Miami NEONATE WITH ESRD, March, 2017
© The Children's Mercy Hospital, 2016
Bradley A. Warady, M.D.Professor of Pediatrics
University of Missouri - Kansas CityDirector, Division of Nephrology
Director, Dialysis and TransplantationChildren’s Mercy Kansas City
International Pediatric Dialysis Network (IPDN)
Objectives of IPDN■ Improve the quality of pediatric dialysis care worldwide
■ Collect basic information regarding pediatric dialysis practices and outcomes
■ Provide useful tools and management algorithms for daily dialysis practice
■ Provide global benchmarking of pediatric dialysis outcomes
■ Perform prospective observational studies on important clinical issues in pediatric dialysis

Miami NEONATE WITH ESRD, March, 2017
©2015 Children's Mercy Hospitals and Clinics. All Rights Reserved.
International Pediatric Dialysis Network
IPPN3403 Patients
122 Centers43 Countries
IPHN799 Patients
81 Centers36 Countries
©2015 Children's Mercy Hospitals and Clinics. All Rights Reserved.
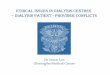
Characterization of 452 Access Revisions by Indication and Time on Peritoneal Dialysis
Borzych-Duzalka et al. CJASN , 2016

Miami NEONATE WITH ESRD, March, 2017
©2015 Children's Mercy Hospitals and Clinics. All Rights Reserved. Borzych-Duzalka et al. CJASN, 2016
Access Survival in 824 Incident Patients According to Patient Age at Catheter Insertion
©2015 Children's Mercy Hospitals and Clinics. All Rights Reserved.
Technique Survival
Borzych-Duzalka et al. CJASN, 2016
©2015 Children's Mercy Hospitals and Clinics. All Rights Reserved.

Miami NEONATE WITH ESRD, March, 2017
©2015 Children's Mercy Hospitals and Clinics. All Rights Reserved.
Baseline Patient and Treatment Characteristics
Total population
BMI <2.5th
percentile8.9%
BMI 2.5th-85th pct
71.4%
BMI > 85th pct
19.7%P
N=1001 n=89 n=715 n=197Country GNI per capita (1000$) 27.1 � 13.6 24.0 � 13.2 27.0 � 13.4 28.6 � 14.5 0.030Age (yrs) 8.5 � 5.8 7.7 � 5.9 8.7 � 5.8 8.1 � 5.8 0.176Male gender 550 (55%) 50 ( 56.2%) 388 (54.3%) 112 ( 56.9%) 0.788Renal diagnosisCAKUTGlomerulopathyOther
424 (42.4%)388 (38.8%)189 (18.9%)
44 (49.4%)30 (33.7%)15 (16.9%)
291 (40.7%)292 (40.8%)132 (18.5%)
89 (45.2%)66 (33.5%)42 ( 21.3%)
0.235
Comorbidities 355 (35.5%) 38 (42.7%) 250 (35.0%) 67 (34.0%) 0.318eGFR at PD start (ml/min/1.73m2) 8.0 (5.3) 7.3 (5.1) 7.9 (5.2) 8.8 (5.6) 0.007Urine output (L/m2/d) 0.61 (0.94) 0.53 (0.85) 0.63 (0.93) 0.56 (1.05) 0.803PD modalityCAPDAPD Other
222 ( 22.6%)759 ( 77.4%)13 (1.3 %)
23 (25.8%)60 (67.4%)6 (6.7 %)
156 (21.8%)547 (76.5%)
6 (0.8%)
43 (21.8%)152 (77.2%)
1 (0.5%)
0.512
Biocompatible PD fluid use 428 (42.8 %) 33 (37%) 316 (44.2%) 79 (40.1%) 0.313Height SDS -1.9 � 1.7 -1.6 � 2.1 -1.8 � 1.6 -2.3 � 1.8 <0.001Nutritional supplementationNone Oral supplementsNG tubePEG
595 (59.4%)218 (21.8%)
92 (9.2%)96 (9.6%)
54 (60.7%)24 (27%)6 (6.7%)5 (5.6%)
428 (59.9%)160 (22.4%)69 (9.6%)58 (8.1%)
113 (57.4%)34 (17.3%)17 (8.6%)33 (16.7%)
0.007
Amino acid PD fluid use 12 (1.2 %) 4 (4.5%) 5 (0.6%) 3 (1.5%) 0.007Growth hormone use 64 (6.4%) 3 (3.4 %) 50 (7.0%) 11 (5.6%) 0.367Hemoglobin (g/L) 10.8 � 1.9 11.0 � 2.1 10.8 � 1.9 10.8 � 1.8 0.612Serum albumin (g/l) 35.8 � 6.9 36.2 � 5.4 35.6 � 7.2 36.2 � 6.6 0.519Blood urea (mg/dl) 96 (63) 93 (64) 97 (63) 93 (62) 0.524Serum bicarbonate (mM) 23.9 � 4.3 23.7 � 4.1 23.9 � 4.2 24.2 � 4.7 0.631Serum phosphorus (mM) 1.8 � 0.6 1.8 � 0.6 1.8 � 0.6 1.7 � 0.6 0.204
Baseline Patient and Treatment Characteristics
Total population
BMI <2.5th
percentile8.9%
BMI 2.5th-85th pct
71.4%
BMI > 85th pct
19.7%P
N=1001 n=89 n=715 n=197Country GNI per capita (1000$) 27.1 � 13.6 24.0 � 13.2 27.0 � 13.4 28.6 � 14.5 0.030Age (yrs) 8.5 � 5.8 7.7 � 5.9 8.7 � 5.8 8.1 � 5.8 0.176Male gender 550 (55%) 50 ( 56.2%) 388 (54.3%) 112 ( 56.9%) 0.788Renal diagnosisCAKUTGlomerulopathyOther
424 (42.4%)388 (38.8%)189 (18.9%)
44 (49.4%)30 (33.7%)15 (16.9%)
291 (40.7%)292 (40.8%)132 (18.5%)
89 (45.2%)66 (33.5%)42 ( 21.3%)
0.235
Comorbidities 355 (35.5%) 38 (42.7%) 250 (35.0%) 67 (34.0%) 0.318eGFR at PD start (ml/min/1.73m2) 8.0 (5.3) 7.3 (5.1) 7.9 (5.2) 8.8 (5.6) 0.007Urine output (L/m2/d) 0.61 (0.94) 0.53 (0.85) 0.63 (0.93) 0.56 (1.05) 0.803PD modalityCAPDAPD Other
222 ( 22.6%)759 ( 77.4%)13 (1.3 %)
23 (25.8%)60 (67.4%)6 (6.7 %)
156 (21.8%)547 (76.5%)
6 (0.8%)
43 (21.8%)152 (77.2%)
1 (0.5%)
0.512
Biocompatible PD fluid use 428 (42.8 %) 33 (37%) 316 (44.2%) 79 (40.1%) 0.313Height SDS -1.9 � 1.7 -1.6 � 2.1 -1.8 � 1.6 -2.3 � 1.8 <0.001Nutritional supplementationNone Oral supplementsNG tubePEG
595 (59.4%)218 (21.8%)
92 (9.2%)96 (9.6%)
54 (60.7%)24 (27%)6 (6.7%)5 (5.6%)
428 (59.9%)160 (22.4%)69 (9.6%)58 (8.1%)
113 (57.4%)34 (17.3%)17 (8.6%)33 (16.7%)
0.007
Amino acid PD fluid use 12 (1.2 %) 4 (4.5%) 5 (0.6%) 3 (1.5%) 0.007Growth hormone use 64 (6.4%) 3 (3.4 %) 50 (7.0%) 11 (5.6%) 0.367Hemoglobin (g/L) 10.8 � 1.9 11.0 � 2.1 10.8 � 1.9 10.8 � 1.8 0.612Serum albumin (g/l) 35.8 � 6.9 36.2 � 5.4 35.6 � 7.2 36.2 � 6.6 0.519Blood urea (mg/dl) 96 (63) 93 (64) 97 (63) 93 (62) 0.524Serum bicarbonate (mM) 23.9 � 4.3 23.7 � 4.1 23.9 � 4.2 24.2 � 4.7 0.631Serum phosphorus (mM) 1.8 � 0.6 1.8 � 0.6 1.8 � 0.6 1.7 � 0.6 0.204

Miami NEONATE WITH ESRD, March, 2017
Regional Variation of Nutritional Status at Start of CPD
0%
20%
40%
60%
80%
100%
Korea (24) Canada(13)
LatinAmerica
(202)
WesternEurope(300)
China /Hong Kong
(77)
NewZealand
(18)
Turkey(105)
CentralEurope(120)
USA (97) India/SEAsia (30)
MiddleEast (15)
Malnutrition Normal Weight Overweight Obesity
15.7% 16.7%
33%40%
20%
Regional Differences in Supplementary Feeding Practices in 386 Children < 6 Years
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
ANZAC (8
)
USA (3
5)
West EU (1
46)
Latin Americ
a (66)
Canada (
3)
Korea (4)
ME (8)
India/SE Asia
(8)
Central EU
(47)
Turkey (
42)
China/HKG (1
9)
None
Oral Suppl
NGT
PEG
Multivariate Analysis of Factors Predicting BMI SDS at Start of CPD
Estimate (SE) P
Intercept -0.284 (0.130) 0.029
eGFR 0.020 (0.009) 0.036
Comorbidities -0.156 (0.101) 0.121
Nutritional supplementation (reference = none)
OralNGTPEG
-0.180 0.1560.446
(0.117)(0.169)(0.169)
0.1230.3570.009

Miami NEONATE WITH ESRD, March, 2017
Multivariate Analysis of Factors Predicting BMI SDS at Start of CPD
Estimate (SE) P
Intercept -0.284 (0.130) 0.029
eGFR 0.020 (0.009) 0.036
Comorbidities -0.156 (0.101) 0.121
Nutritional supplementation (reference = none)
OralNGTPEG
-0.180 0.1560.446
(0.117)(0.169)(0.169)
0.1230.3570.009
Course of BMI SDS According to Nutritional Status at Start of PD
Overwt/obesityNormalMalnutrition
Factors Predicting Prospective Annualized Change in BMI SDS
Parameter Estimate (SE) P
Intercept -0.056 (0.259) 0.828Duration of PD (years) -0.060 (0.036) 0.094Diagnosis (reference: CAKUT)
GlomerulopathyOther
-0.229 -0.364
(0.089)(0.110)
0.0100.001
BMI SDS -0.456 (0.026) <0.001Height SDS 0.113 (0.025) <0.001% deviation from estimated dry weight -0.040 (0.014) 0.008Serum albumin (g/L) 0.015 (0.006) 0.015Nutritional supplementation (reference: none)
OralNGTPEG
-0.195 0.122 0.633
(0.090)(0.133)(0.132)
0.0310.358
<0.001

Miami NEONATE WITH ESRD, March, 2017
Factors Predicting Prospective Annualized Change in BMI SDS
Parameter Estimate (SE) P
Intercept -0.056 (0.259) 0.828Duration of PD (years) -0.060 (0.036) 0.094Diagnosis (reference: CAKUT)
GlomerulopathyOther
-0.229 -0.364
(0.089)(0.110)
0.0100.001
BMI SDS -0.456 (0.026) <0.001Height SDS 0.113 (0.025) <0.001% deviation from estimated dry weight -0.040 (0.014) 0.008Serum albumin (g/L) 0.015 (0.006) 0.015Nutritional supplementation (reference: none)
OralNGTPEG
-0.195 0.122 0.633
(0.090)(0.133)(0.132)
0.0310.358
<0.001
Survival of Patients with and without Malnutrition at Last Observation
p = 0.028
Hazard Ratios of Death According to Age and BMI SDS

Miami NEONATE WITH ESRD, March, 2017
©2015 Children's Mercy Hospitals and Clinics. All Rights Reserved.
Vascular Access in Prevalent Pediatric HD Patients
USRDS, 2017
©2015 Children's Mercy Hospitals and Clinics. All Rights Reserved.
CVL (n = 404) AVF (n = 143) AVG (n = 5) p
Males (n/%) 224 (55) 84 (59) 2 (40) 0.5
Initial Modality (n/% HDF) 45 (11) 42 (29) 1 (20) <0.001
Age (median /IQR) 11.1 (6.5; 14.7) 13.7 (11.4; 15.8) 13.6 (12.4; 16.3) <0.001
Diagnosis:CAKUT (n, %)GLM (n, T)
171 (42)101 (24)
63 (44)35 (25)
3 (60)--
0.60.7
Comorbidities (n, %):Syndromal/genetic diseaseCardiopulmonarySensory loss (vision, hearing)
105 (26)61 (15)55 (14)
28 (20)12 (8)13 (9)
1 (20)1 (20)3 (60)
0.050.020.01
Height SDS (median/IQR) -1.8 (-3.3; -0.8) -1.4 (-2.2; -0.6) 0.2 (0.0; 0.7) 0.01
BMI SDS (median/IQR) -0.1 (-1; 0.8) -0.2 (0-0.7; 0.5) 0.2 (0; 0.8) 0.4
Region n (% of access per region): 0.01
Western EuropeCentral/Eastern EuropeTurkeyAsiaMiddle EastNorth AmericaLatin AmericaANZAC
191 (68)41 (65)
50 (73.5)72 (90)16 (84)25 (93)7 (70)2 (67)
89 (31)21 (33)
16 (23.5)8 (10)3 (16)2 (7)
3 (30)1 (33)
2 (1)1 (2)2 (3)
00000
Renal transplantationCadaveric n (%)Living related n (%)
156 (39)101 (65)55 (35)
56 (36)46 (82)10 (18)
0 0.50.010.01
Demographics of Patients with CVL andAVF/AVG at First Access Placement
CVL (n = 404) AVF (n = 143) AVG (n = 5) p
Males (n/%) 224 (55) 84 (59) 2 (40) 0.5
Initial Modality (n/% HDF) 45 (11) 42 (29) 1 (20) <0.001
Age (median /IQR) 11.1 (6.5; 14.7) 13.7 (11.4; 15.8) 13.6 (12.4; 16.3) <0.001
Diagnosis:CAKUT (n, %)GLM (n, T)
171 (42)101 (24)
63 (44)35 (25)
3 (60)--
0.60.7
Comorbidities (n, %):Syndromal/genetic diseaseCardiopulmonarySensory loss (vision, hearing)
105 (26)61 (15)55 (14)
28 (20)12 (8)13 (9)
1 (20)1 (20)3 (60)
0.050.020.01
Height SDS (median/IQR) -1.8 (-3.3; -0.8) -1.4 (-2.2; -0.6) 0.2 (0.0; 0.7) 0.01
BMI SDS (median/IQR) -0.1 (-1; 0.8) -0.2 (0-0.7; 0.5) 0.2 (0; 0.8) 0.4
Region n (% of access per region): 0.01
Western EuropeCentral/Eastern EuropeTurkeyAsiaMiddle EastNorth AmericaLatin AmericaANZAC
191 (68)41 (65)
50 (73.5)72 (90)16 (84)25 (93)7 (70)2 (67)
89 (31)21 (33)
16 (23.5)8 (10)3 (16)2 (7)
3 (30)1 (33)
2 (1)1 (2)2 (3)
00000
Renal transplantationCadaveric n (%)Living related n (%)
156 (39)101 (65)55 (35)
56 (36)46 (82)10 (18)
0 0.50.010.01
Demographics of Patients with CVL andAVF/AVG at First Access Placement

Miami NEONATE WITH ESRD, March, 2017
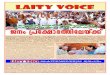
Choice of Vascular Accessby Age
-30
20
70
120
170
220
<2 2 to 6 6 to 10 10 to 15 >15
Num
ber o
f pat
ient
s
CVL
AVFAVG
CVL (72%)
AVF (26%)
AVG (2%)
Clinical, Dialytic and Biochemical Parameters and ESA Dosing at Study Entry and 6 Monthly Updates
by Vascular Access Type CVC AVF AVG p
Age at access placement (median /IQR)
11.0 (6.3;14.7) 13.7 (10.9; 15.8) 16.5 (12.1; 18) <0.001
Access observation time (mo) 15 (6;25)bc 22 (11;40)a 24 (9;28)a <0.001Blood flow rate (ml/min/m2) 167±54b 176±53a 180±57 0.02Dialysate flow rate (ml/min/m²) 508±229bc 374±112a 423±161a <0.001Kt/V urea 1.66±0.59bc 1.74±0.54ac 1.99±0.68ab <0.001
Hemoglobin (g/l) 10.4 ± 1.76b 11.09 ± 1.7c 10.1 ± 1.6b <0.001Serum ferritin (ng/ml) 401 ± 386bc 459 ± 485a 568 ± 396a 0.003Transferrin Saturation (%) 30.2 ± 17.2 30.7 ± 16.6 27.1 ± 13.8 0.3Serum albumin (g/l) 39.4 ± 5.5b 40.6 ± 4.9a 39.2 ± 4.44 <0.001CRP (mg/l) 16 ± 50b 10 ± 36a 13 ± 20 0.06ESA dose (IU/kg/wk) 266 ± 190bc 195 ± 148a 191 ± 142a <0.001ESA dose (IU/m2/wk) 7055 ± 4693bc 5911 ± 4052a 5483 ± 3939a <0.001ERI (IU/m2/wk per g/dl Hb) 704 ± 499b 564 ± 482a 569 ± 439 <0.001
a p<0.05 versus CVC; b p<0.05 versus AVF ; C p<0.05 versus AVG; ESA=erythropoiesis stimulating agent, ERI = ESA resistance index
Clinical, Dialytic and Biochemical Parameters and ESA Dosing at Study Entry and 6 Monthly Updates
by Vascular Access Type
CVC AVF AVG p
Age at access placement (median /IQR)
11.0 (6.3;14.7) 13.7 (10.9; 15.8) 16.5 (12.1; 18) <0.001
Access observation time (mo) 15 (6;25)bc 22 (11;40)a 24 (9;28)a <0.001Blood flow rate (ml/min/m2) 167±54b 176±53a 180±57 0.02Dialysate flow rate (ml/min/m²) 508±229bc 374±112a 423±161a <0.001Kt/V urea 1.66±0.59bc 1.74±0.54ac 1.99±0.68ab <0.001
Hemoglobin (g/l) 10.4 ± 1.76b 11.09 ± 1.7c 10.1 ± 1.6b <0.001Serum ferritin (ng/ml) 401 ± 386bc 459 ± 485a 568 ± 396a 0.003Transferrin Saturation (%) 30.2 ± 17.2 30.7 ± 16.6 27.1 ± 13.8 0.3Serum albumin (g/l) 39.4 ± 5.5b 40.6 ± 4.9a 39.2 ± 4.44 <0.001CRP (mg/l) 16 ± 50b 10 ± 36a 13 ± 20 0.06ESA dose (IU/kg/wk) 266 ± 190bc 195 ± 148a 191 ± 142a <0.001ESA dose (IU/m2/wk) 7055 ± 4693bc 5911 ± 4052a 5483 ± 3939a <0.001ERI (IU/m2/wk per g/dl Hb) 704 ± 499b 564 ± 482a 569 ± 439 <0.001a p<0.05 versus CVC; b p<0.05 versus AVF ; C p<0.05 versus AVG; ESA=erythropoiesis stimulating agent, ERI = ESA resistance index

Miami NEONATE WITH ESRD, March, 2017
Multivariate Logistic Regression Analysis of Risk Factors for CVC Dysfunction
OR (95% CI) P
Age 0.98 (0.94 – 1.02) 0.26
Access site – internal jugular 0.30 (0.13 – 0.68) <0.001
Access site – subvlavian 0.66 (0.26 – 1.66) 0.79
Access site – femoral 1.2 (0.40 – 3.59) 0.08
©2015 Children's Mercy Hospitals and Clinics. All Rights Reserved.
Primary Access Patency Rates
p = <0.0001
©2015 Children's Mercy Hospitals and Clinics. All Rights Reserved.
Remote Patient Monitoring
1.43.9
0.02
0.4
3.6
1.25
0.4
2.2
0.1
0.1
0.17
0.7
4.115.9
8.1
4.0
11.8
11.4
Shortage of nephrologists and hospitals offering dialysis and transplantation for adults in the developing world
(www.globaldialysis.com, 2007) Dialysis unit per million population

Miami NEONATE WITH ESRD, March, 2017
©2015 Children's Mercy Hospitals and Clinics. All Rights Reserved.
PD Cyclers
©2015 Children's Mercy Hospitals and Clinics. All Rights Reserved.
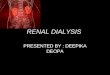
Sharesource Clinical Portal-Two Way Communication
Baxter
• Remote firmware upgrades
• Technical service support
Sharesource Platform
Patient at Home
• Conversations with clinician more fruitful, as all patient treatment data is accessible through portal.
Clinician at Clinic
• Access to review each patient’s dialysis therapy each morning
• Dashboard with flagged alarms. highlighting patient events.
• Potential earlier detection of clinical issues.
• Access to patient’s historical treatment files.
• Remote change of device dialysis settings from the hospital direct to patient’s device at home.

Miami NEONATE WITH ESRD, March, 2017
*Initial RPM questionnaire■ Frequency of RPM data assessment ■ Alert systems chosen ■ Procedure for health care provider RPM feedback to patients
*Annual RPM questionnaires■ Specific changes in center RPM settings ■ Work load for doctors / nurses (semi-quantitatively) ■ Acceptance by patients, parents, doctors and nurses (semi-quantitatively)■ Estimates on changes in PD regime / medication performed based on RPM
data and estimates on how often the modification proved to be beneficial
6 month updates:■ Type of RPM* ■ Number of outpatient visits ■ Body weight/length, biochemistry, medication, PD modalities, blood pressure,
echocardiography, 24 h ABPM ….■ Access revisions, peritonitis, exit-site infections, hospitalizations …■ Transient / permanent discontinuation of RPM (reasons)
Remote Patient Monitoring
■ Frequency of outpatient and emergency room visits
■ Frequency, reasons and duration of hospitalizations
■ PD prescription, UF capacity, % deviation from estimated dry weight
■ Bioimpedance data, blood pressure control (office and 24 h ABPMs), echocardiography findings
■ Biochemical profile
■ Medication usage
■ Infectious complications and outcome, catheter revisions, technique failure, modality switch and death
Answers from the IPPN: RPM versus non-RPM PD
■ The IPDN is a source of global information on the performance of
dialysis in children cared for in pediatric dialysis programs
■ The linking of treatment data to longitudinal patient outcome data
makes the IPDN a valuable resource to help guide clinical
management and improve patient care
■ The success of the IPDN is dependent on the voluntary
participation of dialysis programs and patients worldwide
■ Individuals/sites interested in participating in the IPDN should
contact Brad Warady ([email protected]) or Franz Schaefer
Summary

Miami NEONATE WITH ESRD, March, 2017
©2015 Children's Mercy Hospitals and Clinics. All Rights Reserved.
International Pediatric Dialysis Network
www.pedpd.org
End
History of Peritoneal DialysisInvestigator Description DateGanter First human peritoneal dialysis 1923
Wear, Sisk & Trinkle First successful treatment of ARF with PD 1938
Frank, Seligman & Fine Seminal studies of PD in ARF in animals and humans
1946-1948
Grollman Long-dwell PD for uremia in animals & humans 1951
Maxwell IPD for ARF, commercially available dialysis solutions, and nylon catheter
1959
Doolan IPD for ARF, PVC catheter 1959
Palmer, Tenckhoff Silicone catheters 1963-67
Popovich, Moncrief Described CAPD 1976
Diaz-Buxo Described CCPD 1981

Miami NEONATE WITH ESRD, March, 2017
©2015 Children's Mercy Hospitals and Clinics. All Rights Reserved.
Weight Status Stratified by Modality and Age
Bonthuis, M. et al., Nephrol Dial Transplant, 2013
©2015 Children's Mercy Hospitals and Clinics. All Rights Reserved.
PD Cyclers
©2015 Children's Mercy Hospitals and Clinics. All Rights Reserved.
0
20
40
60
80
100
120
Before PD start (n=25) <1 mo (n=100) 1mo to 1y (n=162) >1y (n=165)
Num
ber o
f cat
hter
s
Leak
Dysfunction
Peritonitis
ESI/Tunnel Inf
Other
Characterization of 452 Access Revisions by Indication and Time on PD
Borzych-Duzalka D., et al., (Submitted)

Miami NEONATE WITH ESRD, March, 2017
©2015 Children's Mercy Hospitals and Clinics. All Rights Reserved.
Residual Diuresis by Diuretic Therapy
Ha I-S, et al., Kidney Int, 2015

Miami NEONATE WITH ESRD, March, 2017
PD Cycler Card System Non- Adherence of Pediatric Patients to
Automated PD
51 children, 45% exhibited some non-adherence to prescribed PD regimen
Chua A and Warady B. Ped Neph (2011)
Sharesource Key Features
Patient Daily TreatmentSummary:
■ Full cycle visibility
■ Drain pattern
■ Weight, blood pressure and UF trends
■ Record of all continuous alarms
Example of Drain Problems Secondary to Constipation

Miami NEONATE WITH ESRD, March, 2017
Multivariate Logistic Regression Analysis of Risk Factors for AVF Dysfunction
Age OR (95% CI) P
Access site – upper arm (ref. forearm) 0.98 (0.87 – 1.11) 0.002
Access site – cubital (ref. forearm) 1.09 (0.35 – 3.38) 0.45
Access site – brachiocephalic (ref. forearm) 0.23 (0.03 – 1.84) 0.13
Puncture technique – button hole (ref. rope ladder) 0.66 (0.25 – 1.76) 0.41
Weight Status Stratified by Modality and Age
Bonthuis, M. et al., Nephrol Dial Transplant, 2013
Supplemental Feeding and Growth
Rees L et al. JASN 2011;22:2303-2312
•Mean BMI improved in NGT/Gtube while it decreased in Demand (p<0.05)•Mean Length decreased the least in Gtube vs Demand (p<0.05)

Miami NEONATE WITH ESRD, March, 2017
©2015 Children's Mercy Hospitals and Clinics. All Rights Reserved.
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
NorthAm
Europe LatinAm
Asia Turkey
CCPD
NIPD
CAPD
PD Modalities
©2015 Children's Mercy Hospitals and Clinics. All Rights Reserved.
IPDN Website
©2015 Children's Mercy Hospitals and Clinics. All Rights Reserved.
IDPN Aims■ Improve the quality of pediatric dialysis care worldwide
■ Collect basic information regarding pediatric dialysis practices and outcomes
■ Provide useful tools and management algorithms for daily dialysis practice
■ Provide global benchmarking of pediatric dialysis outcomes
■ Perform prospective observational studies on important clinical issues in pediatric dialysis

Miami NEONATE WITH ESRD, March, 2017
Variation of Nutritional Status at Start of CPD by Age
Title?
Thumfart J. Ped Neph 2017
Factors Predicting Prospective Annualized Change in BMI SDS
Parameter Estimate (SE) P
Intercept -0.056 (0.259) 0.828Duration of PD (years) -0.060 (0.036) 0.094Diagnosis (reference: CAKUT)
GlomerulopathyOther
-0.229 -0.364
(0.089)(0.110)
0.0100.001
BMI SDS -0.456 (0.026) <0.001Height SDS 0.113 (0.025) <0.001% deviation from estimated dry weight -0.040 (0.014) 0.008Serum albumin (g/L) 0.015 (0.006) 0.015Nutritional supplementation (reference: none)
OralNGTPEG
-0.195 0.122 0.633
(0.090)(0.133)(0.132)
0.0310.358
<0.001

Miami NEONATE WITH ESRD, March, 2017
Multivariate Analysis of Factors Predicting BMI SDS at Start of CPD
Estimate (SE) P
Intercept -0.284 (0.130) 0.029
eGFR 0.020 (0.009) 0.036
Comorbidities -0.156 (0.101) 0.121
Nutritional supplementation (reference = none)
OralNGTPEG
-0.180 0.1560.446
(0.117)(0.169)(0.169)
0.1230.3570.009
CVL (n = 404) AVF (n = 143) AVG (n = 5) p
Males (n/%) 224 (55) 84 (59) 2 (40) 0.5
Initial Modality (n/% HDF) 45 (11) 42 (29) 1 (20) <0.001
Age (median /IQR) 11.1 (6.5; 14.7) 13.7 (11.4; 15.8) 13.6 (12.4; 16.3) <0.001
Diagnosis:CAKUT (n, %)GLM (n, T)
171 (42)101 (24)
63 (44)35 (25)
3 (60)--
0.60.7
Comorbidities (n, %):Syndromal/genetic diseaseCardiopulmonarySensory loss (vision, hearing)
105 (26)61 (15)55 (14)
28 (20)12 (8)13 (9)
1 (20)1 (20)3 (60)
0.050.020.01
Height SDS (median/IQR) -1.8 (-3.3; -0.8) -1.4 (-2.2; -0.6) 0.2 (0.0; 0.7) 0.01
BMI SDS (median/IQR) -0.1 (-1; 0.8) -0.2 (0-0.7; 0.5) 0.2 (0; 0.8) 0.4
Region n (% of access per region): 0.01
Western EuropeCentral/Eastern EuropeTurkeyAsiaMiddle EastNorth AmericaLatin AmericaANZAC
191 (68)41 (65)
50 (73.5)72 (90)16 (84)25 (93)7 (70)2 (67)
89 (31)21 (33)
16 (23.5)8 (10)3 (16)2 (7)
3 (30)1 (33)
2 (1)1 (2)2 (3)
00000
Renal transplantationCadaveric n (%)Living related n (%)
156 (39)101 (65)55 (35)
56 (36)46 (82)10 (18)
0 0.50.010.01
Demographics of Patients with CVL andAVF/AVG at First Access Placement
Clinical, Dialytic and Biochemical Parameters and ESA Dosing at Study Entry and 6 Monthly Updates
by Vascular Access Type CVC AVF AVG p
No of observations 907 559 48Age at access placement (median /IQR)
11.0 (6.3;14.7) 13.7 (10.9; 15.8) 16.5 (12.1; 18) <0.001
Access observation time (mo) 15 (6;25)bc 22 (11;40)a 24 (9;28)a <0.001
Blood flow rate (ml/min/m2) 167±54b 176±53a 180±57 0.02Dialysate flow rate (ml/min/m²) 508±229bc 374±112a 423±161a <0.001Kt/V urea 1.66±0.59bc 1.74±0.54ac 1.99±0.68ab <0.001
Hemoglobin (g/l) 10.4 ± 1.76b 11.09 ± 1.7c 10.1 ± 1.6b <0.001Serum ferritin (ng/ml) 401 ± 386bc 459 ± 485a 568 ± 396a 0.003Transferrin Saturation (%) 30.2 ± 17.2 30.7 ± 16.6 27.1 ± 13.8 0.3Serum albumin (g/l) 39.4 ± 5.5b 40.6 ± 4.9a 39.2 ± 4.44 <0.001CRP (mg/l) 16 ± 50b 10 ± 36a 13 ± 20 0.06ESA dose (IU/kg/wk) 266 ± 190bc 195 ± 148a 191 ± 142a <0.001ESA dose (IU/m2/wk) 7055 ± 4693bc 5911 ± 4052a 5483 ± 3939a <0.001ERI (IU/m2/wk per g/dl Hb) 704 ± 499b 564 ± 482a 569 ± 439 <0.001
a p<0.05 versus CVC; b p<0.05 versus AVF ; C p<0.05 versus AVG; ESA=erythropoiesis stimulating agent, ERI = ESA resistance index

Miami NEONATE WITH ESRD, March, 2017
Clinical, Dialytic and Biochemical Parameters and ESA Dosing at Study Entry and 6 Monthly Updates
by Vascular Access Type CVC AVF AVG p
No of observations 907 559 48Age at access placement (median /IQR)
11.0 (6.3;14.7) 13.7 (10.9; 15.8) 16.5 (12.1; 18) <0.001
Access observation time (mo) 15 (6;25)bc 22 (11;40)a 24 (9;28)a <0.001
Blood flow rate (ml/min/m2) 167±54b 176±53a 180±57 0.02Dialysate flow rate (ml/min/m²) 508±229bc 374±112a 423±161a <0.001Kt/V urea 1.66±0.59bc 1.74±0.54ac 1.99±0.68ab <0.001
Hemoglobin (g/l) 10.4 ± 1.76b 11.09 ± 1.7c 10.1 ± 1.6b <0.001Serum ferritin (ng/ml) 401 ± 386bc 459 ± 485a 568 ± 396a 0.003Transferrin Saturation (%) 30.2 ± 17.2 30.7 ± 16.6 27.1 ± 13.8 0.3Serum albumin (g/l) 39.4 ± 5.5b 40.6 ± 4.9a 39.2 ± 4.44 <0.001CRP (mg/l) 16 ± 50b 10 ± 36a 13 ± 20 0.06ESA dose (IU/kg/wk) 266 ± 190bc 195 ± 148a 191 ± 142a <0.001ESA dose (IU/m2/wk) 7055 ± 4693bc 5911 ± 4052a 5483 ± 3939a <0.001ERI (IU/m2/wk per g/dl Hb) 704 ± 499b 564 ± 482a 569 ± 439 <0.001
a p<0.05 versus CVC; b p<0.05 versus AVF ; C p<0.05 versus AVG; ESA=erythropoiesis stimulating agent, ERI = ESA resistance index
Patient and Treatment Baseline Characteristics
Total population
BMI <2.5th
percentile8.9%
BMI 2.5th-85th pct
71.4%
BMI > 85th pct
19.7%P
N=1001 n=89 n=715 n=197Country GNI per capita (1000$) 27.1 � 13.6 24.0 � 13.2 27.0 � 13.4 28.6 � 14.5 0.030Age (yrs) 8.5 � 5.8 7.7 � 5.9 8.7 � 5.8 8.1 � 5.8 0.176Male gender 550 (55%) 50 ( 56.2%) 388 (54.3%) 112 ( 56.9%) 0.788Renal diagnosisCAKUTGlomerulopathyOther
424 (42.4%)388 (38.8%)189 (18.9%)
44 (49.4%)30 (33.7%)15 (16.9%)
291 (40.7%)292 (40.8%)132 (18.5%)
89 (45.2%)66 (33.5%)42 ( 21.3%)
0.235
Comorbidities 355 (35.5%) 38 (42.7%) 250 (35.0%) 67 (34.0%) 0.318eGFR at PD start (ml/min/1.73m2) 8.0 (5.3) 7.3 (5.1) 7.9 (5.2) 8.8 (5.6) 0.007Urine output (L/m2/d) 0.61 (0.94) 0.53 (0.85) 0.63 (0.93) 0.56 (1.05) 0.803PD modalityCAPDAPD Other
222 ( 22.6%)759 ( 77.4%)13 (1.3 %)
23 (25.8%)60 (67.4%)6 (6.7 %)
156 (21.8%)547 (76.5%)
6 (0.8%)
43 (21.8%)152 (77.2%)
1 (0.5%)
0.512
Biocompatible PD fluid use 428 (42.8 %) 33 (37%) 316 (44.2%) 79 (40.1%) 0.313Height SDS -1.9 � 1.7 -1.6 � 2.1 -1.8 � 1.6 -2.3 � 1.8 <0.001Nutritional supplementationNone Oral supplementsNG tubePEG
595 (59.4%)218 (21.8%)
92 (9.2%)96 (9.6%)
54 (60.7%)24 (27%)6 (6.7%)5 (5.6%)
428 (59.9%)160 (22.4%)69 (9.6%)58 (8.1%)
113 (57.4%)34 (17.3%)17 (8.6%)33 (16.7%)
0.007
Amino acid PD fluid use 12 (1.2 %) 4 (4.5%) 5 (0.6%) 3 (1.5%) 0.007Growth hormone use 64 (6.4%) 3 (3.4 %) 50 (7.0%) 11 (5.6%) 0.367Hemoglobin (g/L) 10.8 � 1.9 11.0 � 2.1 10.8 � 1.9 10.8 � 1.8 0.612Serum albumin (g/l) 35.8 � 6.9 36.2 � 5.4 35.6 � 7.2 36.2 � 6.6 0.519Blood urea (mg/dl) 96 (63) 93 (64) 97 (63) 93 (62) 0.524Serum bicarbonate (mM) 23.9 � 4.3 23.7 � 4.1 23.9 � 4.2 24.2 � 4.7 0.631Serum phosphorus (mM) 1.8 � 0.6 1.8 � 0.6 1.8 � 0.6 1.7 � 0.6 0.204

Miami NEONATE WITH ESRD, March, 2017
Clinical, Dialytic and Biochemical Parameters and ESA Dosing at Study Entry and 6 Monthly Updates
by Vascular Access Type CVC AVF AVG p
No of observations 907 559 48Age at access placement (median /IQR)
11.0 (6.3;14.7) 13.7 (10.9; 15.8) 16.5 (12.1; 18) <0.001
Access observation time (mo) 15 (6;25)bc 22 (11;40)a 24 (9;28)a <0.001
Blood flow rate (ml/min/m2) 167±54b 176±53a 180±57 0.02Dialysate flow rate (ml/min/m²) 508±229bc 374±112a 423±161a <0.001Kt/V urea 1.66±0.59bc 1.74±0.54ac 1.99±0.68ab <0.001
Hemoglobin (g/l) 10.4 ± 1.76b 11.09 ± 1.7c 10.1 ± 1.6b <0.001Serum ferritin (ng/ml) 401 ± 386bc 459 ± 485a 568 ± 396a 0.003Transferrin Saturation (%) 30.2 ± 17.2 30.7 ± 16.6 27.1 ± 13.8 0.3Serum albumin (g/l) 39.4 ± 5.5b 40.6 ± 4.9a 39.2 ± 4.44 <0.001CRP (mg/l) 16 ± 50b 10 ± 36a 13 ± 20 0.06ESA dose (IU/kg/wk) 266 ± 190bc 195 ± 148a 191 ± 142a <0.001ESA dose (IU/m2/wk) 7055 ± 4693bc 5911 ± 4052a 5483 ± 3939a <0.001ERI (IU/m2/wk per g/dl Hb) 704 ± 499b 564 ± 482a 569 ± 439 <0.001
a p<0.05 versus CVC; b p<0.05 versus AVF ; C p<0.05 versus AVG; ESA=erythropoiesis stimulating agent, ERI = ESA resistance index
Generalized Linear Model Analysis of Factors Predicting Hemoglobin Level
Estimate (SE) PIntercept 10.059 (0.383) <0.001Age - 0.019 (0.011) 0.079Dialysis vintage 0.001 (0.002) 0.863Vascular access type (reference = none)
CVC
AVF
Underlying renal disease - CAKUT
Presence of comorbidities
ESA dose (IU/kg/week)
Dialysis hrs per week
0.452
0.162
0.267
0.033
-0.001
0.033
(0.283)
(0.284)
(0.095)
(0.096)
(0.001)
(0.014)
0.111
<0.001
0.005
0.729
<0.001
0.024
CAKUT – congenital anomalies of kidney or urinary tract
Generalized Linear Model Analysis of Factors Predicting Hemoglobin Level
Estimate (SE) PIntercept 10.059 (0.383) <0.001Age - 0.019 (0.011) 0.079Dialysis vintage 0.001 (0.002) 0.863Vascular access type (reference = none)
CVC
AVF
Underlying renal disease - CAKUT
Presence of comorbidities
ESA dose (IU/kg/week)
Dialysis hrs per week
0.452
0.162
0.267
0.033
-0.001
0.033
(0.283)
(0.284)
(0.095)
(0.096)
(0.001)
(0.014)
0.111
<0.001
0.005
0.729
<0.001
0.024
CAKUT – congenital anomalies of kidney or urinary tract
Recommended