Occult Bacteremia in Infants
Current controversies and future developments
Denise WattDec. 6, 2001

Outline
• background and epidemiology• management algorithms• evidence for Abx
– oral vs. parenteral
• antibiotic resistance• pneumococcal conjugate vaccine

Case
• 10 month old girl, previously well• URI symptoms x 10 days
– drinking well, wetting diapers, no N/V/D
• 2hr hx fever, lethargy, irritability• O/E: 180, 42, T39.2, 95%
– looks unwell, moaning/crying, HEENT normal, clear BS, some indrawing, CVS normal, abd benign, no rash

Occult Bacteremia: definitions
• FWS: rectal temp 38C, no focus, no obviousvirus, ‘non-toxic’, no significant underlyingillness/immunocompromise
• OB: FWS and +ve BC
• 10-20% PED visits for febrile illness• 20% febrile children <3yr: no source

Epidemiology: pre-HIB
• prior to early 1990’s• OB incidence 3-12% of FWS
– 60-85% S.pneumo– 5-20% HIB
• 40% complication rate

Epidemiology: post-HIB
• incidence of OB (FWS, 3-36 mos, T39°C)– 1.6-2.8%, highest age 1-2 yr
(Kupperman 1998, Lee 1998)
– 90-95% S.pneumo– 96% invasive HIB <5 yr (Alpern 2000)
– 5% non-typhoid Salmonella– others: Neisseria, GAS, GBS,
Moraxella, E.coli, S. aureus

Implications of OB
• 10% SBI if untreated, 17% persistent bacteremia (Harper, Baraff)
• meningitis: 1% (Baraff), 2.7% (Rothrock)
– 7.7% mort, 25-30% neuro sequelae
• overall risk of meningitis in untreated FWS = 0.02-0.05%
• natural course of OPB?– 96% resolve without Abx (Alpern 2000)
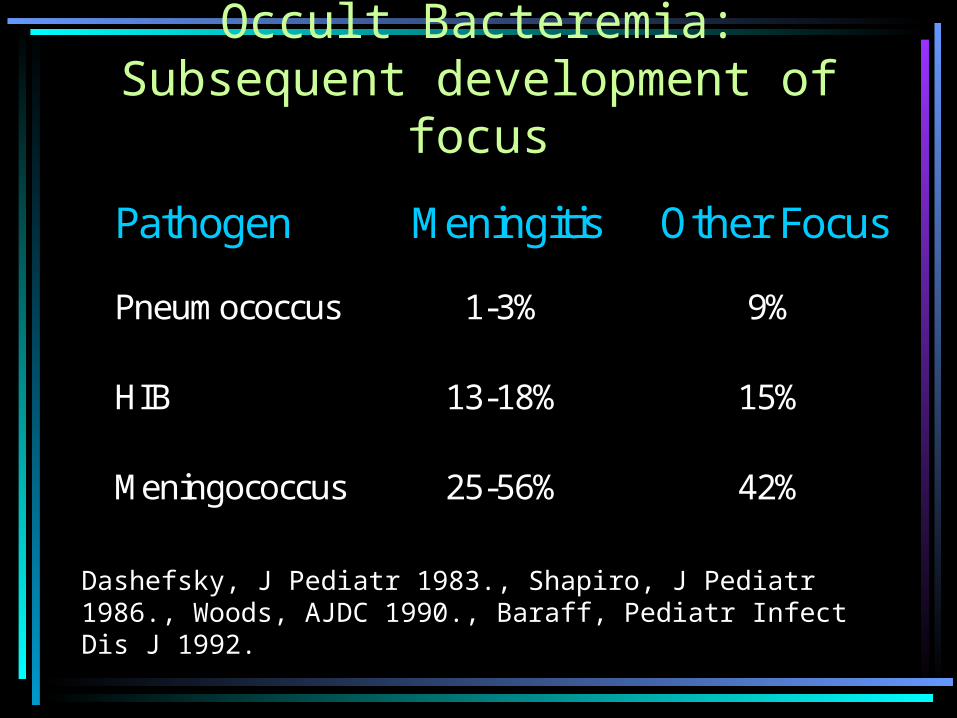
Occult Bacteremia:Subsequent development of
focus
Pathogen Meningitis Other Focus
Pneumococcus 1-3% 9%
HIB 13-18% 15%
Meningococcus 25-56% 42%
Dashefsky, J Pediatr 1983., Shapiro, J Pediatr 1986., Woods, AJDC 1990., Baraff, Pediatr Infect Dis J 1992.

Local Microbiology
• S. pneumo bacteremia rates vary widely across Canada– related to rates of BC drawn– rate in Calgary unknown
• 30 OPB/yr, 10 SBI/yr, 4-5 meningitis/yr• 20 cases invasive HIB/yr (most adults)• 139 +BC last year age 1-15 (all comers)
– 27% contaminants

Predicting OB
• Hx and PE unreliable– may appear well– subjective vs. objective ‘toxicity’– YOS >10: sensitivity 77%, specificity 88%– age– fever
• OPB rare if temp <39.0 (<1%); 3.7% if >40
– similar response to defervescence ± OB (Baker 1989, Bonadio 1993)
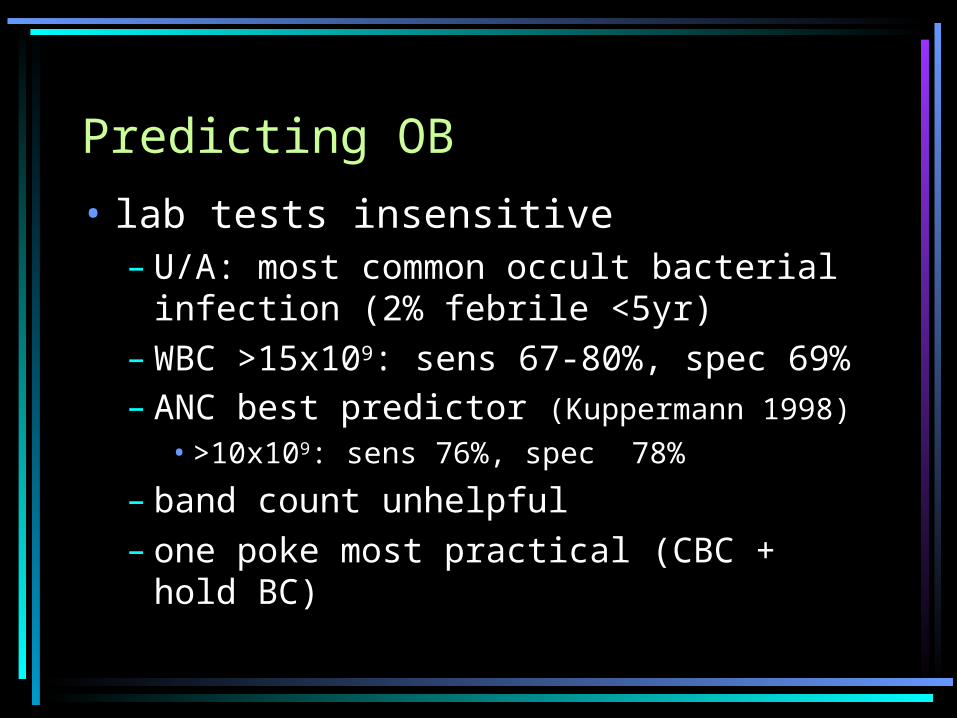
Predicting OB
• lab tests insensitive– U/A: most common occult bacterial
infection (2% febrile <5yr)– WBC >15x109: sens 67-80%, spec 69%– ANC best predictor (Kuppermann 1998)
• >10x109: sens 76%, spec 78%
– band count unhelpful– one poke most practical (CBC + hold
BC)

Blood Cultures
• 12% +ves return for F/U before BC result, 50% called back (Joffe 1992)
– time to +ve = 36hr, time to F/U = 43hr– most pathogens +ve < 18hrF/U more important than BC
• 76% SBI or PB called back (Bachur 2000)
BC allow earlier F/U and Rx
• faster lab techniques coming?

Approach to FWS
• <2-3 mos, 3-36mos, >3 yr treated differently
• <1980s, all pt <3mos admitted for septic W/U and empiric Abx
• low risk criteria developed to avoid hospital admission
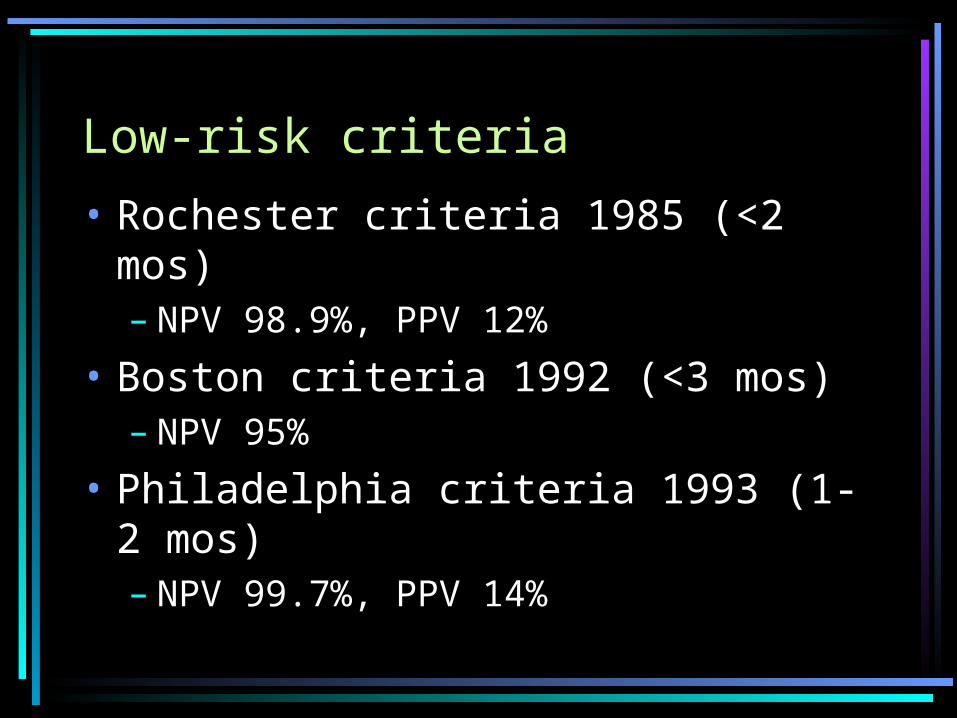
Low-risk criteria
• Rochester criteria 1985 (<2 mos)– NPV 98.9%, PPV 12%
• Boston criteria 1992 (<3 mos)– NPV 95%
• Philadelphia criteria 1993 (1-2 mos)– NPV 99.7%, PPV 14%

Baraff
• “expert consensus” (Pediatrics 1993)– 1-3 mos, ‘low risk’
• option 1: septic W/U and Abx• option 2: urine C&S and observe
– 3-36 mos, non-toxic: septic W/U if T>39.0
• update (Annals Emerg Med 2000)– 3-36 mos
• T39.0: U/A; T39.5: WBC BC (send if >15)
– if empiric Abx, do LP!

Bachur 2001
• Recursive partitioning model– U/A first step– WBC <4 or >20– T > 39.6– age < 13d
• 82% sensitive• admit 28% (vs. 53% with
Rochester)

Cost-Effectiveness of FWS strategies
• 1990’s: BC and empiric Abx for all• Lee (Pediatrics 2001)
– FWS, age 3-36 mos, OPB (1.5%)– meningitis 1° outcome
• incl. health care and societal costs
– CE: CBC + selective BC + Rx if WBC 15– $30,800 / life-year saved – if rate OPB, less aggressive aproach

Why guidelines need re-evaluation
• controversy among ‘experts’• lower incidence of OB • elimination of HIB• cost and complications of tests and
Rx• pen-resistant S. pneumo• not followed anyway (Finklestein 2000)
• vaccine…..

Antibiotics and FWS
• Only 2 prospective RCTs with placebo– both small, pre-HIB– Jaffe 1987:
• no change in SBI• Abx fever, improved appearance
• large, retrospective study (Harpur 1995)
– more focal infection, admissions w/o Abx
• Abx and meningitis (meta-analysis Baraff)
– no Abx 5.8%; oral or parenteral Abx 0.4%

Rothrock 1997: Meta-analysis
• not all RCTs, underpowered• no significant meningitis • significant SBI (OR 0.35 p=0.003)• NNT to prevent 1 meningitis = 651• NNT to prevent 1 SBI = 2190• NNH with Abx for every meningitis
prevented = 567 no prospective studies post-HIB

Oral vs. Parenteral Antibiotics
• Fleisher (1994)– no sign difference in focal infections persistent fever with Ctx– not blinded, not intention-to-treat, pre-HIB
• Rothrock (1997); meta-analysis– meningitis OR=0.67 (oral vs. parenteral)– SBI OR=1.48
• closer F/U with parenteral

Risks of Empiric Antibiotics
• cost (tests, Rx, F/U, hospitalization)• side effects• discomfort of tests, treatment• altered presentation (Rothrock 1992)
• development of resistant strains• missed/partially Rx focal infections• parental preference?
– will accept small risk of SBI vs. discomfort of tests & Rx (Kramer, Oppenheim)

Penicillin-resistant Pneumococcus
• Castillo– San Diego 1991-8: 18% pen
resistance– 14% int. resistance 1991, 42% in
1998– no difference in mortality– NS increased resistance with prior
Abx use

Pen and Cephalosporin resistance
• Silverstein– 11 year review: 8% resistance– no diff in outcome, LOS in pen-
resistant– Ceftriaxone-resistant: more focal
infection, more LPs, more febrile at F/U, more admitted (NS), HR and temp at presentation

Antibiotic resistant Pneumococcus in Calgary
• 15% pen resistance• <2% amoxicillin resistance• 10% Cefuroxime resistance• 3-4% Ceftriaxone resistance
– need higher MIC for CNS clinically, has not been an issue

Conjugate Pneumococcal Vaccine
• heptavalent, 4 doses: 2,4,6,12-15 mos• FDA approval Feb 2000 (Prevnar)• 3 RCTs of safety and immunogenicity
– Rennels (1998)– Shinefield (1999)– Black (2000)
• efficacy 97%, intention-to-treat 94%• including ALL S.pneumo serotypes: 89%• similar SE as DPTP/HIB, none severe

Pneumococcal Vaccine
• significantly OM• Black: ongoing trial on herd immunity• long-term efficacy?• strain selection?Bottom line:• will significantly decrease burden of
S.pneumo disease• likely lag time to change practices

Impact Of Prevnar in N. California~33,000 with ≥1 dose Feb 2000-Mar 2001
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
<1 year <2 years <5 years
=1 dose vaccine
Fully vaccinated
% Reductionvaccine serotypedisease
Shinefield et al. 3rd Int’l PID Conference Monterey, 2001
Pneumococcal Vaccine:Cost Effectiveness
• Lieu (JAMA 2000)– cost < savings if each dose <$46 (US)– present: $56 (US) = $278,000/life-yr saved– >2x savings for society vs. health payer
$760 million/3.8M infants/yr in US• most from parental work loss, productivity
• Calgary: $110/dose ($84 at ACH)• current immunization budget: $17M/yr• cost of SP vaccine: $13M/yr

Occult Bacteremia: Summary
• age, temp, appearance important• don’t forget U/A• save labs for ‘unwell’• faster BC techniques in distant future• F/U most important tool• empiric Abx have very limited role• no clear evidence favouring
parenteral

Occult Bacteremia: Summary II
• antibiotic-resistance is rising; impact small in Calgary
• vaccine WILL change the face of FWS– ‘It’s viral!’
• until then, the controversy continues!
– “Are you a risk-minimizer or test-minimizer?”
(Green, Rothrock. Annals Emerg Med. 1999)

Case revisited
• WBC 14.9– ANC 8.3
• BC +ve S.pneumo in 24hr (pen I)• R/A: looks well, T 38.5• Mgt?
Case cont.
• Ceftriaxone IV• F/U ID clinic:
– well-looking– Ctx IV x 3 days, then Amoxil x 7 days

QUESTIONS?
Recommended