Provide comprehensive care
• Strengthen the National Health System

Prevention, Care and Treatment of Prevention, Care and Treatment of HIV and AIDSHIV and AIDS
• Prevention, care and treatment• Nutrition-related Interventions• Traditional Medicine

Care and Treatment PlanCare and Treatment Plan
• Aim– prolonged and improved quality of life
• Approach
– Continuum of care• Service coordination and integration• Referral systems• HBC approach
• Integration into current services :– E.g. VCT, PMTCT, TB, PEP, STI management, – Add on ARVs for people who have progressed to stage
3 or 4
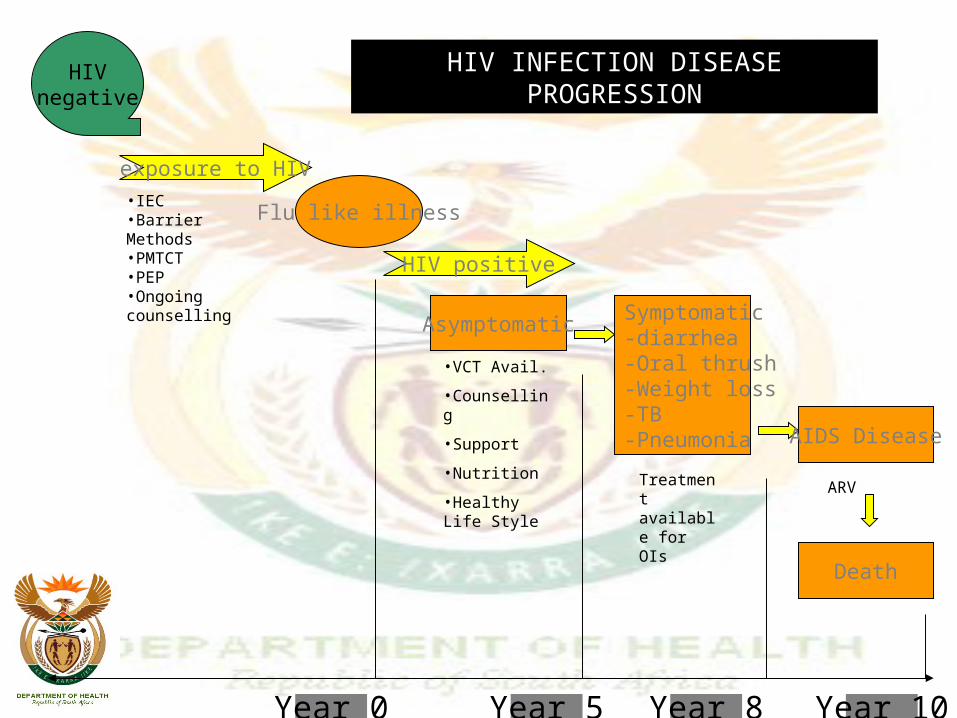
HIVnegative
exposure to HIV
Flu like illness
HIV positive
AsymptomaticSymptomatic-diarrhea-Oral thrush-Weight loss-TB-Pneumonia AIDS Disease
Death
Year 0 Year 5 Year 10Year 8
HIV INFECTION DISEASE PROGRESSION
•IEC•Barrier Methods•PMTCT•PEP•Ongoing counselling
•VCT Avail.
•Counselling
•Support
•Nutrition
•Healthy Life Style
Treatment available for OIs
ARV
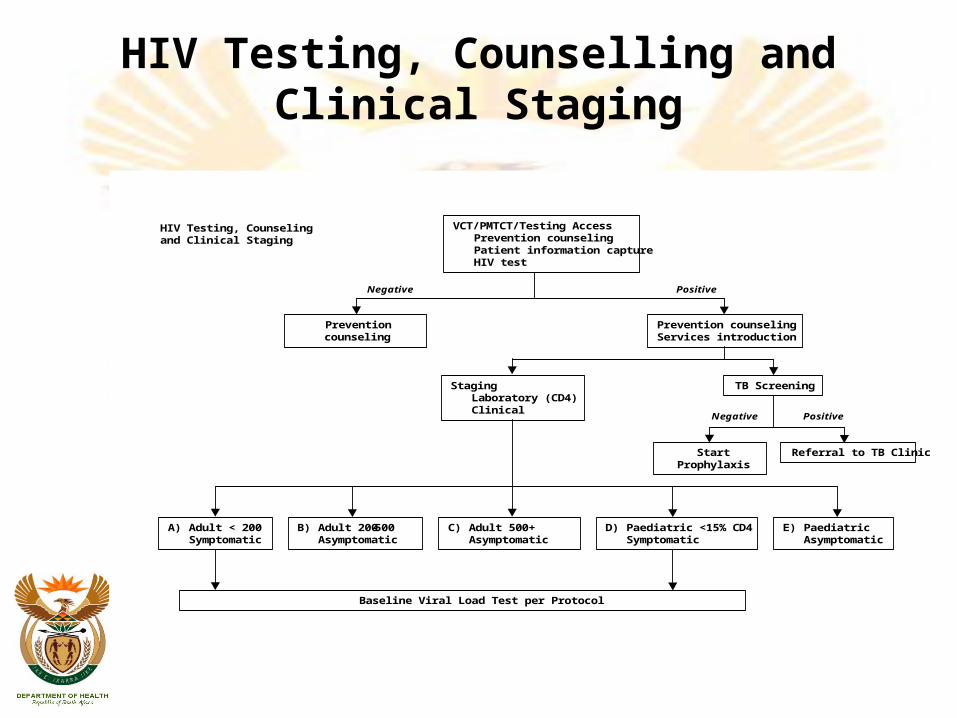
HIV Testing, Counselling and Clinical Staging
VCT/PMTCT/Testing AccessPrevention counselingPatient information captureHIV test
Prevention counseling
Prevention counselingServices introduction
StagingLaboratory (CD4)Clinical
TB Screening
Start Prophylaxis
Referral to TB Clinic
A) Adult < 200Symptomatic
B) Adult 200-500Asymptomatic
C) Adult 500+Asymptomatic
D) Paediatric <15% CD4Symptomatic
E) PaediatricAsymptomatic
HIV Testing, Counseling and Clinical Staging
Baseline Viral Load Test per Protocol
Positive
Positive
Negative
Negative

DRUG REGIMENS
Regimen Drugs Test Frequency
1a d4T / 3TC / NVP CD4 VL ALT
Staging, 6-monthly Baseline, 6-monthly Baseline
1b d4T / 3TC / efavirenz CD4 VL
Staging, 6-monthly Baseline, 6-monthly ALT –
2 AZT / DDI /Lopinavir/ritonavir
CD4 FBC Fasting cholesterol
Staging, 6-monthly Baseline, 1, 3, 6 mo, continue 6-
monthly Baseline only
Regimen Drugs Test Frequency
1a d4T/3TC
Lopinavir / Ritonavir
•CD4•VL•ALT•Chol/TG
Staging, 6 monthly
Baseline, 6 monthly
Baseline
Baseline, 12 monthly
1b d4T/3TC/NVP •CD4•VL•ALT
Staging, 6 monthly
Baseline, 6 monthly
Baseline, 1m, 6 monthly
1c d4T/3TC
efavirenz
•CD4•FBC
Staging, 6 monthly
Baseline, 1,3,6 mo, 6 monthly
2a AZT/ddI
Lopinavir / Ritonavir
•CD4•FBC•Chol/TG
Staging, 6 monthly
Baseline, 1,3,6 mo, 6 monthly
Baseline, q 12 monthly
2b AZT/ddI
Efavirenz or NVP
•CD4•ALT•FBC
6 monthly
Baseline, 1mo, 6mo (NVP only)
Baseline, 1,3,6 mo, then 6 monthly
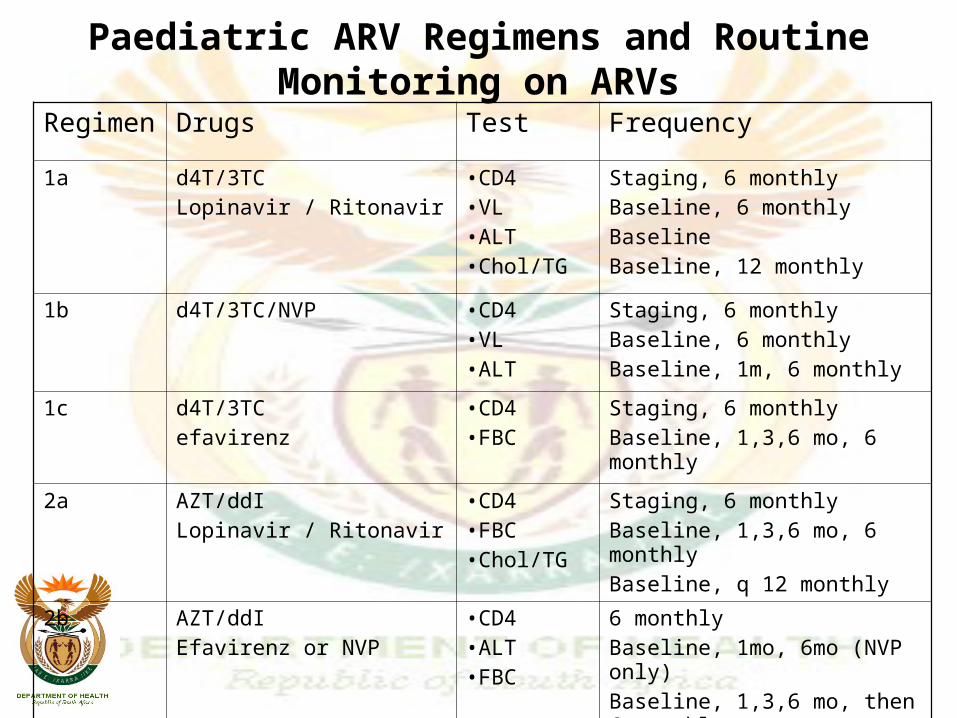
Paediatric ARV Regimens and Routine Monitoring on ARVs

Paediatric ARV Regimens and Routine Monitoring on ARVs
• Notes:• d4T syrup requires refrigeration. If no refrigerator at home, switch
d4T to AZT. Clinician discretion to substitute ABC for d4T in infants > 3 months of age.
• NVP - Choice between first-line regimens is informed by: (a) previous exposure to NVP within last 12 months consider lopinavir/ritonavir; (b) children without history of NVP exposure can receive regimen 1b or 1c, 2b is 2nd line if regimen 1a was given
• efavirenz - limited to children >3 yrs of age and >13 kg. • For drug failure criteria in paediatrics refer to: Continuum of Care
Building for HIV - Paediatric Section, developed by the national Department of Health
• ‘Staging’ – initial testing for all infants/children after confirmed HIV-positive
• ‘Baseline’ – for ARV eligible children at time of ARV initiation• (See Annex I.6 for paediatric ARV detailed dosing and drug
information)
Nutrition
• Contextualised within broader nutritional strategies in Government
• Criteria:– Individual with TB and/or HIV and AIDS– No secure food
• Monthly supply of nutritional supplement• Monthly supply of supplementary meal
• DOH will:– Review and set specifications of supplement meals– Review criteria for implementation– Negotiate on pricing and supply– Evaluate ongoing research– Develop appropriate training material– Coordinate with Social Development & Agriculture

Traditional HealersTraditional Healers
• Role and function in the continuum of care if recognised (prevention, treatment, care and support)
• Compliance, adherence, adverse event reporting, referral system– Ensuring safe traditional health practices
• Support the development of QA mechanisms and establishing training priorities
• Research– traditional medicines on immune system – Interaction with ARVs, TB and STI treatment

Human Resources and Facilities
• Accreditation of Service Points• Human Resource & Training• Provincial Site Assessments

Strengthening and Accreditation
• Objectives:– Provision of a continuum of care– Gold standard of care– Equitable manner
• Service site:– Single facility or grouping of facilities which
combined meet accreditation criteria– Can include NGOs, private sector etc.

Strengthening and Accreditation
• Accreditation requirements which broadly address capacity w.r.t. HR, labs, pharmacies, drug procurement & distribution, referral patterns etc
• Process:– National defines requirements– Provincial assessment teams for site evaluation;
identification of gaps; and developing strengthening plan to address gaps (with time frames)
Context of Human Resources in Health
• Public system is under-funded and resources not equitably spread across country
• Long-standing vacancies across categories; acute for dieticians, nutritionists and pharmacists
• Half of hospital beds are occupied by patients being treated for AIDS-related illnesses
• 15% of health care workers are HIV-positive
Short-Term StrategyShort-Term Strategy
• Recruitment strategy to attract new graduates• Service contracts with health professionals in
private practice• Partnerships with the private sector, NGOs and
CBOs• Incentives to support health professionals with
scarce skills and in rural areas• Streamline requirements for registration of foreign
health professionals to work in public and rural health services
• Development of human resource and skills development plans for years 2 - 5
Short-Term StrategyShort-Term Strategy
• National Training Programme• Establishment of regional training centres• Standardised curricula for comprehensive training of
health professionals in the identified service points– Training of existing health professionals– Multi-skilling of available health professionals– Training of & utilisation of community service
practitioners for 2004 to address the immediate gaps• Telephonic clinical consultation support at a provincial
level for all health professionals providing ART treatment & care
• Development of skills development plans for years 2- 5
Operational IssuesOperational Issues
• Drug procurement• Drug distribution• Laboratory services

Drug Procurement
• Key elements:– Reliability, security and sustainability– Quality– Sufficient volumes consistently with
envisaged demands– Affordability– Local production
Drug ProcurementDrug Procurement
• Approach– Pooled procurement– Flexibility
– Compliance with regulatory standards Medicines Act, Patent Act, TRIPS
– API production– Parallel importation
• Activities– Tendering
• Supplier pre-qualification• Request for proposals• Contracts• Monitoring &Evaluation• Administrative Issues & Programme Assessment
Drug distributionDrug distribution• Reliable supply consistently through:
– Inventory management– Patient prescription information– Secured storage facilities– Efficient & secure transport– Improved packaging
• Key Activities– Provincial Depot Level (Contingency stock plan)– Public Health Service level (Pharmacy Contingency
stock plan)– Accreditation (checklist)– Prescription tracking

Laboratory Services• Key in: disease staging, monitoring
• Infrastructure– List of baseline tests (biochemistry, full blood count)– Diagnostic, clinical monitoring, viral resistance– Viral load, CD4
Strengthening of system
• Facility location• Volumes• Transportation• Turnaround times• Staffing • Research

Social Mobilisation and Communication
• Guiding Principles– Content
• Balance prevention and care• Clear messages on ARVs• Information on the programme• Healthy lifestyles• Nutrition• Adherence
– Process• 3 tiers of government – focus on political leaders and key opinion-
makers• PLWHA• General public • Health care providers, including traditional healers• Families, communities and caregivers• NGOs and CBOs• Sectors of civil society
Information, Monitoring and Research
• Patient Information System• Monitoring and Evaluation• Pharmacovigilance• Research

Patient Information System
• Aim– collect patient-related information to monitor
compliance, adherence, response etc.
• Standardised forms (integrated with M&E)• Patient-linked through personal identifier• Build on existing data and IT infrastructure• Upgrading existing data management & IT
capabilities• Paper-based systems backup• Integrated with electronic patient records
Pharmacovigilance
• Aimed at providing safety profiles for patients and determine morbidity & mortality associated with the use of ARVs
• Existing programme at UCT, but this initiative focuses on supporting the ARV rollout
• Strong technical and training support to specific groups/audiences

ResearchResearch
• Aim– developing a research agenda for research which
defines most effective provision of care and treatment
• Primary focus: operational/health systems and behavioural as well as resistance monitoring
• Structures and process to build on current arrangements with an advisory group advising on priority research and support of the programme
Funding• Presents a national budget• Details all resource requirements for implementation
• Combined to provide a uniform estimate of the resources required to support the integrated HIV and AIDS care and
treatment plan over a five-year period
Prevention Component
• Funding for prevention– The JHTTT report noted the fundamental
importance of maintaining and strengthening an effective HIV prevention programme, and that the availability of resources for prevention must not be compromised by the expansion of the care and treatment response.
– Funds allocated for Prevention through the existing enhanced response programme• R550m per year allocated

Budget Estimates
• 2003/4 - R296 million• 2007/8 - R4.5 billion• 2007/8 includes:
– R1 billion - health professionals– R1.6 billion - ARV’s– R800 million - laboratory monitoring– R650 million – nutritional support
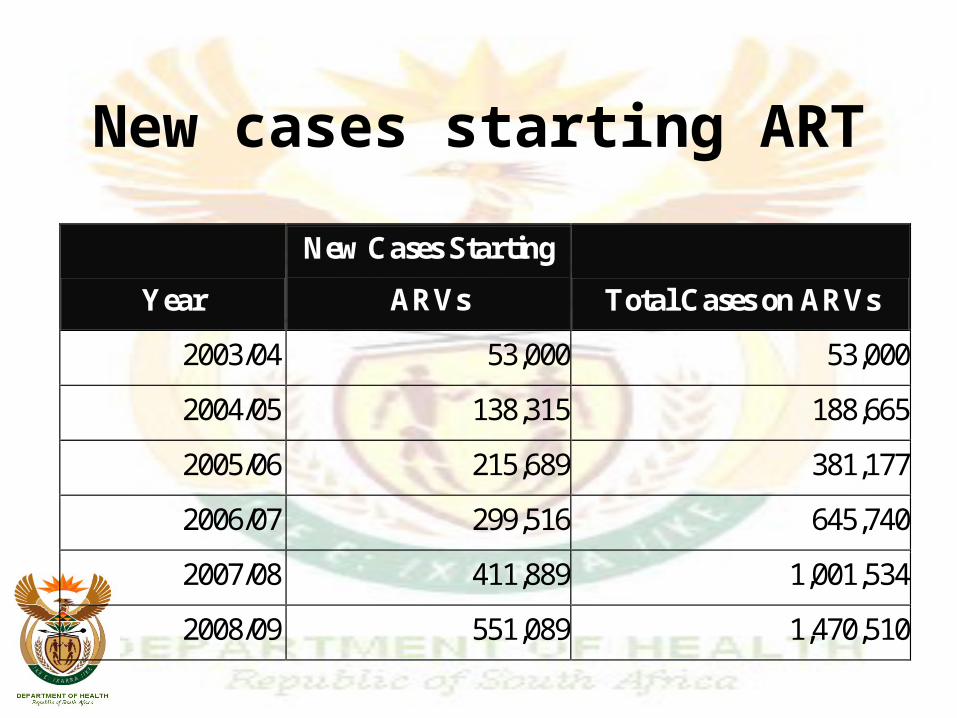
New cases starting ART
Year
New Cases Starting
ARVs Total Cases on ARVs
2003/04 53,000 53,000
2004/05 138,315 188,665
2005/06 215,689 381,177
2006/07 299,516 645,740
2007/08 411,889 1,001,534
2008/09 551,089 1,470,510
Strengthening and Upgrading the
Health System • Staffing Requirements • Upgrading Facilities and Pharmacies • Upgrading Patient Information, Monitoring &
Evaluation Systems • Upgrading the National Health Laboratory Service • Maintaining Health After HIV Infection
– Nutritional Support and Supplementation – Diagnostic Monitoring Following Diagnosis of HIV
Infection

BudgetBudgetTotal Programme Budget Estimate (Millions of Rands)
2003/04 2004/05 2005/06 2006/07 2007/08
New Healthcare Staff 21 322 432 662 1027
Laboratory Testing 20* 152 311 520 806
Antiretroviral Drugs 42 369 725 1118 1650
Nutrition 63 343 421 532 656
Other Health System Upgrades 70 171 184 160 160
Programme Management (National & Provincial) 16 103 128 128 128
Capital Investment 30 75 100 100 0
Research 34 55 55 48 48
Total 296 1590 2358 3268 4474
Challenges
• Strengthening prevention programmes
• Strengthen VCT, PMTCT : synergistic effect
• The recruitment, training and retention of health care professionals
• Building strong partnerships between health facilities and community support structures
• Strong communication and community mobilisation
• Additional financial resources
• Complex to manage; integrated
Challenges
• Improving the integration of services at facility level• Integration of traditional and complementary medicines
with Western therapies• Strengthening the National Health Laboratory System to
meet the demands of the programme• Coordination of human resources, training, laboratory
services, pharmaceutical services, drug procurement, and information systems
• Ensuring high quality of care in the private sector• Pharmacovigilance in the public and private health
sectors• Good patient information
Recommended

















