int j language amp communication disorders 1998 vol 33 no 3 329ndash352
Notes and Discussion
Active versus passive cleft-type speechcharacteristics
Anne Harding and Pamela GrunwellDe Montfort University Leicester UK
(Received December 1996 accepted September 1997)
Abstract
Cleft palate speech is generally described in terms of nasal resonance nasalemission and compensatory articulations A longitudinal study of children atdiVerent stages of surgical treatment revealed a distinction between passive andactive cleft-type speech characteristics whereby passive characteristics werethought to be the product of structural abnormality or dysfunction and activecharacteristics were speci c articulatory gestures replacing intended consonantsPassive and active patterns of articulation are described and de ned in thecontext of three longitudinal studies of subjects who were at various stages oftwo diVerent surgical regimes ve bilateral cleft lip and palate (BCLP) subjectsaged 16ndash46 12 mixed unilateral cleft lip and palate (UCLP) and BCLP subjectsaged 46ndash76 and nine mixed UCLP and BCLP subjects aged 90ndash110 Referenceis also made to data from 12 mixed cleft-type subjects aged 130 who had beentreated with diVerent surgical timing regimes Comparison is made between theincidence of active versus passive processes in relation to oral structure At age46 speech samples taken from BCLP subjects who had been treated with1-stage versus 2-stage palate repair all evidenced both active and passive pro-cesses The lack of diVerentiation in speech results irrespective of their currentsurgical status ie completely repaired palates versus residual cleft of the hardpalate was unexpected Cleft-type processes in completely repaired subjectsmight be accounted for by the inevitable anterior defect following repair of abilateral cleft Older subjects with structural defects also evidenced more cleft-type processes The relevance of distinguishing between active and passiveprocesses is underlined by consideration of the eVects of structural changesfollowing surgery The eVect of surgery on seven subjectsrsquo speech is discussedusing the activepassive distinction Active cleft-type characteristics did notchange as a direct result of surgery whereas passive characteristics were largelyeliminated following surgery A speci c distinction is made between active andpassive nasal fricatives with the implication that active nasal fricatives may not beaVected by surgical intervention whereas passive nasal fricatives may be eliminatedby surgery Accurate distinction between active and passive patterns of articula-tion may serve to identify those cleft-type speech error patterns most likely torespond to surgical intervention Indications from this study are that activecleft-type characteristics require destabilization in a course of speech and lan-
Address correspondence to Anne Harding 31 Mill Road Buckden Huntingdon CambsPE18 9SS UK
1368-282298 $12middot00 copy 1998 Royal College of Speech amp Language Therapists
A Harding and P Grunwell330
guage therapy before the potential bene ts of surgery can be properly assessedAn analytical protocol for the interpretation of speech samples is presented andsome therapy strategies are proposed for active and passive processes
Keywords activepassive processes cleft palate speech and language therapysurgical timing
Introduction
Whilst lsquocleft palate speech problemsrsquo are commonly regarded as lsquoarticulatory dis-ordersrsquo Russell and Grunwell (1993) Harding and Grunwell (1993) and Hardingand Grunwell (1996) have reconsidered cleft palate speech characteristics in thecontext of phonological development The outcome of this phonological and devel-opmental perspective on cleft palate speech in uenced the GOSSPASS protocol(Sell et al 1994) and GOSSPASSrsquo98 (Sell et al 1998) which has recently beenselected by a panel of experienced clinicians as the preferred protocol for assessingcleft palate speech in the UK It is sensitive not only to the articulatory eVects ofthe cleft but also to idiosyncratic phonological processes commonly heard in cleftpalate speech
As described by Harding and Grunwell (1996) Hutters and Brondsted (1987)observed that some children with a cleft palate apparently respond to a subconsciousawareness of their limited phonetic and phonological repertoire by activelyemploying non-native sounds from their phonetic repertoire in order to maximizetheir range of meaningful contrasts Other children more passively continue tomake the appropriate articulatory movements with no apparent response to theabsence of adequate contrasts in their speech This distinction between active andpassive responses to the articulatory constraints imposed by the cleft forms thebasis of the 1987 theory of Hutters and Brondsted of active and passive strategiesMorley (1970) categorized her speech results into Groups A and B such that GroupA made no adaptations to articulation but nasal escape nasal tone and weakconsonants were noted These characteristics resemble Hutters and Brondstedrsquos(1987) passive strategies whereas speech characteristics in Group B included addi-tional symptoms of nasopharyngeal snort glottal and pharyngeal articulation andincorrect articulation Morleyrsquos (1970) Group B is equivalent to Hutters andBrondstedrsquos (1987) active strategies Subjects with normal velopharyngeal functionbut persisting articulatory errors were included in this group Trost-Cardamone(1990) made a similar distinction in her description of categories I and II in cleftpalate speech characteristics Category I misarticulations were said to be lsquostructurallybased and revealed in audible nasal emission of high pressure consonantsrsquo (stopsfricative and aVricates) and Category II misarticulations were compensatory articu-lations and atypical backed distortions Category I is equivalent to Hutters andBrondstedrsquos (1987) passive strategies and Category II to active strategies Golding-Kushner (1995) distinguishes between compensatory and obligatory articulatoryerrors Compensatory errors would be product of active strategies and obligatoryerrors would be the product of passive strategies Obligatory errors are describedas resulting from an anatomic defect and are lsquonot easily amenable to therapyrsquo(Golding-Kushner 1995)
The four ways of grouping cleft-type characteristics described above all indicatethat some characteristics are an inevitable consequence of structural imperfection
Active versus passive cleft-type speech characteristics 331
andor velopharyngeal dysfunction However none of the distinctions have beenexpressed with reference to their potential impact on phonological developmentStengelhofen (1989) noted that reduced intra-oral pressure may result in nasalrealization of voiced plosives b d gmdash[m n Icirc] This can have a devastating eVecton speech development because plosives [b d] usually represent most fricative targetconsonants in early speech acquisition (age 10ndash20 approx) The phonologicalconsequence of loss of intra-oral pressure may be that a childrsquos early consonantrepertoire could be restricted to nasals and approximants [m n Icirc w j] with [h]sometimes representing voiceless plosive and fricative targets Russell (1991) andHarding (1993) observed nasal fricative consonants in developing speech patternswhich in some but not all cases resolved Russell and Grunwell (1993) consideredthe eVect of abnormal learned neuromotor patterns which can dominate phonolo-gical development A restricted phonetic repertoire in babble can persist into earlyspeech irrespective of increasing potential for velopharyngeal function In the workof Russell (Russell 1991 Grunwell and Russell 1993) established articulatory pat-terns were more readily modi ed by some children than others Harding (1993)found that some speakers made placement distinctions in their nasal fricativerealizations but others used one nasal fricative [Icircdeg
k] for all fricative target consonantsApplication of the phonetic repertoire into speech is usually systematic and as aresult most families are able to understand their childrsquos distinctively cleft-typespeech Strategies employed in early speech inevitably aVect phonological processesErrors are process-speci c not phoneme speci c A phonological perspective ininterpretation of speech assessments is therefore both necessary and enlightening
This paper proposes a phonologically based categorization system for cleftpalate speech patterns observed in a longitudinal study of pre-speech and speechdevelopment in diVerent groups of children whose ages ranged from 16 to 130The proposed system predicts an association between certain speech characteristicsand the structure and function of the speech mechanism Since subjects had beentreated with either 1-stage surgery or 2-stage repair in which the hard palate remainedunrepaired until between 4 and 8 years the speech data could be considered inrelation to a range of oral structures Two subjects were recorded before palatesurgery at age 16 other samples were taken when palates were partially repairedor when fully repaired with or without stulae and with or without suspectedvelopharyngeal incompetence During the course of the longitudinal studies sevensubjects underwent surgery and the eVects of surgery on speech were monitored
Pre-speech and speech samples were taken at 6-monthly intervals at diVerentstages of surgical repair and at diVerent stages of speech development Detailedanalysis of 141 speech samples led to the identi cation of the activepassiveframework which is described here
Four concurrent studies three of which were longitudinal included subjects bornwith complete clefts of lip and palate aged between 16 and 130 Study 1 followedpre-speech vocalizations into speech from ages 16 to 46 and Study 2 recorded patternsof change in speech production from ages 46 to 76 Studies 3 and 4 comprised 2groups of older subjects Study 3 ages 90ndash110 and Study 4 130 were primarilyincluded to facilitate comparison between speech and facial growth
Method
Speech samples were elicited from younger subjects by use of the prototype of thePACSTOYS Screening Assessment (Grunwell and Harding 1995) whereas older
A Harding and P Grunwell332
subjects were asked to describe PACS pictures (Grunwell 1987) Speech was tran-scribed both live and from audio recordings Live transcription was thought to bean essential supplement to audio recordings since some visually perceived character-istics could not be detected on the audio-recordings eg labiodental nasal [Iacute] mightbe perceived as a bilabial nasal on audio recording Slight audible nasal emission asin [pk] might be suspected on audio but it would be con rmed by live transcription
The following speech parameters were studied nasal resonance nasal emissionnasal turbulence voice lip posture intelligibility and consonant production Speechsamples were taken in the home and hence routine endoscopy and uoroscopywere impracticable It is furthermore questionable whether such investigationswould be thought ethical unless they were necessary for clinical management Theprimary area of interest in this investigation has therefore been detailed examinationof the nature of consonant production in relation to oral structure Harding andGrunwell (1996) have identi ed articulatory errors of place as glottal pharyngealuvular velar lateral palatal double articulations For the seven individuals whounderwent surgery the pre-operative data were compared with the processesobserved post-operatively to ascertain whether any trends in post-operative conson-ant production could be identi ed Phoneme realizations were transcribed andcharted on to phoneme evolution charts (Harding 1993) and phonetic diagrams(Harding and Grunwell 1993) were completed for each speech sample
Analytical approach
Initially cleft-type consonant production errors were distinguished from thosedevelopmental errors thought to be unrelated to the cleft Errors related to the cleftpalate were categorized as Cleft-Type Realizations (CTRs) (Harding and Grunwell1993)
Since most articulatory errors aVected groups of consonants speech errors werefurther categorized within a phonologically based framework of cleft-type processesThe speci c processes were de ned within the 1987 concept of Hutters andBrondstedrsquos active versus passive strategies
Activepassive analytical framework
Active processes are de ned here as alternative articulations thought to have beenactively generated in order to establish the necessary phoneme distinctions betweenindividual consonant targets Where one strategy systematically aVected more thanone consonant target and these targets were phonologically related then that strategywas identi ed as a process a cleft-type phonological process For example backingusually aVected several alveolar targets t d n s z resulting in a backing pro-cess In this de nition alternative articulations include both non-English consonantrealizations eg s to [x] and alternative English consonants as in t backed to [k]
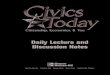
Figure 1 illustrates the nature of realizations involved in active processes As agroup they resemble but are not the same as Trostrsquos (1981) compensatory articula-tions In early speech attempts at several fricative target consonants might all berealized by a single realization for example s z S Z might be any of the followingnasal fricative [n
degk] post-oral glottal [h] or pharyngeal [Eacute] backed to uvular [X] or
to velar [x] lateral [Euml] palatal [c] A backing process aVecting production of [s]might also result in backing of both alveolar target plosive consonants eg t to
Active versus passive cleft-type speech characteristics 333
Figure 1 Active cleft-type processes
[k] and of nasal andor lateral alveolar target consonants n l to [Icirc] Whilst thesecharacteristics might as has been assumed in the past be pure articulatory errorsthere are phonological consequences (Grundy and Harding 1995) when severalclasses of consonants eg voiced and voiceless alveolar fricatives and alveolarplosives are realized by one consonant [g] resulting in multiple loss of phonologicalcontrasts or systematic sound preference (Grunwell 1985)
In viewing gure 1 it is worth noting that pharyngeal and glottal articulationare lsquonon-oralrsquo productions which do not require intra-oral pressure or velopharyngealclosure and their production would not evoke sphincteric movement A speakermust at least intend an oral production if potential velopharyngeal sphincter functionis to be accurately assessed Hence predominance of glottal and pharyngeal patternsof articulation imply but do not prove the existence of an inadequate sphincter
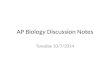
lsquoActiversquo processes which establish meaningful contrasts did not account for allthe cleft-type speech patterns observed in the data Consideration is now given tothe cleft-type realizations thought to be passive products of either structural defector dysfunction Hypernasal resonance co-occurring with passive patterns of articula-tion are frequently a direct consequence of weak or absent intra-oral pressure In apassive realization there is no alteration of the articulatory pattern for the intendedconsonant eg the bilabial b in ball is produced [m] [mO~] As shown by gure 2exclusively passive patterns of articulation employ few consonants (approximantsand nasals and glottal [h]) [m n Icirc w j l h] to represent all adult consonants Thisrange of consonants when associated with nasalized vowels suggests a lack ofpotential to establish intra-oral pressure for speech To date passive consequencesof the cleft on speech have received minimal attention perhaps because they donot involve non-English consonant realizations Lack of intra-oral pressure isassociated with hypernasal resonance and nasal emission (Kummer et al 1992)Nasal emission is perceived either accompanying or replacing voiceless pressureconsonant targets hence it will not be present until a child is actively targetingvoiceless pressure consonants (Sell et al 1994) Severely hypernasal speech may notevidence nasal emission until fricative targets are intended and realized as [(sk)n
deg]
for examplePassive processes which severely limit the range of consonants can impair
communication more than a combination of active processes Speech samples
A Harding and P Grunwell334
Figure 2 Passive cleft-type processes
containing active processes usually sound distinctive but communicative compet-ence can be impressive because more meaningful diVerences can be signalled thanmay be possible with the restricted phonetic repertoire of passive processes Giventhat the velopharyngeal sphincter is complex and dynamic it is possible for arestricted phonetic repertoire with hypernasal resonance to persist into early speechdevelopment because a child has been unable to achieve velopharyngeal functionfor speech after palate repair
The distinction between active and passive cleft-type processes has been integ-rated into the revised cleft palate speech assessment GOSSPASSrsquo98 (Sell et al1998) De nitions of cleft-type characteristics are given in GOSSPASSrsquo98 butGOSSPASS does not interpret the phonological consequences of the cleft-typecharacteristics The following de nitions of active and passive cleft-type processesare based on data analysis in the present study and on Harding and Grunwellrsquos(1996) characteristics of cleft palate speech Analysis of patterns of phonemeevolution throughout speech acquisition has generated a hierarchy of error-severityThe following descriptions of the diVerent types of processes are illustrated byreference to the data collected in the research studies (Harding 1993)
Active cleft type processes
Active nasal fricatives
[mdegk] [n
degk] [ Daggerk
deg] Nasal realizations of voiceless and sometimes voiced fricative targets
f v s z S Z were categorized as nasal fricatives Comparison of gures 1 and 2shows that nasal realizations occurred in both passive and active processes Inproduction of active nasal fricatives the pulmonary air is actively directed nasallyas an alternative articulation to an oral fricative realization Figure 3 illustrates thatoral air ow is stopped by either lips or tongue thus achieving 100 nasal air owThis strategy is developed in order to signal the fricative nature of intended targetfricative consonants In the active nasal fricative [m
degk] for f n
degk for s [n
degk O] for
lsquosorersquo [mdegk O] for lsquofourrsquo is the product of actively directed nasal air Where fricative
consonants are the only targets aVected by a cleft-type process the presence ofnasal fricatives have been referred to as phoneme speci c nasality (Trost-Cardamone
Active versus passive cleft-type speech characteristics 335
Figure 3 Active nasal fricative [ndegk]
1990) This characteristic has been found in speakers with no cleft palate historyoften with no explanation for its occurence
DiVerent places of articulation signalled placement contrasts between nasalfricative consonants in the same way that target nasal consonants [m n Icirc] arediVerentiated by place of articulation [m
degk] for f [n
degk] for s S Where a strong
backing process existed alveolar and post-alveolar fricatives were realized by velarnasal fricatives [ Daggerk
deg]
Occasionally nasal air ow was constricted such that nasal fricatives were pro-duced with a noisier turbulent quality [m
deg] [n
deg] [ Dagger] In a detailed assessment of cleft
pa la te speech GOSSPASSrsquo98 (Sell et al 1994 1998) these turbulent realizationswould be categorized in the resonance section as lsquonasal turbulence replacing conson-antsrsquo and in the cleft-type characteristics section as either lsquoactive nasal fricativesrsquo orpassive nasal realization of fricatives
Glottal articulation
[] frequently occurred in early plosive and aVricate production [p b t d T] up toage 46 Sometimes this process aVected only alveolar plosives t d in SIWI andSIWW position At times glottal stop represented voiced plosives [b d g] while[h] represented voiceless plosives [p t k] In SFWF position glottal stop representedboth voiced and voiceless plosives It may be the case that diVerent strengths ofglottal stop were used to distinguish voiceless and voiced plosives but this couldnot be reliably judged without spectographic analysis An undergraduate study ofspectographic analysis (Shorter 1995) of cleft palate speech identi ed some subtlediVerences in glottal stop productions which suggests a need for further investigationinto the phonological functions of glottal stops in cleft palate speech
Pharyngeal fricatives
[Eacute iquest] Early attempts at fricatives (ages 20ndash30) were frequently realized with acombination of posterior fricative cleft-type realizations (CTRs) Where plosiveswere exclusively glottal fricative consonants were frequently realized as pharyngeal
A Harding and P Grunwell336
fricatives In early phonological development obstruent realizations were commonlynon-oral but gradually moved anteriorly to uvular and velar positions Targetconsonants were not generally corrected independently of each other The gradualmovement of pharyngeal realizations towards oral uvularvelar articulation whichunderlines the relevance of a phonological interpretation of cleft palate speechcharacteristics
Exclusively pharyngealglottal patterns of articulation might imply velopharyn-geal insuYciency but it is noted here that all infants use pharyngeal and glottalarticulation until they acquire velopharyngeal competence during the rst 6 monthsof life It is possible for children with cleft palate to persist with this phoneticrepertoire for some time after palate repair Indeed such cases have been reportedby Russell and Grunwell (1993) Non-oral articulatory patterns indicate that thesphincter is not employed during speech which implies that the sphincter may notbe functional but unless oral air ow is consciously intended it cannot be assumedthat the sphincter is unable to function in speech (Henningsson and Isberg 1986)
Backing [k g q G]
A backing pattern is described by Stengelhofen (1989) as a lsquotendency for oralcontacts to be to the back of the oral cavityrsquo GOSSPASSrsquo98 (Sell et al 1998) makesa distinction here between backing to uvular and backing to velar place ofarticulation
E Backing to uvular [q G X Ograve ] Alveolar target consonants were backed touvular realizations and occasionally velar targets were backed to uvular Thepresence of velar and uvular realizations indicated the presence of some VPfunction but this might have been achieved with tongue humping In thedata acquisition of uvular and velar fricatives generally co-occurred withacquisition of f v which provides further evidence of velopharyngealfunction In the longitudinal study from age 16 to 46 subjects with bilateralclefts spent a period of months realizing all alveolar and post- alveolar voicedand voiceless consonant targets in uvular placement This degree of backingis deemed to be more severe and distracting for listeners than backing tovelar perhaps because uvular articulation is more distinctively non-EnglishHowever uvular fricatives are frequently used to achieve some meaningfulcontrasts which improve intelligibility
E Backing to velar In the younger subjects (aged 16ndash46) as articulatorypatterns progressed anteriorly a preference for [g] was common Mostcommonly backing resulted in t d realized as [k g] and s z as [x aring ]which contrasts with the fronting pattern seen in normal development
Double articulation
This is de ned as two simultaneous equal strictures at two places of articulationwhich was frequently noted in realizations of target alveolar consonants t d whenalveolarvelar contacts [tkk dkg] were used Double articulation may have beendeveloped to distinguish between alveolar and velar consonants in the presence ofa backing pattern Interestingly double articulation became evident in these develop-ing speech patterns with the emergence of fricative realizations Both plosives andfricatives tended to be realized with double articulation eg tndash[tkk] sndash[skagrave ]
Active versus passive cleft-type speech characteristics 337
Palatal fricatives [c J ]
These fricative realizations of alveolar target consonants appeared towards the endof the study period (ages 16ndash46) They were the most common realizations ofalveolar fricatives in older children (46ndash76 and 100ndash110) This nding was inaccordance with Alberyrsquos results (Albery 1991 Albery and Grunwell 1993)
Lateral fricatives [l Igrave]
As with palatal fricatives lateral fricatives were frequently present as realizations offricative consonant targets becoming particularly prevalent in later phonologicaldevelopment
Gliding of fricatives s S= [ j] or [w]
This phenomenon is seen in the non-cleft population as an uncommon develop-mental process (Grunwell 1987) It is classi ed here as an active process because[ j] was consistently produced as an apparently active alternative to target conson-ant(s) s z S [ j] is a normal consonant-like production in non-cleft babble whichcleft palate children often integrate into their phonological system It may betherefore that it is a persisting immaturity in the cleft palate population In thesedata [ j] was eVective in signalling a contrast between plosives and fricatives inSIWI position It functioned for the following consonants in diVerent speakers [ j]for S [ j] for m p f s z Ÿ h and co-articulation [hkj] for T
Passive cleft type processes
The criteria for passive cleft type processes is that they are (1) an attempt toproduce the correct articulatory placement and stricture (manner) which (2) failsbecause of a lack of intra-oral air pressure For example voiced plosives realized asnasals b[ [m] d[ [n] g[ [Icirc] No compensatory articulatory pattern hasbeen used to replace the intended consonant As the above examples demonstratetarget realizations often match a similar English consonant
Absence of pressure consonantspredominantly sonorant articulation
This phenomenon is de ned here as a pattern of articulation which was restrictedto English nasal and approximant articulations [m n Icirc w j] and [h] Some of thevoiced consonants were also employed as voiceless counterparts [m
degndeg Icircdeg ] thereby
increasing the range of available consonants for distribution in the phonologicalsystem Despite the limited consonant repertoire these patterns were often eVec-tively interpreted by close family members
Weak articulation [bV dV]
This category refers to normal articulatory movement in the production of obstruenttargets (plosive fricative and aVricate targets) which were produced with reducedoral air pressure and therefore articulation was considerably weakened In the speechsample data (ages 16ndash46) many target consonants were weakened to some degreeand at times may have been realised as nasals
A Harding and P Grunwell338
Passive nasal fricative [(fk)m (sk)ndeg]
Incomplete velopharyngeal closure inevitably reduces control of oral air ow with apassive loss of air ow and an increase of resonance in the nasal cavity Grunwelland Harding (1996) de ned the passively nasal fricative as an unreleased [(s)]double-articulated with a lowered voiceless nasal [n
Aacute
deg] This realization is the product
of an intended s with an unintended nasal air ow (see gure 4) The precisetranscription for a passive nasal transcription is [(sk)n
Aacute
deg] but an acceptable simpli cation
for transcription purposes is [(sk)ndeg] This is distinct from the active nasal fricative
which involves stopping of the oral air ow and active direction of air nasally whichcan be transcribed as a voiceless nasal with additional nasal emission [n
degk] Nasal
emission signals the fricative nature of for example target consonant s Thesetwo productions can sound the same and might initially be transcribed as [n
degk]
Nasendoscopic investigation of velopharyngeal activity during active and passivenasal realizations of s both show a lack of velopharyngeal closure It is predictedthat close examination by use of electropalatography might show slight diVerencesin tongue tip posture for an active and passive nasal fricative as illustrated in gures3 and 4 Passive nasal fricatives were converted into oral fricatives with nose-holding
Voiceless [h] for voiceless plosives
There was evidence that voiceless plosives were at times passively realized as [h]The consequence of reduced oral air pressure on production of voiceless plosivescan leave aspiration as the only perceptible distinctive feature This process usuallyaVected all voiceless plosive targets p t k Where this process was a passiveprocess use of noseholding during speech facilitated accurate target productionHowever it would also be possible for this distribution of [h] to be an active cleft-type process which would be part of a pharyngealglottal patternprocess
Nasal realization of voiced plosives b d g[ [m n Icirc]
Some subjects with residual clefts stulae or suspected VPI realized voiced conson-ants as nasal counterparts As summarized by Harding and Grunwell (1996) voiced
Figure 4 Passive nasal fricative [(sk)nAacute
deg]
Active versus passive cleft-type speech characteristics 339
consonants can be more diYcult to produce than voiceless consonants (Isshiki andRingel 1964) Distinction between active versus passive nasal realizations of plosivetargets was made in the same way that active and passive nasal fricatives weredistinguished by observing the eVect of noseholding on consonant production Inpassive nasal realizations noseholding facilitated normal consonant production(Golding-Kushner 1995)
Nasal emission accompanying consonants [pk sk]
Nasal emission was frequently heard accompanying consonants but on occasions itapparently replaced consonants It has been linked with velopharyngeal incompet-ence (VPI) (Kummer et al 1992)
Results
Comparison of activepassive processes in the speech data
Quantitative results of Hardingrsquos research into the relationship between timing ofsurgery and speech development have already been published (Harding andGrunwell 1993) The following interpretation of the data speci cally identi esactivepassive cleft-type processes in relation to oral structure in a wide age rangeof subjects (16ndash130) Tables 1 2 3 and 4 show the passive and active processeson the left-hand column and the subjectrsquos code along the top The code identi esthose subjects who were treated with 1-stage versus 2-stage surgery Comparisonof the 4 tables at age 46 (BCLP and UCLP) at age 90 and at age 130 illustratesa pattern of diminishing cleft-type processes with increasing age Irrespective ofsurgical timing few cleft-type processes remained at age 130 (table 4) A generalobservation was that earlier speech samples (ages 16ndash76) frequently combined
Table 1 Cleft-type processes in BCLP subjects at age 46 (studies 1 and 2)
1-stage surgery 2-stage surgery
A G Rf JW D B JF JG AB
Passive cleft-type processespredominantly sonorant articulation m
weak articulation m m m m m m m m
voiceless h for plosive m m m m m
nasal release of plosives m m m m m
nasal emission with consonants m m m m m m
passive nasal fricativeActive cleft-type processes
nasal fricatives m m m m m m m m
pharyngeal glottal articulation m m m m m m m m
backing to uvular m m m m m m m m
backing to velar m m m m m m m m m
lateral palatal fricatives m m m m m m m m m
double articulation m m m m m m m m m
gliding fricative m m
f=post-operative stula
A Harding and P Grunwell340
Table 2 Cleft-type processes in UCLP subjects at age 46 (study 2)
1-stage surgery 2-stage surgery
SE TB CK MS NC TS ZG CP
Passive cleft-type processespredominantly sonorant artic m
weak articulation m m m
voiceless h for plosives m m m
nasal release of plosives m m m
nasal emission with consonants m m
passive nasal fricative m m
Active cleft-type processesnasal fricativepharyngeal glottal articulation m m m
backing to uvular m
backing to velar m m
lateral palatal fricatives m m m m m
double articulation m m m m m m
gliding fricative m
Table 3 Cleft-type processes at age 90
2-stage surgery 2-stage surgery1-stage surgery completed at 4 yrs completed at 8 yrs
DAf SBf RL NR JD AR LJ RP MB
Passive cleft-type processespredominantly sonorant articweak articulation m
voiceless h for plosives m m
nasal release of plosives m m
nasal emission with consonants m m m m
passive nasal fricatives m m
Active cleft-type processesnasal fricatives m m
pharyngeal glottal articulation m m
backing to uvular m m
backing to velar m m m m m m m
lateral palatal fricatives m m m m m m m
double articulation m m m m m
gliding fricative m
f=subject had a stula
both active and passive strategies whereas later samples (ages 90ndash130) rarelyevidenced passive processes
At age 46 four out of ve BCLP subjects used active non-oral pharyngeal andglottal processes and oral velar and uvular fricatives irrespective of surgical status(see table 1) All had some anterior palatal defect which might have reduced theirpotential to achieve intra-oral pressure
By comparison two out of three partially repaired 2-stage UCLP subjects at age46 (table 2) showed evidence of passive processes This suggested that their
Active versus passive cleft-type speech characteristics 341
Tab
le4
Spee
chin
rela
tion
tosu
rgic
altim
ing
atag
e13
0
2-st
age
surg
ery
2-st
age
surg
ery
1-st
age
surg
ery
subj
ects
com
plet
edat
4yr
sco
mpl
eted
at8
yrs
1-A
1-B
1-C
1-D
1-E
1-F
24-
G2
4-H
24-
J2
8-K
28-
L2
8-M
Pass
ive
clef
t-ty
pepr
oces
ses
pred
omin
antly
sono
rant
artic
wea
kar
ticul
atio
nm
voic
eles
sh
fo
rpl
osiv
esna
sal
rele
ase
ofpl
osiv
esna
sal
emis
sion
with
cons
onan
tsm
pass
ive
nasa
lfr
icat
ives
Act
ive
clef
t-ty
pepr
oces
ses
nasa
lfr
icat
ives
phar
ynge
alg
lott
alar
ticul
atio
nba
ckin
gto
uvul
arba
ckin
gto
vela
rm
m
late
ral
pala
tal
fric
ativ
esm
mm
doub
lear
ticul
atio
ngl
idin
gfr
icat
ive
1=1-
stag
esu
rger
ysu
bjec
ts
24=
2-st
age
surg
ery
hard
pala
tere
pair
edat
abou
t4
yrs
28=
2-st
age
surg
ery
with
hard
pala
tere
pair
edat
abou
t8
yrs
A Harding and P Grunwell342
unrepaired hard palates had in fact restricted their phonetic repertoire imposing aneed for individual adaptability The additional active processes employed by thesesubjects were presumably a response to the restrictions imposed by their oro-nasalstructure and velopharyngeal function at the time of consonant acquisition Asshown in table 2 the most common active cleft-type processes persisting at age46 with a residual cleft of the hard palate were backing double articulation andlateralpalatal articulation Two 1-stage surgery subjects whose entire palates hadbeen repaired at ages 09 and 010 did not use any cleft-type processes at age 46
By age 90 (table 3) a much-diminished number of cleft type processes wasevident except in subjects with sizeable anterior stulae who had received littlespeech and language therapy A similarity was noted between the speech patternsof 1-stage surgery subjects with stulae (DA and SB) at age 90 (table 3) and theyounger BCLP subjects at age 46 (table 1) who also had anterior palatal defectsThey included non-oral realizations of t d s k g occasional nasal fricatives andpharyngealglottal articulations Fistulae had apparently continued to in uencearticulation and phonological development in these subjects
Finally at age 130 (table 4) the diVerences between 1-stage and 2-stage surgerysubjects had diminished leaving only one 2-stage subject with occasional backingand four subjects with slight palatal and lateral release of fricative consonants Onlytwo of the 1-stage surgery subjects were using minor distortions of grooved fricativeproduction
Whilst there were apparent trends in speech production relating to surgicaltiming and oral structure it is noted that there were exceptions to each tentativegeneralization Subjects with marked structural imperfections occasionally producedrealizations of which they would not have been thought capable and subjects withno visible imperfections produced inexplicably distorted speech patterns It istherefore concluded that whilst there is homogeneity in the range of processesproduced by this population assumptions cannot be made about speech based onsurgical timing or type of cleft Tentative predictions based on detailed assessmentmay be clinically very useful
EVects of surgery on speech
Activepassive processes have identi ed those cleft-type characteristics thought tobe associated with a physical inability to produce pressure consonants The followinganalysis of speech changes after surgical intervention at diVerent ages identi es thechanges eVected by surgery when intra-oral pressure could be more readily achieved
Two children were rst recorded prior to the rst stage of a 2-stage procedureTheir lips were repaired at approximately 6 months of age and soft palate repairwas carried out at ages 18 and 19 respectively Their hard palates were leftunrepaired to facilitate unrestricted growth of the mid-face (Hotz et al 1978) Pre-and post-operative consonant-like sounds present in the recorded speech samplesare listed in table 5 Interestingly prior to soft palate repair both these childrenproduced some oral consonants Subject B was producing pressure consonants [kg] in his babble prior to soft palate repair Considering that he had an unrepairedbilateral cleft palate at this point it was surprising that he had any oral consonantsPost-operatively at 20 years he used [b bkm t d g gkb] which indicated that surgeryto repair the soft palate had facilitated an increased range of oral pressure consonantsSubject D was producing [p b k g] pre-operatively Post-operatively following soft
Active versus passive cleft-type speech characteristics 343
Tab
le5
EV
ects
ofso
ftp
alat
ere
pair
atag
e1
6on
BC
LP
subj
ects
h
ard
pal
ate
rem
ain
sun
repa
ired
2-st
age
subj
ects
Surg
ery
Pre
-ope
rati
vesp
eech
patt
ern
atag
e1
6Po
st-o
pera
tive
chan
ges
insp
eech
atag
e2
0
Stud
y1
BSo
ftpa
late
repa
irat
16
Adu
ltta
rget
sk
gA
t2
0[b
b kmg kb
td
g]D
Soft
pala
tere
pair
17
Adu
ltta
rget
sp
bk
gA
t2
0[p
bd
b kdk
g]
Tab
le6
EV
ects
ofha
rdpa
late
rep
air
atag
e6
6an
d
stu
lare
pair
atag
e10
0
Subj
ect
Surg
ery
Pre
-ope
rati
vesp
eech
patt
ern
Post
-ope
rati
vech
ange
sin
spee
ch
MS
Har
dpa
late
repa
ir6
6Pa
ssiv
epr
oces
s7
6E
limin
ated
pass
ive
proc
ess
Var
iabl
ena
sal
rele
ase
ofco
nson
ants
Hyp
onas
alna
sals
JFH
ard
pala
tere
pair
(uns
ucce
ssfu
l)6
6Se
vera
lac
tive
and
pass
ive
proc
esse
s7
6A
ctiv
epr
oces
ses
rem
aine
dPa
ssiv
epr
oces
ses
elim
inat
ed
DA
Fis
tula
repa
ir10
0A
ctiv
epr
oces
ses
110
Elim
inat
ion
ofph
aryn
geal
glo
ttal
Var
iabi
lity+
+an
dna
sal
arti
cula
tion
Art
icul
ator
yva
riab
ility
++
Act
ive
CT
Rs
proc
esse
spe
rsis
t
A Harding and P Grunwell344
palate repair but with a residual cleft in the hard palate his range of consonantsincluded [d] which was particularly surprising since the hard palate remainedunrepaired Whilst it is unlikely that toddlers of 18 months could be consciouslytrying to compensate for articulatory inadequacy in producing velar plosives inbabble prior to soft palate repair and an alveolar plosive prior to hard palate repairboth these subjects showed evidence of actively pursuing their articulatory potential
Table 6 summarizes changes following surgery to repair the hard palate in moremature speech patterns These subjects who were aged 66 and 100 pre-operativelyhad learned to speak with residual clefts and were apparently unaware of theconsonant productions that failed to match normal production
Subject MS used only passive processes in his speech pattern He realized someconsonants nasally such that lsquoballrsquo was [mO~] and lsquosockrsquo was [(sk)n
deg Aacute~ k] Looking atpost-operative changes at age 76 his consonant production was normal but hisresonance had become hyponasal Pre-operatively at age 66 Subject JF was usingseveral active and passive processes The active processes were unaVected by surgerybut passive processes were eliminated
Fistula repair was carried out at age 100 on Subject DA who had many activeprocesses and very variable articulation pre-operatively Post-operatively at age110 he was not using non-oral pharyngeal and glottal active processes or nasalrealizations but many oral cleft-type realizations remained
As shown in table 7 hard palate re-repair and pharyngoplasty was carried outon two subjects whose hard palate repairs had been unsuccessful at approximately4 years Subject NC assessed pre-operatively at age 56 was using predominantlypassive processes in her speech She was also using [ j] for fricatives s S whichwas thought to be an active process At age 60 following hard palate re-repair andpharyngoplasty all cleft-type processes had been eliminated without post-operativespeech therapy Since [ j] for s apparently resolved spontaneously followingsurgery it can be assumed that this was a passive process in this speech sample
Subject CP who underwent this procedure presented pre-operatively at age 46with both passive and active processes but his nasal resonance was not consistentlyhypernasal In addition to his cleft-related speech disorder this subject had additionaldevelopmental speech diYculties which were identi ed as being unrelated to thecleft Post-operatively at age 56 little had changedmdashnotably the passive processnasal [m] for b was retained His nasal resonance had become hyponasal andthere was no apparent bene t from surgical intervention The realization of b as[m] had become phonologically stable and surgery alone had not destabilized thephonological system This realization may have been a passive product of VPI inearly speech acquisition which had subsequently become part of a phonologicaldisorder Post-operatively CPrsquos phonetic repertoire did increase but the phonologicaldistribution was variable Plosive targets were still realized as nasals in spontaneousspeech at the nal speech recording at age 76 This was not as an inevitableconsequence of VPI but a result of an inability to destabilize the phonologicalprocess determining that voiced plosives would be realized as nasals This resultfollowing surgery highlights the importance of identifying phonological learningproblems and distinguishing them from structural constraints on articulationIn CPrsquos case pre-operative exploration of the eVect of nares occlusion duringspeech might have indicated that structural change would not improve consonantproduction spontaneously
A general observation was that consonant realizations did not move rapidly
Active versus passive cleft-type speech characteristics 345
Tab
le7
EV
ects
ofha
rdpa
late
re-r
epai
ran
dp
hary
ngo
pla
sty
Subj
ect
Surg
ery
Pre
-ope
rati
vesp
eech
patt
ern
Post
-ope
rativ
ech
ange
sin
spee
ch
Stud
y2
NC
Har
dpa
late
re-r
epai
ran
d5
6Pa
ssiv
ecl
eft-
type
proc
esse
s6
0A
llcl
eft-
type
phar
yngo
plas
ty5
10[
j]
for
fric
ativ
espr
oces
ses
elim
inat
ed[
h]
for
plos
ives
SIW
IV
aria
ble
arti
cula
rypr
ecis
ion
CP
Har
dpa
late
repa
iran
d4
6Pa
ssiv
ean
dac
tive
proc
esse
s5
6Pa
ssiv
epr
oces
sph
aryn
gopl
asty
50
Pho
nolo
gica
lco
nfus
ion
[m]
for
[b
]re
tain
edH
ypon
asal
nasa
lsPe
rsis
ting
phon
olog
ical
conf
usio
ns
A Harding and P Grunwell346
from incorrect to correct but progressed incrementally towards normal realizationsas described by Morley (1970) Where an early realization of target s might beglottal [h] a gradual pattern of change showed subsequent realizations to bepharyngeal [Eacute] then uvular [X] then velar [x] and eventually palatal [c] or lateral [Euml]It was interesting to note that speech patterns continued to change as late as90ndash110 years with the result that diVerences related to surgical timing and cleft-type gradually disappeared Persisting stulae were thought to account for the mostmarked cleft type processes at age 90
Implications for surgical management
This analysis of speech changes following surgery suggests some implications forsurgical management which are compatible with Sell and Grunwellrsquos (1990) ndingsin the Sri Lankan study
Surgery can change passive speech processes but it is also possible that speechtherapy may be able to change passive patterns Surgery alone is unlikely to modifyactive cleft-type processes whereas speech therapy should be able to modify activeprocesses Indications from these case studies is that where speech is the primaryproblem speech assessment should distinguish between active and passive processesin order to evaluate the necessity for full investigations and to plan therapeuticintervention Where past speech therapy has not been successful it cannot beassumed that surgical intervention will facilitate further speech progress A furthercourse of speech therapy which is sensitive to active versus passive processes todevelopmental phonological in uences on cleft-type speech development and toarticulatory diYculties in diVerent speech contexts might facilitate optimal progressWhere structural imperfection exists it is quite possible for single-word productionto be more precise than target realizations in spontaneous speech This may not bea failure of phonological generalization (Grunwell 1992) but the result of diYcultysustaining the necessary lsquoarticulatory eVort rsquo (Harding and Grunwell 1993) resultingin articulatory imprecision Deteriorating articulatory accuracy should not be over-looked in interpretation of speech results
An analytical protocol
As a result of analysing the speech data and identifying the active and passiveprocesses a protocol has been developed which records examples of each cleft-typeprocess over a series of assessments It demonstrates the progression of individualprocesses towards an adult target (see the Appendix) At each assessment onecolumn is used to indicate nasal resonance nasal emission and nasal turbulenceratings and cleft-type processes Changes in the nature of error realizations mightshow progress towards target consonants Hence whilst the total correct scoremight not have increased increments of change can be observed This observationof patterns of change may function as an adjunct to GOSSPASSrsquo98 (Sell et al 1998)giving access to a greater depth of both quantitative and qualitative data aboutconsonant production in relation to resonance nasal emission nasal turbulenceoral structure and cleft-type
Active versus passive cleft-type speech characteristics 347
Diagnostic implications
Passive versus active nasal fricatives
The important management consideration related to this distinction is that an activenasal fricative is an established phonological process which is unlikely to be directlyaVected by surgery alone Therapy would be necessary to destabilize nasal realizationsof oral consonants In contrast passive nasal fricatives may be eliminated by surgeryOf particular relevance is diVerential diagnosis between passive and active nasalfricatives in surgical and therapeutic management When hypernasality co-occurswith nasal air ow during consonant production which can be redirected by nose-holding passive nasal fricatives are diagnosed These would be transcribed as [(sk)n
deg]
passive alveolar nasal fricatives [(Wk)mdeg
] bilabial nasal fricatives or [(fk)Iacutedeg ] labiodentalnasal fricatives Full VPI investigations would be recommended to diagnose thenature of the structural or functional de ciency and distinguish between velopharyn-geal incompetence and velopharyngeal mislearning
It is highly likely that plosive targets would be aVected by reduced intra-oral airpressure such that plosives would either be realized by nasal counterparts eg bd[ [m n] or [b d] may be nasalized and weak Voiceless plosives may be eitheraccompanied by nasal emission [p t k] or realized as glottal fricative [h]
Production of the target sentence lsquoI saw Sam sitting on a busrsquo might be
[aI (sk)ndeg O~ (sk)n
degaelig~m (sk)n
deg IhIn Aacute~n mouml~(sk)ndeg] passive processes and
[aI xO xaeligm xIkIIcirc AacuteIcirc goumlx] active processes
Contribution to surgical management decisions
Passiveactive interpretation of clinical assessments might facilitate surgical manage-ment decisions If noseholding does not facilitate correct production of targetconsonants then it is likely that an alternative articulatory pattern has becomephonologically established ie particular realizations for one or more targets areconsistently distributed in the phonological system These realizations may haveevolved because of initial diYculty producing articulatory targets and subsequentlystabilized within the phonological system Grundy and Harding (1995) refer to thisphenomenon as an lsquoarticulatory disorder with phonological consequencesrsquo
Therapy
Where obvious structural defects or diagnosed dysfunction exists clinicians fre-quently defer therapeutic intervention until surgery has been undertaken Theexpectation would be that normal structure and function is essential for normalspeech However pre-operative therapy may facilitate oral consonant productionwhich may serve to reduce hypernasal resonance Hence therapy prior to surgerymay avoid unnecessary surgery or reduce the extent of surgery required All activeprocesses are likely to require therapy
Principled selection of targets for therapy
Speech patterns frequently evidence a mixture of apparently passive and activeprocesses which complicates decisions about target selection Target selection can
A Harding and P Grunwell348
be based on assessment of which consonant targets can be most easily elicted inisolation (stimulability) This may lead to a sequence of target selection which isopposite to the sequence of consonant acquisition in normal development Forexample where reduced intra-oral pressure is present in a passive pattern [T] maybe easier to elicit in imitation than more nely grooved [s] or [S] Therapy maytarget [T] followed by [S ] and nally [s] As in non-cleft phonological therapywhere a class of consonants is aVected by the cleft then it is helpful to target theentire class The following decision-making process can be applied for both activeand passive processes
Decision making procedure for target selection
(1) Voiced versus voiceless targets(2) Front versus back placements(3) Syllable initial versus syllable nal targets(4) Plosives versus fricative targets
Voiceless plosives and fricatives are produced with an open glottis whichfacilitates topping up of air ow from the lungs hence voiceless plosive and fricativetargets are frequently more successful than voiced counterparts (Isshiki and Ringel1964) Front targets usually cause more diYculty than back particularly where analveolar defect or stula exists Contrary to normal development back targets maybe targeted before front Word- nal targets generally require less oral air pressurethan word initial targets and similarly fricatives may be more easily elicited thanplosives Fricatives do require a greater volume of air than plosives (Fletcher 1985)but in the presence of nasal escape weak fricative production appears to be morereadily achieved than weak plosive production Since nal fricatives would normallybe acquired in advance of word-initial fricatives (Ferguson 1978) targeting word- nal fricatives is frequently a productive starting point for therapy
Principles of therapy for passive processes
(1) Use of soft attack similar to gentle whisper for all target models ensuresminimal articulatory eVort (Harding and Grunwell 1993) and requires min-imal intra-oral air pressure It may be appropriate to gradually increase thearticulatory attack when the articulatory posture and evidence of intendedoral air ow have been established
(2) Slightly stretched duration of segment transitions in models of consonantto vowel (CndashV) or vowel to consonant (VndashC) facilitates review of motorplanning and extends the available time for execution of the new motorprogrammer whilst maintaining control of the oral airstream
(3) Noseholding can be used to provide exclusively oral air ow Gradual releaseof the nostrils during production of sustained [VVVVVf ] or [hhhhh ] allowsthe child to attempt to sustain an oral consonant despite increasing nasalemission This maximizes the use of available oral air ow Procedures forusing noseholding are described in some detail by Golding-Kushner (1995)
Principles of therapy for active processes
This is more like phonological therapy and can follow Grunwellrsquos (1991) processesfor phonological change and principled decision-making (Grunwell 1992) Some
Active versus passive cleft-type speech characteristics 349
examples are given here by way of illustration of ways to eVect the rst twoprocesses of change which may need to be approached diVerently in cleft palateversus non-cleft speech disorders DiVerent approaches may also be appropriate formodifying active versus passive cleft-type processes
Innovation production of new targets Some useful principles
(1) Introduction of new lsquonon-speech likersquo targets in sound play using a conson-ant sound segment model such as [ph ] note not a syllable like [p] whichis the type of pronunciation used when target sounds are presented as lettersfor reading Target [s] might be introduced as a lsquoTrain Slowing Down Noisersquo[ts ts ts tssssssss]
(2) lsquoNew consonantsrsquo can later be modelled and elicited in soft productions ofsyllable structure [tssssndashi] [ indashtssss] which can subsequently be identi ed assimilar to words lsquosearsquo and lsquoeatsrsquo
(3) lsquoDeferring responsibilityrsquo transfers responsibility or lsquoblamersquo for errors fromthe child and attributes it to the articulators eg lsquoyour tongue is havingtrouble with hellip rsquo lsquoLetrsquos show your tongue how to hellip rsquo
(4) New targets can be modelled repeatedly and recorded on audio or videotape which can be listened to at home
(5) Targeting classes of consonants (eg alveolars t d s n l voiceless fricativesf s S perhaps with aVricate T avoids phonological confusion whichmight occur if production ofsis achieved whilst other alveolar targetsremain backed The risk is that s might not integrate into the phonologicalsystem unless all backed alveolar consonants are destabilized
(6) Increased eye contact during auditory and production work can be invaluablein holding visual and auditory attention and ensures that visual informationabout the sound has been processed This is easily achieved by the clinicianlifting any focus of the childrsquos attention close to hisher mouth at theprecise moment when the target is modelled
Stimulation of non-speech related sounds such as a lsquoTrain Slowing DownNoisersquo [ts ts tsss] con rms that target [s] is physically achievable whether or not[ssss] can be imitated Some children continue to access [s] through the lsquoTrainSlowing Down Noisersquo throughout therapy until it is occurring spontaneouslywithout conscious planning This can be an eVective means of underminingestablished motor programmers (Hewlett 1990) for active cleft-type processes
Destabilizing active processes
As it is likely that children will be unaware of each occurrence of their alternativearticulatory pattern for speci c consonant errors it is preferrable to destabilizeactive processes with minimal conscious eVort by the child As children becomeaware of their mismatches they frequently add the newly acquired target realizationto their existing production eg target word tu childrsquos old realization [ku] childrsquoscorrected realization [t-ku] Destabilization can be achieved with minimal consciouseVort through input therapy techniques such as auditory bombardment (Lancasterand Pope 1989) auditory decision-making such as lsquowhich bear says this wordproperlyrsquo Red Bear says lsquotworsquo or Blue Bear says lsquocoorsquo This type of strategy oftenprecipitates attention to the target consonant with possible lsquoreplayrsquo and lsquoreviewrsquo of
A Harding and P Grunwell350
their own production Frequent stimulation of cognitive alertness to the targetconsonant can develop awareness without confronting the child with errors orrisking hisher failure The child is then free to attempt to repair hisher ownrealization to continue to re ect and to silently rehearse the adult realizationTraditional articulation therapy is thus combined with development of metaphonol-ogical skills ie the ability to re ect upon onersquos own speech production The resultshould be that new target realizations will be more phonologically stable thanexclusively production-based articulation therapy might have facilitated
Stabilizationgeneralization
Procedures to ensure stabilization and generalization of new target consonantswould be as described by Grunwell (1992) Success may be constrained by theconsiderable articulatory eVort sometimes required to maintain pressure consonantproduction in spontaneous speech (Harding and Grunwell 1993)
Conclusions
In speech assessment it is helpful to distinguish between errors which are cleft-type and non-cleft type and those which are part of active versus passive processesThe active and passive processes have been de ned and their phonological implica-tions discussed Focus on active and passive processes has facilitated focus on thephonological consequences of cleft palate on speech development In the futureawareness of the likely eVect of a cleft palate on normal phonological developmentcould avoid extended periods of unsuccessful clinical intervention Furthermoresensitivity to the relationship between phonological processes and structural con-straints should facilitate theoretically based management decisions Incidences suchas the case of CP in which nasal realizations were thought to indicate VPI but weresubsequently unaVected by surgery might be avoided if phonological analysiscontributes to management decisions
Surgery did improve hypernasal resonance and eliminated passive processes buthad little eVect on active processes Active processes in younger subjects werethought to require therapeutic intervention but in the longer term the oldersubjects showed few cleft-type processes Whilst it is possible that active cleft-typeprocesses may resolve with increasing age the implication for the future is thatactive cleft-type processes should be treated with skilled therapeutic interventionnot surgery Therapy which addresses the phonological consequences of cleft palateon speech development by combining metaphonologicalphonologicalarticulatoryapproaches is likely to be successful
References
Albery E 1991 Consonant articulation in the diVerent types of cleft lip and palate UnpublishedMPhil thesis Leicester Polytechnic
Albery E and Grunwell P 1993 Consonant articulation in diVerent types of cleft palate InP Grunwell (Ed) Analysing Cleft Palate Speech (London Whurr)
Ferguson C A 1978 Fricatives in child language acquisition In V Honsa and M Hardmann-Battista (Eds) Papers on Linguistics and Child Language (Mouton The Hague)
Fletcher S G 1985 Speech production and oral motor skill in an adult with an unrepaired palatalcleft Journal of Speech and Hearing Disorders 50 254ndash261
Active versus passive cleft-type speech characteristics 351
Golding-Kushner K J 1995 Treatment of articulation and resonancne disorders associated withcleft palate management and VPI In R Shprintzen (Ed) Cleft Palate Speech Management AMultidisciplinary Approach (St Louis Mosby)
Grundy K and Harding A 1995 Developmental speech disorders In K Grundy (Ed) Linguisticsin Clinical Practice (2nd edition) (London Whurr)
Grunwell P 1985 Phonological Assessment of Child Speech (Windsor NFER-Nelson)Grunwell P 1987a Clinical Phonology (2nd edition) (London Croom Helm)Grunwell P 1987b PACS Pictures Language Elicitation Materials (Windsor NFER-Nelson)Grunwell P 1991 Processes of phonological change in developmental speech disorders Clinical
Linguistics and Phonetics 6 101ndash122Grunwell P 1992 Principled decision making in the remediation of children with phonological
disorders In P Fletcher and D Hall (Eds) Specic Speech and Language Disorders in Children(London Whurr)
Grunwell P and Harding A 1995 PACSTOYS A Screening Assessment of Phonological Development(Windsor NFER-Nelson)
Grunwell P and Harding A 1996 A note on describing types of nasality Clinical Linguistics andPhonetics 10 157ndash161
Harding A 1993 An Investigation into the Relationship Between Timing of Cleft Palate Repairand Speech Development Unpublished PhD thesis
Harding A and Grunwell P 1993 The relationship between speech and timing of hard palaterepair In P Grunwell (Ed) Analysisng Cleft Palate Speech (London Whurr)
Harding A and Grunwell P 1996 Characteristics of cleft palate speech European Journal ofDisorders of Communication 31 331ndash358
Henningsson G and Isberg A M 1986 Velopharyngeal movement patterns in patients alternatingbetween oral and glottal articulation A clinical and cineradiographicical study Cleft Palate Journal23 1ndash9
Hewlett N 1990 Processes of development and production In P Grunwell (Ed) DevelopmentalSpeech Disorders (Edinburgh Churchill Livingstone)
Hotz M M Gnoinski W M Nussbaumer H and Kistler E 1978 Early orthopaedics in CLPcases guidelines for surgery Cleft Palate Journal 15 405ndash411
Hutters B and Brondsted K 1987 Strategies in cleft palate with special reference to DanishCleft Palate Journal 24 127ndash136
Isshiki N and Ringel R 1964 Airow during the production of selected consonants Journal ofSpeech and Hearing Research 7 233ndash244
Kummer A W Curtis C Wiggs M Lee L and Strife J L 1992 Comparison of velopharyngealgap size in patients with hypernasality hypernasality with nasal emission and nasal emissionor nasal turbulence (rustle) as the primary speech characteristic Cleft-palate-Craniofacial Journal29 152ndash156
Lancaster G and Pope L 1989 Working with Childrenrsquos Phonology (Oxford Winslow)Morley M E 1970 Cleft Palate and Speech (7th edition) (Edinburgh Churchill Livingstone)Russell V J 1991 Speech Development in Children with Cleft Lip and Palate Unpublished PhD
thesis Leicester PolytechnicRussell V J and Grunwell P 1993 Speech development in children with cleft lip and palate In
P Grunwell (Ed) Analysing Cleft Palate Speech (London Whurr)Sell D A and Grunwell P 1990 Speech results following late palatal surgery in previously
unoperated Sri Lankan adolescents with cleft palate Cleft Palate Journal 27 162ndash168Sell D Harding A and Grunwell P 1994 GOSSPASS A screening assessment of cleft palate
speech European Journal of Disorders of Communication 29 1ndash15Sell D Harding A and Grunwell P 1998 GOSSPASSrsquo98 An assessment for speech disorders
associated with cleft palate andor velopharyngeal dysfunction International Journal of Languageamp Communication Disorders ( in press)
Shorter E 1995 A spectographic analyis of child homophones Unpublished honours project DeMontfort University Leicester
Stenglehoffen J 1989 Nature and causes of communication diYculties In J Stengelhofen (Ed)Cleft Palate Nature and Remediation of Communication Problems (Edinburgh Churchill Livingstone)
Trost J E 1981 Articulatory additions to the classical description of the speech of persons withcleft palate Cleft Palate Journal 18
Trost-Cardamone J E 1990 The development of speech assessing cleft palate misarticulationsIn D A Kernahan and S N Rosenstein (Eds) Cleft Lip and Palate A System of Management(Baltimore Williams amp Wilkins)
A Harding and P Grunwell352
Appendix Active passive analysis of cleft palate speech

A Harding and P Grunwell330
guage therapy before the potential bene ts of surgery can be properly assessedAn analytical protocol for the interpretation of speech samples is presented andsome therapy strategies are proposed for active and passive processes
Keywords activepassive processes cleft palate speech and language therapysurgical timing
Introduction
Whilst lsquocleft palate speech problemsrsquo are commonly regarded as lsquoarticulatory dis-ordersrsquo Russell and Grunwell (1993) Harding and Grunwell (1993) and Hardingand Grunwell (1996) have reconsidered cleft palate speech characteristics in thecontext of phonological development The outcome of this phonological and devel-opmental perspective on cleft palate speech in uenced the GOSSPASS protocol(Sell et al 1994) and GOSSPASSrsquo98 (Sell et al 1998) which has recently beenselected by a panel of experienced clinicians as the preferred protocol for assessingcleft palate speech in the UK It is sensitive not only to the articulatory eVects ofthe cleft but also to idiosyncratic phonological processes commonly heard in cleftpalate speech
As described by Harding and Grunwell (1996) Hutters and Brondsted (1987)observed that some children with a cleft palate apparently respond to a subconsciousawareness of their limited phonetic and phonological repertoire by activelyemploying non-native sounds from their phonetic repertoire in order to maximizetheir range of meaningful contrasts Other children more passively continue tomake the appropriate articulatory movements with no apparent response to theabsence of adequate contrasts in their speech This distinction between active andpassive responses to the articulatory constraints imposed by the cleft forms thebasis of the 1987 theory of Hutters and Brondsted of active and passive strategiesMorley (1970) categorized her speech results into Groups A and B such that GroupA made no adaptations to articulation but nasal escape nasal tone and weakconsonants were noted These characteristics resemble Hutters and Brondstedrsquos(1987) passive strategies whereas speech characteristics in Group B included addi-tional symptoms of nasopharyngeal snort glottal and pharyngeal articulation andincorrect articulation Morleyrsquos (1970) Group B is equivalent to Hutters andBrondstedrsquos (1987) active strategies Subjects with normal velopharyngeal functionbut persisting articulatory errors were included in this group Trost-Cardamone(1990) made a similar distinction in her description of categories I and II in cleftpalate speech characteristics Category I misarticulations were said to be lsquostructurallybased and revealed in audible nasal emission of high pressure consonantsrsquo (stopsfricative and aVricates) and Category II misarticulations were compensatory articu-lations and atypical backed distortions Category I is equivalent to Hutters andBrondstedrsquos (1987) passive strategies and Category II to active strategies Golding-Kushner (1995) distinguishes between compensatory and obligatory articulatoryerrors Compensatory errors would be product of active strategies and obligatoryerrors would be the product of passive strategies Obligatory errors are describedas resulting from an anatomic defect and are lsquonot easily amenable to therapyrsquo(Golding-Kushner 1995)
The four ways of grouping cleft-type characteristics described above all indicatethat some characteristics are an inevitable consequence of structural imperfection
Active versus passive cleft-type speech characteristics 331
andor velopharyngeal dysfunction However none of the distinctions have beenexpressed with reference to their potential impact on phonological developmentStengelhofen (1989) noted that reduced intra-oral pressure may result in nasalrealization of voiced plosives b d gmdash[m n Icirc] This can have a devastating eVecton speech development because plosives [b d] usually represent most fricative targetconsonants in early speech acquisition (age 10ndash20 approx) The phonologicalconsequence of loss of intra-oral pressure may be that a childrsquos early consonantrepertoire could be restricted to nasals and approximants [m n Icirc w j] with [h]sometimes representing voiceless plosive and fricative targets Russell (1991) andHarding (1993) observed nasal fricative consonants in developing speech patternswhich in some but not all cases resolved Russell and Grunwell (1993) consideredthe eVect of abnormal learned neuromotor patterns which can dominate phonolo-gical development A restricted phonetic repertoire in babble can persist into earlyspeech irrespective of increasing potential for velopharyngeal function In the workof Russell (Russell 1991 Grunwell and Russell 1993) established articulatory pat-terns were more readily modi ed by some children than others Harding (1993)found that some speakers made placement distinctions in their nasal fricativerealizations but others used one nasal fricative [Icircdeg
k] for all fricative target consonantsApplication of the phonetic repertoire into speech is usually systematic and as aresult most families are able to understand their childrsquos distinctively cleft-typespeech Strategies employed in early speech inevitably aVect phonological processesErrors are process-speci c not phoneme speci c A phonological perspective ininterpretation of speech assessments is therefore both necessary and enlightening
This paper proposes a phonologically based categorization system for cleftpalate speech patterns observed in a longitudinal study of pre-speech and speechdevelopment in diVerent groups of children whose ages ranged from 16 to 130The proposed system predicts an association between certain speech characteristicsand the structure and function of the speech mechanism Since subjects had beentreated with either 1-stage surgery or 2-stage repair in which the hard palate remainedunrepaired until between 4 and 8 years the speech data could be considered inrelation to a range of oral structures Two subjects were recorded before palatesurgery at age 16 other samples were taken when palates were partially repairedor when fully repaired with or without stulae and with or without suspectedvelopharyngeal incompetence During the course of the longitudinal studies sevensubjects underwent surgery and the eVects of surgery on speech were monitored
Pre-speech and speech samples were taken at 6-monthly intervals at diVerentstages of surgical repair and at diVerent stages of speech development Detailedanalysis of 141 speech samples led to the identi cation of the activepassiveframework which is described here
Four concurrent studies three of which were longitudinal included subjects bornwith complete clefts of lip and palate aged between 16 and 130 Study 1 followedpre-speech vocalizations into speech from ages 16 to 46 and Study 2 recorded patternsof change in speech production from ages 46 to 76 Studies 3 and 4 comprised 2groups of older subjects Study 3 ages 90ndash110 and Study 4 130 were primarilyincluded to facilitate comparison between speech and facial growth
Method
Speech samples were elicited from younger subjects by use of the prototype of thePACSTOYS Screening Assessment (Grunwell and Harding 1995) whereas older
A Harding and P Grunwell332
subjects were asked to describe PACS pictures (Grunwell 1987) Speech was tran-scribed both live and from audio recordings Live transcription was thought to bean essential supplement to audio recordings since some visually perceived character-istics could not be detected on the audio-recordings eg labiodental nasal [Iacute] mightbe perceived as a bilabial nasal on audio recording Slight audible nasal emission asin [pk] might be suspected on audio but it would be con rmed by live transcription
The following speech parameters were studied nasal resonance nasal emissionnasal turbulence voice lip posture intelligibility and consonant production Speechsamples were taken in the home and hence routine endoscopy and uoroscopywere impracticable It is furthermore questionable whether such investigationswould be thought ethical unless they were necessary for clinical management Theprimary area of interest in this investigation has therefore been detailed examinationof the nature of consonant production in relation to oral structure Harding andGrunwell (1996) have identi ed articulatory errors of place as glottal pharyngealuvular velar lateral palatal double articulations For the seven individuals whounderwent surgery the pre-operative data were compared with the processesobserved post-operatively to ascertain whether any trends in post-operative conson-ant production could be identi ed Phoneme realizations were transcribed andcharted on to phoneme evolution charts (Harding 1993) and phonetic diagrams(Harding and Grunwell 1993) were completed for each speech sample
Analytical approach
Initially cleft-type consonant production errors were distinguished from thosedevelopmental errors thought to be unrelated to the cleft Errors related to the cleftpalate were categorized as Cleft-Type Realizations (CTRs) (Harding and Grunwell1993)
Since most articulatory errors aVected groups of consonants speech errors werefurther categorized within a phonologically based framework of cleft-type processesThe speci c processes were de ned within the 1987 concept of Hutters andBrondstedrsquos active versus passive strategies
Activepassive analytical framework
Active processes are de ned here as alternative articulations thought to have beenactively generated in order to establish the necessary phoneme distinctions betweenindividual consonant targets Where one strategy systematically aVected more thanone consonant target and these targets were phonologically related then that strategywas identi ed as a process a cleft-type phonological process For example backingusually aVected several alveolar targets t d n s z resulting in a backing pro-cess In this de nition alternative articulations include both non-English consonantrealizations eg s to [x] and alternative English consonants as in t backed to [k]
Figure 1 illustrates the nature of realizations involved in active processes As agroup they resemble but are not the same as Trostrsquos (1981) compensatory articula-tions In early speech attempts at several fricative target consonants might all berealized by a single realization for example s z S Z might be any of the followingnasal fricative [n
degk] post-oral glottal [h] or pharyngeal [Eacute] backed to uvular [X] or
to velar [x] lateral [Euml] palatal [c] A backing process aVecting production of [s]might also result in backing of both alveolar target plosive consonants eg t to
Active versus passive cleft-type speech characteristics 333
Figure 1 Active cleft-type processes
[k] and of nasal andor lateral alveolar target consonants n l to [Icirc] Whilst thesecharacteristics might as has been assumed in the past be pure articulatory errorsthere are phonological consequences (Grundy and Harding 1995) when severalclasses of consonants eg voiced and voiceless alveolar fricatives and alveolarplosives are realized by one consonant [g] resulting in multiple loss of phonologicalcontrasts or systematic sound preference (Grunwell 1985)
In viewing gure 1 it is worth noting that pharyngeal and glottal articulationare lsquonon-oralrsquo productions which do not require intra-oral pressure or velopharyngealclosure and their production would not evoke sphincteric movement A speakermust at least intend an oral production if potential velopharyngeal sphincter functionis to be accurately assessed Hence predominance of glottal and pharyngeal patternsof articulation imply but do not prove the existence of an inadequate sphincter
lsquoActiversquo processes which establish meaningful contrasts did not account for allthe cleft-type speech patterns observed in the data Consideration is now given tothe cleft-type realizations thought to be passive products of either structural defector dysfunction Hypernasal resonance co-occurring with passive patterns of articula-tion are frequently a direct consequence of weak or absent intra-oral pressure In apassive realization there is no alteration of the articulatory pattern for the intendedconsonant eg the bilabial b in ball is produced [m] [mO~] As shown by gure 2exclusively passive patterns of articulation employ few consonants (approximantsand nasals and glottal [h]) [m n Icirc w j l h] to represent all adult consonants Thisrange of consonants when associated with nasalized vowels suggests a lack ofpotential to establish intra-oral pressure for speech To date passive consequencesof the cleft on speech have received minimal attention perhaps because they donot involve non-English consonant realizations Lack of intra-oral pressure isassociated with hypernasal resonance and nasal emission (Kummer et al 1992)Nasal emission is perceived either accompanying or replacing voiceless pressureconsonant targets hence it will not be present until a child is actively targetingvoiceless pressure consonants (Sell et al 1994) Severely hypernasal speech may notevidence nasal emission until fricative targets are intended and realized as [(sk)n
deg]
for examplePassive processes which severely limit the range of consonants can impair
communication more than a combination of active processes Speech samples
A Harding and P Grunwell334
Figure 2 Passive cleft-type processes
containing active processes usually sound distinctive but communicative compet-ence can be impressive because more meaningful diVerences can be signalled thanmay be possible with the restricted phonetic repertoire of passive processes Giventhat the velopharyngeal sphincter is complex and dynamic it is possible for arestricted phonetic repertoire with hypernasal resonance to persist into early speechdevelopment because a child has been unable to achieve velopharyngeal functionfor speech after palate repair
The distinction between active and passive cleft-type processes has been integ-rated into the revised cleft palate speech assessment GOSSPASSrsquo98 (Sell et al1998) De nitions of cleft-type characteristics are given in GOSSPASSrsquo98 butGOSSPASS does not interpret the phonological consequences of the cleft-typecharacteristics The following de nitions of active and passive cleft-type processesare based on data analysis in the present study and on Harding and Grunwellrsquos(1996) characteristics of cleft palate speech Analysis of patterns of phonemeevolution throughout speech acquisition has generated a hierarchy of error-severityThe following descriptions of the diVerent types of processes are illustrated byreference to the data collected in the research studies (Harding 1993)
Active cleft type processes
Active nasal fricatives
[mdegk] [n
degk] [ Daggerk
deg] Nasal realizations of voiceless and sometimes voiced fricative targets
f v s z S Z were categorized as nasal fricatives Comparison of gures 1 and 2shows that nasal realizations occurred in both passive and active processes Inproduction of active nasal fricatives the pulmonary air is actively directed nasallyas an alternative articulation to an oral fricative realization Figure 3 illustrates thatoral air ow is stopped by either lips or tongue thus achieving 100 nasal air owThis strategy is developed in order to signal the fricative nature of intended targetfricative consonants In the active nasal fricative [m
degk] for f n
degk for s [n
degk O] for
lsquosorersquo [mdegk O] for lsquofourrsquo is the product of actively directed nasal air Where fricative
consonants are the only targets aVected by a cleft-type process the presence ofnasal fricatives have been referred to as phoneme speci c nasality (Trost-Cardamone
Active versus passive cleft-type speech characteristics 335
Figure 3 Active nasal fricative [ndegk]
1990) This characteristic has been found in speakers with no cleft palate historyoften with no explanation for its occurence
DiVerent places of articulation signalled placement contrasts between nasalfricative consonants in the same way that target nasal consonants [m n Icirc] arediVerentiated by place of articulation [m
degk] for f [n
degk] for s S Where a strong
backing process existed alveolar and post-alveolar fricatives were realized by velarnasal fricatives [ Daggerk
deg]
Occasionally nasal air ow was constricted such that nasal fricatives were pro-duced with a noisier turbulent quality [m
deg] [n
deg] [ Dagger] In a detailed assessment of cleft
pa la te speech GOSSPASSrsquo98 (Sell et al 1994 1998) these turbulent realizationswould be categorized in the resonance section as lsquonasal turbulence replacing conson-antsrsquo and in the cleft-type characteristics section as either lsquoactive nasal fricativesrsquo orpassive nasal realization of fricatives
Glottal articulation
[] frequently occurred in early plosive and aVricate production [p b t d T] up toage 46 Sometimes this process aVected only alveolar plosives t d in SIWI andSIWW position At times glottal stop represented voiced plosives [b d g] while[h] represented voiceless plosives [p t k] In SFWF position glottal stop representedboth voiced and voiceless plosives It may be the case that diVerent strengths ofglottal stop were used to distinguish voiceless and voiced plosives but this couldnot be reliably judged without spectographic analysis An undergraduate study ofspectographic analysis (Shorter 1995) of cleft palate speech identi ed some subtlediVerences in glottal stop productions which suggests a need for further investigationinto the phonological functions of glottal stops in cleft palate speech
Pharyngeal fricatives
[Eacute iquest] Early attempts at fricatives (ages 20ndash30) were frequently realized with acombination of posterior fricative cleft-type realizations (CTRs) Where plosiveswere exclusively glottal fricative consonants were frequently realized as pharyngeal
A Harding and P Grunwell336
fricatives In early phonological development obstruent realizations were commonlynon-oral but gradually moved anteriorly to uvular and velar positions Targetconsonants were not generally corrected independently of each other The gradualmovement of pharyngeal realizations towards oral uvularvelar articulation whichunderlines the relevance of a phonological interpretation of cleft palate speechcharacteristics
Exclusively pharyngealglottal patterns of articulation might imply velopharyn-geal insuYciency but it is noted here that all infants use pharyngeal and glottalarticulation until they acquire velopharyngeal competence during the rst 6 monthsof life It is possible for children with cleft palate to persist with this phoneticrepertoire for some time after palate repair Indeed such cases have been reportedby Russell and Grunwell (1993) Non-oral articulatory patterns indicate that thesphincter is not employed during speech which implies that the sphincter may notbe functional but unless oral air ow is consciously intended it cannot be assumedthat the sphincter is unable to function in speech (Henningsson and Isberg 1986)
Backing [k g q G]
A backing pattern is described by Stengelhofen (1989) as a lsquotendency for oralcontacts to be to the back of the oral cavityrsquo GOSSPASSrsquo98 (Sell et al 1998) makesa distinction here between backing to uvular and backing to velar place ofarticulation
E Backing to uvular [q G X Ograve ] Alveolar target consonants were backed touvular realizations and occasionally velar targets were backed to uvular Thepresence of velar and uvular realizations indicated the presence of some VPfunction but this might have been achieved with tongue humping In thedata acquisition of uvular and velar fricatives generally co-occurred withacquisition of f v which provides further evidence of velopharyngealfunction In the longitudinal study from age 16 to 46 subjects with bilateralclefts spent a period of months realizing all alveolar and post- alveolar voicedand voiceless consonant targets in uvular placement This degree of backingis deemed to be more severe and distracting for listeners than backing tovelar perhaps because uvular articulation is more distinctively non-EnglishHowever uvular fricatives are frequently used to achieve some meaningfulcontrasts which improve intelligibility
E Backing to velar In the younger subjects (aged 16ndash46) as articulatorypatterns progressed anteriorly a preference for [g] was common Mostcommonly backing resulted in t d realized as [k g] and s z as [x aring ]which contrasts with the fronting pattern seen in normal development
Double articulation
This is de ned as two simultaneous equal strictures at two places of articulationwhich was frequently noted in realizations of target alveolar consonants t d whenalveolarvelar contacts [tkk dkg] were used Double articulation may have beendeveloped to distinguish between alveolar and velar consonants in the presence ofa backing pattern Interestingly double articulation became evident in these develop-ing speech patterns with the emergence of fricative realizations Both plosives andfricatives tended to be realized with double articulation eg tndash[tkk] sndash[skagrave ]
Active versus passive cleft-type speech characteristics 337
Palatal fricatives [c J ]
These fricative realizations of alveolar target consonants appeared towards the endof the study period (ages 16ndash46) They were the most common realizations ofalveolar fricatives in older children (46ndash76 and 100ndash110) This nding was inaccordance with Alberyrsquos results (Albery 1991 Albery and Grunwell 1993)
Lateral fricatives [l Igrave]
As with palatal fricatives lateral fricatives were frequently present as realizations offricative consonant targets becoming particularly prevalent in later phonologicaldevelopment
Gliding of fricatives s S= [ j] or [w]
This phenomenon is seen in the non-cleft population as an uncommon develop-mental process (Grunwell 1987) It is classi ed here as an active process because[ j] was consistently produced as an apparently active alternative to target conson-ant(s) s z S [ j] is a normal consonant-like production in non-cleft babble whichcleft palate children often integrate into their phonological system It may betherefore that it is a persisting immaturity in the cleft palate population In thesedata [ j] was eVective in signalling a contrast between plosives and fricatives inSIWI position It functioned for the following consonants in diVerent speakers [ j]for S [ j] for m p f s z Ÿ h and co-articulation [hkj] for T
Passive cleft type processes
The criteria for passive cleft type processes is that they are (1) an attempt toproduce the correct articulatory placement and stricture (manner) which (2) failsbecause of a lack of intra-oral air pressure For example voiced plosives realized asnasals b[ [m] d[ [n] g[ [Icirc] No compensatory articulatory pattern hasbeen used to replace the intended consonant As the above examples demonstratetarget realizations often match a similar English consonant
Absence of pressure consonantspredominantly sonorant articulation
This phenomenon is de ned here as a pattern of articulation which was restrictedto English nasal and approximant articulations [m n Icirc w j] and [h] Some of thevoiced consonants were also employed as voiceless counterparts [m
degndeg Icircdeg ] thereby
increasing the range of available consonants for distribution in the phonologicalsystem Despite the limited consonant repertoire these patterns were often eVec-tively interpreted by close family members
Weak articulation [bV dV]
This category refers to normal articulatory movement in the production of obstruenttargets (plosive fricative and aVricate targets) which were produced with reducedoral air pressure and therefore articulation was considerably weakened In the speechsample data (ages 16ndash46) many target consonants were weakened to some degreeand at times may have been realised as nasals
A Harding and P Grunwell338
Passive nasal fricative [(fk)m (sk)ndeg]
Incomplete velopharyngeal closure inevitably reduces control of oral air ow with apassive loss of air ow and an increase of resonance in the nasal cavity Grunwelland Harding (1996) de ned the passively nasal fricative as an unreleased [(s)]double-articulated with a lowered voiceless nasal [n
Aacute
deg] This realization is the product
of an intended s with an unintended nasal air ow (see gure 4) The precisetranscription for a passive nasal transcription is [(sk)n
Aacute
deg] but an acceptable simpli cation
for transcription purposes is [(sk)ndeg] This is distinct from the active nasal fricative
which involves stopping of the oral air ow and active direction of air nasally whichcan be transcribed as a voiceless nasal with additional nasal emission [n
degk] Nasal
emission signals the fricative nature of for example target consonant s Thesetwo productions can sound the same and might initially be transcribed as [n
degk]
Nasendoscopic investigation of velopharyngeal activity during active and passivenasal realizations of s both show a lack of velopharyngeal closure It is predictedthat close examination by use of electropalatography might show slight diVerencesin tongue tip posture for an active and passive nasal fricative as illustrated in gures3 and 4 Passive nasal fricatives were converted into oral fricatives with nose-holding
Voiceless [h] for voiceless plosives
There was evidence that voiceless plosives were at times passively realized as [h]The consequence of reduced oral air pressure on production of voiceless plosivescan leave aspiration as the only perceptible distinctive feature This process usuallyaVected all voiceless plosive targets p t k Where this process was a passiveprocess use of noseholding during speech facilitated accurate target productionHowever it would also be possible for this distribution of [h] to be an active cleft-type process which would be part of a pharyngealglottal patternprocess
Nasal realization of voiced plosives b d g[ [m n Icirc]
Some subjects with residual clefts stulae or suspected VPI realized voiced conson-ants as nasal counterparts As summarized by Harding and Grunwell (1996) voiced
Figure 4 Passive nasal fricative [(sk)nAacute
deg]
Active versus passive cleft-type speech characteristics 339
consonants can be more diYcult to produce than voiceless consonants (Isshiki andRingel 1964) Distinction between active versus passive nasal realizations of plosivetargets was made in the same way that active and passive nasal fricatives weredistinguished by observing the eVect of noseholding on consonant production Inpassive nasal realizations noseholding facilitated normal consonant production(Golding-Kushner 1995)
Nasal emission accompanying consonants [pk sk]
Nasal emission was frequently heard accompanying consonants but on occasions itapparently replaced consonants It has been linked with velopharyngeal incompet-ence (VPI) (Kummer et al 1992)
Results
Comparison of activepassive processes in the speech data
Quantitative results of Hardingrsquos research into the relationship between timing ofsurgery and speech development have already been published (Harding andGrunwell 1993) The following interpretation of the data speci cally identi esactivepassive cleft-type processes in relation to oral structure in a wide age rangeof subjects (16ndash130) Tables 1 2 3 and 4 show the passive and active processeson the left-hand column and the subjectrsquos code along the top The code identi esthose subjects who were treated with 1-stage versus 2-stage surgery Comparisonof the 4 tables at age 46 (BCLP and UCLP) at age 90 and at age 130 illustratesa pattern of diminishing cleft-type processes with increasing age Irrespective ofsurgical timing few cleft-type processes remained at age 130 (table 4) A generalobservation was that earlier speech samples (ages 16ndash76) frequently combined
Table 1 Cleft-type processes in BCLP subjects at age 46 (studies 1 and 2)
1-stage surgery 2-stage surgery
A G Rf JW D B JF JG AB
Passive cleft-type processespredominantly sonorant articulation m
weak articulation m m m m m m m m
voiceless h for plosive m m m m m
nasal release of plosives m m m m m
nasal emission with consonants m m m m m m
passive nasal fricativeActive cleft-type processes
nasal fricatives m m m m m m m m
pharyngeal glottal articulation m m m m m m m m
backing to uvular m m m m m m m m
backing to velar m m m m m m m m m
lateral palatal fricatives m m m m m m m m m
double articulation m m m m m m m m m
gliding fricative m m
f=post-operative stula
A Harding and P Grunwell340
Table 2 Cleft-type processes in UCLP subjects at age 46 (study 2)
1-stage surgery 2-stage surgery
SE TB CK MS NC TS ZG CP
Passive cleft-type processespredominantly sonorant artic m
weak articulation m m m
voiceless h for plosives m m m
nasal release of plosives m m m
nasal emission with consonants m m
passive nasal fricative m m
Active cleft-type processesnasal fricativepharyngeal glottal articulation m m m
backing to uvular m
backing to velar m m
lateral palatal fricatives m m m m m
double articulation m m m m m m
gliding fricative m
Table 3 Cleft-type processes at age 90
2-stage surgery 2-stage surgery1-stage surgery completed at 4 yrs completed at 8 yrs
DAf SBf RL NR JD AR LJ RP MB
Passive cleft-type processespredominantly sonorant articweak articulation m
voiceless h for plosives m m
nasal release of plosives m m
nasal emission with consonants m m m m
passive nasal fricatives m m
Active cleft-type processesnasal fricatives m m
pharyngeal glottal articulation m m
backing to uvular m m
backing to velar m m m m m m m
lateral palatal fricatives m m m m m m m
double articulation m m m m m
gliding fricative m
f=subject had a stula
both active and passive strategies whereas later samples (ages 90ndash130) rarelyevidenced passive processes
At age 46 four out of ve BCLP subjects used active non-oral pharyngeal andglottal processes and oral velar and uvular fricatives irrespective of surgical status(see table 1) All had some anterior palatal defect which might have reduced theirpotential to achieve intra-oral pressure
By comparison two out of three partially repaired 2-stage UCLP subjects at age46 (table 2) showed evidence of passive processes This suggested that their
Active versus passive cleft-type speech characteristics 341
Tab
le4
Spee
chin
rela
tion
tosu
rgic
altim
ing
atag
e13
0
2-st
age
surg
ery
2-st
age
surg
ery
1-st
age
surg
ery
subj
ects
com
plet
edat
4yr
sco
mpl
eted
at8
yrs
1-A
1-B
1-C
1-D
1-E
1-F
24-
G2
4-H
24-
J2
8-K
28-
L2
8-M
Pass
ive
clef
t-ty
pepr
oces
ses
pred
omin
antly
sono
rant
artic
wea
kar
ticul
atio
nm
voic
eles
sh
fo
rpl
osiv
esna
sal
rele
ase
ofpl
osiv
esna
sal
emis
sion
with
cons
onan
tsm
pass
ive
nasa
lfr
icat
ives
Act
ive
clef
t-ty
pepr
oces
ses
nasa
lfr
icat
ives
phar
ynge
alg
lott
alar
ticul
atio
nba
ckin
gto
uvul
arba
ckin
gto
vela
rm
m
late
ral
pala
tal
fric
ativ
esm
mm
doub
lear
ticul
atio
ngl
idin
gfr
icat
ive
1=1-
stag
esu
rger
ysu
bjec
ts
24=
2-st
age
surg
ery
hard
pala
tere
pair
edat
abou
t4
yrs
28=
2-st
age
surg
ery
with
hard
pala
tere
pair
edat
abou
t8
yrs
A Harding and P Grunwell342
unrepaired hard palates had in fact restricted their phonetic repertoire imposing aneed for individual adaptability The additional active processes employed by thesesubjects were presumably a response to the restrictions imposed by their oro-nasalstructure and velopharyngeal function at the time of consonant acquisition Asshown in table 2 the most common active cleft-type processes persisting at age46 with a residual cleft of the hard palate were backing double articulation andlateralpalatal articulation Two 1-stage surgery subjects whose entire palates hadbeen repaired at ages 09 and 010 did not use any cleft-type processes at age 46
By age 90 (table 3) a much-diminished number of cleft type processes wasevident except in subjects with sizeable anterior stulae who had received littlespeech and language therapy A similarity was noted between the speech patternsof 1-stage surgery subjects with stulae (DA and SB) at age 90 (table 3) and theyounger BCLP subjects at age 46 (table 1) who also had anterior palatal defectsThey included non-oral realizations of t d s k g occasional nasal fricatives andpharyngealglottal articulations Fistulae had apparently continued to in uencearticulation and phonological development in these subjects
Finally at age 130 (table 4) the diVerences between 1-stage and 2-stage surgerysubjects had diminished leaving only one 2-stage subject with occasional backingand four subjects with slight palatal and lateral release of fricative consonants Onlytwo of the 1-stage surgery subjects were using minor distortions of grooved fricativeproduction
Whilst there were apparent trends in speech production relating to surgicaltiming and oral structure it is noted that there were exceptions to each tentativegeneralization Subjects with marked structural imperfections occasionally producedrealizations of which they would not have been thought capable and subjects withno visible imperfections produced inexplicably distorted speech patterns It istherefore concluded that whilst there is homogeneity in the range of processesproduced by this population assumptions cannot be made about speech based onsurgical timing or type of cleft Tentative predictions based on detailed assessmentmay be clinically very useful
EVects of surgery on speech
Activepassive processes have identi ed those cleft-type characteristics thought tobe associated with a physical inability to produce pressure consonants The followinganalysis of speech changes after surgical intervention at diVerent ages identi es thechanges eVected by surgery when intra-oral pressure could be more readily achieved
Two children were rst recorded prior to the rst stage of a 2-stage procedureTheir lips were repaired at approximately 6 months of age and soft palate repairwas carried out at ages 18 and 19 respectively Their hard palates were leftunrepaired to facilitate unrestricted growth of the mid-face (Hotz et al 1978) Pre-and post-operative consonant-like sounds present in the recorded speech samplesare listed in table 5 Interestingly prior to soft palate repair both these childrenproduced some oral consonants Subject B was producing pressure consonants [kg] in his babble prior to soft palate repair Considering that he had an unrepairedbilateral cleft palate at this point it was surprising that he had any oral consonantsPost-operatively at 20 years he used [b bkm t d g gkb] which indicated that surgeryto repair the soft palate had facilitated an increased range of oral pressure consonantsSubject D was producing [p b k g] pre-operatively Post-operatively following soft
Active versus passive cleft-type speech characteristics 343
Tab
le5
EV
ects
ofso
ftp
alat
ere
pair
atag
e1
6on
BC
LP
subj
ects
h
ard
pal
ate
rem
ain
sun
repa
ired
2-st
age
subj
ects
Surg
ery
Pre
-ope
rati
vesp
eech
patt
ern
atag
e1
6Po
st-o
pera
tive
chan
ges
insp
eech
atag
e2
0
Stud
y1
BSo
ftpa
late
repa
irat
16
Adu
ltta
rget
sk
gA
t2
0[b
b kmg kb
td
g]D
Soft
pala
tere
pair
17
Adu
ltta
rget
sp
bk
gA
t2
0[p
bd
b kdk
g]
Tab
le6
EV
ects
ofha
rdpa
late
rep
air
atag
e6
6an
d
stu
lare
pair
atag
e10
0
Subj
ect
Surg
ery
Pre
-ope
rati
vesp
eech
patt
ern
Post
-ope
rati
vech
ange
sin
spee
ch
MS
Har
dpa
late
repa
ir6
6Pa
ssiv
epr
oces
s7
6E
limin
ated
pass
ive
proc
ess
Var
iabl
ena
sal
rele
ase
ofco
nson
ants
Hyp
onas
alna
sals
JFH
ard
pala
tere
pair
(uns
ucce
ssfu
l)6
6Se
vera
lac
tive
and
pass
ive
proc
esse
s7
6A
ctiv
epr
oces
ses
rem
aine
dPa
ssiv
epr
oces
ses
elim
inat
ed
DA
Fis
tula
repa
ir10
0A
ctiv
epr
oces
ses
110
Elim
inat
ion
ofph
aryn
geal
glo
ttal
Var
iabi
lity+
+an
dna
sal
arti
cula
tion
Art
icul
ator
yva
riab
ility
++
Act
ive
CT
Rs
proc
esse
spe
rsis
t
A Harding and P Grunwell344
palate repair but with a residual cleft in the hard palate his range of consonantsincluded [d] which was particularly surprising since the hard palate remainedunrepaired Whilst it is unlikely that toddlers of 18 months could be consciouslytrying to compensate for articulatory inadequacy in producing velar plosives inbabble prior to soft palate repair and an alveolar plosive prior to hard palate repairboth these subjects showed evidence of actively pursuing their articulatory potential
Table 6 summarizes changes following surgery to repair the hard palate in moremature speech patterns These subjects who were aged 66 and 100 pre-operativelyhad learned to speak with residual clefts and were apparently unaware of theconsonant productions that failed to match normal production
Subject MS used only passive processes in his speech pattern He realized someconsonants nasally such that lsquoballrsquo was [mO~] and lsquosockrsquo was [(sk)n
deg Aacute~ k] Looking atpost-operative changes at age 76 his consonant production was normal but hisresonance had become hyponasal Pre-operatively at age 66 Subject JF was usingseveral active and passive processes The active processes were unaVected by surgerybut passive processes were eliminated
Fistula repair was carried out at age 100 on Subject DA who had many activeprocesses and very variable articulation pre-operatively Post-operatively at age110 he was not using non-oral pharyngeal and glottal active processes or nasalrealizations but many oral cleft-type realizations remained
As shown in table 7 hard palate re-repair and pharyngoplasty was carried outon two subjects whose hard palate repairs had been unsuccessful at approximately4 years Subject NC assessed pre-operatively at age 56 was using predominantlypassive processes in her speech She was also using [ j] for fricatives s S whichwas thought to be an active process At age 60 following hard palate re-repair andpharyngoplasty all cleft-type processes had been eliminated without post-operativespeech therapy Since [ j] for s apparently resolved spontaneously followingsurgery it can be assumed that this was a passive process in this speech sample
Subject CP who underwent this procedure presented pre-operatively at age 46with both passive and active processes but his nasal resonance was not consistentlyhypernasal In addition to his cleft-related speech disorder this subject had additionaldevelopmental speech diYculties which were identi ed as being unrelated to thecleft Post-operatively at age 56 little had changedmdashnotably the passive processnasal [m] for b was retained His nasal resonance had become hyponasal andthere was no apparent bene t from surgical intervention The realization of b as[m] had become phonologically stable and surgery alone had not destabilized thephonological system This realization may have been a passive product of VPI inearly speech acquisition which had subsequently become part of a phonologicaldisorder Post-operatively CPrsquos phonetic repertoire did increase but the phonologicaldistribution was variable Plosive targets were still realized as nasals in spontaneousspeech at the nal speech recording at age 76 This was not as an inevitableconsequence of VPI but a result of an inability to destabilize the phonologicalprocess determining that voiced plosives would be realized as nasals This resultfollowing surgery highlights the importance of identifying phonological learningproblems and distinguishing them from structural constraints on articulationIn CPrsquos case pre-operative exploration of the eVect of nares occlusion duringspeech might have indicated that structural change would not improve consonantproduction spontaneously
A general observation was that consonant realizations did not move rapidly
Active versus passive cleft-type speech characteristics 345
Tab
le7
EV
ects
ofha
rdpa
late
re-r
epai
ran
dp
hary
ngo
pla
sty
Subj
ect
Surg
ery
Pre
-ope
rati
vesp
eech
patt
ern
Post
-ope
rativ
ech
ange
sin
spee
ch
Stud
y2
NC
Har
dpa
late
re-r
epai
ran
d5
6Pa
ssiv
ecl
eft-
type
proc
esse
s6
0A
llcl
eft-
type
phar
yngo
plas
ty5
10[
j]
for
fric
ativ
espr
oces
ses
elim
inat
ed[
h]
for
plos
ives
SIW
IV
aria
ble
arti
cula
rypr
ecis
ion
CP
Har
dpa
late
repa
iran
d4
6Pa
ssiv
ean
dac
tive
proc
esse
s5
6Pa
ssiv
epr
oces
sph
aryn
gopl
asty
50
Pho
nolo
gica
lco
nfus
ion
[m]
for
[b
]re
tain
edH
ypon
asal
nasa
lsPe
rsis
ting
phon
olog
ical
conf
usio
ns
A Harding and P Grunwell346
from incorrect to correct but progressed incrementally towards normal realizationsas described by Morley (1970) Where an early realization of target s might beglottal [h] a gradual pattern of change showed subsequent realizations to bepharyngeal [Eacute] then uvular [X] then velar [x] and eventually palatal [c] or lateral [Euml]It was interesting to note that speech patterns continued to change as late as90ndash110 years with the result that diVerences related to surgical timing and cleft-type gradually disappeared Persisting stulae were thought to account for the mostmarked cleft type processes at age 90
Implications for surgical management
This analysis of speech changes following surgery suggests some implications forsurgical management which are compatible with Sell and Grunwellrsquos (1990) ndingsin the Sri Lankan study
Surgery can change passive speech processes but it is also possible that speechtherapy may be able to change passive patterns Surgery alone is unlikely to modifyactive cleft-type processes whereas speech therapy should be able to modify activeprocesses Indications from these case studies is that where speech is the primaryproblem speech assessment should distinguish between active and passive processesin order to evaluate the necessity for full investigations and to plan therapeuticintervention Where past speech therapy has not been successful it cannot beassumed that surgical intervention will facilitate further speech progress A furthercourse of speech therapy which is sensitive to active versus passive processes todevelopmental phonological in uences on cleft-type speech development and toarticulatory diYculties in diVerent speech contexts might facilitate optimal progressWhere structural imperfection exists it is quite possible for single-word productionto be more precise than target realizations in spontaneous speech This may not bea failure of phonological generalization (Grunwell 1992) but the result of diYcultysustaining the necessary lsquoarticulatory eVort rsquo (Harding and Grunwell 1993) resultingin articulatory imprecision Deteriorating articulatory accuracy should not be over-looked in interpretation of speech results
An analytical protocol
As a result of analysing the speech data and identifying the active and passiveprocesses a protocol has been developed which records examples of each cleft-typeprocess over a series of assessments It demonstrates the progression of individualprocesses towards an adult target (see the Appendix) At each assessment onecolumn is used to indicate nasal resonance nasal emission and nasal turbulenceratings and cleft-type processes Changes in the nature of error realizations mightshow progress towards target consonants Hence whilst the total correct scoremight not have increased increments of change can be observed This observationof patterns of change may function as an adjunct to GOSSPASSrsquo98 (Sell et al 1998)giving access to a greater depth of both quantitative and qualitative data aboutconsonant production in relation to resonance nasal emission nasal turbulenceoral structure and cleft-type
Active versus passive cleft-type speech characteristics 347
Diagnostic implications
Passive versus active nasal fricatives
The important management consideration related to this distinction is that an activenasal fricative is an established phonological process which is unlikely to be directlyaVected by surgery alone Therapy would be necessary to destabilize nasal realizationsof oral consonants In contrast passive nasal fricatives may be eliminated by surgeryOf particular relevance is diVerential diagnosis between passive and active nasalfricatives in surgical and therapeutic management When hypernasality co-occurswith nasal air ow during consonant production which can be redirected by nose-holding passive nasal fricatives are diagnosed These would be transcribed as [(sk)n
deg]
passive alveolar nasal fricatives [(Wk)mdeg
] bilabial nasal fricatives or [(fk)Iacutedeg ] labiodentalnasal fricatives Full VPI investigations would be recommended to diagnose thenature of the structural or functional de ciency and distinguish between velopharyn-geal incompetence and velopharyngeal mislearning
It is highly likely that plosive targets would be aVected by reduced intra-oral airpressure such that plosives would either be realized by nasal counterparts eg bd[ [m n] or [b d] may be nasalized and weak Voiceless plosives may be eitheraccompanied by nasal emission [p t k] or realized as glottal fricative [h]
Production of the target sentence lsquoI saw Sam sitting on a busrsquo might be
[aI (sk)ndeg O~ (sk)n
degaelig~m (sk)n
deg IhIn Aacute~n mouml~(sk)ndeg] passive processes and
[aI xO xaeligm xIkIIcirc AacuteIcirc goumlx] active processes
Contribution to surgical management decisions
Passiveactive interpretation of clinical assessments might facilitate surgical manage-ment decisions If noseholding does not facilitate correct production of targetconsonants then it is likely that an alternative articulatory pattern has becomephonologically established ie particular realizations for one or more targets areconsistently distributed in the phonological system These realizations may haveevolved because of initial diYculty producing articulatory targets and subsequentlystabilized within the phonological system Grundy and Harding (1995) refer to thisphenomenon as an lsquoarticulatory disorder with phonological consequencesrsquo
Therapy
Where obvious structural defects or diagnosed dysfunction exists clinicians fre-quently defer therapeutic intervention until surgery has been undertaken Theexpectation would be that normal structure and function is essential for normalspeech However pre-operative therapy may facilitate oral consonant productionwhich may serve to reduce hypernasal resonance Hence therapy prior to surgerymay avoid unnecessary surgery or reduce the extent of surgery required All activeprocesses are likely to require therapy
Principled selection of targets for therapy
Speech patterns frequently evidence a mixture of apparently passive and activeprocesses which complicates decisions about target selection Target selection can
A Harding and P Grunwell348
be based on assessment of which consonant targets can be most easily elicted inisolation (stimulability) This may lead to a sequence of target selection which isopposite to the sequence of consonant acquisition in normal development Forexample where reduced intra-oral pressure is present in a passive pattern [T] maybe easier to elicit in imitation than more nely grooved [s] or [S] Therapy maytarget [T] followed by [S ] and nally [s] As in non-cleft phonological therapywhere a class of consonants is aVected by the cleft then it is helpful to target theentire class The following decision-making process can be applied for both activeand passive processes
Decision making procedure for target selection
(1) Voiced versus voiceless targets(2) Front versus back placements(3) Syllable initial versus syllable nal targets(4) Plosives versus fricative targets
Voiceless plosives and fricatives are produced with an open glottis whichfacilitates topping up of air ow from the lungs hence voiceless plosive and fricativetargets are frequently more successful than voiced counterparts (Isshiki and Ringel1964) Front targets usually cause more diYculty than back particularly where analveolar defect or stula exists Contrary to normal development back targets maybe targeted before front Word- nal targets generally require less oral air pressurethan word initial targets and similarly fricatives may be more easily elicited thanplosives Fricatives do require a greater volume of air than plosives (Fletcher 1985)but in the presence of nasal escape weak fricative production appears to be morereadily achieved than weak plosive production Since nal fricatives would normallybe acquired in advance of word-initial fricatives (Ferguson 1978) targeting word- nal fricatives is frequently a productive starting point for therapy
Principles of therapy for passive processes
(1) Use of soft attack similar to gentle whisper for all target models ensuresminimal articulatory eVort (Harding and Grunwell 1993) and requires min-imal intra-oral air pressure It may be appropriate to gradually increase thearticulatory attack when the articulatory posture and evidence of intendedoral air ow have been established
(2) Slightly stretched duration of segment transitions in models of consonantto vowel (CndashV) or vowel to consonant (VndashC) facilitates review of motorplanning and extends the available time for execution of the new motorprogrammer whilst maintaining control of the oral airstream
(3) Noseholding can be used to provide exclusively oral air ow Gradual releaseof the nostrils during production of sustained [VVVVVf ] or [hhhhh ] allowsthe child to attempt to sustain an oral consonant despite increasing nasalemission This maximizes the use of available oral air ow Procedures forusing noseholding are described in some detail by Golding-Kushner (1995)
Principles of therapy for active processes
This is more like phonological therapy and can follow Grunwellrsquos (1991) processesfor phonological change and principled decision-making (Grunwell 1992) Some
Active versus passive cleft-type speech characteristics 349
examples are given here by way of illustration of ways to eVect the rst twoprocesses of change which may need to be approached diVerently in cleft palateversus non-cleft speech disorders DiVerent approaches may also be appropriate formodifying active versus passive cleft-type processes
Innovation production of new targets Some useful principles
(1) Introduction of new lsquonon-speech likersquo targets in sound play using a conson-ant sound segment model such as [ph ] note not a syllable like [p] whichis the type of pronunciation used when target sounds are presented as lettersfor reading Target [s] might be introduced as a lsquoTrain Slowing Down Noisersquo[ts ts ts tssssssss]
(2) lsquoNew consonantsrsquo can later be modelled and elicited in soft productions ofsyllable structure [tssssndashi] [ indashtssss] which can subsequently be identi ed assimilar to words lsquosearsquo and lsquoeatsrsquo
(3) lsquoDeferring responsibilityrsquo transfers responsibility or lsquoblamersquo for errors fromthe child and attributes it to the articulators eg lsquoyour tongue is havingtrouble with hellip rsquo lsquoLetrsquos show your tongue how to hellip rsquo
(4) New targets can be modelled repeatedly and recorded on audio or videotape which can be listened to at home
(5) Targeting classes of consonants (eg alveolars t d s n l voiceless fricativesf s S perhaps with aVricate T avoids phonological confusion whichmight occur if production ofsis achieved whilst other alveolar targetsremain backed The risk is that s might not integrate into the phonologicalsystem unless all backed alveolar consonants are destabilized
(6) Increased eye contact during auditory and production work can be invaluablein holding visual and auditory attention and ensures that visual informationabout the sound has been processed This is easily achieved by the clinicianlifting any focus of the childrsquos attention close to hisher mouth at theprecise moment when the target is modelled
Stimulation of non-speech related sounds such as a lsquoTrain Slowing DownNoisersquo [ts ts tsss] con rms that target [s] is physically achievable whether or not[ssss] can be imitated Some children continue to access [s] through the lsquoTrainSlowing Down Noisersquo throughout therapy until it is occurring spontaneouslywithout conscious planning This can be an eVective means of underminingestablished motor programmers (Hewlett 1990) for active cleft-type processes
Destabilizing active processes
As it is likely that children will be unaware of each occurrence of their alternativearticulatory pattern for speci c consonant errors it is preferrable to destabilizeactive processes with minimal conscious eVort by the child As children becomeaware of their mismatches they frequently add the newly acquired target realizationto their existing production eg target word tu childrsquos old realization [ku] childrsquoscorrected realization [t-ku] Destabilization can be achieved with minimal consciouseVort through input therapy techniques such as auditory bombardment (Lancasterand Pope 1989) auditory decision-making such as lsquowhich bear says this wordproperlyrsquo Red Bear says lsquotworsquo or Blue Bear says lsquocoorsquo This type of strategy oftenprecipitates attention to the target consonant with possible lsquoreplayrsquo and lsquoreviewrsquo of
A Harding and P Grunwell350
their own production Frequent stimulation of cognitive alertness to the targetconsonant can develop awareness without confronting the child with errors orrisking hisher failure The child is then free to attempt to repair hisher ownrealization to continue to re ect and to silently rehearse the adult realizationTraditional articulation therapy is thus combined with development of metaphonol-ogical skills ie the ability to re ect upon onersquos own speech production The resultshould be that new target realizations will be more phonologically stable thanexclusively production-based articulation therapy might have facilitated
Stabilizationgeneralization
Procedures to ensure stabilization and generalization of new target consonantswould be as described by Grunwell (1992) Success may be constrained by theconsiderable articulatory eVort sometimes required to maintain pressure consonantproduction in spontaneous speech (Harding and Grunwell 1993)
Conclusions
In speech assessment it is helpful to distinguish between errors which are cleft-type and non-cleft type and those which are part of active versus passive processesThe active and passive processes have been de ned and their phonological implica-tions discussed Focus on active and passive processes has facilitated focus on thephonological consequences of cleft palate on speech development In the futureawareness of the likely eVect of a cleft palate on normal phonological developmentcould avoid extended periods of unsuccessful clinical intervention Furthermoresensitivity to the relationship between phonological processes and structural con-straints should facilitate theoretically based management decisions Incidences suchas the case of CP in which nasal realizations were thought to indicate VPI but weresubsequently unaVected by surgery might be avoided if phonological analysiscontributes to management decisions
Surgery did improve hypernasal resonance and eliminated passive processes buthad little eVect on active processes Active processes in younger subjects werethought to require therapeutic intervention but in the longer term the oldersubjects showed few cleft-type processes Whilst it is possible that active cleft-typeprocesses may resolve with increasing age the implication for the future is thatactive cleft-type processes should be treated with skilled therapeutic interventionnot surgery Therapy which addresses the phonological consequences of cleft palateon speech development by combining metaphonologicalphonologicalarticulatoryapproaches is likely to be successful
References
Albery E 1991 Consonant articulation in the diVerent types of cleft lip and palate UnpublishedMPhil thesis Leicester Polytechnic
Albery E and Grunwell P 1993 Consonant articulation in diVerent types of cleft palate InP Grunwell (Ed) Analysing Cleft Palate Speech (London Whurr)
Ferguson C A 1978 Fricatives in child language acquisition In V Honsa and M Hardmann-Battista (Eds) Papers on Linguistics and Child Language (Mouton The Hague)
Fletcher S G 1985 Speech production and oral motor skill in an adult with an unrepaired palatalcleft Journal of Speech and Hearing Disorders 50 254ndash261
Active versus passive cleft-type speech characteristics 351
Golding-Kushner K J 1995 Treatment of articulation and resonancne disorders associated withcleft palate management and VPI In R Shprintzen (Ed) Cleft Palate Speech Management AMultidisciplinary Approach (St Louis Mosby)
Grundy K and Harding A 1995 Developmental speech disorders In K Grundy (Ed) Linguisticsin Clinical Practice (2nd edition) (London Whurr)
Grunwell P 1985 Phonological Assessment of Child Speech (Windsor NFER-Nelson)Grunwell P 1987a Clinical Phonology (2nd edition) (London Croom Helm)Grunwell P 1987b PACS Pictures Language Elicitation Materials (Windsor NFER-Nelson)Grunwell P 1991 Processes of phonological change in developmental speech disorders Clinical
Linguistics and Phonetics 6 101ndash122Grunwell P 1992 Principled decision making in the remediation of children with phonological
disorders In P Fletcher and D Hall (Eds) Specic Speech and Language Disorders in Children(London Whurr)
Grunwell P and Harding A 1995 PACSTOYS A Screening Assessment of Phonological Development(Windsor NFER-Nelson)
Grunwell P and Harding A 1996 A note on describing types of nasality Clinical Linguistics andPhonetics 10 157ndash161
Harding A 1993 An Investigation into the Relationship Between Timing of Cleft Palate Repairand Speech Development Unpublished PhD thesis
Harding A and Grunwell P 1993 The relationship between speech and timing of hard palaterepair In P Grunwell (Ed) Analysisng Cleft Palate Speech (London Whurr)
Harding A and Grunwell P 1996 Characteristics of cleft palate speech European Journal ofDisorders of Communication 31 331ndash358
Henningsson G and Isberg A M 1986 Velopharyngeal movement patterns in patients alternatingbetween oral and glottal articulation A clinical and cineradiographicical study Cleft Palate Journal23 1ndash9
Hewlett N 1990 Processes of development and production In P Grunwell (Ed) DevelopmentalSpeech Disorders (Edinburgh Churchill Livingstone)
Hotz M M Gnoinski W M Nussbaumer H and Kistler E 1978 Early orthopaedics in CLPcases guidelines for surgery Cleft Palate Journal 15 405ndash411
Hutters B and Brondsted K 1987 Strategies in cleft palate with special reference to DanishCleft Palate Journal 24 127ndash136
Isshiki N and Ringel R 1964 Airow during the production of selected consonants Journal ofSpeech and Hearing Research 7 233ndash244
Kummer A W Curtis C Wiggs M Lee L and Strife J L 1992 Comparison of velopharyngealgap size in patients with hypernasality hypernasality with nasal emission and nasal emissionor nasal turbulence (rustle) as the primary speech characteristic Cleft-palate-Craniofacial Journal29 152ndash156
Lancaster G and Pope L 1989 Working with Childrenrsquos Phonology (Oxford Winslow)Morley M E 1970 Cleft Palate and Speech (7th edition) (Edinburgh Churchill Livingstone)Russell V J 1991 Speech Development in Children with Cleft Lip and Palate Unpublished PhD
thesis Leicester PolytechnicRussell V J and Grunwell P 1993 Speech development in children with cleft lip and palate In
P Grunwell (Ed) Analysing Cleft Palate Speech (London Whurr)Sell D A and Grunwell P 1990 Speech results following late palatal surgery in previously
unoperated Sri Lankan adolescents with cleft palate Cleft Palate Journal 27 162ndash168Sell D Harding A and Grunwell P 1994 GOSSPASS A screening assessment of cleft palate
speech European Journal of Disorders of Communication 29 1ndash15Sell D Harding A and Grunwell P 1998 GOSSPASSrsquo98 An assessment for speech disorders
associated with cleft palate andor velopharyngeal dysfunction International Journal of Languageamp Communication Disorders ( in press)
Shorter E 1995 A spectographic analyis of child homophones Unpublished honours project DeMontfort University Leicester
Stenglehoffen J 1989 Nature and causes of communication diYculties In J Stengelhofen (Ed)Cleft Palate Nature and Remediation of Communication Problems (Edinburgh Churchill Livingstone)
Trost J E 1981 Articulatory additions to the classical description of the speech of persons withcleft palate Cleft Palate Journal 18
Trost-Cardamone J E 1990 The development of speech assessing cleft palate misarticulationsIn D A Kernahan and S N Rosenstein (Eds) Cleft Lip and Palate A System of Management(Baltimore Williams amp Wilkins)
A Harding and P Grunwell352
Appendix Active passive analysis of cleft palate speech

Active versus passive cleft-type speech characteristics 331
andor velopharyngeal dysfunction However none of the distinctions have beenexpressed with reference to their potential impact on phonological developmentStengelhofen (1989) noted that reduced intra-oral pressure may result in nasalrealization of voiced plosives b d gmdash[m n Icirc] This can have a devastating eVecton speech development because plosives [b d] usually represent most fricative targetconsonants in early speech acquisition (age 10ndash20 approx) The phonologicalconsequence of loss of intra-oral pressure may be that a childrsquos early consonantrepertoire could be restricted to nasals and approximants [m n Icirc w j] with [h]sometimes representing voiceless plosive and fricative targets Russell (1991) andHarding (1993) observed nasal fricative consonants in developing speech patternswhich in some but not all cases resolved Russell and Grunwell (1993) consideredthe eVect of abnormal learned neuromotor patterns which can dominate phonolo-gical development A restricted phonetic repertoire in babble can persist into earlyspeech irrespective of increasing potential for velopharyngeal function In the workof Russell (Russell 1991 Grunwell and Russell 1993) established articulatory pat-terns were more readily modi ed by some children than others Harding (1993)found that some speakers made placement distinctions in their nasal fricativerealizations but others used one nasal fricative [Icircdeg
k] for all fricative target consonantsApplication of the phonetic repertoire into speech is usually systematic and as aresult most families are able to understand their childrsquos distinctively cleft-typespeech Strategies employed in early speech inevitably aVect phonological processesErrors are process-speci c not phoneme speci c A phonological perspective ininterpretation of speech assessments is therefore both necessary and enlightening
This paper proposes a phonologically based categorization system for cleftpalate speech patterns observed in a longitudinal study of pre-speech and speechdevelopment in diVerent groups of children whose ages ranged from 16 to 130The proposed system predicts an association between certain speech characteristicsand the structure and function of the speech mechanism Since subjects had beentreated with either 1-stage surgery or 2-stage repair in which the hard palate remainedunrepaired until between 4 and 8 years the speech data could be considered inrelation to a range of oral structures Two subjects were recorded before palatesurgery at age 16 other samples were taken when palates were partially repairedor when fully repaired with or without stulae and with or without suspectedvelopharyngeal incompetence During the course of the longitudinal studies sevensubjects underwent surgery and the eVects of surgery on speech were monitored
Pre-speech and speech samples were taken at 6-monthly intervals at diVerentstages of surgical repair and at diVerent stages of speech development Detailedanalysis of 141 speech samples led to the identi cation of the activepassiveframework which is described here
Four concurrent studies three of which were longitudinal included subjects bornwith complete clefts of lip and palate aged between 16 and 130 Study 1 followedpre-speech vocalizations into speech from ages 16 to 46 and Study 2 recorded patternsof change in speech production from ages 46 to 76 Studies 3 and 4 comprised 2groups of older subjects Study 3 ages 90ndash110 and Study 4 130 were primarilyincluded to facilitate comparison between speech and facial growth
Method
Speech samples were elicited from younger subjects by use of the prototype of thePACSTOYS Screening Assessment (Grunwell and Harding 1995) whereas older
A Harding and P Grunwell332
subjects were asked to describe PACS pictures (Grunwell 1987) Speech was tran-scribed both live and from audio recordings Live transcription was thought to bean essential supplement to audio recordings since some visually perceived character-istics could not be detected on the audio-recordings eg labiodental nasal [Iacute] mightbe perceived as a bilabial nasal on audio recording Slight audible nasal emission asin [pk] might be suspected on audio but it would be con rmed by live transcription
The following speech parameters were studied nasal resonance nasal emissionnasal turbulence voice lip posture intelligibility and consonant production Speechsamples were taken in the home and hence routine endoscopy and uoroscopywere impracticable It is furthermore questionable whether such investigationswould be thought ethical unless they were necessary for clinical management Theprimary area of interest in this investigation has therefore been detailed examinationof the nature of consonant production in relation to oral structure Harding andGrunwell (1996) have identi ed articulatory errors of place as glottal pharyngealuvular velar lateral palatal double articulations For the seven individuals whounderwent surgery the pre-operative data were compared with the processesobserved post-operatively to ascertain whether any trends in post-operative conson-ant production could be identi ed Phoneme realizations were transcribed andcharted on to phoneme evolution charts (Harding 1993) and phonetic diagrams(Harding and Grunwell 1993) were completed for each speech sample
Analytical approach
Initially cleft-type consonant production errors were distinguished from thosedevelopmental errors thought to be unrelated to the cleft Errors related to the cleftpalate were categorized as Cleft-Type Realizations (CTRs) (Harding and Grunwell1993)
Since most articulatory errors aVected groups of consonants speech errors werefurther categorized within a phonologically based framework of cleft-type processesThe speci c processes were de ned within the 1987 concept of Hutters andBrondstedrsquos active versus passive strategies
Activepassive analytical framework
Active processes are de ned here as alternative articulations thought to have beenactively generated in order to establish the necessary phoneme distinctions betweenindividual consonant targets Where one strategy systematically aVected more thanone consonant target and these targets were phonologically related then that strategywas identi ed as a process a cleft-type phonological process For example backingusually aVected several alveolar targets t d n s z resulting in a backing pro-cess In this de nition alternative articulations include both non-English consonantrealizations eg s to [x] and alternative English consonants as in t backed to [k]
Figure 1 illustrates the nature of realizations involved in active processes As agroup they resemble but are not the same as Trostrsquos (1981) compensatory articula-tions In early speech attempts at several fricative target consonants might all berealized by a single realization for example s z S Z might be any of the followingnasal fricative [n
degk] post-oral glottal [h] or pharyngeal [Eacute] backed to uvular [X] or
to velar [x] lateral [Euml] palatal [c] A backing process aVecting production of [s]might also result in backing of both alveolar target plosive consonants eg t to
Active versus passive cleft-type speech characteristics 333
Figure 1 Active cleft-type processes
[k] and of nasal andor lateral alveolar target consonants n l to [Icirc] Whilst thesecharacteristics might as has been assumed in the past be pure articulatory errorsthere are phonological consequences (Grundy and Harding 1995) when severalclasses of consonants eg voiced and voiceless alveolar fricatives and alveolarplosives are realized by one consonant [g] resulting in multiple loss of phonologicalcontrasts or systematic sound preference (Grunwell 1985)
In viewing gure 1 it is worth noting that pharyngeal and glottal articulationare lsquonon-oralrsquo productions which do not require intra-oral pressure or velopharyngealclosure and their production would not evoke sphincteric movement A speakermust at least intend an oral production if potential velopharyngeal sphincter functionis to be accurately assessed Hence predominance of glottal and pharyngeal patternsof articulation imply but do not prove the existence of an inadequate sphincter
lsquoActiversquo processes which establish meaningful contrasts did not account for allthe cleft-type speech patterns observed in the data Consideration is now given tothe cleft-type realizations thought to be passive products of either structural defector dysfunction Hypernasal resonance co-occurring with passive patterns of articula-tion are frequently a direct consequence of weak or absent intra-oral pressure In apassive realization there is no alteration of the articulatory pattern for the intendedconsonant eg the bilabial b in ball is produced [m] [mO~] As shown by gure 2exclusively passive patterns of articulation employ few consonants (approximantsand nasals and glottal [h]) [m n Icirc w j l h] to represent all adult consonants Thisrange of consonants when associated with nasalized vowels suggests a lack ofpotential to establish intra-oral pressure for speech To date passive consequencesof the cleft on speech have received minimal attention perhaps because they donot involve non-English consonant realizations Lack of intra-oral pressure isassociated with hypernasal resonance and nasal emission (Kummer et al 1992)Nasal emission is perceived either accompanying or replacing voiceless pressureconsonant targets hence it will not be present until a child is actively targetingvoiceless pressure consonants (Sell et al 1994) Severely hypernasal speech may notevidence nasal emission until fricative targets are intended and realized as [(sk)n
deg]
for examplePassive processes which severely limit the range of consonants can impair
communication more than a combination of active processes Speech samples
A Harding and P Grunwell334
Figure 2 Passive cleft-type processes
containing active processes usually sound distinctive but communicative compet-ence can be impressive because more meaningful diVerences can be signalled thanmay be possible with the restricted phonetic repertoire of passive processes Giventhat the velopharyngeal sphincter is complex and dynamic it is possible for arestricted phonetic repertoire with hypernasal resonance to persist into early speechdevelopment because a child has been unable to achieve velopharyngeal functionfor speech after palate repair
The distinction between active and passive cleft-type processes has been integ-rated into the revised cleft palate speech assessment GOSSPASSrsquo98 (Sell et al1998) De nitions of cleft-type characteristics are given in GOSSPASSrsquo98 butGOSSPASS does not interpret the phonological consequences of the cleft-typecharacteristics The following de nitions of active and passive cleft-type processesare based on data analysis in the present study and on Harding and Grunwellrsquos(1996) characteristics of cleft palate speech Analysis of patterns of phonemeevolution throughout speech acquisition has generated a hierarchy of error-severityThe following descriptions of the diVerent types of processes are illustrated byreference to the data collected in the research studies (Harding 1993)
Active cleft type processes
Active nasal fricatives
[mdegk] [n
degk] [ Daggerk
deg] Nasal realizations of voiceless and sometimes voiced fricative targets
f v s z S Z were categorized as nasal fricatives Comparison of gures 1 and 2shows that nasal realizations occurred in both passive and active processes Inproduction of active nasal fricatives the pulmonary air is actively directed nasallyas an alternative articulation to an oral fricative realization Figure 3 illustrates thatoral air ow is stopped by either lips or tongue thus achieving 100 nasal air owThis strategy is developed in order to signal the fricative nature of intended targetfricative consonants In the active nasal fricative [m
degk] for f n
degk for s [n
degk O] for
lsquosorersquo [mdegk O] for lsquofourrsquo is the product of actively directed nasal air Where fricative
consonants are the only targets aVected by a cleft-type process the presence ofnasal fricatives have been referred to as phoneme speci c nasality (Trost-Cardamone
Active versus passive cleft-type speech characteristics 335
Figure 3 Active nasal fricative [ndegk]
1990) This characteristic has been found in speakers with no cleft palate historyoften with no explanation for its occurence
DiVerent places of articulation signalled placement contrasts between nasalfricative consonants in the same way that target nasal consonants [m n Icirc] arediVerentiated by place of articulation [m
degk] for f [n
degk] for s S Where a strong
backing process existed alveolar and post-alveolar fricatives were realized by velarnasal fricatives [ Daggerk
deg]
Occasionally nasal air ow was constricted such that nasal fricatives were pro-duced with a noisier turbulent quality [m
deg] [n
deg] [ Dagger] In a detailed assessment of cleft
pa la te speech GOSSPASSrsquo98 (Sell et al 1994 1998) these turbulent realizationswould be categorized in the resonance section as lsquonasal turbulence replacing conson-antsrsquo and in the cleft-type characteristics section as either lsquoactive nasal fricativesrsquo orpassive nasal realization of fricatives
Glottal articulation
[] frequently occurred in early plosive and aVricate production [p b t d T] up toage 46 Sometimes this process aVected only alveolar plosives t d in SIWI andSIWW position At times glottal stop represented voiced plosives [b d g] while[h] represented voiceless plosives [p t k] In SFWF position glottal stop representedboth voiced and voiceless plosives It may be the case that diVerent strengths ofglottal stop were used to distinguish voiceless and voiced plosives but this couldnot be reliably judged without spectographic analysis An undergraduate study ofspectographic analysis (Shorter 1995) of cleft palate speech identi ed some subtlediVerences in glottal stop productions which suggests a need for further investigationinto the phonological functions of glottal stops in cleft palate speech
Pharyngeal fricatives
[Eacute iquest] Early attempts at fricatives (ages 20ndash30) were frequently realized with acombination of posterior fricative cleft-type realizations (CTRs) Where plosiveswere exclusively glottal fricative consonants were frequently realized as pharyngeal
A Harding and P Grunwell336
fricatives In early phonological development obstruent realizations were commonlynon-oral but gradually moved anteriorly to uvular and velar positions Targetconsonants were not generally corrected independently of each other The gradualmovement of pharyngeal realizations towards oral uvularvelar articulation whichunderlines the relevance of a phonological interpretation of cleft palate speechcharacteristics
Exclusively pharyngealglottal patterns of articulation might imply velopharyn-geal insuYciency but it is noted here that all infants use pharyngeal and glottalarticulation until they acquire velopharyngeal competence during the rst 6 monthsof life It is possible for children with cleft palate to persist with this phoneticrepertoire for some time after palate repair Indeed such cases have been reportedby Russell and Grunwell (1993) Non-oral articulatory patterns indicate that thesphincter is not employed during speech which implies that the sphincter may notbe functional but unless oral air ow is consciously intended it cannot be assumedthat the sphincter is unable to function in speech (Henningsson and Isberg 1986)
Backing [k g q G]
A backing pattern is described by Stengelhofen (1989) as a lsquotendency for oralcontacts to be to the back of the oral cavityrsquo GOSSPASSrsquo98 (Sell et al 1998) makesa distinction here between backing to uvular and backing to velar place ofarticulation
E Backing to uvular [q G X Ograve ] Alveolar target consonants were backed touvular realizations and occasionally velar targets were backed to uvular Thepresence of velar and uvular realizations indicated the presence of some VPfunction but this might have been achieved with tongue humping In thedata acquisition of uvular and velar fricatives generally co-occurred withacquisition of f v which provides further evidence of velopharyngealfunction In the longitudinal study from age 16 to 46 subjects with bilateralclefts spent a period of months realizing all alveolar and post- alveolar voicedand voiceless consonant targets in uvular placement This degree of backingis deemed to be more severe and distracting for listeners than backing tovelar perhaps because uvular articulation is more distinctively non-EnglishHowever uvular fricatives are frequently used to achieve some meaningfulcontrasts which improve intelligibility
E Backing to velar In the younger subjects (aged 16ndash46) as articulatorypatterns progressed anteriorly a preference for [g] was common Mostcommonly backing resulted in t d realized as [k g] and s z as [x aring ]which contrasts with the fronting pattern seen in normal development
Double articulation
This is de ned as two simultaneous equal strictures at two places of articulationwhich was frequently noted in realizations of target alveolar consonants t d whenalveolarvelar contacts [tkk dkg] were used Double articulation may have beendeveloped to distinguish between alveolar and velar consonants in the presence ofa backing pattern Interestingly double articulation became evident in these develop-ing speech patterns with the emergence of fricative realizations Both plosives andfricatives tended to be realized with double articulation eg tndash[tkk] sndash[skagrave ]
Active versus passive cleft-type speech characteristics 337
Palatal fricatives [c J ]
These fricative realizations of alveolar target consonants appeared towards the endof the study period (ages 16ndash46) They were the most common realizations ofalveolar fricatives in older children (46ndash76 and 100ndash110) This nding was inaccordance with Alberyrsquos results (Albery 1991 Albery and Grunwell 1993)
Lateral fricatives [l Igrave]
As with palatal fricatives lateral fricatives were frequently present as realizations offricative consonant targets becoming particularly prevalent in later phonologicaldevelopment
Gliding of fricatives s S= [ j] or [w]
This phenomenon is seen in the non-cleft population as an uncommon develop-mental process (Grunwell 1987) It is classi ed here as an active process because[ j] was consistently produced as an apparently active alternative to target conson-ant(s) s z S [ j] is a normal consonant-like production in non-cleft babble whichcleft palate children often integrate into their phonological system It may betherefore that it is a persisting immaturity in the cleft palate population In thesedata [ j] was eVective in signalling a contrast between plosives and fricatives inSIWI position It functioned for the following consonants in diVerent speakers [ j]for S [ j] for m p f s z Ÿ h and co-articulation [hkj] for T
Passive cleft type processes
The criteria for passive cleft type processes is that they are (1) an attempt toproduce the correct articulatory placement and stricture (manner) which (2) failsbecause of a lack of intra-oral air pressure For example voiced plosives realized asnasals b[ [m] d[ [n] g[ [Icirc] No compensatory articulatory pattern hasbeen used to replace the intended consonant As the above examples demonstratetarget realizations often match a similar English consonant
Absence of pressure consonantspredominantly sonorant articulation
This phenomenon is de ned here as a pattern of articulation which was restrictedto English nasal and approximant articulations [m n Icirc w j] and [h] Some of thevoiced consonants were also employed as voiceless counterparts [m
degndeg Icircdeg ] thereby
increasing the range of available consonants for distribution in the phonologicalsystem Despite the limited consonant repertoire these patterns were often eVec-tively interpreted by close family members
Weak articulation [bV dV]
This category refers to normal articulatory movement in the production of obstruenttargets (plosive fricative and aVricate targets) which were produced with reducedoral air pressure and therefore articulation was considerably weakened In the speechsample data (ages 16ndash46) many target consonants were weakened to some degreeand at times may have been realised as nasals
A Harding and P Grunwell338
Passive nasal fricative [(fk)m (sk)ndeg]
Incomplete velopharyngeal closure inevitably reduces control of oral air ow with apassive loss of air ow and an increase of resonance in the nasal cavity Grunwelland Harding (1996) de ned the passively nasal fricative as an unreleased [(s)]double-articulated with a lowered voiceless nasal [n
Aacute
deg] This realization is the product
of an intended s with an unintended nasal air ow (see gure 4) The precisetranscription for a passive nasal transcription is [(sk)n
Aacute
deg] but an acceptable simpli cation
for transcription purposes is [(sk)ndeg] This is distinct from the active nasal fricative
which involves stopping of the oral air ow and active direction of air nasally whichcan be transcribed as a voiceless nasal with additional nasal emission [n
degk] Nasal
emission signals the fricative nature of for example target consonant s Thesetwo productions can sound the same and might initially be transcribed as [n
degk]
Nasendoscopic investigation of velopharyngeal activity during active and passivenasal realizations of s both show a lack of velopharyngeal closure It is predictedthat close examination by use of electropalatography might show slight diVerencesin tongue tip posture for an active and passive nasal fricative as illustrated in gures3 and 4 Passive nasal fricatives were converted into oral fricatives with nose-holding
Voiceless [h] for voiceless plosives
There was evidence that voiceless plosives were at times passively realized as [h]The consequence of reduced oral air pressure on production of voiceless plosivescan leave aspiration as the only perceptible distinctive feature This process usuallyaVected all voiceless plosive targets p t k Where this process was a passiveprocess use of noseholding during speech facilitated accurate target productionHowever it would also be possible for this distribution of [h] to be an active cleft-type process which would be part of a pharyngealglottal patternprocess
Nasal realization of voiced plosives b d g[ [m n Icirc]
Some subjects with residual clefts stulae or suspected VPI realized voiced conson-ants as nasal counterparts As summarized by Harding and Grunwell (1996) voiced
Figure 4 Passive nasal fricative [(sk)nAacute
deg]
Active versus passive cleft-type speech characteristics 339
consonants can be more diYcult to produce than voiceless consonants (Isshiki andRingel 1964) Distinction between active versus passive nasal realizations of plosivetargets was made in the same way that active and passive nasal fricatives weredistinguished by observing the eVect of noseholding on consonant production Inpassive nasal realizations noseholding facilitated normal consonant production(Golding-Kushner 1995)
Nasal emission accompanying consonants [pk sk]
Nasal emission was frequently heard accompanying consonants but on occasions itapparently replaced consonants It has been linked with velopharyngeal incompet-ence (VPI) (Kummer et al 1992)
Results
Comparison of activepassive processes in the speech data
Quantitative results of Hardingrsquos research into the relationship between timing ofsurgery and speech development have already been published (Harding andGrunwell 1993) The following interpretation of the data speci cally identi esactivepassive cleft-type processes in relation to oral structure in a wide age rangeof subjects (16ndash130) Tables 1 2 3 and 4 show the passive and active processeson the left-hand column and the subjectrsquos code along the top The code identi esthose subjects who were treated with 1-stage versus 2-stage surgery Comparisonof the 4 tables at age 46 (BCLP and UCLP) at age 90 and at age 130 illustratesa pattern of diminishing cleft-type processes with increasing age Irrespective ofsurgical timing few cleft-type processes remained at age 130 (table 4) A generalobservation was that earlier speech samples (ages 16ndash76) frequently combined
Table 1 Cleft-type processes in BCLP subjects at age 46 (studies 1 and 2)
1-stage surgery 2-stage surgery
A G Rf JW D B JF JG AB
Passive cleft-type processespredominantly sonorant articulation m
weak articulation m m m m m m m m
voiceless h for plosive m m m m m
nasal release of plosives m m m m m
nasal emission with consonants m m m m m m
passive nasal fricativeActive cleft-type processes
nasal fricatives m m m m m m m m
pharyngeal glottal articulation m m m m m m m m
backing to uvular m m m m m m m m
backing to velar m m m m m m m m m
lateral palatal fricatives m m m m m m m m m
double articulation m m m m m m m m m
gliding fricative m m
f=post-operative stula
A Harding and P Grunwell340
Table 2 Cleft-type processes in UCLP subjects at age 46 (study 2)
1-stage surgery 2-stage surgery
SE TB CK MS NC TS ZG CP
Passive cleft-type processespredominantly sonorant artic m
weak articulation m m m
voiceless h for plosives m m m
nasal release of plosives m m m
nasal emission with consonants m m
passive nasal fricative m m
Active cleft-type processesnasal fricativepharyngeal glottal articulation m m m
backing to uvular m
backing to velar m m
lateral palatal fricatives m m m m m
double articulation m m m m m m
gliding fricative m
Table 3 Cleft-type processes at age 90
2-stage surgery 2-stage surgery1-stage surgery completed at 4 yrs completed at 8 yrs
DAf SBf RL NR JD AR LJ RP MB
Passive cleft-type processespredominantly sonorant articweak articulation m
voiceless h for plosives m m
nasal release of plosives m m
nasal emission with consonants m m m m
passive nasal fricatives m m
Active cleft-type processesnasal fricatives m m
pharyngeal glottal articulation m m
backing to uvular m m
backing to velar m m m m m m m
lateral palatal fricatives m m m m m m m
double articulation m m m m m
gliding fricative m
f=subject had a stula
both active and passive strategies whereas later samples (ages 90ndash130) rarelyevidenced passive processes
At age 46 four out of ve BCLP subjects used active non-oral pharyngeal andglottal processes and oral velar and uvular fricatives irrespective of surgical status(see table 1) All had some anterior palatal defect which might have reduced theirpotential to achieve intra-oral pressure
By comparison two out of three partially repaired 2-stage UCLP subjects at age46 (table 2) showed evidence of passive processes This suggested that their
Active versus passive cleft-type speech characteristics 341
Tab
le4
Spee
chin
rela
tion
tosu
rgic
altim
ing
atag
e13
0
2-st
age
surg
ery
2-st
age
surg
ery
1-st
age
surg
ery
subj
ects
com
plet
edat
4yr
sco
mpl
eted
at8
yrs
1-A
1-B
1-C
1-D
1-E
1-F
24-
G2
4-H
24-
J2
8-K
28-
L2
8-M
Pass
ive
clef
t-ty
pepr
oces
ses
pred
omin
antly
sono
rant
artic
wea
kar
ticul
atio
nm
voic
eles
sh
fo
rpl
osiv
esna
sal
rele
ase
ofpl
osiv
esna
sal
emis
sion
with
cons
onan
tsm
pass
ive
nasa
lfr
icat
ives
Act
ive
clef
t-ty
pepr
oces
ses
nasa
lfr
icat
ives
phar
ynge
alg
lott
alar
ticul
atio
nba
ckin
gto
uvul
arba
ckin
gto
vela
rm
m
late
ral
pala
tal
fric
ativ
esm
mm
doub
lear
ticul
atio
ngl
idin
gfr
icat
ive
1=1-
stag
esu
rger
ysu
bjec
ts
24=
2-st
age
surg
ery
hard
pala
tere
pair
edat
abou
t4
yrs
28=
2-st
age
surg
ery
with
hard
pala
tere
pair
edat
abou
t8
yrs
A Harding and P Grunwell342
unrepaired hard palates had in fact restricted their phonetic repertoire imposing aneed for individual adaptability The additional active processes employed by thesesubjects were presumably a response to the restrictions imposed by their oro-nasalstructure and velopharyngeal function at the time of consonant acquisition Asshown in table 2 the most common active cleft-type processes persisting at age46 with a residual cleft of the hard palate were backing double articulation andlateralpalatal articulation Two 1-stage surgery subjects whose entire palates hadbeen repaired at ages 09 and 010 did not use any cleft-type processes at age 46
By age 90 (table 3) a much-diminished number of cleft type processes wasevident except in subjects with sizeable anterior stulae who had received littlespeech and language therapy A similarity was noted between the speech patternsof 1-stage surgery subjects with stulae (DA and SB) at age 90 (table 3) and theyounger BCLP subjects at age 46 (table 1) who also had anterior palatal defectsThey included non-oral realizations of t d s k g occasional nasal fricatives andpharyngealglottal articulations Fistulae had apparently continued to in uencearticulation and phonological development in these subjects
Finally at age 130 (table 4) the diVerences between 1-stage and 2-stage surgerysubjects had diminished leaving only one 2-stage subject with occasional backingand four subjects with slight palatal and lateral release of fricative consonants Onlytwo of the 1-stage surgery subjects were using minor distortions of grooved fricativeproduction
Whilst there were apparent trends in speech production relating to surgicaltiming and oral structure it is noted that there were exceptions to each tentativegeneralization Subjects with marked structural imperfections occasionally producedrealizations of which they would not have been thought capable and subjects withno visible imperfections produced inexplicably distorted speech patterns It istherefore concluded that whilst there is homogeneity in the range of processesproduced by this population assumptions cannot be made about speech based onsurgical timing or type of cleft Tentative predictions based on detailed assessmentmay be clinically very useful
EVects of surgery on speech
Activepassive processes have identi ed those cleft-type characteristics thought tobe associated with a physical inability to produce pressure consonants The followinganalysis of speech changes after surgical intervention at diVerent ages identi es thechanges eVected by surgery when intra-oral pressure could be more readily achieved
Two children were rst recorded prior to the rst stage of a 2-stage procedureTheir lips were repaired at approximately 6 months of age and soft palate repairwas carried out at ages 18 and 19 respectively Their hard palates were leftunrepaired to facilitate unrestricted growth of the mid-face (Hotz et al 1978) Pre-and post-operative consonant-like sounds present in the recorded speech samplesare listed in table 5 Interestingly prior to soft palate repair both these childrenproduced some oral consonants Subject B was producing pressure consonants [kg] in his babble prior to soft palate repair Considering that he had an unrepairedbilateral cleft palate at this point it was surprising that he had any oral consonantsPost-operatively at 20 years he used [b bkm t d g gkb] which indicated that surgeryto repair the soft palate had facilitated an increased range of oral pressure consonantsSubject D was producing [p b k g] pre-operatively Post-operatively following soft
Active versus passive cleft-type speech characteristics 343
Tab
le5
EV
ects
ofso
ftp
alat
ere
pair
atag
e1
6on
BC
LP
subj
ects
h
ard
pal
ate
rem
ain
sun
repa
ired
2-st
age
subj
ects
Surg
ery
Pre
-ope
rati
vesp
eech
patt
ern
atag
e1
6Po
st-o
pera
tive
chan
ges
insp
eech
atag
e2
0
Stud
y1
BSo
ftpa
late
repa
irat
16
Adu
ltta
rget
sk
gA
t2
0[b
b kmg kb
td
g]D
Soft
pala
tere
pair
17
Adu
ltta
rget
sp
bk
gA
t2
0[p
bd
b kdk
g]
Tab
le6
EV
ects
ofha
rdpa
late
rep
air
atag
e6
6an
d
stu
lare
pair
atag
e10
0
Subj
ect
Surg
ery
Pre
-ope
rati
vesp
eech
patt
ern
Post
-ope
rati
vech
ange
sin
spee
ch
MS
Har
dpa
late
repa
ir6
6Pa
ssiv
epr
oces
s7
6E
limin
ated
pass
ive
proc
ess
Var
iabl
ena
sal
rele
ase
ofco
nson
ants
Hyp
onas
alna
sals
JFH
ard
pala
tere
pair
(uns
ucce
ssfu
l)6
6Se
vera
lac
tive
and
pass
ive
proc
esse
s7
6A
ctiv
epr
oces
ses
rem
aine
dPa
ssiv
epr
oces
ses
elim
inat
ed
DA
Fis
tula
repa
ir10
0A
ctiv
epr
oces
ses
110
Elim
inat
ion
ofph
aryn
geal
glo
ttal
Var
iabi
lity+
+an
dna
sal
arti
cula
tion
Art
icul
ator
yva
riab
ility
++
Act
ive
CT
Rs
proc
esse
spe
rsis
t
A Harding and P Grunwell344
palate repair but with a residual cleft in the hard palate his range of consonantsincluded [d] which was particularly surprising since the hard palate remainedunrepaired Whilst it is unlikely that toddlers of 18 months could be consciouslytrying to compensate for articulatory inadequacy in producing velar plosives inbabble prior to soft palate repair and an alveolar plosive prior to hard palate repairboth these subjects showed evidence of actively pursuing their articulatory potential
Table 6 summarizes changes following surgery to repair the hard palate in moremature speech patterns These subjects who were aged 66 and 100 pre-operativelyhad learned to speak with residual clefts and were apparently unaware of theconsonant productions that failed to match normal production
Subject MS used only passive processes in his speech pattern He realized someconsonants nasally such that lsquoballrsquo was [mO~] and lsquosockrsquo was [(sk)n
deg Aacute~ k] Looking atpost-operative changes at age 76 his consonant production was normal but hisresonance had become hyponasal Pre-operatively at age 66 Subject JF was usingseveral active and passive processes The active processes were unaVected by surgerybut passive processes were eliminated
Fistula repair was carried out at age 100 on Subject DA who had many activeprocesses and very variable articulation pre-operatively Post-operatively at age110 he was not using non-oral pharyngeal and glottal active processes or nasalrealizations but many oral cleft-type realizations remained
As shown in table 7 hard palate re-repair and pharyngoplasty was carried outon two subjects whose hard palate repairs had been unsuccessful at approximately4 years Subject NC assessed pre-operatively at age 56 was using predominantlypassive processes in her speech She was also using [ j] for fricatives s S whichwas thought to be an active process At age 60 following hard palate re-repair andpharyngoplasty all cleft-type processes had been eliminated without post-operativespeech therapy Since [ j] for s apparently resolved spontaneously followingsurgery it can be assumed that this was a passive process in this speech sample
Subject CP who underwent this procedure presented pre-operatively at age 46with both passive and active processes but his nasal resonance was not consistentlyhypernasal In addition to his cleft-related speech disorder this subject had additionaldevelopmental speech diYculties which were identi ed as being unrelated to thecleft Post-operatively at age 56 little had changedmdashnotably the passive processnasal [m] for b was retained His nasal resonance had become hyponasal andthere was no apparent bene t from surgical intervention The realization of b as[m] had become phonologically stable and surgery alone had not destabilized thephonological system This realization may have been a passive product of VPI inearly speech acquisition which had subsequently become part of a phonologicaldisorder Post-operatively CPrsquos phonetic repertoire did increase but the phonologicaldistribution was variable Plosive targets were still realized as nasals in spontaneousspeech at the nal speech recording at age 76 This was not as an inevitableconsequence of VPI but a result of an inability to destabilize the phonologicalprocess determining that voiced plosives would be realized as nasals This resultfollowing surgery highlights the importance of identifying phonological learningproblems and distinguishing them from structural constraints on articulationIn CPrsquos case pre-operative exploration of the eVect of nares occlusion duringspeech might have indicated that structural change would not improve consonantproduction spontaneously
A general observation was that consonant realizations did not move rapidly
Active versus passive cleft-type speech characteristics 345
Tab
le7
EV
ects
ofha
rdpa
late
re-r
epai
ran
dp
hary
ngo
pla
sty
Subj
ect
Surg
ery
Pre
-ope
rati
vesp
eech
patt
ern
Post
-ope
rativ
ech
ange
sin
spee
ch
Stud
y2
NC
Har
dpa
late
re-r
epai
ran
d5
6Pa
ssiv
ecl
eft-
type
proc
esse
s6
0A
llcl
eft-
type
phar
yngo
plas
ty5
10[
j]
for
fric
ativ
espr
oces
ses
elim
inat
ed[
h]
for
plos
ives
SIW
IV
aria
ble
arti
cula
rypr
ecis
ion
CP
Har
dpa
late
repa
iran
d4
6Pa
ssiv
ean
dac
tive
proc
esse
s5
6Pa
ssiv
epr
oces
sph
aryn
gopl
asty
50
Pho
nolo
gica
lco
nfus
ion
[m]
for
[b
]re
tain
edH
ypon
asal
nasa
lsPe
rsis
ting
phon
olog
ical
conf
usio
ns
A Harding and P Grunwell346
from incorrect to correct but progressed incrementally towards normal realizationsas described by Morley (1970) Where an early realization of target s might beglottal [h] a gradual pattern of change showed subsequent realizations to bepharyngeal [Eacute] then uvular [X] then velar [x] and eventually palatal [c] or lateral [Euml]It was interesting to note that speech patterns continued to change as late as90ndash110 years with the result that diVerences related to surgical timing and cleft-type gradually disappeared Persisting stulae were thought to account for the mostmarked cleft type processes at age 90
Implications for surgical management
This analysis of speech changes following surgery suggests some implications forsurgical management which are compatible with Sell and Grunwellrsquos (1990) ndingsin the Sri Lankan study
Surgery can change passive speech processes but it is also possible that speechtherapy may be able to change passive patterns Surgery alone is unlikely to modifyactive cleft-type processes whereas speech therapy should be able to modify activeprocesses Indications from these case studies is that where speech is the primaryproblem speech assessment should distinguish between active and passive processesin order to evaluate the necessity for full investigations and to plan therapeuticintervention Where past speech therapy has not been successful it cannot beassumed that surgical intervention will facilitate further speech progress A furthercourse of speech therapy which is sensitive to active versus passive processes todevelopmental phonological in uences on cleft-type speech development and toarticulatory diYculties in diVerent speech contexts might facilitate optimal progressWhere structural imperfection exists it is quite possible for single-word productionto be more precise than target realizations in spontaneous speech This may not bea failure of phonological generalization (Grunwell 1992) but the result of diYcultysustaining the necessary lsquoarticulatory eVort rsquo (Harding and Grunwell 1993) resultingin articulatory imprecision Deteriorating articulatory accuracy should not be over-looked in interpretation of speech results
An analytical protocol
As a result of analysing the speech data and identifying the active and passiveprocesses a protocol has been developed which records examples of each cleft-typeprocess over a series of assessments It demonstrates the progression of individualprocesses towards an adult target (see the Appendix) At each assessment onecolumn is used to indicate nasal resonance nasal emission and nasal turbulenceratings and cleft-type processes Changes in the nature of error realizations mightshow progress towards target consonants Hence whilst the total correct scoremight not have increased increments of change can be observed This observationof patterns of change may function as an adjunct to GOSSPASSrsquo98 (Sell et al 1998)giving access to a greater depth of both quantitative and qualitative data aboutconsonant production in relation to resonance nasal emission nasal turbulenceoral structure and cleft-type
Active versus passive cleft-type speech characteristics 347
Diagnostic implications
Passive versus active nasal fricatives
The important management consideration related to this distinction is that an activenasal fricative is an established phonological process which is unlikely to be directlyaVected by surgery alone Therapy would be necessary to destabilize nasal realizationsof oral consonants In contrast passive nasal fricatives may be eliminated by surgeryOf particular relevance is diVerential diagnosis between passive and active nasalfricatives in surgical and therapeutic management When hypernasality co-occurswith nasal air ow during consonant production which can be redirected by nose-holding passive nasal fricatives are diagnosed These would be transcribed as [(sk)n
deg]
passive alveolar nasal fricatives [(Wk)mdeg
] bilabial nasal fricatives or [(fk)Iacutedeg ] labiodentalnasal fricatives Full VPI investigations would be recommended to diagnose thenature of the structural or functional de ciency and distinguish between velopharyn-geal incompetence and velopharyngeal mislearning
It is highly likely that plosive targets would be aVected by reduced intra-oral airpressure such that plosives would either be realized by nasal counterparts eg bd[ [m n] or [b d] may be nasalized and weak Voiceless plosives may be eitheraccompanied by nasal emission [p t k] or realized as glottal fricative [h]
Production of the target sentence lsquoI saw Sam sitting on a busrsquo might be
[aI (sk)ndeg O~ (sk)n
degaelig~m (sk)n
deg IhIn Aacute~n mouml~(sk)ndeg] passive processes and
[aI xO xaeligm xIkIIcirc AacuteIcirc goumlx] active processes
Contribution to surgical management decisions
Passiveactive interpretation of clinical assessments might facilitate surgical manage-ment decisions If noseholding does not facilitate correct production of targetconsonants then it is likely that an alternative articulatory pattern has becomephonologically established ie particular realizations for one or more targets areconsistently distributed in the phonological system These realizations may haveevolved because of initial diYculty producing articulatory targets and subsequentlystabilized within the phonological system Grundy and Harding (1995) refer to thisphenomenon as an lsquoarticulatory disorder with phonological consequencesrsquo
Therapy
Where obvious structural defects or diagnosed dysfunction exists clinicians fre-quently defer therapeutic intervention until surgery has been undertaken Theexpectation would be that normal structure and function is essential for normalspeech However pre-operative therapy may facilitate oral consonant productionwhich may serve to reduce hypernasal resonance Hence therapy prior to surgerymay avoid unnecessary surgery or reduce the extent of surgery required All activeprocesses are likely to require therapy
Principled selection of targets for therapy
Speech patterns frequently evidence a mixture of apparently passive and activeprocesses which complicates decisions about target selection Target selection can
A Harding and P Grunwell348
be based on assessment of which consonant targets can be most easily elicted inisolation (stimulability) This may lead to a sequence of target selection which isopposite to the sequence of consonant acquisition in normal development Forexample where reduced intra-oral pressure is present in a passive pattern [T] maybe easier to elicit in imitation than more nely grooved [s] or [S] Therapy maytarget [T] followed by [S ] and nally [s] As in non-cleft phonological therapywhere a class of consonants is aVected by the cleft then it is helpful to target theentire class The following decision-making process can be applied for both activeand passive processes
Decision making procedure for target selection
(1) Voiced versus voiceless targets(2) Front versus back placements(3) Syllable initial versus syllable nal targets(4) Plosives versus fricative targets
Voiceless plosives and fricatives are produced with an open glottis whichfacilitates topping up of air ow from the lungs hence voiceless plosive and fricativetargets are frequently more successful than voiced counterparts (Isshiki and Ringel1964) Front targets usually cause more diYculty than back particularly where analveolar defect or stula exists Contrary to normal development back targets maybe targeted before front Word- nal targets generally require less oral air pressurethan word initial targets and similarly fricatives may be more easily elicited thanplosives Fricatives do require a greater volume of air than plosives (Fletcher 1985)but in the presence of nasal escape weak fricative production appears to be morereadily achieved than weak plosive production Since nal fricatives would normallybe acquired in advance of word-initial fricatives (Ferguson 1978) targeting word- nal fricatives is frequently a productive starting point for therapy
Principles of therapy for passive processes
(1) Use of soft attack similar to gentle whisper for all target models ensuresminimal articulatory eVort (Harding and Grunwell 1993) and requires min-imal intra-oral air pressure It may be appropriate to gradually increase thearticulatory attack when the articulatory posture and evidence of intendedoral air ow have been established
(2) Slightly stretched duration of segment transitions in models of consonantto vowel (CndashV) or vowel to consonant (VndashC) facilitates review of motorplanning and extends the available time for execution of the new motorprogrammer whilst maintaining control of the oral airstream
(3) Noseholding can be used to provide exclusively oral air ow Gradual releaseof the nostrils during production of sustained [VVVVVf ] or [hhhhh ] allowsthe child to attempt to sustain an oral consonant despite increasing nasalemission This maximizes the use of available oral air ow Procedures forusing noseholding are described in some detail by Golding-Kushner (1995)
Principles of therapy for active processes
This is more like phonological therapy and can follow Grunwellrsquos (1991) processesfor phonological change and principled decision-making (Grunwell 1992) Some
Active versus passive cleft-type speech characteristics 349
examples are given here by way of illustration of ways to eVect the rst twoprocesses of change which may need to be approached diVerently in cleft palateversus non-cleft speech disorders DiVerent approaches may also be appropriate formodifying active versus passive cleft-type processes
Innovation production of new targets Some useful principles
(1) Introduction of new lsquonon-speech likersquo targets in sound play using a conson-ant sound segment model such as [ph ] note not a syllable like [p] whichis the type of pronunciation used when target sounds are presented as lettersfor reading Target [s] might be introduced as a lsquoTrain Slowing Down Noisersquo[ts ts ts tssssssss]
(2) lsquoNew consonantsrsquo can later be modelled and elicited in soft productions ofsyllable structure [tssssndashi] [ indashtssss] which can subsequently be identi ed assimilar to words lsquosearsquo and lsquoeatsrsquo
(3) lsquoDeferring responsibilityrsquo transfers responsibility or lsquoblamersquo for errors fromthe child and attributes it to the articulators eg lsquoyour tongue is havingtrouble with hellip rsquo lsquoLetrsquos show your tongue how to hellip rsquo
(4) New targets can be modelled repeatedly and recorded on audio or videotape which can be listened to at home
(5) Targeting classes of consonants (eg alveolars t d s n l voiceless fricativesf s S perhaps with aVricate T avoids phonological confusion whichmight occur if production ofsis achieved whilst other alveolar targetsremain backed The risk is that s might not integrate into the phonologicalsystem unless all backed alveolar consonants are destabilized
(6) Increased eye contact during auditory and production work can be invaluablein holding visual and auditory attention and ensures that visual informationabout the sound has been processed This is easily achieved by the clinicianlifting any focus of the childrsquos attention close to hisher mouth at theprecise moment when the target is modelled
Stimulation of non-speech related sounds such as a lsquoTrain Slowing DownNoisersquo [ts ts tsss] con rms that target [s] is physically achievable whether or not[ssss] can be imitated Some children continue to access [s] through the lsquoTrainSlowing Down Noisersquo throughout therapy until it is occurring spontaneouslywithout conscious planning This can be an eVective means of underminingestablished motor programmers (Hewlett 1990) for active cleft-type processes
Destabilizing active processes
As it is likely that children will be unaware of each occurrence of their alternativearticulatory pattern for speci c consonant errors it is preferrable to destabilizeactive processes with minimal conscious eVort by the child As children becomeaware of their mismatches they frequently add the newly acquired target realizationto their existing production eg target word tu childrsquos old realization [ku] childrsquoscorrected realization [t-ku] Destabilization can be achieved with minimal consciouseVort through input therapy techniques such as auditory bombardment (Lancasterand Pope 1989) auditory decision-making such as lsquowhich bear says this wordproperlyrsquo Red Bear says lsquotworsquo or Blue Bear says lsquocoorsquo This type of strategy oftenprecipitates attention to the target consonant with possible lsquoreplayrsquo and lsquoreviewrsquo of
A Harding and P Grunwell350
their own production Frequent stimulation of cognitive alertness to the targetconsonant can develop awareness without confronting the child with errors orrisking hisher failure The child is then free to attempt to repair hisher ownrealization to continue to re ect and to silently rehearse the adult realizationTraditional articulation therapy is thus combined with development of metaphonol-ogical skills ie the ability to re ect upon onersquos own speech production The resultshould be that new target realizations will be more phonologically stable thanexclusively production-based articulation therapy might have facilitated
Stabilizationgeneralization
Procedures to ensure stabilization and generalization of new target consonantswould be as described by Grunwell (1992) Success may be constrained by theconsiderable articulatory eVort sometimes required to maintain pressure consonantproduction in spontaneous speech (Harding and Grunwell 1993)
Conclusions
In speech assessment it is helpful to distinguish between errors which are cleft-type and non-cleft type and those which are part of active versus passive processesThe active and passive processes have been de ned and their phonological implica-tions discussed Focus on active and passive processes has facilitated focus on thephonological consequences of cleft palate on speech development In the futureawareness of the likely eVect of a cleft palate on normal phonological developmentcould avoid extended periods of unsuccessful clinical intervention Furthermoresensitivity to the relationship between phonological processes and structural con-straints should facilitate theoretically based management decisions Incidences suchas the case of CP in which nasal realizations were thought to indicate VPI but weresubsequently unaVected by surgery might be avoided if phonological analysiscontributes to management decisions
Surgery did improve hypernasal resonance and eliminated passive processes buthad little eVect on active processes Active processes in younger subjects werethought to require therapeutic intervention but in the longer term the oldersubjects showed few cleft-type processes Whilst it is possible that active cleft-typeprocesses may resolve with increasing age the implication for the future is thatactive cleft-type processes should be treated with skilled therapeutic interventionnot surgery Therapy which addresses the phonological consequences of cleft palateon speech development by combining metaphonologicalphonologicalarticulatoryapproaches is likely to be successful
References
Albery E 1991 Consonant articulation in the diVerent types of cleft lip and palate UnpublishedMPhil thesis Leicester Polytechnic
Albery E and Grunwell P 1993 Consonant articulation in diVerent types of cleft palate InP Grunwell (Ed) Analysing Cleft Palate Speech (London Whurr)
Ferguson C A 1978 Fricatives in child language acquisition In V Honsa and M Hardmann-Battista (Eds) Papers on Linguistics and Child Language (Mouton The Hague)
Fletcher S G 1985 Speech production and oral motor skill in an adult with an unrepaired palatalcleft Journal of Speech and Hearing Disorders 50 254ndash261
Active versus passive cleft-type speech characteristics 351
Golding-Kushner K J 1995 Treatment of articulation and resonancne disorders associated withcleft palate management and VPI In R Shprintzen (Ed) Cleft Palate Speech Management AMultidisciplinary Approach (St Louis Mosby)
Grundy K and Harding A 1995 Developmental speech disorders In K Grundy (Ed) Linguisticsin Clinical Practice (2nd edition) (London Whurr)
Grunwell P 1985 Phonological Assessment of Child Speech (Windsor NFER-Nelson)Grunwell P 1987a Clinical Phonology (2nd edition) (London Croom Helm)Grunwell P 1987b PACS Pictures Language Elicitation Materials (Windsor NFER-Nelson)Grunwell P 1991 Processes of phonological change in developmental speech disorders Clinical
Linguistics and Phonetics 6 101ndash122Grunwell P 1992 Principled decision making in the remediation of children with phonological
disorders In P Fletcher and D Hall (Eds) Specic Speech and Language Disorders in Children(London Whurr)
Grunwell P and Harding A 1995 PACSTOYS A Screening Assessment of Phonological Development(Windsor NFER-Nelson)
Grunwell P and Harding A 1996 A note on describing types of nasality Clinical Linguistics andPhonetics 10 157ndash161
Harding A 1993 An Investigation into the Relationship Between Timing of Cleft Palate Repairand Speech Development Unpublished PhD thesis
Harding A and Grunwell P 1993 The relationship between speech and timing of hard palaterepair In P Grunwell (Ed) Analysisng Cleft Palate Speech (London Whurr)
Harding A and Grunwell P 1996 Characteristics of cleft palate speech European Journal ofDisorders of Communication 31 331ndash358
Henningsson G and Isberg A M 1986 Velopharyngeal movement patterns in patients alternatingbetween oral and glottal articulation A clinical and cineradiographicical study Cleft Palate Journal23 1ndash9
Hewlett N 1990 Processes of development and production In P Grunwell (Ed) DevelopmentalSpeech Disorders (Edinburgh Churchill Livingstone)
Hotz M M Gnoinski W M Nussbaumer H and Kistler E 1978 Early orthopaedics in CLPcases guidelines for surgery Cleft Palate Journal 15 405ndash411
Hutters B and Brondsted K 1987 Strategies in cleft palate with special reference to DanishCleft Palate Journal 24 127ndash136
Isshiki N and Ringel R 1964 Airow during the production of selected consonants Journal ofSpeech and Hearing Research 7 233ndash244
Kummer A W Curtis C Wiggs M Lee L and Strife J L 1992 Comparison of velopharyngealgap size in patients with hypernasality hypernasality with nasal emission and nasal emissionor nasal turbulence (rustle) as the primary speech characteristic Cleft-palate-Craniofacial Journal29 152ndash156
Lancaster G and Pope L 1989 Working with Childrenrsquos Phonology (Oxford Winslow)Morley M E 1970 Cleft Palate and Speech (7th edition) (Edinburgh Churchill Livingstone)Russell V J 1991 Speech Development in Children with Cleft Lip and Palate Unpublished PhD
thesis Leicester PolytechnicRussell V J and Grunwell P 1993 Speech development in children with cleft lip and palate In
P Grunwell (Ed) Analysing Cleft Palate Speech (London Whurr)Sell D A and Grunwell P 1990 Speech results following late palatal surgery in previously
unoperated Sri Lankan adolescents with cleft palate Cleft Palate Journal 27 162ndash168Sell D Harding A and Grunwell P 1994 GOSSPASS A screening assessment of cleft palate
speech European Journal of Disorders of Communication 29 1ndash15Sell D Harding A and Grunwell P 1998 GOSSPASSrsquo98 An assessment for speech disorders
associated with cleft palate andor velopharyngeal dysfunction International Journal of Languageamp Communication Disorders ( in press)
Shorter E 1995 A spectographic analyis of child homophones Unpublished honours project DeMontfort University Leicester
Stenglehoffen J 1989 Nature and causes of communication diYculties In J Stengelhofen (Ed)Cleft Palate Nature and Remediation of Communication Problems (Edinburgh Churchill Livingstone)
Trost J E 1981 Articulatory additions to the classical description of the speech of persons withcleft palate Cleft Palate Journal 18
Trost-Cardamone J E 1990 The development of speech assessing cleft palate misarticulationsIn D A Kernahan and S N Rosenstein (Eds) Cleft Lip and Palate A System of Management(Baltimore Williams amp Wilkins)
A Harding and P Grunwell352
Appendix Active passive analysis of cleft palate speech

A Harding and P Grunwell332
subjects were asked to describe PACS pictures (Grunwell 1987) Speech was tran-scribed both live and from audio recordings Live transcription was thought to bean essential supplement to audio recordings since some visually perceived character-istics could not be detected on the audio-recordings eg labiodental nasal [Iacute] mightbe perceived as a bilabial nasal on audio recording Slight audible nasal emission asin [pk] might be suspected on audio but it would be con rmed by live transcription
The following speech parameters were studied nasal resonance nasal emissionnasal turbulence voice lip posture intelligibility and consonant production Speechsamples were taken in the home and hence routine endoscopy and uoroscopywere impracticable It is furthermore questionable whether such investigationswould be thought ethical unless they were necessary for clinical management Theprimary area of interest in this investigation has therefore been detailed examinationof the nature of consonant production in relation to oral structure Harding andGrunwell (1996) have identi ed articulatory errors of place as glottal pharyngealuvular velar lateral palatal double articulations For the seven individuals whounderwent surgery the pre-operative data were compared with the processesobserved post-operatively to ascertain whether any trends in post-operative conson-ant production could be identi ed Phoneme realizations were transcribed andcharted on to phoneme evolution charts (Harding 1993) and phonetic diagrams(Harding and Grunwell 1993) were completed for each speech sample
Analytical approach
Initially cleft-type consonant production errors were distinguished from thosedevelopmental errors thought to be unrelated to the cleft Errors related to the cleftpalate were categorized as Cleft-Type Realizations (CTRs) (Harding and Grunwell1993)
Since most articulatory errors aVected groups of consonants speech errors werefurther categorized within a phonologically based framework of cleft-type processesThe speci c processes were de ned within the 1987 concept of Hutters andBrondstedrsquos active versus passive strategies
Activepassive analytical framework
Active processes are de ned here as alternative articulations thought to have beenactively generated in order to establish the necessary phoneme distinctions betweenindividual consonant targets Where one strategy systematically aVected more thanone consonant target and these targets were phonologically related then that strategywas identi ed as a process a cleft-type phonological process For example backingusually aVected several alveolar targets t d n s z resulting in a backing pro-cess In this de nition alternative articulations include both non-English consonantrealizations eg s to [x] and alternative English consonants as in t backed to [k]
Figure 1 illustrates the nature of realizations involved in active processes As agroup they resemble but are not the same as Trostrsquos (1981) compensatory articula-tions In early speech attempts at several fricative target consonants might all berealized by a single realization for example s z S Z might be any of the followingnasal fricative [n
degk] post-oral glottal [h] or pharyngeal [Eacute] backed to uvular [X] or
to velar [x] lateral [Euml] palatal [c] A backing process aVecting production of [s]might also result in backing of both alveolar target plosive consonants eg t to
Active versus passive cleft-type speech characteristics 333
Figure 1 Active cleft-type processes
[k] and of nasal andor lateral alveolar target consonants n l to [Icirc] Whilst thesecharacteristics might as has been assumed in the past be pure articulatory errorsthere are phonological consequences (Grundy and Harding 1995) when severalclasses of consonants eg voiced and voiceless alveolar fricatives and alveolarplosives are realized by one consonant [g] resulting in multiple loss of phonologicalcontrasts or systematic sound preference (Grunwell 1985)
In viewing gure 1 it is worth noting that pharyngeal and glottal articulationare lsquonon-oralrsquo productions which do not require intra-oral pressure or velopharyngealclosure and their production would not evoke sphincteric movement A speakermust at least intend an oral production if potential velopharyngeal sphincter functionis to be accurately assessed Hence predominance of glottal and pharyngeal patternsof articulation imply but do not prove the existence of an inadequate sphincter
lsquoActiversquo processes which establish meaningful contrasts did not account for allthe cleft-type speech patterns observed in the data Consideration is now given tothe cleft-type realizations thought to be passive products of either structural defector dysfunction Hypernasal resonance co-occurring with passive patterns of articula-tion are frequently a direct consequence of weak or absent intra-oral pressure In apassive realization there is no alteration of the articulatory pattern for the intendedconsonant eg the bilabial b in ball is produced [m] [mO~] As shown by gure 2exclusively passive patterns of articulation employ few consonants (approximantsand nasals and glottal [h]) [m n Icirc w j l h] to represent all adult consonants Thisrange of consonants when associated with nasalized vowels suggests a lack ofpotential to establish intra-oral pressure for speech To date passive consequencesof the cleft on speech have received minimal attention perhaps because they donot involve non-English consonant realizations Lack of intra-oral pressure isassociated with hypernasal resonance and nasal emission (Kummer et al 1992)Nasal emission is perceived either accompanying or replacing voiceless pressureconsonant targets hence it will not be present until a child is actively targetingvoiceless pressure consonants (Sell et al 1994) Severely hypernasal speech may notevidence nasal emission until fricative targets are intended and realized as [(sk)n
deg]
for examplePassive processes which severely limit the range of consonants can impair
communication more than a combination of active processes Speech samples
A Harding and P Grunwell334
Figure 2 Passive cleft-type processes
containing active processes usually sound distinctive but communicative compet-ence can be impressive because more meaningful diVerences can be signalled thanmay be possible with the restricted phonetic repertoire of passive processes Giventhat the velopharyngeal sphincter is complex and dynamic it is possible for arestricted phonetic repertoire with hypernasal resonance to persist into early speechdevelopment because a child has been unable to achieve velopharyngeal functionfor speech after palate repair
The distinction between active and passive cleft-type processes has been integ-rated into the revised cleft palate speech assessment GOSSPASSrsquo98 (Sell et al1998) De nitions of cleft-type characteristics are given in GOSSPASSrsquo98 butGOSSPASS does not interpret the phonological consequences of the cleft-typecharacteristics The following de nitions of active and passive cleft-type processesare based on data analysis in the present study and on Harding and Grunwellrsquos(1996) characteristics of cleft palate speech Analysis of patterns of phonemeevolution throughout speech acquisition has generated a hierarchy of error-severityThe following descriptions of the diVerent types of processes are illustrated byreference to the data collected in the research studies (Harding 1993)
Active cleft type processes
Active nasal fricatives
[mdegk] [n
degk] [ Daggerk
deg] Nasal realizations of voiceless and sometimes voiced fricative targets
f v s z S Z were categorized as nasal fricatives Comparison of gures 1 and 2shows that nasal realizations occurred in both passive and active processes Inproduction of active nasal fricatives the pulmonary air is actively directed nasallyas an alternative articulation to an oral fricative realization Figure 3 illustrates thatoral air ow is stopped by either lips or tongue thus achieving 100 nasal air owThis strategy is developed in order to signal the fricative nature of intended targetfricative consonants In the active nasal fricative [m
degk] for f n
degk for s [n
degk O] for
lsquosorersquo [mdegk O] for lsquofourrsquo is the product of actively directed nasal air Where fricative
consonants are the only targets aVected by a cleft-type process the presence ofnasal fricatives have been referred to as phoneme speci c nasality (Trost-Cardamone
Active versus passive cleft-type speech characteristics 335
Figure 3 Active nasal fricative [ndegk]
1990) This characteristic has been found in speakers with no cleft palate historyoften with no explanation for its occurence
DiVerent places of articulation signalled placement contrasts between nasalfricative consonants in the same way that target nasal consonants [m n Icirc] arediVerentiated by place of articulation [m
degk] for f [n
degk] for s S Where a strong
backing process existed alveolar and post-alveolar fricatives were realized by velarnasal fricatives [ Daggerk
deg]
Occasionally nasal air ow was constricted such that nasal fricatives were pro-duced with a noisier turbulent quality [m
deg] [n
deg] [ Dagger] In a detailed assessment of cleft
pa la te speech GOSSPASSrsquo98 (Sell et al 1994 1998) these turbulent realizationswould be categorized in the resonance section as lsquonasal turbulence replacing conson-antsrsquo and in the cleft-type characteristics section as either lsquoactive nasal fricativesrsquo orpassive nasal realization of fricatives
Glottal articulation
[] frequently occurred in early plosive and aVricate production [p b t d T] up toage 46 Sometimes this process aVected only alveolar plosives t d in SIWI andSIWW position At times glottal stop represented voiced plosives [b d g] while[h] represented voiceless plosives [p t k] In SFWF position glottal stop representedboth voiced and voiceless plosives It may be the case that diVerent strengths ofglottal stop were used to distinguish voiceless and voiced plosives but this couldnot be reliably judged without spectographic analysis An undergraduate study ofspectographic analysis (Shorter 1995) of cleft palate speech identi ed some subtlediVerences in glottal stop productions which suggests a need for further investigationinto the phonological functions of glottal stops in cleft palate speech
Pharyngeal fricatives
[Eacute iquest] Early attempts at fricatives (ages 20ndash30) were frequently realized with acombination of posterior fricative cleft-type realizations (CTRs) Where plosiveswere exclusively glottal fricative consonants were frequently realized as pharyngeal
A Harding and P Grunwell336
fricatives In early phonological development obstruent realizations were commonlynon-oral but gradually moved anteriorly to uvular and velar positions Targetconsonants were not generally corrected independently of each other The gradualmovement of pharyngeal realizations towards oral uvularvelar articulation whichunderlines the relevance of a phonological interpretation of cleft palate speechcharacteristics
Exclusively pharyngealglottal patterns of articulation might imply velopharyn-geal insuYciency but it is noted here that all infants use pharyngeal and glottalarticulation until they acquire velopharyngeal competence during the rst 6 monthsof life It is possible for children with cleft palate to persist with this phoneticrepertoire for some time after palate repair Indeed such cases have been reportedby Russell and Grunwell (1993) Non-oral articulatory patterns indicate that thesphincter is not employed during speech which implies that the sphincter may notbe functional but unless oral air ow is consciously intended it cannot be assumedthat the sphincter is unable to function in speech (Henningsson and Isberg 1986)
Backing [k g q G]
A backing pattern is described by Stengelhofen (1989) as a lsquotendency for oralcontacts to be to the back of the oral cavityrsquo GOSSPASSrsquo98 (Sell et al 1998) makesa distinction here between backing to uvular and backing to velar place ofarticulation
E Backing to uvular [q G X Ograve ] Alveolar target consonants were backed touvular realizations and occasionally velar targets were backed to uvular Thepresence of velar and uvular realizations indicated the presence of some VPfunction but this might have been achieved with tongue humping In thedata acquisition of uvular and velar fricatives generally co-occurred withacquisition of f v which provides further evidence of velopharyngealfunction In the longitudinal study from age 16 to 46 subjects with bilateralclefts spent a period of months realizing all alveolar and post- alveolar voicedand voiceless consonant targets in uvular placement This degree of backingis deemed to be more severe and distracting for listeners than backing tovelar perhaps because uvular articulation is more distinctively non-EnglishHowever uvular fricatives are frequently used to achieve some meaningfulcontrasts which improve intelligibility
E Backing to velar In the younger subjects (aged 16ndash46) as articulatorypatterns progressed anteriorly a preference for [g] was common Mostcommonly backing resulted in t d realized as [k g] and s z as [x aring ]which contrasts with the fronting pattern seen in normal development
Double articulation
This is de ned as two simultaneous equal strictures at two places of articulationwhich was frequently noted in realizations of target alveolar consonants t d whenalveolarvelar contacts [tkk dkg] were used Double articulation may have beendeveloped to distinguish between alveolar and velar consonants in the presence ofa backing pattern Interestingly double articulation became evident in these develop-ing speech patterns with the emergence of fricative realizations Both plosives andfricatives tended to be realized with double articulation eg tndash[tkk] sndash[skagrave ]
Active versus passive cleft-type speech characteristics 337
Palatal fricatives [c J ]
These fricative realizations of alveolar target consonants appeared towards the endof the study period (ages 16ndash46) They were the most common realizations ofalveolar fricatives in older children (46ndash76 and 100ndash110) This nding was inaccordance with Alberyrsquos results (Albery 1991 Albery and Grunwell 1993)
Lateral fricatives [l Igrave]
As with palatal fricatives lateral fricatives were frequently present as realizations offricative consonant targets becoming particularly prevalent in later phonologicaldevelopment
Gliding of fricatives s S= [ j] or [w]
This phenomenon is seen in the non-cleft population as an uncommon develop-mental process (Grunwell 1987) It is classi ed here as an active process because[ j] was consistently produced as an apparently active alternative to target conson-ant(s) s z S [ j] is a normal consonant-like production in non-cleft babble whichcleft palate children often integrate into their phonological system It may betherefore that it is a persisting immaturity in the cleft palate population In thesedata [ j] was eVective in signalling a contrast between plosives and fricatives inSIWI position It functioned for the following consonants in diVerent speakers [ j]for S [ j] for m p f s z Ÿ h and co-articulation [hkj] for T
Passive cleft type processes
The criteria for passive cleft type processes is that they are (1) an attempt toproduce the correct articulatory placement and stricture (manner) which (2) failsbecause of a lack of intra-oral air pressure For example voiced plosives realized asnasals b[ [m] d[ [n] g[ [Icirc] No compensatory articulatory pattern hasbeen used to replace the intended consonant As the above examples demonstratetarget realizations often match a similar English consonant
Absence of pressure consonantspredominantly sonorant articulation
This phenomenon is de ned here as a pattern of articulation which was restrictedto English nasal and approximant articulations [m n Icirc w j] and [h] Some of thevoiced consonants were also employed as voiceless counterparts [m
degndeg Icircdeg ] thereby
increasing the range of available consonants for distribution in the phonologicalsystem Despite the limited consonant repertoire these patterns were often eVec-tively interpreted by close family members
Weak articulation [bV dV]
This category refers to normal articulatory movement in the production of obstruenttargets (plosive fricative and aVricate targets) which were produced with reducedoral air pressure and therefore articulation was considerably weakened In the speechsample data (ages 16ndash46) many target consonants were weakened to some degreeand at times may have been realised as nasals
A Harding and P Grunwell338
Passive nasal fricative [(fk)m (sk)ndeg]
Incomplete velopharyngeal closure inevitably reduces control of oral air ow with apassive loss of air ow and an increase of resonance in the nasal cavity Grunwelland Harding (1996) de ned the passively nasal fricative as an unreleased [(s)]double-articulated with a lowered voiceless nasal [n
Aacute
deg] This realization is the product
of an intended s with an unintended nasal air ow (see gure 4) The precisetranscription for a passive nasal transcription is [(sk)n
Aacute
deg] but an acceptable simpli cation
for transcription purposes is [(sk)ndeg] This is distinct from the active nasal fricative
which involves stopping of the oral air ow and active direction of air nasally whichcan be transcribed as a voiceless nasal with additional nasal emission [n
degk] Nasal
emission signals the fricative nature of for example target consonant s Thesetwo productions can sound the same and might initially be transcribed as [n
degk]
Nasendoscopic investigation of velopharyngeal activity during active and passivenasal realizations of s both show a lack of velopharyngeal closure It is predictedthat close examination by use of electropalatography might show slight diVerencesin tongue tip posture for an active and passive nasal fricative as illustrated in gures3 and 4 Passive nasal fricatives were converted into oral fricatives with nose-holding
Voiceless [h] for voiceless plosives
There was evidence that voiceless plosives were at times passively realized as [h]The consequence of reduced oral air pressure on production of voiceless plosivescan leave aspiration as the only perceptible distinctive feature This process usuallyaVected all voiceless plosive targets p t k Where this process was a passiveprocess use of noseholding during speech facilitated accurate target productionHowever it would also be possible for this distribution of [h] to be an active cleft-type process which would be part of a pharyngealglottal patternprocess
Nasal realization of voiced plosives b d g[ [m n Icirc]
Some subjects with residual clefts stulae or suspected VPI realized voiced conson-ants as nasal counterparts As summarized by Harding and Grunwell (1996) voiced
Figure 4 Passive nasal fricative [(sk)nAacute
deg]
Active versus passive cleft-type speech characteristics 339
consonants can be more diYcult to produce than voiceless consonants (Isshiki andRingel 1964) Distinction between active versus passive nasal realizations of plosivetargets was made in the same way that active and passive nasal fricatives weredistinguished by observing the eVect of noseholding on consonant production Inpassive nasal realizations noseholding facilitated normal consonant production(Golding-Kushner 1995)
Nasal emission accompanying consonants [pk sk]
Nasal emission was frequently heard accompanying consonants but on occasions itapparently replaced consonants It has been linked with velopharyngeal incompet-ence (VPI) (Kummer et al 1992)
Results
Comparison of activepassive processes in the speech data
Quantitative results of Hardingrsquos research into the relationship between timing ofsurgery and speech development have already been published (Harding andGrunwell 1993) The following interpretation of the data speci cally identi esactivepassive cleft-type processes in relation to oral structure in a wide age rangeof subjects (16ndash130) Tables 1 2 3 and 4 show the passive and active processeson the left-hand column and the subjectrsquos code along the top The code identi esthose subjects who were treated with 1-stage versus 2-stage surgery Comparisonof the 4 tables at age 46 (BCLP and UCLP) at age 90 and at age 130 illustratesa pattern of diminishing cleft-type processes with increasing age Irrespective ofsurgical timing few cleft-type processes remained at age 130 (table 4) A generalobservation was that earlier speech samples (ages 16ndash76) frequently combined
Table 1 Cleft-type processes in BCLP subjects at age 46 (studies 1 and 2)
1-stage surgery 2-stage surgery
A G Rf JW D B JF JG AB
Passive cleft-type processespredominantly sonorant articulation m
weak articulation m m m m m m m m
voiceless h for plosive m m m m m
nasal release of plosives m m m m m
nasal emission with consonants m m m m m m
passive nasal fricativeActive cleft-type processes
nasal fricatives m m m m m m m m
pharyngeal glottal articulation m m m m m m m m
backing to uvular m m m m m m m m
backing to velar m m m m m m m m m
lateral palatal fricatives m m m m m m m m m
double articulation m m m m m m m m m
gliding fricative m m
f=post-operative stula
A Harding and P Grunwell340
Table 2 Cleft-type processes in UCLP subjects at age 46 (study 2)
1-stage surgery 2-stage surgery
SE TB CK MS NC TS ZG CP
Passive cleft-type processespredominantly sonorant artic m
weak articulation m m m
voiceless h for plosives m m m
nasal release of plosives m m m
nasal emission with consonants m m
passive nasal fricative m m
Active cleft-type processesnasal fricativepharyngeal glottal articulation m m m
backing to uvular m
backing to velar m m
lateral palatal fricatives m m m m m
double articulation m m m m m m
gliding fricative m
Table 3 Cleft-type processes at age 90
2-stage surgery 2-stage surgery1-stage surgery completed at 4 yrs completed at 8 yrs
DAf SBf RL NR JD AR LJ RP MB
Passive cleft-type processespredominantly sonorant articweak articulation m
voiceless h for plosives m m
nasal release of plosives m m
nasal emission with consonants m m m m
passive nasal fricatives m m
Active cleft-type processesnasal fricatives m m
pharyngeal glottal articulation m m
backing to uvular m m
backing to velar m m m m m m m
lateral palatal fricatives m m m m m m m
double articulation m m m m m
gliding fricative m
f=subject had a stula
both active and passive strategies whereas later samples (ages 90ndash130) rarelyevidenced passive processes
At age 46 four out of ve BCLP subjects used active non-oral pharyngeal andglottal processes and oral velar and uvular fricatives irrespective of surgical status(see table 1) All had some anterior palatal defect which might have reduced theirpotential to achieve intra-oral pressure
By comparison two out of three partially repaired 2-stage UCLP subjects at age46 (table 2) showed evidence of passive processes This suggested that their
Active versus passive cleft-type speech characteristics 341
Tab
le4
Spee
chin
rela
tion
tosu
rgic
altim
ing
atag
e13
0
2-st
age
surg
ery
2-st
age
surg
ery
1-st
age
surg
ery
subj
ects
com
plet
edat
4yr
sco
mpl
eted
at8
yrs
1-A
1-B
1-C
1-D
1-E
1-F
24-
G2
4-H
24-
J2
8-K
28-
L2
8-M
Pass
ive
clef
t-ty
pepr
oces
ses
pred
omin
antly
sono
rant
artic
wea
kar
ticul
atio
nm
voic
eles
sh
fo
rpl
osiv
esna
sal
rele
ase
ofpl
osiv
esna
sal
emis
sion
with
cons
onan
tsm
pass
ive
nasa
lfr
icat
ives
Act
ive
clef
t-ty
pepr
oces
ses
nasa
lfr
icat
ives
phar
ynge
alg
lott
alar
ticul
atio
nba
ckin
gto
uvul
arba
ckin
gto
vela
rm
m
late
ral
pala
tal
fric
ativ
esm
mm
doub
lear
ticul
atio
ngl
idin
gfr
icat
ive
1=1-
stag
esu
rger
ysu
bjec
ts
24=
2-st
age
surg
ery
hard
pala
tere
pair
edat
abou
t4
yrs
28=
2-st
age
surg
ery
with
hard
pala
tere
pair
edat
abou
t8
yrs
A Harding and P Grunwell342
unrepaired hard palates had in fact restricted their phonetic repertoire imposing aneed for individual adaptability The additional active processes employed by thesesubjects were presumably a response to the restrictions imposed by their oro-nasalstructure and velopharyngeal function at the time of consonant acquisition Asshown in table 2 the most common active cleft-type processes persisting at age46 with a residual cleft of the hard palate were backing double articulation andlateralpalatal articulation Two 1-stage surgery subjects whose entire palates hadbeen repaired at ages 09 and 010 did not use any cleft-type processes at age 46
By age 90 (table 3) a much-diminished number of cleft type processes wasevident except in subjects with sizeable anterior stulae who had received littlespeech and language therapy A similarity was noted between the speech patternsof 1-stage surgery subjects with stulae (DA and SB) at age 90 (table 3) and theyounger BCLP subjects at age 46 (table 1) who also had anterior palatal defectsThey included non-oral realizations of t d s k g occasional nasal fricatives andpharyngealglottal articulations Fistulae had apparently continued to in uencearticulation and phonological development in these subjects
Finally at age 130 (table 4) the diVerences between 1-stage and 2-stage surgerysubjects had diminished leaving only one 2-stage subject with occasional backingand four subjects with slight palatal and lateral release of fricative consonants Onlytwo of the 1-stage surgery subjects were using minor distortions of grooved fricativeproduction
Whilst there were apparent trends in speech production relating to surgicaltiming and oral structure it is noted that there were exceptions to each tentativegeneralization Subjects with marked structural imperfections occasionally producedrealizations of which they would not have been thought capable and subjects withno visible imperfections produced inexplicably distorted speech patterns It istherefore concluded that whilst there is homogeneity in the range of processesproduced by this population assumptions cannot be made about speech based onsurgical timing or type of cleft Tentative predictions based on detailed assessmentmay be clinically very useful
EVects of surgery on speech
Activepassive processes have identi ed those cleft-type characteristics thought tobe associated with a physical inability to produce pressure consonants The followinganalysis of speech changes after surgical intervention at diVerent ages identi es thechanges eVected by surgery when intra-oral pressure could be more readily achieved
Two children were rst recorded prior to the rst stage of a 2-stage procedureTheir lips were repaired at approximately 6 months of age and soft palate repairwas carried out at ages 18 and 19 respectively Their hard palates were leftunrepaired to facilitate unrestricted growth of the mid-face (Hotz et al 1978) Pre-and post-operative consonant-like sounds present in the recorded speech samplesare listed in table 5 Interestingly prior to soft palate repair both these childrenproduced some oral consonants Subject B was producing pressure consonants [kg] in his babble prior to soft palate repair Considering that he had an unrepairedbilateral cleft palate at this point it was surprising that he had any oral consonantsPost-operatively at 20 years he used [b bkm t d g gkb] which indicated that surgeryto repair the soft palate had facilitated an increased range of oral pressure consonantsSubject D was producing [p b k g] pre-operatively Post-operatively following soft
Active versus passive cleft-type speech characteristics 343
Tab
le5
EV
ects
ofso
ftp
alat
ere
pair
atag
e1
6on
BC
LP
subj
ects
h
ard
pal
ate
rem
ain
sun
repa
ired
2-st
age
subj
ects
Surg
ery
Pre
-ope
rati
vesp
eech
patt
ern
atag
e1
6Po
st-o
pera
tive
chan
ges
insp
eech
atag
e2
0
Stud
y1
BSo
ftpa
late
repa
irat
16
Adu
ltta
rget
sk
gA
t2
0[b
b kmg kb
td
g]D
Soft
pala
tere
pair
17
Adu
ltta
rget
sp
bk
gA
t2
0[p
bd
b kdk
g]
Tab
le6
EV
ects
ofha
rdpa
late
rep
air
atag
e6
6an
d
stu
lare
pair
atag
e10
0
Subj
ect
Surg
ery
Pre
-ope
rati
vesp
eech
patt
ern
Post
-ope
rati
vech
ange
sin
spee
ch
MS
Har
dpa
late
repa
ir6
6Pa
ssiv
epr
oces
s7
6E
limin
ated
pass
ive
proc
ess
Var
iabl
ena
sal
rele
ase
ofco
nson
ants
Hyp
onas
alna
sals
JFH
ard
pala
tere
pair
(uns
ucce
ssfu
l)6
6Se
vera
lac
tive
and
pass
ive
proc
esse
s7
6A
ctiv
epr
oces
ses
rem
aine
dPa
ssiv
epr
oces
ses
elim
inat
ed
DA
Fis
tula
repa
ir10
0A
ctiv
epr
oces
ses
110
Elim
inat
ion
ofph
aryn
geal
glo
ttal
Var
iabi
lity+
+an
dna
sal
arti
cula
tion
Art
icul
ator
yva
riab
ility
++
Act
ive
CT
Rs
proc
esse
spe
rsis
t
A Harding and P Grunwell344
palate repair but with a residual cleft in the hard palate his range of consonantsincluded [d] which was particularly surprising since the hard palate remainedunrepaired Whilst it is unlikely that toddlers of 18 months could be consciouslytrying to compensate for articulatory inadequacy in producing velar plosives inbabble prior to soft palate repair and an alveolar plosive prior to hard palate repairboth these subjects showed evidence of actively pursuing their articulatory potential
Table 6 summarizes changes following surgery to repair the hard palate in moremature speech patterns These subjects who were aged 66 and 100 pre-operativelyhad learned to speak with residual clefts and were apparently unaware of theconsonant productions that failed to match normal production
Subject MS used only passive processes in his speech pattern He realized someconsonants nasally such that lsquoballrsquo was [mO~] and lsquosockrsquo was [(sk)n
deg Aacute~ k] Looking atpost-operative changes at age 76 his consonant production was normal but hisresonance had become hyponasal Pre-operatively at age 66 Subject JF was usingseveral active and passive processes The active processes were unaVected by surgerybut passive processes were eliminated
Fistula repair was carried out at age 100 on Subject DA who had many activeprocesses and very variable articulation pre-operatively Post-operatively at age110 he was not using non-oral pharyngeal and glottal active processes or nasalrealizations but many oral cleft-type realizations remained
As shown in table 7 hard palate re-repair and pharyngoplasty was carried outon two subjects whose hard palate repairs had been unsuccessful at approximately4 years Subject NC assessed pre-operatively at age 56 was using predominantlypassive processes in her speech She was also using [ j] for fricatives s S whichwas thought to be an active process At age 60 following hard palate re-repair andpharyngoplasty all cleft-type processes had been eliminated without post-operativespeech therapy Since [ j] for s apparently resolved spontaneously followingsurgery it can be assumed that this was a passive process in this speech sample
Subject CP who underwent this procedure presented pre-operatively at age 46with both passive and active processes but his nasal resonance was not consistentlyhypernasal In addition to his cleft-related speech disorder this subject had additionaldevelopmental speech diYculties which were identi ed as being unrelated to thecleft Post-operatively at age 56 little had changedmdashnotably the passive processnasal [m] for b was retained His nasal resonance had become hyponasal andthere was no apparent bene t from surgical intervention The realization of b as[m] had become phonologically stable and surgery alone had not destabilized thephonological system This realization may have been a passive product of VPI inearly speech acquisition which had subsequently become part of a phonologicaldisorder Post-operatively CPrsquos phonetic repertoire did increase but the phonologicaldistribution was variable Plosive targets were still realized as nasals in spontaneousspeech at the nal speech recording at age 76 This was not as an inevitableconsequence of VPI but a result of an inability to destabilize the phonologicalprocess determining that voiced plosives would be realized as nasals This resultfollowing surgery highlights the importance of identifying phonological learningproblems and distinguishing them from structural constraints on articulationIn CPrsquos case pre-operative exploration of the eVect of nares occlusion duringspeech might have indicated that structural change would not improve consonantproduction spontaneously
A general observation was that consonant realizations did not move rapidly
Active versus passive cleft-type speech characteristics 345
Tab
le7
EV
ects
ofha
rdpa
late
re-r
epai
ran
dp
hary
ngo
pla
sty
Subj
ect
Surg
ery
Pre
-ope
rati
vesp
eech
patt
ern
Post
-ope
rativ
ech
ange
sin
spee
ch
Stud
y2
NC
Har
dpa
late
re-r
epai
ran
d5
6Pa
ssiv
ecl
eft-
type
proc
esse
s6
0A
llcl
eft-
type
phar
yngo
plas
ty5
10[
j]
for
fric
ativ
espr
oces
ses
elim
inat
ed[
h]
for
plos
ives
SIW
IV
aria
ble
arti
cula
rypr
ecis
ion
CP
Har
dpa
late
repa
iran
d4
6Pa
ssiv
ean
dac
tive
proc
esse
s5
6Pa
ssiv
epr
oces
sph
aryn
gopl
asty
50
Pho
nolo
gica
lco
nfus
ion
[m]
for
[b
]re
tain
edH
ypon
asal
nasa
lsPe
rsis
ting
phon
olog
ical
conf
usio
ns
A Harding and P Grunwell346
from incorrect to correct but progressed incrementally towards normal realizationsas described by Morley (1970) Where an early realization of target s might beglottal [h] a gradual pattern of change showed subsequent realizations to bepharyngeal [Eacute] then uvular [X] then velar [x] and eventually palatal [c] or lateral [Euml]It was interesting to note that speech patterns continued to change as late as90ndash110 years with the result that diVerences related to surgical timing and cleft-type gradually disappeared Persisting stulae were thought to account for the mostmarked cleft type processes at age 90
Implications for surgical management
This analysis of speech changes following surgery suggests some implications forsurgical management which are compatible with Sell and Grunwellrsquos (1990) ndingsin the Sri Lankan study
Surgery can change passive speech processes but it is also possible that speechtherapy may be able to change passive patterns Surgery alone is unlikely to modifyactive cleft-type processes whereas speech therapy should be able to modify activeprocesses Indications from these case studies is that where speech is the primaryproblem speech assessment should distinguish between active and passive processesin order to evaluate the necessity for full investigations and to plan therapeuticintervention Where past speech therapy has not been successful it cannot beassumed that surgical intervention will facilitate further speech progress A furthercourse of speech therapy which is sensitive to active versus passive processes todevelopmental phonological in uences on cleft-type speech development and toarticulatory diYculties in diVerent speech contexts might facilitate optimal progressWhere structural imperfection exists it is quite possible for single-word productionto be more precise than target realizations in spontaneous speech This may not bea failure of phonological generalization (Grunwell 1992) but the result of diYcultysustaining the necessary lsquoarticulatory eVort rsquo (Harding and Grunwell 1993) resultingin articulatory imprecision Deteriorating articulatory accuracy should not be over-looked in interpretation of speech results
An analytical protocol
As a result of analysing the speech data and identifying the active and passiveprocesses a protocol has been developed which records examples of each cleft-typeprocess over a series of assessments It demonstrates the progression of individualprocesses towards an adult target (see the Appendix) At each assessment onecolumn is used to indicate nasal resonance nasal emission and nasal turbulenceratings and cleft-type processes Changes in the nature of error realizations mightshow progress towards target consonants Hence whilst the total correct scoremight not have increased increments of change can be observed This observationof patterns of change may function as an adjunct to GOSSPASSrsquo98 (Sell et al 1998)giving access to a greater depth of both quantitative and qualitative data aboutconsonant production in relation to resonance nasal emission nasal turbulenceoral structure and cleft-type
Active versus passive cleft-type speech characteristics 347
Diagnostic implications
Passive versus active nasal fricatives
The important management consideration related to this distinction is that an activenasal fricative is an established phonological process which is unlikely to be directlyaVected by surgery alone Therapy would be necessary to destabilize nasal realizationsof oral consonants In contrast passive nasal fricatives may be eliminated by surgeryOf particular relevance is diVerential diagnosis between passive and active nasalfricatives in surgical and therapeutic management When hypernasality co-occurswith nasal air ow during consonant production which can be redirected by nose-holding passive nasal fricatives are diagnosed These would be transcribed as [(sk)n
deg]
passive alveolar nasal fricatives [(Wk)mdeg
] bilabial nasal fricatives or [(fk)Iacutedeg ] labiodentalnasal fricatives Full VPI investigations would be recommended to diagnose thenature of the structural or functional de ciency and distinguish between velopharyn-geal incompetence and velopharyngeal mislearning
It is highly likely that plosive targets would be aVected by reduced intra-oral airpressure such that plosives would either be realized by nasal counterparts eg bd[ [m n] or [b d] may be nasalized and weak Voiceless plosives may be eitheraccompanied by nasal emission [p t k] or realized as glottal fricative [h]
Production of the target sentence lsquoI saw Sam sitting on a busrsquo might be
[aI (sk)ndeg O~ (sk)n
degaelig~m (sk)n
deg IhIn Aacute~n mouml~(sk)ndeg] passive processes and
[aI xO xaeligm xIkIIcirc AacuteIcirc goumlx] active processes
Contribution to surgical management decisions
Passiveactive interpretation of clinical assessments might facilitate surgical manage-ment decisions If noseholding does not facilitate correct production of targetconsonants then it is likely that an alternative articulatory pattern has becomephonologically established ie particular realizations for one or more targets areconsistently distributed in the phonological system These realizations may haveevolved because of initial diYculty producing articulatory targets and subsequentlystabilized within the phonological system Grundy and Harding (1995) refer to thisphenomenon as an lsquoarticulatory disorder with phonological consequencesrsquo
Therapy
Where obvious structural defects or diagnosed dysfunction exists clinicians fre-quently defer therapeutic intervention until surgery has been undertaken Theexpectation would be that normal structure and function is essential for normalspeech However pre-operative therapy may facilitate oral consonant productionwhich may serve to reduce hypernasal resonance Hence therapy prior to surgerymay avoid unnecessary surgery or reduce the extent of surgery required All activeprocesses are likely to require therapy
Principled selection of targets for therapy
Speech patterns frequently evidence a mixture of apparently passive and activeprocesses which complicates decisions about target selection Target selection can
A Harding and P Grunwell348
be based on assessment of which consonant targets can be most easily elicted inisolation (stimulability) This may lead to a sequence of target selection which isopposite to the sequence of consonant acquisition in normal development Forexample where reduced intra-oral pressure is present in a passive pattern [T] maybe easier to elicit in imitation than more nely grooved [s] or [S] Therapy maytarget [T] followed by [S ] and nally [s] As in non-cleft phonological therapywhere a class of consonants is aVected by the cleft then it is helpful to target theentire class The following decision-making process can be applied for both activeand passive processes
Decision making procedure for target selection
(1) Voiced versus voiceless targets(2) Front versus back placements(3) Syllable initial versus syllable nal targets(4) Plosives versus fricative targets
Voiceless plosives and fricatives are produced with an open glottis whichfacilitates topping up of air ow from the lungs hence voiceless plosive and fricativetargets are frequently more successful than voiced counterparts (Isshiki and Ringel1964) Front targets usually cause more diYculty than back particularly where analveolar defect or stula exists Contrary to normal development back targets maybe targeted before front Word- nal targets generally require less oral air pressurethan word initial targets and similarly fricatives may be more easily elicited thanplosives Fricatives do require a greater volume of air than plosives (Fletcher 1985)but in the presence of nasal escape weak fricative production appears to be morereadily achieved than weak plosive production Since nal fricatives would normallybe acquired in advance of word-initial fricatives (Ferguson 1978) targeting word- nal fricatives is frequently a productive starting point for therapy
Principles of therapy for passive processes
(1) Use of soft attack similar to gentle whisper for all target models ensuresminimal articulatory eVort (Harding and Grunwell 1993) and requires min-imal intra-oral air pressure It may be appropriate to gradually increase thearticulatory attack when the articulatory posture and evidence of intendedoral air ow have been established
(2) Slightly stretched duration of segment transitions in models of consonantto vowel (CndashV) or vowel to consonant (VndashC) facilitates review of motorplanning and extends the available time for execution of the new motorprogrammer whilst maintaining control of the oral airstream
(3) Noseholding can be used to provide exclusively oral air ow Gradual releaseof the nostrils during production of sustained [VVVVVf ] or [hhhhh ] allowsthe child to attempt to sustain an oral consonant despite increasing nasalemission This maximizes the use of available oral air ow Procedures forusing noseholding are described in some detail by Golding-Kushner (1995)
Principles of therapy for active processes
This is more like phonological therapy and can follow Grunwellrsquos (1991) processesfor phonological change and principled decision-making (Grunwell 1992) Some
Active versus passive cleft-type speech characteristics 349
examples are given here by way of illustration of ways to eVect the rst twoprocesses of change which may need to be approached diVerently in cleft palateversus non-cleft speech disorders DiVerent approaches may also be appropriate formodifying active versus passive cleft-type processes
Innovation production of new targets Some useful principles
(1) Introduction of new lsquonon-speech likersquo targets in sound play using a conson-ant sound segment model such as [ph ] note not a syllable like [p] whichis the type of pronunciation used when target sounds are presented as lettersfor reading Target [s] might be introduced as a lsquoTrain Slowing Down Noisersquo[ts ts ts tssssssss]
(2) lsquoNew consonantsrsquo can later be modelled and elicited in soft productions ofsyllable structure [tssssndashi] [ indashtssss] which can subsequently be identi ed assimilar to words lsquosearsquo and lsquoeatsrsquo
(3) lsquoDeferring responsibilityrsquo transfers responsibility or lsquoblamersquo for errors fromthe child and attributes it to the articulators eg lsquoyour tongue is havingtrouble with hellip rsquo lsquoLetrsquos show your tongue how to hellip rsquo
(4) New targets can be modelled repeatedly and recorded on audio or videotape which can be listened to at home
(5) Targeting classes of consonants (eg alveolars t d s n l voiceless fricativesf s S perhaps with aVricate T avoids phonological confusion whichmight occur if production ofsis achieved whilst other alveolar targetsremain backed The risk is that s might not integrate into the phonologicalsystem unless all backed alveolar consonants are destabilized
(6) Increased eye contact during auditory and production work can be invaluablein holding visual and auditory attention and ensures that visual informationabout the sound has been processed This is easily achieved by the clinicianlifting any focus of the childrsquos attention close to hisher mouth at theprecise moment when the target is modelled
Stimulation of non-speech related sounds such as a lsquoTrain Slowing DownNoisersquo [ts ts tsss] con rms that target [s] is physically achievable whether or not[ssss] can be imitated Some children continue to access [s] through the lsquoTrainSlowing Down Noisersquo throughout therapy until it is occurring spontaneouslywithout conscious planning This can be an eVective means of underminingestablished motor programmers (Hewlett 1990) for active cleft-type processes
Destabilizing active processes
As it is likely that children will be unaware of each occurrence of their alternativearticulatory pattern for speci c consonant errors it is preferrable to destabilizeactive processes with minimal conscious eVort by the child As children becomeaware of their mismatches they frequently add the newly acquired target realizationto their existing production eg target word tu childrsquos old realization [ku] childrsquoscorrected realization [t-ku] Destabilization can be achieved with minimal consciouseVort through input therapy techniques such as auditory bombardment (Lancasterand Pope 1989) auditory decision-making such as lsquowhich bear says this wordproperlyrsquo Red Bear says lsquotworsquo or Blue Bear says lsquocoorsquo This type of strategy oftenprecipitates attention to the target consonant with possible lsquoreplayrsquo and lsquoreviewrsquo of
A Harding and P Grunwell350
their own production Frequent stimulation of cognitive alertness to the targetconsonant can develop awareness without confronting the child with errors orrisking hisher failure The child is then free to attempt to repair hisher ownrealization to continue to re ect and to silently rehearse the adult realizationTraditional articulation therapy is thus combined with development of metaphonol-ogical skills ie the ability to re ect upon onersquos own speech production The resultshould be that new target realizations will be more phonologically stable thanexclusively production-based articulation therapy might have facilitated
Stabilizationgeneralization
Procedures to ensure stabilization and generalization of new target consonantswould be as described by Grunwell (1992) Success may be constrained by theconsiderable articulatory eVort sometimes required to maintain pressure consonantproduction in spontaneous speech (Harding and Grunwell 1993)
Conclusions
In speech assessment it is helpful to distinguish between errors which are cleft-type and non-cleft type and those which are part of active versus passive processesThe active and passive processes have been de ned and their phonological implica-tions discussed Focus on active and passive processes has facilitated focus on thephonological consequences of cleft palate on speech development In the futureawareness of the likely eVect of a cleft palate on normal phonological developmentcould avoid extended periods of unsuccessful clinical intervention Furthermoresensitivity to the relationship between phonological processes and structural con-straints should facilitate theoretically based management decisions Incidences suchas the case of CP in which nasal realizations were thought to indicate VPI but weresubsequently unaVected by surgery might be avoided if phonological analysiscontributes to management decisions
Surgery did improve hypernasal resonance and eliminated passive processes buthad little eVect on active processes Active processes in younger subjects werethought to require therapeutic intervention but in the longer term the oldersubjects showed few cleft-type processes Whilst it is possible that active cleft-typeprocesses may resolve with increasing age the implication for the future is thatactive cleft-type processes should be treated with skilled therapeutic interventionnot surgery Therapy which addresses the phonological consequences of cleft palateon speech development by combining metaphonologicalphonologicalarticulatoryapproaches is likely to be successful
References
Albery E 1991 Consonant articulation in the diVerent types of cleft lip and palate UnpublishedMPhil thesis Leicester Polytechnic
Albery E and Grunwell P 1993 Consonant articulation in diVerent types of cleft palate InP Grunwell (Ed) Analysing Cleft Palate Speech (London Whurr)
Ferguson C A 1978 Fricatives in child language acquisition In V Honsa and M Hardmann-Battista (Eds) Papers on Linguistics and Child Language (Mouton The Hague)
Fletcher S G 1985 Speech production and oral motor skill in an adult with an unrepaired palatalcleft Journal of Speech and Hearing Disorders 50 254ndash261
Active versus passive cleft-type speech characteristics 351
Golding-Kushner K J 1995 Treatment of articulation and resonancne disorders associated withcleft palate management and VPI In R Shprintzen (Ed) Cleft Palate Speech Management AMultidisciplinary Approach (St Louis Mosby)
Grundy K and Harding A 1995 Developmental speech disorders In K Grundy (Ed) Linguisticsin Clinical Practice (2nd edition) (London Whurr)
Grunwell P 1985 Phonological Assessment of Child Speech (Windsor NFER-Nelson)Grunwell P 1987a Clinical Phonology (2nd edition) (London Croom Helm)Grunwell P 1987b PACS Pictures Language Elicitation Materials (Windsor NFER-Nelson)Grunwell P 1991 Processes of phonological change in developmental speech disorders Clinical
Linguistics and Phonetics 6 101ndash122Grunwell P 1992 Principled decision making in the remediation of children with phonological
disorders In P Fletcher and D Hall (Eds) Specic Speech and Language Disorders in Children(London Whurr)
Grunwell P and Harding A 1995 PACSTOYS A Screening Assessment of Phonological Development(Windsor NFER-Nelson)
Grunwell P and Harding A 1996 A note on describing types of nasality Clinical Linguistics andPhonetics 10 157ndash161
Harding A 1993 An Investigation into the Relationship Between Timing of Cleft Palate Repairand Speech Development Unpublished PhD thesis
Harding A and Grunwell P 1993 The relationship between speech and timing of hard palaterepair In P Grunwell (Ed) Analysisng Cleft Palate Speech (London Whurr)
Harding A and Grunwell P 1996 Characteristics of cleft palate speech European Journal ofDisorders of Communication 31 331ndash358
Henningsson G and Isberg A M 1986 Velopharyngeal movement patterns in patients alternatingbetween oral and glottal articulation A clinical and cineradiographicical study Cleft Palate Journal23 1ndash9
Hewlett N 1990 Processes of development and production In P Grunwell (Ed) DevelopmentalSpeech Disorders (Edinburgh Churchill Livingstone)
Hotz M M Gnoinski W M Nussbaumer H and Kistler E 1978 Early orthopaedics in CLPcases guidelines for surgery Cleft Palate Journal 15 405ndash411
Hutters B and Brondsted K 1987 Strategies in cleft palate with special reference to DanishCleft Palate Journal 24 127ndash136
Isshiki N and Ringel R 1964 Airow during the production of selected consonants Journal ofSpeech and Hearing Research 7 233ndash244
Kummer A W Curtis C Wiggs M Lee L and Strife J L 1992 Comparison of velopharyngealgap size in patients with hypernasality hypernasality with nasal emission and nasal emissionor nasal turbulence (rustle) as the primary speech characteristic Cleft-palate-Craniofacial Journal29 152ndash156
Lancaster G and Pope L 1989 Working with Childrenrsquos Phonology (Oxford Winslow)Morley M E 1970 Cleft Palate and Speech (7th edition) (Edinburgh Churchill Livingstone)Russell V J 1991 Speech Development in Children with Cleft Lip and Palate Unpublished PhD
thesis Leicester PolytechnicRussell V J and Grunwell P 1993 Speech development in children with cleft lip and palate In
P Grunwell (Ed) Analysing Cleft Palate Speech (London Whurr)Sell D A and Grunwell P 1990 Speech results following late palatal surgery in previously
unoperated Sri Lankan adolescents with cleft palate Cleft Palate Journal 27 162ndash168Sell D Harding A and Grunwell P 1994 GOSSPASS A screening assessment of cleft palate
speech European Journal of Disorders of Communication 29 1ndash15Sell D Harding A and Grunwell P 1998 GOSSPASSrsquo98 An assessment for speech disorders
associated with cleft palate andor velopharyngeal dysfunction International Journal of Languageamp Communication Disorders ( in press)
Shorter E 1995 A spectographic analyis of child homophones Unpublished honours project DeMontfort University Leicester
Stenglehoffen J 1989 Nature and causes of communication diYculties In J Stengelhofen (Ed)Cleft Palate Nature and Remediation of Communication Problems (Edinburgh Churchill Livingstone)
Trost J E 1981 Articulatory additions to the classical description of the speech of persons withcleft palate Cleft Palate Journal 18
Trost-Cardamone J E 1990 The development of speech assessing cleft palate misarticulationsIn D A Kernahan and S N Rosenstein (Eds) Cleft Lip and Palate A System of Management(Baltimore Williams amp Wilkins)
A Harding and P Grunwell352
Appendix Active passive analysis of cleft palate speech

Active versus passive cleft-type speech characteristics 333
Figure 1 Active cleft-type processes
[k] and of nasal andor lateral alveolar target consonants n l to [Icirc] Whilst thesecharacteristics might as has been assumed in the past be pure articulatory errorsthere are phonological consequences (Grundy and Harding 1995) when severalclasses of consonants eg voiced and voiceless alveolar fricatives and alveolarplosives are realized by one consonant [g] resulting in multiple loss of phonologicalcontrasts or systematic sound preference (Grunwell 1985)
In viewing gure 1 it is worth noting that pharyngeal and glottal articulationare lsquonon-oralrsquo productions which do not require intra-oral pressure or velopharyngealclosure and their production would not evoke sphincteric movement A speakermust at least intend an oral production if potential velopharyngeal sphincter functionis to be accurately assessed Hence predominance of glottal and pharyngeal patternsof articulation imply but do not prove the existence of an inadequate sphincter
lsquoActiversquo processes which establish meaningful contrasts did not account for allthe cleft-type speech patterns observed in the data Consideration is now given tothe cleft-type realizations thought to be passive products of either structural defector dysfunction Hypernasal resonance co-occurring with passive patterns of articula-tion are frequently a direct consequence of weak or absent intra-oral pressure In apassive realization there is no alteration of the articulatory pattern for the intendedconsonant eg the bilabial b in ball is produced [m] [mO~] As shown by gure 2exclusively passive patterns of articulation employ few consonants (approximantsand nasals and glottal [h]) [m n Icirc w j l h] to represent all adult consonants Thisrange of consonants when associated with nasalized vowels suggests a lack ofpotential to establish intra-oral pressure for speech To date passive consequencesof the cleft on speech have received minimal attention perhaps because they donot involve non-English consonant realizations Lack of intra-oral pressure isassociated with hypernasal resonance and nasal emission (Kummer et al 1992)Nasal emission is perceived either accompanying or replacing voiceless pressureconsonant targets hence it will not be present until a child is actively targetingvoiceless pressure consonants (Sell et al 1994) Severely hypernasal speech may notevidence nasal emission until fricative targets are intended and realized as [(sk)n
deg]
for examplePassive processes which severely limit the range of consonants can impair
communication more than a combination of active processes Speech samples
A Harding and P Grunwell334
Figure 2 Passive cleft-type processes
containing active processes usually sound distinctive but communicative compet-ence can be impressive because more meaningful diVerences can be signalled thanmay be possible with the restricted phonetic repertoire of passive processes Giventhat the velopharyngeal sphincter is complex and dynamic it is possible for arestricted phonetic repertoire with hypernasal resonance to persist into early speechdevelopment because a child has been unable to achieve velopharyngeal functionfor speech after palate repair
The distinction between active and passive cleft-type processes has been integ-rated into the revised cleft palate speech assessment GOSSPASSrsquo98 (Sell et al1998) De nitions of cleft-type characteristics are given in GOSSPASSrsquo98 butGOSSPASS does not interpret the phonological consequences of the cleft-typecharacteristics The following de nitions of active and passive cleft-type processesare based on data analysis in the present study and on Harding and Grunwellrsquos(1996) characteristics of cleft palate speech Analysis of patterns of phonemeevolution throughout speech acquisition has generated a hierarchy of error-severityThe following descriptions of the diVerent types of processes are illustrated byreference to the data collected in the research studies (Harding 1993)
Active cleft type processes
Active nasal fricatives
[mdegk] [n
degk] [ Daggerk
deg] Nasal realizations of voiceless and sometimes voiced fricative targets
f v s z S Z were categorized as nasal fricatives Comparison of gures 1 and 2shows that nasal realizations occurred in both passive and active processes Inproduction of active nasal fricatives the pulmonary air is actively directed nasallyas an alternative articulation to an oral fricative realization Figure 3 illustrates thatoral air ow is stopped by either lips or tongue thus achieving 100 nasal air owThis strategy is developed in order to signal the fricative nature of intended targetfricative consonants In the active nasal fricative [m
degk] for f n
degk for s [n
degk O] for
lsquosorersquo [mdegk O] for lsquofourrsquo is the product of actively directed nasal air Where fricative
consonants are the only targets aVected by a cleft-type process the presence ofnasal fricatives have been referred to as phoneme speci c nasality (Trost-Cardamone
Active versus passive cleft-type speech characteristics 335
Figure 3 Active nasal fricative [ndegk]
1990) This characteristic has been found in speakers with no cleft palate historyoften with no explanation for its occurence
DiVerent places of articulation signalled placement contrasts between nasalfricative consonants in the same way that target nasal consonants [m n Icirc] arediVerentiated by place of articulation [m
degk] for f [n
degk] for s S Where a strong
backing process existed alveolar and post-alveolar fricatives were realized by velarnasal fricatives [ Daggerk
deg]
Occasionally nasal air ow was constricted such that nasal fricatives were pro-duced with a noisier turbulent quality [m
deg] [n
deg] [ Dagger] In a detailed assessment of cleft
pa la te speech GOSSPASSrsquo98 (Sell et al 1994 1998) these turbulent realizationswould be categorized in the resonance section as lsquonasal turbulence replacing conson-antsrsquo and in the cleft-type characteristics section as either lsquoactive nasal fricativesrsquo orpassive nasal realization of fricatives
Glottal articulation
[] frequently occurred in early plosive and aVricate production [p b t d T] up toage 46 Sometimes this process aVected only alveolar plosives t d in SIWI andSIWW position At times glottal stop represented voiced plosives [b d g] while[h] represented voiceless plosives [p t k] In SFWF position glottal stop representedboth voiced and voiceless plosives It may be the case that diVerent strengths ofglottal stop were used to distinguish voiceless and voiced plosives but this couldnot be reliably judged without spectographic analysis An undergraduate study ofspectographic analysis (Shorter 1995) of cleft palate speech identi ed some subtlediVerences in glottal stop productions which suggests a need for further investigationinto the phonological functions of glottal stops in cleft palate speech
Pharyngeal fricatives
[Eacute iquest] Early attempts at fricatives (ages 20ndash30) were frequently realized with acombination of posterior fricative cleft-type realizations (CTRs) Where plosiveswere exclusively glottal fricative consonants were frequently realized as pharyngeal
A Harding and P Grunwell336
fricatives In early phonological development obstruent realizations were commonlynon-oral but gradually moved anteriorly to uvular and velar positions Targetconsonants were not generally corrected independently of each other The gradualmovement of pharyngeal realizations towards oral uvularvelar articulation whichunderlines the relevance of a phonological interpretation of cleft palate speechcharacteristics
Exclusively pharyngealglottal patterns of articulation might imply velopharyn-geal insuYciency but it is noted here that all infants use pharyngeal and glottalarticulation until they acquire velopharyngeal competence during the rst 6 monthsof life It is possible for children with cleft palate to persist with this phoneticrepertoire for some time after palate repair Indeed such cases have been reportedby Russell and Grunwell (1993) Non-oral articulatory patterns indicate that thesphincter is not employed during speech which implies that the sphincter may notbe functional but unless oral air ow is consciously intended it cannot be assumedthat the sphincter is unable to function in speech (Henningsson and Isberg 1986)
Backing [k g q G]
A backing pattern is described by Stengelhofen (1989) as a lsquotendency for oralcontacts to be to the back of the oral cavityrsquo GOSSPASSrsquo98 (Sell et al 1998) makesa distinction here between backing to uvular and backing to velar place ofarticulation
E Backing to uvular [q G X Ograve ] Alveolar target consonants were backed touvular realizations and occasionally velar targets were backed to uvular Thepresence of velar and uvular realizations indicated the presence of some VPfunction but this might have been achieved with tongue humping In thedata acquisition of uvular and velar fricatives generally co-occurred withacquisition of f v which provides further evidence of velopharyngealfunction In the longitudinal study from age 16 to 46 subjects with bilateralclefts spent a period of months realizing all alveolar and post- alveolar voicedand voiceless consonant targets in uvular placement This degree of backingis deemed to be more severe and distracting for listeners than backing tovelar perhaps because uvular articulation is more distinctively non-EnglishHowever uvular fricatives are frequently used to achieve some meaningfulcontrasts which improve intelligibility
E Backing to velar In the younger subjects (aged 16ndash46) as articulatorypatterns progressed anteriorly a preference for [g] was common Mostcommonly backing resulted in t d realized as [k g] and s z as [x aring ]which contrasts with the fronting pattern seen in normal development
Double articulation
This is de ned as two simultaneous equal strictures at two places of articulationwhich was frequently noted in realizations of target alveolar consonants t d whenalveolarvelar contacts [tkk dkg] were used Double articulation may have beendeveloped to distinguish between alveolar and velar consonants in the presence ofa backing pattern Interestingly double articulation became evident in these develop-ing speech patterns with the emergence of fricative realizations Both plosives andfricatives tended to be realized with double articulation eg tndash[tkk] sndash[skagrave ]
Active versus passive cleft-type speech characteristics 337
Palatal fricatives [c J ]
These fricative realizations of alveolar target consonants appeared towards the endof the study period (ages 16ndash46) They were the most common realizations ofalveolar fricatives in older children (46ndash76 and 100ndash110) This nding was inaccordance with Alberyrsquos results (Albery 1991 Albery and Grunwell 1993)
Lateral fricatives [l Igrave]
As with palatal fricatives lateral fricatives were frequently present as realizations offricative consonant targets becoming particularly prevalent in later phonologicaldevelopment
Gliding of fricatives s S= [ j] or [w]
This phenomenon is seen in the non-cleft population as an uncommon develop-mental process (Grunwell 1987) It is classi ed here as an active process because[ j] was consistently produced as an apparently active alternative to target conson-ant(s) s z S [ j] is a normal consonant-like production in non-cleft babble whichcleft palate children often integrate into their phonological system It may betherefore that it is a persisting immaturity in the cleft palate population In thesedata [ j] was eVective in signalling a contrast between plosives and fricatives inSIWI position It functioned for the following consonants in diVerent speakers [ j]for S [ j] for m p f s z Ÿ h and co-articulation [hkj] for T
Passive cleft type processes
The criteria for passive cleft type processes is that they are (1) an attempt toproduce the correct articulatory placement and stricture (manner) which (2) failsbecause of a lack of intra-oral air pressure For example voiced plosives realized asnasals b[ [m] d[ [n] g[ [Icirc] No compensatory articulatory pattern hasbeen used to replace the intended consonant As the above examples demonstratetarget realizations often match a similar English consonant
Absence of pressure consonantspredominantly sonorant articulation
This phenomenon is de ned here as a pattern of articulation which was restrictedto English nasal and approximant articulations [m n Icirc w j] and [h] Some of thevoiced consonants were also employed as voiceless counterparts [m
degndeg Icircdeg ] thereby
increasing the range of available consonants for distribution in the phonologicalsystem Despite the limited consonant repertoire these patterns were often eVec-tively interpreted by close family members
Weak articulation [bV dV]
This category refers to normal articulatory movement in the production of obstruenttargets (plosive fricative and aVricate targets) which were produced with reducedoral air pressure and therefore articulation was considerably weakened In the speechsample data (ages 16ndash46) many target consonants were weakened to some degreeand at times may have been realised as nasals
A Harding and P Grunwell338
Passive nasal fricative [(fk)m (sk)ndeg]
Incomplete velopharyngeal closure inevitably reduces control of oral air ow with apassive loss of air ow and an increase of resonance in the nasal cavity Grunwelland Harding (1996) de ned the passively nasal fricative as an unreleased [(s)]double-articulated with a lowered voiceless nasal [n
Aacute
deg] This realization is the product
of an intended s with an unintended nasal air ow (see gure 4) The precisetranscription for a passive nasal transcription is [(sk)n
Aacute
deg] but an acceptable simpli cation
for transcription purposes is [(sk)ndeg] This is distinct from the active nasal fricative
which involves stopping of the oral air ow and active direction of air nasally whichcan be transcribed as a voiceless nasal with additional nasal emission [n
degk] Nasal
emission signals the fricative nature of for example target consonant s Thesetwo productions can sound the same and might initially be transcribed as [n
degk]
Nasendoscopic investigation of velopharyngeal activity during active and passivenasal realizations of s both show a lack of velopharyngeal closure It is predictedthat close examination by use of electropalatography might show slight diVerencesin tongue tip posture for an active and passive nasal fricative as illustrated in gures3 and 4 Passive nasal fricatives were converted into oral fricatives with nose-holding
Voiceless [h] for voiceless plosives
There was evidence that voiceless plosives were at times passively realized as [h]The consequence of reduced oral air pressure on production of voiceless plosivescan leave aspiration as the only perceptible distinctive feature This process usuallyaVected all voiceless plosive targets p t k Where this process was a passiveprocess use of noseholding during speech facilitated accurate target productionHowever it would also be possible for this distribution of [h] to be an active cleft-type process which would be part of a pharyngealglottal patternprocess
Nasal realization of voiced plosives b d g[ [m n Icirc]
Some subjects with residual clefts stulae or suspected VPI realized voiced conson-ants as nasal counterparts As summarized by Harding and Grunwell (1996) voiced
Figure 4 Passive nasal fricative [(sk)nAacute
deg]
Active versus passive cleft-type speech characteristics 339
consonants can be more diYcult to produce than voiceless consonants (Isshiki andRingel 1964) Distinction between active versus passive nasal realizations of plosivetargets was made in the same way that active and passive nasal fricatives weredistinguished by observing the eVect of noseholding on consonant production Inpassive nasal realizations noseholding facilitated normal consonant production(Golding-Kushner 1995)
Nasal emission accompanying consonants [pk sk]
Nasal emission was frequently heard accompanying consonants but on occasions itapparently replaced consonants It has been linked with velopharyngeal incompet-ence (VPI) (Kummer et al 1992)
Results
Comparison of activepassive processes in the speech data
Quantitative results of Hardingrsquos research into the relationship between timing ofsurgery and speech development have already been published (Harding andGrunwell 1993) The following interpretation of the data speci cally identi esactivepassive cleft-type processes in relation to oral structure in a wide age rangeof subjects (16ndash130) Tables 1 2 3 and 4 show the passive and active processeson the left-hand column and the subjectrsquos code along the top The code identi esthose subjects who were treated with 1-stage versus 2-stage surgery Comparisonof the 4 tables at age 46 (BCLP and UCLP) at age 90 and at age 130 illustratesa pattern of diminishing cleft-type processes with increasing age Irrespective ofsurgical timing few cleft-type processes remained at age 130 (table 4) A generalobservation was that earlier speech samples (ages 16ndash76) frequently combined
Table 1 Cleft-type processes in BCLP subjects at age 46 (studies 1 and 2)
1-stage surgery 2-stage surgery
A G Rf JW D B JF JG AB
Passive cleft-type processespredominantly sonorant articulation m
weak articulation m m m m m m m m
voiceless h for plosive m m m m m
nasal release of plosives m m m m m
nasal emission with consonants m m m m m m
passive nasal fricativeActive cleft-type processes
nasal fricatives m m m m m m m m
pharyngeal glottal articulation m m m m m m m m
backing to uvular m m m m m m m m
backing to velar m m m m m m m m m
lateral palatal fricatives m m m m m m m m m
double articulation m m m m m m m m m
gliding fricative m m
f=post-operative stula
A Harding and P Grunwell340
Table 2 Cleft-type processes in UCLP subjects at age 46 (study 2)
1-stage surgery 2-stage surgery
SE TB CK MS NC TS ZG CP
Passive cleft-type processespredominantly sonorant artic m
weak articulation m m m
voiceless h for plosives m m m
nasal release of plosives m m m
nasal emission with consonants m m
passive nasal fricative m m
Active cleft-type processesnasal fricativepharyngeal glottal articulation m m m
backing to uvular m
backing to velar m m
lateral palatal fricatives m m m m m
double articulation m m m m m m
gliding fricative m
Table 3 Cleft-type processes at age 90
2-stage surgery 2-stage surgery1-stage surgery completed at 4 yrs completed at 8 yrs
DAf SBf RL NR JD AR LJ RP MB
Passive cleft-type processespredominantly sonorant articweak articulation m
voiceless h for plosives m m
nasal release of plosives m m
nasal emission with consonants m m m m
passive nasal fricatives m m
Active cleft-type processesnasal fricatives m m
pharyngeal glottal articulation m m
backing to uvular m m
backing to velar m m m m m m m
lateral palatal fricatives m m m m m m m
double articulation m m m m m
gliding fricative m
f=subject had a stula
both active and passive strategies whereas later samples (ages 90ndash130) rarelyevidenced passive processes
At age 46 four out of ve BCLP subjects used active non-oral pharyngeal andglottal processes and oral velar and uvular fricatives irrespective of surgical status(see table 1) All had some anterior palatal defect which might have reduced theirpotential to achieve intra-oral pressure
By comparison two out of three partially repaired 2-stage UCLP subjects at age46 (table 2) showed evidence of passive processes This suggested that their
Active versus passive cleft-type speech characteristics 341
Tab
le4
Spee
chin
rela
tion
tosu
rgic
altim
ing
atag
e13
0
2-st
age
surg
ery
2-st
age
surg
ery
1-st
age
surg
ery
subj
ects
com
plet
edat
4yr
sco
mpl
eted
at8
yrs
1-A
1-B
1-C
1-D
1-E
1-F
24-
G2
4-H
24-
J2
8-K
28-
L2
8-M
Pass
ive
clef
t-ty
pepr
oces
ses
pred
omin
antly
sono
rant
artic
wea
kar
ticul
atio
nm
voic
eles
sh
fo
rpl
osiv
esna
sal
rele
ase
ofpl
osiv
esna
sal
emis
sion
with
cons
onan
tsm
pass
ive
nasa
lfr
icat
ives
Act
ive
clef
t-ty
pepr
oces
ses
nasa
lfr
icat
ives
phar
ynge
alg
lott
alar
ticul
atio
nba
ckin
gto
uvul
arba
ckin
gto
vela
rm
m
late
ral
pala
tal
fric
ativ
esm
mm
doub
lear
ticul
atio
ngl
idin
gfr
icat
ive
1=1-
stag
esu
rger
ysu
bjec
ts
24=
2-st
age
surg
ery
hard
pala
tere
pair
edat
abou
t4
yrs
28=
2-st
age
surg
ery
with
hard
pala
tere
pair
edat
abou
t8
yrs
A Harding and P Grunwell342
unrepaired hard palates had in fact restricted their phonetic repertoire imposing aneed for individual adaptability The additional active processes employed by thesesubjects were presumably a response to the restrictions imposed by their oro-nasalstructure and velopharyngeal function at the time of consonant acquisition Asshown in table 2 the most common active cleft-type processes persisting at age46 with a residual cleft of the hard palate were backing double articulation andlateralpalatal articulation Two 1-stage surgery subjects whose entire palates hadbeen repaired at ages 09 and 010 did not use any cleft-type processes at age 46
By age 90 (table 3) a much-diminished number of cleft type processes wasevident except in subjects with sizeable anterior stulae who had received littlespeech and language therapy A similarity was noted between the speech patternsof 1-stage surgery subjects with stulae (DA and SB) at age 90 (table 3) and theyounger BCLP subjects at age 46 (table 1) who also had anterior palatal defectsThey included non-oral realizations of t d s k g occasional nasal fricatives andpharyngealglottal articulations Fistulae had apparently continued to in uencearticulation and phonological development in these subjects
Finally at age 130 (table 4) the diVerences between 1-stage and 2-stage surgerysubjects had diminished leaving only one 2-stage subject with occasional backingand four subjects with slight palatal and lateral release of fricative consonants Onlytwo of the 1-stage surgery subjects were using minor distortions of grooved fricativeproduction
Whilst there were apparent trends in speech production relating to surgicaltiming and oral structure it is noted that there were exceptions to each tentativegeneralization Subjects with marked structural imperfections occasionally producedrealizations of which they would not have been thought capable and subjects withno visible imperfections produced inexplicably distorted speech patterns It istherefore concluded that whilst there is homogeneity in the range of processesproduced by this population assumptions cannot be made about speech based onsurgical timing or type of cleft Tentative predictions based on detailed assessmentmay be clinically very useful
EVects of surgery on speech
Activepassive processes have identi ed those cleft-type characteristics thought tobe associated with a physical inability to produce pressure consonants The followinganalysis of speech changes after surgical intervention at diVerent ages identi es thechanges eVected by surgery when intra-oral pressure could be more readily achieved
Two children were rst recorded prior to the rst stage of a 2-stage procedureTheir lips were repaired at approximately 6 months of age and soft palate repairwas carried out at ages 18 and 19 respectively Their hard palates were leftunrepaired to facilitate unrestricted growth of the mid-face (Hotz et al 1978) Pre-and post-operative consonant-like sounds present in the recorded speech samplesare listed in table 5 Interestingly prior to soft palate repair both these childrenproduced some oral consonants Subject B was producing pressure consonants [kg] in his babble prior to soft palate repair Considering that he had an unrepairedbilateral cleft palate at this point it was surprising that he had any oral consonantsPost-operatively at 20 years he used [b bkm t d g gkb] which indicated that surgeryto repair the soft palate had facilitated an increased range of oral pressure consonantsSubject D was producing [p b k g] pre-operatively Post-operatively following soft
Active versus passive cleft-type speech characteristics 343
Tab
le5
EV
ects
ofso
ftp
alat
ere
pair
atag
e1
6on
BC
LP
subj
ects
h
ard
pal
ate
rem
ain
sun
repa
ired
2-st
age
subj
ects
Surg
ery
Pre
-ope
rati
vesp
eech
patt
ern
atag
e1
6Po
st-o
pera
tive
chan
ges
insp
eech
atag
e2
0
Stud
y1
BSo
ftpa
late
repa
irat
16
Adu
ltta
rget
sk
gA
t2
0[b
b kmg kb
td
g]D
Soft
pala
tere
pair
17
Adu
ltta
rget
sp
bk
gA
t2
0[p
bd
b kdk
g]
Tab
le6
EV
ects
ofha
rdpa
late
rep
air
atag
e6
6an
d
stu
lare
pair
atag
e10
0
Subj
ect
Surg
ery
Pre
-ope
rati
vesp
eech
patt
ern
Post
-ope
rati
vech
ange
sin
spee
ch
MS
Har
dpa
late
repa
ir6
6Pa
ssiv
epr
oces
s7
6E
limin
ated
pass
ive
proc
ess
Var
iabl
ena
sal
rele
ase
ofco
nson
ants
Hyp
onas
alna
sals
JFH
ard
pala
tere
pair
(uns
ucce
ssfu
l)6
6Se
vera
lac
tive
and
pass
ive
proc
esse
s7
6A
ctiv
epr
oces
ses
rem
aine
dPa
ssiv
epr
oces
ses
elim
inat
ed
DA
Fis
tula
repa
ir10
0A
ctiv
epr
oces
ses
110
Elim
inat
ion
ofph
aryn
geal
glo
ttal
Var
iabi
lity+
+an
dna
sal
arti
cula
tion
Art
icul
ator
yva
riab
ility
++
Act
ive
CT
Rs
proc
esse
spe
rsis
t
A Harding and P Grunwell344
palate repair but with a residual cleft in the hard palate his range of consonantsincluded [d] which was particularly surprising since the hard palate remainedunrepaired Whilst it is unlikely that toddlers of 18 months could be consciouslytrying to compensate for articulatory inadequacy in producing velar plosives inbabble prior to soft palate repair and an alveolar plosive prior to hard palate repairboth these subjects showed evidence of actively pursuing their articulatory potential
Table 6 summarizes changes following surgery to repair the hard palate in moremature speech patterns These subjects who were aged 66 and 100 pre-operativelyhad learned to speak with residual clefts and were apparently unaware of theconsonant productions that failed to match normal production
Subject MS used only passive processes in his speech pattern He realized someconsonants nasally such that lsquoballrsquo was [mO~] and lsquosockrsquo was [(sk)n
deg Aacute~ k] Looking atpost-operative changes at age 76 his consonant production was normal but hisresonance had become hyponasal Pre-operatively at age 66 Subject JF was usingseveral active and passive processes The active processes were unaVected by surgerybut passive processes were eliminated
Fistula repair was carried out at age 100 on Subject DA who had many activeprocesses and very variable articulation pre-operatively Post-operatively at age110 he was not using non-oral pharyngeal and glottal active processes or nasalrealizations but many oral cleft-type realizations remained
As shown in table 7 hard palate re-repair and pharyngoplasty was carried outon two subjects whose hard palate repairs had been unsuccessful at approximately4 years Subject NC assessed pre-operatively at age 56 was using predominantlypassive processes in her speech She was also using [ j] for fricatives s S whichwas thought to be an active process At age 60 following hard palate re-repair andpharyngoplasty all cleft-type processes had been eliminated without post-operativespeech therapy Since [ j] for s apparently resolved spontaneously followingsurgery it can be assumed that this was a passive process in this speech sample
Subject CP who underwent this procedure presented pre-operatively at age 46with both passive and active processes but his nasal resonance was not consistentlyhypernasal In addition to his cleft-related speech disorder this subject had additionaldevelopmental speech diYculties which were identi ed as being unrelated to thecleft Post-operatively at age 56 little had changedmdashnotably the passive processnasal [m] for b was retained His nasal resonance had become hyponasal andthere was no apparent bene t from surgical intervention The realization of b as[m] had become phonologically stable and surgery alone had not destabilized thephonological system This realization may have been a passive product of VPI inearly speech acquisition which had subsequently become part of a phonologicaldisorder Post-operatively CPrsquos phonetic repertoire did increase but the phonologicaldistribution was variable Plosive targets were still realized as nasals in spontaneousspeech at the nal speech recording at age 76 This was not as an inevitableconsequence of VPI but a result of an inability to destabilize the phonologicalprocess determining that voiced plosives would be realized as nasals This resultfollowing surgery highlights the importance of identifying phonological learningproblems and distinguishing them from structural constraints on articulationIn CPrsquos case pre-operative exploration of the eVect of nares occlusion duringspeech might have indicated that structural change would not improve consonantproduction spontaneously
A general observation was that consonant realizations did not move rapidly
Active versus passive cleft-type speech characteristics 345
Tab
le7
EV
ects
ofha
rdpa
late
re-r
epai
ran
dp
hary
ngo
pla
sty
Subj
ect
Surg
ery
Pre
-ope
rati
vesp
eech
patt
ern
Post
-ope
rativ
ech
ange
sin
spee
ch
Stud
y2
NC
Har
dpa
late
re-r
epai
ran
d5
6Pa
ssiv
ecl
eft-
type
proc
esse
s6
0A
llcl
eft-
type
phar
yngo
plas
ty5
10[
j]
for
fric
ativ
espr
oces
ses
elim
inat
ed[
h]
for
plos
ives
SIW
IV
aria
ble
arti
cula
rypr
ecis
ion
CP
Har
dpa
late
repa
iran
d4
6Pa
ssiv
ean
dac
tive
proc
esse
s5
6Pa
ssiv
epr
oces
sph
aryn
gopl
asty
50
Pho
nolo
gica
lco
nfus
ion
[m]
for
[b
]re
tain
edH
ypon
asal
nasa
lsPe
rsis
ting
phon
olog
ical
conf
usio
ns
A Harding and P Grunwell346
from incorrect to correct but progressed incrementally towards normal realizationsas described by Morley (1970) Where an early realization of target s might beglottal [h] a gradual pattern of change showed subsequent realizations to bepharyngeal [Eacute] then uvular [X] then velar [x] and eventually palatal [c] or lateral [Euml]It was interesting to note that speech patterns continued to change as late as90ndash110 years with the result that diVerences related to surgical timing and cleft-type gradually disappeared Persisting stulae were thought to account for the mostmarked cleft type processes at age 90
Implications for surgical management
This analysis of speech changes following surgery suggests some implications forsurgical management which are compatible with Sell and Grunwellrsquos (1990) ndingsin the Sri Lankan study
Surgery can change passive speech processes but it is also possible that speechtherapy may be able to change passive patterns Surgery alone is unlikely to modifyactive cleft-type processes whereas speech therapy should be able to modify activeprocesses Indications from these case studies is that where speech is the primaryproblem speech assessment should distinguish between active and passive processesin order to evaluate the necessity for full investigations and to plan therapeuticintervention Where past speech therapy has not been successful it cannot beassumed that surgical intervention will facilitate further speech progress A furthercourse of speech therapy which is sensitive to active versus passive processes todevelopmental phonological in uences on cleft-type speech development and toarticulatory diYculties in diVerent speech contexts might facilitate optimal progressWhere structural imperfection exists it is quite possible for single-word productionto be more precise than target realizations in spontaneous speech This may not bea failure of phonological generalization (Grunwell 1992) but the result of diYcultysustaining the necessary lsquoarticulatory eVort rsquo (Harding and Grunwell 1993) resultingin articulatory imprecision Deteriorating articulatory accuracy should not be over-looked in interpretation of speech results
An analytical protocol
As a result of analysing the speech data and identifying the active and passiveprocesses a protocol has been developed which records examples of each cleft-typeprocess over a series of assessments It demonstrates the progression of individualprocesses towards an adult target (see the Appendix) At each assessment onecolumn is used to indicate nasal resonance nasal emission and nasal turbulenceratings and cleft-type processes Changes in the nature of error realizations mightshow progress towards target consonants Hence whilst the total correct scoremight not have increased increments of change can be observed This observationof patterns of change may function as an adjunct to GOSSPASSrsquo98 (Sell et al 1998)giving access to a greater depth of both quantitative and qualitative data aboutconsonant production in relation to resonance nasal emission nasal turbulenceoral structure and cleft-type
Active versus passive cleft-type speech characteristics 347
Diagnostic implications
Passive versus active nasal fricatives
The important management consideration related to this distinction is that an activenasal fricative is an established phonological process which is unlikely to be directlyaVected by surgery alone Therapy would be necessary to destabilize nasal realizationsof oral consonants In contrast passive nasal fricatives may be eliminated by surgeryOf particular relevance is diVerential diagnosis between passive and active nasalfricatives in surgical and therapeutic management When hypernasality co-occurswith nasal air ow during consonant production which can be redirected by nose-holding passive nasal fricatives are diagnosed These would be transcribed as [(sk)n
deg]
passive alveolar nasal fricatives [(Wk)mdeg
] bilabial nasal fricatives or [(fk)Iacutedeg ] labiodentalnasal fricatives Full VPI investigations would be recommended to diagnose thenature of the structural or functional de ciency and distinguish between velopharyn-geal incompetence and velopharyngeal mislearning
It is highly likely that plosive targets would be aVected by reduced intra-oral airpressure such that plosives would either be realized by nasal counterparts eg bd[ [m n] or [b d] may be nasalized and weak Voiceless plosives may be eitheraccompanied by nasal emission [p t k] or realized as glottal fricative [h]
Production of the target sentence lsquoI saw Sam sitting on a busrsquo might be
[aI (sk)ndeg O~ (sk)n
degaelig~m (sk)n
deg IhIn Aacute~n mouml~(sk)ndeg] passive processes and
[aI xO xaeligm xIkIIcirc AacuteIcirc goumlx] active processes
Contribution to surgical management decisions
Passiveactive interpretation of clinical assessments might facilitate surgical manage-ment decisions If noseholding does not facilitate correct production of targetconsonants then it is likely that an alternative articulatory pattern has becomephonologically established ie particular realizations for one or more targets areconsistently distributed in the phonological system These realizations may haveevolved because of initial diYculty producing articulatory targets and subsequentlystabilized within the phonological system Grundy and Harding (1995) refer to thisphenomenon as an lsquoarticulatory disorder with phonological consequencesrsquo
Therapy
Where obvious structural defects or diagnosed dysfunction exists clinicians fre-quently defer therapeutic intervention until surgery has been undertaken Theexpectation would be that normal structure and function is essential for normalspeech However pre-operative therapy may facilitate oral consonant productionwhich may serve to reduce hypernasal resonance Hence therapy prior to surgerymay avoid unnecessary surgery or reduce the extent of surgery required All activeprocesses are likely to require therapy
Principled selection of targets for therapy
Speech patterns frequently evidence a mixture of apparently passive and activeprocesses which complicates decisions about target selection Target selection can
A Harding and P Grunwell348
be based on assessment of which consonant targets can be most easily elicted inisolation (stimulability) This may lead to a sequence of target selection which isopposite to the sequence of consonant acquisition in normal development Forexample where reduced intra-oral pressure is present in a passive pattern [T] maybe easier to elicit in imitation than more nely grooved [s] or [S] Therapy maytarget [T] followed by [S ] and nally [s] As in non-cleft phonological therapywhere a class of consonants is aVected by the cleft then it is helpful to target theentire class The following decision-making process can be applied for both activeand passive processes
Decision making procedure for target selection
(1) Voiced versus voiceless targets(2) Front versus back placements(3) Syllable initial versus syllable nal targets(4) Plosives versus fricative targets
Voiceless plosives and fricatives are produced with an open glottis whichfacilitates topping up of air ow from the lungs hence voiceless plosive and fricativetargets are frequently more successful than voiced counterparts (Isshiki and Ringel1964) Front targets usually cause more diYculty than back particularly where analveolar defect or stula exists Contrary to normal development back targets maybe targeted before front Word- nal targets generally require less oral air pressurethan word initial targets and similarly fricatives may be more easily elicited thanplosives Fricatives do require a greater volume of air than plosives (Fletcher 1985)but in the presence of nasal escape weak fricative production appears to be morereadily achieved than weak plosive production Since nal fricatives would normallybe acquired in advance of word-initial fricatives (Ferguson 1978) targeting word- nal fricatives is frequently a productive starting point for therapy
Principles of therapy for passive processes
(1) Use of soft attack similar to gentle whisper for all target models ensuresminimal articulatory eVort (Harding and Grunwell 1993) and requires min-imal intra-oral air pressure It may be appropriate to gradually increase thearticulatory attack when the articulatory posture and evidence of intendedoral air ow have been established
(2) Slightly stretched duration of segment transitions in models of consonantto vowel (CndashV) or vowel to consonant (VndashC) facilitates review of motorplanning and extends the available time for execution of the new motorprogrammer whilst maintaining control of the oral airstream
(3) Noseholding can be used to provide exclusively oral air ow Gradual releaseof the nostrils during production of sustained [VVVVVf ] or [hhhhh ] allowsthe child to attempt to sustain an oral consonant despite increasing nasalemission This maximizes the use of available oral air ow Procedures forusing noseholding are described in some detail by Golding-Kushner (1995)
Principles of therapy for active processes
This is more like phonological therapy and can follow Grunwellrsquos (1991) processesfor phonological change and principled decision-making (Grunwell 1992) Some
Active versus passive cleft-type speech characteristics 349
examples are given here by way of illustration of ways to eVect the rst twoprocesses of change which may need to be approached diVerently in cleft palateversus non-cleft speech disorders DiVerent approaches may also be appropriate formodifying active versus passive cleft-type processes
Innovation production of new targets Some useful principles
(1) Introduction of new lsquonon-speech likersquo targets in sound play using a conson-ant sound segment model such as [ph ] note not a syllable like [p] whichis the type of pronunciation used when target sounds are presented as lettersfor reading Target [s] might be introduced as a lsquoTrain Slowing Down Noisersquo[ts ts ts tssssssss]
(2) lsquoNew consonantsrsquo can later be modelled and elicited in soft productions ofsyllable structure [tssssndashi] [ indashtssss] which can subsequently be identi ed assimilar to words lsquosearsquo and lsquoeatsrsquo
(3) lsquoDeferring responsibilityrsquo transfers responsibility or lsquoblamersquo for errors fromthe child and attributes it to the articulators eg lsquoyour tongue is havingtrouble with hellip rsquo lsquoLetrsquos show your tongue how to hellip rsquo
(4) New targets can be modelled repeatedly and recorded on audio or videotape which can be listened to at home
(5) Targeting classes of consonants (eg alveolars t d s n l voiceless fricativesf s S perhaps with aVricate T avoids phonological confusion whichmight occur if production ofsis achieved whilst other alveolar targetsremain backed The risk is that s might not integrate into the phonologicalsystem unless all backed alveolar consonants are destabilized
(6) Increased eye contact during auditory and production work can be invaluablein holding visual and auditory attention and ensures that visual informationabout the sound has been processed This is easily achieved by the clinicianlifting any focus of the childrsquos attention close to hisher mouth at theprecise moment when the target is modelled
Stimulation of non-speech related sounds such as a lsquoTrain Slowing DownNoisersquo [ts ts tsss] con rms that target [s] is physically achievable whether or not[ssss] can be imitated Some children continue to access [s] through the lsquoTrainSlowing Down Noisersquo throughout therapy until it is occurring spontaneouslywithout conscious planning This can be an eVective means of underminingestablished motor programmers (Hewlett 1990) for active cleft-type processes
Destabilizing active processes
As it is likely that children will be unaware of each occurrence of their alternativearticulatory pattern for speci c consonant errors it is preferrable to destabilizeactive processes with minimal conscious eVort by the child As children becomeaware of their mismatches they frequently add the newly acquired target realizationto their existing production eg target word tu childrsquos old realization [ku] childrsquoscorrected realization [t-ku] Destabilization can be achieved with minimal consciouseVort through input therapy techniques such as auditory bombardment (Lancasterand Pope 1989) auditory decision-making such as lsquowhich bear says this wordproperlyrsquo Red Bear says lsquotworsquo or Blue Bear says lsquocoorsquo This type of strategy oftenprecipitates attention to the target consonant with possible lsquoreplayrsquo and lsquoreviewrsquo of
A Harding and P Grunwell350
their own production Frequent stimulation of cognitive alertness to the targetconsonant can develop awareness without confronting the child with errors orrisking hisher failure The child is then free to attempt to repair hisher ownrealization to continue to re ect and to silently rehearse the adult realizationTraditional articulation therapy is thus combined with development of metaphonol-ogical skills ie the ability to re ect upon onersquos own speech production The resultshould be that new target realizations will be more phonologically stable thanexclusively production-based articulation therapy might have facilitated
Stabilizationgeneralization
Procedures to ensure stabilization and generalization of new target consonantswould be as described by Grunwell (1992) Success may be constrained by theconsiderable articulatory eVort sometimes required to maintain pressure consonantproduction in spontaneous speech (Harding and Grunwell 1993)
Conclusions
In speech assessment it is helpful to distinguish between errors which are cleft-type and non-cleft type and those which are part of active versus passive processesThe active and passive processes have been de ned and their phonological implica-tions discussed Focus on active and passive processes has facilitated focus on thephonological consequences of cleft palate on speech development In the futureawareness of the likely eVect of a cleft palate on normal phonological developmentcould avoid extended periods of unsuccessful clinical intervention Furthermoresensitivity to the relationship between phonological processes and structural con-straints should facilitate theoretically based management decisions Incidences suchas the case of CP in which nasal realizations were thought to indicate VPI but weresubsequently unaVected by surgery might be avoided if phonological analysiscontributes to management decisions
Surgery did improve hypernasal resonance and eliminated passive processes buthad little eVect on active processes Active processes in younger subjects werethought to require therapeutic intervention but in the longer term the oldersubjects showed few cleft-type processes Whilst it is possible that active cleft-typeprocesses may resolve with increasing age the implication for the future is thatactive cleft-type processes should be treated with skilled therapeutic interventionnot surgery Therapy which addresses the phonological consequences of cleft palateon speech development by combining metaphonologicalphonologicalarticulatoryapproaches is likely to be successful
References
Albery E 1991 Consonant articulation in the diVerent types of cleft lip and palate UnpublishedMPhil thesis Leicester Polytechnic
Albery E and Grunwell P 1993 Consonant articulation in diVerent types of cleft palate InP Grunwell (Ed) Analysing Cleft Palate Speech (London Whurr)
Ferguson C A 1978 Fricatives in child language acquisition In V Honsa and M Hardmann-Battista (Eds) Papers on Linguistics and Child Language (Mouton The Hague)
Fletcher S G 1985 Speech production and oral motor skill in an adult with an unrepaired palatalcleft Journal of Speech and Hearing Disorders 50 254ndash261
Active versus passive cleft-type speech characteristics 351
Golding-Kushner K J 1995 Treatment of articulation and resonancne disorders associated withcleft palate management and VPI In R Shprintzen (Ed) Cleft Palate Speech Management AMultidisciplinary Approach (St Louis Mosby)
Grundy K and Harding A 1995 Developmental speech disorders In K Grundy (Ed) Linguisticsin Clinical Practice (2nd edition) (London Whurr)
Grunwell P 1985 Phonological Assessment of Child Speech (Windsor NFER-Nelson)Grunwell P 1987a Clinical Phonology (2nd edition) (London Croom Helm)Grunwell P 1987b PACS Pictures Language Elicitation Materials (Windsor NFER-Nelson)Grunwell P 1991 Processes of phonological change in developmental speech disorders Clinical
Linguistics and Phonetics 6 101ndash122Grunwell P 1992 Principled decision making in the remediation of children with phonological
disorders In P Fletcher and D Hall (Eds) Specic Speech and Language Disorders in Children(London Whurr)
Grunwell P and Harding A 1995 PACSTOYS A Screening Assessment of Phonological Development(Windsor NFER-Nelson)
Grunwell P and Harding A 1996 A note on describing types of nasality Clinical Linguistics andPhonetics 10 157ndash161
Harding A 1993 An Investigation into the Relationship Between Timing of Cleft Palate Repairand Speech Development Unpublished PhD thesis
Harding A and Grunwell P 1993 The relationship between speech and timing of hard palaterepair In P Grunwell (Ed) Analysisng Cleft Palate Speech (London Whurr)
Harding A and Grunwell P 1996 Characteristics of cleft palate speech European Journal ofDisorders of Communication 31 331ndash358
Henningsson G and Isberg A M 1986 Velopharyngeal movement patterns in patients alternatingbetween oral and glottal articulation A clinical and cineradiographicical study Cleft Palate Journal23 1ndash9
Hewlett N 1990 Processes of development and production In P Grunwell (Ed) DevelopmentalSpeech Disorders (Edinburgh Churchill Livingstone)
Hotz M M Gnoinski W M Nussbaumer H and Kistler E 1978 Early orthopaedics in CLPcases guidelines for surgery Cleft Palate Journal 15 405ndash411
Hutters B and Brondsted K 1987 Strategies in cleft palate with special reference to DanishCleft Palate Journal 24 127ndash136
Isshiki N and Ringel R 1964 Airow during the production of selected consonants Journal ofSpeech and Hearing Research 7 233ndash244
Kummer A W Curtis C Wiggs M Lee L and Strife J L 1992 Comparison of velopharyngealgap size in patients with hypernasality hypernasality with nasal emission and nasal emissionor nasal turbulence (rustle) as the primary speech characteristic Cleft-palate-Craniofacial Journal29 152ndash156
Lancaster G and Pope L 1989 Working with Childrenrsquos Phonology (Oxford Winslow)Morley M E 1970 Cleft Palate and Speech (7th edition) (Edinburgh Churchill Livingstone)Russell V J 1991 Speech Development in Children with Cleft Lip and Palate Unpublished PhD
thesis Leicester PolytechnicRussell V J and Grunwell P 1993 Speech development in children with cleft lip and palate In
P Grunwell (Ed) Analysing Cleft Palate Speech (London Whurr)Sell D A and Grunwell P 1990 Speech results following late palatal surgery in previously
unoperated Sri Lankan adolescents with cleft palate Cleft Palate Journal 27 162ndash168Sell D Harding A and Grunwell P 1994 GOSSPASS A screening assessment of cleft palate
speech European Journal of Disorders of Communication 29 1ndash15Sell D Harding A and Grunwell P 1998 GOSSPASSrsquo98 An assessment for speech disorders
associated with cleft palate andor velopharyngeal dysfunction International Journal of Languageamp Communication Disorders ( in press)
Shorter E 1995 A spectographic analyis of child homophones Unpublished honours project DeMontfort University Leicester
Stenglehoffen J 1989 Nature and causes of communication diYculties In J Stengelhofen (Ed)Cleft Palate Nature and Remediation of Communication Problems (Edinburgh Churchill Livingstone)
Trost J E 1981 Articulatory additions to the classical description of the speech of persons withcleft palate Cleft Palate Journal 18
Trost-Cardamone J E 1990 The development of speech assessing cleft palate misarticulationsIn D A Kernahan and S N Rosenstein (Eds) Cleft Lip and Palate A System of Management(Baltimore Williams amp Wilkins)
A Harding and P Grunwell352
Appendix Active passive analysis of cleft palate speech

A Harding and P Grunwell334
Figure 2 Passive cleft-type processes
containing active processes usually sound distinctive but communicative compet-ence can be impressive because more meaningful diVerences can be signalled thanmay be possible with the restricted phonetic repertoire of passive processes Giventhat the velopharyngeal sphincter is complex and dynamic it is possible for arestricted phonetic repertoire with hypernasal resonance to persist into early speechdevelopment because a child has been unable to achieve velopharyngeal functionfor speech after palate repair
The distinction between active and passive cleft-type processes has been integ-rated into the revised cleft palate speech assessment GOSSPASSrsquo98 (Sell et al1998) De nitions of cleft-type characteristics are given in GOSSPASSrsquo98 butGOSSPASS does not interpret the phonological consequences of the cleft-typecharacteristics The following de nitions of active and passive cleft-type processesare based on data analysis in the present study and on Harding and Grunwellrsquos(1996) characteristics of cleft palate speech Analysis of patterns of phonemeevolution throughout speech acquisition has generated a hierarchy of error-severityThe following descriptions of the diVerent types of processes are illustrated byreference to the data collected in the research studies (Harding 1993)
Active cleft type processes
Active nasal fricatives
[mdegk] [n
degk] [ Daggerk
deg] Nasal realizations of voiceless and sometimes voiced fricative targets
f v s z S Z were categorized as nasal fricatives Comparison of gures 1 and 2shows that nasal realizations occurred in both passive and active processes Inproduction of active nasal fricatives the pulmonary air is actively directed nasallyas an alternative articulation to an oral fricative realization Figure 3 illustrates thatoral air ow is stopped by either lips or tongue thus achieving 100 nasal air owThis strategy is developed in order to signal the fricative nature of intended targetfricative consonants In the active nasal fricative [m
degk] for f n
degk for s [n
degk O] for
lsquosorersquo [mdegk O] for lsquofourrsquo is the product of actively directed nasal air Where fricative
consonants are the only targets aVected by a cleft-type process the presence ofnasal fricatives have been referred to as phoneme speci c nasality (Trost-Cardamone
Active versus passive cleft-type speech characteristics 335
Figure 3 Active nasal fricative [ndegk]
1990) This characteristic has been found in speakers with no cleft palate historyoften with no explanation for its occurence
DiVerent places of articulation signalled placement contrasts between nasalfricative consonants in the same way that target nasal consonants [m n Icirc] arediVerentiated by place of articulation [m
degk] for f [n
degk] for s S Where a strong
backing process existed alveolar and post-alveolar fricatives were realized by velarnasal fricatives [ Daggerk
deg]
Occasionally nasal air ow was constricted such that nasal fricatives were pro-duced with a noisier turbulent quality [m
deg] [n
deg] [ Dagger] In a detailed assessment of cleft
pa la te speech GOSSPASSrsquo98 (Sell et al 1994 1998) these turbulent realizationswould be categorized in the resonance section as lsquonasal turbulence replacing conson-antsrsquo and in the cleft-type characteristics section as either lsquoactive nasal fricativesrsquo orpassive nasal realization of fricatives
Glottal articulation
[] frequently occurred in early plosive and aVricate production [p b t d T] up toage 46 Sometimes this process aVected only alveolar plosives t d in SIWI andSIWW position At times glottal stop represented voiced plosives [b d g] while[h] represented voiceless plosives [p t k] In SFWF position glottal stop representedboth voiced and voiceless plosives It may be the case that diVerent strengths ofglottal stop were used to distinguish voiceless and voiced plosives but this couldnot be reliably judged without spectographic analysis An undergraduate study ofspectographic analysis (Shorter 1995) of cleft palate speech identi ed some subtlediVerences in glottal stop productions which suggests a need for further investigationinto the phonological functions of glottal stops in cleft palate speech
Pharyngeal fricatives
[Eacute iquest] Early attempts at fricatives (ages 20ndash30) were frequently realized with acombination of posterior fricative cleft-type realizations (CTRs) Where plosiveswere exclusively glottal fricative consonants were frequently realized as pharyngeal
A Harding and P Grunwell336
fricatives In early phonological development obstruent realizations were commonlynon-oral but gradually moved anteriorly to uvular and velar positions Targetconsonants were not generally corrected independently of each other The gradualmovement of pharyngeal realizations towards oral uvularvelar articulation whichunderlines the relevance of a phonological interpretation of cleft palate speechcharacteristics
Exclusively pharyngealglottal patterns of articulation might imply velopharyn-geal insuYciency but it is noted here that all infants use pharyngeal and glottalarticulation until they acquire velopharyngeal competence during the rst 6 monthsof life It is possible for children with cleft palate to persist with this phoneticrepertoire for some time after palate repair Indeed such cases have been reportedby Russell and Grunwell (1993) Non-oral articulatory patterns indicate that thesphincter is not employed during speech which implies that the sphincter may notbe functional but unless oral air ow is consciously intended it cannot be assumedthat the sphincter is unable to function in speech (Henningsson and Isberg 1986)
Backing [k g q G]
A backing pattern is described by Stengelhofen (1989) as a lsquotendency for oralcontacts to be to the back of the oral cavityrsquo GOSSPASSrsquo98 (Sell et al 1998) makesa distinction here between backing to uvular and backing to velar place ofarticulation
E Backing to uvular [q G X Ograve ] Alveolar target consonants were backed touvular realizations and occasionally velar targets were backed to uvular Thepresence of velar and uvular realizations indicated the presence of some VPfunction but this might have been achieved with tongue humping In thedata acquisition of uvular and velar fricatives generally co-occurred withacquisition of f v which provides further evidence of velopharyngealfunction In the longitudinal study from age 16 to 46 subjects with bilateralclefts spent a period of months realizing all alveolar and post- alveolar voicedand voiceless consonant targets in uvular placement This degree of backingis deemed to be more severe and distracting for listeners than backing tovelar perhaps because uvular articulation is more distinctively non-EnglishHowever uvular fricatives are frequently used to achieve some meaningfulcontrasts which improve intelligibility
E Backing to velar In the younger subjects (aged 16ndash46) as articulatorypatterns progressed anteriorly a preference for [g] was common Mostcommonly backing resulted in t d realized as [k g] and s z as [x aring ]which contrasts with the fronting pattern seen in normal development
Double articulation
This is de ned as two simultaneous equal strictures at two places of articulationwhich was frequently noted in realizations of target alveolar consonants t d whenalveolarvelar contacts [tkk dkg] were used Double articulation may have beendeveloped to distinguish between alveolar and velar consonants in the presence ofa backing pattern Interestingly double articulation became evident in these develop-ing speech patterns with the emergence of fricative realizations Both plosives andfricatives tended to be realized with double articulation eg tndash[tkk] sndash[skagrave ]
Active versus passive cleft-type speech characteristics 337
Palatal fricatives [c J ]
These fricative realizations of alveolar target consonants appeared towards the endof the study period (ages 16ndash46) They were the most common realizations ofalveolar fricatives in older children (46ndash76 and 100ndash110) This nding was inaccordance with Alberyrsquos results (Albery 1991 Albery and Grunwell 1993)
Lateral fricatives [l Igrave]
As with palatal fricatives lateral fricatives were frequently present as realizations offricative consonant targets becoming particularly prevalent in later phonologicaldevelopment
Gliding of fricatives s S= [ j] or [w]
This phenomenon is seen in the non-cleft population as an uncommon develop-mental process (Grunwell 1987) It is classi ed here as an active process because[ j] was consistently produced as an apparently active alternative to target conson-ant(s) s z S [ j] is a normal consonant-like production in non-cleft babble whichcleft palate children often integrate into their phonological system It may betherefore that it is a persisting immaturity in the cleft palate population In thesedata [ j] was eVective in signalling a contrast between plosives and fricatives inSIWI position It functioned for the following consonants in diVerent speakers [ j]for S [ j] for m p f s z Ÿ h and co-articulation [hkj] for T
Passive cleft type processes
The criteria for passive cleft type processes is that they are (1) an attempt toproduce the correct articulatory placement and stricture (manner) which (2) failsbecause of a lack of intra-oral air pressure For example voiced plosives realized asnasals b[ [m] d[ [n] g[ [Icirc] No compensatory articulatory pattern hasbeen used to replace the intended consonant As the above examples demonstratetarget realizations often match a similar English consonant
Absence of pressure consonantspredominantly sonorant articulation
This phenomenon is de ned here as a pattern of articulation which was restrictedto English nasal and approximant articulations [m n Icirc w j] and [h] Some of thevoiced consonants were also employed as voiceless counterparts [m
degndeg Icircdeg ] thereby
increasing the range of available consonants for distribution in the phonologicalsystem Despite the limited consonant repertoire these patterns were often eVec-tively interpreted by close family members
Weak articulation [bV dV]
This category refers to normal articulatory movement in the production of obstruenttargets (plosive fricative and aVricate targets) which were produced with reducedoral air pressure and therefore articulation was considerably weakened In the speechsample data (ages 16ndash46) many target consonants were weakened to some degreeand at times may have been realised as nasals
A Harding and P Grunwell338
Passive nasal fricative [(fk)m (sk)ndeg]
Incomplete velopharyngeal closure inevitably reduces control of oral air ow with apassive loss of air ow and an increase of resonance in the nasal cavity Grunwelland Harding (1996) de ned the passively nasal fricative as an unreleased [(s)]double-articulated with a lowered voiceless nasal [n
Aacute
deg] This realization is the product
of an intended s with an unintended nasal air ow (see gure 4) The precisetranscription for a passive nasal transcription is [(sk)n
Aacute
deg] but an acceptable simpli cation
for transcription purposes is [(sk)ndeg] This is distinct from the active nasal fricative
which involves stopping of the oral air ow and active direction of air nasally whichcan be transcribed as a voiceless nasal with additional nasal emission [n
degk] Nasal
emission signals the fricative nature of for example target consonant s Thesetwo productions can sound the same and might initially be transcribed as [n
degk]
Nasendoscopic investigation of velopharyngeal activity during active and passivenasal realizations of s both show a lack of velopharyngeal closure It is predictedthat close examination by use of electropalatography might show slight diVerencesin tongue tip posture for an active and passive nasal fricative as illustrated in gures3 and 4 Passive nasal fricatives were converted into oral fricatives with nose-holding
Voiceless [h] for voiceless plosives
There was evidence that voiceless plosives were at times passively realized as [h]The consequence of reduced oral air pressure on production of voiceless plosivescan leave aspiration as the only perceptible distinctive feature This process usuallyaVected all voiceless plosive targets p t k Where this process was a passiveprocess use of noseholding during speech facilitated accurate target productionHowever it would also be possible for this distribution of [h] to be an active cleft-type process which would be part of a pharyngealglottal patternprocess
Nasal realization of voiced plosives b d g[ [m n Icirc]
Some subjects with residual clefts stulae or suspected VPI realized voiced conson-ants as nasal counterparts As summarized by Harding and Grunwell (1996) voiced
Figure 4 Passive nasal fricative [(sk)nAacute
deg]
Active versus passive cleft-type speech characteristics 339
consonants can be more diYcult to produce than voiceless consonants (Isshiki andRingel 1964) Distinction between active versus passive nasal realizations of plosivetargets was made in the same way that active and passive nasal fricatives weredistinguished by observing the eVect of noseholding on consonant production Inpassive nasal realizations noseholding facilitated normal consonant production(Golding-Kushner 1995)
Nasal emission accompanying consonants [pk sk]
Nasal emission was frequently heard accompanying consonants but on occasions itapparently replaced consonants It has been linked with velopharyngeal incompet-ence (VPI) (Kummer et al 1992)
Results
Comparison of activepassive processes in the speech data
Quantitative results of Hardingrsquos research into the relationship between timing ofsurgery and speech development have already been published (Harding andGrunwell 1993) The following interpretation of the data speci cally identi esactivepassive cleft-type processes in relation to oral structure in a wide age rangeof subjects (16ndash130) Tables 1 2 3 and 4 show the passive and active processeson the left-hand column and the subjectrsquos code along the top The code identi esthose subjects who were treated with 1-stage versus 2-stage surgery Comparisonof the 4 tables at age 46 (BCLP and UCLP) at age 90 and at age 130 illustratesa pattern of diminishing cleft-type processes with increasing age Irrespective ofsurgical timing few cleft-type processes remained at age 130 (table 4) A generalobservation was that earlier speech samples (ages 16ndash76) frequently combined
Table 1 Cleft-type processes in BCLP subjects at age 46 (studies 1 and 2)
1-stage surgery 2-stage surgery
A G Rf JW D B JF JG AB
Passive cleft-type processespredominantly sonorant articulation m
weak articulation m m m m m m m m
voiceless h for plosive m m m m m
nasal release of plosives m m m m m
nasal emission with consonants m m m m m m
passive nasal fricativeActive cleft-type processes
nasal fricatives m m m m m m m m
pharyngeal glottal articulation m m m m m m m m
backing to uvular m m m m m m m m
backing to velar m m m m m m m m m
lateral palatal fricatives m m m m m m m m m
double articulation m m m m m m m m m
gliding fricative m m
f=post-operative stula
A Harding and P Grunwell340
Table 2 Cleft-type processes in UCLP subjects at age 46 (study 2)
1-stage surgery 2-stage surgery
SE TB CK MS NC TS ZG CP
Passive cleft-type processespredominantly sonorant artic m
weak articulation m m m
voiceless h for plosives m m m
nasal release of plosives m m m
nasal emission with consonants m m
passive nasal fricative m m
Active cleft-type processesnasal fricativepharyngeal glottal articulation m m m
backing to uvular m
backing to velar m m
lateral palatal fricatives m m m m m
double articulation m m m m m m
gliding fricative m
Table 3 Cleft-type processes at age 90
2-stage surgery 2-stage surgery1-stage surgery completed at 4 yrs completed at 8 yrs
DAf SBf RL NR JD AR LJ RP MB
Passive cleft-type processespredominantly sonorant articweak articulation m
voiceless h for plosives m m
nasal release of plosives m m
nasal emission with consonants m m m m
passive nasal fricatives m m
Active cleft-type processesnasal fricatives m m
pharyngeal glottal articulation m m
backing to uvular m m
backing to velar m m m m m m m
lateral palatal fricatives m m m m m m m
double articulation m m m m m
gliding fricative m
f=subject had a stula
both active and passive strategies whereas later samples (ages 90ndash130) rarelyevidenced passive processes
At age 46 four out of ve BCLP subjects used active non-oral pharyngeal andglottal processes and oral velar and uvular fricatives irrespective of surgical status(see table 1) All had some anterior palatal defect which might have reduced theirpotential to achieve intra-oral pressure
By comparison two out of three partially repaired 2-stage UCLP subjects at age46 (table 2) showed evidence of passive processes This suggested that their
Active versus passive cleft-type speech characteristics 341
Tab
le4
Spee
chin
rela
tion
tosu
rgic
altim
ing
atag
e13
0
2-st
age
surg
ery
2-st
age
surg
ery
1-st
age
surg
ery
subj
ects
com
plet
edat
4yr
sco
mpl
eted
at8
yrs
1-A
1-B
1-C
1-D
1-E
1-F
24-
G2
4-H
24-
J2
8-K
28-
L2
8-M
Pass
ive
clef
t-ty
pepr
oces
ses
pred
omin
antly
sono
rant
artic
wea
kar
ticul
atio
nm
voic
eles
sh
fo
rpl
osiv
esna
sal
rele
ase
ofpl
osiv
esna
sal
emis
sion
with
cons
onan
tsm
pass
ive
nasa
lfr
icat
ives
Act
ive
clef
t-ty
pepr
oces
ses
nasa
lfr
icat
ives
phar
ynge
alg
lott
alar
ticul
atio
nba
ckin
gto
uvul
arba
ckin
gto
vela
rm
m
late
ral
pala
tal
fric
ativ
esm
mm
doub
lear
ticul
atio
ngl
idin
gfr
icat
ive
1=1-
stag
esu
rger
ysu
bjec
ts
24=
2-st
age
surg
ery
hard
pala
tere
pair
edat
abou
t4
yrs
28=
2-st
age
surg
ery
with
hard
pala
tere
pair
edat
abou
t8
yrs
A Harding and P Grunwell342
unrepaired hard palates had in fact restricted their phonetic repertoire imposing aneed for individual adaptability The additional active processes employed by thesesubjects were presumably a response to the restrictions imposed by their oro-nasalstructure and velopharyngeal function at the time of consonant acquisition Asshown in table 2 the most common active cleft-type processes persisting at age46 with a residual cleft of the hard palate were backing double articulation andlateralpalatal articulation Two 1-stage surgery subjects whose entire palates hadbeen repaired at ages 09 and 010 did not use any cleft-type processes at age 46
By age 90 (table 3) a much-diminished number of cleft type processes wasevident except in subjects with sizeable anterior stulae who had received littlespeech and language therapy A similarity was noted between the speech patternsof 1-stage surgery subjects with stulae (DA and SB) at age 90 (table 3) and theyounger BCLP subjects at age 46 (table 1) who also had anterior palatal defectsThey included non-oral realizations of t d s k g occasional nasal fricatives andpharyngealglottal articulations Fistulae had apparently continued to in uencearticulation and phonological development in these subjects
Finally at age 130 (table 4) the diVerences between 1-stage and 2-stage surgerysubjects had diminished leaving only one 2-stage subject with occasional backingand four subjects with slight palatal and lateral release of fricative consonants Onlytwo of the 1-stage surgery subjects were using minor distortions of grooved fricativeproduction
Whilst there were apparent trends in speech production relating to surgicaltiming and oral structure it is noted that there were exceptions to each tentativegeneralization Subjects with marked structural imperfections occasionally producedrealizations of which they would not have been thought capable and subjects withno visible imperfections produced inexplicably distorted speech patterns It istherefore concluded that whilst there is homogeneity in the range of processesproduced by this population assumptions cannot be made about speech based onsurgical timing or type of cleft Tentative predictions based on detailed assessmentmay be clinically very useful
EVects of surgery on speech
Activepassive processes have identi ed those cleft-type characteristics thought tobe associated with a physical inability to produce pressure consonants The followinganalysis of speech changes after surgical intervention at diVerent ages identi es thechanges eVected by surgery when intra-oral pressure could be more readily achieved
Two children were rst recorded prior to the rst stage of a 2-stage procedureTheir lips were repaired at approximately 6 months of age and soft palate repairwas carried out at ages 18 and 19 respectively Their hard palates were leftunrepaired to facilitate unrestricted growth of the mid-face (Hotz et al 1978) Pre-and post-operative consonant-like sounds present in the recorded speech samplesare listed in table 5 Interestingly prior to soft palate repair both these childrenproduced some oral consonants Subject B was producing pressure consonants [kg] in his babble prior to soft palate repair Considering that he had an unrepairedbilateral cleft palate at this point it was surprising that he had any oral consonantsPost-operatively at 20 years he used [b bkm t d g gkb] which indicated that surgeryto repair the soft palate had facilitated an increased range of oral pressure consonantsSubject D was producing [p b k g] pre-operatively Post-operatively following soft
Active versus passive cleft-type speech characteristics 343
Tab
le5
EV
ects
ofso
ftp
alat
ere
pair
atag
e1
6on
BC
LP
subj
ects
h
ard
pal
ate
rem
ain
sun
repa
ired
2-st
age
subj
ects
Surg
ery
Pre
-ope
rati
vesp
eech
patt
ern
atag
e1
6Po
st-o
pera
tive
chan
ges
insp
eech
atag
e2
0
Stud
y1
BSo
ftpa
late
repa
irat
16
Adu
ltta
rget
sk
gA
t2
0[b
b kmg kb
td
g]D
Soft
pala
tere
pair
17
Adu
ltta
rget
sp
bk
gA
t2
0[p
bd
b kdk
g]
Tab
le6
EV
ects
ofha
rdpa
late
rep
air
atag
e6
6an
d
stu
lare
pair
atag
e10
0
Subj
ect
Surg
ery
Pre
-ope
rati
vesp
eech
patt
ern
Post
-ope
rati
vech
ange
sin
spee
ch
MS
Har
dpa
late
repa
ir6
6Pa
ssiv
epr
oces
s7
6E
limin
ated
pass
ive
proc
ess
Var
iabl
ena
sal
rele
ase
ofco
nson
ants
Hyp
onas
alna
sals
JFH
ard
pala
tere
pair
(uns
ucce
ssfu
l)6
6Se
vera
lac
tive
and
pass
ive
proc
esse
s7
6A
ctiv
epr
oces
ses
rem
aine
dPa
ssiv
epr
oces
ses
elim
inat
ed
DA
Fis
tula
repa
ir10
0A
ctiv
epr
oces
ses
110
Elim
inat
ion
ofph
aryn
geal
glo
ttal
Var
iabi
lity+
+an
dna
sal
arti
cula
tion
Art
icul
ator
yva
riab
ility
++
Act
ive
CT
Rs
proc
esse
spe
rsis
t
A Harding and P Grunwell344
palate repair but with a residual cleft in the hard palate his range of consonantsincluded [d] which was particularly surprising since the hard palate remainedunrepaired Whilst it is unlikely that toddlers of 18 months could be consciouslytrying to compensate for articulatory inadequacy in producing velar plosives inbabble prior to soft palate repair and an alveolar plosive prior to hard palate repairboth these subjects showed evidence of actively pursuing their articulatory potential
Table 6 summarizes changes following surgery to repair the hard palate in moremature speech patterns These subjects who were aged 66 and 100 pre-operativelyhad learned to speak with residual clefts and were apparently unaware of theconsonant productions that failed to match normal production
Subject MS used only passive processes in his speech pattern He realized someconsonants nasally such that lsquoballrsquo was [mO~] and lsquosockrsquo was [(sk)n
deg Aacute~ k] Looking atpost-operative changes at age 76 his consonant production was normal but hisresonance had become hyponasal Pre-operatively at age 66 Subject JF was usingseveral active and passive processes The active processes were unaVected by surgerybut passive processes were eliminated
Fistula repair was carried out at age 100 on Subject DA who had many activeprocesses and very variable articulation pre-operatively Post-operatively at age110 he was not using non-oral pharyngeal and glottal active processes or nasalrealizations but many oral cleft-type realizations remained
As shown in table 7 hard palate re-repair and pharyngoplasty was carried outon two subjects whose hard palate repairs had been unsuccessful at approximately4 years Subject NC assessed pre-operatively at age 56 was using predominantlypassive processes in her speech She was also using [ j] for fricatives s S whichwas thought to be an active process At age 60 following hard palate re-repair andpharyngoplasty all cleft-type processes had been eliminated without post-operativespeech therapy Since [ j] for s apparently resolved spontaneously followingsurgery it can be assumed that this was a passive process in this speech sample
Subject CP who underwent this procedure presented pre-operatively at age 46with both passive and active processes but his nasal resonance was not consistentlyhypernasal In addition to his cleft-related speech disorder this subject had additionaldevelopmental speech diYculties which were identi ed as being unrelated to thecleft Post-operatively at age 56 little had changedmdashnotably the passive processnasal [m] for b was retained His nasal resonance had become hyponasal andthere was no apparent bene t from surgical intervention The realization of b as[m] had become phonologically stable and surgery alone had not destabilized thephonological system This realization may have been a passive product of VPI inearly speech acquisition which had subsequently become part of a phonologicaldisorder Post-operatively CPrsquos phonetic repertoire did increase but the phonologicaldistribution was variable Plosive targets were still realized as nasals in spontaneousspeech at the nal speech recording at age 76 This was not as an inevitableconsequence of VPI but a result of an inability to destabilize the phonologicalprocess determining that voiced plosives would be realized as nasals This resultfollowing surgery highlights the importance of identifying phonological learningproblems and distinguishing them from structural constraints on articulationIn CPrsquos case pre-operative exploration of the eVect of nares occlusion duringspeech might have indicated that structural change would not improve consonantproduction spontaneously
A general observation was that consonant realizations did not move rapidly
Active versus passive cleft-type speech characteristics 345
Tab
le7
EV
ects
ofha
rdpa
late
re-r
epai
ran
dp
hary
ngo
pla
sty
Subj
ect
Surg
ery
Pre
-ope
rati
vesp
eech
patt
ern
Post
-ope
rativ
ech
ange
sin
spee
ch
Stud
y2
NC
Har
dpa
late
re-r
epai
ran
d5
6Pa
ssiv
ecl
eft-
type
proc
esse
s6
0A
llcl
eft-
type
phar
yngo
plas
ty5
10[
j]
for
fric
ativ
espr
oces
ses
elim
inat
ed[
h]
for
plos
ives
SIW
IV
aria
ble
arti
cula
rypr
ecis
ion
CP
Har
dpa
late
repa
iran
d4
6Pa
ssiv
ean
dac
tive
proc
esse
s5
6Pa
ssiv
epr
oces
sph
aryn
gopl
asty
50
Pho
nolo
gica
lco
nfus
ion
[m]
for
[b
]re
tain
edH
ypon
asal
nasa
lsPe
rsis
ting
phon
olog
ical
conf
usio
ns
A Harding and P Grunwell346
from incorrect to correct but progressed incrementally towards normal realizationsas described by Morley (1970) Where an early realization of target s might beglottal [h] a gradual pattern of change showed subsequent realizations to bepharyngeal [Eacute] then uvular [X] then velar [x] and eventually palatal [c] or lateral [Euml]It was interesting to note that speech patterns continued to change as late as90ndash110 years with the result that diVerences related to surgical timing and cleft-type gradually disappeared Persisting stulae were thought to account for the mostmarked cleft type processes at age 90
Implications for surgical management
This analysis of speech changes following surgery suggests some implications forsurgical management which are compatible with Sell and Grunwellrsquos (1990) ndingsin the Sri Lankan study
Surgery can change passive speech processes but it is also possible that speechtherapy may be able to change passive patterns Surgery alone is unlikely to modifyactive cleft-type processes whereas speech therapy should be able to modify activeprocesses Indications from these case studies is that where speech is the primaryproblem speech assessment should distinguish between active and passive processesin order to evaluate the necessity for full investigations and to plan therapeuticintervention Where past speech therapy has not been successful it cannot beassumed that surgical intervention will facilitate further speech progress A furthercourse of speech therapy which is sensitive to active versus passive processes todevelopmental phonological in uences on cleft-type speech development and toarticulatory diYculties in diVerent speech contexts might facilitate optimal progressWhere structural imperfection exists it is quite possible for single-word productionto be more precise than target realizations in spontaneous speech This may not bea failure of phonological generalization (Grunwell 1992) but the result of diYcultysustaining the necessary lsquoarticulatory eVort rsquo (Harding and Grunwell 1993) resultingin articulatory imprecision Deteriorating articulatory accuracy should not be over-looked in interpretation of speech results
An analytical protocol
As a result of analysing the speech data and identifying the active and passiveprocesses a protocol has been developed which records examples of each cleft-typeprocess over a series of assessments It demonstrates the progression of individualprocesses towards an adult target (see the Appendix) At each assessment onecolumn is used to indicate nasal resonance nasal emission and nasal turbulenceratings and cleft-type processes Changes in the nature of error realizations mightshow progress towards target consonants Hence whilst the total correct scoremight not have increased increments of change can be observed This observationof patterns of change may function as an adjunct to GOSSPASSrsquo98 (Sell et al 1998)giving access to a greater depth of both quantitative and qualitative data aboutconsonant production in relation to resonance nasal emission nasal turbulenceoral structure and cleft-type
Active versus passive cleft-type speech characteristics 347
Diagnostic implications
Passive versus active nasal fricatives
The important management consideration related to this distinction is that an activenasal fricative is an established phonological process which is unlikely to be directlyaVected by surgery alone Therapy would be necessary to destabilize nasal realizationsof oral consonants In contrast passive nasal fricatives may be eliminated by surgeryOf particular relevance is diVerential diagnosis between passive and active nasalfricatives in surgical and therapeutic management When hypernasality co-occurswith nasal air ow during consonant production which can be redirected by nose-holding passive nasal fricatives are diagnosed These would be transcribed as [(sk)n
deg]
passive alveolar nasal fricatives [(Wk)mdeg
] bilabial nasal fricatives or [(fk)Iacutedeg ] labiodentalnasal fricatives Full VPI investigations would be recommended to diagnose thenature of the structural or functional de ciency and distinguish between velopharyn-geal incompetence and velopharyngeal mislearning
It is highly likely that plosive targets would be aVected by reduced intra-oral airpressure such that plosives would either be realized by nasal counterparts eg bd[ [m n] or [b d] may be nasalized and weak Voiceless plosives may be eitheraccompanied by nasal emission [p t k] or realized as glottal fricative [h]
Production of the target sentence lsquoI saw Sam sitting on a busrsquo might be
[aI (sk)ndeg O~ (sk)n
degaelig~m (sk)n
deg IhIn Aacute~n mouml~(sk)ndeg] passive processes and
[aI xO xaeligm xIkIIcirc AacuteIcirc goumlx] active processes
Contribution to surgical management decisions
Passiveactive interpretation of clinical assessments might facilitate surgical manage-ment decisions If noseholding does not facilitate correct production of targetconsonants then it is likely that an alternative articulatory pattern has becomephonologically established ie particular realizations for one or more targets areconsistently distributed in the phonological system These realizations may haveevolved because of initial diYculty producing articulatory targets and subsequentlystabilized within the phonological system Grundy and Harding (1995) refer to thisphenomenon as an lsquoarticulatory disorder with phonological consequencesrsquo
Therapy
Where obvious structural defects or diagnosed dysfunction exists clinicians fre-quently defer therapeutic intervention until surgery has been undertaken Theexpectation would be that normal structure and function is essential for normalspeech However pre-operative therapy may facilitate oral consonant productionwhich may serve to reduce hypernasal resonance Hence therapy prior to surgerymay avoid unnecessary surgery or reduce the extent of surgery required All activeprocesses are likely to require therapy
Principled selection of targets for therapy
Speech patterns frequently evidence a mixture of apparently passive and activeprocesses which complicates decisions about target selection Target selection can
A Harding and P Grunwell348
be based on assessment of which consonant targets can be most easily elicted inisolation (stimulability) This may lead to a sequence of target selection which isopposite to the sequence of consonant acquisition in normal development Forexample where reduced intra-oral pressure is present in a passive pattern [T] maybe easier to elicit in imitation than more nely grooved [s] or [S] Therapy maytarget [T] followed by [S ] and nally [s] As in non-cleft phonological therapywhere a class of consonants is aVected by the cleft then it is helpful to target theentire class The following decision-making process can be applied for both activeand passive processes
Decision making procedure for target selection
(1) Voiced versus voiceless targets(2) Front versus back placements(3) Syllable initial versus syllable nal targets(4) Plosives versus fricative targets
Voiceless plosives and fricatives are produced with an open glottis whichfacilitates topping up of air ow from the lungs hence voiceless plosive and fricativetargets are frequently more successful than voiced counterparts (Isshiki and Ringel1964) Front targets usually cause more diYculty than back particularly where analveolar defect or stula exists Contrary to normal development back targets maybe targeted before front Word- nal targets generally require less oral air pressurethan word initial targets and similarly fricatives may be more easily elicited thanplosives Fricatives do require a greater volume of air than plosives (Fletcher 1985)but in the presence of nasal escape weak fricative production appears to be morereadily achieved than weak plosive production Since nal fricatives would normallybe acquired in advance of word-initial fricatives (Ferguson 1978) targeting word- nal fricatives is frequently a productive starting point for therapy
Principles of therapy for passive processes
(1) Use of soft attack similar to gentle whisper for all target models ensuresminimal articulatory eVort (Harding and Grunwell 1993) and requires min-imal intra-oral air pressure It may be appropriate to gradually increase thearticulatory attack when the articulatory posture and evidence of intendedoral air ow have been established
(2) Slightly stretched duration of segment transitions in models of consonantto vowel (CndashV) or vowel to consonant (VndashC) facilitates review of motorplanning and extends the available time for execution of the new motorprogrammer whilst maintaining control of the oral airstream
(3) Noseholding can be used to provide exclusively oral air ow Gradual releaseof the nostrils during production of sustained [VVVVVf ] or [hhhhh ] allowsthe child to attempt to sustain an oral consonant despite increasing nasalemission This maximizes the use of available oral air ow Procedures forusing noseholding are described in some detail by Golding-Kushner (1995)
Principles of therapy for active processes
This is more like phonological therapy and can follow Grunwellrsquos (1991) processesfor phonological change and principled decision-making (Grunwell 1992) Some
Active versus passive cleft-type speech characteristics 349
examples are given here by way of illustration of ways to eVect the rst twoprocesses of change which may need to be approached diVerently in cleft palateversus non-cleft speech disorders DiVerent approaches may also be appropriate formodifying active versus passive cleft-type processes
Innovation production of new targets Some useful principles
(1) Introduction of new lsquonon-speech likersquo targets in sound play using a conson-ant sound segment model such as [ph ] note not a syllable like [p] whichis the type of pronunciation used when target sounds are presented as lettersfor reading Target [s] might be introduced as a lsquoTrain Slowing Down Noisersquo[ts ts ts tssssssss]
(2) lsquoNew consonantsrsquo can later be modelled and elicited in soft productions ofsyllable structure [tssssndashi] [ indashtssss] which can subsequently be identi ed assimilar to words lsquosearsquo and lsquoeatsrsquo
(3) lsquoDeferring responsibilityrsquo transfers responsibility or lsquoblamersquo for errors fromthe child and attributes it to the articulators eg lsquoyour tongue is havingtrouble with hellip rsquo lsquoLetrsquos show your tongue how to hellip rsquo
(4) New targets can be modelled repeatedly and recorded on audio or videotape which can be listened to at home
(5) Targeting classes of consonants (eg alveolars t d s n l voiceless fricativesf s S perhaps with aVricate T avoids phonological confusion whichmight occur if production ofsis achieved whilst other alveolar targetsremain backed The risk is that s might not integrate into the phonologicalsystem unless all backed alveolar consonants are destabilized
(6) Increased eye contact during auditory and production work can be invaluablein holding visual and auditory attention and ensures that visual informationabout the sound has been processed This is easily achieved by the clinicianlifting any focus of the childrsquos attention close to hisher mouth at theprecise moment when the target is modelled
Stimulation of non-speech related sounds such as a lsquoTrain Slowing DownNoisersquo [ts ts tsss] con rms that target [s] is physically achievable whether or not[ssss] can be imitated Some children continue to access [s] through the lsquoTrainSlowing Down Noisersquo throughout therapy until it is occurring spontaneouslywithout conscious planning This can be an eVective means of underminingestablished motor programmers (Hewlett 1990) for active cleft-type processes
Destabilizing active processes
As it is likely that children will be unaware of each occurrence of their alternativearticulatory pattern for speci c consonant errors it is preferrable to destabilizeactive processes with minimal conscious eVort by the child As children becomeaware of their mismatches they frequently add the newly acquired target realizationto their existing production eg target word tu childrsquos old realization [ku] childrsquoscorrected realization [t-ku] Destabilization can be achieved with minimal consciouseVort through input therapy techniques such as auditory bombardment (Lancasterand Pope 1989) auditory decision-making such as lsquowhich bear says this wordproperlyrsquo Red Bear says lsquotworsquo or Blue Bear says lsquocoorsquo This type of strategy oftenprecipitates attention to the target consonant with possible lsquoreplayrsquo and lsquoreviewrsquo of
A Harding and P Grunwell350
their own production Frequent stimulation of cognitive alertness to the targetconsonant can develop awareness without confronting the child with errors orrisking hisher failure The child is then free to attempt to repair hisher ownrealization to continue to re ect and to silently rehearse the adult realizationTraditional articulation therapy is thus combined with development of metaphonol-ogical skills ie the ability to re ect upon onersquos own speech production The resultshould be that new target realizations will be more phonologically stable thanexclusively production-based articulation therapy might have facilitated
Stabilizationgeneralization
Procedures to ensure stabilization and generalization of new target consonantswould be as described by Grunwell (1992) Success may be constrained by theconsiderable articulatory eVort sometimes required to maintain pressure consonantproduction in spontaneous speech (Harding and Grunwell 1993)
Conclusions
In speech assessment it is helpful to distinguish between errors which are cleft-type and non-cleft type and those which are part of active versus passive processesThe active and passive processes have been de ned and their phonological implica-tions discussed Focus on active and passive processes has facilitated focus on thephonological consequences of cleft palate on speech development In the futureawareness of the likely eVect of a cleft palate on normal phonological developmentcould avoid extended periods of unsuccessful clinical intervention Furthermoresensitivity to the relationship between phonological processes and structural con-straints should facilitate theoretically based management decisions Incidences suchas the case of CP in which nasal realizations were thought to indicate VPI but weresubsequently unaVected by surgery might be avoided if phonological analysiscontributes to management decisions
Surgery did improve hypernasal resonance and eliminated passive processes buthad little eVect on active processes Active processes in younger subjects werethought to require therapeutic intervention but in the longer term the oldersubjects showed few cleft-type processes Whilst it is possible that active cleft-typeprocesses may resolve with increasing age the implication for the future is thatactive cleft-type processes should be treated with skilled therapeutic interventionnot surgery Therapy which addresses the phonological consequences of cleft palateon speech development by combining metaphonologicalphonologicalarticulatoryapproaches is likely to be successful
References
Albery E 1991 Consonant articulation in the diVerent types of cleft lip and palate UnpublishedMPhil thesis Leicester Polytechnic
Albery E and Grunwell P 1993 Consonant articulation in diVerent types of cleft palate InP Grunwell (Ed) Analysing Cleft Palate Speech (London Whurr)
Ferguson C A 1978 Fricatives in child language acquisition In V Honsa and M Hardmann-Battista (Eds) Papers on Linguistics and Child Language (Mouton The Hague)
Fletcher S G 1985 Speech production and oral motor skill in an adult with an unrepaired palatalcleft Journal of Speech and Hearing Disorders 50 254ndash261
Active versus passive cleft-type speech characteristics 351
Golding-Kushner K J 1995 Treatment of articulation and resonancne disorders associated withcleft palate management and VPI In R Shprintzen (Ed) Cleft Palate Speech Management AMultidisciplinary Approach (St Louis Mosby)
Grundy K and Harding A 1995 Developmental speech disorders In K Grundy (Ed) Linguisticsin Clinical Practice (2nd edition) (London Whurr)
Grunwell P 1985 Phonological Assessment of Child Speech (Windsor NFER-Nelson)Grunwell P 1987a Clinical Phonology (2nd edition) (London Croom Helm)Grunwell P 1987b PACS Pictures Language Elicitation Materials (Windsor NFER-Nelson)Grunwell P 1991 Processes of phonological change in developmental speech disorders Clinical
Linguistics and Phonetics 6 101ndash122Grunwell P 1992 Principled decision making in the remediation of children with phonological
disorders In P Fletcher and D Hall (Eds) Specic Speech and Language Disorders in Children(London Whurr)
Grunwell P and Harding A 1995 PACSTOYS A Screening Assessment of Phonological Development(Windsor NFER-Nelson)
Grunwell P and Harding A 1996 A note on describing types of nasality Clinical Linguistics andPhonetics 10 157ndash161
Harding A 1993 An Investigation into the Relationship Between Timing of Cleft Palate Repairand Speech Development Unpublished PhD thesis
Harding A and Grunwell P 1993 The relationship between speech and timing of hard palaterepair In P Grunwell (Ed) Analysisng Cleft Palate Speech (London Whurr)
Harding A and Grunwell P 1996 Characteristics of cleft palate speech European Journal ofDisorders of Communication 31 331ndash358
Henningsson G and Isberg A M 1986 Velopharyngeal movement patterns in patients alternatingbetween oral and glottal articulation A clinical and cineradiographicical study Cleft Palate Journal23 1ndash9
Hewlett N 1990 Processes of development and production In P Grunwell (Ed) DevelopmentalSpeech Disorders (Edinburgh Churchill Livingstone)
Hotz M M Gnoinski W M Nussbaumer H and Kistler E 1978 Early orthopaedics in CLPcases guidelines for surgery Cleft Palate Journal 15 405ndash411
Hutters B and Brondsted K 1987 Strategies in cleft palate with special reference to DanishCleft Palate Journal 24 127ndash136
Isshiki N and Ringel R 1964 Airow during the production of selected consonants Journal ofSpeech and Hearing Research 7 233ndash244
Kummer A W Curtis C Wiggs M Lee L and Strife J L 1992 Comparison of velopharyngealgap size in patients with hypernasality hypernasality with nasal emission and nasal emissionor nasal turbulence (rustle) as the primary speech characteristic Cleft-palate-Craniofacial Journal29 152ndash156
Lancaster G and Pope L 1989 Working with Childrenrsquos Phonology (Oxford Winslow)Morley M E 1970 Cleft Palate and Speech (7th edition) (Edinburgh Churchill Livingstone)Russell V J 1991 Speech Development in Children with Cleft Lip and Palate Unpublished PhD
thesis Leicester PolytechnicRussell V J and Grunwell P 1993 Speech development in children with cleft lip and palate In
P Grunwell (Ed) Analysing Cleft Palate Speech (London Whurr)Sell D A and Grunwell P 1990 Speech results following late palatal surgery in previously
unoperated Sri Lankan adolescents with cleft palate Cleft Palate Journal 27 162ndash168Sell D Harding A and Grunwell P 1994 GOSSPASS A screening assessment of cleft palate
speech European Journal of Disorders of Communication 29 1ndash15Sell D Harding A and Grunwell P 1998 GOSSPASSrsquo98 An assessment for speech disorders
associated with cleft palate andor velopharyngeal dysfunction International Journal of Languageamp Communication Disorders ( in press)
Shorter E 1995 A spectographic analyis of child homophones Unpublished honours project DeMontfort University Leicester
Stenglehoffen J 1989 Nature and causes of communication diYculties In J Stengelhofen (Ed)Cleft Palate Nature and Remediation of Communication Problems (Edinburgh Churchill Livingstone)
Trost J E 1981 Articulatory additions to the classical description of the speech of persons withcleft palate Cleft Palate Journal 18
Trost-Cardamone J E 1990 The development of speech assessing cleft palate misarticulationsIn D A Kernahan and S N Rosenstein (Eds) Cleft Lip and Palate A System of Management(Baltimore Williams amp Wilkins)
A Harding and P Grunwell352
Appendix Active passive analysis of cleft palate speech

Active versus passive cleft-type speech characteristics 335
Figure 3 Active nasal fricative [ndegk]
1990) This characteristic has been found in speakers with no cleft palate historyoften with no explanation for its occurence
DiVerent places of articulation signalled placement contrasts between nasalfricative consonants in the same way that target nasal consonants [m n Icirc] arediVerentiated by place of articulation [m
degk] for f [n
degk] for s S Where a strong
backing process existed alveolar and post-alveolar fricatives were realized by velarnasal fricatives [ Daggerk
deg]
Occasionally nasal air ow was constricted such that nasal fricatives were pro-duced with a noisier turbulent quality [m
deg] [n
deg] [ Dagger] In a detailed assessment of cleft
pa la te speech GOSSPASSrsquo98 (Sell et al 1994 1998) these turbulent realizationswould be categorized in the resonance section as lsquonasal turbulence replacing conson-antsrsquo and in the cleft-type characteristics section as either lsquoactive nasal fricativesrsquo orpassive nasal realization of fricatives
Glottal articulation
[] frequently occurred in early plosive and aVricate production [p b t d T] up toage 46 Sometimes this process aVected only alveolar plosives t d in SIWI andSIWW position At times glottal stop represented voiced plosives [b d g] while[h] represented voiceless plosives [p t k] In SFWF position glottal stop representedboth voiced and voiceless plosives It may be the case that diVerent strengths ofglottal stop were used to distinguish voiceless and voiced plosives but this couldnot be reliably judged without spectographic analysis An undergraduate study ofspectographic analysis (Shorter 1995) of cleft palate speech identi ed some subtlediVerences in glottal stop productions which suggests a need for further investigationinto the phonological functions of glottal stops in cleft palate speech
Pharyngeal fricatives
[Eacute iquest] Early attempts at fricatives (ages 20ndash30) were frequently realized with acombination of posterior fricative cleft-type realizations (CTRs) Where plosiveswere exclusively glottal fricative consonants were frequently realized as pharyngeal
A Harding and P Grunwell336
fricatives In early phonological development obstruent realizations were commonlynon-oral but gradually moved anteriorly to uvular and velar positions Targetconsonants were not generally corrected independently of each other The gradualmovement of pharyngeal realizations towards oral uvularvelar articulation whichunderlines the relevance of a phonological interpretation of cleft palate speechcharacteristics
Exclusively pharyngealglottal patterns of articulation might imply velopharyn-geal insuYciency but it is noted here that all infants use pharyngeal and glottalarticulation until they acquire velopharyngeal competence during the rst 6 monthsof life It is possible for children with cleft palate to persist with this phoneticrepertoire for some time after palate repair Indeed such cases have been reportedby Russell and Grunwell (1993) Non-oral articulatory patterns indicate that thesphincter is not employed during speech which implies that the sphincter may notbe functional but unless oral air ow is consciously intended it cannot be assumedthat the sphincter is unable to function in speech (Henningsson and Isberg 1986)
Backing [k g q G]
A backing pattern is described by Stengelhofen (1989) as a lsquotendency for oralcontacts to be to the back of the oral cavityrsquo GOSSPASSrsquo98 (Sell et al 1998) makesa distinction here between backing to uvular and backing to velar place ofarticulation
E Backing to uvular [q G X Ograve ] Alveolar target consonants were backed touvular realizations and occasionally velar targets were backed to uvular Thepresence of velar and uvular realizations indicated the presence of some VPfunction but this might have been achieved with tongue humping In thedata acquisition of uvular and velar fricatives generally co-occurred withacquisition of f v which provides further evidence of velopharyngealfunction In the longitudinal study from age 16 to 46 subjects with bilateralclefts spent a period of months realizing all alveolar and post- alveolar voicedand voiceless consonant targets in uvular placement This degree of backingis deemed to be more severe and distracting for listeners than backing tovelar perhaps because uvular articulation is more distinctively non-EnglishHowever uvular fricatives are frequently used to achieve some meaningfulcontrasts which improve intelligibility
E Backing to velar In the younger subjects (aged 16ndash46) as articulatorypatterns progressed anteriorly a preference for [g] was common Mostcommonly backing resulted in t d realized as [k g] and s z as [x aring ]which contrasts with the fronting pattern seen in normal development
Double articulation
This is de ned as two simultaneous equal strictures at two places of articulationwhich was frequently noted in realizations of target alveolar consonants t d whenalveolarvelar contacts [tkk dkg] were used Double articulation may have beendeveloped to distinguish between alveolar and velar consonants in the presence ofa backing pattern Interestingly double articulation became evident in these develop-ing speech patterns with the emergence of fricative realizations Both plosives andfricatives tended to be realized with double articulation eg tndash[tkk] sndash[skagrave ]
Active versus passive cleft-type speech characteristics 337
Palatal fricatives [c J ]
These fricative realizations of alveolar target consonants appeared towards the endof the study period (ages 16ndash46) They were the most common realizations ofalveolar fricatives in older children (46ndash76 and 100ndash110) This nding was inaccordance with Alberyrsquos results (Albery 1991 Albery and Grunwell 1993)
Lateral fricatives [l Igrave]
As with palatal fricatives lateral fricatives were frequently present as realizations offricative consonant targets becoming particularly prevalent in later phonologicaldevelopment
Gliding of fricatives s S= [ j] or [w]
This phenomenon is seen in the non-cleft population as an uncommon develop-mental process (Grunwell 1987) It is classi ed here as an active process because[ j] was consistently produced as an apparently active alternative to target conson-ant(s) s z S [ j] is a normal consonant-like production in non-cleft babble whichcleft palate children often integrate into their phonological system It may betherefore that it is a persisting immaturity in the cleft palate population In thesedata [ j] was eVective in signalling a contrast between plosives and fricatives inSIWI position It functioned for the following consonants in diVerent speakers [ j]for S [ j] for m p f s z Ÿ h and co-articulation [hkj] for T
Passive cleft type processes
The criteria for passive cleft type processes is that they are (1) an attempt toproduce the correct articulatory placement and stricture (manner) which (2) failsbecause of a lack of intra-oral air pressure For example voiced plosives realized asnasals b[ [m] d[ [n] g[ [Icirc] No compensatory articulatory pattern hasbeen used to replace the intended consonant As the above examples demonstratetarget realizations often match a similar English consonant
Absence of pressure consonantspredominantly sonorant articulation
This phenomenon is de ned here as a pattern of articulation which was restrictedto English nasal and approximant articulations [m n Icirc w j] and [h] Some of thevoiced consonants were also employed as voiceless counterparts [m
degndeg Icircdeg ] thereby
increasing the range of available consonants for distribution in the phonologicalsystem Despite the limited consonant repertoire these patterns were often eVec-tively interpreted by close family members
Weak articulation [bV dV]
This category refers to normal articulatory movement in the production of obstruenttargets (plosive fricative and aVricate targets) which were produced with reducedoral air pressure and therefore articulation was considerably weakened In the speechsample data (ages 16ndash46) many target consonants were weakened to some degreeand at times may have been realised as nasals
A Harding and P Grunwell338
Passive nasal fricative [(fk)m (sk)ndeg]
Incomplete velopharyngeal closure inevitably reduces control of oral air ow with apassive loss of air ow and an increase of resonance in the nasal cavity Grunwelland Harding (1996) de ned the passively nasal fricative as an unreleased [(s)]double-articulated with a lowered voiceless nasal [n
Aacute
deg] This realization is the product
of an intended s with an unintended nasal air ow (see gure 4) The precisetranscription for a passive nasal transcription is [(sk)n
Aacute
deg] but an acceptable simpli cation
for transcription purposes is [(sk)ndeg] This is distinct from the active nasal fricative
which involves stopping of the oral air ow and active direction of air nasally whichcan be transcribed as a voiceless nasal with additional nasal emission [n
degk] Nasal
emission signals the fricative nature of for example target consonant s Thesetwo productions can sound the same and might initially be transcribed as [n
degk]
Nasendoscopic investigation of velopharyngeal activity during active and passivenasal realizations of s both show a lack of velopharyngeal closure It is predictedthat close examination by use of electropalatography might show slight diVerencesin tongue tip posture for an active and passive nasal fricative as illustrated in gures3 and 4 Passive nasal fricatives were converted into oral fricatives with nose-holding
Voiceless [h] for voiceless plosives
There was evidence that voiceless plosives were at times passively realized as [h]The consequence of reduced oral air pressure on production of voiceless plosivescan leave aspiration as the only perceptible distinctive feature This process usuallyaVected all voiceless plosive targets p t k Where this process was a passiveprocess use of noseholding during speech facilitated accurate target productionHowever it would also be possible for this distribution of [h] to be an active cleft-type process which would be part of a pharyngealglottal patternprocess
Nasal realization of voiced plosives b d g[ [m n Icirc]
Some subjects with residual clefts stulae or suspected VPI realized voiced conson-ants as nasal counterparts As summarized by Harding and Grunwell (1996) voiced
Figure 4 Passive nasal fricative [(sk)nAacute
deg]
Active versus passive cleft-type speech characteristics 339
consonants can be more diYcult to produce than voiceless consonants (Isshiki andRingel 1964) Distinction between active versus passive nasal realizations of plosivetargets was made in the same way that active and passive nasal fricatives weredistinguished by observing the eVect of noseholding on consonant production Inpassive nasal realizations noseholding facilitated normal consonant production(Golding-Kushner 1995)
Nasal emission accompanying consonants [pk sk]
Nasal emission was frequently heard accompanying consonants but on occasions itapparently replaced consonants It has been linked with velopharyngeal incompet-ence (VPI) (Kummer et al 1992)
Results
Comparison of activepassive processes in the speech data
Quantitative results of Hardingrsquos research into the relationship between timing ofsurgery and speech development have already been published (Harding andGrunwell 1993) The following interpretation of the data speci cally identi esactivepassive cleft-type processes in relation to oral structure in a wide age rangeof subjects (16ndash130) Tables 1 2 3 and 4 show the passive and active processeson the left-hand column and the subjectrsquos code along the top The code identi esthose subjects who were treated with 1-stage versus 2-stage surgery Comparisonof the 4 tables at age 46 (BCLP and UCLP) at age 90 and at age 130 illustratesa pattern of diminishing cleft-type processes with increasing age Irrespective ofsurgical timing few cleft-type processes remained at age 130 (table 4) A generalobservation was that earlier speech samples (ages 16ndash76) frequently combined
Table 1 Cleft-type processes in BCLP subjects at age 46 (studies 1 and 2)
1-stage surgery 2-stage surgery
A G Rf JW D B JF JG AB
Passive cleft-type processespredominantly sonorant articulation m
weak articulation m m m m m m m m
voiceless h for plosive m m m m m
nasal release of plosives m m m m m
nasal emission with consonants m m m m m m
passive nasal fricativeActive cleft-type processes
nasal fricatives m m m m m m m m
pharyngeal glottal articulation m m m m m m m m
backing to uvular m m m m m m m m
backing to velar m m m m m m m m m
lateral palatal fricatives m m m m m m m m m
double articulation m m m m m m m m m
gliding fricative m m
f=post-operative stula
A Harding and P Grunwell340
Table 2 Cleft-type processes in UCLP subjects at age 46 (study 2)
1-stage surgery 2-stage surgery
SE TB CK MS NC TS ZG CP
Passive cleft-type processespredominantly sonorant artic m
weak articulation m m m
voiceless h for plosives m m m
nasal release of plosives m m m
nasal emission with consonants m m
passive nasal fricative m m
Active cleft-type processesnasal fricativepharyngeal glottal articulation m m m
backing to uvular m
backing to velar m m
lateral palatal fricatives m m m m m
double articulation m m m m m m
gliding fricative m
Table 3 Cleft-type processes at age 90
2-stage surgery 2-stage surgery1-stage surgery completed at 4 yrs completed at 8 yrs
DAf SBf RL NR JD AR LJ RP MB
Passive cleft-type processespredominantly sonorant articweak articulation m
voiceless h for plosives m m
nasal release of plosives m m
nasal emission with consonants m m m m
passive nasal fricatives m m
Active cleft-type processesnasal fricatives m m
pharyngeal glottal articulation m m
backing to uvular m m
backing to velar m m m m m m m
lateral palatal fricatives m m m m m m m
double articulation m m m m m
gliding fricative m
f=subject had a stula
both active and passive strategies whereas later samples (ages 90ndash130) rarelyevidenced passive processes
At age 46 four out of ve BCLP subjects used active non-oral pharyngeal andglottal processes and oral velar and uvular fricatives irrespective of surgical status(see table 1) All had some anterior palatal defect which might have reduced theirpotential to achieve intra-oral pressure
By comparison two out of three partially repaired 2-stage UCLP subjects at age46 (table 2) showed evidence of passive processes This suggested that their
Active versus passive cleft-type speech characteristics 341
Tab
le4
Spee
chin
rela
tion
tosu
rgic
altim
ing
atag
e13
0
2-st
age
surg
ery
2-st
age
surg
ery
1-st
age
surg
ery
subj
ects
com
plet
edat
4yr
sco
mpl
eted
at8
yrs
1-A
1-B
1-C
1-D
1-E
1-F
24-
G2
4-H
24-
J2
8-K
28-
L2
8-M
Pass
ive
clef
t-ty
pepr
oces
ses
pred
omin
antly
sono
rant
artic
wea
kar
ticul
atio
nm
voic
eles
sh
fo
rpl
osiv
esna
sal
rele
ase
ofpl
osiv
esna
sal
emis
sion
with
cons
onan
tsm
pass
ive
nasa
lfr
icat
ives
Act
ive
clef
t-ty
pepr
oces
ses
nasa
lfr
icat
ives
phar
ynge
alg
lott
alar
ticul
atio
nba
ckin
gto
uvul
arba
ckin
gto
vela
rm
m
late
ral
pala
tal
fric
ativ
esm
mm
doub
lear
ticul
atio
ngl
idin
gfr
icat
ive
1=1-
stag
esu
rger
ysu
bjec
ts
24=
2-st
age
surg
ery
hard
pala
tere
pair
edat
abou
t4
yrs
28=
2-st
age
surg
ery
with
hard
pala
tere
pair
edat
abou
t8
yrs
A Harding and P Grunwell342
unrepaired hard palates had in fact restricted their phonetic repertoire imposing aneed for individual adaptability The additional active processes employed by thesesubjects were presumably a response to the restrictions imposed by their oro-nasalstructure and velopharyngeal function at the time of consonant acquisition Asshown in table 2 the most common active cleft-type processes persisting at age46 with a residual cleft of the hard palate were backing double articulation andlateralpalatal articulation Two 1-stage surgery subjects whose entire palates hadbeen repaired at ages 09 and 010 did not use any cleft-type processes at age 46
By age 90 (table 3) a much-diminished number of cleft type processes wasevident except in subjects with sizeable anterior stulae who had received littlespeech and language therapy A similarity was noted between the speech patternsof 1-stage surgery subjects with stulae (DA and SB) at age 90 (table 3) and theyounger BCLP subjects at age 46 (table 1) who also had anterior palatal defectsThey included non-oral realizations of t d s k g occasional nasal fricatives andpharyngealglottal articulations Fistulae had apparently continued to in uencearticulation and phonological development in these subjects
Finally at age 130 (table 4) the diVerences between 1-stage and 2-stage surgerysubjects had diminished leaving only one 2-stage subject with occasional backingand four subjects with slight palatal and lateral release of fricative consonants Onlytwo of the 1-stage surgery subjects were using minor distortions of grooved fricativeproduction
Whilst there were apparent trends in speech production relating to surgicaltiming and oral structure it is noted that there were exceptions to each tentativegeneralization Subjects with marked structural imperfections occasionally producedrealizations of which they would not have been thought capable and subjects withno visible imperfections produced inexplicably distorted speech patterns It istherefore concluded that whilst there is homogeneity in the range of processesproduced by this population assumptions cannot be made about speech based onsurgical timing or type of cleft Tentative predictions based on detailed assessmentmay be clinically very useful
EVects of surgery on speech
Activepassive processes have identi ed those cleft-type characteristics thought tobe associated with a physical inability to produce pressure consonants The followinganalysis of speech changes after surgical intervention at diVerent ages identi es thechanges eVected by surgery when intra-oral pressure could be more readily achieved
Two children were rst recorded prior to the rst stage of a 2-stage procedureTheir lips were repaired at approximately 6 months of age and soft palate repairwas carried out at ages 18 and 19 respectively Their hard palates were leftunrepaired to facilitate unrestricted growth of the mid-face (Hotz et al 1978) Pre-and post-operative consonant-like sounds present in the recorded speech samplesare listed in table 5 Interestingly prior to soft palate repair both these childrenproduced some oral consonants Subject B was producing pressure consonants [kg] in his babble prior to soft palate repair Considering that he had an unrepairedbilateral cleft palate at this point it was surprising that he had any oral consonantsPost-operatively at 20 years he used [b bkm t d g gkb] which indicated that surgeryto repair the soft palate had facilitated an increased range of oral pressure consonantsSubject D was producing [p b k g] pre-operatively Post-operatively following soft
Active versus passive cleft-type speech characteristics 343
Tab
le5
EV
ects
ofso
ftp
alat
ere
pair
atag
e1
6on
BC
LP
subj
ects
h
ard
pal
ate
rem
ain
sun
repa
ired
2-st
age
subj
ects
Surg
ery
Pre
-ope
rati
vesp
eech
patt
ern
atag
e1
6Po
st-o
pera
tive
chan
ges
insp
eech
atag
e2
0
Stud
y1
BSo
ftpa
late
repa
irat
16
Adu
ltta
rget
sk
gA
t2
0[b
b kmg kb
td
g]D
Soft
pala
tere
pair
17
Adu
ltta
rget
sp
bk
gA
t2
0[p
bd
b kdk
g]
Tab
le6
EV
ects
ofha
rdpa
late
rep
air
atag
e6
6an
d
stu
lare
pair
atag
e10
0
Subj
ect
Surg
ery
Pre
-ope
rati
vesp
eech
patt
ern
Post
-ope
rati
vech
ange
sin
spee
ch
MS
Har
dpa
late
repa
ir6
6Pa
ssiv
epr
oces
s7
6E
limin
ated
pass
ive
proc
ess
Var
iabl
ena
sal
rele
ase
ofco
nson
ants
Hyp
onas
alna
sals
JFH
ard
pala
tere
pair
(uns
ucce
ssfu
l)6
6Se
vera
lac
tive
and
pass
ive
proc
esse
s7
6A
ctiv
epr
oces
ses
rem
aine
dPa
ssiv
epr
oces
ses
elim
inat
ed
DA
Fis
tula
repa
ir10
0A
ctiv
epr
oces
ses
110
Elim
inat
ion
ofph
aryn
geal
glo
ttal
Var
iabi
lity+
+an
dna
sal
arti
cula
tion
Art
icul
ator
yva
riab
ility
++
Act
ive
CT
Rs
proc
esse
spe
rsis
t
A Harding and P Grunwell344
palate repair but with a residual cleft in the hard palate his range of consonantsincluded [d] which was particularly surprising since the hard palate remainedunrepaired Whilst it is unlikely that toddlers of 18 months could be consciouslytrying to compensate for articulatory inadequacy in producing velar plosives inbabble prior to soft palate repair and an alveolar plosive prior to hard palate repairboth these subjects showed evidence of actively pursuing their articulatory potential
Table 6 summarizes changes following surgery to repair the hard palate in moremature speech patterns These subjects who were aged 66 and 100 pre-operativelyhad learned to speak with residual clefts and were apparently unaware of theconsonant productions that failed to match normal production
Subject MS used only passive processes in his speech pattern He realized someconsonants nasally such that lsquoballrsquo was [mO~] and lsquosockrsquo was [(sk)n
deg Aacute~ k] Looking atpost-operative changes at age 76 his consonant production was normal but hisresonance had become hyponasal Pre-operatively at age 66 Subject JF was usingseveral active and passive processes The active processes were unaVected by surgerybut passive processes were eliminated
Fistula repair was carried out at age 100 on Subject DA who had many activeprocesses and very variable articulation pre-operatively Post-operatively at age110 he was not using non-oral pharyngeal and glottal active processes or nasalrealizations but many oral cleft-type realizations remained
As shown in table 7 hard palate re-repair and pharyngoplasty was carried outon two subjects whose hard palate repairs had been unsuccessful at approximately4 years Subject NC assessed pre-operatively at age 56 was using predominantlypassive processes in her speech She was also using [ j] for fricatives s S whichwas thought to be an active process At age 60 following hard palate re-repair andpharyngoplasty all cleft-type processes had been eliminated without post-operativespeech therapy Since [ j] for s apparently resolved spontaneously followingsurgery it can be assumed that this was a passive process in this speech sample
Subject CP who underwent this procedure presented pre-operatively at age 46with both passive and active processes but his nasal resonance was not consistentlyhypernasal In addition to his cleft-related speech disorder this subject had additionaldevelopmental speech diYculties which were identi ed as being unrelated to thecleft Post-operatively at age 56 little had changedmdashnotably the passive processnasal [m] for b was retained His nasal resonance had become hyponasal andthere was no apparent bene t from surgical intervention The realization of b as[m] had become phonologically stable and surgery alone had not destabilized thephonological system This realization may have been a passive product of VPI inearly speech acquisition which had subsequently become part of a phonologicaldisorder Post-operatively CPrsquos phonetic repertoire did increase but the phonologicaldistribution was variable Plosive targets were still realized as nasals in spontaneousspeech at the nal speech recording at age 76 This was not as an inevitableconsequence of VPI but a result of an inability to destabilize the phonologicalprocess determining that voiced plosives would be realized as nasals This resultfollowing surgery highlights the importance of identifying phonological learningproblems and distinguishing them from structural constraints on articulationIn CPrsquos case pre-operative exploration of the eVect of nares occlusion duringspeech might have indicated that structural change would not improve consonantproduction spontaneously
A general observation was that consonant realizations did not move rapidly
Active versus passive cleft-type speech characteristics 345
Tab
le7
EV
ects
ofha
rdpa
late
re-r
epai
ran
dp
hary
ngo
pla
sty
Subj
ect
Surg
ery
Pre
-ope
rati
vesp
eech
patt
ern
Post
-ope
rativ
ech
ange
sin
spee
ch
Stud
y2
NC
Har
dpa
late
re-r
epai
ran
d5
6Pa
ssiv
ecl
eft-
type
proc
esse
s6
0A
llcl
eft-
type
phar
yngo
plas
ty5
10[
j]
for
fric
ativ
espr
oces
ses
elim
inat
ed[
h]
for
plos
ives
SIW
IV
aria
ble
arti
cula
rypr
ecis
ion
CP
Har
dpa
late
repa
iran
d4
6Pa
ssiv
ean
dac
tive
proc
esse
s5
6Pa
ssiv
epr
oces
sph
aryn
gopl
asty
50
Pho
nolo
gica
lco
nfus
ion
[m]
for
[b
]re
tain
edH
ypon
asal
nasa
lsPe
rsis
ting
phon
olog
ical
conf
usio
ns
A Harding and P Grunwell346
from incorrect to correct but progressed incrementally towards normal realizationsas described by Morley (1970) Where an early realization of target s might beglottal [h] a gradual pattern of change showed subsequent realizations to bepharyngeal [Eacute] then uvular [X] then velar [x] and eventually palatal [c] or lateral [Euml]It was interesting to note that speech patterns continued to change as late as90ndash110 years with the result that diVerences related to surgical timing and cleft-type gradually disappeared Persisting stulae were thought to account for the mostmarked cleft type processes at age 90
Implications for surgical management
This analysis of speech changes following surgery suggests some implications forsurgical management which are compatible with Sell and Grunwellrsquos (1990) ndingsin the Sri Lankan study
Surgery can change passive speech processes but it is also possible that speechtherapy may be able to change passive patterns Surgery alone is unlikely to modifyactive cleft-type processes whereas speech therapy should be able to modify activeprocesses Indications from these case studies is that where speech is the primaryproblem speech assessment should distinguish between active and passive processesin order to evaluate the necessity for full investigations and to plan therapeuticintervention Where past speech therapy has not been successful it cannot beassumed that surgical intervention will facilitate further speech progress A furthercourse of speech therapy which is sensitive to active versus passive processes todevelopmental phonological in uences on cleft-type speech development and toarticulatory diYculties in diVerent speech contexts might facilitate optimal progressWhere structural imperfection exists it is quite possible for single-word productionto be more precise than target realizations in spontaneous speech This may not bea failure of phonological generalization (Grunwell 1992) but the result of diYcultysustaining the necessary lsquoarticulatory eVort rsquo (Harding and Grunwell 1993) resultingin articulatory imprecision Deteriorating articulatory accuracy should not be over-looked in interpretation of speech results
An analytical protocol
As a result of analysing the speech data and identifying the active and passiveprocesses a protocol has been developed which records examples of each cleft-typeprocess over a series of assessments It demonstrates the progression of individualprocesses towards an adult target (see the Appendix) At each assessment onecolumn is used to indicate nasal resonance nasal emission and nasal turbulenceratings and cleft-type processes Changes in the nature of error realizations mightshow progress towards target consonants Hence whilst the total correct scoremight not have increased increments of change can be observed This observationof patterns of change may function as an adjunct to GOSSPASSrsquo98 (Sell et al 1998)giving access to a greater depth of both quantitative and qualitative data aboutconsonant production in relation to resonance nasal emission nasal turbulenceoral structure and cleft-type
Active versus passive cleft-type speech characteristics 347
Diagnostic implications
Passive versus active nasal fricatives
The important management consideration related to this distinction is that an activenasal fricative is an established phonological process which is unlikely to be directlyaVected by surgery alone Therapy would be necessary to destabilize nasal realizationsof oral consonants In contrast passive nasal fricatives may be eliminated by surgeryOf particular relevance is diVerential diagnosis between passive and active nasalfricatives in surgical and therapeutic management When hypernasality co-occurswith nasal air ow during consonant production which can be redirected by nose-holding passive nasal fricatives are diagnosed These would be transcribed as [(sk)n
deg]
passive alveolar nasal fricatives [(Wk)mdeg
] bilabial nasal fricatives or [(fk)Iacutedeg ] labiodentalnasal fricatives Full VPI investigations would be recommended to diagnose thenature of the structural or functional de ciency and distinguish between velopharyn-geal incompetence and velopharyngeal mislearning
It is highly likely that plosive targets would be aVected by reduced intra-oral airpressure such that plosives would either be realized by nasal counterparts eg bd[ [m n] or [b d] may be nasalized and weak Voiceless plosives may be eitheraccompanied by nasal emission [p t k] or realized as glottal fricative [h]
Production of the target sentence lsquoI saw Sam sitting on a busrsquo might be
[aI (sk)ndeg O~ (sk)n
degaelig~m (sk)n
deg IhIn Aacute~n mouml~(sk)ndeg] passive processes and
[aI xO xaeligm xIkIIcirc AacuteIcirc goumlx] active processes
Contribution to surgical management decisions
Passiveactive interpretation of clinical assessments might facilitate surgical manage-ment decisions If noseholding does not facilitate correct production of targetconsonants then it is likely that an alternative articulatory pattern has becomephonologically established ie particular realizations for one or more targets areconsistently distributed in the phonological system These realizations may haveevolved because of initial diYculty producing articulatory targets and subsequentlystabilized within the phonological system Grundy and Harding (1995) refer to thisphenomenon as an lsquoarticulatory disorder with phonological consequencesrsquo
Therapy
Where obvious structural defects or diagnosed dysfunction exists clinicians fre-quently defer therapeutic intervention until surgery has been undertaken Theexpectation would be that normal structure and function is essential for normalspeech However pre-operative therapy may facilitate oral consonant productionwhich may serve to reduce hypernasal resonance Hence therapy prior to surgerymay avoid unnecessary surgery or reduce the extent of surgery required All activeprocesses are likely to require therapy
Principled selection of targets for therapy
Speech patterns frequently evidence a mixture of apparently passive and activeprocesses which complicates decisions about target selection Target selection can
A Harding and P Grunwell348
be based on assessment of which consonant targets can be most easily elicted inisolation (stimulability) This may lead to a sequence of target selection which isopposite to the sequence of consonant acquisition in normal development Forexample where reduced intra-oral pressure is present in a passive pattern [T] maybe easier to elicit in imitation than more nely grooved [s] or [S] Therapy maytarget [T] followed by [S ] and nally [s] As in non-cleft phonological therapywhere a class of consonants is aVected by the cleft then it is helpful to target theentire class The following decision-making process can be applied for both activeand passive processes
Decision making procedure for target selection
(1) Voiced versus voiceless targets(2) Front versus back placements(3) Syllable initial versus syllable nal targets(4) Plosives versus fricative targets
Voiceless plosives and fricatives are produced with an open glottis whichfacilitates topping up of air ow from the lungs hence voiceless plosive and fricativetargets are frequently more successful than voiced counterparts (Isshiki and Ringel1964) Front targets usually cause more diYculty than back particularly where analveolar defect or stula exists Contrary to normal development back targets maybe targeted before front Word- nal targets generally require less oral air pressurethan word initial targets and similarly fricatives may be more easily elicited thanplosives Fricatives do require a greater volume of air than plosives (Fletcher 1985)but in the presence of nasal escape weak fricative production appears to be morereadily achieved than weak plosive production Since nal fricatives would normallybe acquired in advance of word-initial fricatives (Ferguson 1978) targeting word- nal fricatives is frequently a productive starting point for therapy
Principles of therapy for passive processes
(1) Use of soft attack similar to gentle whisper for all target models ensuresminimal articulatory eVort (Harding and Grunwell 1993) and requires min-imal intra-oral air pressure It may be appropriate to gradually increase thearticulatory attack when the articulatory posture and evidence of intendedoral air ow have been established
(2) Slightly stretched duration of segment transitions in models of consonantto vowel (CndashV) or vowel to consonant (VndashC) facilitates review of motorplanning and extends the available time for execution of the new motorprogrammer whilst maintaining control of the oral airstream
(3) Noseholding can be used to provide exclusively oral air ow Gradual releaseof the nostrils during production of sustained [VVVVVf ] or [hhhhh ] allowsthe child to attempt to sustain an oral consonant despite increasing nasalemission This maximizes the use of available oral air ow Procedures forusing noseholding are described in some detail by Golding-Kushner (1995)
Principles of therapy for active processes
This is more like phonological therapy and can follow Grunwellrsquos (1991) processesfor phonological change and principled decision-making (Grunwell 1992) Some
Active versus passive cleft-type speech characteristics 349
examples are given here by way of illustration of ways to eVect the rst twoprocesses of change which may need to be approached diVerently in cleft palateversus non-cleft speech disorders DiVerent approaches may also be appropriate formodifying active versus passive cleft-type processes
Innovation production of new targets Some useful principles
(1) Introduction of new lsquonon-speech likersquo targets in sound play using a conson-ant sound segment model such as [ph ] note not a syllable like [p] whichis the type of pronunciation used when target sounds are presented as lettersfor reading Target [s] might be introduced as a lsquoTrain Slowing Down Noisersquo[ts ts ts tssssssss]
(2) lsquoNew consonantsrsquo can later be modelled and elicited in soft productions ofsyllable structure [tssssndashi] [ indashtssss] which can subsequently be identi ed assimilar to words lsquosearsquo and lsquoeatsrsquo
(3) lsquoDeferring responsibilityrsquo transfers responsibility or lsquoblamersquo for errors fromthe child and attributes it to the articulators eg lsquoyour tongue is havingtrouble with hellip rsquo lsquoLetrsquos show your tongue how to hellip rsquo
(4) New targets can be modelled repeatedly and recorded on audio or videotape which can be listened to at home
(5) Targeting classes of consonants (eg alveolars t d s n l voiceless fricativesf s S perhaps with aVricate T avoids phonological confusion whichmight occur if production ofsis achieved whilst other alveolar targetsremain backed The risk is that s might not integrate into the phonologicalsystem unless all backed alveolar consonants are destabilized
(6) Increased eye contact during auditory and production work can be invaluablein holding visual and auditory attention and ensures that visual informationabout the sound has been processed This is easily achieved by the clinicianlifting any focus of the childrsquos attention close to hisher mouth at theprecise moment when the target is modelled
Stimulation of non-speech related sounds such as a lsquoTrain Slowing DownNoisersquo [ts ts tsss] con rms that target [s] is physically achievable whether or not[ssss] can be imitated Some children continue to access [s] through the lsquoTrainSlowing Down Noisersquo throughout therapy until it is occurring spontaneouslywithout conscious planning This can be an eVective means of underminingestablished motor programmers (Hewlett 1990) for active cleft-type processes
Destabilizing active processes
As it is likely that children will be unaware of each occurrence of their alternativearticulatory pattern for speci c consonant errors it is preferrable to destabilizeactive processes with minimal conscious eVort by the child As children becomeaware of their mismatches they frequently add the newly acquired target realizationto their existing production eg target word tu childrsquos old realization [ku] childrsquoscorrected realization [t-ku] Destabilization can be achieved with minimal consciouseVort through input therapy techniques such as auditory bombardment (Lancasterand Pope 1989) auditory decision-making such as lsquowhich bear says this wordproperlyrsquo Red Bear says lsquotworsquo or Blue Bear says lsquocoorsquo This type of strategy oftenprecipitates attention to the target consonant with possible lsquoreplayrsquo and lsquoreviewrsquo of
A Harding and P Grunwell350
their own production Frequent stimulation of cognitive alertness to the targetconsonant can develop awareness without confronting the child with errors orrisking hisher failure The child is then free to attempt to repair hisher ownrealization to continue to re ect and to silently rehearse the adult realizationTraditional articulation therapy is thus combined with development of metaphonol-ogical skills ie the ability to re ect upon onersquos own speech production The resultshould be that new target realizations will be more phonologically stable thanexclusively production-based articulation therapy might have facilitated
Stabilizationgeneralization
Procedures to ensure stabilization and generalization of new target consonantswould be as described by Grunwell (1992) Success may be constrained by theconsiderable articulatory eVort sometimes required to maintain pressure consonantproduction in spontaneous speech (Harding and Grunwell 1993)
Conclusions
In speech assessment it is helpful to distinguish between errors which are cleft-type and non-cleft type and those which are part of active versus passive processesThe active and passive processes have been de ned and their phonological implica-tions discussed Focus on active and passive processes has facilitated focus on thephonological consequences of cleft palate on speech development In the futureawareness of the likely eVect of a cleft palate on normal phonological developmentcould avoid extended periods of unsuccessful clinical intervention Furthermoresensitivity to the relationship between phonological processes and structural con-straints should facilitate theoretically based management decisions Incidences suchas the case of CP in which nasal realizations were thought to indicate VPI but weresubsequently unaVected by surgery might be avoided if phonological analysiscontributes to management decisions
Surgery did improve hypernasal resonance and eliminated passive processes buthad little eVect on active processes Active processes in younger subjects werethought to require therapeutic intervention but in the longer term the oldersubjects showed few cleft-type processes Whilst it is possible that active cleft-typeprocesses may resolve with increasing age the implication for the future is thatactive cleft-type processes should be treated with skilled therapeutic interventionnot surgery Therapy which addresses the phonological consequences of cleft palateon speech development by combining metaphonologicalphonologicalarticulatoryapproaches is likely to be successful
References
Albery E 1991 Consonant articulation in the diVerent types of cleft lip and palate UnpublishedMPhil thesis Leicester Polytechnic
Albery E and Grunwell P 1993 Consonant articulation in diVerent types of cleft palate InP Grunwell (Ed) Analysing Cleft Palate Speech (London Whurr)
Ferguson C A 1978 Fricatives in child language acquisition In V Honsa and M Hardmann-Battista (Eds) Papers on Linguistics and Child Language (Mouton The Hague)
Fletcher S G 1985 Speech production and oral motor skill in an adult with an unrepaired palatalcleft Journal of Speech and Hearing Disorders 50 254ndash261
Active versus passive cleft-type speech characteristics 351
Golding-Kushner K J 1995 Treatment of articulation and resonancne disorders associated withcleft palate management and VPI In R Shprintzen (Ed) Cleft Palate Speech Management AMultidisciplinary Approach (St Louis Mosby)
Grundy K and Harding A 1995 Developmental speech disorders In K Grundy (Ed) Linguisticsin Clinical Practice (2nd edition) (London Whurr)
Grunwell P 1985 Phonological Assessment of Child Speech (Windsor NFER-Nelson)Grunwell P 1987a Clinical Phonology (2nd edition) (London Croom Helm)Grunwell P 1987b PACS Pictures Language Elicitation Materials (Windsor NFER-Nelson)Grunwell P 1991 Processes of phonological change in developmental speech disorders Clinical
Linguistics and Phonetics 6 101ndash122Grunwell P 1992 Principled decision making in the remediation of children with phonological
disorders In P Fletcher and D Hall (Eds) Specic Speech and Language Disorders in Children(London Whurr)
Grunwell P and Harding A 1995 PACSTOYS A Screening Assessment of Phonological Development(Windsor NFER-Nelson)
Grunwell P and Harding A 1996 A note on describing types of nasality Clinical Linguistics andPhonetics 10 157ndash161
Harding A 1993 An Investigation into the Relationship Between Timing of Cleft Palate Repairand Speech Development Unpublished PhD thesis
Harding A and Grunwell P 1993 The relationship between speech and timing of hard palaterepair In P Grunwell (Ed) Analysisng Cleft Palate Speech (London Whurr)
Harding A and Grunwell P 1996 Characteristics of cleft palate speech European Journal ofDisorders of Communication 31 331ndash358
Henningsson G and Isberg A M 1986 Velopharyngeal movement patterns in patients alternatingbetween oral and glottal articulation A clinical and cineradiographicical study Cleft Palate Journal23 1ndash9
Hewlett N 1990 Processes of development and production In P Grunwell (Ed) DevelopmentalSpeech Disorders (Edinburgh Churchill Livingstone)
Hotz M M Gnoinski W M Nussbaumer H and Kistler E 1978 Early orthopaedics in CLPcases guidelines for surgery Cleft Palate Journal 15 405ndash411
Hutters B and Brondsted K 1987 Strategies in cleft palate with special reference to DanishCleft Palate Journal 24 127ndash136
Isshiki N and Ringel R 1964 Airow during the production of selected consonants Journal ofSpeech and Hearing Research 7 233ndash244
Kummer A W Curtis C Wiggs M Lee L and Strife J L 1992 Comparison of velopharyngealgap size in patients with hypernasality hypernasality with nasal emission and nasal emissionor nasal turbulence (rustle) as the primary speech characteristic Cleft-palate-Craniofacial Journal29 152ndash156
Lancaster G and Pope L 1989 Working with Childrenrsquos Phonology (Oxford Winslow)Morley M E 1970 Cleft Palate and Speech (7th edition) (Edinburgh Churchill Livingstone)Russell V J 1991 Speech Development in Children with Cleft Lip and Palate Unpublished PhD
thesis Leicester PolytechnicRussell V J and Grunwell P 1993 Speech development in children with cleft lip and palate In
P Grunwell (Ed) Analysing Cleft Palate Speech (London Whurr)Sell D A and Grunwell P 1990 Speech results following late palatal surgery in previously
unoperated Sri Lankan adolescents with cleft palate Cleft Palate Journal 27 162ndash168Sell D Harding A and Grunwell P 1994 GOSSPASS A screening assessment of cleft palate
speech European Journal of Disorders of Communication 29 1ndash15Sell D Harding A and Grunwell P 1998 GOSSPASSrsquo98 An assessment for speech disorders
associated with cleft palate andor velopharyngeal dysfunction International Journal of Languageamp Communication Disorders ( in press)
Shorter E 1995 A spectographic analyis of child homophones Unpublished honours project DeMontfort University Leicester
Stenglehoffen J 1989 Nature and causes of communication diYculties In J Stengelhofen (Ed)Cleft Palate Nature and Remediation of Communication Problems (Edinburgh Churchill Livingstone)
Trost J E 1981 Articulatory additions to the classical description of the speech of persons withcleft palate Cleft Palate Journal 18
Trost-Cardamone J E 1990 The development of speech assessing cleft palate misarticulationsIn D A Kernahan and S N Rosenstein (Eds) Cleft Lip and Palate A System of Management(Baltimore Williams amp Wilkins)
A Harding and P Grunwell352
Appendix Active passive analysis of cleft palate speech

A Harding and P Grunwell336
fricatives In early phonological development obstruent realizations were commonlynon-oral but gradually moved anteriorly to uvular and velar positions Targetconsonants were not generally corrected independently of each other The gradualmovement of pharyngeal realizations towards oral uvularvelar articulation whichunderlines the relevance of a phonological interpretation of cleft palate speechcharacteristics
Exclusively pharyngealglottal patterns of articulation might imply velopharyn-geal insuYciency but it is noted here that all infants use pharyngeal and glottalarticulation until they acquire velopharyngeal competence during the rst 6 monthsof life It is possible for children with cleft palate to persist with this phoneticrepertoire for some time after palate repair Indeed such cases have been reportedby Russell and Grunwell (1993) Non-oral articulatory patterns indicate that thesphincter is not employed during speech which implies that the sphincter may notbe functional but unless oral air ow is consciously intended it cannot be assumedthat the sphincter is unable to function in speech (Henningsson and Isberg 1986)
Backing [k g q G]
A backing pattern is described by Stengelhofen (1989) as a lsquotendency for oralcontacts to be to the back of the oral cavityrsquo GOSSPASSrsquo98 (Sell et al 1998) makesa distinction here between backing to uvular and backing to velar place ofarticulation
E Backing to uvular [q G X Ograve ] Alveolar target consonants were backed touvular realizations and occasionally velar targets were backed to uvular Thepresence of velar and uvular realizations indicated the presence of some VPfunction but this might have been achieved with tongue humping In thedata acquisition of uvular and velar fricatives generally co-occurred withacquisition of f v which provides further evidence of velopharyngealfunction In the longitudinal study from age 16 to 46 subjects with bilateralclefts spent a period of months realizing all alveolar and post- alveolar voicedand voiceless consonant targets in uvular placement This degree of backingis deemed to be more severe and distracting for listeners than backing tovelar perhaps because uvular articulation is more distinctively non-EnglishHowever uvular fricatives are frequently used to achieve some meaningfulcontrasts which improve intelligibility
E Backing to velar In the younger subjects (aged 16ndash46) as articulatorypatterns progressed anteriorly a preference for [g] was common Mostcommonly backing resulted in t d realized as [k g] and s z as [x aring ]which contrasts with the fronting pattern seen in normal development
Double articulation
This is de ned as two simultaneous equal strictures at two places of articulationwhich was frequently noted in realizations of target alveolar consonants t d whenalveolarvelar contacts [tkk dkg] were used Double articulation may have beendeveloped to distinguish between alveolar and velar consonants in the presence ofa backing pattern Interestingly double articulation became evident in these develop-ing speech patterns with the emergence of fricative realizations Both plosives andfricatives tended to be realized with double articulation eg tndash[tkk] sndash[skagrave ]
Active versus passive cleft-type speech characteristics 337
Palatal fricatives [c J ]
These fricative realizations of alveolar target consonants appeared towards the endof the study period (ages 16ndash46) They were the most common realizations ofalveolar fricatives in older children (46ndash76 and 100ndash110) This nding was inaccordance with Alberyrsquos results (Albery 1991 Albery and Grunwell 1993)
Lateral fricatives [l Igrave]
As with palatal fricatives lateral fricatives were frequently present as realizations offricative consonant targets becoming particularly prevalent in later phonologicaldevelopment
Gliding of fricatives s S= [ j] or [w]
This phenomenon is seen in the non-cleft population as an uncommon develop-mental process (Grunwell 1987) It is classi ed here as an active process because[ j] was consistently produced as an apparently active alternative to target conson-ant(s) s z S [ j] is a normal consonant-like production in non-cleft babble whichcleft palate children often integrate into their phonological system It may betherefore that it is a persisting immaturity in the cleft palate population In thesedata [ j] was eVective in signalling a contrast between plosives and fricatives inSIWI position It functioned for the following consonants in diVerent speakers [ j]for S [ j] for m p f s z Ÿ h and co-articulation [hkj] for T
Passive cleft type processes
The criteria for passive cleft type processes is that they are (1) an attempt toproduce the correct articulatory placement and stricture (manner) which (2) failsbecause of a lack of intra-oral air pressure For example voiced plosives realized asnasals b[ [m] d[ [n] g[ [Icirc] No compensatory articulatory pattern hasbeen used to replace the intended consonant As the above examples demonstratetarget realizations often match a similar English consonant
Absence of pressure consonantspredominantly sonorant articulation
This phenomenon is de ned here as a pattern of articulation which was restrictedto English nasal and approximant articulations [m n Icirc w j] and [h] Some of thevoiced consonants were also employed as voiceless counterparts [m
degndeg Icircdeg ] thereby
increasing the range of available consonants for distribution in the phonologicalsystem Despite the limited consonant repertoire these patterns were often eVec-tively interpreted by close family members
Weak articulation [bV dV]
This category refers to normal articulatory movement in the production of obstruenttargets (plosive fricative and aVricate targets) which were produced with reducedoral air pressure and therefore articulation was considerably weakened In the speechsample data (ages 16ndash46) many target consonants were weakened to some degreeand at times may have been realised as nasals
A Harding and P Grunwell338
Passive nasal fricative [(fk)m (sk)ndeg]
Incomplete velopharyngeal closure inevitably reduces control of oral air ow with apassive loss of air ow and an increase of resonance in the nasal cavity Grunwelland Harding (1996) de ned the passively nasal fricative as an unreleased [(s)]double-articulated with a lowered voiceless nasal [n
Aacute
deg] This realization is the product
of an intended s with an unintended nasal air ow (see gure 4) The precisetranscription for a passive nasal transcription is [(sk)n
Aacute
deg] but an acceptable simpli cation
for transcription purposes is [(sk)ndeg] This is distinct from the active nasal fricative
which involves stopping of the oral air ow and active direction of air nasally whichcan be transcribed as a voiceless nasal with additional nasal emission [n
degk] Nasal
emission signals the fricative nature of for example target consonant s Thesetwo productions can sound the same and might initially be transcribed as [n
degk]
Nasendoscopic investigation of velopharyngeal activity during active and passivenasal realizations of s both show a lack of velopharyngeal closure It is predictedthat close examination by use of electropalatography might show slight diVerencesin tongue tip posture for an active and passive nasal fricative as illustrated in gures3 and 4 Passive nasal fricatives were converted into oral fricatives with nose-holding
Voiceless [h] for voiceless plosives
There was evidence that voiceless plosives were at times passively realized as [h]The consequence of reduced oral air pressure on production of voiceless plosivescan leave aspiration as the only perceptible distinctive feature This process usuallyaVected all voiceless plosive targets p t k Where this process was a passiveprocess use of noseholding during speech facilitated accurate target productionHowever it would also be possible for this distribution of [h] to be an active cleft-type process which would be part of a pharyngealglottal patternprocess
Nasal realization of voiced plosives b d g[ [m n Icirc]
Some subjects with residual clefts stulae or suspected VPI realized voiced conson-ants as nasal counterparts As summarized by Harding and Grunwell (1996) voiced
Figure 4 Passive nasal fricative [(sk)nAacute
deg]
Active versus passive cleft-type speech characteristics 339
consonants can be more diYcult to produce than voiceless consonants (Isshiki andRingel 1964) Distinction between active versus passive nasal realizations of plosivetargets was made in the same way that active and passive nasal fricatives weredistinguished by observing the eVect of noseholding on consonant production Inpassive nasal realizations noseholding facilitated normal consonant production(Golding-Kushner 1995)
Nasal emission accompanying consonants [pk sk]
Nasal emission was frequently heard accompanying consonants but on occasions itapparently replaced consonants It has been linked with velopharyngeal incompet-ence (VPI) (Kummer et al 1992)
Results
Comparison of activepassive processes in the speech data
Quantitative results of Hardingrsquos research into the relationship between timing ofsurgery and speech development have already been published (Harding andGrunwell 1993) The following interpretation of the data speci cally identi esactivepassive cleft-type processes in relation to oral structure in a wide age rangeof subjects (16ndash130) Tables 1 2 3 and 4 show the passive and active processeson the left-hand column and the subjectrsquos code along the top The code identi esthose subjects who were treated with 1-stage versus 2-stage surgery Comparisonof the 4 tables at age 46 (BCLP and UCLP) at age 90 and at age 130 illustratesa pattern of diminishing cleft-type processes with increasing age Irrespective ofsurgical timing few cleft-type processes remained at age 130 (table 4) A generalobservation was that earlier speech samples (ages 16ndash76) frequently combined
Table 1 Cleft-type processes in BCLP subjects at age 46 (studies 1 and 2)
1-stage surgery 2-stage surgery
A G Rf JW D B JF JG AB
Passive cleft-type processespredominantly sonorant articulation m
weak articulation m m m m m m m m
voiceless h for plosive m m m m m
nasal release of plosives m m m m m
nasal emission with consonants m m m m m m
passive nasal fricativeActive cleft-type processes
nasal fricatives m m m m m m m m
pharyngeal glottal articulation m m m m m m m m
backing to uvular m m m m m m m m
backing to velar m m m m m m m m m
lateral palatal fricatives m m m m m m m m m
double articulation m m m m m m m m m
gliding fricative m m
f=post-operative stula
A Harding and P Grunwell340
Table 2 Cleft-type processes in UCLP subjects at age 46 (study 2)
1-stage surgery 2-stage surgery
SE TB CK MS NC TS ZG CP
Passive cleft-type processespredominantly sonorant artic m
weak articulation m m m
voiceless h for plosives m m m
nasal release of plosives m m m
nasal emission with consonants m m
passive nasal fricative m m
Active cleft-type processesnasal fricativepharyngeal glottal articulation m m m
backing to uvular m
backing to velar m m
lateral palatal fricatives m m m m m
double articulation m m m m m m
gliding fricative m
Table 3 Cleft-type processes at age 90
2-stage surgery 2-stage surgery1-stage surgery completed at 4 yrs completed at 8 yrs
DAf SBf RL NR JD AR LJ RP MB
Passive cleft-type processespredominantly sonorant articweak articulation m
voiceless h for plosives m m
nasal release of plosives m m
nasal emission with consonants m m m m
passive nasal fricatives m m
Active cleft-type processesnasal fricatives m m
pharyngeal glottal articulation m m
backing to uvular m m
backing to velar m m m m m m m
lateral palatal fricatives m m m m m m m
double articulation m m m m m
gliding fricative m
f=subject had a stula
both active and passive strategies whereas later samples (ages 90ndash130) rarelyevidenced passive processes
At age 46 four out of ve BCLP subjects used active non-oral pharyngeal andglottal processes and oral velar and uvular fricatives irrespective of surgical status(see table 1) All had some anterior palatal defect which might have reduced theirpotential to achieve intra-oral pressure
By comparison two out of three partially repaired 2-stage UCLP subjects at age46 (table 2) showed evidence of passive processes This suggested that their
Active versus passive cleft-type speech characteristics 341
Tab
le4
Spee
chin
rela
tion
tosu
rgic
altim
ing
atag
e13
0
2-st
age
surg
ery
2-st
age
surg
ery
1-st
age
surg
ery
subj
ects
com
plet
edat
4yr
sco
mpl
eted
at8
yrs
1-A
1-B
1-C
1-D
1-E
1-F
24-
G2
4-H
24-
J2
8-K
28-
L2
8-M
Pass
ive
clef
t-ty
pepr
oces
ses
pred
omin
antly
sono
rant
artic
wea
kar
ticul
atio
nm
voic
eles
sh
fo
rpl
osiv
esna
sal
rele
ase
ofpl
osiv
esna
sal
emis
sion
with
cons
onan
tsm
pass
ive
nasa
lfr
icat
ives
Act
ive
clef
t-ty
pepr
oces
ses
nasa
lfr
icat
ives
phar
ynge
alg
lott
alar
ticul
atio
nba
ckin
gto
uvul
arba
ckin
gto
vela
rm
m
late
ral
pala
tal
fric
ativ
esm
mm
doub
lear
ticul
atio
ngl
idin
gfr
icat
ive
1=1-
stag
esu
rger
ysu
bjec
ts
24=
2-st
age
surg
ery
hard
pala
tere
pair
edat
abou
t4
yrs
28=
2-st
age
surg
ery
with
hard
pala
tere
pair
edat
abou
t8
yrs
A Harding and P Grunwell342
unrepaired hard palates had in fact restricted their phonetic repertoire imposing aneed for individual adaptability The additional active processes employed by thesesubjects were presumably a response to the restrictions imposed by their oro-nasalstructure and velopharyngeal function at the time of consonant acquisition Asshown in table 2 the most common active cleft-type processes persisting at age46 with a residual cleft of the hard palate were backing double articulation andlateralpalatal articulation Two 1-stage surgery subjects whose entire palates hadbeen repaired at ages 09 and 010 did not use any cleft-type processes at age 46
By age 90 (table 3) a much-diminished number of cleft type processes wasevident except in subjects with sizeable anterior stulae who had received littlespeech and language therapy A similarity was noted between the speech patternsof 1-stage surgery subjects with stulae (DA and SB) at age 90 (table 3) and theyounger BCLP subjects at age 46 (table 1) who also had anterior palatal defectsThey included non-oral realizations of t d s k g occasional nasal fricatives andpharyngealglottal articulations Fistulae had apparently continued to in uencearticulation and phonological development in these subjects
Finally at age 130 (table 4) the diVerences between 1-stage and 2-stage surgerysubjects had diminished leaving only one 2-stage subject with occasional backingand four subjects with slight palatal and lateral release of fricative consonants Onlytwo of the 1-stage surgery subjects were using minor distortions of grooved fricativeproduction
Whilst there were apparent trends in speech production relating to surgicaltiming and oral structure it is noted that there were exceptions to each tentativegeneralization Subjects with marked structural imperfections occasionally producedrealizations of which they would not have been thought capable and subjects withno visible imperfections produced inexplicably distorted speech patterns It istherefore concluded that whilst there is homogeneity in the range of processesproduced by this population assumptions cannot be made about speech based onsurgical timing or type of cleft Tentative predictions based on detailed assessmentmay be clinically very useful
EVects of surgery on speech
Activepassive processes have identi ed those cleft-type characteristics thought tobe associated with a physical inability to produce pressure consonants The followinganalysis of speech changes after surgical intervention at diVerent ages identi es thechanges eVected by surgery when intra-oral pressure could be more readily achieved
Two children were rst recorded prior to the rst stage of a 2-stage procedureTheir lips were repaired at approximately 6 months of age and soft palate repairwas carried out at ages 18 and 19 respectively Their hard palates were leftunrepaired to facilitate unrestricted growth of the mid-face (Hotz et al 1978) Pre-and post-operative consonant-like sounds present in the recorded speech samplesare listed in table 5 Interestingly prior to soft palate repair both these childrenproduced some oral consonants Subject B was producing pressure consonants [kg] in his babble prior to soft palate repair Considering that he had an unrepairedbilateral cleft palate at this point it was surprising that he had any oral consonantsPost-operatively at 20 years he used [b bkm t d g gkb] which indicated that surgeryto repair the soft palate had facilitated an increased range of oral pressure consonantsSubject D was producing [p b k g] pre-operatively Post-operatively following soft
Active versus passive cleft-type speech characteristics 343
Tab
le5
EV
ects
ofso
ftp
alat
ere
pair
atag
e1
6on
BC
LP
subj
ects
h
ard
pal
ate
rem
ain
sun
repa
ired
2-st
age
subj
ects
Surg
ery
Pre
-ope
rati
vesp
eech
patt
ern
atag
e1
6Po
st-o
pera
tive
chan
ges
insp
eech
atag
e2
0
Stud
y1
BSo
ftpa
late
repa
irat
16
Adu
ltta
rget
sk
gA
t2
0[b
b kmg kb
td
g]D
Soft
pala
tere
pair
17
Adu
ltta
rget
sp
bk
gA
t2
0[p
bd
b kdk
g]
Tab
le6
EV
ects
ofha
rdpa
late
rep
air
atag
e6
6an
d
stu
lare
pair
atag
e10
0
Subj
ect
Surg
ery
Pre
-ope
rati
vesp
eech
patt
ern
Post
-ope
rati
vech
ange
sin
spee
ch
MS
Har
dpa
late
repa
ir6
6Pa
ssiv
epr
oces
s7
6E
limin
ated
pass
ive
proc
ess
Var
iabl
ena
sal
rele
ase
ofco
nson
ants
Hyp
onas
alna
sals
JFH
ard
pala
tere
pair
(uns
ucce
ssfu
l)6
6Se
vera
lac
tive
and
pass
ive
proc
esse
s7
6A
ctiv
epr
oces
ses
rem
aine
dPa
ssiv
epr
oces
ses
elim
inat
ed
DA
Fis
tula
repa
ir10
0A
ctiv
epr
oces
ses
110
Elim
inat
ion
ofph
aryn
geal
glo
ttal
Var
iabi
lity+
+an
dna
sal
arti
cula
tion
Art
icul
ator
yva
riab
ility
++
Act
ive
CT
Rs
proc
esse
spe
rsis
t
A Harding and P Grunwell344
palate repair but with a residual cleft in the hard palate his range of consonantsincluded [d] which was particularly surprising since the hard palate remainedunrepaired Whilst it is unlikely that toddlers of 18 months could be consciouslytrying to compensate for articulatory inadequacy in producing velar plosives inbabble prior to soft palate repair and an alveolar plosive prior to hard palate repairboth these subjects showed evidence of actively pursuing their articulatory potential
Table 6 summarizes changes following surgery to repair the hard palate in moremature speech patterns These subjects who were aged 66 and 100 pre-operativelyhad learned to speak with residual clefts and were apparently unaware of theconsonant productions that failed to match normal production
Subject MS used only passive processes in his speech pattern He realized someconsonants nasally such that lsquoballrsquo was [mO~] and lsquosockrsquo was [(sk)n
deg Aacute~ k] Looking atpost-operative changes at age 76 his consonant production was normal but hisresonance had become hyponasal Pre-operatively at age 66 Subject JF was usingseveral active and passive processes The active processes were unaVected by surgerybut passive processes were eliminated
Fistula repair was carried out at age 100 on Subject DA who had many activeprocesses and very variable articulation pre-operatively Post-operatively at age110 he was not using non-oral pharyngeal and glottal active processes or nasalrealizations but many oral cleft-type realizations remained
As shown in table 7 hard palate re-repair and pharyngoplasty was carried outon two subjects whose hard palate repairs had been unsuccessful at approximately4 years Subject NC assessed pre-operatively at age 56 was using predominantlypassive processes in her speech She was also using [ j] for fricatives s S whichwas thought to be an active process At age 60 following hard palate re-repair andpharyngoplasty all cleft-type processes had been eliminated without post-operativespeech therapy Since [ j] for s apparently resolved spontaneously followingsurgery it can be assumed that this was a passive process in this speech sample
Subject CP who underwent this procedure presented pre-operatively at age 46with both passive and active processes but his nasal resonance was not consistentlyhypernasal In addition to his cleft-related speech disorder this subject had additionaldevelopmental speech diYculties which were identi ed as being unrelated to thecleft Post-operatively at age 56 little had changedmdashnotably the passive processnasal [m] for b was retained His nasal resonance had become hyponasal andthere was no apparent bene t from surgical intervention The realization of b as[m] had become phonologically stable and surgery alone had not destabilized thephonological system This realization may have been a passive product of VPI inearly speech acquisition which had subsequently become part of a phonologicaldisorder Post-operatively CPrsquos phonetic repertoire did increase but the phonologicaldistribution was variable Plosive targets were still realized as nasals in spontaneousspeech at the nal speech recording at age 76 This was not as an inevitableconsequence of VPI but a result of an inability to destabilize the phonologicalprocess determining that voiced plosives would be realized as nasals This resultfollowing surgery highlights the importance of identifying phonological learningproblems and distinguishing them from structural constraints on articulationIn CPrsquos case pre-operative exploration of the eVect of nares occlusion duringspeech might have indicated that structural change would not improve consonantproduction spontaneously
A general observation was that consonant realizations did not move rapidly
Active versus passive cleft-type speech characteristics 345
Tab
le7
EV
ects
ofha
rdpa
late
re-r
epai
ran
dp
hary
ngo
pla
sty
Subj
ect
Surg
ery
Pre
-ope
rati
vesp
eech
patt
ern
Post
-ope
rativ
ech
ange
sin
spee
ch
Stud
y2
NC
Har
dpa
late
re-r
epai
ran
d5
6Pa
ssiv
ecl
eft-
type
proc
esse
s6
0A
llcl
eft-
type
phar
yngo
plas
ty5
10[
j]
for
fric
ativ
espr
oces
ses
elim
inat
ed[
h]
for
plos
ives
SIW
IV
aria
ble
arti
cula
rypr
ecis
ion
CP
Har
dpa
late
repa
iran
d4
6Pa
ssiv
ean
dac
tive
proc
esse
s5
6Pa
ssiv
epr
oces
sph
aryn
gopl
asty
50
Pho
nolo
gica
lco
nfus
ion
[m]
for
[b
]re
tain
edH
ypon
asal
nasa
lsPe
rsis
ting
phon
olog
ical
conf
usio
ns
A Harding and P Grunwell346
from incorrect to correct but progressed incrementally towards normal realizationsas described by Morley (1970) Where an early realization of target s might beglottal [h] a gradual pattern of change showed subsequent realizations to bepharyngeal [Eacute] then uvular [X] then velar [x] and eventually palatal [c] or lateral [Euml]It was interesting to note that speech patterns continued to change as late as90ndash110 years with the result that diVerences related to surgical timing and cleft-type gradually disappeared Persisting stulae were thought to account for the mostmarked cleft type processes at age 90
Implications for surgical management
This analysis of speech changes following surgery suggests some implications forsurgical management which are compatible with Sell and Grunwellrsquos (1990) ndingsin the Sri Lankan study
Surgery can change passive speech processes but it is also possible that speechtherapy may be able to change passive patterns Surgery alone is unlikely to modifyactive cleft-type processes whereas speech therapy should be able to modify activeprocesses Indications from these case studies is that where speech is the primaryproblem speech assessment should distinguish between active and passive processesin order to evaluate the necessity for full investigations and to plan therapeuticintervention Where past speech therapy has not been successful it cannot beassumed that surgical intervention will facilitate further speech progress A furthercourse of speech therapy which is sensitive to active versus passive processes todevelopmental phonological in uences on cleft-type speech development and toarticulatory diYculties in diVerent speech contexts might facilitate optimal progressWhere structural imperfection exists it is quite possible for single-word productionto be more precise than target realizations in spontaneous speech This may not bea failure of phonological generalization (Grunwell 1992) but the result of diYcultysustaining the necessary lsquoarticulatory eVort rsquo (Harding and Grunwell 1993) resultingin articulatory imprecision Deteriorating articulatory accuracy should not be over-looked in interpretation of speech results
An analytical protocol
As a result of analysing the speech data and identifying the active and passiveprocesses a protocol has been developed which records examples of each cleft-typeprocess over a series of assessments It demonstrates the progression of individualprocesses towards an adult target (see the Appendix) At each assessment onecolumn is used to indicate nasal resonance nasal emission and nasal turbulenceratings and cleft-type processes Changes in the nature of error realizations mightshow progress towards target consonants Hence whilst the total correct scoremight not have increased increments of change can be observed This observationof patterns of change may function as an adjunct to GOSSPASSrsquo98 (Sell et al 1998)giving access to a greater depth of both quantitative and qualitative data aboutconsonant production in relation to resonance nasal emission nasal turbulenceoral structure and cleft-type
Active versus passive cleft-type speech characteristics 347
Diagnostic implications
Passive versus active nasal fricatives
The important management consideration related to this distinction is that an activenasal fricative is an established phonological process which is unlikely to be directlyaVected by surgery alone Therapy would be necessary to destabilize nasal realizationsof oral consonants In contrast passive nasal fricatives may be eliminated by surgeryOf particular relevance is diVerential diagnosis between passive and active nasalfricatives in surgical and therapeutic management When hypernasality co-occurswith nasal air ow during consonant production which can be redirected by nose-holding passive nasal fricatives are diagnosed These would be transcribed as [(sk)n
deg]
passive alveolar nasal fricatives [(Wk)mdeg
] bilabial nasal fricatives or [(fk)Iacutedeg ] labiodentalnasal fricatives Full VPI investigations would be recommended to diagnose thenature of the structural or functional de ciency and distinguish between velopharyn-geal incompetence and velopharyngeal mislearning
It is highly likely that plosive targets would be aVected by reduced intra-oral airpressure such that plosives would either be realized by nasal counterparts eg bd[ [m n] or [b d] may be nasalized and weak Voiceless plosives may be eitheraccompanied by nasal emission [p t k] or realized as glottal fricative [h]
Production of the target sentence lsquoI saw Sam sitting on a busrsquo might be
[aI (sk)ndeg O~ (sk)n
degaelig~m (sk)n
deg IhIn Aacute~n mouml~(sk)ndeg] passive processes and
[aI xO xaeligm xIkIIcirc AacuteIcirc goumlx] active processes
Contribution to surgical management decisions
Passiveactive interpretation of clinical assessments might facilitate surgical manage-ment decisions If noseholding does not facilitate correct production of targetconsonants then it is likely that an alternative articulatory pattern has becomephonologically established ie particular realizations for one or more targets areconsistently distributed in the phonological system These realizations may haveevolved because of initial diYculty producing articulatory targets and subsequentlystabilized within the phonological system Grundy and Harding (1995) refer to thisphenomenon as an lsquoarticulatory disorder with phonological consequencesrsquo
Therapy
Where obvious structural defects or diagnosed dysfunction exists clinicians fre-quently defer therapeutic intervention until surgery has been undertaken Theexpectation would be that normal structure and function is essential for normalspeech However pre-operative therapy may facilitate oral consonant productionwhich may serve to reduce hypernasal resonance Hence therapy prior to surgerymay avoid unnecessary surgery or reduce the extent of surgery required All activeprocesses are likely to require therapy
Principled selection of targets for therapy
Speech patterns frequently evidence a mixture of apparently passive and activeprocesses which complicates decisions about target selection Target selection can
A Harding and P Grunwell348
be based on assessment of which consonant targets can be most easily elicted inisolation (stimulability) This may lead to a sequence of target selection which isopposite to the sequence of consonant acquisition in normal development Forexample where reduced intra-oral pressure is present in a passive pattern [T] maybe easier to elicit in imitation than more nely grooved [s] or [S] Therapy maytarget [T] followed by [S ] and nally [s] As in non-cleft phonological therapywhere a class of consonants is aVected by the cleft then it is helpful to target theentire class The following decision-making process can be applied for both activeand passive processes
Decision making procedure for target selection
(1) Voiced versus voiceless targets(2) Front versus back placements(3) Syllable initial versus syllable nal targets(4) Plosives versus fricative targets
Voiceless plosives and fricatives are produced with an open glottis whichfacilitates topping up of air ow from the lungs hence voiceless plosive and fricativetargets are frequently more successful than voiced counterparts (Isshiki and Ringel1964) Front targets usually cause more diYculty than back particularly where analveolar defect or stula exists Contrary to normal development back targets maybe targeted before front Word- nal targets generally require less oral air pressurethan word initial targets and similarly fricatives may be more easily elicited thanplosives Fricatives do require a greater volume of air than plosives (Fletcher 1985)but in the presence of nasal escape weak fricative production appears to be morereadily achieved than weak plosive production Since nal fricatives would normallybe acquired in advance of word-initial fricatives (Ferguson 1978) targeting word- nal fricatives is frequently a productive starting point for therapy
Principles of therapy for passive processes
(1) Use of soft attack similar to gentle whisper for all target models ensuresminimal articulatory eVort (Harding and Grunwell 1993) and requires min-imal intra-oral air pressure It may be appropriate to gradually increase thearticulatory attack when the articulatory posture and evidence of intendedoral air ow have been established
(2) Slightly stretched duration of segment transitions in models of consonantto vowel (CndashV) or vowel to consonant (VndashC) facilitates review of motorplanning and extends the available time for execution of the new motorprogrammer whilst maintaining control of the oral airstream
(3) Noseholding can be used to provide exclusively oral air ow Gradual releaseof the nostrils during production of sustained [VVVVVf ] or [hhhhh ] allowsthe child to attempt to sustain an oral consonant despite increasing nasalemission This maximizes the use of available oral air ow Procedures forusing noseholding are described in some detail by Golding-Kushner (1995)
Principles of therapy for active processes
This is more like phonological therapy and can follow Grunwellrsquos (1991) processesfor phonological change and principled decision-making (Grunwell 1992) Some
Active versus passive cleft-type speech characteristics 349
examples are given here by way of illustration of ways to eVect the rst twoprocesses of change which may need to be approached diVerently in cleft palateversus non-cleft speech disorders DiVerent approaches may also be appropriate formodifying active versus passive cleft-type processes
Innovation production of new targets Some useful principles
(1) Introduction of new lsquonon-speech likersquo targets in sound play using a conson-ant sound segment model such as [ph ] note not a syllable like [p] whichis the type of pronunciation used when target sounds are presented as lettersfor reading Target [s] might be introduced as a lsquoTrain Slowing Down Noisersquo[ts ts ts tssssssss]
(2) lsquoNew consonantsrsquo can later be modelled and elicited in soft productions ofsyllable structure [tssssndashi] [ indashtssss] which can subsequently be identi ed assimilar to words lsquosearsquo and lsquoeatsrsquo
(3) lsquoDeferring responsibilityrsquo transfers responsibility or lsquoblamersquo for errors fromthe child and attributes it to the articulators eg lsquoyour tongue is havingtrouble with hellip rsquo lsquoLetrsquos show your tongue how to hellip rsquo
(4) New targets can be modelled repeatedly and recorded on audio or videotape which can be listened to at home
(5) Targeting classes of consonants (eg alveolars t d s n l voiceless fricativesf s S perhaps with aVricate T avoids phonological confusion whichmight occur if production ofsis achieved whilst other alveolar targetsremain backed The risk is that s might not integrate into the phonologicalsystem unless all backed alveolar consonants are destabilized
(6) Increased eye contact during auditory and production work can be invaluablein holding visual and auditory attention and ensures that visual informationabout the sound has been processed This is easily achieved by the clinicianlifting any focus of the childrsquos attention close to hisher mouth at theprecise moment when the target is modelled
Stimulation of non-speech related sounds such as a lsquoTrain Slowing DownNoisersquo [ts ts tsss] con rms that target [s] is physically achievable whether or not[ssss] can be imitated Some children continue to access [s] through the lsquoTrainSlowing Down Noisersquo throughout therapy until it is occurring spontaneouslywithout conscious planning This can be an eVective means of underminingestablished motor programmers (Hewlett 1990) for active cleft-type processes
Destabilizing active processes
As it is likely that children will be unaware of each occurrence of their alternativearticulatory pattern for speci c consonant errors it is preferrable to destabilizeactive processes with minimal conscious eVort by the child As children becomeaware of their mismatches they frequently add the newly acquired target realizationto their existing production eg target word tu childrsquos old realization [ku] childrsquoscorrected realization [t-ku] Destabilization can be achieved with minimal consciouseVort through input therapy techniques such as auditory bombardment (Lancasterand Pope 1989) auditory decision-making such as lsquowhich bear says this wordproperlyrsquo Red Bear says lsquotworsquo or Blue Bear says lsquocoorsquo This type of strategy oftenprecipitates attention to the target consonant with possible lsquoreplayrsquo and lsquoreviewrsquo of
A Harding and P Grunwell350
their own production Frequent stimulation of cognitive alertness to the targetconsonant can develop awareness without confronting the child with errors orrisking hisher failure The child is then free to attempt to repair hisher ownrealization to continue to re ect and to silently rehearse the adult realizationTraditional articulation therapy is thus combined with development of metaphonol-ogical skills ie the ability to re ect upon onersquos own speech production The resultshould be that new target realizations will be more phonologically stable thanexclusively production-based articulation therapy might have facilitated
Stabilizationgeneralization
Procedures to ensure stabilization and generalization of new target consonantswould be as described by Grunwell (1992) Success may be constrained by theconsiderable articulatory eVort sometimes required to maintain pressure consonantproduction in spontaneous speech (Harding and Grunwell 1993)
Conclusions
In speech assessment it is helpful to distinguish between errors which are cleft-type and non-cleft type and those which are part of active versus passive processesThe active and passive processes have been de ned and their phonological implica-tions discussed Focus on active and passive processes has facilitated focus on thephonological consequences of cleft palate on speech development In the futureawareness of the likely eVect of a cleft palate on normal phonological developmentcould avoid extended periods of unsuccessful clinical intervention Furthermoresensitivity to the relationship between phonological processes and structural con-straints should facilitate theoretically based management decisions Incidences suchas the case of CP in which nasal realizations were thought to indicate VPI but weresubsequently unaVected by surgery might be avoided if phonological analysiscontributes to management decisions
Surgery did improve hypernasal resonance and eliminated passive processes buthad little eVect on active processes Active processes in younger subjects werethought to require therapeutic intervention but in the longer term the oldersubjects showed few cleft-type processes Whilst it is possible that active cleft-typeprocesses may resolve with increasing age the implication for the future is thatactive cleft-type processes should be treated with skilled therapeutic interventionnot surgery Therapy which addresses the phonological consequences of cleft palateon speech development by combining metaphonologicalphonologicalarticulatoryapproaches is likely to be successful
References
Albery E 1991 Consonant articulation in the diVerent types of cleft lip and palate UnpublishedMPhil thesis Leicester Polytechnic
Albery E and Grunwell P 1993 Consonant articulation in diVerent types of cleft palate InP Grunwell (Ed) Analysing Cleft Palate Speech (London Whurr)
Ferguson C A 1978 Fricatives in child language acquisition In V Honsa and M Hardmann-Battista (Eds) Papers on Linguistics and Child Language (Mouton The Hague)
Fletcher S G 1985 Speech production and oral motor skill in an adult with an unrepaired palatalcleft Journal of Speech and Hearing Disorders 50 254ndash261
Active versus passive cleft-type speech characteristics 351
Golding-Kushner K J 1995 Treatment of articulation and resonancne disorders associated withcleft palate management and VPI In R Shprintzen (Ed) Cleft Palate Speech Management AMultidisciplinary Approach (St Louis Mosby)
Grundy K and Harding A 1995 Developmental speech disorders In K Grundy (Ed) Linguisticsin Clinical Practice (2nd edition) (London Whurr)
Grunwell P 1985 Phonological Assessment of Child Speech (Windsor NFER-Nelson)Grunwell P 1987a Clinical Phonology (2nd edition) (London Croom Helm)Grunwell P 1987b PACS Pictures Language Elicitation Materials (Windsor NFER-Nelson)Grunwell P 1991 Processes of phonological change in developmental speech disorders Clinical
Linguistics and Phonetics 6 101ndash122Grunwell P 1992 Principled decision making in the remediation of children with phonological
disorders In P Fletcher and D Hall (Eds) Specic Speech and Language Disorders in Children(London Whurr)
Grunwell P and Harding A 1995 PACSTOYS A Screening Assessment of Phonological Development(Windsor NFER-Nelson)
Grunwell P and Harding A 1996 A note on describing types of nasality Clinical Linguistics andPhonetics 10 157ndash161
Harding A 1993 An Investigation into the Relationship Between Timing of Cleft Palate Repairand Speech Development Unpublished PhD thesis
Harding A and Grunwell P 1993 The relationship between speech and timing of hard palaterepair In P Grunwell (Ed) Analysisng Cleft Palate Speech (London Whurr)
Harding A and Grunwell P 1996 Characteristics of cleft palate speech European Journal ofDisorders of Communication 31 331ndash358
Henningsson G and Isberg A M 1986 Velopharyngeal movement patterns in patients alternatingbetween oral and glottal articulation A clinical and cineradiographicical study Cleft Palate Journal23 1ndash9
Hewlett N 1990 Processes of development and production In P Grunwell (Ed) DevelopmentalSpeech Disorders (Edinburgh Churchill Livingstone)
Hotz M M Gnoinski W M Nussbaumer H and Kistler E 1978 Early orthopaedics in CLPcases guidelines for surgery Cleft Palate Journal 15 405ndash411
Hutters B and Brondsted K 1987 Strategies in cleft palate with special reference to DanishCleft Palate Journal 24 127ndash136
Isshiki N and Ringel R 1964 Airow during the production of selected consonants Journal ofSpeech and Hearing Research 7 233ndash244
Kummer A W Curtis C Wiggs M Lee L and Strife J L 1992 Comparison of velopharyngealgap size in patients with hypernasality hypernasality with nasal emission and nasal emissionor nasal turbulence (rustle) as the primary speech characteristic Cleft-palate-Craniofacial Journal29 152ndash156
Lancaster G and Pope L 1989 Working with Childrenrsquos Phonology (Oxford Winslow)Morley M E 1970 Cleft Palate and Speech (7th edition) (Edinburgh Churchill Livingstone)Russell V J 1991 Speech Development in Children with Cleft Lip and Palate Unpublished PhD
thesis Leicester PolytechnicRussell V J and Grunwell P 1993 Speech development in children with cleft lip and palate In
P Grunwell (Ed) Analysing Cleft Palate Speech (London Whurr)Sell D A and Grunwell P 1990 Speech results following late palatal surgery in previously
unoperated Sri Lankan adolescents with cleft palate Cleft Palate Journal 27 162ndash168Sell D Harding A and Grunwell P 1994 GOSSPASS A screening assessment of cleft palate
speech European Journal of Disorders of Communication 29 1ndash15Sell D Harding A and Grunwell P 1998 GOSSPASSrsquo98 An assessment for speech disorders
associated with cleft palate andor velopharyngeal dysfunction International Journal of Languageamp Communication Disorders ( in press)
Shorter E 1995 A spectographic analyis of child homophones Unpublished honours project DeMontfort University Leicester
Stenglehoffen J 1989 Nature and causes of communication diYculties In J Stengelhofen (Ed)Cleft Palate Nature and Remediation of Communication Problems (Edinburgh Churchill Livingstone)
Trost J E 1981 Articulatory additions to the classical description of the speech of persons withcleft palate Cleft Palate Journal 18
Trost-Cardamone J E 1990 The development of speech assessing cleft palate misarticulationsIn D A Kernahan and S N Rosenstein (Eds) Cleft Lip and Palate A System of Management(Baltimore Williams amp Wilkins)
A Harding and P Grunwell352
Appendix Active passive analysis of cleft palate speech

Active versus passive cleft-type speech characteristics 337
Palatal fricatives [c J ]
These fricative realizations of alveolar target consonants appeared towards the endof the study period (ages 16ndash46) They were the most common realizations ofalveolar fricatives in older children (46ndash76 and 100ndash110) This nding was inaccordance with Alberyrsquos results (Albery 1991 Albery and Grunwell 1993)
Lateral fricatives [l Igrave]
As with palatal fricatives lateral fricatives were frequently present as realizations offricative consonant targets becoming particularly prevalent in later phonologicaldevelopment
Gliding of fricatives s S= [ j] or [w]
This phenomenon is seen in the non-cleft population as an uncommon develop-mental process (Grunwell 1987) It is classi ed here as an active process because[ j] was consistently produced as an apparently active alternative to target conson-ant(s) s z S [ j] is a normal consonant-like production in non-cleft babble whichcleft palate children often integrate into their phonological system It may betherefore that it is a persisting immaturity in the cleft palate population In thesedata [ j] was eVective in signalling a contrast between plosives and fricatives inSIWI position It functioned for the following consonants in diVerent speakers [ j]for S [ j] for m p f s z Ÿ h and co-articulation [hkj] for T
Passive cleft type processes
The criteria for passive cleft type processes is that they are (1) an attempt toproduce the correct articulatory placement and stricture (manner) which (2) failsbecause of a lack of intra-oral air pressure For example voiced plosives realized asnasals b[ [m] d[ [n] g[ [Icirc] No compensatory articulatory pattern hasbeen used to replace the intended consonant As the above examples demonstratetarget realizations often match a similar English consonant
Absence of pressure consonantspredominantly sonorant articulation
This phenomenon is de ned here as a pattern of articulation which was restrictedto English nasal and approximant articulations [m n Icirc w j] and [h] Some of thevoiced consonants were also employed as voiceless counterparts [m
degndeg Icircdeg ] thereby
increasing the range of available consonants for distribution in the phonologicalsystem Despite the limited consonant repertoire these patterns were often eVec-tively interpreted by close family members
Weak articulation [bV dV]
This category refers to normal articulatory movement in the production of obstruenttargets (plosive fricative and aVricate targets) which were produced with reducedoral air pressure and therefore articulation was considerably weakened In the speechsample data (ages 16ndash46) many target consonants were weakened to some degreeand at times may have been realised as nasals
A Harding and P Grunwell338
Passive nasal fricative [(fk)m (sk)ndeg]
Incomplete velopharyngeal closure inevitably reduces control of oral air ow with apassive loss of air ow and an increase of resonance in the nasal cavity Grunwelland Harding (1996) de ned the passively nasal fricative as an unreleased [(s)]double-articulated with a lowered voiceless nasal [n
Aacute
deg] This realization is the product
of an intended s with an unintended nasal air ow (see gure 4) The precisetranscription for a passive nasal transcription is [(sk)n
Aacute
deg] but an acceptable simpli cation
for transcription purposes is [(sk)ndeg] This is distinct from the active nasal fricative
which involves stopping of the oral air ow and active direction of air nasally whichcan be transcribed as a voiceless nasal with additional nasal emission [n
degk] Nasal
emission signals the fricative nature of for example target consonant s Thesetwo productions can sound the same and might initially be transcribed as [n
degk]
Nasendoscopic investigation of velopharyngeal activity during active and passivenasal realizations of s both show a lack of velopharyngeal closure It is predictedthat close examination by use of electropalatography might show slight diVerencesin tongue tip posture for an active and passive nasal fricative as illustrated in gures3 and 4 Passive nasal fricatives were converted into oral fricatives with nose-holding
Voiceless [h] for voiceless plosives
There was evidence that voiceless plosives were at times passively realized as [h]The consequence of reduced oral air pressure on production of voiceless plosivescan leave aspiration as the only perceptible distinctive feature This process usuallyaVected all voiceless plosive targets p t k Where this process was a passiveprocess use of noseholding during speech facilitated accurate target productionHowever it would also be possible for this distribution of [h] to be an active cleft-type process which would be part of a pharyngealglottal patternprocess
Nasal realization of voiced plosives b d g[ [m n Icirc]
Some subjects with residual clefts stulae or suspected VPI realized voiced conson-ants as nasal counterparts As summarized by Harding and Grunwell (1996) voiced
Figure 4 Passive nasal fricative [(sk)nAacute
deg]
Active versus passive cleft-type speech characteristics 339
consonants can be more diYcult to produce than voiceless consonants (Isshiki andRingel 1964) Distinction between active versus passive nasal realizations of plosivetargets was made in the same way that active and passive nasal fricatives weredistinguished by observing the eVect of noseholding on consonant production Inpassive nasal realizations noseholding facilitated normal consonant production(Golding-Kushner 1995)
Nasal emission accompanying consonants [pk sk]
Nasal emission was frequently heard accompanying consonants but on occasions itapparently replaced consonants It has been linked with velopharyngeal incompet-ence (VPI) (Kummer et al 1992)
Results
Comparison of activepassive processes in the speech data
Quantitative results of Hardingrsquos research into the relationship between timing ofsurgery and speech development have already been published (Harding andGrunwell 1993) The following interpretation of the data speci cally identi esactivepassive cleft-type processes in relation to oral structure in a wide age rangeof subjects (16ndash130) Tables 1 2 3 and 4 show the passive and active processeson the left-hand column and the subjectrsquos code along the top The code identi esthose subjects who were treated with 1-stage versus 2-stage surgery Comparisonof the 4 tables at age 46 (BCLP and UCLP) at age 90 and at age 130 illustratesa pattern of diminishing cleft-type processes with increasing age Irrespective ofsurgical timing few cleft-type processes remained at age 130 (table 4) A generalobservation was that earlier speech samples (ages 16ndash76) frequently combined
Table 1 Cleft-type processes in BCLP subjects at age 46 (studies 1 and 2)
1-stage surgery 2-stage surgery
A G Rf JW D B JF JG AB
Passive cleft-type processespredominantly sonorant articulation m
weak articulation m m m m m m m m
voiceless h for plosive m m m m m
nasal release of plosives m m m m m
nasal emission with consonants m m m m m m
passive nasal fricativeActive cleft-type processes
nasal fricatives m m m m m m m m
pharyngeal glottal articulation m m m m m m m m
backing to uvular m m m m m m m m
backing to velar m m m m m m m m m
lateral palatal fricatives m m m m m m m m m
double articulation m m m m m m m m m
gliding fricative m m
f=post-operative stula
A Harding and P Grunwell340
Table 2 Cleft-type processes in UCLP subjects at age 46 (study 2)
1-stage surgery 2-stage surgery
SE TB CK MS NC TS ZG CP
Passive cleft-type processespredominantly sonorant artic m
weak articulation m m m
voiceless h for plosives m m m
nasal release of plosives m m m
nasal emission with consonants m m
passive nasal fricative m m
Active cleft-type processesnasal fricativepharyngeal glottal articulation m m m
backing to uvular m
backing to velar m m
lateral palatal fricatives m m m m m
double articulation m m m m m m
gliding fricative m
Table 3 Cleft-type processes at age 90
2-stage surgery 2-stage surgery1-stage surgery completed at 4 yrs completed at 8 yrs
DAf SBf RL NR JD AR LJ RP MB
Passive cleft-type processespredominantly sonorant articweak articulation m
voiceless h for plosives m m
nasal release of plosives m m
nasal emission with consonants m m m m
passive nasal fricatives m m
Active cleft-type processesnasal fricatives m m
pharyngeal glottal articulation m m
backing to uvular m m
backing to velar m m m m m m m
lateral palatal fricatives m m m m m m m
double articulation m m m m m
gliding fricative m
f=subject had a stula
both active and passive strategies whereas later samples (ages 90ndash130) rarelyevidenced passive processes
At age 46 four out of ve BCLP subjects used active non-oral pharyngeal andglottal processes and oral velar and uvular fricatives irrespective of surgical status(see table 1) All had some anterior palatal defect which might have reduced theirpotential to achieve intra-oral pressure
By comparison two out of three partially repaired 2-stage UCLP subjects at age46 (table 2) showed evidence of passive processes This suggested that their
Active versus passive cleft-type speech characteristics 341
Tab
le4
Spee
chin
rela
tion
tosu
rgic
altim
ing
atag
e13
0
2-st
age
surg
ery
2-st
age
surg
ery
1-st
age
surg
ery
subj
ects
com
plet
edat
4yr
sco
mpl
eted
at8
yrs
1-A
1-B
1-C
1-D
1-E
1-F
24-
G2
4-H
24-
J2
8-K
28-
L2
8-M
Pass
ive
clef
t-ty
pepr
oces
ses
pred
omin
antly
sono
rant
artic
wea
kar
ticul
atio
nm
voic
eles
sh
fo
rpl
osiv
esna
sal
rele
ase
ofpl
osiv
esna
sal
emis
sion
with
cons
onan
tsm
pass
ive
nasa
lfr
icat
ives
Act
ive
clef
t-ty
pepr
oces
ses
nasa
lfr
icat
ives
phar
ynge
alg
lott
alar
ticul
atio
nba
ckin
gto
uvul
arba
ckin
gto
vela
rm
m
late
ral
pala
tal
fric
ativ
esm
mm
doub
lear
ticul
atio
ngl
idin
gfr
icat
ive
1=1-
stag
esu
rger
ysu
bjec
ts
24=
2-st
age
surg
ery
hard
pala
tere
pair
edat
abou
t4
yrs
28=
2-st
age
surg
ery
with
hard
pala
tere
pair
edat
abou
t8
yrs
A Harding and P Grunwell342
unrepaired hard palates had in fact restricted their phonetic repertoire imposing aneed for individual adaptability The additional active processes employed by thesesubjects were presumably a response to the restrictions imposed by their oro-nasalstructure and velopharyngeal function at the time of consonant acquisition Asshown in table 2 the most common active cleft-type processes persisting at age46 with a residual cleft of the hard palate were backing double articulation andlateralpalatal articulation Two 1-stage surgery subjects whose entire palates hadbeen repaired at ages 09 and 010 did not use any cleft-type processes at age 46
By age 90 (table 3) a much-diminished number of cleft type processes wasevident except in subjects with sizeable anterior stulae who had received littlespeech and language therapy A similarity was noted between the speech patternsof 1-stage surgery subjects with stulae (DA and SB) at age 90 (table 3) and theyounger BCLP subjects at age 46 (table 1) who also had anterior palatal defectsThey included non-oral realizations of t d s k g occasional nasal fricatives andpharyngealglottal articulations Fistulae had apparently continued to in uencearticulation and phonological development in these subjects
Finally at age 130 (table 4) the diVerences between 1-stage and 2-stage surgerysubjects had diminished leaving only one 2-stage subject with occasional backingand four subjects with slight palatal and lateral release of fricative consonants Onlytwo of the 1-stage surgery subjects were using minor distortions of grooved fricativeproduction
Whilst there were apparent trends in speech production relating to surgicaltiming and oral structure it is noted that there were exceptions to each tentativegeneralization Subjects with marked structural imperfections occasionally producedrealizations of which they would not have been thought capable and subjects withno visible imperfections produced inexplicably distorted speech patterns It istherefore concluded that whilst there is homogeneity in the range of processesproduced by this population assumptions cannot be made about speech based onsurgical timing or type of cleft Tentative predictions based on detailed assessmentmay be clinically very useful
EVects of surgery on speech
Activepassive processes have identi ed those cleft-type characteristics thought tobe associated with a physical inability to produce pressure consonants The followinganalysis of speech changes after surgical intervention at diVerent ages identi es thechanges eVected by surgery when intra-oral pressure could be more readily achieved
Two children were rst recorded prior to the rst stage of a 2-stage procedureTheir lips were repaired at approximately 6 months of age and soft palate repairwas carried out at ages 18 and 19 respectively Their hard palates were leftunrepaired to facilitate unrestricted growth of the mid-face (Hotz et al 1978) Pre-and post-operative consonant-like sounds present in the recorded speech samplesare listed in table 5 Interestingly prior to soft palate repair both these childrenproduced some oral consonants Subject B was producing pressure consonants [kg] in his babble prior to soft palate repair Considering that he had an unrepairedbilateral cleft palate at this point it was surprising that he had any oral consonantsPost-operatively at 20 years he used [b bkm t d g gkb] which indicated that surgeryto repair the soft palate had facilitated an increased range of oral pressure consonantsSubject D was producing [p b k g] pre-operatively Post-operatively following soft
Active versus passive cleft-type speech characteristics 343
Tab
le5
EV
ects
ofso
ftp
alat
ere
pair
atag
e1
6on
BC
LP
subj
ects
h
ard
pal
ate
rem
ain
sun
repa
ired
2-st
age
subj
ects
Surg
ery
Pre
-ope
rati
vesp
eech
patt
ern
atag
e1
6Po
st-o
pera
tive
chan
ges
insp
eech
atag
e2
0
Stud
y1
BSo
ftpa
late
repa
irat
16
Adu
ltta
rget
sk
gA
t2
0[b
b kmg kb
td
g]D
Soft
pala
tere
pair
17
Adu
ltta
rget
sp
bk
gA
t2
0[p
bd
b kdk
g]
Tab
le6
EV
ects
ofha
rdpa
late
rep
air
atag
e6
6an
d
stu
lare
pair
atag
e10
0
Subj
ect
Surg
ery
Pre
-ope
rati
vesp
eech
patt
ern
Post
-ope
rati
vech
ange
sin
spee
ch
MS
Har
dpa
late
repa
ir6
6Pa
ssiv
epr
oces
s7
6E
limin
ated
pass
ive
proc
ess
Var
iabl
ena
sal
rele
ase
ofco
nson
ants
Hyp
onas
alna
sals
JFH
ard
pala
tere
pair
(uns
ucce
ssfu
l)6
6Se
vera
lac
tive
and
pass
ive
proc
esse
s7
6A
ctiv
epr
oces
ses
rem
aine
dPa
ssiv
epr
oces
ses
elim
inat
ed
DA
Fis
tula
repa
ir10
0A
ctiv
epr
oces
ses
110
Elim
inat
ion
ofph
aryn
geal
glo
ttal
Var
iabi
lity+
+an
dna
sal
arti
cula
tion
Art
icul
ator
yva
riab
ility
++
Act
ive
CT
Rs
proc
esse
spe
rsis
t
A Harding and P Grunwell344
palate repair but with a residual cleft in the hard palate his range of consonantsincluded [d] which was particularly surprising since the hard palate remainedunrepaired Whilst it is unlikely that toddlers of 18 months could be consciouslytrying to compensate for articulatory inadequacy in producing velar plosives inbabble prior to soft palate repair and an alveolar plosive prior to hard palate repairboth these subjects showed evidence of actively pursuing their articulatory potential
Table 6 summarizes changes following surgery to repair the hard palate in moremature speech patterns These subjects who were aged 66 and 100 pre-operativelyhad learned to speak with residual clefts and were apparently unaware of theconsonant productions that failed to match normal production
Subject MS used only passive processes in his speech pattern He realized someconsonants nasally such that lsquoballrsquo was [mO~] and lsquosockrsquo was [(sk)n
deg Aacute~ k] Looking atpost-operative changes at age 76 his consonant production was normal but hisresonance had become hyponasal Pre-operatively at age 66 Subject JF was usingseveral active and passive processes The active processes were unaVected by surgerybut passive processes were eliminated
Fistula repair was carried out at age 100 on Subject DA who had many activeprocesses and very variable articulation pre-operatively Post-operatively at age110 he was not using non-oral pharyngeal and glottal active processes or nasalrealizations but many oral cleft-type realizations remained
As shown in table 7 hard palate re-repair and pharyngoplasty was carried outon two subjects whose hard palate repairs had been unsuccessful at approximately4 years Subject NC assessed pre-operatively at age 56 was using predominantlypassive processes in her speech She was also using [ j] for fricatives s S whichwas thought to be an active process At age 60 following hard palate re-repair andpharyngoplasty all cleft-type processes had been eliminated without post-operativespeech therapy Since [ j] for s apparently resolved spontaneously followingsurgery it can be assumed that this was a passive process in this speech sample
Subject CP who underwent this procedure presented pre-operatively at age 46with both passive and active processes but his nasal resonance was not consistentlyhypernasal In addition to his cleft-related speech disorder this subject had additionaldevelopmental speech diYculties which were identi ed as being unrelated to thecleft Post-operatively at age 56 little had changedmdashnotably the passive processnasal [m] for b was retained His nasal resonance had become hyponasal andthere was no apparent bene t from surgical intervention The realization of b as[m] had become phonologically stable and surgery alone had not destabilized thephonological system This realization may have been a passive product of VPI inearly speech acquisition which had subsequently become part of a phonologicaldisorder Post-operatively CPrsquos phonetic repertoire did increase but the phonologicaldistribution was variable Plosive targets were still realized as nasals in spontaneousspeech at the nal speech recording at age 76 This was not as an inevitableconsequence of VPI but a result of an inability to destabilize the phonologicalprocess determining that voiced plosives would be realized as nasals This resultfollowing surgery highlights the importance of identifying phonological learningproblems and distinguishing them from structural constraints on articulationIn CPrsquos case pre-operative exploration of the eVect of nares occlusion duringspeech might have indicated that structural change would not improve consonantproduction spontaneously
A general observation was that consonant realizations did not move rapidly
Active versus passive cleft-type speech characteristics 345
Tab
le7
EV
ects
ofha
rdpa
late
re-r
epai
ran
dp
hary
ngo
pla
sty
Subj
ect
Surg
ery
Pre
-ope
rati
vesp
eech
patt
ern
Post
-ope
rativ
ech
ange
sin
spee
ch
Stud
y2
NC
Har
dpa
late
re-r
epai
ran
d5
6Pa
ssiv
ecl
eft-
type
proc
esse
s6
0A
llcl
eft-
type
phar
yngo
plas
ty5
10[
j]
for
fric
ativ
espr
oces
ses
elim
inat
ed[
h]
for
plos
ives
SIW
IV
aria
ble
arti
cula
rypr
ecis
ion
CP
Har
dpa
late
repa
iran
d4
6Pa
ssiv
ean
dac
tive
proc
esse
s5
6Pa
ssiv
epr
oces
sph
aryn
gopl
asty
50
Pho
nolo
gica
lco
nfus
ion
[m]
for
[b
]re
tain
edH
ypon
asal
nasa
lsPe
rsis
ting
phon
olog
ical
conf
usio
ns
A Harding and P Grunwell346
from incorrect to correct but progressed incrementally towards normal realizationsas described by Morley (1970) Where an early realization of target s might beglottal [h] a gradual pattern of change showed subsequent realizations to bepharyngeal [Eacute] then uvular [X] then velar [x] and eventually palatal [c] or lateral [Euml]It was interesting to note that speech patterns continued to change as late as90ndash110 years with the result that diVerences related to surgical timing and cleft-type gradually disappeared Persisting stulae were thought to account for the mostmarked cleft type processes at age 90
Implications for surgical management
This analysis of speech changes following surgery suggests some implications forsurgical management which are compatible with Sell and Grunwellrsquos (1990) ndingsin the Sri Lankan study
Surgery can change passive speech processes but it is also possible that speechtherapy may be able to change passive patterns Surgery alone is unlikely to modifyactive cleft-type processes whereas speech therapy should be able to modify activeprocesses Indications from these case studies is that where speech is the primaryproblem speech assessment should distinguish between active and passive processesin order to evaluate the necessity for full investigations and to plan therapeuticintervention Where past speech therapy has not been successful it cannot beassumed that surgical intervention will facilitate further speech progress A furthercourse of speech therapy which is sensitive to active versus passive processes todevelopmental phonological in uences on cleft-type speech development and toarticulatory diYculties in diVerent speech contexts might facilitate optimal progressWhere structural imperfection exists it is quite possible for single-word productionto be more precise than target realizations in spontaneous speech This may not bea failure of phonological generalization (Grunwell 1992) but the result of diYcultysustaining the necessary lsquoarticulatory eVort rsquo (Harding and Grunwell 1993) resultingin articulatory imprecision Deteriorating articulatory accuracy should not be over-looked in interpretation of speech results
An analytical protocol
As a result of analysing the speech data and identifying the active and passiveprocesses a protocol has been developed which records examples of each cleft-typeprocess over a series of assessments It demonstrates the progression of individualprocesses towards an adult target (see the Appendix) At each assessment onecolumn is used to indicate nasal resonance nasal emission and nasal turbulenceratings and cleft-type processes Changes in the nature of error realizations mightshow progress towards target consonants Hence whilst the total correct scoremight not have increased increments of change can be observed This observationof patterns of change may function as an adjunct to GOSSPASSrsquo98 (Sell et al 1998)giving access to a greater depth of both quantitative and qualitative data aboutconsonant production in relation to resonance nasal emission nasal turbulenceoral structure and cleft-type
Active versus passive cleft-type speech characteristics 347
Diagnostic implications
Passive versus active nasal fricatives
The important management consideration related to this distinction is that an activenasal fricative is an established phonological process which is unlikely to be directlyaVected by surgery alone Therapy would be necessary to destabilize nasal realizationsof oral consonants In contrast passive nasal fricatives may be eliminated by surgeryOf particular relevance is diVerential diagnosis between passive and active nasalfricatives in surgical and therapeutic management When hypernasality co-occurswith nasal air ow during consonant production which can be redirected by nose-holding passive nasal fricatives are diagnosed These would be transcribed as [(sk)n
deg]
passive alveolar nasal fricatives [(Wk)mdeg
] bilabial nasal fricatives or [(fk)Iacutedeg ] labiodentalnasal fricatives Full VPI investigations would be recommended to diagnose thenature of the structural or functional de ciency and distinguish between velopharyn-geal incompetence and velopharyngeal mislearning
It is highly likely that plosive targets would be aVected by reduced intra-oral airpressure such that plosives would either be realized by nasal counterparts eg bd[ [m n] or [b d] may be nasalized and weak Voiceless plosives may be eitheraccompanied by nasal emission [p t k] or realized as glottal fricative [h]
Production of the target sentence lsquoI saw Sam sitting on a busrsquo might be
[aI (sk)ndeg O~ (sk)n
degaelig~m (sk)n
deg IhIn Aacute~n mouml~(sk)ndeg] passive processes and
[aI xO xaeligm xIkIIcirc AacuteIcirc goumlx] active processes
Contribution to surgical management decisions
Passiveactive interpretation of clinical assessments might facilitate surgical manage-ment decisions If noseholding does not facilitate correct production of targetconsonants then it is likely that an alternative articulatory pattern has becomephonologically established ie particular realizations for one or more targets areconsistently distributed in the phonological system These realizations may haveevolved because of initial diYculty producing articulatory targets and subsequentlystabilized within the phonological system Grundy and Harding (1995) refer to thisphenomenon as an lsquoarticulatory disorder with phonological consequencesrsquo
Therapy
Where obvious structural defects or diagnosed dysfunction exists clinicians fre-quently defer therapeutic intervention until surgery has been undertaken Theexpectation would be that normal structure and function is essential for normalspeech However pre-operative therapy may facilitate oral consonant productionwhich may serve to reduce hypernasal resonance Hence therapy prior to surgerymay avoid unnecessary surgery or reduce the extent of surgery required All activeprocesses are likely to require therapy
Principled selection of targets for therapy
Speech patterns frequently evidence a mixture of apparently passive and activeprocesses which complicates decisions about target selection Target selection can
A Harding and P Grunwell348
be based on assessment of which consonant targets can be most easily elicted inisolation (stimulability) This may lead to a sequence of target selection which isopposite to the sequence of consonant acquisition in normal development Forexample where reduced intra-oral pressure is present in a passive pattern [T] maybe easier to elicit in imitation than more nely grooved [s] or [S] Therapy maytarget [T] followed by [S ] and nally [s] As in non-cleft phonological therapywhere a class of consonants is aVected by the cleft then it is helpful to target theentire class The following decision-making process can be applied for both activeand passive processes
Decision making procedure for target selection
(1) Voiced versus voiceless targets(2) Front versus back placements(3) Syllable initial versus syllable nal targets(4) Plosives versus fricative targets
Voiceless plosives and fricatives are produced with an open glottis whichfacilitates topping up of air ow from the lungs hence voiceless plosive and fricativetargets are frequently more successful than voiced counterparts (Isshiki and Ringel1964) Front targets usually cause more diYculty than back particularly where analveolar defect or stula exists Contrary to normal development back targets maybe targeted before front Word- nal targets generally require less oral air pressurethan word initial targets and similarly fricatives may be more easily elicited thanplosives Fricatives do require a greater volume of air than plosives (Fletcher 1985)but in the presence of nasal escape weak fricative production appears to be morereadily achieved than weak plosive production Since nal fricatives would normallybe acquired in advance of word-initial fricatives (Ferguson 1978) targeting word- nal fricatives is frequently a productive starting point for therapy
Principles of therapy for passive processes
(1) Use of soft attack similar to gentle whisper for all target models ensuresminimal articulatory eVort (Harding and Grunwell 1993) and requires min-imal intra-oral air pressure It may be appropriate to gradually increase thearticulatory attack when the articulatory posture and evidence of intendedoral air ow have been established
(2) Slightly stretched duration of segment transitions in models of consonantto vowel (CndashV) or vowel to consonant (VndashC) facilitates review of motorplanning and extends the available time for execution of the new motorprogrammer whilst maintaining control of the oral airstream
(3) Noseholding can be used to provide exclusively oral air ow Gradual releaseof the nostrils during production of sustained [VVVVVf ] or [hhhhh ] allowsthe child to attempt to sustain an oral consonant despite increasing nasalemission This maximizes the use of available oral air ow Procedures forusing noseholding are described in some detail by Golding-Kushner (1995)
Principles of therapy for active processes
This is more like phonological therapy and can follow Grunwellrsquos (1991) processesfor phonological change and principled decision-making (Grunwell 1992) Some
Active versus passive cleft-type speech characteristics 349
examples are given here by way of illustration of ways to eVect the rst twoprocesses of change which may need to be approached diVerently in cleft palateversus non-cleft speech disorders DiVerent approaches may also be appropriate formodifying active versus passive cleft-type processes
Innovation production of new targets Some useful principles
(1) Introduction of new lsquonon-speech likersquo targets in sound play using a conson-ant sound segment model such as [ph ] note not a syllable like [p] whichis the type of pronunciation used when target sounds are presented as lettersfor reading Target [s] might be introduced as a lsquoTrain Slowing Down Noisersquo[ts ts ts tssssssss]
(2) lsquoNew consonantsrsquo can later be modelled and elicited in soft productions ofsyllable structure [tssssndashi] [ indashtssss] which can subsequently be identi ed assimilar to words lsquosearsquo and lsquoeatsrsquo
(3) lsquoDeferring responsibilityrsquo transfers responsibility or lsquoblamersquo for errors fromthe child and attributes it to the articulators eg lsquoyour tongue is havingtrouble with hellip rsquo lsquoLetrsquos show your tongue how to hellip rsquo
(4) New targets can be modelled repeatedly and recorded on audio or videotape which can be listened to at home
(5) Targeting classes of consonants (eg alveolars t d s n l voiceless fricativesf s S perhaps with aVricate T avoids phonological confusion whichmight occur if production ofsis achieved whilst other alveolar targetsremain backed The risk is that s might not integrate into the phonologicalsystem unless all backed alveolar consonants are destabilized
(6) Increased eye contact during auditory and production work can be invaluablein holding visual and auditory attention and ensures that visual informationabout the sound has been processed This is easily achieved by the clinicianlifting any focus of the childrsquos attention close to hisher mouth at theprecise moment when the target is modelled
Stimulation of non-speech related sounds such as a lsquoTrain Slowing DownNoisersquo [ts ts tsss] con rms that target [s] is physically achievable whether or not[ssss] can be imitated Some children continue to access [s] through the lsquoTrainSlowing Down Noisersquo throughout therapy until it is occurring spontaneouslywithout conscious planning This can be an eVective means of underminingestablished motor programmers (Hewlett 1990) for active cleft-type processes
Destabilizing active processes
As it is likely that children will be unaware of each occurrence of their alternativearticulatory pattern for speci c consonant errors it is preferrable to destabilizeactive processes with minimal conscious eVort by the child As children becomeaware of their mismatches they frequently add the newly acquired target realizationto their existing production eg target word tu childrsquos old realization [ku] childrsquoscorrected realization [t-ku] Destabilization can be achieved with minimal consciouseVort through input therapy techniques such as auditory bombardment (Lancasterand Pope 1989) auditory decision-making such as lsquowhich bear says this wordproperlyrsquo Red Bear says lsquotworsquo or Blue Bear says lsquocoorsquo This type of strategy oftenprecipitates attention to the target consonant with possible lsquoreplayrsquo and lsquoreviewrsquo of
A Harding and P Grunwell350
their own production Frequent stimulation of cognitive alertness to the targetconsonant can develop awareness without confronting the child with errors orrisking hisher failure The child is then free to attempt to repair hisher ownrealization to continue to re ect and to silently rehearse the adult realizationTraditional articulation therapy is thus combined with development of metaphonol-ogical skills ie the ability to re ect upon onersquos own speech production The resultshould be that new target realizations will be more phonologically stable thanexclusively production-based articulation therapy might have facilitated
Stabilizationgeneralization
Procedures to ensure stabilization and generalization of new target consonantswould be as described by Grunwell (1992) Success may be constrained by theconsiderable articulatory eVort sometimes required to maintain pressure consonantproduction in spontaneous speech (Harding and Grunwell 1993)
Conclusions
In speech assessment it is helpful to distinguish between errors which are cleft-type and non-cleft type and those which are part of active versus passive processesThe active and passive processes have been de ned and their phonological implica-tions discussed Focus on active and passive processes has facilitated focus on thephonological consequences of cleft palate on speech development In the futureawareness of the likely eVect of a cleft palate on normal phonological developmentcould avoid extended periods of unsuccessful clinical intervention Furthermoresensitivity to the relationship between phonological processes and structural con-straints should facilitate theoretically based management decisions Incidences suchas the case of CP in which nasal realizations were thought to indicate VPI but weresubsequently unaVected by surgery might be avoided if phonological analysiscontributes to management decisions
Surgery did improve hypernasal resonance and eliminated passive processes buthad little eVect on active processes Active processes in younger subjects werethought to require therapeutic intervention but in the longer term the oldersubjects showed few cleft-type processes Whilst it is possible that active cleft-typeprocesses may resolve with increasing age the implication for the future is thatactive cleft-type processes should be treated with skilled therapeutic interventionnot surgery Therapy which addresses the phonological consequences of cleft palateon speech development by combining metaphonologicalphonologicalarticulatoryapproaches is likely to be successful
References
Albery E 1991 Consonant articulation in the diVerent types of cleft lip and palate UnpublishedMPhil thesis Leicester Polytechnic
Albery E and Grunwell P 1993 Consonant articulation in diVerent types of cleft palate InP Grunwell (Ed) Analysing Cleft Palate Speech (London Whurr)
Ferguson C A 1978 Fricatives in child language acquisition In V Honsa and M Hardmann-Battista (Eds) Papers on Linguistics and Child Language (Mouton The Hague)
Fletcher S G 1985 Speech production and oral motor skill in an adult with an unrepaired palatalcleft Journal of Speech and Hearing Disorders 50 254ndash261
Active versus passive cleft-type speech characteristics 351
Golding-Kushner K J 1995 Treatment of articulation and resonancne disorders associated withcleft palate management and VPI In R Shprintzen (Ed) Cleft Palate Speech Management AMultidisciplinary Approach (St Louis Mosby)
Grundy K and Harding A 1995 Developmental speech disorders In K Grundy (Ed) Linguisticsin Clinical Practice (2nd edition) (London Whurr)
Grunwell P 1985 Phonological Assessment of Child Speech (Windsor NFER-Nelson)Grunwell P 1987a Clinical Phonology (2nd edition) (London Croom Helm)Grunwell P 1987b PACS Pictures Language Elicitation Materials (Windsor NFER-Nelson)Grunwell P 1991 Processes of phonological change in developmental speech disorders Clinical
Linguistics and Phonetics 6 101ndash122Grunwell P 1992 Principled decision making in the remediation of children with phonological
disorders In P Fletcher and D Hall (Eds) Specic Speech and Language Disorders in Children(London Whurr)
Grunwell P and Harding A 1995 PACSTOYS A Screening Assessment of Phonological Development(Windsor NFER-Nelson)
Grunwell P and Harding A 1996 A note on describing types of nasality Clinical Linguistics andPhonetics 10 157ndash161
Harding A 1993 An Investigation into the Relationship Between Timing of Cleft Palate Repairand Speech Development Unpublished PhD thesis
Harding A and Grunwell P 1993 The relationship between speech and timing of hard palaterepair In P Grunwell (Ed) Analysisng Cleft Palate Speech (London Whurr)
Harding A and Grunwell P 1996 Characteristics of cleft palate speech European Journal ofDisorders of Communication 31 331ndash358
Henningsson G and Isberg A M 1986 Velopharyngeal movement patterns in patients alternatingbetween oral and glottal articulation A clinical and cineradiographicical study Cleft Palate Journal23 1ndash9
Hewlett N 1990 Processes of development and production In P Grunwell (Ed) DevelopmentalSpeech Disorders (Edinburgh Churchill Livingstone)
Hotz M M Gnoinski W M Nussbaumer H and Kistler E 1978 Early orthopaedics in CLPcases guidelines for surgery Cleft Palate Journal 15 405ndash411
Hutters B and Brondsted K 1987 Strategies in cleft palate with special reference to DanishCleft Palate Journal 24 127ndash136
Isshiki N and Ringel R 1964 Airow during the production of selected consonants Journal ofSpeech and Hearing Research 7 233ndash244
Kummer A W Curtis C Wiggs M Lee L and Strife J L 1992 Comparison of velopharyngealgap size in patients with hypernasality hypernasality with nasal emission and nasal emissionor nasal turbulence (rustle) as the primary speech characteristic Cleft-palate-Craniofacial Journal29 152ndash156
Lancaster G and Pope L 1989 Working with Childrenrsquos Phonology (Oxford Winslow)Morley M E 1970 Cleft Palate and Speech (7th edition) (Edinburgh Churchill Livingstone)Russell V J 1991 Speech Development in Children with Cleft Lip and Palate Unpublished PhD
thesis Leicester PolytechnicRussell V J and Grunwell P 1993 Speech development in children with cleft lip and palate In
P Grunwell (Ed) Analysing Cleft Palate Speech (London Whurr)Sell D A and Grunwell P 1990 Speech results following late palatal surgery in previously
unoperated Sri Lankan adolescents with cleft palate Cleft Palate Journal 27 162ndash168Sell D Harding A and Grunwell P 1994 GOSSPASS A screening assessment of cleft palate
speech European Journal of Disorders of Communication 29 1ndash15Sell D Harding A and Grunwell P 1998 GOSSPASSrsquo98 An assessment for speech disorders
associated with cleft palate andor velopharyngeal dysfunction International Journal of Languageamp Communication Disorders ( in press)
Shorter E 1995 A spectographic analyis of child homophones Unpublished honours project DeMontfort University Leicester
Stenglehoffen J 1989 Nature and causes of communication diYculties In J Stengelhofen (Ed)Cleft Palate Nature and Remediation of Communication Problems (Edinburgh Churchill Livingstone)
Trost J E 1981 Articulatory additions to the classical description of the speech of persons withcleft palate Cleft Palate Journal 18
Trost-Cardamone J E 1990 The development of speech assessing cleft palate misarticulationsIn D A Kernahan and S N Rosenstein (Eds) Cleft Lip and Palate A System of Management(Baltimore Williams amp Wilkins)
A Harding and P Grunwell352
Appendix Active passive analysis of cleft palate speech

A Harding and P Grunwell338
Passive nasal fricative [(fk)m (sk)ndeg]
Incomplete velopharyngeal closure inevitably reduces control of oral air ow with apassive loss of air ow and an increase of resonance in the nasal cavity Grunwelland Harding (1996) de ned the passively nasal fricative as an unreleased [(s)]double-articulated with a lowered voiceless nasal [n
Aacute
deg] This realization is the product
of an intended s with an unintended nasal air ow (see gure 4) The precisetranscription for a passive nasal transcription is [(sk)n
Aacute
deg] but an acceptable simpli cation
for transcription purposes is [(sk)ndeg] This is distinct from the active nasal fricative
which involves stopping of the oral air ow and active direction of air nasally whichcan be transcribed as a voiceless nasal with additional nasal emission [n
degk] Nasal
emission signals the fricative nature of for example target consonant s Thesetwo productions can sound the same and might initially be transcribed as [n
degk]
Nasendoscopic investigation of velopharyngeal activity during active and passivenasal realizations of s both show a lack of velopharyngeal closure It is predictedthat close examination by use of electropalatography might show slight diVerencesin tongue tip posture for an active and passive nasal fricative as illustrated in gures3 and 4 Passive nasal fricatives were converted into oral fricatives with nose-holding
Voiceless [h] for voiceless plosives
There was evidence that voiceless plosives were at times passively realized as [h]The consequence of reduced oral air pressure on production of voiceless plosivescan leave aspiration as the only perceptible distinctive feature This process usuallyaVected all voiceless plosive targets p t k Where this process was a passiveprocess use of noseholding during speech facilitated accurate target productionHowever it would also be possible for this distribution of [h] to be an active cleft-type process which would be part of a pharyngealglottal patternprocess
Nasal realization of voiced plosives b d g[ [m n Icirc]
Some subjects with residual clefts stulae or suspected VPI realized voiced conson-ants as nasal counterparts As summarized by Harding and Grunwell (1996) voiced
Figure 4 Passive nasal fricative [(sk)nAacute
deg]
Active versus passive cleft-type speech characteristics 339
consonants can be more diYcult to produce than voiceless consonants (Isshiki andRingel 1964) Distinction between active versus passive nasal realizations of plosivetargets was made in the same way that active and passive nasal fricatives weredistinguished by observing the eVect of noseholding on consonant production Inpassive nasal realizations noseholding facilitated normal consonant production(Golding-Kushner 1995)
Nasal emission accompanying consonants [pk sk]
Nasal emission was frequently heard accompanying consonants but on occasions itapparently replaced consonants It has been linked with velopharyngeal incompet-ence (VPI) (Kummer et al 1992)
Results
Comparison of activepassive processes in the speech data
Quantitative results of Hardingrsquos research into the relationship between timing ofsurgery and speech development have already been published (Harding andGrunwell 1993) The following interpretation of the data speci cally identi esactivepassive cleft-type processes in relation to oral structure in a wide age rangeof subjects (16ndash130) Tables 1 2 3 and 4 show the passive and active processeson the left-hand column and the subjectrsquos code along the top The code identi esthose subjects who were treated with 1-stage versus 2-stage surgery Comparisonof the 4 tables at age 46 (BCLP and UCLP) at age 90 and at age 130 illustratesa pattern of diminishing cleft-type processes with increasing age Irrespective ofsurgical timing few cleft-type processes remained at age 130 (table 4) A generalobservation was that earlier speech samples (ages 16ndash76) frequently combined
Table 1 Cleft-type processes in BCLP subjects at age 46 (studies 1 and 2)
1-stage surgery 2-stage surgery
A G Rf JW D B JF JG AB
Passive cleft-type processespredominantly sonorant articulation m
weak articulation m m m m m m m m
voiceless h for plosive m m m m m
nasal release of plosives m m m m m
nasal emission with consonants m m m m m m
passive nasal fricativeActive cleft-type processes
nasal fricatives m m m m m m m m
pharyngeal glottal articulation m m m m m m m m
backing to uvular m m m m m m m m
backing to velar m m m m m m m m m
lateral palatal fricatives m m m m m m m m m
double articulation m m m m m m m m m
gliding fricative m m
f=post-operative stula
A Harding and P Grunwell340
Table 2 Cleft-type processes in UCLP subjects at age 46 (study 2)
1-stage surgery 2-stage surgery
SE TB CK MS NC TS ZG CP
Passive cleft-type processespredominantly sonorant artic m
weak articulation m m m
voiceless h for plosives m m m
nasal release of plosives m m m
nasal emission with consonants m m
passive nasal fricative m m
Active cleft-type processesnasal fricativepharyngeal glottal articulation m m m
backing to uvular m
backing to velar m m
lateral palatal fricatives m m m m m
double articulation m m m m m m
gliding fricative m
Table 3 Cleft-type processes at age 90
2-stage surgery 2-stage surgery1-stage surgery completed at 4 yrs completed at 8 yrs
DAf SBf RL NR JD AR LJ RP MB
Passive cleft-type processespredominantly sonorant articweak articulation m
voiceless h for plosives m m
nasal release of plosives m m
nasal emission with consonants m m m m
passive nasal fricatives m m
Active cleft-type processesnasal fricatives m m
pharyngeal glottal articulation m m
backing to uvular m m
backing to velar m m m m m m m
lateral palatal fricatives m m m m m m m
double articulation m m m m m
gliding fricative m
f=subject had a stula
both active and passive strategies whereas later samples (ages 90ndash130) rarelyevidenced passive processes
At age 46 four out of ve BCLP subjects used active non-oral pharyngeal andglottal processes and oral velar and uvular fricatives irrespective of surgical status(see table 1) All had some anterior palatal defect which might have reduced theirpotential to achieve intra-oral pressure
By comparison two out of three partially repaired 2-stage UCLP subjects at age46 (table 2) showed evidence of passive processes This suggested that their
Active versus passive cleft-type speech characteristics 341
Tab
le4
Spee
chin
rela
tion
tosu
rgic
altim
ing
atag
e13
0
2-st
age
surg
ery
2-st
age
surg
ery
1-st
age
surg
ery
subj
ects
com
plet
edat
4yr
sco
mpl
eted
at8
yrs
1-A
1-B
1-C
1-D
1-E
1-F
24-
G2
4-H
24-
J2
8-K
28-
L2
8-M
Pass
ive
clef
t-ty
pepr
oces
ses
pred
omin
antly
sono
rant
artic
wea
kar
ticul
atio
nm
voic
eles
sh
fo
rpl
osiv
esna
sal
rele
ase
ofpl
osiv
esna
sal
emis
sion
with
cons
onan
tsm
pass
ive
nasa
lfr
icat
ives
Act
ive
clef
t-ty
pepr
oces
ses
nasa
lfr
icat
ives
phar
ynge
alg
lott
alar
ticul
atio
nba
ckin
gto
uvul
arba
ckin
gto
vela
rm
m
late
ral
pala
tal
fric
ativ
esm
mm
doub
lear
ticul
atio
ngl
idin
gfr
icat
ive
1=1-
stag
esu
rger
ysu
bjec
ts
24=
2-st
age
surg
ery
hard
pala
tere
pair
edat
abou
t4
yrs
28=
2-st
age
surg
ery
with
hard
pala
tere
pair
edat
abou
t8
yrs
A Harding and P Grunwell342
unrepaired hard palates had in fact restricted their phonetic repertoire imposing aneed for individual adaptability The additional active processes employed by thesesubjects were presumably a response to the restrictions imposed by their oro-nasalstructure and velopharyngeal function at the time of consonant acquisition Asshown in table 2 the most common active cleft-type processes persisting at age46 with a residual cleft of the hard palate were backing double articulation andlateralpalatal articulation Two 1-stage surgery subjects whose entire palates hadbeen repaired at ages 09 and 010 did not use any cleft-type processes at age 46
By age 90 (table 3) a much-diminished number of cleft type processes wasevident except in subjects with sizeable anterior stulae who had received littlespeech and language therapy A similarity was noted between the speech patternsof 1-stage surgery subjects with stulae (DA and SB) at age 90 (table 3) and theyounger BCLP subjects at age 46 (table 1) who also had anterior palatal defectsThey included non-oral realizations of t d s k g occasional nasal fricatives andpharyngealglottal articulations Fistulae had apparently continued to in uencearticulation and phonological development in these subjects
Finally at age 130 (table 4) the diVerences between 1-stage and 2-stage surgerysubjects had diminished leaving only one 2-stage subject with occasional backingand four subjects with slight palatal and lateral release of fricative consonants Onlytwo of the 1-stage surgery subjects were using minor distortions of grooved fricativeproduction
Whilst there were apparent trends in speech production relating to surgicaltiming and oral structure it is noted that there were exceptions to each tentativegeneralization Subjects with marked structural imperfections occasionally producedrealizations of which they would not have been thought capable and subjects withno visible imperfections produced inexplicably distorted speech patterns It istherefore concluded that whilst there is homogeneity in the range of processesproduced by this population assumptions cannot be made about speech based onsurgical timing or type of cleft Tentative predictions based on detailed assessmentmay be clinically very useful
EVects of surgery on speech
Activepassive processes have identi ed those cleft-type characteristics thought tobe associated with a physical inability to produce pressure consonants The followinganalysis of speech changes after surgical intervention at diVerent ages identi es thechanges eVected by surgery when intra-oral pressure could be more readily achieved
Two children were rst recorded prior to the rst stage of a 2-stage procedureTheir lips were repaired at approximately 6 months of age and soft palate repairwas carried out at ages 18 and 19 respectively Their hard palates were leftunrepaired to facilitate unrestricted growth of the mid-face (Hotz et al 1978) Pre-and post-operative consonant-like sounds present in the recorded speech samplesare listed in table 5 Interestingly prior to soft palate repair both these childrenproduced some oral consonants Subject B was producing pressure consonants [kg] in his babble prior to soft palate repair Considering that he had an unrepairedbilateral cleft palate at this point it was surprising that he had any oral consonantsPost-operatively at 20 years he used [b bkm t d g gkb] which indicated that surgeryto repair the soft palate had facilitated an increased range of oral pressure consonantsSubject D was producing [p b k g] pre-operatively Post-operatively following soft
Active versus passive cleft-type speech characteristics 343
Tab
le5
EV
ects
ofso
ftp
alat
ere
pair
atag
e1
6on
BC
LP
subj
ects
h
ard
pal
ate
rem
ain
sun
repa
ired
2-st
age
subj
ects
Surg
ery
Pre
-ope
rati
vesp
eech
patt
ern
atag
e1
6Po
st-o
pera
tive
chan
ges
insp
eech
atag
e2
0
Stud
y1
BSo
ftpa
late
repa
irat
16
Adu
ltta
rget
sk
gA
t2
0[b
b kmg kb
td
g]D
Soft
pala
tere
pair
17
Adu
ltta
rget
sp
bk
gA
t2
0[p
bd
b kdk
g]
Tab
le6
EV
ects
ofha
rdpa
late
rep
air
atag
e6
6an
d
stu
lare
pair
atag
e10
0
Subj
ect
Surg
ery
Pre
-ope
rati
vesp
eech
patt
ern
Post
-ope
rati
vech
ange
sin
spee
ch
MS
Har
dpa
late
repa
ir6
6Pa
ssiv
epr
oces
s7
6E
limin
ated
pass
ive
proc
ess
Var
iabl
ena
sal
rele
ase
ofco
nson
ants
Hyp
onas
alna
sals
JFH
ard
pala
tere
pair
(uns
ucce
ssfu
l)6
6Se
vera
lac
tive
and
pass
ive
proc
esse
s7
6A
ctiv
epr
oces
ses
rem
aine
dPa
ssiv
epr
oces
ses
elim
inat
ed
DA
Fis
tula
repa
ir10
0A
ctiv
epr
oces
ses
110
Elim
inat
ion
ofph
aryn
geal
glo
ttal
Var
iabi
lity+
+an
dna
sal
arti
cula
tion
Art
icul
ator
yva
riab
ility
++
Act
ive
CT
Rs
proc
esse
spe
rsis
t
A Harding and P Grunwell344
palate repair but with a residual cleft in the hard palate his range of consonantsincluded [d] which was particularly surprising since the hard palate remainedunrepaired Whilst it is unlikely that toddlers of 18 months could be consciouslytrying to compensate for articulatory inadequacy in producing velar plosives inbabble prior to soft palate repair and an alveolar plosive prior to hard palate repairboth these subjects showed evidence of actively pursuing their articulatory potential
Table 6 summarizes changes following surgery to repair the hard palate in moremature speech patterns These subjects who were aged 66 and 100 pre-operativelyhad learned to speak with residual clefts and were apparently unaware of theconsonant productions that failed to match normal production
Subject MS used only passive processes in his speech pattern He realized someconsonants nasally such that lsquoballrsquo was [mO~] and lsquosockrsquo was [(sk)n
deg Aacute~ k] Looking atpost-operative changes at age 76 his consonant production was normal but hisresonance had become hyponasal Pre-operatively at age 66 Subject JF was usingseveral active and passive processes The active processes were unaVected by surgerybut passive processes were eliminated
Fistula repair was carried out at age 100 on Subject DA who had many activeprocesses and very variable articulation pre-operatively Post-operatively at age110 he was not using non-oral pharyngeal and glottal active processes or nasalrealizations but many oral cleft-type realizations remained
As shown in table 7 hard palate re-repair and pharyngoplasty was carried outon two subjects whose hard palate repairs had been unsuccessful at approximately4 years Subject NC assessed pre-operatively at age 56 was using predominantlypassive processes in her speech She was also using [ j] for fricatives s S whichwas thought to be an active process At age 60 following hard palate re-repair andpharyngoplasty all cleft-type processes had been eliminated without post-operativespeech therapy Since [ j] for s apparently resolved spontaneously followingsurgery it can be assumed that this was a passive process in this speech sample
Subject CP who underwent this procedure presented pre-operatively at age 46with both passive and active processes but his nasal resonance was not consistentlyhypernasal In addition to his cleft-related speech disorder this subject had additionaldevelopmental speech diYculties which were identi ed as being unrelated to thecleft Post-operatively at age 56 little had changedmdashnotably the passive processnasal [m] for b was retained His nasal resonance had become hyponasal andthere was no apparent bene t from surgical intervention The realization of b as[m] had become phonologically stable and surgery alone had not destabilized thephonological system This realization may have been a passive product of VPI inearly speech acquisition which had subsequently become part of a phonologicaldisorder Post-operatively CPrsquos phonetic repertoire did increase but the phonologicaldistribution was variable Plosive targets were still realized as nasals in spontaneousspeech at the nal speech recording at age 76 This was not as an inevitableconsequence of VPI but a result of an inability to destabilize the phonologicalprocess determining that voiced plosives would be realized as nasals This resultfollowing surgery highlights the importance of identifying phonological learningproblems and distinguishing them from structural constraints on articulationIn CPrsquos case pre-operative exploration of the eVect of nares occlusion duringspeech might have indicated that structural change would not improve consonantproduction spontaneously
A general observation was that consonant realizations did not move rapidly
Active versus passive cleft-type speech characteristics 345
Tab
le7
EV
ects
ofha
rdpa
late
re-r
epai
ran
dp
hary
ngo
pla
sty
Subj
ect
Surg
ery
Pre
-ope
rati
vesp
eech
patt
ern
Post
-ope
rativ
ech
ange
sin
spee
ch
Stud
y2
NC
Har
dpa
late
re-r
epai
ran
d5
6Pa
ssiv
ecl
eft-
type
proc
esse
s6
0A
llcl
eft-
type
phar
yngo
plas
ty5
10[
j]
for
fric
ativ
espr
oces
ses
elim
inat
ed[
h]
for
plos
ives
SIW
IV
aria
ble
arti
cula
rypr
ecis
ion
CP
Har
dpa
late
repa
iran
d4
6Pa
ssiv
ean
dac
tive
proc
esse
s5
6Pa
ssiv
epr
oces
sph
aryn
gopl
asty
50
Pho
nolo
gica
lco
nfus
ion
[m]
for
[b
]re
tain
edH
ypon
asal
nasa
lsPe
rsis
ting
phon
olog
ical
conf
usio
ns
A Harding and P Grunwell346
from incorrect to correct but progressed incrementally towards normal realizationsas described by Morley (1970) Where an early realization of target s might beglottal [h] a gradual pattern of change showed subsequent realizations to bepharyngeal [Eacute] then uvular [X] then velar [x] and eventually palatal [c] or lateral [Euml]It was interesting to note that speech patterns continued to change as late as90ndash110 years with the result that diVerences related to surgical timing and cleft-type gradually disappeared Persisting stulae were thought to account for the mostmarked cleft type processes at age 90
Implications for surgical management
This analysis of speech changes following surgery suggests some implications forsurgical management which are compatible with Sell and Grunwellrsquos (1990) ndingsin the Sri Lankan study
Surgery can change passive speech processes but it is also possible that speechtherapy may be able to change passive patterns Surgery alone is unlikely to modifyactive cleft-type processes whereas speech therapy should be able to modify activeprocesses Indications from these case studies is that where speech is the primaryproblem speech assessment should distinguish between active and passive processesin order to evaluate the necessity for full investigations and to plan therapeuticintervention Where past speech therapy has not been successful it cannot beassumed that surgical intervention will facilitate further speech progress A furthercourse of speech therapy which is sensitive to active versus passive processes todevelopmental phonological in uences on cleft-type speech development and toarticulatory diYculties in diVerent speech contexts might facilitate optimal progressWhere structural imperfection exists it is quite possible for single-word productionto be more precise than target realizations in spontaneous speech This may not bea failure of phonological generalization (Grunwell 1992) but the result of diYcultysustaining the necessary lsquoarticulatory eVort rsquo (Harding and Grunwell 1993) resultingin articulatory imprecision Deteriorating articulatory accuracy should not be over-looked in interpretation of speech results
An analytical protocol
As a result of analysing the speech data and identifying the active and passiveprocesses a protocol has been developed which records examples of each cleft-typeprocess over a series of assessments It demonstrates the progression of individualprocesses towards an adult target (see the Appendix) At each assessment onecolumn is used to indicate nasal resonance nasal emission and nasal turbulenceratings and cleft-type processes Changes in the nature of error realizations mightshow progress towards target consonants Hence whilst the total correct scoremight not have increased increments of change can be observed This observationof patterns of change may function as an adjunct to GOSSPASSrsquo98 (Sell et al 1998)giving access to a greater depth of both quantitative and qualitative data aboutconsonant production in relation to resonance nasal emission nasal turbulenceoral structure and cleft-type
Active versus passive cleft-type speech characteristics 347
Diagnostic implications
Passive versus active nasal fricatives
The important management consideration related to this distinction is that an activenasal fricative is an established phonological process which is unlikely to be directlyaVected by surgery alone Therapy would be necessary to destabilize nasal realizationsof oral consonants In contrast passive nasal fricatives may be eliminated by surgeryOf particular relevance is diVerential diagnosis between passive and active nasalfricatives in surgical and therapeutic management When hypernasality co-occurswith nasal air ow during consonant production which can be redirected by nose-holding passive nasal fricatives are diagnosed These would be transcribed as [(sk)n
deg]
passive alveolar nasal fricatives [(Wk)mdeg
] bilabial nasal fricatives or [(fk)Iacutedeg ] labiodentalnasal fricatives Full VPI investigations would be recommended to diagnose thenature of the structural or functional de ciency and distinguish between velopharyn-geal incompetence and velopharyngeal mislearning
It is highly likely that plosive targets would be aVected by reduced intra-oral airpressure such that plosives would either be realized by nasal counterparts eg bd[ [m n] or [b d] may be nasalized and weak Voiceless plosives may be eitheraccompanied by nasal emission [p t k] or realized as glottal fricative [h]
Production of the target sentence lsquoI saw Sam sitting on a busrsquo might be
[aI (sk)ndeg O~ (sk)n
degaelig~m (sk)n
deg IhIn Aacute~n mouml~(sk)ndeg] passive processes and
[aI xO xaeligm xIkIIcirc AacuteIcirc goumlx] active processes
Contribution to surgical management decisions
Passiveactive interpretation of clinical assessments might facilitate surgical manage-ment decisions If noseholding does not facilitate correct production of targetconsonants then it is likely that an alternative articulatory pattern has becomephonologically established ie particular realizations for one or more targets areconsistently distributed in the phonological system These realizations may haveevolved because of initial diYculty producing articulatory targets and subsequentlystabilized within the phonological system Grundy and Harding (1995) refer to thisphenomenon as an lsquoarticulatory disorder with phonological consequencesrsquo
Therapy
Where obvious structural defects or diagnosed dysfunction exists clinicians fre-quently defer therapeutic intervention until surgery has been undertaken Theexpectation would be that normal structure and function is essential for normalspeech However pre-operative therapy may facilitate oral consonant productionwhich may serve to reduce hypernasal resonance Hence therapy prior to surgerymay avoid unnecessary surgery or reduce the extent of surgery required All activeprocesses are likely to require therapy
Principled selection of targets for therapy
Speech patterns frequently evidence a mixture of apparently passive and activeprocesses which complicates decisions about target selection Target selection can
A Harding and P Grunwell348
be based on assessment of which consonant targets can be most easily elicted inisolation (stimulability) This may lead to a sequence of target selection which isopposite to the sequence of consonant acquisition in normal development Forexample where reduced intra-oral pressure is present in a passive pattern [T] maybe easier to elicit in imitation than more nely grooved [s] or [S] Therapy maytarget [T] followed by [S ] and nally [s] As in non-cleft phonological therapywhere a class of consonants is aVected by the cleft then it is helpful to target theentire class The following decision-making process can be applied for both activeand passive processes
Decision making procedure for target selection
(1) Voiced versus voiceless targets(2) Front versus back placements(3) Syllable initial versus syllable nal targets(4) Plosives versus fricative targets
Voiceless plosives and fricatives are produced with an open glottis whichfacilitates topping up of air ow from the lungs hence voiceless plosive and fricativetargets are frequently more successful than voiced counterparts (Isshiki and Ringel1964) Front targets usually cause more diYculty than back particularly where analveolar defect or stula exists Contrary to normal development back targets maybe targeted before front Word- nal targets generally require less oral air pressurethan word initial targets and similarly fricatives may be more easily elicited thanplosives Fricatives do require a greater volume of air than plosives (Fletcher 1985)but in the presence of nasal escape weak fricative production appears to be morereadily achieved than weak plosive production Since nal fricatives would normallybe acquired in advance of word-initial fricatives (Ferguson 1978) targeting word- nal fricatives is frequently a productive starting point for therapy
Principles of therapy for passive processes
(1) Use of soft attack similar to gentle whisper for all target models ensuresminimal articulatory eVort (Harding and Grunwell 1993) and requires min-imal intra-oral air pressure It may be appropriate to gradually increase thearticulatory attack when the articulatory posture and evidence of intendedoral air ow have been established
(2) Slightly stretched duration of segment transitions in models of consonantto vowel (CndashV) or vowel to consonant (VndashC) facilitates review of motorplanning and extends the available time for execution of the new motorprogrammer whilst maintaining control of the oral airstream
(3) Noseholding can be used to provide exclusively oral air ow Gradual releaseof the nostrils during production of sustained [VVVVVf ] or [hhhhh ] allowsthe child to attempt to sustain an oral consonant despite increasing nasalemission This maximizes the use of available oral air ow Procedures forusing noseholding are described in some detail by Golding-Kushner (1995)
Principles of therapy for active processes
This is more like phonological therapy and can follow Grunwellrsquos (1991) processesfor phonological change and principled decision-making (Grunwell 1992) Some
Active versus passive cleft-type speech characteristics 349
examples are given here by way of illustration of ways to eVect the rst twoprocesses of change which may need to be approached diVerently in cleft palateversus non-cleft speech disorders DiVerent approaches may also be appropriate formodifying active versus passive cleft-type processes
Innovation production of new targets Some useful principles
(1) Introduction of new lsquonon-speech likersquo targets in sound play using a conson-ant sound segment model such as [ph ] note not a syllable like [p] whichis the type of pronunciation used when target sounds are presented as lettersfor reading Target [s] might be introduced as a lsquoTrain Slowing Down Noisersquo[ts ts ts tssssssss]
(2) lsquoNew consonantsrsquo can later be modelled and elicited in soft productions ofsyllable structure [tssssndashi] [ indashtssss] which can subsequently be identi ed assimilar to words lsquosearsquo and lsquoeatsrsquo
(3) lsquoDeferring responsibilityrsquo transfers responsibility or lsquoblamersquo for errors fromthe child and attributes it to the articulators eg lsquoyour tongue is havingtrouble with hellip rsquo lsquoLetrsquos show your tongue how to hellip rsquo
(4) New targets can be modelled repeatedly and recorded on audio or videotape which can be listened to at home
(5) Targeting classes of consonants (eg alveolars t d s n l voiceless fricativesf s S perhaps with aVricate T avoids phonological confusion whichmight occur if production ofsis achieved whilst other alveolar targetsremain backed The risk is that s might not integrate into the phonologicalsystem unless all backed alveolar consonants are destabilized
(6) Increased eye contact during auditory and production work can be invaluablein holding visual and auditory attention and ensures that visual informationabout the sound has been processed This is easily achieved by the clinicianlifting any focus of the childrsquos attention close to hisher mouth at theprecise moment when the target is modelled
Stimulation of non-speech related sounds such as a lsquoTrain Slowing DownNoisersquo [ts ts tsss] con rms that target [s] is physically achievable whether or not[ssss] can be imitated Some children continue to access [s] through the lsquoTrainSlowing Down Noisersquo throughout therapy until it is occurring spontaneouslywithout conscious planning This can be an eVective means of underminingestablished motor programmers (Hewlett 1990) for active cleft-type processes
Destabilizing active processes
As it is likely that children will be unaware of each occurrence of their alternativearticulatory pattern for speci c consonant errors it is preferrable to destabilizeactive processes with minimal conscious eVort by the child As children becomeaware of their mismatches they frequently add the newly acquired target realizationto their existing production eg target word tu childrsquos old realization [ku] childrsquoscorrected realization [t-ku] Destabilization can be achieved with minimal consciouseVort through input therapy techniques such as auditory bombardment (Lancasterand Pope 1989) auditory decision-making such as lsquowhich bear says this wordproperlyrsquo Red Bear says lsquotworsquo or Blue Bear says lsquocoorsquo This type of strategy oftenprecipitates attention to the target consonant with possible lsquoreplayrsquo and lsquoreviewrsquo of
A Harding and P Grunwell350
their own production Frequent stimulation of cognitive alertness to the targetconsonant can develop awareness without confronting the child with errors orrisking hisher failure The child is then free to attempt to repair hisher ownrealization to continue to re ect and to silently rehearse the adult realizationTraditional articulation therapy is thus combined with development of metaphonol-ogical skills ie the ability to re ect upon onersquos own speech production The resultshould be that new target realizations will be more phonologically stable thanexclusively production-based articulation therapy might have facilitated
Stabilizationgeneralization
Procedures to ensure stabilization and generalization of new target consonantswould be as described by Grunwell (1992) Success may be constrained by theconsiderable articulatory eVort sometimes required to maintain pressure consonantproduction in spontaneous speech (Harding and Grunwell 1993)
Conclusions
In speech assessment it is helpful to distinguish between errors which are cleft-type and non-cleft type and those which are part of active versus passive processesThe active and passive processes have been de ned and their phonological implica-tions discussed Focus on active and passive processes has facilitated focus on thephonological consequences of cleft palate on speech development In the futureawareness of the likely eVect of a cleft palate on normal phonological developmentcould avoid extended periods of unsuccessful clinical intervention Furthermoresensitivity to the relationship between phonological processes and structural con-straints should facilitate theoretically based management decisions Incidences suchas the case of CP in which nasal realizations were thought to indicate VPI but weresubsequently unaVected by surgery might be avoided if phonological analysiscontributes to management decisions
Surgery did improve hypernasal resonance and eliminated passive processes buthad little eVect on active processes Active processes in younger subjects werethought to require therapeutic intervention but in the longer term the oldersubjects showed few cleft-type processes Whilst it is possible that active cleft-typeprocesses may resolve with increasing age the implication for the future is thatactive cleft-type processes should be treated with skilled therapeutic interventionnot surgery Therapy which addresses the phonological consequences of cleft palateon speech development by combining metaphonologicalphonologicalarticulatoryapproaches is likely to be successful
References
Albery E 1991 Consonant articulation in the diVerent types of cleft lip and palate UnpublishedMPhil thesis Leicester Polytechnic
Albery E and Grunwell P 1993 Consonant articulation in diVerent types of cleft palate InP Grunwell (Ed) Analysing Cleft Palate Speech (London Whurr)
Ferguson C A 1978 Fricatives in child language acquisition In V Honsa and M Hardmann-Battista (Eds) Papers on Linguistics and Child Language (Mouton The Hague)
Fletcher S G 1985 Speech production and oral motor skill in an adult with an unrepaired palatalcleft Journal of Speech and Hearing Disorders 50 254ndash261
Active versus passive cleft-type speech characteristics 351
Golding-Kushner K J 1995 Treatment of articulation and resonancne disorders associated withcleft palate management and VPI In R Shprintzen (Ed) Cleft Palate Speech Management AMultidisciplinary Approach (St Louis Mosby)
Grundy K and Harding A 1995 Developmental speech disorders In K Grundy (Ed) Linguisticsin Clinical Practice (2nd edition) (London Whurr)
Grunwell P 1985 Phonological Assessment of Child Speech (Windsor NFER-Nelson)Grunwell P 1987a Clinical Phonology (2nd edition) (London Croom Helm)Grunwell P 1987b PACS Pictures Language Elicitation Materials (Windsor NFER-Nelson)Grunwell P 1991 Processes of phonological change in developmental speech disorders Clinical
Linguistics and Phonetics 6 101ndash122Grunwell P 1992 Principled decision making in the remediation of children with phonological
disorders In P Fletcher and D Hall (Eds) Specic Speech and Language Disorders in Children(London Whurr)
Grunwell P and Harding A 1995 PACSTOYS A Screening Assessment of Phonological Development(Windsor NFER-Nelson)
Grunwell P and Harding A 1996 A note on describing types of nasality Clinical Linguistics andPhonetics 10 157ndash161
Harding A 1993 An Investigation into the Relationship Between Timing of Cleft Palate Repairand Speech Development Unpublished PhD thesis
Harding A and Grunwell P 1993 The relationship between speech and timing of hard palaterepair In P Grunwell (Ed) Analysisng Cleft Palate Speech (London Whurr)
Harding A and Grunwell P 1996 Characteristics of cleft palate speech European Journal ofDisorders of Communication 31 331ndash358
Henningsson G and Isberg A M 1986 Velopharyngeal movement patterns in patients alternatingbetween oral and glottal articulation A clinical and cineradiographicical study Cleft Palate Journal23 1ndash9
Hewlett N 1990 Processes of development and production In P Grunwell (Ed) DevelopmentalSpeech Disorders (Edinburgh Churchill Livingstone)
Hotz M M Gnoinski W M Nussbaumer H and Kistler E 1978 Early orthopaedics in CLPcases guidelines for surgery Cleft Palate Journal 15 405ndash411
Hutters B and Brondsted K 1987 Strategies in cleft palate with special reference to DanishCleft Palate Journal 24 127ndash136
Isshiki N and Ringel R 1964 Airow during the production of selected consonants Journal ofSpeech and Hearing Research 7 233ndash244
Kummer A W Curtis C Wiggs M Lee L and Strife J L 1992 Comparison of velopharyngealgap size in patients with hypernasality hypernasality with nasal emission and nasal emissionor nasal turbulence (rustle) as the primary speech characteristic Cleft-palate-Craniofacial Journal29 152ndash156
Lancaster G and Pope L 1989 Working with Childrenrsquos Phonology (Oxford Winslow)Morley M E 1970 Cleft Palate and Speech (7th edition) (Edinburgh Churchill Livingstone)Russell V J 1991 Speech Development in Children with Cleft Lip and Palate Unpublished PhD
thesis Leicester PolytechnicRussell V J and Grunwell P 1993 Speech development in children with cleft lip and palate In
P Grunwell (Ed) Analysing Cleft Palate Speech (London Whurr)Sell D A and Grunwell P 1990 Speech results following late palatal surgery in previously
unoperated Sri Lankan adolescents with cleft palate Cleft Palate Journal 27 162ndash168Sell D Harding A and Grunwell P 1994 GOSSPASS A screening assessment of cleft palate
speech European Journal of Disorders of Communication 29 1ndash15Sell D Harding A and Grunwell P 1998 GOSSPASSrsquo98 An assessment for speech disorders
associated with cleft palate andor velopharyngeal dysfunction International Journal of Languageamp Communication Disorders ( in press)
Shorter E 1995 A spectographic analyis of child homophones Unpublished honours project DeMontfort University Leicester
Stenglehoffen J 1989 Nature and causes of communication diYculties In J Stengelhofen (Ed)Cleft Palate Nature and Remediation of Communication Problems (Edinburgh Churchill Livingstone)
Trost J E 1981 Articulatory additions to the classical description of the speech of persons withcleft palate Cleft Palate Journal 18
Trost-Cardamone J E 1990 The development of speech assessing cleft palate misarticulationsIn D A Kernahan and S N Rosenstein (Eds) Cleft Lip and Palate A System of Management(Baltimore Williams amp Wilkins)
A Harding and P Grunwell352
Appendix Active passive analysis of cleft palate speech

Active versus passive cleft-type speech characteristics 339
consonants can be more diYcult to produce than voiceless consonants (Isshiki andRingel 1964) Distinction between active versus passive nasal realizations of plosivetargets was made in the same way that active and passive nasal fricatives weredistinguished by observing the eVect of noseholding on consonant production Inpassive nasal realizations noseholding facilitated normal consonant production(Golding-Kushner 1995)
Nasal emission accompanying consonants [pk sk]
Nasal emission was frequently heard accompanying consonants but on occasions itapparently replaced consonants It has been linked with velopharyngeal incompet-ence (VPI) (Kummer et al 1992)
Results
Comparison of activepassive processes in the speech data
Quantitative results of Hardingrsquos research into the relationship between timing ofsurgery and speech development have already been published (Harding andGrunwell 1993) The following interpretation of the data speci cally identi esactivepassive cleft-type processes in relation to oral structure in a wide age rangeof subjects (16ndash130) Tables 1 2 3 and 4 show the passive and active processeson the left-hand column and the subjectrsquos code along the top The code identi esthose subjects who were treated with 1-stage versus 2-stage surgery Comparisonof the 4 tables at age 46 (BCLP and UCLP) at age 90 and at age 130 illustratesa pattern of diminishing cleft-type processes with increasing age Irrespective ofsurgical timing few cleft-type processes remained at age 130 (table 4) A generalobservation was that earlier speech samples (ages 16ndash76) frequently combined
Table 1 Cleft-type processes in BCLP subjects at age 46 (studies 1 and 2)
1-stage surgery 2-stage surgery
A G Rf JW D B JF JG AB
Passive cleft-type processespredominantly sonorant articulation m
weak articulation m m m m m m m m
voiceless h for plosive m m m m m
nasal release of plosives m m m m m
nasal emission with consonants m m m m m m
passive nasal fricativeActive cleft-type processes
nasal fricatives m m m m m m m m
pharyngeal glottal articulation m m m m m m m m
backing to uvular m m m m m m m m
backing to velar m m m m m m m m m
lateral palatal fricatives m m m m m m m m m
double articulation m m m m m m m m m
gliding fricative m m
f=post-operative stula
A Harding and P Grunwell340
Table 2 Cleft-type processes in UCLP subjects at age 46 (study 2)
1-stage surgery 2-stage surgery
SE TB CK MS NC TS ZG CP
Passive cleft-type processespredominantly sonorant artic m
weak articulation m m m
voiceless h for plosives m m m
nasal release of plosives m m m
nasal emission with consonants m m
passive nasal fricative m m
Active cleft-type processesnasal fricativepharyngeal glottal articulation m m m
backing to uvular m
backing to velar m m
lateral palatal fricatives m m m m m
double articulation m m m m m m
gliding fricative m
Table 3 Cleft-type processes at age 90
2-stage surgery 2-stage surgery1-stage surgery completed at 4 yrs completed at 8 yrs
DAf SBf RL NR JD AR LJ RP MB
Passive cleft-type processespredominantly sonorant articweak articulation m
voiceless h for plosives m m
nasal release of plosives m m
nasal emission with consonants m m m m
passive nasal fricatives m m
Active cleft-type processesnasal fricatives m m
pharyngeal glottal articulation m m
backing to uvular m m
backing to velar m m m m m m m
lateral palatal fricatives m m m m m m m
double articulation m m m m m
gliding fricative m
f=subject had a stula
both active and passive strategies whereas later samples (ages 90ndash130) rarelyevidenced passive processes
At age 46 four out of ve BCLP subjects used active non-oral pharyngeal andglottal processes and oral velar and uvular fricatives irrespective of surgical status(see table 1) All had some anterior palatal defect which might have reduced theirpotential to achieve intra-oral pressure
By comparison two out of three partially repaired 2-stage UCLP subjects at age46 (table 2) showed evidence of passive processes This suggested that their
Active versus passive cleft-type speech characteristics 341
Tab
le4
Spee
chin
rela
tion
tosu
rgic
altim
ing
atag
e13
0
2-st
age
surg
ery
2-st
age
surg
ery
1-st
age
surg
ery
subj
ects
com
plet
edat
4yr
sco
mpl
eted
at8
yrs
1-A
1-B
1-C
1-D
1-E
1-F
24-
G2
4-H
24-
J2
8-K
28-
L2
8-M
Pass
ive
clef
t-ty
pepr
oces
ses
pred
omin
antly
sono
rant
artic
wea
kar
ticul
atio
nm
voic
eles
sh
fo
rpl
osiv
esna
sal
rele
ase
ofpl
osiv
esna
sal
emis
sion
with
cons
onan
tsm
pass
ive
nasa
lfr
icat
ives
Act
ive
clef
t-ty
pepr
oces
ses
nasa
lfr
icat
ives
phar
ynge
alg
lott
alar
ticul
atio
nba
ckin
gto
uvul
arba
ckin
gto
vela
rm
m
late
ral
pala
tal
fric
ativ
esm
mm
doub
lear
ticul
atio
ngl
idin
gfr
icat
ive
1=1-
stag
esu
rger
ysu
bjec
ts
24=
2-st
age
surg
ery
hard
pala
tere
pair
edat
abou
t4
yrs
28=
2-st
age
surg
ery
with
hard
pala
tere
pair
edat
abou
t8
yrs
A Harding and P Grunwell342
unrepaired hard palates had in fact restricted their phonetic repertoire imposing aneed for individual adaptability The additional active processes employed by thesesubjects were presumably a response to the restrictions imposed by their oro-nasalstructure and velopharyngeal function at the time of consonant acquisition Asshown in table 2 the most common active cleft-type processes persisting at age46 with a residual cleft of the hard palate were backing double articulation andlateralpalatal articulation Two 1-stage surgery subjects whose entire palates hadbeen repaired at ages 09 and 010 did not use any cleft-type processes at age 46
By age 90 (table 3) a much-diminished number of cleft type processes wasevident except in subjects with sizeable anterior stulae who had received littlespeech and language therapy A similarity was noted between the speech patternsof 1-stage surgery subjects with stulae (DA and SB) at age 90 (table 3) and theyounger BCLP subjects at age 46 (table 1) who also had anterior palatal defectsThey included non-oral realizations of t d s k g occasional nasal fricatives andpharyngealglottal articulations Fistulae had apparently continued to in uencearticulation and phonological development in these subjects
Finally at age 130 (table 4) the diVerences between 1-stage and 2-stage surgerysubjects had diminished leaving only one 2-stage subject with occasional backingand four subjects with slight palatal and lateral release of fricative consonants Onlytwo of the 1-stage surgery subjects were using minor distortions of grooved fricativeproduction
Whilst there were apparent trends in speech production relating to surgicaltiming and oral structure it is noted that there were exceptions to each tentativegeneralization Subjects with marked structural imperfections occasionally producedrealizations of which they would not have been thought capable and subjects withno visible imperfections produced inexplicably distorted speech patterns It istherefore concluded that whilst there is homogeneity in the range of processesproduced by this population assumptions cannot be made about speech based onsurgical timing or type of cleft Tentative predictions based on detailed assessmentmay be clinically very useful
EVects of surgery on speech
Activepassive processes have identi ed those cleft-type characteristics thought tobe associated with a physical inability to produce pressure consonants The followinganalysis of speech changes after surgical intervention at diVerent ages identi es thechanges eVected by surgery when intra-oral pressure could be more readily achieved
Two children were rst recorded prior to the rst stage of a 2-stage procedureTheir lips were repaired at approximately 6 months of age and soft palate repairwas carried out at ages 18 and 19 respectively Their hard palates were leftunrepaired to facilitate unrestricted growth of the mid-face (Hotz et al 1978) Pre-and post-operative consonant-like sounds present in the recorded speech samplesare listed in table 5 Interestingly prior to soft palate repair both these childrenproduced some oral consonants Subject B was producing pressure consonants [kg] in his babble prior to soft palate repair Considering that he had an unrepairedbilateral cleft palate at this point it was surprising that he had any oral consonantsPost-operatively at 20 years he used [b bkm t d g gkb] which indicated that surgeryto repair the soft palate had facilitated an increased range of oral pressure consonantsSubject D was producing [p b k g] pre-operatively Post-operatively following soft
Active versus passive cleft-type speech characteristics 343
Tab
le5
EV
ects
ofso
ftp
alat
ere
pair
atag
e1
6on
BC
LP
subj
ects
h
ard
pal
ate
rem
ain
sun
repa
ired
2-st
age
subj
ects
Surg
ery
Pre
-ope
rati
vesp
eech
patt
ern
atag
e1
6Po
st-o
pera
tive
chan
ges
insp
eech
atag
e2
0
Stud
y1
BSo
ftpa
late
repa
irat
16
Adu
ltta
rget
sk
gA
t2
0[b
b kmg kb
td
g]D
Soft
pala
tere
pair
17
Adu
ltta
rget
sp
bk
gA
t2
0[p
bd
b kdk
g]
Tab
le6
EV
ects
ofha
rdpa
late
rep
air
atag
e6
6an
d
stu
lare
pair
atag
e10
0
Subj
ect
Surg
ery
Pre
-ope
rati
vesp
eech
patt
ern
Post
-ope
rati
vech
ange
sin
spee
ch
MS
Har
dpa
late
repa
ir6
6Pa
ssiv
epr
oces
s7
6E
limin
ated
pass
ive
proc
ess
Var
iabl
ena
sal
rele
ase
ofco
nson
ants
Hyp
onas
alna
sals
JFH
ard
pala
tere
pair
(uns
ucce
ssfu
l)6
6Se
vera
lac
tive
and
pass
ive
proc
esse
s7
6A
ctiv
epr
oces
ses
rem
aine
dPa
ssiv
epr
oces
ses
elim
inat
ed
DA
Fis
tula
repa
ir10
0A
ctiv
epr
oces
ses
110
Elim
inat
ion
ofph
aryn
geal
glo
ttal
Var
iabi
lity+
+an
dna
sal
arti
cula
tion
Art
icul
ator
yva
riab
ility
++
Act
ive
CT
Rs
proc
esse
spe
rsis
t
A Harding and P Grunwell344
palate repair but with a residual cleft in the hard palate his range of consonantsincluded [d] which was particularly surprising since the hard palate remainedunrepaired Whilst it is unlikely that toddlers of 18 months could be consciouslytrying to compensate for articulatory inadequacy in producing velar plosives inbabble prior to soft palate repair and an alveolar plosive prior to hard palate repairboth these subjects showed evidence of actively pursuing their articulatory potential
Table 6 summarizes changes following surgery to repair the hard palate in moremature speech patterns These subjects who were aged 66 and 100 pre-operativelyhad learned to speak with residual clefts and were apparently unaware of theconsonant productions that failed to match normal production
Subject MS used only passive processes in his speech pattern He realized someconsonants nasally such that lsquoballrsquo was [mO~] and lsquosockrsquo was [(sk)n
deg Aacute~ k] Looking atpost-operative changes at age 76 his consonant production was normal but hisresonance had become hyponasal Pre-operatively at age 66 Subject JF was usingseveral active and passive processes The active processes were unaVected by surgerybut passive processes were eliminated
Fistula repair was carried out at age 100 on Subject DA who had many activeprocesses and very variable articulation pre-operatively Post-operatively at age110 he was not using non-oral pharyngeal and glottal active processes or nasalrealizations but many oral cleft-type realizations remained
As shown in table 7 hard palate re-repair and pharyngoplasty was carried outon two subjects whose hard palate repairs had been unsuccessful at approximately4 years Subject NC assessed pre-operatively at age 56 was using predominantlypassive processes in her speech She was also using [ j] for fricatives s S whichwas thought to be an active process At age 60 following hard palate re-repair andpharyngoplasty all cleft-type processes had been eliminated without post-operativespeech therapy Since [ j] for s apparently resolved spontaneously followingsurgery it can be assumed that this was a passive process in this speech sample
Subject CP who underwent this procedure presented pre-operatively at age 46with both passive and active processes but his nasal resonance was not consistentlyhypernasal In addition to his cleft-related speech disorder this subject had additionaldevelopmental speech diYculties which were identi ed as being unrelated to thecleft Post-operatively at age 56 little had changedmdashnotably the passive processnasal [m] for b was retained His nasal resonance had become hyponasal andthere was no apparent bene t from surgical intervention The realization of b as[m] had become phonologically stable and surgery alone had not destabilized thephonological system This realization may have been a passive product of VPI inearly speech acquisition which had subsequently become part of a phonologicaldisorder Post-operatively CPrsquos phonetic repertoire did increase but the phonologicaldistribution was variable Plosive targets were still realized as nasals in spontaneousspeech at the nal speech recording at age 76 This was not as an inevitableconsequence of VPI but a result of an inability to destabilize the phonologicalprocess determining that voiced plosives would be realized as nasals This resultfollowing surgery highlights the importance of identifying phonological learningproblems and distinguishing them from structural constraints on articulationIn CPrsquos case pre-operative exploration of the eVect of nares occlusion duringspeech might have indicated that structural change would not improve consonantproduction spontaneously
A general observation was that consonant realizations did not move rapidly
Active versus passive cleft-type speech characteristics 345
Tab
le7
EV
ects
ofha
rdpa
late
re-r
epai
ran
dp
hary
ngo
pla
sty
Subj
ect
Surg
ery
Pre
-ope
rati
vesp
eech
patt
ern
Post
-ope
rativ
ech
ange
sin
spee
ch
Stud
y2
NC
Har
dpa
late
re-r
epai
ran
d5
6Pa
ssiv
ecl
eft-
type
proc
esse
s6
0A
llcl
eft-
type
phar
yngo
plas
ty5
10[
j]
for
fric
ativ
espr
oces
ses
elim
inat
ed[
h]
for
plos
ives
SIW
IV
aria
ble
arti
cula
rypr
ecis
ion
CP
Har
dpa
late
repa
iran
d4
6Pa
ssiv
ean
dac
tive
proc
esse
s5
6Pa
ssiv
epr
oces
sph
aryn
gopl
asty
50
Pho
nolo
gica
lco
nfus
ion
[m]
for
[b
]re
tain
edH
ypon
asal
nasa
lsPe
rsis
ting
phon
olog
ical
conf
usio
ns
A Harding and P Grunwell346
from incorrect to correct but progressed incrementally towards normal realizationsas described by Morley (1970) Where an early realization of target s might beglottal [h] a gradual pattern of change showed subsequent realizations to bepharyngeal [Eacute] then uvular [X] then velar [x] and eventually palatal [c] or lateral [Euml]It was interesting to note that speech patterns continued to change as late as90ndash110 years with the result that diVerences related to surgical timing and cleft-type gradually disappeared Persisting stulae were thought to account for the mostmarked cleft type processes at age 90
Implications for surgical management
This analysis of speech changes following surgery suggests some implications forsurgical management which are compatible with Sell and Grunwellrsquos (1990) ndingsin the Sri Lankan study
Surgery can change passive speech processes but it is also possible that speechtherapy may be able to change passive patterns Surgery alone is unlikely to modifyactive cleft-type processes whereas speech therapy should be able to modify activeprocesses Indications from these case studies is that where speech is the primaryproblem speech assessment should distinguish between active and passive processesin order to evaluate the necessity for full investigations and to plan therapeuticintervention Where past speech therapy has not been successful it cannot beassumed that surgical intervention will facilitate further speech progress A furthercourse of speech therapy which is sensitive to active versus passive processes todevelopmental phonological in uences on cleft-type speech development and toarticulatory diYculties in diVerent speech contexts might facilitate optimal progressWhere structural imperfection exists it is quite possible for single-word productionto be more precise than target realizations in spontaneous speech This may not bea failure of phonological generalization (Grunwell 1992) but the result of diYcultysustaining the necessary lsquoarticulatory eVort rsquo (Harding and Grunwell 1993) resultingin articulatory imprecision Deteriorating articulatory accuracy should not be over-looked in interpretation of speech results
An analytical protocol
As a result of analysing the speech data and identifying the active and passiveprocesses a protocol has been developed which records examples of each cleft-typeprocess over a series of assessments It demonstrates the progression of individualprocesses towards an adult target (see the Appendix) At each assessment onecolumn is used to indicate nasal resonance nasal emission and nasal turbulenceratings and cleft-type processes Changes in the nature of error realizations mightshow progress towards target consonants Hence whilst the total correct scoremight not have increased increments of change can be observed This observationof patterns of change may function as an adjunct to GOSSPASSrsquo98 (Sell et al 1998)giving access to a greater depth of both quantitative and qualitative data aboutconsonant production in relation to resonance nasal emission nasal turbulenceoral structure and cleft-type
Active versus passive cleft-type speech characteristics 347
Diagnostic implications
Passive versus active nasal fricatives
The important management consideration related to this distinction is that an activenasal fricative is an established phonological process which is unlikely to be directlyaVected by surgery alone Therapy would be necessary to destabilize nasal realizationsof oral consonants In contrast passive nasal fricatives may be eliminated by surgeryOf particular relevance is diVerential diagnosis between passive and active nasalfricatives in surgical and therapeutic management When hypernasality co-occurswith nasal air ow during consonant production which can be redirected by nose-holding passive nasal fricatives are diagnosed These would be transcribed as [(sk)n
deg]
passive alveolar nasal fricatives [(Wk)mdeg
] bilabial nasal fricatives or [(fk)Iacutedeg ] labiodentalnasal fricatives Full VPI investigations would be recommended to diagnose thenature of the structural or functional de ciency and distinguish between velopharyn-geal incompetence and velopharyngeal mislearning
It is highly likely that plosive targets would be aVected by reduced intra-oral airpressure such that plosives would either be realized by nasal counterparts eg bd[ [m n] or [b d] may be nasalized and weak Voiceless plosives may be eitheraccompanied by nasal emission [p t k] or realized as glottal fricative [h]
Production of the target sentence lsquoI saw Sam sitting on a busrsquo might be
[aI (sk)ndeg O~ (sk)n
degaelig~m (sk)n
deg IhIn Aacute~n mouml~(sk)ndeg] passive processes and
[aI xO xaeligm xIkIIcirc AacuteIcirc goumlx] active processes
Contribution to surgical management decisions
Passiveactive interpretation of clinical assessments might facilitate surgical manage-ment decisions If noseholding does not facilitate correct production of targetconsonants then it is likely that an alternative articulatory pattern has becomephonologically established ie particular realizations for one or more targets areconsistently distributed in the phonological system These realizations may haveevolved because of initial diYculty producing articulatory targets and subsequentlystabilized within the phonological system Grundy and Harding (1995) refer to thisphenomenon as an lsquoarticulatory disorder with phonological consequencesrsquo
Therapy
Where obvious structural defects or diagnosed dysfunction exists clinicians fre-quently defer therapeutic intervention until surgery has been undertaken Theexpectation would be that normal structure and function is essential for normalspeech However pre-operative therapy may facilitate oral consonant productionwhich may serve to reduce hypernasal resonance Hence therapy prior to surgerymay avoid unnecessary surgery or reduce the extent of surgery required All activeprocesses are likely to require therapy
Principled selection of targets for therapy
Speech patterns frequently evidence a mixture of apparently passive and activeprocesses which complicates decisions about target selection Target selection can
A Harding and P Grunwell348
be based on assessment of which consonant targets can be most easily elicted inisolation (stimulability) This may lead to a sequence of target selection which isopposite to the sequence of consonant acquisition in normal development Forexample where reduced intra-oral pressure is present in a passive pattern [T] maybe easier to elicit in imitation than more nely grooved [s] or [S] Therapy maytarget [T] followed by [S ] and nally [s] As in non-cleft phonological therapywhere a class of consonants is aVected by the cleft then it is helpful to target theentire class The following decision-making process can be applied for both activeand passive processes
Decision making procedure for target selection
(1) Voiced versus voiceless targets(2) Front versus back placements(3) Syllable initial versus syllable nal targets(4) Plosives versus fricative targets
Voiceless plosives and fricatives are produced with an open glottis whichfacilitates topping up of air ow from the lungs hence voiceless plosive and fricativetargets are frequently more successful than voiced counterparts (Isshiki and Ringel1964) Front targets usually cause more diYculty than back particularly where analveolar defect or stula exists Contrary to normal development back targets maybe targeted before front Word- nal targets generally require less oral air pressurethan word initial targets and similarly fricatives may be more easily elicited thanplosives Fricatives do require a greater volume of air than plosives (Fletcher 1985)but in the presence of nasal escape weak fricative production appears to be morereadily achieved than weak plosive production Since nal fricatives would normallybe acquired in advance of word-initial fricatives (Ferguson 1978) targeting word- nal fricatives is frequently a productive starting point for therapy
Principles of therapy for passive processes
(1) Use of soft attack similar to gentle whisper for all target models ensuresminimal articulatory eVort (Harding and Grunwell 1993) and requires min-imal intra-oral air pressure It may be appropriate to gradually increase thearticulatory attack when the articulatory posture and evidence of intendedoral air ow have been established
(2) Slightly stretched duration of segment transitions in models of consonantto vowel (CndashV) or vowel to consonant (VndashC) facilitates review of motorplanning and extends the available time for execution of the new motorprogrammer whilst maintaining control of the oral airstream
(3) Noseholding can be used to provide exclusively oral air ow Gradual releaseof the nostrils during production of sustained [VVVVVf ] or [hhhhh ] allowsthe child to attempt to sustain an oral consonant despite increasing nasalemission This maximizes the use of available oral air ow Procedures forusing noseholding are described in some detail by Golding-Kushner (1995)
Principles of therapy for active processes
This is more like phonological therapy and can follow Grunwellrsquos (1991) processesfor phonological change and principled decision-making (Grunwell 1992) Some
Active versus passive cleft-type speech characteristics 349
examples are given here by way of illustration of ways to eVect the rst twoprocesses of change which may need to be approached diVerently in cleft palateversus non-cleft speech disorders DiVerent approaches may also be appropriate formodifying active versus passive cleft-type processes
Innovation production of new targets Some useful principles
(1) Introduction of new lsquonon-speech likersquo targets in sound play using a conson-ant sound segment model such as [ph ] note not a syllable like [p] whichis the type of pronunciation used when target sounds are presented as lettersfor reading Target [s] might be introduced as a lsquoTrain Slowing Down Noisersquo[ts ts ts tssssssss]
(2) lsquoNew consonantsrsquo can later be modelled and elicited in soft productions ofsyllable structure [tssssndashi] [ indashtssss] which can subsequently be identi ed assimilar to words lsquosearsquo and lsquoeatsrsquo
(3) lsquoDeferring responsibilityrsquo transfers responsibility or lsquoblamersquo for errors fromthe child and attributes it to the articulators eg lsquoyour tongue is havingtrouble with hellip rsquo lsquoLetrsquos show your tongue how to hellip rsquo
(4) New targets can be modelled repeatedly and recorded on audio or videotape which can be listened to at home
(5) Targeting classes of consonants (eg alveolars t d s n l voiceless fricativesf s S perhaps with aVricate T avoids phonological confusion whichmight occur if production ofsis achieved whilst other alveolar targetsremain backed The risk is that s might not integrate into the phonologicalsystem unless all backed alveolar consonants are destabilized
(6) Increased eye contact during auditory and production work can be invaluablein holding visual and auditory attention and ensures that visual informationabout the sound has been processed This is easily achieved by the clinicianlifting any focus of the childrsquos attention close to hisher mouth at theprecise moment when the target is modelled
Stimulation of non-speech related sounds such as a lsquoTrain Slowing DownNoisersquo [ts ts tsss] con rms that target [s] is physically achievable whether or not[ssss] can be imitated Some children continue to access [s] through the lsquoTrainSlowing Down Noisersquo throughout therapy until it is occurring spontaneouslywithout conscious planning This can be an eVective means of underminingestablished motor programmers (Hewlett 1990) for active cleft-type processes
Destabilizing active processes
As it is likely that children will be unaware of each occurrence of their alternativearticulatory pattern for speci c consonant errors it is preferrable to destabilizeactive processes with minimal conscious eVort by the child As children becomeaware of their mismatches they frequently add the newly acquired target realizationto their existing production eg target word tu childrsquos old realization [ku] childrsquoscorrected realization [t-ku] Destabilization can be achieved with minimal consciouseVort through input therapy techniques such as auditory bombardment (Lancasterand Pope 1989) auditory decision-making such as lsquowhich bear says this wordproperlyrsquo Red Bear says lsquotworsquo or Blue Bear says lsquocoorsquo This type of strategy oftenprecipitates attention to the target consonant with possible lsquoreplayrsquo and lsquoreviewrsquo of
A Harding and P Grunwell350
their own production Frequent stimulation of cognitive alertness to the targetconsonant can develop awareness without confronting the child with errors orrisking hisher failure The child is then free to attempt to repair hisher ownrealization to continue to re ect and to silently rehearse the adult realizationTraditional articulation therapy is thus combined with development of metaphonol-ogical skills ie the ability to re ect upon onersquos own speech production The resultshould be that new target realizations will be more phonologically stable thanexclusively production-based articulation therapy might have facilitated
Stabilizationgeneralization
Procedures to ensure stabilization and generalization of new target consonantswould be as described by Grunwell (1992) Success may be constrained by theconsiderable articulatory eVort sometimes required to maintain pressure consonantproduction in spontaneous speech (Harding and Grunwell 1993)
Conclusions
In speech assessment it is helpful to distinguish between errors which are cleft-type and non-cleft type and those which are part of active versus passive processesThe active and passive processes have been de ned and their phonological implica-tions discussed Focus on active and passive processes has facilitated focus on thephonological consequences of cleft palate on speech development In the futureawareness of the likely eVect of a cleft palate on normal phonological developmentcould avoid extended periods of unsuccessful clinical intervention Furthermoresensitivity to the relationship between phonological processes and structural con-straints should facilitate theoretically based management decisions Incidences suchas the case of CP in which nasal realizations were thought to indicate VPI but weresubsequently unaVected by surgery might be avoided if phonological analysiscontributes to management decisions
Surgery did improve hypernasal resonance and eliminated passive processes buthad little eVect on active processes Active processes in younger subjects werethought to require therapeutic intervention but in the longer term the oldersubjects showed few cleft-type processes Whilst it is possible that active cleft-typeprocesses may resolve with increasing age the implication for the future is thatactive cleft-type processes should be treated with skilled therapeutic interventionnot surgery Therapy which addresses the phonological consequences of cleft palateon speech development by combining metaphonologicalphonologicalarticulatoryapproaches is likely to be successful
References
Albery E 1991 Consonant articulation in the diVerent types of cleft lip and palate UnpublishedMPhil thesis Leicester Polytechnic
Albery E and Grunwell P 1993 Consonant articulation in diVerent types of cleft palate InP Grunwell (Ed) Analysing Cleft Palate Speech (London Whurr)
Ferguson C A 1978 Fricatives in child language acquisition In V Honsa and M Hardmann-Battista (Eds) Papers on Linguistics and Child Language (Mouton The Hague)
Fletcher S G 1985 Speech production and oral motor skill in an adult with an unrepaired palatalcleft Journal of Speech and Hearing Disorders 50 254ndash261
Active versus passive cleft-type speech characteristics 351
Golding-Kushner K J 1995 Treatment of articulation and resonancne disorders associated withcleft palate management and VPI In R Shprintzen (Ed) Cleft Palate Speech Management AMultidisciplinary Approach (St Louis Mosby)
Grundy K and Harding A 1995 Developmental speech disorders In K Grundy (Ed) Linguisticsin Clinical Practice (2nd edition) (London Whurr)
Grunwell P 1985 Phonological Assessment of Child Speech (Windsor NFER-Nelson)Grunwell P 1987a Clinical Phonology (2nd edition) (London Croom Helm)Grunwell P 1987b PACS Pictures Language Elicitation Materials (Windsor NFER-Nelson)Grunwell P 1991 Processes of phonological change in developmental speech disorders Clinical
Linguistics and Phonetics 6 101ndash122Grunwell P 1992 Principled decision making in the remediation of children with phonological
disorders In P Fletcher and D Hall (Eds) Specic Speech and Language Disorders in Children(London Whurr)
Grunwell P and Harding A 1995 PACSTOYS A Screening Assessment of Phonological Development(Windsor NFER-Nelson)
Grunwell P and Harding A 1996 A note on describing types of nasality Clinical Linguistics andPhonetics 10 157ndash161
Harding A 1993 An Investigation into the Relationship Between Timing of Cleft Palate Repairand Speech Development Unpublished PhD thesis
Harding A and Grunwell P 1993 The relationship between speech and timing of hard palaterepair In P Grunwell (Ed) Analysisng Cleft Palate Speech (London Whurr)
Harding A and Grunwell P 1996 Characteristics of cleft palate speech European Journal ofDisorders of Communication 31 331ndash358
Henningsson G and Isberg A M 1986 Velopharyngeal movement patterns in patients alternatingbetween oral and glottal articulation A clinical and cineradiographicical study Cleft Palate Journal23 1ndash9
Hewlett N 1990 Processes of development and production In P Grunwell (Ed) DevelopmentalSpeech Disorders (Edinburgh Churchill Livingstone)
Hotz M M Gnoinski W M Nussbaumer H and Kistler E 1978 Early orthopaedics in CLPcases guidelines for surgery Cleft Palate Journal 15 405ndash411
Hutters B and Brondsted K 1987 Strategies in cleft palate with special reference to DanishCleft Palate Journal 24 127ndash136
Isshiki N and Ringel R 1964 Airow during the production of selected consonants Journal ofSpeech and Hearing Research 7 233ndash244
Kummer A W Curtis C Wiggs M Lee L and Strife J L 1992 Comparison of velopharyngealgap size in patients with hypernasality hypernasality with nasal emission and nasal emissionor nasal turbulence (rustle) as the primary speech characteristic Cleft-palate-Craniofacial Journal29 152ndash156
Lancaster G and Pope L 1989 Working with Childrenrsquos Phonology (Oxford Winslow)Morley M E 1970 Cleft Palate and Speech (7th edition) (Edinburgh Churchill Livingstone)Russell V J 1991 Speech Development in Children with Cleft Lip and Palate Unpublished PhD
thesis Leicester PolytechnicRussell V J and Grunwell P 1993 Speech development in children with cleft lip and palate In
P Grunwell (Ed) Analysing Cleft Palate Speech (London Whurr)Sell D A and Grunwell P 1990 Speech results following late palatal surgery in previously
unoperated Sri Lankan adolescents with cleft palate Cleft Palate Journal 27 162ndash168Sell D Harding A and Grunwell P 1994 GOSSPASS A screening assessment of cleft palate
speech European Journal of Disorders of Communication 29 1ndash15Sell D Harding A and Grunwell P 1998 GOSSPASSrsquo98 An assessment for speech disorders
associated with cleft palate andor velopharyngeal dysfunction International Journal of Languageamp Communication Disorders ( in press)
Shorter E 1995 A spectographic analyis of child homophones Unpublished honours project DeMontfort University Leicester
Stenglehoffen J 1989 Nature and causes of communication diYculties In J Stengelhofen (Ed)Cleft Palate Nature and Remediation of Communication Problems (Edinburgh Churchill Livingstone)
Trost J E 1981 Articulatory additions to the classical description of the speech of persons withcleft palate Cleft Palate Journal 18
Trost-Cardamone J E 1990 The development of speech assessing cleft palate misarticulationsIn D A Kernahan and S N Rosenstein (Eds) Cleft Lip and Palate A System of Management(Baltimore Williams amp Wilkins)
A Harding and P Grunwell352
Appendix Active passive analysis of cleft palate speech

A Harding and P Grunwell340
Table 2 Cleft-type processes in UCLP subjects at age 46 (study 2)
1-stage surgery 2-stage surgery
SE TB CK MS NC TS ZG CP
Passive cleft-type processespredominantly sonorant artic m
weak articulation m m m
voiceless h for plosives m m m
nasal release of plosives m m m
nasal emission with consonants m m
passive nasal fricative m m
Active cleft-type processesnasal fricativepharyngeal glottal articulation m m m
backing to uvular m
backing to velar m m
lateral palatal fricatives m m m m m
double articulation m m m m m m
gliding fricative m
Table 3 Cleft-type processes at age 90
2-stage surgery 2-stage surgery1-stage surgery completed at 4 yrs completed at 8 yrs
DAf SBf RL NR JD AR LJ RP MB
Passive cleft-type processespredominantly sonorant articweak articulation m
voiceless h for plosives m m
nasal release of plosives m m
nasal emission with consonants m m m m
passive nasal fricatives m m
Active cleft-type processesnasal fricatives m m
pharyngeal glottal articulation m m
backing to uvular m m
backing to velar m m m m m m m
lateral palatal fricatives m m m m m m m
double articulation m m m m m
gliding fricative m
f=subject had a stula
both active and passive strategies whereas later samples (ages 90ndash130) rarelyevidenced passive processes
At age 46 four out of ve BCLP subjects used active non-oral pharyngeal andglottal processes and oral velar and uvular fricatives irrespective of surgical status(see table 1) All had some anterior palatal defect which might have reduced theirpotential to achieve intra-oral pressure
By comparison two out of three partially repaired 2-stage UCLP subjects at age46 (table 2) showed evidence of passive processes This suggested that their
Active versus passive cleft-type speech characteristics 341
Tab
le4
Spee
chin
rela
tion
tosu
rgic
altim
ing
atag
e13
0
2-st
age
surg
ery
2-st
age
surg
ery
1-st
age
surg
ery
subj
ects
com
plet
edat
4yr
sco
mpl
eted
at8
yrs
1-A
1-B
1-C
1-D
1-E
1-F
24-
G2
4-H
24-
J2
8-K
28-
L2
8-M
Pass
ive
clef
t-ty
pepr
oces
ses
pred
omin
antly
sono
rant
artic
wea
kar
ticul
atio
nm
voic
eles
sh
fo
rpl
osiv
esna
sal
rele
ase
ofpl
osiv
esna
sal
emis
sion
with
cons
onan
tsm
pass
ive
nasa
lfr
icat
ives
Act
ive
clef
t-ty
pepr
oces
ses
nasa
lfr
icat
ives
phar
ynge
alg
lott
alar
ticul
atio
nba
ckin
gto
uvul
arba
ckin
gto
vela
rm
m
late
ral
pala
tal
fric
ativ
esm
mm
doub
lear
ticul
atio
ngl
idin
gfr
icat
ive
1=1-
stag
esu
rger
ysu
bjec
ts
24=
2-st
age
surg
ery
hard
pala
tere
pair
edat
abou
t4
yrs
28=
2-st
age
surg
ery
with
hard
pala
tere
pair
edat
abou
t8
yrs
A Harding and P Grunwell342
unrepaired hard palates had in fact restricted their phonetic repertoire imposing aneed for individual adaptability The additional active processes employed by thesesubjects were presumably a response to the restrictions imposed by their oro-nasalstructure and velopharyngeal function at the time of consonant acquisition Asshown in table 2 the most common active cleft-type processes persisting at age46 with a residual cleft of the hard palate were backing double articulation andlateralpalatal articulation Two 1-stage surgery subjects whose entire palates hadbeen repaired at ages 09 and 010 did not use any cleft-type processes at age 46
By age 90 (table 3) a much-diminished number of cleft type processes wasevident except in subjects with sizeable anterior stulae who had received littlespeech and language therapy A similarity was noted between the speech patternsof 1-stage surgery subjects with stulae (DA and SB) at age 90 (table 3) and theyounger BCLP subjects at age 46 (table 1) who also had anterior palatal defectsThey included non-oral realizations of t d s k g occasional nasal fricatives andpharyngealglottal articulations Fistulae had apparently continued to in uencearticulation and phonological development in these subjects
Finally at age 130 (table 4) the diVerences between 1-stage and 2-stage surgerysubjects had diminished leaving only one 2-stage subject with occasional backingand four subjects with slight palatal and lateral release of fricative consonants Onlytwo of the 1-stage surgery subjects were using minor distortions of grooved fricativeproduction
Whilst there were apparent trends in speech production relating to surgicaltiming and oral structure it is noted that there were exceptions to each tentativegeneralization Subjects with marked structural imperfections occasionally producedrealizations of which they would not have been thought capable and subjects withno visible imperfections produced inexplicably distorted speech patterns It istherefore concluded that whilst there is homogeneity in the range of processesproduced by this population assumptions cannot be made about speech based onsurgical timing or type of cleft Tentative predictions based on detailed assessmentmay be clinically very useful
EVects of surgery on speech
Activepassive processes have identi ed those cleft-type characteristics thought tobe associated with a physical inability to produce pressure consonants The followinganalysis of speech changes after surgical intervention at diVerent ages identi es thechanges eVected by surgery when intra-oral pressure could be more readily achieved
Two children were rst recorded prior to the rst stage of a 2-stage procedureTheir lips were repaired at approximately 6 months of age and soft palate repairwas carried out at ages 18 and 19 respectively Their hard palates were leftunrepaired to facilitate unrestricted growth of the mid-face (Hotz et al 1978) Pre-and post-operative consonant-like sounds present in the recorded speech samplesare listed in table 5 Interestingly prior to soft palate repair both these childrenproduced some oral consonants Subject B was producing pressure consonants [kg] in his babble prior to soft palate repair Considering that he had an unrepairedbilateral cleft palate at this point it was surprising that he had any oral consonantsPost-operatively at 20 years he used [b bkm t d g gkb] which indicated that surgeryto repair the soft palate had facilitated an increased range of oral pressure consonantsSubject D was producing [p b k g] pre-operatively Post-operatively following soft
Active versus passive cleft-type speech characteristics 343
Tab
le5
EV
ects
ofso
ftp
alat
ere
pair
atag
e1
6on
BC
LP
subj
ects
h
ard
pal
ate
rem
ain
sun
repa
ired
2-st
age
subj
ects
Surg
ery
Pre
-ope
rati
vesp
eech
patt
ern
atag
e1
6Po
st-o
pera
tive
chan
ges
insp
eech
atag
e2
0
Stud
y1
BSo
ftpa
late
repa
irat
16
Adu
ltta
rget
sk
gA
t2
0[b
b kmg kb
td
g]D
Soft
pala
tere
pair
17
Adu
ltta
rget
sp
bk
gA
t2
0[p
bd
b kdk
g]
Tab
le6
EV
ects
ofha
rdpa
late
rep
air
atag
e6
6an
d
stu
lare
pair
atag
e10
0
Subj
ect
Surg
ery
Pre
-ope
rati
vesp
eech
patt
ern
Post
-ope
rati
vech
ange
sin
spee
ch
MS
Har
dpa
late
repa
ir6
6Pa
ssiv
epr
oces
s7
6E
limin
ated
pass
ive
proc
ess
Var
iabl
ena
sal
rele
ase
ofco
nson
ants
Hyp
onas
alna
sals
JFH
ard
pala
tere
pair
(uns
ucce
ssfu
l)6
6Se
vera
lac
tive
and
pass
ive
proc
esse
s7
6A
ctiv
epr
oces
ses
rem
aine
dPa
ssiv
epr
oces
ses
elim
inat
ed
DA
Fis
tula
repa
ir10
0A
ctiv
epr
oces
ses
110
Elim
inat
ion
ofph
aryn
geal
glo
ttal
Var
iabi
lity+
+an
dna
sal
arti
cula
tion
Art
icul
ator
yva
riab
ility
++
Act
ive
CT
Rs
proc
esse
spe
rsis
t
A Harding and P Grunwell344
palate repair but with a residual cleft in the hard palate his range of consonantsincluded [d] which was particularly surprising since the hard palate remainedunrepaired Whilst it is unlikely that toddlers of 18 months could be consciouslytrying to compensate for articulatory inadequacy in producing velar plosives inbabble prior to soft palate repair and an alveolar plosive prior to hard palate repairboth these subjects showed evidence of actively pursuing their articulatory potential
Table 6 summarizes changes following surgery to repair the hard palate in moremature speech patterns These subjects who were aged 66 and 100 pre-operativelyhad learned to speak with residual clefts and were apparently unaware of theconsonant productions that failed to match normal production
Subject MS used only passive processes in his speech pattern He realized someconsonants nasally such that lsquoballrsquo was [mO~] and lsquosockrsquo was [(sk)n
deg Aacute~ k] Looking atpost-operative changes at age 76 his consonant production was normal but hisresonance had become hyponasal Pre-operatively at age 66 Subject JF was usingseveral active and passive processes The active processes were unaVected by surgerybut passive processes were eliminated
Fistula repair was carried out at age 100 on Subject DA who had many activeprocesses and very variable articulation pre-operatively Post-operatively at age110 he was not using non-oral pharyngeal and glottal active processes or nasalrealizations but many oral cleft-type realizations remained
As shown in table 7 hard palate re-repair and pharyngoplasty was carried outon two subjects whose hard palate repairs had been unsuccessful at approximately4 years Subject NC assessed pre-operatively at age 56 was using predominantlypassive processes in her speech She was also using [ j] for fricatives s S whichwas thought to be an active process At age 60 following hard palate re-repair andpharyngoplasty all cleft-type processes had been eliminated without post-operativespeech therapy Since [ j] for s apparently resolved spontaneously followingsurgery it can be assumed that this was a passive process in this speech sample
Subject CP who underwent this procedure presented pre-operatively at age 46with both passive and active processes but his nasal resonance was not consistentlyhypernasal In addition to his cleft-related speech disorder this subject had additionaldevelopmental speech diYculties which were identi ed as being unrelated to thecleft Post-operatively at age 56 little had changedmdashnotably the passive processnasal [m] for b was retained His nasal resonance had become hyponasal andthere was no apparent bene t from surgical intervention The realization of b as[m] had become phonologically stable and surgery alone had not destabilized thephonological system This realization may have been a passive product of VPI inearly speech acquisition which had subsequently become part of a phonologicaldisorder Post-operatively CPrsquos phonetic repertoire did increase but the phonologicaldistribution was variable Plosive targets were still realized as nasals in spontaneousspeech at the nal speech recording at age 76 This was not as an inevitableconsequence of VPI but a result of an inability to destabilize the phonologicalprocess determining that voiced plosives would be realized as nasals This resultfollowing surgery highlights the importance of identifying phonological learningproblems and distinguishing them from structural constraints on articulationIn CPrsquos case pre-operative exploration of the eVect of nares occlusion duringspeech might have indicated that structural change would not improve consonantproduction spontaneously
A general observation was that consonant realizations did not move rapidly
Active versus passive cleft-type speech characteristics 345
Tab
le7
EV
ects
ofha
rdpa
late
re-r
epai
ran
dp
hary
ngo
pla
sty
Subj
ect
Surg
ery
Pre
-ope
rati
vesp
eech
patt
ern
Post
-ope
rativ
ech
ange
sin
spee
ch
Stud
y2
NC
Har
dpa
late
re-r
epai
ran
d5
6Pa
ssiv
ecl
eft-
type
proc
esse
s6
0A
llcl
eft-
type
phar
yngo
plas
ty5
10[
j]
for
fric
ativ
espr
oces
ses
elim
inat
ed[
h]
for
plos
ives
SIW
IV
aria
ble
arti
cula
rypr
ecis
ion
CP
Har
dpa
late
repa
iran
d4
6Pa
ssiv
ean
dac
tive
proc
esse
s5
6Pa
ssiv
epr
oces
sph
aryn
gopl
asty
50
Pho
nolo
gica
lco
nfus
ion
[m]
for
[b
]re
tain
edH
ypon
asal
nasa
lsPe
rsis
ting
phon
olog
ical
conf
usio
ns
A Harding and P Grunwell346
from incorrect to correct but progressed incrementally towards normal realizationsas described by Morley (1970) Where an early realization of target s might beglottal [h] a gradual pattern of change showed subsequent realizations to bepharyngeal [Eacute] then uvular [X] then velar [x] and eventually palatal [c] or lateral [Euml]It was interesting to note that speech patterns continued to change as late as90ndash110 years with the result that diVerences related to surgical timing and cleft-type gradually disappeared Persisting stulae were thought to account for the mostmarked cleft type processes at age 90
Implications for surgical management
This analysis of speech changes following surgery suggests some implications forsurgical management which are compatible with Sell and Grunwellrsquos (1990) ndingsin the Sri Lankan study
Surgery can change passive speech processes but it is also possible that speechtherapy may be able to change passive patterns Surgery alone is unlikely to modifyactive cleft-type processes whereas speech therapy should be able to modify activeprocesses Indications from these case studies is that where speech is the primaryproblem speech assessment should distinguish between active and passive processesin order to evaluate the necessity for full investigations and to plan therapeuticintervention Where past speech therapy has not been successful it cannot beassumed that surgical intervention will facilitate further speech progress A furthercourse of speech therapy which is sensitive to active versus passive processes todevelopmental phonological in uences on cleft-type speech development and toarticulatory diYculties in diVerent speech contexts might facilitate optimal progressWhere structural imperfection exists it is quite possible for single-word productionto be more precise than target realizations in spontaneous speech This may not bea failure of phonological generalization (Grunwell 1992) but the result of diYcultysustaining the necessary lsquoarticulatory eVort rsquo (Harding and Grunwell 1993) resultingin articulatory imprecision Deteriorating articulatory accuracy should not be over-looked in interpretation of speech results
An analytical protocol
As a result of analysing the speech data and identifying the active and passiveprocesses a protocol has been developed which records examples of each cleft-typeprocess over a series of assessments It demonstrates the progression of individualprocesses towards an adult target (see the Appendix) At each assessment onecolumn is used to indicate nasal resonance nasal emission and nasal turbulenceratings and cleft-type processes Changes in the nature of error realizations mightshow progress towards target consonants Hence whilst the total correct scoremight not have increased increments of change can be observed This observationof patterns of change may function as an adjunct to GOSSPASSrsquo98 (Sell et al 1998)giving access to a greater depth of both quantitative and qualitative data aboutconsonant production in relation to resonance nasal emission nasal turbulenceoral structure and cleft-type
Active versus passive cleft-type speech characteristics 347
Diagnostic implications
Passive versus active nasal fricatives
The important management consideration related to this distinction is that an activenasal fricative is an established phonological process which is unlikely to be directlyaVected by surgery alone Therapy would be necessary to destabilize nasal realizationsof oral consonants In contrast passive nasal fricatives may be eliminated by surgeryOf particular relevance is diVerential diagnosis between passive and active nasalfricatives in surgical and therapeutic management When hypernasality co-occurswith nasal air ow during consonant production which can be redirected by nose-holding passive nasal fricatives are diagnosed These would be transcribed as [(sk)n
deg]
passive alveolar nasal fricatives [(Wk)mdeg
] bilabial nasal fricatives or [(fk)Iacutedeg ] labiodentalnasal fricatives Full VPI investigations would be recommended to diagnose thenature of the structural or functional de ciency and distinguish between velopharyn-geal incompetence and velopharyngeal mislearning
It is highly likely that plosive targets would be aVected by reduced intra-oral airpressure such that plosives would either be realized by nasal counterparts eg bd[ [m n] or [b d] may be nasalized and weak Voiceless plosives may be eitheraccompanied by nasal emission [p t k] or realized as glottal fricative [h]
Production of the target sentence lsquoI saw Sam sitting on a busrsquo might be
[aI (sk)ndeg O~ (sk)n
degaelig~m (sk)n
deg IhIn Aacute~n mouml~(sk)ndeg] passive processes and
[aI xO xaeligm xIkIIcirc AacuteIcirc goumlx] active processes
Contribution to surgical management decisions
Passiveactive interpretation of clinical assessments might facilitate surgical manage-ment decisions If noseholding does not facilitate correct production of targetconsonants then it is likely that an alternative articulatory pattern has becomephonologically established ie particular realizations for one or more targets areconsistently distributed in the phonological system These realizations may haveevolved because of initial diYculty producing articulatory targets and subsequentlystabilized within the phonological system Grundy and Harding (1995) refer to thisphenomenon as an lsquoarticulatory disorder with phonological consequencesrsquo
Therapy
Where obvious structural defects or diagnosed dysfunction exists clinicians fre-quently defer therapeutic intervention until surgery has been undertaken Theexpectation would be that normal structure and function is essential for normalspeech However pre-operative therapy may facilitate oral consonant productionwhich may serve to reduce hypernasal resonance Hence therapy prior to surgerymay avoid unnecessary surgery or reduce the extent of surgery required All activeprocesses are likely to require therapy
Principled selection of targets for therapy
Speech patterns frequently evidence a mixture of apparently passive and activeprocesses which complicates decisions about target selection Target selection can
A Harding and P Grunwell348
be based on assessment of which consonant targets can be most easily elicted inisolation (stimulability) This may lead to a sequence of target selection which isopposite to the sequence of consonant acquisition in normal development Forexample where reduced intra-oral pressure is present in a passive pattern [T] maybe easier to elicit in imitation than more nely grooved [s] or [S] Therapy maytarget [T] followed by [S ] and nally [s] As in non-cleft phonological therapywhere a class of consonants is aVected by the cleft then it is helpful to target theentire class The following decision-making process can be applied for both activeand passive processes
Decision making procedure for target selection
(1) Voiced versus voiceless targets(2) Front versus back placements(3) Syllable initial versus syllable nal targets(4) Plosives versus fricative targets
Voiceless plosives and fricatives are produced with an open glottis whichfacilitates topping up of air ow from the lungs hence voiceless plosive and fricativetargets are frequently more successful than voiced counterparts (Isshiki and Ringel1964) Front targets usually cause more diYculty than back particularly where analveolar defect or stula exists Contrary to normal development back targets maybe targeted before front Word- nal targets generally require less oral air pressurethan word initial targets and similarly fricatives may be more easily elicited thanplosives Fricatives do require a greater volume of air than plosives (Fletcher 1985)but in the presence of nasal escape weak fricative production appears to be morereadily achieved than weak plosive production Since nal fricatives would normallybe acquired in advance of word-initial fricatives (Ferguson 1978) targeting word- nal fricatives is frequently a productive starting point for therapy
Principles of therapy for passive processes
(1) Use of soft attack similar to gentle whisper for all target models ensuresminimal articulatory eVort (Harding and Grunwell 1993) and requires min-imal intra-oral air pressure It may be appropriate to gradually increase thearticulatory attack when the articulatory posture and evidence of intendedoral air ow have been established
(2) Slightly stretched duration of segment transitions in models of consonantto vowel (CndashV) or vowel to consonant (VndashC) facilitates review of motorplanning and extends the available time for execution of the new motorprogrammer whilst maintaining control of the oral airstream
(3) Noseholding can be used to provide exclusively oral air ow Gradual releaseof the nostrils during production of sustained [VVVVVf ] or [hhhhh ] allowsthe child to attempt to sustain an oral consonant despite increasing nasalemission This maximizes the use of available oral air ow Procedures forusing noseholding are described in some detail by Golding-Kushner (1995)
Principles of therapy for active processes
This is more like phonological therapy and can follow Grunwellrsquos (1991) processesfor phonological change and principled decision-making (Grunwell 1992) Some
Active versus passive cleft-type speech characteristics 349
examples are given here by way of illustration of ways to eVect the rst twoprocesses of change which may need to be approached diVerently in cleft palateversus non-cleft speech disorders DiVerent approaches may also be appropriate formodifying active versus passive cleft-type processes
Innovation production of new targets Some useful principles
(1) Introduction of new lsquonon-speech likersquo targets in sound play using a conson-ant sound segment model such as [ph ] note not a syllable like [p] whichis the type of pronunciation used when target sounds are presented as lettersfor reading Target [s] might be introduced as a lsquoTrain Slowing Down Noisersquo[ts ts ts tssssssss]
(2) lsquoNew consonantsrsquo can later be modelled and elicited in soft productions ofsyllable structure [tssssndashi] [ indashtssss] which can subsequently be identi ed assimilar to words lsquosearsquo and lsquoeatsrsquo
(3) lsquoDeferring responsibilityrsquo transfers responsibility or lsquoblamersquo for errors fromthe child and attributes it to the articulators eg lsquoyour tongue is havingtrouble with hellip rsquo lsquoLetrsquos show your tongue how to hellip rsquo
(4) New targets can be modelled repeatedly and recorded on audio or videotape which can be listened to at home
(5) Targeting classes of consonants (eg alveolars t d s n l voiceless fricativesf s S perhaps with aVricate T avoids phonological confusion whichmight occur if production ofsis achieved whilst other alveolar targetsremain backed The risk is that s might not integrate into the phonologicalsystem unless all backed alveolar consonants are destabilized
(6) Increased eye contact during auditory and production work can be invaluablein holding visual and auditory attention and ensures that visual informationabout the sound has been processed This is easily achieved by the clinicianlifting any focus of the childrsquos attention close to hisher mouth at theprecise moment when the target is modelled
Stimulation of non-speech related sounds such as a lsquoTrain Slowing DownNoisersquo [ts ts tsss] con rms that target [s] is physically achievable whether or not[ssss] can be imitated Some children continue to access [s] through the lsquoTrainSlowing Down Noisersquo throughout therapy until it is occurring spontaneouslywithout conscious planning This can be an eVective means of underminingestablished motor programmers (Hewlett 1990) for active cleft-type processes
Destabilizing active processes
As it is likely that children will be unaware of each occurrence of their alternativearticulatory pattern for speci c consonant errors it is preferrable to destabilizeactive processes with minimal conscious eVort by the child As children becomeaware of their mismatches they frequently add the newly acquired target realizationto their existing production eg target word tu childrsquos old realization [ku] childrsquoscorrected realization [t-ku] Destabilization can be achieved with minimal consciouseVort through input therapy techniques such as auditory bombardment (Lancasterand Pope 1989) auditory decision-making such as lsquowhich bear says this wordproperlyrsquo Red Bear says lsquotworsquo or Blue Bear says lsquocoorsquo This type of strategy oftenprecipitates attention to the target consonant with possible lsquoreplayrsquo and lsquoreviewrsquo of
A Harding and P Grunwell350
their own production Frequent stimulation of cognitive alertness to the targetconsonant can develop awareness without confronting the child with errors orrisking hisher failure The child is then free to attempt to repair hisher ownrealization to continue to re ect and to silently rehearse the adult realizationTraditional articulation therapy is thus combined with development of metaphonol-ogical skills ie the ability to re ect upon onersquos own speech production The resultshould be that new target realizations will be more phonologically stable thanexclusively production-based articulation therapy might have facilitated
Stabilizationgeneralization
Procedures to ensure stabilization and generalization of new target consonantswould be as described by Grunwell (1992) Success may be constrained by theconsiderable articulatory eVort sometimes required to maintain pressure consonantproduction in spontaneous speech (Harding and Grunwell 1993)
Conclusions
In speech assessment it is helpful to distinguish between errors which are cleft-type and non-cleft type and those which are part of active versus passive processesThe active and passive processes have been de ned and their phonological implica-tions discussed Focus on active and passive processes has facilitated focus on thephonological consequences of cleft palate on speech development In the futureawareness of the likely eVect of a cleft palate on normal phonological developmentcould avoid extended periods of unsuccessful clinical intervention Furthermoresensitivity to the relationship between phonological processes and structural con-straints should facilitate theoretically based management decisions Incidences suchas the case of CP in which nasal realizations were thought to indicate VPI but weresubsequently unaVected by surgery might be avoided if phonological analysiscontributes to management decisions
Surgery did improve hypernasal resonance and eliminated passive processes buthad little eVect on active processes Active processes in younger subjects werethought to require therapeutic intervention but in the longer term the oldersubjects showed few cleft-type processes Whilst it is possible that active cleft-typeprocesses may resolve with increasing age the implication for the future is thatactive cleft-type processes should be treated with skilled therapeutic interventionnot surgery Therapy which addresses the phonological consequences of cleft palateon speech development by combining metaphonologicalphonologicalarticulatoryapproaches is likely to be successful
References
Albery E 1991 Consonant articulation in the diVerent types of cleft lip and palate UnpublishedMPhil thesis Leicester Polytechnic
Albery E and Grunwell P 1993 Consonant articulation in diVerent types of cleft palate InP Grunwell (Ed) Analysing Cleft Palate Speech (London Whurr)
Ferguson C A 1978 Fricatives in child language acquisition In V Honsa and M Hardmann-Battista (Eds) Papers on Linguistics and Child Language (Mouton The Hague)
Fletcher S G 1985 Speech production and oral motor skill in an adult with an unrepaired palatalcleft Journal of Speech and Hearing Disorders 50 254ndash261
Active versus passive cleft-type speech characteristics 351
Golding-Kushner K J 1995 Treatment of articulation and resonancne disorders associated withcleft palate management and VPI In R Shprintzen (Ed) Cleft Palate Speech Management AMultidisciplinary Approach (St Louis Mosby)
Grundy K and Harding A 1995 Developmental speech disorders In K Grundy (Ed) Linguisticsin Clinical Practice (2nd edition) (London Whurr)
Grunwell P 1985 Phonological Assessment of Child Speech (Windsor NFER-Nelson)Grunwell P 1987a Clinical Phonology (2nd edition) (London Croom Helm)Grunwell P 1987b PACS Pictures Language Elicitation Materials (Windsor NFER-Nelson)Grunwell P 1991 Processes of phonological change in developmental speech disorders Clinical
Linguistics and Phonetics 6 101ndash122Grunwell P 1992 Principled decision making in the remediation of children with phonological
disorders In P Fletcher and D Hall (Eds) Specic Speech and Language Disorders in Children(London Whurr)
Grunwell P and Harding A 1995 PACSTOYS A Screening Assessment of Phonological Development(Windsor NFER-Nelson)
Grunwell P and Harding A 1996 A note on describing types of nasality Clinical Linguistics andPhonetics 10 157ndash161
Harding A 1993 An Investigation into the Relationship Between Timing of Cleft Palate Repairand Speech Development Unpublished PhD thesis
Harding A and Grunwell P 1993 The relationship between speech and timing of hard palaterepair In P Grunwell (Ed) Analysisng Cleft Palate Speech (London Whurr)
Harding A and Grunwell P 1996 Characteristics of cleft palate speech European Journal ofDisorders of Communication 31 331ndash358
Henningsson G and Isberg A M 1986 Velopharyngeal movement patterns in patients alternatingbetween oral and glottal articulation A clinical and cineradiographicical study Cleft Palate Journal23 1ndash9
Hewlett N 1990 Processes of development and production In P Grunwell (Ed) DevelopmentalSpeech Disorders (Edinburgh Churchill Livingstone)
Hotz M M Gnoinski W M Nussbaumer H and Kistler E 1978 Early orthopaedics in CLPcases guidelines for surgery Cleft Palate Journal 15 405ndash411
Hutters B and Brondsted K 1987 Strategies in cleft palate with special reference to DanishCleft Palate Journal 24 127ndash136
Isshiki N and Ringel R 1964 Airow during the production of selected consonants Journal ofSpeech and Hearing Research 7 233ndash244
Kummer A W Curtis C Wiggs M Lee L and Strife J L 1992 Comparison of velopharyngealgap size in patients with hypernasality hypernasality with nasal emission and nasal emissionor nasal turbulence (rustle) as the primary speech characteristic Cleft-palate-Craniofacial Journal29 152ndash156
Lancaster G and Pope L 1989 Working with Childrenrsquos Phonology (Oxford Winslow)Morley M E 1970 Cleft Palate and Speech (7th edition) (Edinburgh Churchill Livingstone)Russell V J 1991 Speech Development in Children with Cleft Lip and Palate Unpublished PhD
thesis Leicester PolytechnicRussell V J and Grunwell P 1993 Speech development in children with cleft lip and palate In
P Grunwell (Ed) Analysing Cleft Palate Speech (London Whurr)Sell D A and Grunwell P 1990 Speech results following late palatal surgery in previously
unoperated Sri Lankan adolescents with cleft palate Cleft Palate Journal 27 162ndash168Sell D Harding A and Grunwell P 1994 GOSSPASS A screening assessment of cleft palate
speech European Journal of Disorders of Communication 29 1ndash15Sell D Harding A and Grunwell P 1998 GOSSPASSrsquo98 An assessment for speech disorders
associated with cleft palate andor velopharyngeal dysfunction International Journal of Languageamp Communication Disorders ( in press)
Shorter E 1995 A spectographic analyis of child homophones Unpublished honours project DeMontfort University Leicester
Stenglehoffen J 1989 Nature and causes of communication diYculties In J Stengelhofen (Ed)Cleft Palate Nature and Remediation of Communication Problems (Edinburgh Churchill Livingstone)
Trost J E 1981 Articulatory additions to the classical description of the speech of persons withcleft palate Cleft Palate Journal 18
Trost-Cardamone J E 1990 The development of speech assessing cleft palate misarticulationsIn D A Kernahan and S N Rosenstein (Eds) Cleft Lip and Palate A System of Management(Baltimore Williams amp Wilkins)
A Harding and P Grunwell352
Appendix Active passive analysis of cleft palate speech

Active versus passive cleft-type speech characteristics 341
Tab
le4
Spee
chin
rela
tion
tosu
rgic
altim
ing
atag
e13
0
2-st
age
surg
ery
2-st
age
surg
ery
1-st
age
surg
ery
subj
ects
com
plet
edat
4yr
sco
mpl
eted
at8
yrs
1-A
1-B
1-C
1-D
1-E
1-F
24-
G2
4-H
24-
J2
8-K
28-
L2
8-M
Pass
ive
clef
t-ty
pepr
oces
ses
pred
omin
antly
sono
rant
artic
wea
kar
ticul
atio
nm
voic
eles
sh
fo
rpl
osiv
esna
sal
rele
ase
ofpl
osiv
esna
sal
emis
sion
with
cons
onan
tsm
pass
ive
nasa
lfr
icat
ives
Act
ive
clef
t-ty
pepr
oces
ses
nasa
lfr
icat
ives
phar
ynge
alg
lott
alar
ticul
atio
nba
ckin
gto
uvul
arba
ckin
gto
vela
rm
m
late
ral
pala
tal
fric
ativ
esm
mm
doub
lear
ticul
atio
ngl
idin
gfr
icat
ive
1=1-
stag
esu
rger
ysu
bjec
ts
24=
2-st
age
surg
ery
hard
pala
tere
pair
edat
abou
t4
yrs
28=
2-st
age
surg
ery
with
hard
pala
tere
pair
edat
abou
t8
yrs
A Harding and P Grunwell342
unrepaired hard palates had in fact restricted their phonetic repertoire imposing aneed for individual adaptability The additional active processes employed by thesesubjects were presumably a response to the restrictions imposed by their oro-nasalstructure and velopharyngeal function at the time of consonant acquisition Asshown in table 2 the most common active cleft-type processes persisting at age46 with a residual cleft of the hard palate were backing double articulation andlateralpalatal articulation Two 1-stage surgery subjects whose entire palates hadbeen repaired at ages 09 and 010 did not use any cleft-type processes at age 46
By age 90 (table 3) a much-diminished number of cleft type processes wasevident except in subjects with sizeable anterior stulae who had received littlespeech and language therapy A similarity was noted between the speech patternsof 1-stage surgery subjects with stulae (DA and SB) at age 90 (table 3) and theyounger BCLP subjects at age 46 (table 1) who also had anterior palatal defectsThey included non-oral realizations of t d s k g occasional nasal fricatives andpharyngealglottal articulations Fistulae had apparently continued to in uencearticulation and phonological development in these subjects
Finally at age 130 (table 4) the diVerences between 1-stage and 2-stage surgerysubjects had diminished leaving only one 2-stage subject with occasional backingand four subjects with slight palatal and lateral release of fricative consonants Onlytwo of the 1-stage surgery subjects were using minor distortions of grooved fricativeproduction
Whilst there were apparent trends in speech production relating to surgicaltiming and oral structure it is noted that there were exceptions to each tentativegeneralization Subjects with marked structural imperfections occasionally producedrealizations of which they would not have been thought capable and subjects withno visible imperfections produced inexplicably distorted speech patterns It istherefore concluded that whilst there is homogeneity in the range of processesproduced by this population assumptions cannot be made about speech based onsurgical timing or type of cleft Tentative predictions based on detailed assessmentmay be clinically very useful
EVects of surgery on speech
Activepassive processes have identi ed those cleft-type characteristics thought tobe associated with a physical inability to produce pressure consonants The followinganalysis of speech changes after surgical intervention at diVerent ages identi es thechanges eVected by surgery when intra-oral pressure could be more readily achieved
Two children were rst recorded prior to the rst stage of a 2-stage procedureTheir lips were repaired at approximately 6 months of age and soft palate repairwas carried out at ages 18 and 19 respectively Their hard palates were leftunrepaired to facilitate unrestricted growth of the mid-face (Hotz et al 1978) Pre-and post-operative consonant-like sounds present in the recorded speech samplesare listed in table 5 Interestingly prior to soft palate repair both these childrenproduced some oral consonants Subject B was producing pressure consonants [kg] in his babble prior to soft palate repair Considering that he had an unrepairedbilateral cleft palate at this point it was surprising that he had any oral consonantsPost-operatively at 20 years he used [b bkm t d g gkb] which indicated that surgeryto repair the soft palate had facilitated an increased range of oral pressure consonantsSubject D was producing [p b k g] pre-operatively Post-operatively following soft
Active versus passive cleft-type speech characteristics 343
Tab
le5
EV
ects
ofso
ftp
alat
ere
pair
atag
e1
6on
BC
LP
subj
ects
h
ard
pal
ate
rem
ain
sun
repa
ired
2-st
age
subj
ects
Surg
ery
Pre
-ope
rati
vesp
eech
patt
ern
atag
e1
6Po
st-o
pera
tive
chan
ges
insp
eech
atag
e2
0
Stud
y1
BSo
ftpa
late
repa
irat
16
Adu
ltta
rget
sk
gA
t2
0[b
b kmg kb
td
g]D
Soft
pala
tere
pair
17
Adu
ltta
rget
sp
bk
gA
t2
0[p
bd
b kdk
g]
Tab
le6
EV
ects
ofha
rdpa
late
rep
air
atag
e6
6an
d
stu
lare
pair
atag
e10
0
Subj
ect
Surg
ery
Pre
-ope
rati
vesp
eech
patt
ern
Post
-ope
rati
vech
ange
sin
spee
ch
MS
Har
dpa
late
repa
ir6
6Pa
ssiv
epr
oces
s7
6E
limin
ated
pass
ive
proc
ess
Var
iabl
ena
sal
rele
ase
ofco
nson
ants
Hyp
onas
alna
sals
JFH
ard
pala
tere
pair
(uns
ucce
ssfu
l)6
6Se
vera
lac
tive
and
pass
ive
proc
esse
s7
6A
ctiv
epr
oces
ses
rem
aine
dPa
ssiv
epr
oces
ses
elim
inat
ed
DA
Fis
tula
repa
ir10
0A
ctiv
epr
oces
ses
110
Elim
inat
ion
ofph
aryn
geal
glo
ttal
Var
iabi
lity+
+an
dna
sal
arti
cula
tion
Art
icul
ator
yva
riab
ility
++
Act
ive
CT
Rs
proc
esse
spe
rsis
t
A Harding and P Grunwell344
palate repair but with a residual cleft in the hard palate his range of consonantsincluded [d] which was particularly surprising since the hard palate remainedunrepaired Whilst it is unlikely that toddlers of 18 months could be consciouslytrying to compensate for articulatory inadequacy in producing velar plosives inbabble prior to soft palate repair and an alveolar plosive prior to hard palate repairboth these subjects showed evidence of actively pursuing their articulatory potential
Table 6 summarizes changes following surgery to repair the hard palate in moremature speech patterns These subjects who were aged 66 and 100 pre-operativelyhad learned to speak with residual clefts and were apparently unaware of theconsonant productions that failed to match normal production
Subject MS used only passive processes in his speech pattern He realized someconsonants nasally such that lsquoballrsquo was [mO~] and lsquosockrsquo was [(sk)n
deg Aacute~ k] Looking atpost-operative changes at age 76 his consonant production was normal but hisresonance had become hyponasal Pre-operatively at age 66 Subject JF was usingseveral active and passive processes The active processes were unaVected by surgerybut passive processes were eliminated
Fistula repair was carried out at age 100 on Subject DA who had many activeprocesses and very variable articulation pre-operatively Post-operatively at age110 he was not using non-oral pharyngeal and glottal active processes or nasalrealizations but many oral cleft-type realizations remained
As shown in table 7 hard palate re-repair and pharyngoplasty was carried outon two subjects whose hard palate repairs had been unsuccessful at approximately4 years Subject NC assessed pre-operatively at age 56 was using predominantlypassive processes in her speech She was also using [ j] for fricatives s S whichwas thought to be an active process At age 60 following hard palate re-repair andpharyngoplasty all cleft-type processes had been eliminated without post-operativespeech therapy Since [ j] for s apparently resolved spontaneously followingsurgery it can be assumed that this was a passive process in this speech sample
Subject CP who underwent this procedure presented pre-operatively at age 46with both passive and active processes but his nasal resonance was not consistentlyhypernasal In addition to his cleft-related speech disorder this subject had additionaldevelopmental speech diYculties which were identi ed as being unrelated to thecleft Post-operatively at age 56 little had changedmdashnotably the passive processnasal [m] for b was retained His nasal resonance had become hyponasal andthere was no apparent bene t from surgical intervention The realization of b as[m] had become phonologically stable and surgery alone had not destabilized thephonological system This realization may have been a passive product of VPI inearly speech acquisition which had subsequently become part of a phonologicaldisorder Post-operatively CPrsquos phonetic repertoire did increase but the phonologicaldistribution was variable Plosive targets were still realized as nasals in spontaneousspeech at the nal speech recording at age 76 This was not as an inevitableconsequence of VPI but a result of an inability to destabilize the phonologicalprocess determining that voiced plosives would be realized as nasals This resultfollowing surgery highlights the importance of identifying phonological learningproblems and distinguishing them from structural constraints on articulationIn CPrsquos case pre-operative exploration of the eVect of nares occlusion duringspeech might have indicated that structural change would not improve consonantproduction spontaneously
A general observation was that consonant realizations did not move rapidly
Active versus passive cleft-type speech characteristics 345
Tab
le7
EV
ects
ofha
rdpa
late
re-r
epai
ran
dp
hary
ngo
pla
sty
Subj
ect
Surg
ery
Pre
-ope
rati
vesp
eech
patt
ern
Post
-ope
rativ
ech
ange
sin
spee
ch
Stud
y2
NC
Har
dpa
late
re-r
epai
ran
d5
6Pa
ssiv
ecl
eft-
type
proc
esse
s6
0A
llcl
eft-
type
phar
yngo
plas
ty5
10[
j]
for
fric
ativ
espr
oces
ses
elim
inat
ed[
h]
for
plos
ives
SIW
IV
aria
ble
arti
cula
rypr
ecis
ion
CP
Har
dpa
late
repa
iran
d4
6Pa
ssiv
ean
dac
tive
proc
esse
s5
6Pa
ssiv
epr
oces
sph
aryn
gopl
asty
50
Pho
nolo
gica
lco
nfus
ion
[m]
for
[b
]re
tain
edH
ypon
asal
nasa
lsPe
rsis
ting
phon
olog
ical
conf
usio
ns
A Harding and P Grunwell346
from incorrect to correct but progressed incrementally towards normal realizationsas described by Morley (1970) Where an early realization of target s might beglottal [h] a gradual pattern of change showed subsequent realizations to bepharyngeal [Eacute] then uvular [X] then velar [x] and eventually palatal [c] or lateral [Euml]It was interesting to note that speech patterns continued to change as late as90ndash110 years with the result that diVerences related to surgical timing and cleft-type gradually disappeared Persisting stulae were thought to account for the mostmarked cleft type processes at age 90
Implications for surgical management
This analysis of speech changes following surgery suggests some implications forsurgical management which are compatible with Sell and Grunwellrsquos (1990) ndingsin the Sri Lankan study
Surgery can change passive speech processes but it is also possible that speechtherapy may be able to change passive patterns Surgery alone is unlikely to modifyactive cleft-type processes whereas speech therapy should be able to modify activeprocesses Indications from these case studies is that where speech is the primaryproblem speech assessment should distinguish between active and passive processesin order to evaluate the necessity for full investigations and to plan therapeuticintervention Where past speech therapy has not been successful it cannot beassumed that surgical intervention will facilitate further speech progress A furthercourse of speech therapy which is sensitive to active versus passive processes todevelopmental phonological in uences on cleft-type speech development and toarticulatory diYculties in diVerent speech contexts might facilitate optimal progressWhere structural imperfection exists it is quite possible for single-word productionto be more precise than target realizations in spontaneous speech This may not bea failure of phonological generalization (Grunwell 1992) but the result of diYcultysustaining the necessary lsquoarticulatory eVort rsquo (Harding and Grunwell 1993) resultingin articulatory imprecision Deteriorating articulatory accuracy should not be over-looked in interpretation of speech results
An analytical protocol
As a result of analysing the speech data and identifying the active and passiveprocesses a protocol has been developed which records examples of each cleft-typeprocess over a series of assessments It demonstrates the progression of individualprocesses towards an adult target (see the Appendix) At each assessment onecolumn is used to indicate nasal resonance nasal emission and nasal turbulenceratings and cleft-type processes Changes in the nature of error realizations mightshow progress towards target consonants Hence whilst the total correct scoremight not have increased increments of change can be observed This observationof patterns of change may function as an adjunct to GOSSPASSrsquo98 (Sell et al 1998)giving access to a greater depth of both quantitative and qualitative data aboutconsonant production in relation to resonance nasal emission nasal turbulenceoral structure and cleft-type
Active versus passive cleft-type speech characteristics 347
Diagnostic implications
Passive versus active nasal fricatives
The important management consideration related to this distinction is that an activenasal fricative is an established phonological process which is unlikely to be directlyaVected by surgery alone Therapy would be necessary to destabilize nasal realizationsof oral consonants In contrast passive nasal fricatives may be eliminated by surgeryOf particular relevance is diVerential diagnosis between passive and active nasalfricatives in surgical and therapeutic management When hypernasality co-occurswith nasal air ow during consonant production which can be redirected by nose-holding passive nasal fricatives are diagnosed These would be transcribed as [(sk)n
deg]
passive alveolar nasal fricatives [(Wk)mdeg
] bilabial nasal fricatives or [(fk)Iacutedeg ] labiodentalnasal fricatives Full VPI investigations would be recommended to diagnose thenature of the structural or functional de ciency and distinguish between velopharyn-geal incompetence and velopharyngeal mislearning
It is highly likely that plosive targets would be aVected by reduced intra-oral airpressure such that plosives would either be realized by nasal counterparts eg bd[ [m n] or [b d] may be nasalized and weak Voiceless plosives may be eitheraccompanied by nasal emission [p t k] or realized as glottal fricative [h]
Production of the target sentence lsquoI saw Sam sitting on a busrsquo might be
[aI (sk)ndeg O~ (sk)n
degaelig~m (sk)n
deg IhIn Aacute~n mouml~(sk)ndeg] passive processes and
[aI xO xaeligm xIkIIcirc AacuteIcirc goumlx] active processes
Contribution to surgical management decisions
Passiveactive interpretation of clinical assessments might facilitate surgical manage-ment decisions If noseholding does not facilitate correct production of targetconsonants then it is likely that an alternative articulatory pattern has becomephonologically established ie particular realizations for one or more targets areconsistently distributed in the phonological system These realizations may haveevolved because of initial diYculty producing articulatory targets and subsequentlystabilized within the phonological system Grundy and Harding (1995) refer to thisphenomenon as an lsquoarticulatory disorder with phonological consequencesrsquo
Therapy
Where obvious structural defects or diagnosed dysfunction exists clinicians fre-quently defer therapeutic intervention until surgery has been undertaken Theexpectation would be that normal structure and function is essential for normalspeech However pre-operative therapy may facilitate oral consonant productionwhich may serve to reduce hypernasal resonance Hence therapy prior to surgerymay avoid unnecessary surgery or reduce the extent of surgery required All activeprocesses are likely to require therapy
Principled selection of targets for therapy
Speech patterns frequently evidence a mixture of apparently passive and activeprocesses which complicates decisions about target selection Target selection can
A Harding and P Grunwell348
be based on assessment of which consonant targets can be most easily elicted inisolation (stimulability) This may lead to a sequence of target selection which isopposite to the sequence of consonant acquisition in normal development Forexample where reduced intra-oral pressure is present in a passive pattern [T] maybe easier to elicit in imitation than more nely grooved [s] or [S] Therapy maytarget [T] followed by [S ] and nally [s] As in non-cleft phonological therapywhere a class of consonants is aVected by the cleft then it is helpful to target theentire class The following decision-making process can be applied for both activeand passive processes
Decision making procedure for target selection
(1) Voiced versus voiceless targets(2) Front versus back placements(3) Syllable initial versus syllable nal targets(4) Plosives versus fricative targets
Voiceless plosives and fricatives are produced with an open glottis whichfacilitates topping up of air ow from the lungs hence voiceless plosive and fricativetargets are frequently more successful than voiced counterparts (Isshiki and Ringel1964) Front targets usually cause more diYculty than back particularly where analveolar defect or stula exists Contrary to normal development back targets maybe targeted before front Word- nal targets generally require less oral air pressurethan word initial targets and similarly fricatives may be more easily elicited thanplosives Fricatives do require a greater volume of air than plosives (Fletcher 1985)but in the presence of nasal escape weak fricative production appears to be morereadily achieved than weak plosive production Since nal fricatives would normallybe acquired in advance of word-initial fricatives (Ferguson 1978) targeting word- nal fricatives is frequently a productive starting point for therapy
Principles of therapy for passive processes
(1) Use of soft attack similar to gentle whisper for all target models ensuresminimal articulatory eVort (Harding and Grunwell 1993) and requires min-imal intra-oral air pressure It may be appropriate to gradually increase thearticulatory attack when the articulatory posture and evidence of intendedoral air ow have been established
(2) Slightly stretched duration of segment transitions in models of consonantto vowel (CndashV) or vowel to consonant (VndashC) facilitates review of motorplanning and extends the available time for execution of the new motorprogrammer whilst maintaining control of the oral airstream
(3) Noseholding can be used to provide exclusively oral air ow Gradual releaseof the nostrils during production of sustained [VVVVVf ] or [hhhhh ] allowsthe child to attempt to sustain an oral consonant despite increasing nasalemission This maximizes the use of available oral air ow Procedures forusing noseholding are described in some detail by Golding-Kushner (1995)
Principles of therapy for active processes
This is more like phonological therapy and can follow Grunwellrsquos (1991) processesfor phonological change and principled decision-making (Grunwell 1992) Some
Active versus passive cleft-type speech characteristics 349
examples are given here by way of illustration of ways to eVect the rst twoprocesses of change which may need to be approached diVerently in cleft palateversus non-cleft speech disorders DiVerent approaches may also be appropriate formodifying active versus passive cleft-type processes
Innovation production of new targets Some useful principles
(1) Introduction of new lsquonon-speech likersquo targets in sound play using a conson-ant sound segment model such as [ph ] note not a syllable like [p] whichis the type of pronunciation used when target sounds are presented as lettersfor reading Target [s] might be introduced as a lsquoTrain Slowing Down Noisersquo[ts ts ts tssssssss]
(2) lsquoNew consonantsrsquo can later be modelled and elicited in soft productions ofsyllable structure [tssssndashi] [ indashtssss] which can subsequently be identi ed assimilar to words lsquosearsquo and lsquoeatsrsquo
(3) lsquoDeferring responsibilityrsquo transfers responsibility or lsquoblamersquo for errors fromthe child and attributes it to the articulators eg lsquoyour tongue is havingtrouble with hellip rsquo lsquoLetrsquos show your tongue how to hellip rsquo
(4) New targets can be modelled repeatedly and recorded on audio or videotape which can be listened to at home
(5) Targeting classes of consonants (eg alveolars t d s n l voiceless fricativesf s S perhaps with aVricate T avoids phonological confusion whichmight occur if production ofsis achieved whilst other alveolar targetsremain backed The risk is that s might not integrate into the phonologicalsystem unless all backed alveolar consonants are destabilized
(6) Increased eye contact during auditory and production work can be invaluablein holding visual and auditory attention and ensures that visual informationabout the sound has been processed This is easily achieved by the clinicianlifting any focus of the childrsquos attention close to hisher mouth at theprecise moment when the target is modelled
Stimulation of non-speech related sounds such as a lsquoTrain Slowing DownNoisersquo [ts ts tsss] con rms that target [s] is physically achievable whether or not[ssss] can be imitated Some children continue to access [s] through the lsquoTrainSlowing Down Noisersquo throughout therapy until it is occurring spontaneouslywithout conscious planning This can be an eVective means of underminingestablished motor programmers (Hewlett 1990) for active cleft-type processes
Destabilizing active processes
As it is likely that children will be unaware of each occurrence of their alternativearticulatory pattern for speci c consonant errors it is preferrable to destabilizeactive processes with minimal conscious eVort by the child As children becomeaware of their mismatches they frequently add the newly acquired target realizationto their existing production eg target word tu childrsquos old realization [ku] childrsquoscorrected realization [t-ku] Destabilization can be achieved with minimal consciouseVort through input therapy techniques such as auditory bombardment (Lancasterand Pope 1989) auditory decision-making such as lsquowhich bear says this wordproperlyrsquo Red Bear says lsquotworsquo or Blue Bear says lsquocoorsquo This type of strategy oftenprecipitates attention to the target consonant with possible lsquoreplayrsquo and lsquoreviewrsquo of
A Harding and P Grunwell350
their own production Frequent stimulation of cognitive alertness to the targetconsonant can develop awareness without confronting the child with errors orrisking hisher failure The child is then free to attempt to repair hisher ownrealization to continue to re ect and to silently rehearse the adult realizationTraditional articulation therapy is thus combined with development of metaphonol-ogical skills ie the ability to re ect upon onersquos own speech production The resultshould be that new target realizations will be more phonologically stable thanexclusively production-based articulation therapy might have facilitated
Stabilizationgeneralization
Procedures to ensure stabilization and generalization of new target consonantswould be as described by Grunwell (1992) Success may be constrained by theconsiderable articulatory eVort sometimes required to maintain pressure consonantproduction in spontaneous speech (Harding and Grunwell 1993)
Conclusions
In speech assessment it is helpful to distinguish between errors which are cleft-type and non-cleft type and those which are part of active versus passive processesThe active and passive processes have been de ned and their phonological implica-tions discussed Focus on active and passive processes has facilitated focus on thephonological consequences of cleft palate on speech development In the futureawareness of the likely eVect of a cleft palate on normal phonological developmentcould avoid extended periods of unsuccessful clinical intervention Furthermoresensitivity to the relationship between phonological processes and structural con-straints should facilitate theoretically based management decisions Incidences suchas the case of CP in which nasal realizations were thought to indicate VPI but weresubsequently unaVected by surgery might be avoided if phonological analysiscontributes to management decisions
Surgery did improve hypernasal resonance and eliminated passive processes buthad little eVect on active processes Active processes in younger subjects werethought to require therapeutic intervention but in the longer term the oldersubjects showed few cleft-type processes Whilst it is possible that active cleft-typeprocesses may resolve with increasing age the implication for the future is thatactive cleft-type processes should be treated with skilled therapeutic interventionnot surgery Therapy which addresses the phonological consequences of cleft palateon speech development by combining metaphonologicalphonologicalarticulatoryapproaches is likely to be successful
References
Albery E 1991 Consonant articulation in the diVerent types of cleft lip and palate UnpublishedMPhil thesis Leicester Polytechnic
Albery E and Grunwell P 1993 Consonant articulation in diVerent types of cleft palate InP Grunwell (Ed) Analysing Cleft Palate Speech (London Whurr)
Ferguson C A 1978 Fricatives in child language acquisition In V Honsa and M Hardmann-Battista (Eds) Papers on Linguistics and Child Language (Mouton The Hague)
Fletcher S G 1985 Speech production and oral motor skill in an adult with an unrepaired palatalcleft Journal of Speech and Hearing Disorders 50 254ndash261
Active versus passive cleft-type speech characteristics 351
Golding-Kushner K J 1995 Treatment of articulation and resonancne disorders associated withcleft palate management and VPI In R Shprintzen (Ed) Cleft Palate Speech Management AMultidisciplinary Approach (St Louis Mosby)
Grundy K and Harding A 1995 Developmental speech disorders In K Grundy (Ed) Linguisticsin Clinical Practice (2nd edition) (London Whurr)
Grunwell P 1985 Phonological Assessment of Child Speech (Windsor NFER-Nelson)Grunwell P 1987a Clinical Phonology (2nd edition) (London Croom Helm)Grunwell P 1987b PACS Pictures Language Elicitation Materials (Windsor NFER-Nelson)Grunwell P 1991 Processes of phonological change in developmental speech disorders Clinical
Linguistics and Phonetics 6 101ndash122Grunwell P 1992 Principled decision making in the remediation of children with phonological
disorders In P Fletcher and D Hall (Eds) Specic Speech and Language Disorders in Children(London Whurr)
Grunwell P and Harding A 1995 PACSTOYS A Screening Assessment of Phonological Development(Windsor NFER-Nelson)
Grunwell P and Harding A 1996 A note on describing types of nasality Clinical Linguistics andPhonetics 10 157ndash161
Harding A 1993 An Investigation into the Relationship Between Timing of Cleft Palate Repairand Speech Development Unpublished PhD thesis
Harding A and Grunwell P 1993 The relationship between speech and timing of hard palaterepair In P Grunwell (Ed) Analysisng Cleft Palate Speech (London Whurr)
Harding A and Grunwell P 1996 Characteristics of cleft palate speech European Journal ofDisorders of Communication 31 331ndash358
Henningsson G and Isberg A M 1986 Velopharyngeal movement patterns in patients alternatingbetween oral and glottal articulation A clinical and cineradiographicical study Cleft Palate Journal23 1ndash9
Hewlett N 1990 Processes of development and production In P Grunwell (Ed) DevelopmentalSpeech Disorders (Edinburgh Churchill Livingstone)
Hotz M M Gnoinski W M Nussbaumer H and Kistler E 1978 Early orthopaedics in CLPcases guidelines for surgery Cleft Palate Journal 15 405ndash411
Hutters B and Brondsted K 1987 Strategies in cleft palate with special reference to DanishCleft Palate Journal 24 127ndash136
Isshiki N and Ringel R 1964 Airow during the production of selected consonants Journal ofSpeech and Hearing Research 7 233ndash244
Kummer A W Curtis C Wiggs M Lee L and Strife J L 1992 Comparison of velopharyngealgap size in patients with hypernasality hypernasality with nasal emission and nasal emissionor nasal turbulence (rustle) as the primary speech characteristic Cleft-palate-Craniofacial Journal29 152ndash156
Lancaster G and Pope L 1989 Working with Childrenrsquos Phonology (Oxford Winslow)Morley M E 1970 Cleft Palate and Speech (7th edition) (Edinburgh Churchill Livingstone)Russell V J 1991 Speech Development in Children with Cleft Lip and Palate Unpublished PhD
thesis Leicester PolytechnicRussell V J and Grunwell P 1993 Speech development in children with cleft lip and palate In
P Grunwell (Ed) Analysing Cleft Palate Speech (London Whurr)Sell D A and Grunwell P 1990 Speech results following late palatal surgery in previously
unoperated Sri Lankan adolescents with cleft palate Cleft Palate Journal 27 162ndash168Sell D Harding A and Grunwell P 1994 GOSSPASS A screening assessment of cleft palate
speech European Journal of Disorders of Communication 29 1ndash15Sell D Harding A and Grunwell P 1998 GOSSPASSrsquo98 An assessment for speech disorders
associated with cleft palate andor velopharyngeal dysfunction International Journal of Languageamp Communication Disorders ( in press)
Shorter E 1995 A spectographic analyis of child homophones Unpublished honours project DeMontfort University Leicester
Stenglehoffen J 1989 Nature and causes of communication diYculties In J Stengelhofen (Ed)Cleft Palate Nature and Remediation of Communication Problems (Edinburgh Churchill Livingstone)
Trost J E 1981 Articulatory additions to the classical description of the speech of persons withcleft palate Cleft Palate Journal 18
Trost-Cardamone J E 1990 The development of speech assessing cleft palate misarticulationsIn D A Kernahan and S N Rosenstein (Eds) Cleft Lip and Palate A System of Management(Baltimore Williams amp Wilkins)
A Harding and P Grunwell352
Appendix Active passive analysis of cleft palate speech

A Harding and P Grunwell342
unrepaired hard palates had in fact restricted their phonetic repertoire imposing aneed for individual adaptability The additional active processes employed by thesesubjects were presumably a response to the restrictions imposed by their oro-nasalstructure and velopharyngeal function at the time of consonant acquisition Asshown in table 2 the most common active cleft-type processes persisting at age46 with a residual cleft of the hard palate were backing double articulation andlateralpalatal articulation Two 1-stage surgery subjects whose entire palates hadbeen repaired at ages 09 and 010 did not use any cleft-type processes at age 46
By age 90 (table 3) a much-diminished number of cleft type processes wasevident except in subjects with sizeable anterior stulae who had received littlespeech and language therapy A similarity was noted between the speech patternsof 1-stage surgery subjects with stulae (DA and SB) at age 90 (table 3) and theyounger BCLP subjects at age 46 (table 1) who also had anterior palatal defectsThey included non-oral realizations of t d s k g occasional nasal fricatives andpharyngealglottal articulations Fistulae had apparently continued to in uencearticulation and phonological development in these subjects
Finally at age 130 (table 4) the diVerences between 1-stage and 2-stage surgerysubjects had diminished leaving only one 2-stage subject with occasional backingand four subjects with slight palatal and lateral release of fricative consonants Onlytwo of the 1-stage surgery subjects were using minor distortions of grooved fricativeproduction
Whilst there were apparent trends in speech production relating to surgicaltiming and oral structure it is noted that there were exceptions to each tentativegeneralization Subjects with marked structural imperfections occasionally producedrealizations of which they would not have been thought capable and subjects withno visible imperfections produced inexplicably distorted speech patterns It istherefore concluded that whilst there is homogeneity in the range of processesproduced by this population assumptions cannot be made about speech based onsurgical timing or type of cleft Tentative predictions based on detailed assessmentmay be clinically very useful
EVects of surgery on speech
Activepassive processes have identi ed those cleft-type characteristics thought tobe associated with a physical inability to produce pressure consonants The followinganalysis of speech changes after surgical intervention at diVerent ages identi es thechanges eVected by surgery when intra-oral pressure could be more readily achieved
Two children were rst recorded prior to the rst stage of a 2-stage procedureTheir lips were repaired at approximately 6 months of age and soft palate repairwas carried out at ages 18 and 19 respectively Their hard palates were leftunrepaired to facilitate unrestricted growth of the mid-face (Hotz et al 1978) Pre-and post-operative consonant-like sounds present in the recorded speech samplesare listed in table 5 Interestingly prior to soft palate repair both these childrenproduced some oral consonants Subject B was producing pressure consonants [kg] in his babble prior to soft palate repair Considering that he had an unrepairedbilateral cleft palate at this point it was surprising that he had any oral consonantsPost-operatively at 20 years he used [b bkm t d g gkb] which indicated that surgeryto repair the soft palate had facilitated an increased range of oral pressure consonantsSubject D was producing [p b k g] pre-operatively Post-operatively following soft
Active versus passive cleft-type speech characteristics 343
Tab
le5
EV
ects
ofso
ftp
alat
ere
pair
atag
e1
6on
BC
LP
subj
ects
h
ard
pal
ate
rem
ain
sun
repa
ired
2-st
age
subj
ects
Surg
ery
Pre
-ope
rati
vesp
eech
patt
ern
atag
e1
6Po
st-o
pera
tive
chan
ges
insp
eech
atag
e2
0
Stud
y1
BSo
ftpa
late
repa
irat
16
Adu
ltta
rget
sk
gA
t2
0[b
b kmg kb
td
g]D
Soft
pala
tere
pair
17
Adu
ltta
rget
sp
bk
gA
t2
0[p
bd
b kdk
g]
Tab
le6
EV
ects
ofha
rdpa
late
rep
air
atag
e6
6an
d
stu
lare
pair
atag
e10
0
Subj
ect
Surg
ery
Pre
-ope
rati
vesp
eech
patt
ern
Post
-ope
rati
vech
ange
sin
spee
ch
MS
Har
dpa
late
repa
ir6
6Pa
ssiv
epr
oces
s7
6E
limin
ated
pass
ive
proc
ess
Var
iabl
ena
sal
rele
ase
ofco
nson
ants
Hyp
onas
alna
sals
JFH
ard
pala
tere
pair
(uns
ucce
ssfu
l)6
6Se
vera
lac
tive
and
pass
ive
proc
esse
s7
6A
ctiv
epr
oces
ses
rem
aine
dPa
ssiv
epr
oces
ses
elim
inat
ed
DA
Fis
tula
repa
ir10
0A
ctiv
epr
oces
ses
110
Elim
inat
ion
ofph
aryn
geal
glo
ttal
Var
iabi
lity+
+an
dna
sal
arti
cula
tion
Art
icul
ator
yva
riab
ility
++
Act
ive
CT
Rs
proc
esse
spe
rsis
t
A Harding and P Grunwell344
palate repair but with a residual cleft in the hard palate his range of consonantsincluded [d] which was particularly surprising since the hard palate remainedunrepaired Whilst it is unlikely that toddlers of 18 months could be consciouslytrying to compensate for articulatory inadequacy in producing velar plosives inbabble prior to soft palate repair and an alveolar plosive prior to hard palate repairboth these subjects showed evidence of actively pursuing their articulatory potential
Table 6 summarizes changes following surgery to repair the hard palate in moremature speech patterns These subjects who were aged 66 and 100 pre-operativelyhad learned to speak with residual clefts and were apparently unaware of theconsonant productions that failed to match normal production
Subject MS used only passive processes in his speech pattern He realized someconsonants nasally such that lsquoballrsquo was [mO~] and lsquosockrsquo was [(sk)n
deg Aacute~ k] Looking atpost-operative changes at age 76 his consonant production was normal but hisresonance had become hyponasal Pre-operatively at age 66 Subject JF was usingseveral active and passive processes The active processes were unaVected by surgerybut passive processes were eliminated
Fistula repair was carried out at age 100 on Subject DA who had many activeprocesses and very variable articulation pre-operatively Post-operatively at age110 he was not using non-oral pharyngeal and glottal active processes or nasalrealizations but many oral cleft-type realizations remained
As shown in table 7 hard palate re-repair and pharyngoplasty was carried outon two subjects whose hard palate repairs had been unsuccessful at approximately4 years Subject NC assessed pre-operatively at age 56 was using predominantlypassive processes in her speech She was also using [ j] for fricatives s S whichwas thought to be an active process At age 60 following hard palate re-repair andpharyngoplasty all cleft-type processes had been eliminated without post-operativespeech therapy Since [ j] for s apparently resolved spontaneously followingsurgery it can be assumed that this was a passive process in this speech sample
Subject CP who underwent this procedure presented pre-operatively at age 46with both passive and active processes but his nasal resonance was not consistentlyhypernasal In addition to his cleft-related speech disorder this subject had additionaldevelopmental speech diYculties which were identi ed as being unrelated to thecleft Post-operatively at age 56 little had changedmdashnotably the passive processnasal [m] for b was retained His nasal resonance had become hyponasal andthere was no apparent bene t from surgical intervention The realization of b as[m] had become phonologically stable and surgery alone had not destabilized thephonological system This realization may have been a passive product of VPI inearly speech acquisition which had subsequently become part of a phonologicaldisorder Post-operatively CPrsquos phonetic repertoire did increase but the phonologicaldistribution was variable Plosive targets were still realized as nasals in spontaneousspeech at the nal speech recording at age 76 This was not as an inevitableconsequence of VPI but a result of an inability to destabilize the phonologicalprocess determining that voiced plosives would be realized as nasals This resultfollowing surgery highlights the importance of identifying phonological learningproblems and distinguishing them from structural constraints on articulationIn CPrsquos case pre-operative exploration of the eVect of nares occlusion duringspeech might have indicated that structural change would not improve consonantproduction spontaneously
A general observation was that consonant realizations did not move rapidly
Active versus passive cleft-type speech characteristics 345
Tab
le7
EV
ects
ofha
rdpa
late
re-r
epai
ran
dp
hary
ngo
pla
sty
Subj
ect
Surg
ery
Pre
-ope
rati
vesp
eech
patt
ern
Post
-ope
rativ
ech
ange
sin
spee
ch
Stud
y2
NC
Har
dpa
late
re-r
epai
ran
d5
6Pa
ssiv
ecl
eft-
type
proc
esse
s6
0A
llcl
eft-
type
phar
yngo
plas
ty5
10[
j]
for
fric
ativ
espr
oces
ses
elim
inat
ed[
h]
for
plos
ives
SIW
IV
aria
ble
arti
cula
rypr
ecis
ion
CP
Har
dpa
late
repa
iran
d4
6Pa
ssiv
ean
dac
tive
proc
esse
s5
6Pa
ssiv
epr
oces
sph
aryn
gopl
asty
50
Pho
nolo
gica
lco
nfus
ion
[m]
for
[b
]re
tain
edH
ypon
asal
nasa
lsPe
rsis
ting
phon
olog
ical
conf
usio
ns
A Harding and P Grunwell346
from incorrect to correct but progressed incrementally towards normal realizationsas described by Morley (1970) Where an early realization of target s might beglottal [h] a gradual pattern of change showed subsequent realizations to bepharyngeal [Eacute] then uvular [X] then velar [x] and eventually palatal [c] or lateral [Euml]It was interesting to note that speech patterns continued to change as late as90ndash110 years with the result that diVerences related to surgical timing and cleft-type gradually disappeared Persisting stulae were thought to account for the mostmarked cleft type processes at age 90
Implications for surgical management
This analysis of speech changes following surgery suggests some implications forsurgical management which are compatible with Sell and Grunwellrsquos (1990) ndingsin the Sri Lankan study
Surgery can change passive speech processes but it is also possible that speechtherapy may be able to change passive patterns Surgery alone is unlikely to modifyactive cleft-type processes whereas speech therapy should be able to modify activeprocesses Indications from these case studies is that where speech is the primaryproblem speech assessment should distinguish between active and passive processesin order to evaluate the necessity for full investigations and to plan therapeuticintervention Where past speech therapy has not been successful it cannot beassumed that surgical intervention will facilitate further speech progress A furthercourse of speech therapy which is sensitive to active versus passive processes todevelopmental phonological in uences on cleft-type speech development and toarticulatory diYculties in diVerent speech contexts might facilitate optimal progressWhere structural imperfection exists it is quite possible for single-word productionto be more precise than target realizations in spontaneous speech This may not bea failure of phonological generalization (Grunwell 1992) but the result of diYcultysustaining the necessary lsquoarticulatory eVort rsquo (Harding and Grunwell 1993) resultingin articulatory imprecision Deteriorating articulatory accuracy should not be over-looked in interpretation of speech results
An analytical protocol
As a result of analysing the speech data and identifying the active and passiveprocesses a protocol has been developed which records examples of each cleft-typeprocess over a series of assessments It demonstrates the progression of individualprocesses towards an adult target (see the Appendix) At each assessment onecolumn is used to indicate nasal resonance nasal emission and nasal turbulenceratings and cleft-type processes Changes in the nature of error realizations mightshow progress towards target consonants Hence whilst the total correct scoremight not have increased increments of change can be observed This observationof patterns of change may function as an adjunct to GOSSPASSrsquo98 (Sell et al 1998)giving access to a greater depth of both quantitative and qualitative data aboutconsonant production in relation to resonance nasal emission nasal turbulenceoral structure and cleft-type
Active versus passive cleft-type speech characteristics 347
Diagnostic implications
Passive versus active nasal fricatives
The important management consideration related to this distinction is that an activenasal fricative is an established phonological process which is unlikely to be directlyaVected by surgery alone Therapy would be necessary to destabilize nasal realizationsof oral consonants In contrast passive nasal fricatives may be eliminated by surgeryOf particular relevance is diVerential diagnosis between passive and active nasalfricatives in surgical and therapeutic management When hypernasality co-occurswith nasal air ow during consonant production which can be redirected by nose-holding passive nasal fricatives are diagnosed These would be transcribed as [(sk)n
deg]
passive alveolar nasal fricatives [(Wk)mdeg
] bilabial nasal fricatives or [(fk)Iacutedeg ] labiodentalnasal fricatives Full VPI investigations would be recommended to diagnose thenature of the structural or functional de ciency and distinguish between velopharyn-geal incompetence and velopharyngeal mislearning
It is highly likely that plosive targets would be aVected by reduced intra-oral airpressure such that plosives would either be realized by nasal counterparts eg bd[ [m n] or [b d] may be nasalized and weak Voiceless plosives may be eitheraccompanied by nasal emission [p t k] or realized as glottal fricative [h]
Production of the target sentence lsquoI saw Sam sitting on a busrsquo might be
[aI (sk)ndeg O~ (sk)n
degaelig~m (sk)n
deg IhIn Aacute~n mouml~(sk)ndeg] passive processes and
[aI xO xaeligm xIkIIcirc AacuteIcirc goumlx] active processes
Contribution to surgical management decisions
Passiveactive interpretation of clinical assessments might facilitate surgical manage-ment decisions If noseholding does not facilitate correct production of targetconsonants then it is likely that an alternative articulatory pattern has becomephonologically established ie particular realizations for one or more targets areconsistently distributed in the phonological system These realizations may haveevolved because of initial diYculty producing articulatory targets and subsequentlystabilized within the phonological system Grundy and Harding (1995) refer to thisphenomenon as an lsquoarticulatory disorder with phonological consequencesrsquo
Therapy
Where obvious structural defects or diagnosed dysfunction exists clinicians fre-quently defer therapeutic intervention until surgery has been undertaken Theexpectation would be that normal structure and function is essential for normalspeech However pre-operative therapy may facilitate oral consonant productionwhich may serve to reduce hypernasal resonance Hence therapy prior to surgerymay avoid unnecessary surgery or reduce the extent of surgery required All activeprocesses are likely to require therapy
Principled selection of targets for therapy
Speech patterns frequently evidence a mixture of apparently passive and activeprocesses which complicates decisions about target selection Target selection can
A Harding and P Grunwell348
be based on assessment of which consonant targets can be most easily elicted inisolation (stimulability) This may lead to a sequence of target selection which isopposite to the sequence of consonant acquisition in normal development Forexample where reduced intra-oral pressure is present in a passive pattern [T] maybe easier to elicit in imitation than more nely grooved [s] or [S] Therapy maytarget [T] followed by [S ] and nally [s] As in non-cleft phonological therapywhere a class of consonants is aVected by the cleft then it is helpful to target theentire class The following decision-making process can be applied for both activeand passive processes
Decision making procedure for target selection
(1) Voiced versus voiceless targets(2) Front versus back placements(3) Syllable initial versus syllable nal targets(4) Plosives versus fricative targets
Voiceless plosives and fricatives are produced with an open glottis whichfacilitates topping up of air ow from the lungs hence voiceless plosive and fricativetargets are frequently more successful than voiced counterparts (Isshiki and Ringel1964) Front targets usually cause more diYculty than back particularly where analveolar defect or stula exists Contrary to normal development back targets maybe targeted before front Word- nal targets generally require less oral air pressurethan word initial targets and similarly fricatives may be more easily elicited thanplosives Fricatives do require a greater volume of air than plosives (Fletcher 1985)but in the presence of nasal escape weak fricative production appears to be morereadily achieved than weak plosive production Since nal fricatives would normallybe acquired in advance of word-initial fricatives (Ferguson 1978) targeting word- nal fricatives is frequently a productive starting point for therapy
Principles of therapy for passive processes
(1) Use of soft attack similar to gentle whisper for all target models ensuresminimal articulatory eVort (Harding and Grunwell 1993) and requires min-imal intra-oral air pressure It may be appropriate to gradually increase thearticulatory attack when the articulatory posture and evidence of intendedoral air ow have been established
(2) Slightly stretched duration of segment transitions in models of consonantto vowel (CndashV) or vowel to consonant (VndashC) facilitates review of motorplanning and extends the available time for execution of the new motorprogrammer whilst maintaining control of the oral airstream
(3) Noseholding can be used to provide exclusively oral air ow Gradual releaseof the nostrils during production of sustained [VVVVVf ] or [hhhhh ] allowsthe child to attempt to sustain an oral consonant despite increasing nasalemission This maximizes the use of available oral air ow Procedures forusing noseholding are described in some detail by Golding-Kushner (1995)
Principles of therapy for active processes
This is more like phonological therapy and can follow Grunwellrsquos (1991) processesfor phonological change and principled decision-making (Grunwell 1992) Some
Active versus passive cleft-type speech characteristics 349
examples are given here by way of illustration of ways to eVect the rst twoprocesses of change which may need to be approached diVerently in cleft palateversus non-cleft speech disorders DiVerent approaches may also be appropriate formodifying active versus passive cleft-type processes
Innovation production of new targets Some useful principles
(1) Introduction of new lsquonon-speech likersquo targets in sound play using a conson-ant sound segment model such as [ph ] note not a syllable like [p] whichis the type of pronunciation used when target sounds are presented as lettersfor reading Target [s] might be introduced as a lsquoTrain Slowing Down Noisersquo[ts ts ts tssssssss]
(2) lsquoNew consonantsrsquo can later be modelled and elicited in soft productions ofsyllable structure [tssssndashi] [ indashtssss] which can subsequently be identi ed assimilar to words lsquosearsquo and lsquoeatsrsquo
(3) lsquoDeferring responsibilityrsquo transfers responsibility or lsquoblamersquo for errors fromthe child and attributes it to the articulators eg lsquoyour tongue is havingtrouble with hellip rsquo lsquoLetrsquos show your tongue how to hellip rsquo
(4) New targets can be modelled repeatedly and recorded on audio or videotape which can be listened to at home
(5) Targeting classes of consonants (eg alveolars t d s n l voiceless fricativesf s S perhaps with aVricate T avoids phonological confusion whichmight occur if production ofsis achieved whilst other alveolar targetsremain backed The risk is that s might not integrate into the phonologicalsystem unless all backed alveolar consonants are destabilized
(6) Increased eye contact during auditory and production work can be invaluablein holding visual and auditory attention and ensures that visual informationabout the sound has been processed This is easily achieved by the clinicianlifting any focus of the childrsquos attention close to hisher mouth at theprecise moment when the target is modelled
Stimulation of non-speech related sounds such as a lsquoTrain Slowing DownNoisersquo [ts ts tsss] con rms that target [s] is physically achievable whether or not[ssss] can be imitated Some children continue to access [s] through the lsquoTrainSlowing Down Noisersquo throughout therapy until it is occurring spontaneouslywithout conscious planning This can be an eVective means of underminingestablished motor programmers (Hewlett 1990) for active cleft-type processes
Destabilizing active processes
As it is likely that children will be unaware of each occurrence of their alternativearticulatory pattern for speci c consonant errors it is preferrable to destabilizeactive processes with minimal conscious eVort by the child As children becomeaware of their mismatches they frequently add the newly acquired target realizationto their existing production eg target word tu childrsquos old realization [ku] childrsquoscorrected realization [t-ku] Destabilization can be achieved with minimal consciouseVort through input therapy techniques such as auditory bombardment (Lancasterand Pope 1989) auditory decision-making such as lsquowhich bear says this wordproperlyrsquo Red Bear says lsquotworsquo or Blue Bear says lsquocoorsquo This type of strategy oftenprecipitates attention to the target consonant with possible lsquoreplayrsquo and lsquoreviewrsquo of
A Harding and P Grunwell350
their own production Frequent stimulation of cognitive alertness to the targetconsonant can develop awareness without confronting the child with errors orrisking hisher failure The child is then free to attempt to repair hisher ownrealization to continue to re ect and to silently rehearse the adult realizationTraditional articulation therapy is thus combined with development of metaphonol-ogical skills ie the ability to re ect upon onersquos own speech production The resultshould be that new target realizations will be more phonologically stable thanexclusively production-based articulation therapy might have facilitated
Stabilizationgeneralization
Procedures to ensure stabilization and generalization of new target consonantswould be as described by Grunwell (1992) Success may be constrained by theconsiderable articulatory eVort sometimes required to maintain pressure consonantproduction in spontaneous speech (Harding and Grunwell 1993)
Conclusions
In speech assessment it is helpful to distinguish between errors which are cleft-type and non-cleft type and those which are part of active versus passive processesThe active and passive processes have been de ned and their phonological implica-tions discussed Focus on active and passive processes has facilitated focus on thephonological consequences of cleft palate on speech development In the futureawareness of the likely eVect of a cleft palate on normal phonological developmentcould avoid extended periods of unsuccessful clinical intervention Furthermoresensitivity to the relationship between phonological processes and structural con-straints should facilitate theoretically based management decisions Incidences suchas the case of CP in which nasal realizations were thought to indicate VPI but weresubsequently unaVected by surgery might be avoided if phonological analysiscontributes to management decisions
Surgery did improve hypernasal resonance and eliminated passive processes buthad little eVect on active processes Active processes in younger subjects werethought to require therapeutic intervention but in the longer term the oldersubjects showed few cleft-type processes Whilst it is possible that active cleft-typeprocesses may resolve with increasing age the implication for the future is thatactive cleft-type processes should be treated with skilled therapeutic interventionnot surgery Therapy which addresses the phonological consequences of cleft palateon speech development by combining metaphonologicalphonologicalarticulatoryapproaches is likely to be successful
References
Albery E 1991 Consonant articulation in the diVerent types of cleft lip and palate UnpublishedMPhil thesis Leicester Polytechnic
Albery E and Grunwell P 1993 Consonant articulation in diVerent types of cleft palate InP Grunwell (Ed) Analysing Cleft Palate Speech (London Whurr)
Ferguson C A 1978 Fricatives in child language acquisition In V Honsa and M Hardmann-Battista (Eds) Papers on Linguistics and Child Language (Mouton The Hague)
Fletcher S G 1985 Speech production and oral motor skill in an adult with an unrepaired palatalcleft Journal of Speech and Hearing Disorders 50 254ndash261
Active versus passive cleft-type speech characteristics 351
Golding-Kushner K J 1995 Treatment of articulation and resonancne disorders associated withcleft palate management and VPI In R Shprintzen (Ed) Cleft Palate Speech Management AMultidisciplinary Approach (St Louis Mosby)
Grundy K and Harding A 1995 Developmental speech disorders In K Grundy (Ed) Linguisticsin Clinical Practice (2nd edition) (London Whurr)
Grunwell P 1985 Phonological Assessment of Child Speech (Windsor NFER-Nelson)Grunwell P 1987a Clinical Phonology (2nd edition) (London Croom Helm)Grunwell P 1987b PACS Pictures Language Elicitation Materials (Windsor NFER-Nelson)Grunwell P 1991 Processes of phonological change in developmental speech disorders Clinical
Linguistics and Phonetics 6 101ndash122Grunwell P 1992 Principled decision making in the remediation of children with phonological
disorders In P Fletcher and D Hall (Eds) Specic Speech and Language Disorders in Children(London Whurr)
Grunwell P and Harding A 1995 PACSTOYS A Screening Assessment of Phonological Development(Windsor NFER-Nelson)
Grunwell P and Harding A 1996 A note on describing types of nasality Clinical Linguistics andPhonetics 10 157ndash161
Harding A 1993 An Investigation into the Relationship Between Timing of Cleft Palate Repairand Speech Development Unpublished PhD thesis
Harding A and Grunwell P 1993 The relationship between speech and timing of hard palaterepair In P Grunwell (Ed) Analysisng Cleft Palate Speech (London Whurr)
Harding A and Grunwell P 1996 Characteristics of cleft palate speech European Journal ofDisorders of Communication 31 331ndash358
Henningsson G and Isberg A M 1986 Velopharyngeal movement patterns in patients alternatingbetween oral and glottal articulation A clinical and cineradiographicical study Cleft Palate Journal23 1ndash9
Hewlett N 1990 Processes of development and production In P Grunwell (Ed) DevelopmentalSpeech Disorders (Edinburgh Churchill Livingstone)
Hotz M M Gnoinski W M Nussbaumer H and Kistler E 1978 Early orthopaedics in CLPcases guidelines for surgery Cleft Palate Journal 15 405ndash411
Hutters B and Brondsted K 1987 Strategies in cleft palate with special reference to DanishCleft Palate Journal 24 127ndash136
Isshiki N and Ringel R 1964 Airow during the production of selected consonants Journal ofSpeech and Hearing Research 7 233ndash244
Kummer A W Curtis C Wiggs M Lee L and Strife J L 1992 Comparison of velopharyngealgap size in patients with hypernasality hypernasality with nasal emission and nasal emissionor nasal turbulence (rustle) as the primary speech characteristic Cleft-palate-Craniofacial Journal29 152ndash156
Lancaster G and Pope L 1989 Working with Childrenrsquos Phonology (Oxford Winslow)Morley M E 1970 Cleft Palate and Speech (7th edition) (Edinburgh Churchill Livingstone)Russell V J 1991 Speech Development in Children with Cleft Lip and Palate Unpublished PhD
thesis Leicester PolytechnicRussell V J and Grunwell P 1993 Speech development in children with cleft lip and palate In
P Grunwell (Ed) Analysing Cleft Palate Speech (London Whurr)Sell D A and Grunwell P 1990 Speech results following late palatal surgery in previously
unoperated Sri Lankan adolescents with cleft palate Cleft Palate Journal 27 162ndash168Sell D Harding A and Grunwell P 1994 GOSSPASS A screening assessment of cleft palate
speech European Journal of Disorders of Communication 29 1ndash15Sell D Harding A and Grunwell P 1998 GOSSPASSrsquo98 An assessment for speech disorders
associated with cleft palate andor velopharyngeal dysfunction International Journal of Languageamp Communication Disorders ( in press)
Shorter E 1995 A spectographic analyis of child homophones Unpublished honours project DeMontfort University Leicester
Stenglehoffen J 1989 Nature and causes of communication diYculties In J Stengelhofen (Ed)Cleft Palate Nature and Remediation of Communication Problems (Edinburgh Churchill Livingstone)
Trost J E 1981 Articulatory additions to the classical description of the speech of persons withcleft palate Cleft Palate Journal 18
Trost-Cardamone J E 1990 The development of speech assessing cleft palate misarticulationsIn D A Kernahan and S N Rosenstein (Eds) Cleft Lip and Palate A System of Management(Baltimore Williams amp Wilkins)
A Harding and P Grunwell352
Appendix Active passive analysis of cleft palate speech

Active versus passive cleft-type speech characteristics 343
Tab
le5
EV
ects
ofso
ftp
alat
ere
pair
atag
e1
6on
BC
LP
subj
ects
h
ard
pal
ate
rem
ain
sun
repa
ired
2-st
age
subj
ects
Surg
ery
Pre
-ope
rati
vesp
eech
patt
ern
atag
e1
6Po
st-o
pera
tive
chan
ges
insp
eech
atag
e2
0
Stud
y1
BSo
ftpa
late
repa
irat
16
Adu
ltta
rget
sk
gA
t2
0[b
b kmg kb
td
g]D
Soft
pala
tere
pair
17
Adu
ltta
rget
sp
bk
gA
t2
0[p
bd
b kdk
g]
Tab
le6
EV
ects
ofha
rdpa
late
rep
air
atag
e6
6an
d
stu
lare
pair
atag
e10
0
Subj
ect
Surg
ery
Pre
-ope
rati
vesp
eech
patt
ern
Post
-ope
rati
vech
ange
sin
spee
ch
MS
Har
dpa
late
repa
ir6
6Pa
ssiv
epr
oces
s7
6E
limin
ated
pass
ive
proc
ess
Var
iabl
ena
sal
rele
ase
ofco
nson
ants
Hyp
onas
alna
sals
JFH
ard
pala
tere
pair
(uns
ucce
ssfu
l)6
6Se
vera
lac
tive
and
pass
ive
proc
esse
s7
6A
ctiv
epr
oces
ses
rem
aine
dPa
ssiv
epr
oces
ses
elim
inat
ed
DA
Fis
tula
repa
ir10
0A
ctiv
epr
oces
ses
110
Elim
inat
ion
ofph
aryn
geal
glo
ttal
Var
iabi
lity+
+an
dna
sal
arti
cula
tion
Art
icul
ator
yva
riab
ility
++
Act
ive
CT
Rs
proc
esse
spe
rsis
t
A Harding and P Grunwell344
palate repair but with a residual cleft in the hard palate his range of consonantsincluded [d] which was particularly surprising since the hard palate remainedunrepaired Whilst it is unlikely that toddlers of 18 months could be consciouslytrying to compensate for articulatory inadequacy in producing velar plosives inbabble prior to soft palate repair and an alveolar plosive prior to hard palate repairboth these subjects showed evidence of actively pursuing their articulatory potential
Table 6 summarizes changes following surgery to repair the hard palate in moremature speech patterns These subjects who were aged 66 and 100 pre-operativelyhad learned to speak with residual clefts and were apparently unaware of theconsonant productions that failed to match normal production
Subject MS used only passive processes in his speech pattern He realized someconsonants nasally such that lsquoballrsquo was [mO~] and lsquosockrsquo was [(sk)n
deg Aacute~ k] Looking atpost-operative changes at age 76 his consonant production was normal but hisresonance had become hyponasal Pre-operatively at age 66 Subject JF was usingseveral active and passive processes The active processes were unaVected by surgerybut passive processes were eliminated
Fistula repair was carried out at age 100 on Subject DA who had many activeprocesses and very variable articulation pre-operatively Post-operatively at age110 he was not using non-oral pharyngeal and glottal active processes or nasalrealizations but many oral cleft-type realizations remained
As shown in table 7 hard palate re-repair and pharyngoplasty was carried outon two subjects whose hard palate repairs had been unsuccessful at approximately4 years Subject NC assessed pre-operatively at age 56 was using predominantlypassive processes in her speech She was also using [ j] for fricatives s S whichwas thought to be an active process At age 60 following hard palate re-repair andpharyngoplasty all cleft-type processes had been eliminated without post-operativespeech therapy Since [ j] for s apparently resolved spontaneously followingsurgery it can be assumed that this was a passive process in this speech sample
Subject CP who underwent this procedure presented pre-operatively at age 46with both passive and active processes but his nasal resonance was not consistentlyhypernasal In addition to his cleft-related speech disorder this subject had additionaldevelopmental speech diYculties which were identi ed as being unrelated to thecleft Post-operatively at age 56 little had changedmdashnotably the passive processnasal [m] for b was retained His nasal resonance had become hyponasal andthere was no apparent bene t from surgical intervention The realization of b as[m] had become phonologically stable and surgery alone had not destabilized thephonological system This realization may have been a passive product of VPI inearly speech acquisition which had subsequently become part of a phonologicaldisorder Post-operatively CPrsquos phonetic repertoire did increase but the phonologicaldistribution was variable Plosive targets were still realized as nasals in spontaneousspeech at the nal speech recording at age 76 This was not as an inevitableconsequence of VPI but a result of an inability to destabilize the phonologicalprocess determining that voiced plosives would be realized as nasals This resultfollowing surgery highlights the importance of identifying phonological learningproblems and distinguishing them from structural constraints on articulationIn CPrsquos case pre-operative exploration of the eVect of nares occlusion duringspeech might have indicated that structural change would not improve consonantproduction spontaneously
A general observation was that consonant realizations did not move rapidly
Active versus passive cleft-type speech characteristics 345
Tab
le7
EV
ects
ofha
rdpa
late
re-r
epai
ran
dp
hary
ngo
pla
sty
Subj
ect
Surg
ery
Pre
-ope
rati
vesp
eech
patt
ern
Post
-ope
rativ
ech
ange
sin
spee
ch
Stud
y2
NC
Har
dpa
late
re-r
epai
ran
d5
6Pa
ssiv
ecl
eft-
type
proc
esse
s6
0A
llcl
eft-
type
phar
yngo
plas
ty5
10[
j]
for
fric
ativ
espr
oces
ses
elim
inat
ed[
h]
for
plos
ives
SIW
IV
aria
ble
arti
cula
rypr
ecis
ion
CP
Har
dpa
late
repa
iran
d4
6Pa
ssiv
ean
dac
tive
proc
esse
s5
6Pa
ssiv
epr
oces
sph
aryn
gopl
asty
50
Pho
nolo
gica
lco
nfus
ion
[m]
for
[b
]re
tain
edH
ypon
asal
nasa
lsPe
rsis
ting
phon
olog
ical
conf
usio
ns
A Harding and P Grunwell346
from incorrect to correct but progressed incrementally towards normal realizationsas described by Morley (1970) Where an early realization of target s might beglottal [h] a gradual pattern of change showed subsequent realizations to bepharyngeal [Eacute] then uvular [X] then velar [x] and eventually palatal [c] or lateral [Euml]It was interesting to note that speech patterns continued to change as late as90ndash110 years with the result that diVerences related to surgical timing and cleft-type gradually disappeared Persisting stulae were thought to account for the mostmarked cleft type processes at age 90
Implications for surgical management
This analysis of speech changes following surgery suggests some implications forsurgical management which are compatible with Sell and Grunwellrsquos (1990) ndingsin the Sri Lankan study
Surgery can change passive speech processes but it is also possible that speechtherapy may be able to change passive patterns Surgery alone is unlikely to modifyactive cleft-type processes whereas speech therapy should be able to modify activeprocesses Indications from these case studies is that where speech is the primaryproblem speech assessment should distinguish between active and passive processesin order to evaluate the necessity for full investigations and to plan therapeuticintervention Where past speech therapy has not been successful it cannot beassumed that surgical intervention will facilitate further speech progress A furthercourse of speech therapy which is sensitive to active versus passive processes todevelopmental phonological in uences on cleft-type speech development and toarticulatory diYculties in diVerent speech contexts might facilitate optimal progressWhere structural imperfection exists it is quite possible for single-word productionto be more precise than target realizations in spontaneous speech This may not bea failure of phonological generalization (Grunwell 1992) but the result of diYcultysustaining the necessary lsquoarticulatory eVort rsquo (Harding and Grunwell 1993) resultingin articulatory imprecision Deteriorating articulatory accuracy should not be over-looked in interpretation of speech results
An analytical protocol
As a result of analysing the speech data and identifying the active and passiveprocesses a protocol has been developed which records examples of each cleft-typeprocess over a series of assessments It demonstrates the progression of individualprocesses towards an adult target (see the Appendix) At each assessment onecolumn is used to indicate nasal resonance nasal emission and nasal turbulenceratings and cleft-type processes Changes in the nature of error realizations mightshow progress towards target consonants Hence whilst the total correct scoremight not have increased increments of change can be observed This observationof patterns of change may function as an adjunct to GOSSPASSrsquo98 (Sell et al 1998)giving access to a greater depth of both quantitative and qualitative data aboutconsonant production in relation to resonance nasal emission nasal turbulenceoral structure and cleft-type
Active versus passive cleft-type speech characteristics 347
Diagnostic implications
Passive versus active nasal fricatives
The important management consideration related to this distinction is that an activenasal fricative is an established phonological process which is unlikely to be directlyaVected by surgery alone Therapy would be necessary to destabilize nasal realizationsof oral consonants In contrast passive nasal fricatives may be eliminated by surgeryOf particular relevance is diVerential diagnosis between passive and active nasalfricatives in surgical and therapeutic management When hypernasality co-occurswith nasal air ow during consonant production which can be redirected by nose-holding passive nasal fricatives are diagnosed These would be transcribed as [(sk)n
deg]
passive alveolar nasal fricatives [(Wk)mdeg
] bilabial nasal fricatives or [(fk)Iacutedeg ] labiodentalnasal fricatives Full VPI investigations would be recommended to diagnose thenature of the structural or functional de ciency and distinguish between velopharyn-geal incompetence and velopharyngeal mislearning
It is highly likely that plosive targets would be aVected by reduced intra-oral airpressure such that plosives would either be realized by nasal counterparts eg bd[ [m n] or [b d] may be nasalized and weak Voiceless plosives may be eitheraccompanied by nasal emission [p t k] or realized as glottal fricative [h]
Production of the target sentence lsquoI saw Sam sitting on a busrsquo might be
[aI (sk)ndeg O~ (sk)n
degaelig~m (sk)n
deg IhIn Aacute~n mouml~(sk)ndeg] passive processes and
[aI xO xaeligm xIkIIcirc AacuteIcirc goumlx] active processes
Contribution to surgical management decisions
Passiveactive interpretation of clinical assessments might facilitate surgical manage-ment decisions If noseholding does not facilitate correct production of targetconsonants then it is likely that an alternative articulatory pattern has becomephonologically established ie particular realizations for one or more targets areconsistently distributed in the phonological system These realizations may haveevolved because of initial diYculty producing articulatory targets and subsequentlystabilized within the phonological system Grundy and Harding (1995) refer to thisphenomenon as an lsquoarticulatory disorder with phonological consequencesrsquo
Therapy
Where obvious structural defects or diagnosed dysfunction exists clinicians fre-quently defer therapeutic intervention until surgery has been undertaken Theexpectation would be that normal structure and function is essential for normalspeech However pre-operative therapy may facilitate oral consonant productionwhich may serve to reduce hypernasal resonance Hence therapy prior to surgerymay avoid unnecessary surgery or reduce the extent of surgery required All activeprocesses are likely to require therapy
Principled selection of targets for therapy
Speech patterns frequently evidence a mixture of apparently passive and activeprocesses which complicates decisions about target selection Target selection can
A Harding and P Grunwell348
be based on assessment of which consonant targets can be most easily elicted inisolation (stimulability) This may lead to a sequence of target selection which isopposite to the sequence of consonant acquisition in normal development Forexample where reduced intra-oral pressure is present in a passive pattern [T] maybe easier to elicit in imitation than more nely grooved [s] or [S] Therapy maytarget [T] followed by [S ] and nally [s] As in non-cleft phonological therapywhere a class of consonants is aVected by the cleft then it is helpful to target theentire class The following decision-making process can be applied for both activeand passive processes
Decision making procedure for target selection
(1) Voiced versus voiceless targets(2) Front versus back placements(3) Syllable initial versus syllable nal targets(4) Plosives versus fricative targets
Voiceless plosives and fricatives are produced with an open glottis whichfacilitates topping up of air ow from the lungs hence voiceless plosive and fricativetargets are frequently more successful than voiced counterparts (Isshiki and Ringel1964) Front targets usually cause more diYculty than back particularly where analveolar defect or stula exists Contrary to normal development back targets maybe targeted before front Word- nal targets generally require less oral air pressurethan word initial targets and similarly fricatives may be more easily elicited thanplosives Fricatives do require a greater volume of air than plosives (Fletcher 1985)but in the presence of nasal escape weak fricative production appears to be morereadily achieved than weak plosive production Since nal fricatives would normallybe acquired in advance of word-initial fricatives (Ferguson 1978) targeting word- nal fricatives is frequently a productive starting point for therapy
Principles of therapy for passive processes
(1) Use of soft attack similar to gentle whisper for all target models ensuresminimal articulatory eVort (Harding and Grunwell 1993) and requires min-imal intra-oral air pressure It may be appropriate to gradually increase thearticulatory attack when the articulatory posture and evidence of intendedoral air ow have been established
(2) Slightly stretched duration of segment transitions in models of consonantto vowel (CndashV) or vowel to consonant (VndashC) facilitates review of motorplanning and extends the available time for execution of the new motorprogrammer whilst maintaining control of the oral airstream
(3) Noseholding can be used to provide exclusively oral air ow Gradual releaseof the nostrils during production of sustained [VVVVVf ] or [hhhhh ] allowsthe child to attempt to sustain an oral consonant despite increasing nasalemission This maximizes the use of available oral air ow Procedures forusing noseholding are described in some detail by Golding-Kushner (1995)
Principles of therapy for active processes
This is more like phonological therapy and can follow Grunwellrsquos (1991) processesfor phonological change and principled decision-making (Grunwell 1992) Some
Active versus passive cleft-type speech characteristics 349
examples are given here by way of illustration of ways to eVect the rst twoprocesses of change which may need to be approached diVerently in cleft palateversus non-cleft speech disorders DiVerent approaches may also be appropriate formodifying active versus passive cleft-type processes
Innovation production of new targets Some useful principles
(1) Introduction of new lsquonon-speech likersquo targets in sound play using a conson-ant sound segment model such as [ph ] note not a syllable like [p] whichis the type of pronunciation used when target sounds are presented as lettersfor reading Target [s] might be introduced as a lsquoTrain Slowing Down Noisersquo[ts ts ts tssssssss]
(2) lsquoNew consonantsrsquo can later be modelled and elicited in soft productions ofsyllable structure [tssssndashi] [ indashtssss] which can subsequently be identi ed assimilar to words lsquosearsquo and lsquoeatsrsquo
(3) lsquoDeferring responsibilityrsquo transfers responsibility or lsquoblamersquo for errors fromthe child and attributes it to the articulators eg lsquoyour tongue is havingtrouble with hellip rsquo lsquoLetrsquos show your tongue how to hellip rsquo
(4) New targets can be modelled repeatedly and recorded on audio or videotape which can be listened to at home
(5) Targeting classes of consonants (eg alveolars t d s n l voiceless fricativesf s S perhaps with aVricate T avoids phonological confusion whichmight occur if production ofsis achieved whilst other alveolar targetsremain backed The risk is that s might not integrate into the phonologicalsystem unless all backed alveolar consonants are destabilized
(6) Increased eye contact during auditory and production work can be invaluablein holding visual and auditory attention and ensures that visual informationabout the sound has been processed This is easily achieved by the clinicianlifting any focus of the childrsquos attention close to hisher mouth at theprecise moment when the target is modelled
Stimulation of non-speech related sounds such as a lsquoTrain Slowing DownNoisersquo [ts ts tsss] con rms that target [s] is physically achievable whether or not[ssss] can be imitated Some children continue to access [s] through the lsquoTrainSlowing Down Noisersquo throughout therapy until it is occurring spontaneouslywithout conscious planning This can be an eVective means of underminingestablished motor programmers (Hewlett 1990) for active cleft-type processes
Destabilizing active processes
As it is likely that children will be unaware of each occurrence of their alternativearticulatory pattern for speci c consonant errors it is preferrable to destabilizeactive processes with minimal conscious eVort by the child As children becomeaware of their mismatches they frequently add the newly acquired target realizationto their existing production eg target word tu childrsquos old realization [ku] childrsquoscorrected realization [t-ku] Destabilization can be achieved with minimal consciouseVort through input therapy techniques such as auditory bombardment (Lancasterand Pope 1989) auditory decision-making such as lsquowhich bear says this wordproperlyrsquo Red Bear says lsquotworsquo or Blue Bear says lsquocoorsquo This type of strategy oftenprecipitates attention to the target consonant with possible lsquoreplayrsquo and lsquoreviewrsquo of
A Harding and P Grunwell350
their own production Frequent stimulation of cognitive alertness to the targetconsonant can develop awareness without confronting the child with errors orrisking hisher failure The child is then free to attempt to repair hisher ownrealization to continue to re ect and to silently rehearse the adult realizationTraditional articulation therapy is thus combined with development of metaphonol-ogical skills ie the ability to re ect upon onersquos own speech production The resultshould be that new target realizations will be more phonologically stable thanexclusively production-based articulation therapy might have facilitated
Stabilizationgeneralization
Procedures to ensure stabilization and generalization of new target consonantswould be as described by Grunwell (1992) Success may be constrained by theconsiderable articulatory eVort sometimes required to maintain pressure consonantproduction in spontaneous speech (Harding and Grunwell 1993)
Conclusions
In speech assessment it is helpful to distinguish between errors which are cleft-type and non-cleft type and those which are part of active versus passive processesThe active and passive processes have been de ned and their phonological implica-tions discussed Focus on active and passive processes has facilitated focus on thephonological consequences of cleft palate on speech development In the futureawareness of the likely eVect of a cleft palate on normal phonological developmentcould avoid extended periods of unsuccessful clinical intervention Furthermoresensitivity to the relationship between phonological processes and structural con-straints should facilitate theoretically based management decisions Incidences suchas the case of CP in which nasal realizations were thought to indicate VPI but weresubsequently unaVected by surgery might be avoided if phonological analysiscontributes to management decisions
Surgery did improve hypernasal resonance and eliminated passive processes buthad little eVect on active processes Active processes in younger subjects werethought to require therapeutic intervention but in the longer term the oldersubjects showed few cleft-type processes Whilst it is possible that active cleft-typeprocesses may resolve with increasing age the implication for the future is thatactive cleft-type processes should be treated with skilled therapeutic interventionnot surgery Therapy which addresses the phonological consequences of cleft palateon speech development by combining metaphonologicalphonologicalarticulatoryapproaches is likely to be successful
References
Albery E 1991 Consonant articulation in the diVerent types of cleft lip and palate UnpublishedMPhil thesis Leicester Polytechnic
Albery E and Grunwell P 1993 Consonant articulation in diVerent types of cleft palate InP Grunwell (Ed) Analysing Cleft Palate Speech (London Whurr)
Ferguson C A 1978 Fricatives in child language acquisition In V Honsa and M Hardmann-Battista (Eds) Papers on Linguistics and Child Language (Mouton The Hague)
Fletcher S G 1985 Speech production and oral motor skill in an adult with an unrepaired palatalcleft Journal of Speech and Hearing Disorders 50 254ndash261
Active versus passive cleft-type speech characteristics 351
Golding-Kushner K J 1995 Treatment of articulation and resonancne disorders associated withcleft palate management and VPI In R Shprintzen (Ed) Cleft Palate Speech Management AMultidisciplinary Approach (St Louis Mosby)
Grundy K and Harding A 1995 Developmental speech disorders In K Grundy (Ed) Linguisticsin Clinical Practice (2nd edition) (London Whurr)
Grunwell P 1985 Phonological Assessment of Child Speech (Windsor NFER-Nelson)Grunwell P 1987a Clinical Phonology (2nd edition) (London Croom Helm)Grunwell P 1987b PACS Pictures Language Elicitation Materials (Windsor NFER-Nelson)Grunwell P 1991 Processes of phonological change in developmental speech disorders Clinical
Linguistics and Phonetics 6 101ndash122Grunwell P 1992 Principled decision making in the remediation of children with phonological
disorders In P Fletcher and D Hall (Eds) Specic Speech and Language Disorders in Children(London Whurr)
Grunwell P and Harding A 1995 PACSTOYS A Screening Assessment of Phonological Development(Windsor NFER-Nelson)
Grunwell P and Harding A 1996 A note on describing types of nasality Clinical Linguistics andPhonetics 10 157ndash161
Harding A 1993 An Investigation into the Relationship Between Timing of Cleft Palate Repairand Speech Development Unpublished PhD thesis
Harding A and Grunwell P 1993 The relationship between speech and timing of hard palaterepair In P Grunwell (Ed) Analysisng Cleft Palate Speech (London Whurr)
Harding A and Grunwell P 1996 Characteristics of cleft palate speech European Journal ofDisorders of Communication 31 331ndash358
Henningsson G and Isberg A M 1986 Velopharyngeal movement patterns in patients alternatingbetween oral and glottal articulation A clinical and cineradiographicical study Cleft Palate Journal23 1ndash9
Hewlett N 1990 Processes of development and production In P Grunwell (Ed) DevelopmentalSpeech Disorders (Edinburgh Churchill Livingstone)
Hotz M M Gnoinski W M Nussbaumer H and Kistler E 1978 Early orthopaedics in CLPcases guidelines for surgery Cleft Palate Journal 15 405ndash411
Hutters B and Brondsted K 1987 Strategies in cleft palate with special reference to DanishCleft Palate Journal 24 127ndash136
Isshiki N and Ringel R 1964 Airow during the production of selected consonants Journal ofSpeech and Hearing Research 7 233ndash244
Kummer A W Curtis C Wiggs M Lee L and Strife J L 1992 Comparison of velopharyngealgap size in patients with hypernasality hypernasality with nasal emission and nasal emissionor nasal turbulence (rustle) as the primary speech characteristic Cleft-palate-Craniofacial Journal29 152ndash156
Lancaster G and Pope L 1989 Working with Childrenrsquos Phonology (Oxford Winslow)Morley M E 1970 Cleft Palate and Speech (7th edition) (Edinburgh Churchill Livingstone)Russell V J 1991 Speech Development in Children with Cleft Lip and Palate Unpublished PhD
thesis Leicester PolytechnicRussell V J and Grunwell P 1993 Speech development in children with cleft lip and palate In
P Grunwell (Ed) Analysing Cleft Palate Speech (London Whurr)Sell D A and Grunwell P 1990 Speech results following late palatal surgery in previously
unoperated Sri Lankan adolescents with cleft palate Cleft Palate Journal 27 162ndash168Sell D Harding A and Grunwell P 1994 GOSSPASS A screening assessment of cleft palate
speech European Journal of Disorders of Communication 29 1ndash15Sell D Harding A and Grunwell P 1998 GOSSPASSrsquo98 An assessment for speech disorders
associated with cleft palate andor velopharyngeal dysfunction International Journal of Languageamp Communication Disorders ( in press)
Shorter E 1995 A spectographic analyis of child homophones Unpublished honours project DeMontfort University Leicester
Stenglehoffen J 1989 Nature and causes of communication diYculties In J Stengelhofen (Ed)Cleft Palate Nature and Remediation of Communication Problems (Edinburgh Churchill Livingstone)
Trost J E 1981 Articulatory additions to the classical description of the speech of persons withcleft palate Cleft Palate Journal 18
Trost-Cardamone J E 1990 The development of speech assessing cleft palate misarticulationsIn D A Kernahan and S N Rosenstein (Eds) Cleft Lip and Palate A System of Management(Baltimore Williams amp Wilkins)
A Harding and P Grunwell352
Appendix Active passive analysis of cleft palate speech

A Harding and P Grunwell344
palate repair but with a residual cleft in the hard palate his range of consonantsincluded [d] which was particularly surprising since the hard palate remainedunrepaired Whilst it is unlikely that toddlers of 18 months could be consciouslytrying to compensate for articulatory inadequacy in producing velar plosives inbabble prior to soft palate repair and an alveolar plosive prior to hard palate repairboth these subjects showed evidence of actively pursuing their articulatory potential
Table 6 summarizes changes following surgery to repair the hard palate in moremature speech patterns These subjects who were aged 66 and 100 pre-operativelyhad learned to speak with residual clefts and were apparently unaware of theconsonant productions that failed to match normal production
Subject MS used only passive processes in his speech pattern He realized someconsonants nasally such that lsquoballrsquo was [mO~] and lsquosockrsquo was [(sk)n
deg Aacute~ k] Looking atpost-operative changes at age 76 his consonant production was normal but hisresonance had become hyponasal Pre-operatively at age 66 Subject JF was usingseveral active and passive processes The active processes were unaVected by surgerybut passive processes were eliminated
Fistula repair was carried out at age 100 on Subject DA who had many activeprocesses and very variable articulation pre-operatively Post-operatively at age110 he was not using non-oral pharyngeal and glottal active processes or nasalrealizations but many oral cleft-type realizations remained
As shown in table 7 hard palate re-repair and pharyngoplasty was carried outon two subjects whose hard palate repairs had been unsuccessful at approximately4 years Subject NC assessed pre-operatively at age 56 was using predominantlypassive processes in her speech She was also using [ j] for fricatives s S whichwas thought to be an active process At age 60 following hard palate re-repair andpharyngoplasty all cleft-type processes had been eliminated without post-operativespeech therapy Since [ j] for s apparently resolved spontaneously followingsurgery it can be assumed that this was a passive process in this speech sample
Subject CP who underwent this procedure presented pre-operatively at age 46with both passive and active processes but his nasal resonance was not consistentlyhypernasal In addition to his cleft-related speech disorder this subject had additionaldevelopmental speech diYculties which were identi ed as being unrelated to thecleft Post-operatively at age 56 little had changedmdashnotably the passive processnasal [m] for b was retained His nasal resonance had become hyponasal andthere was no apparent bene t from surgical intervention The realization of b as[m] had become phonologically stable and surgery alone had not destabilized thephonological system This realization may have been a passive product of VPI inearly speech acquisition which had subsequently become part of a phonologicaldisorder Post-operatively CPrsquos phonetic repertoire did increase but the phonologicaldistribution was variable Plosive targets were still realized as nasals in spontaneousspeech at the nal speech recording at age 76 This was not as an inevitableconsequence of VPI but a result of an inability to destabilize the phonologicalprocess determining that voiced plosives would be realized as nasals This resultfollowing surgery highlights the importance of identifying phonological learningproblems and distinguishing them from structural constraints on articulationIn CPrsquos case pre-operative exploration of the eVect of nares occlusion duringspeech might have indicated that structural change would not improve consonantproduction spontaneously
A general observation was that consonant realizations did not move rapidly
Active versus passive cleft-type speech characteristics 345
Tab
le7
EV
ects
ofha
rdpa
late
re-r
epai
ran
dp
hary
ngo
pla
sty
Subj
ect
Surg
ery
Pre
-ope
rati
vesp
eech
patt
ern
Post
-ope
rativ
ech
ange
sin
spee
ch
Stud
y2
NC
Har
dpa
late
re-r
epai
ran
d5
6Pa
ssiv
ecl
eft-
type
proc
esse
s6
0A
llcl
eft-
type
phar
yngo
plas
ty5
10[
j]
for
fric
ativ
espr
oces
ses
elim
inat
ed[
h]
for
plos
ives
SIW
IV
aria
ble
arti
cula
rypr
ecis
ion
CP
Har
dpa
late
repa
iran
d4
6Pa
ssiv
ean
dac
tive
proc
esse
s5
6Pa
ssiv
epr
oces
sph
aryn
gopl
asty
50
Pho
nolo
gica
lco
nfus
ion
[m]
for
[b
]re
tain
edH
ypon
asal
nasa
lsPe
rsis
ting
phon
olog
ical
conf
usio
ns
A Harding and P Grunwell346
from incorrect to correct but progressed incrementally towards normal realizationsas described by Morley (1970) Where an early realization of target s might beglottal [h] a gradual pattern of change showed subsequent realizations to bepharyngeal [Eacute] then uvular [X] then velar [x] and eventually palatal [c] or lateral [Euml]It was interesting to note that speech patterns continued to change as late as90ndash110 years with the result that diVerences related to surgical timing and cleft-type gradually disappeared Persisting stulae were thought to account for the mostmarked cleft type processes at age 90
Implications for surgical management
This analysis of speech changes following surgery suggests some implications forsurgical management which are compatible with Sell and Grunwellrsquos (1990) ndingsin the Sri Lankan study
Surgery can change passive speech processes but it is also possible that speechtherapy may be able to change passive patterns Surgery alone is unlikely to modifyactive cleft-type processes whereas speech therapy should be able to modify activeprocesses Indications from these case studies is that where speech is the primaryproblem speech assessment should distinguish between active and passive processesin order to evaluate the necessity for full investigations and to plan therapeuticintervention Where past speech therapy has not been successful it cannot beassumed that surgical intervention will facilitate further speech progress A furthercourse of speech therapy which is sensitive to active versus passive processes todevelopmental phonological in uences on cleft-type speech development and toarticulatory diYculties in diVerent speech contexts might facilitate optimal progressWhere structural imperfection exists it is quite possible for single-word productionto be more precise than target realizations in spontaneous speech This may not bea failure of phonological generalization (Grunwell 1992) but the result of diYcultysustaining the necessary lsquoarticulatory eVort rsquo (Harding and Grunwell 1993) resultingin articulatory imprecision Deteriorating articulatory accuracy should not be over-looked in interpretation of speech results
An analytical protocol
As a result of analysing the speech data and identifying the active and passiveprocesses a protocol has been developed which records examples of each cleft-typeprocess over a series of assessments It demonstrates the progression of individualprocesses towards an adult target (see the Appendix) At each assessment onecolumn is used to indicate nasal resonance nasal emission and nasal turbulenceratings and cleft-type processes Changes in the nature of error realizations mightshow progress towards target consonants Hence whilst the total correct scoremight not have increased increments of change can be observed This observationof patterns of change may function as an adjunct to GOSSPASSrsquo98 (Sell et al 1998)giving access to a greater depth of both quantitative and qualitative data aboutconsonant production in relation to resonance nasal emission nasal turbulenceoral structure and cleft-type
Active versus passive cleft-type speech characteristics 347
Diagnostic implications
Passive versus active nasal fricatives
The important management consideration related to this distinction is that an activenasal fricative is an established phonological process which is unlikely to be directlyaVected by surgery alone Therapy would be necessary to destabilize nasal realizationsof oral consonants In contrast passive nasal fricatives may be eliminated by surgeryOf particular relevance is diVerential diagnosis between passive and active nasalfricatives in surgical and therapeutic management When hypernasality co-occurswith nasal air ow during consonant production which can be redirected by nose-holding passive nasal fricatives are diagnosed These would be transcribed as [(sk)n
deg]
passive alveolar nasal fricatives [(Wk)mdeg
] bilabial nasal fricatives or [(fk)Iacutedeg ] labiodentalnasal fricatives Full VPI investigations would be recommended to diagnose thenature of the structural or functional de ciency and distinguish between velopharyn-geal incompetence and velopharyngeal mislearning
It is highly likely that plosive targets would be aVected by reduced intra-oral airpressure such that plosives would either be realized by nasal counterparts eg bd[ [m n] or [b d] may be nasalized and weak Voiceless plosives may be eitheraccompanied by nasal emission [p t k] or realized as glottal fricative [h]
Production of the target sentence lsquoI saw Sam sitting on a busrsquo might be
[aI (sk)ndeg O~ (sk)n
degaelig~m (sk)n
deg IhIn Aacute~n mouml~(sk)ndeg] passive processes and
[aI xO xaeligm xIkIIcirc AacuteIcirc goumlx] active processes
Contribution to surgical management decisions
Passiveactive interpretation of clinical assessments might facilitate surgical manage-ment decisions If noseholding does not facilitate correct production of targetconsonants then it is likely that an alternative articulatory pattern has becomephonologically established ie particular realizations for one or more targets areconsistently distributed in the phonological system These realizations may haveevolved because of initial diYculty producing articulatory targets and subsequentlystabilized within the phonological system Grundy and Harding (1995) refer to thisphenomenon as an lsquoarticulatory disorder with phonological consequencesrsquo
Therapy
Where obvious structural defects or diagnosed dysfunction exists clinicians fre-quently defer therapeutic intervention until surgery has been undertaken Theexpectation would be that normal structure and function is essential for normalspeech However pre-operative therapy may facilitate oral consonant productionwhich may serve to reduce hypernasal resonance Hence therapy prior to surgerymay avoid unnecessary surgery or reduce the extent of surgery required All activeprocesses are likely to require therapy
Principled selection of targets for therapy
Speech patterns frequently evidence a mixture of apparently passive and activeprocesses which complicates decisions about target selection Target selection can
A Harding and P Grunwell348
be based on assessment of which consonant targets can be most easily elicted inisolation (stimulability) This may lead to a sequence of target selection which isopposite to the sequence of consonant acquisition in normal development Forexample where reduced intra-oral pressure is present in a passive pattern [T] maybe easier to elicit in imitation than more nely grooved [s] or [S] Therapy maytarget [T] followed by [S ] and nally [s] As in non-cleft phonological therapywhere a class of consonants is aVected by the cleft then it is helpful to target theentire class The following decision-making process can be applied for both activeand passive processes
Decision making procedure for target selection
(1) Voiced versus voiceless targets(2) Front versus back placements(3) Syllable initial versus syllable nal targets(4) Plosives versus fricative targets
Voiceless plosives and fricatives are produced with an open glottis whichfacilitates topping up of air ow from the lungs hence voiceless plosive and fricativetargets are frequently more successful than voiced counterparts (Isshiki and Ringel1964) Front targets usually cause more diYculty than back particularly where analveolar defect or stula exists Contrary to normal development back targets maybe targeted before front Word- nal targets generally require less oral air pressurethan word initial targets and similarly fricatives may be more easily elicited thanplosives Fricatives do require a greater volume of air than plosives (Fletcher 1985)but in the presence of nasal escape weak fricative production appears to be morereadily achieved than weak plosive production Since nal fricatives would normallybe acquired in advance of word-initial fricatives (Ferguson 1978) targeting word- nal fricatives is frequently a productive starting point for therapy
Principles of therapy for passive processes
(1) Use of soft attack similar to gentle whisper for all target models ensuresminimal articulatory eVort (Harding and Grunwell 1993) and requires min-imal intra-oral air pressure It may be appropriate to gradually increase thearticulatory attack when the articulatory posture and evidence of intendedoral air ow have been established
(2) Slightly stretched duration of segment transitions in models of consonantto vowel (CndashV) or vowel to consonant (VndashC) facilitates review of motorplanning and extends the available time for execution of the new motorprogrammer whilst maintaining control of the oral airstream
(3) Noseholding can be used to provide exclusively oral air ow Gradual releaseof the nostrils during production of sustained [VVVVVf ] or [hhhhh ] allowsthe child to attempt to sustain an oral consonant despite increasing nasalemission This maximizes the use of available oral air ow Procedures forusing noseholding are described in some detail by Golding-Kushner (1995)
Principles of therapy for active processes
This is more like phonological therapy and can follow Grunwellrsquos (1991) processesfor phonological change and principled decision-making (Grunwell 1992) Some
Active versus passive cleft-type speech characteristics 349
examples are given here by way of illustration of ways to eVect the rst twoprocesses of change which may need to be approached diVerently in cleft palateversus non-cleft speech disorders DiVerent approaches may also be appropriate formodifying active versus passive cleft-type processes
Innovation production of new targets Some useful principles
(1) Introduction of new lsquonon-speech likersquo targets in sound play using a conson-ant sound segment model such as [ph ] note not a syllable like [p] whichis the type of pronunciation used when target sounds are presented as lettersfor reading Target [s] might be introduced as a lsquoTrain Slowing Down Noisersquo[ts ts ts tssssssss]
(2) lsquoNew consonantsrsquo can later be modelled and elicited in soft productions ofsyllable structure [tssssndashi] [ indashtssss] which can subsequently be identi ed assimilar to words lsquosearsquo and lsquoeatsrsquo
(3) lsquoDeferring responsibilityrsquo transfers responsibility or lsquoblamersquo for errors fromthe child and attributes it to the articulators eg lsquoyour tongue is havingtrouble with hellip rsquo lsquoLetrsquos show your tongue how to hellip rsquo
(4) New targets can be modelled repeatedly and recorded on audio or videotape which can be listened to at home
(5) Targeting classes of consonants (eg alveolars t d s n l voiceless fricativesf s S perhaps with aVricate T avoids phonological confusion whichmight occur if production ofsis achieved whilst other alveolar targetsremain backed The risk is that s might not integrate into the phonologicalsystem unless all backed alveolar consonants are destabilized
(6) Increased eye contact during auditory and production work can be invaluablein holding visual and auditory attention and ensures that visual informationabout the sound has been processed This is easily achieved by the clinicianlifting any focus of the childrsquos attention close to hisher mouth at theprecise moment when the target is modelled
Stimulation of non-speech related sounds such as a lsquoTrain Slowing DownNoisersquo [ts ts tsss] con rms that target [s] is physically achievable whether or not[ssss] can be imitated Some children continue to access [s] through the lsquoTrainSlowing Down Noisersquo throughout therapy until it is occurring spontaneouslywithout conscious planning This can be an eVective means of underminingestablished motor programmers (Hewlett 1990) for active cleft-type processes
Destabilizing active processes
As it is likely that children will be unaware of each occurrence of their alternativearticulatory pattern for speci c consonant errors it is preferrable to destabilizeactive processes with minimal conscious eVort by the child As children becomeaware of their mismatches they frequently add the newly acquired target realizationto their existing production eg target word tu childrsquos old realization [ku] childrsquoscorrected realization [t-ku] Destabilization can be achieved with minimal consciouseVort through input therapy techniques such as auditory bombardment (Lancasterand Pope 1989) auditory decision-making such as lsquowhich bear says this wordproperlyrsquo Red Bear says lsquotworsquo or Blue Bear says lsquocoorsquo This type of strategy oftenprecipitates attention to the target consonant with possible lsquoreplayrsquo and lsquoreviewrsquo of
A Harding and P Grunwell350
their own production Frequent stimulation of cognitive alertness to the targetconsonant can develop awareness without confronting the child with errors orrisking hisher failure The child is then free to attempt to repair hisher ownrealization to continue to re ect and to silently rehearse the adult realizationTraditional articulation therapy is thus combined with development of metaphonol-ogical skills ie the ability to re ect upon onersquos own speech production The resultshould be that new target realizations will be more phonologically stable thanexclusively production-based articulation therapy might have facilitated
Stabilizationgeneralization
Procedures to ensure stabilization and generalization of new target consonantswould be as described by Grunwell (1992) Success may be constrained by theconsiderable articulatory eVort sometimes required to maintain pressure consonantproduction in spontaneous speech (Harding and Grunwell 1993)
Conclusions
In speech assessment it is helpful to distinguish between errors which are cleft-type and non-cleft type and those which are part of active versus passive processesThe active and passive processes have been de ned and their phonological implica-tions discussed Focus on active and passive processes has facilitated focus on thephonological consequences of cleft palate on speech development In the futureawareness of the likely eVect of a cleft palate on normal phonological developmentcould avoid extended periods of unsuccessful clinical intervention Furthermoresensitivity to the relationship between phonological processes and structural con-straints should facilitate theoretically based management decisions Incidences suchas the case of CP in which nasal realizations were thought to indicate VPI but weresubsequently unaVected by surgery might be avoided if phonological analysiscontributes to management decisions
Surgery did improve hypernasal resonance and eliminated passive processes buthad little eVect on active processes Active processes in younger subjects werethought to require therapeutic intervention but in the longer term the oldersubjects showed few cleft-type processes Whilst it is possible that active cleft-typeprocesses may resolve with increasing age the implication for the future is thatactive cleft-type processes should be treated with skilled therapeutic interventionnot surgery Therapy which addresses the phonological consequences of cleft palateon speech development by combining metaphonologicalphonologicalarticulatoryapproaches is likely to be successful
References
Albery E 1991 Consonant articulation in the diVerent types of cleft lip and palate UnpublishedMPhil thesis Leicester Polytechnic
Albery E and Grunwell P 1993 Consonant articulation in diVerent types of cleft palate InP Grunwell (Ed) Analysing Cleft Palate Speech (London Whurr)
Ferguson C A 1978 Fricatives in child language acquisition In V Honsa and M Hardmann-Battista (Eds) Papers on Linguistics and Child Language (Mouton The Hague)
Fletcher S G 1985 Speech production and oral motor skill in an adult with an unrepaired palatalcleft Journal of Speech and Hearing Disorders 50 254ndash261
Active versus passive cleft-type speech characteristics 351
Golding-Kushner K J 1995 Treatment of articulation and resonancne disorders associated withcleft palate management and VPI In R Shprintzen (Ed) Cleft Palate Speech Management AMultidisciplinary Approach (St Louis Mosby)
Grundy K and Harding A 1995 Developmental speech disorders In K Grundy (Ed) Linguisticsin Clinical Practice (2nd edition) (London Whurr)
Grunwell P 1985 Phonological Assessment of Child Speech (Windsor NFER-Nelson)Grunwell P 1987a Clinical Phonology (2nd edition) (London Croom Helm)Grunwell P 1987b PACS Pictures Language Elicitation Materials (Windsor NFER-Nelson)Grunwell P 1991 Processes of phonological change in developmental speech disorders Clinical
Linguistics and Phonetics 6 101ndash122Grunwell P 1992 Principled decision making in the remediation of children with phonological
disorders In P Fletcher and D Hall (Eds) Specic Speech and Language Disorders in Children(London Whurr)
Grunwell P and Harding A 1995 PACSTOYS A Screening Assessment of Phonological Development(Windsor NFER-Nelson)
Grunwell P and Harding A 1996 A note on describing types of nasality Clinical Linguistics andPhonetics 10 157ndash161
Harding A 1993 An Investigation into the Relationship Between Timing of Cleft Palate Repairand Speech Development Unpublished PhD thesis
Harding A and Grunwell P 1993 The relationship between speech and timing of hard palaterepair In P Grunwell (Ed) Analysisng Cleft Palate Speech (London Whurr)
Harding A and Grunwell P 1996 Characteristics of cleft palate speech European Journal ofDisorders of Communication 31 331ndash358
Henningsson G and Isberg A M 1986 Velopharyngeal movement patterns in patients alternatingbetween oral and glottal articulation A clinical and cineradiographicical study Cleft Palate Journal23 1ndash9
Hewlett N 1990 Processes of development and production In P Grunwell (Ed) DevelopmentalSpeech Disorders (Edinburgh Churchill Livingstone)
Hotz M M Gnoinski W M Nussbaumer H and Kistler E 1978 Early orthopaedics in CLPcases guidelines for surgery Cleft Palate Journal 15 405ndash411
Hutters B and Brondsted K 1987 Strategies in cleft palate with special reference to DanishCleft Palate Journal 24 127ndash136
Isshiki N and Ringel R 1964 Airow during the production of selected consonants Journal ofSpeech and Hearing Research 7 233ndash244
Kummer A W Curtis C Wiggs M Lee L and Strife J L 1992 Comparison of velopharyngealgap size in patients with hypernasality hypernasality with nasal emission and nasal emissionor nasal turbulence (rustle) as the primary speech characteristic Cleft-palate-Craniofacial Journal29 152ndash156
Lancaster G and Pope L 1989 Working with Childrenrsquos Phonology (Oxford Winslow)Morley M E 1970 Cleft Palate and Speech (7th edition) (Edinburgh Churchill Livingstone)Russell V J 1991 Speech Development in Children with Cleft Lip and Palate Unpublished PhD
thesis Leicester PolytechnicRussell V J and Grunwell P 1993 Speech development in children with cleft lip and palate In
P Grunwell (Ed) Analysing Cleft Palate Speech (London Whurr)Sell D A and Grunwell P 1990 Speech results following late palatal surgery in previously
unoperated Sri Lankan adolescents with cleft palate Cleft Palate Journal 27 162ndash168Sell D Harding A and Grunwell P 1994 GOSSPASS A screening assessment of cleft palate
speech European Journal of Disorders of Communication 29 1ndash15Sell D Harding A and Grunwell P 1998 GOSSPASSrsquo98 An assessment for speech disorders
associated with cleft palate andor velopharyngeal dysfunction International Journal of Languageamp Communication Disorders ( in press)
Shorter E 1995 A spectographic analyis of child homophones Unpublished honours project DeMontfort University Leicester
Stenglehoffen J 1989 Nature and causes of communication diYculties In J Stengelhofen (Ed)Cleft Palate Nature and Remediation of Communication Problems (Edinburgh Churchill Livingstone)
Trost J E 1981 Articulatory additions to the classical description of the speech of persons withcleft palate Cleft Palate Journal 18
Trost-Cardamone J E 1990 The development of speech assessing cleft palate misarticulationsIn D A Kernahan and S N Rosenstein (Eds) Cleft Lip and Palate A System of Management(Baltimore Williams amp Wilkins)
A Harding and P Grunwell352
Appendix Active passive analysis of cleft palate speech

Active versus passive cleft-type speech characteristics 345
Tab
le7
EV
ects
ofha
rdpa
late
re-r
epai
ran
dp
hary
ngo
pla
sty
Subj
ect
Surg
ery
Pre
-ope
rati
vesp
eech
patt
ern
Post
-ope
rativ
ech
ange
sin
spee
ch
Stud
y2
NC
Har
dpa
late
re-r
epai
ran
d5
6Pa
ssiv
ecl
eft-
type
proc
esse
s6
0A
llcl
eft-
type
phar
yngo
plas
ty5
10[
j]
for
fric
ativ
espr
oces
ses
elim
inat
ed[
h]
for
plos
ives
SIW
IV
aria
ble
arti
cula
rypr
ecis
ion
CP
Har
dpa
late
repa
iran
d4
6Pa
ssiv
ean
dac
tive
proc
esse
s5
6Pa
ssiv
epr
oces
sph
aryn
gopl
asty
50
Pho
nolo
gica
lco
nfus
ion
[m]
for
[b
]re
tain
edH
ypon
asal
nasa
lsPe
rsis
ting
phon
olog
ical
conf
usio
ns
A Harding and P Grunwell346
from incorrect to correct but progressed incrementally towards normal realizationsas described by Morley (1970) Where an early realization of target s might beglottal [h] a gradual pattern of change showed subsequent realizations to bepharyngeal [Eacute] then uvular [X] then velar [x] and eventually palatal [c] or lateral [Euml]It was interesting to note that speech patterns continued to change as late as90ndash110 years with the result that diVerences related to surgical timing and cleft-type gradually disappeared Persisting stulae were thought to account for the mostmarked cleft type processes at age 90
Implications for surgical management
This analysis of speech changes following surgery suggests some implications forsurgical management which are compatible with Sell and Grunwellrsquos (1990) ndingsin the Sri Lankan study
Surgery can change passive speech processes but it is also possible that speechtherapy may be able to change passive patterns Surgery alone is unlikely to modifyactive cleft-type processes whereas speech therapy should be able to modify activeprocesses Indications from these case studies is that where speech is the primaryproblem speech assessment should distinguish between active and passive processesin order to evaluate the necessity for full investigations and to plan therapeuticintervention Where past speech therapy has not been successful it cannot beassumed that surgical intervention will facilitate further speech progress A furthercourse of speech therapy which is sensitive to active versus passive processes todevelopmental phonological in uences on cleft-type speech development and toarticulatory diYculties in diVerent speech contexts might facilitate optimal progressWhere structural imperfection exists it is quite possible for single-word productionto be more precise than target realizations in spontaneous speech This may not bea failure of phonological generalization (Grunwell 1992) but the result of diYcultysustaining the necessary lsquoarticulatory eVort rsquo (Harding and Grunwell 1993) resultingin articulatory imprecision Deteriorating articulatory accuracy should not be over-looked in interpretation of speech results
An analytical protocol
As a result of analysing the speech data and identifying the active and passiveprocesses a protocol has been developed which records examples of each cleft-typeprocess over a series of assessments It demonstrates the progression of individualprocesses towards an adult target (see the Appendix) At each assessment onecolumn is used to indicate nasal resonance nasal emission and nasal turbulenceratings and cleft-type processes Changes in the nature of error realizations mightshow progress towards target consonants Hence whilst the total correct scoremight not have increased increments of change can be observed This observationof patterns of change may function as an adjunct to GOSSPASSrsquo98 (Sell et al 1998)giving access to a greater depth of both quantitative and qualitative data aboutconsonant production in relation to resonance nasal emission nasal turbulenceoral structure and cleft-type
Active versus passive cleft-type speech characteristics 347
Diagnostic implications
Passive versus active nasal fricatives
The important management consideration related to this distinction is that an activenasal fricative is an established phonological process which is unlikely to be directlyaVected by surgery alone Therapy would be necessary to destabilize nasal realizationsof oral consonants In contrast passive nasal fricatives may be eliminated by surgeryOf particular relevance is diVerential diagnosis between passive and active nasalfricatives in surgical and therapeutic management When hypernasality co-occurswith nasal air ow during consonant production which can be redirected by nose-holding passive nasal fricatives are diagnosed These would be transcribed as [(sk)n
deg]
passive alveolar nasal fricatives [(Wk)mdeg
] bilabial nasal fricatives or [(fk)Iacutedeg ] labiodentalnasal fricatives Full VPI investigations would be recommended to diagnose thenature of the structural or functional de ciency and distinguish between velopharyn-geal incompetence and velopharyngeal mislearning
It is highly likely that plosive targets would be aVected by reduced intra-oral airpressure such that plosives would either be realized by nasal counterparts eg bd[ [m n] or [b d] may be nasalized and weak Voiceless plosives may be eitheraccompanied by nasal emission [p t k] or realized as glottal fricative [h]
Production of the target sentence lsquoI saw Sam sitting on a busrsquo might be
[aI (sk)ndeg O~ (sk)n
degaelig~m (sk)n
deg IhIn Aacute~n mouml~(sk)ndeg] passive processes and
[aI xO xaeligm xIkIIcirc AacuteIcirc goumlx] active processes
Contribution to surgical management decisions
Passiveactive interpretation of clinical assessments might facilitate surgical manage-ment decisions If noseholding does not facilitate correct production of targetconsonants then it is likely that an alternative articulatory pattern has becomephonologically established ie particular realizations for one or more targets areconsistently distributed in the phonological system These realizations may haveevolved because of initial diYculty producing articulatory targets and subsequentlystabilized within the phonological system Grundy and Harding (1995) refer to thisphenomenon as an lsquoarticulatory disorder with phonological consequencesrsquo
Therapy
Where obvious structural defects or diagnosed dysfunction exists clinicians fre-quently defer therapeutic intervention until surgery has been undertaken Theexpectation would be that normal structure and function is essential for normalspeech However pre-operative therapy may facilitate oral consonant productionwhich may serve to reduce hypernasal resonance Hence therapy prior to surgerymay avoid unnecessary surgery or reduce the extent of surgery required All activeprocesses are likely to require therapy
Principled selection of targets for therapy
Speech patterns frequently evidence a mixture of apparently passive and activeprocesses which complicates decisions about target selection Target selection can
A Harding and P Grunwell348
be based on assessment of which consonant targets can be most easily elicted inisolation (stimulability) This may lead to a sequence of target selection which isopposite to the sequence of consonant acquisition in normal development Forexample where reduced intra-oral pressure is present in a passive pattern [T] maybe easier to elicit in imitation than more nely grooved [s] or [S] Therapy maytarget [T] followed by [S ] and nally [s] As in non-cleft phonological therapywhere a class of consonants is aVected by the cleft then it is helpful to target theentire class The following decision-making process can be applied for both activeand passive processes
Decision making procedure for target selection
(1) Voiced versus voiceless targets(2) Front versus back placements(3) Syllable initial versus syllable nal targets(4) Plosives versus fricative targets
Voiceless plosives and fricatives are produced with an open glottis whichfacilitates topping up of air ow from the lungs hence voiceless plosive and fricativetargets are frequently more successful than voiced counterparts (Isshiki and Ringel1964) Front targets usually cause more diYculty than back particularly where analveolar defect or stula exists Contrary to normal development back targets maybe targeted before front Word- nal targets generally require less oral air pressurethan word initial targets and similarly fricatives may be more easily elicited thanplosives Fricatives do require a greater volume of air than plosives (Fletcher 1985)but in the presence of nasal escape weak fricative production appears to be morereadily achieved than weak plosive production Since nal fricatives would normallybe acquired in advance of word-initial fricatives (Ferguson 1978) targeting word- nal fricatives is frequently a productive starting point for therapy
Principles of therapy for passive processes
(1) Use of soft attack similar to gentle whisper for all target models ensuresminimal articulatory eVort (Harding and Grunwell 1993) and requires min-imal intra-oral air pressure It may be appropriate to gradually increase thearticulatory attack when the articulatory posture and evidence of intendedoral air ow have been established
(2) Slightly stretched duration of segment transitions in models of consonantto vowel (CndashV) or vowel to consonant (VndashC) facilitates review of motorplanning and extends the available time for execution of the new motorprogrammer whilst maintaining control of the oral airstream
(3) Noseholding can be used to provide exclusively oral air ow Gradual releaseof the nostrils during production of sustained [VVVVVf ] or [hhhhh ] allowsthe child to attempt to sustain an oral consonant despite increasing nasalemission This maximizes the use of available oral air ow Procedures forusing noseholding are described in some detail by Golding-Kushner (1995)
Principles of therapy for active processes
This is more like phonological therapy and can follow Grunwellrsquos (1991) processesfor phonological change and principled decision-making (Grunwell 1992) Some
Active versus passive cleft-type speech characteristics 349
examples are given here by way of illustration of ways to eVect the rst twoprocesses of change which may need to be approached diVerently in cleft palateversus non-cleft speech disorders DiVerent approaches may also be appropriate formodifying active versus passive cleft-type processes
Innovation production of new targets Some useful principles
(1) Introduction of new lsquonon-speech likersquo targets in sound play using a conson-ant sound segment model such as [ph ] note not a syllable like [p] whichis the type of pronunciation used when target sounds are presented as lettersfor reading Target [s] might be introduced as a lsquoTrain Slowing Down Noisersquo[ts ts ts tssssssss]
(2) lsquoNew consonantsrsquo can later be modelled and elicited in soft productions ofsyllable structure [tssssndashi] [ indashtssss] which can subsequently be identi ed assimilar to words lsquosearsquo and lsquoeatsrsquo
(3) lsquoDeferring responsibilityrsquo transfers responsibility or lsquoblamersquo for errors fromthe child and attributes it to the articulators eg lsquoyour tongue is havingtrouble with hellip rsquo lsquoLetrsquos show your tongue how to hellip rsquo
(4) New targets can be modelled repeatedly and recorded on audio or videotape which can be listened to at home
(5) Targeting classes of consonants (eg alveolars t d s n l voiceless fricativesf s S perhaps with aVricate T avoids phonological confusion whichmight occur if production ofsis achieved whilst other alveolar targetsremain backed The risk is that s might not integrate into the phonologicalsystem unless all backed alveolar consonants are destabilized
(6) Increased eye contact during auditory and production work can be invaluablein holding visual and auditory attention and ensures that visual informationabout the sound has been processed This is easily achieved by the clinicianlifting any focus of the childrsquos attention close to hisher mouth at theprecise moment when the target is modelled
Stimulation of non-speech related sounds such as a lsquoTrain Slowing DownNoisersquo [ts ts tsss] con rms that target [s] is physically achievable whether or not[ssss] can be imitated Some children continue to access [s] through the lsquoTrainSlowing Down Noisersquo throughout therapy until it is occurring spontaneouslywithout conscious planning This can be an eVective means of underminingestablished motor programmers (Hewlett 1990) for active cleft-type processes
Destabilizing active processes
As it is likely that children will be unaware of each occurrence of their alternativearticulatory pattern for speci c consonant errors it is preferrable to destabilizeactive processes with minimal conscious eVort by the child As children becomeaware of their mismatches they frequently add the newly acquired target realizationto their existing production eg target word tu childrsquos old realization [ku] childrsquoscorrected realization [t-ku] Destabilization can be achieved with minimal consciouseVort through input therapy techniques such as auditory bombardment (Lancasterand Pope 1989) auditory decision-making such as lsquowhich bear says this wordproperlyrsquo Red Bear says lsquotworsquo or Blue Bear says lsquocoorsquo This type of strategy oftenprecipitates attention to the target consonant with possible lsquoreplayrsquo and lsquoreviewrsquo of
A Harding and P Grunwell350
their own production Frequent stimulation of cognitive alertness to the targetconsonant can develop awareness without confronting the child with errors orrisking hisher failure The child is then free to attempt to repair hisher ownrealization to continue to re ect and to silently rehearse the adult realizationTraditional articulation therapy is thus combined with development of metaphonol-ogical skills ie the ability to re ect upon onersquos own speech production The resultshould be that new target realizations will be more phonologically stable thanexclusively production-based articulation therapy might have facilitated
Stabilizationgeneralization
Procedures to ensure stabilization and generalization of new target consonantswould be as described by Grunwell (1992) Success may be constrained by theconsiderable articulatory eVort sometimes required to maintain pressure consonantproduction in spontaneous speech (Harding and Grunwell 1993)
Conclusions
In speech assessment it is helpful to distinguish between errors which are cleft-type and non-cleft type and those which are part of active versus passive processesThe active and passive processes have been de ned and their phonological implica-tions discussed Focus on active and passive processes has facilitated focus on thephonological consequences of cleft palate on speech development In the futureawareness of the likely eVect of a cleft palate on normal phonological developmentcould avoid extended periods of unsuccessful clinical intervention Furthermoresensitivity to the relationship between phonological processes and structural con-straints should facilitate theoretically based management decisions Incidences suchas the case of CP in which nasal realizations were thought to indicate VPI but weresubsequently unaVected by surgery might be avoided if phonological analysiscontributes to management decisions
Surgery did improve hypernasal resonance and eliminated passive processes buthad little eVect on active processes Active processes in younger subjects werethought to require therapeutic intervention but in the longer term the oldersubjects showed few cleft-type processes Whilst it is possible that active cleft-typeprocesses may resolve with increasing age the implication for the future is thatactive cleft-type processes should be treated with skilled therapeutic interventionnot surgery Therapy which addresses the phonological consequences of cleft palateon speech development by combining metaphonologicalphonologicalarticulatoryapproaches is likely to be successful
References
Albery E 1991 Consonant articulation in the diVerent types of cleft lip and palate UnpublishedMPhil thesis Leicester Polytechnic
Albery E and Grunwell P 1993 Consonant articulation in diVerent types of cleft palate InP Grunwell (Ed) Analysing Cleft Palate Speech (London Whurr)
Ferguson C A 1978 Fricatives in child language acquisition In V Honsa and M Hardmann-Battista (Eds) Papers on Linguistics and Child Language (Mouton The Hague)
Fletcher S G 1985 Speech production and oral motor skill in an adult with an unrepaired palatalcleft Journal of Speech and Hearing Disorders 50 254ndash261
Active versus passive cleft-type speech characteristics 351
Golding-Kushner K J 1995 Treatment of articulation and resonancne disorders associated withcleft palate management and VPI In R Shprintzen (Ed) Cleft Palate Speech Management AMultidisciplinary Approach (St Louis Mosby)
Grundy K and Harding A 1995 Developmental speech disorders In K Grundy (Ed) Linguisticsin Clinical Practice (2nd edition) (London Whurr)
Grunwell P 1985 Phonological Assessment of Child Speech (Windsor NFER-Nelson)Grunwell P 1987a Clinical Phonology (2nd edition) (London Croom Helm)Grunwell P 1987b PACS Pictures Language Elicitation Materials (Windsor NFER-Nelson)Grunwell P 1991 Processes of phonological change in developmental speech disorders Clinical
Linguistics and Phonetics 6 101ndash122Grunwell P 1992 Principled decision making in the remediation of children with phonological
disorders In P Fletcher and D Hall (Eds) Specic Speech and Language Disorders in Children(London Whurr)
Grunwell P and Harding A 1995 PACSTOYS A Screening Assessment of Phonological Development(Windsor NFER-Nelson)
Grunwell P and Harding A 1996 A note on describing types of nasality Clinical Linguistics andPhonetics 10 157ndash161
Harding A 1993 An Investigation into the Relationship Between Timing of Cleft Palate Repairand Speech Development Unpublished PhD thesis
Harding A and Grunwell P 1993 The relationship between speech and timing of hard palaterepair In P Grunwell (Ed) Analysisng Cleft Palate Speech (London Whurr)
Harding A and Grunwell P 1996 Characteristics of cleft palate speech European Journal ofDisorders of Communication 31 331ndash358
Henningsson G and Isberg A M 1986 Velopharyngeal movement patterns in patients alternatingbetween oral and glottal articulation A clinical and cineradiographicical study Cleft Palate Journal23 1ndash9
Hewlett N 1990 Processes of development and production In P Grunwell (Ed) DevelopmentalSpeech Disorders (Edinburgh Churchill Livingstone)
Hotz M M Gnoinski W M Nussbaumer H and Kistler E 1978 Early orthopaedics in CLPcases guidelines for surgery Cleft Palate Journal 15 405ndash411
Hutters B and Brondsted K 1987 Strategies in cleft palate with special reference to DanishCleft Palate Journal 24 127ndash136
Isshiki N and Ringel R 1964 Airow during the production of selected consonants Journal ofSpeech and Hearing Research 7 233ndash244
Kummer A W Curtis C Wiggs M Lee L and Strife J L 1992 Comparison of velopharyngealgap size in patients with hypernasality hypernasality with nasal emission and nasal emissionor nasal turbulence (rustle) as the primary speech characteristic Cleft-palate-Craniofacial Journal29 152ndash156
Lancaster G and Pope L 1989 Working with Childrenrsquos Phonology (Oxford Winslow)Morley M E 1970 Cleft Palate and Speech (7th edition) (Edinburgh Churchill Livingstone)Russell V J 1991 Speech Development in Children with Cleft Lip and Palate Unpublished PhD
thesis Leicester PolytechnicRussell V J and Grunwell P 1993 Speech development in children with cleft lip and palate In
P Grunwell (Ed) Analysing Cleft Palate Speech (London Whurr)Sell D A and Grunwell P 1990 Speech results following late palatal surgery in previously
unoperated Sri Lankan adolescents with cleft palate Cleft Palate Journal 27 162ndash168Sell D Harding A and Grunwell P 1994 GOSSPASS A screening assessment of cleft palate
speech European Journal of Disorders of Communication 29 1ndash15Sell D Harding A and Grunwell P 1998 GOSSPASSrsquo98 An assessment for speech disorders
associated with cleft palate andor velopharyngeal dysfunction International Journal of Languageamp Communication Disorders ( in press)
Shorter E 1995 A spectographic analyis of child homophones Unpublished honours project DeMontfort University Leicester
Stenglehoffen J 1989 Nature and causes of communication diYculties In J Stengelhofen (Ed)Cleft Palate Nature and Remediation of Communication Problems (Edinburgh Churchill Livingstone)
Trost J E 1981 Articulatory additions to the classical description of the speech of persons withcleft palate Cleft Palate Journal 18
Trost-Cardamone J E 1990 The development of speech assessing cleft palate misarticulationsIn D A Kernahan and S N Rosenstein (Eds) Cleft Lip and Palate A System of Management(Baltimore Williams amp Wilkins)
A Harding and P Grunwell352
Appendix Active passive analysis of cleft palate speech

A Harding and P Grunwell346
from incorrect to correct but progressed incrementally towards normal realizationsas described by Morley (1970) Where an early realization of target s might beglottal [h] a gradual pattern of change showed subsequent realizations to bepharyngeal [Eacute] then uvular [X] then velar [x] and eventually palatal [c] or lateral [Euml]It was interesting to note that speech patterns continued to change as late as90ndash110 years with the result that diVerences related to surgical timing and cleft-type gradually disappeared Persisting stulae were thought to account for the mostmarked cleft type processes at age 90
Implications for surgical management
This analysis of speech changes following surgery suggests some implications forsurgical management which are compatible with Sell and Grunwellrsquos (1990) ndingsin the Sri Lankan study
Surgery can change passive speech processes but it is also possible that speechtherapy may be able to change passive patterns Surgery alone is unlikely to modifyactive cleft-type processes whereas speech therapy should be able to modify activeprocesses Indications from these case studies is that where speech is the primaryproblem speech assessment should distinguish between active and passive processesin order to evaluate the necessity for full investigations and to plan therapeuticintervention Where past speech therapy has not been successful it cannot beassumed that surgical intervention will facilitate further speech progress A furthercourse of speech therapy which is sensitive to active versus passive processes todevelopmental phonological in uences on cleft-type speech development and toarticulatory diYculties in diVerent speech contexts might facilitate optimal progressWhere structural imperfection exists it is quite possible for single-word productionto be more precise than target realizations in spontaneous speech This may not bea failure of phonological generalization (Grunwell 1992) but the result of diYcultysustaining the necessary lsquoarticulatory eVort rsquo (Harding and Grunwell 1993) resultingin articulatory imprecision Deteriorating articulatory accuracy should not be over-looked in interpretation of speech results
An analytical protocol
As a result of analysing the speech data and identifying the active and passiveprocesses a protocol has been developed which records examples of each cleft-typeprocess over a series of assessments It demonstrates the progression of individualprocesses towards an adult target (see the Appendix) At each assessment onecolumn is used to indicate nasal resonance nasal emission and nasal turbulenceratings and cleft-type processes Changes in the nature of error realizations mightshow progress towards target consonants Hence whilst the total correct scoremight not have increased increments of change can be observed This observationof patterns of change may function as an adjunct to GOSSPASSrsquo98 (Sell et al 1998)giving access to a greater depth of both quantitative and qualitative data aboutconsonant production in relation to resonance nasal emission nasal turbulenceoral structure and cleft-type
Active versus passive cleft-type speech characteristics 347
Diagnostic implications
Passive versus active nasal fricatives
The important management consideration related to this distinction is that an activenasal fricative is an established phonological process which is unlikely to be directlyaVected by surgery alone Therapy would be necessary to destabilize nasal realizationsof oral consonants In contrast passive nasal fricatives may be eliminated by surgeryOf particular relevance is diVerential diagnosis between passive and active nasalfricatives in surgical and therapeutic management When hypernasality co-occurswith nasal air ow during consonant production which can be redirected by nose-holding passive nasal fricatives are diagnosed These would be transcribed as [(sk)n
deg]
passive alveolar nasal fricatives [(Wk)mdeg
] bilabial nasal fricatives or [(fk)Iacutedeg ] labiodentalnasal fricatives Full VPI investigations would be recommended to diagnose thenature of the structural or functional de ciency and distinguish between velopharyn-geal incompetence and velopharyngeal mislearning
It is highly likely that plosive targets would be aVected by reduced intra-oral airpressure such that plosives would either be realized by nasal counterparts eg bd[ [m n] or [b d] may be nasalized and weak Voiceless plosives may be eitheraccompanied by nasal emission [p t k] or realized as glottal fricative [h]
Production of the target sentence lsquoI saw Sam sitting on a busrsquo might be
[aI (sk)ndeg O~ (sk)n
degaelig~m (sk)n
deg IhIn Aacute~n mouml~(sk)ndeg] passive processes and
[aI xO xaeligm xIkIIcirc AacuteIcirc goumlx] active processes
Contribution to surgical management decisions
Passiveactive interpretation of clinical assessments might facilitate surgical manage-ment decisions If noseholding does not facilitate correct production of targetconsonants then it is likely that an alternative articulatory pattern has becomephonologically established ie particular realizations for one or more targets areconsistently distributed in the phonological system These realizations may haveevolved because of initial diYculty producing articulatory targets and subsequentlystabilized within the phonological system Grundy and Harding (1995) refer to thisphenomenon as an lsquoarticulatory disorder with phonological consequencesrsquo
Therapy
Where obvious structural defects or diagnosed dysfunction exists clinicians fre-quently defer therapeutic intervention until surgery has been undertaken Theexpectation would be that normal structure and function is essential for normalspeech However pre-operative therapy may facilitate oral consonant productionwhich may serve to reduce hypernasal resonance Hence therapy prior to surgerymay avoid unnecessary surgery or reduce the extent of surgery required All activeprocesses are likely to require therapy
Principled selection of targets for therapy
Speech patterns frequently evidence a mixture of apparently passive and activeprocesses which complicates decisions about target selection Target selection can
A Harding and P Grunwell348
be based on assessment of which consonant targets can be most easily elicted inisolation (stimulability) This may lead to a sequence of target selection which isopposite to the sequence of consonant acquisition in normal development Forexample where reduced intra-oral pressure is present in a passive pattern [T] maybe easier to elicit in imitation than more nely grooved [s] or [S] Therapy maytarget [T] followed by [S ] and nally [s] As in non-cleft phonological therapywhere a class of consonants is aVected by the cleft then it is helpful to target theentire class The following decision-making process can be applied for both activeand passive processes
Decision making procedure for target selection
(1) Voiced versus voiceless targets(2) Front versus back placements(3) Syllable initial versus syllable nal targets(4) Plosives versus fricative targets
Voiceless plosives and fricatives are produced with an open glottis whichfacilitates topping up of air ow from the lungs hence voiceless plosive and fricativetargets are frequently more successful than voiced counterparts (Isshiki and Ringel1964) Front targets usually cause more diYculty than back particularly where analveolar defect or stula exists Contrary to normal development back targets maybe targeted before front Word- nal targets generally require less oral air pressurethan word initial targets and similarly fricatives may be more easily elicited thanplosives Fricatives do require a greater volume of air than plosives (Fletcher 1985)but in the presence of nasal escape weak fricative production appears to be morereadily achieved than weak plosive production Since nal fricatives would normallybe acquired in advance of word-initial fricatives (Ferguson 1978) targeting word- nal fricatives is frequently a productive starting point for therapy
Principles of therapy for passive processes
(1) Use of soft attack similar to gentle whisper for all target models ensuresminimal articulatory eVort (Harding and Grunwell 1993) and requires min-imal intra-oral air pressure It may be appropriate to gradually increase thearticulatory attack when the articulatory posture and evidence of intendedoral air ow have been established
(2) Slightly stretched duration of segment transitions in models of consonantto vowel (CndashV) or vowel to consonant (VndashC) facilitates review of motorplanning and extends the available time for execution of the new motorprogrammer whilst maintaining control of the oral airstream
(3) Noseholding can be used to provide exclusively oral air ow Gradual releaseof the nostrils during production of sustained [VVVVVf ] or [hhhhh ] allowsthe child to attempt to sustain an oral consonant despite increasing nasalemission This maximizes the use of available oral air ow Procedures forusing noseholding are described in some detail by Golding-Kushner (1995)
Principles of therapy for active processes
This is more like phonological therapy and can follow Grunwellrsquos (1991) processesfor phonological change and principled decision-making (Grunwell 1992) Some
Active versus passive cleft-type speech characteristics 349
examples are given here by way of illustration of ways to eVect the rst twoprocesses of change which may need to be approached diVerently in cleft palateversus non-cleft speech disorders DiVerent approaches may also be appropriate formodifying active versus passive cleft-type processes
Innovation production of new targets Some useful principles
(1) Introduction of new lsquonon-speech likersquo targets in sound play using a conson-ant sound segment model such as [ph ] note not a syllable like [p] whichis the type of pronunciation used when target sounds are presented as lettersfor reading Target [s] might be introduced as a lsquoTrain Slowing Down Noisersquo[ts ts ts tssssssss]
(2) lsquoNew consonantsrsquo can later be modelled and elicited in soft productions ofsyllable structure [tssssndashi] [ indashtssss] which can subsequently be identi ed assimilar to words lsquosearsquo and lsquoeatsrsquo
(3) lsquoDeferring responsibilityrsquo transfers responsibility or lsquoblamersquo for errors fromthe child and attributes it to the articulators eg lsquoyour tongue is havingtrouble with hellip rsquo lsquoLetrsquos show your tongue how to hellip rsquo
(4) New targets can be modelled repeatedly and recorded on audio or videotape which can be listened to at home
(5) Targeting classes of consonants (eg alveolars t d s n l voiceless fricativesf s S perhaps with aVricate T avoids phonological confusion whichmight occur if production ofsis achieved whilst other alveolar targetsremain backed The risk is that s might not integrate into the phonologicalsystem unless all backed alveolar consonants are destabilized
(6) Increased eye contact during auditory and production work can be invaluablein holding visual and auditory attention and ensures that visual informationabout the sound has been processed This is easily achieved by the clinicianlifting any focus of the childrsquos attention close to hisher mouth at theprecise moment when the target is modelled
Stimulation of non-speech related sounds such as a lsquoTrain Slowing DownNoisersquo [ts ts tsss] con rms that target [s] is physically achievable whether or not[ssss] can be imitated Some children continue to access [s] through the lsquoTrainSlowing Down Noisersquo throughout therapy until it is occurring spontaneouslywithout conscious planning This can be an eVective means of underminingestablished motor programmers (Hewlett 1990) for active cleft-type processes
Destabilizing active processes
As it is likely that children will be unaware of each occurrence of their alternativearticulatory pattern for speci c consonant errors it is preferrable to destabilizeactive processes with minimal conscious eVort by the child As children becomeaware of their mismatches they frequently add the newly acquired target realizationto their existing production eg target word tu childrsquos old realization [ku] childrsquoscorrected realization [t-ku] Destabilization can be achieved with minimal consciouseVort through input therapy techniques such as auditory bombardment (Lancasterand Pope 1989) auditory decision-making such as lsquowhich bear says this wordproperlyrsquo Red Bear says lsquotworsquo or Blue Bear says lsquocoorsquo This type of strategy oftenprecipitates attention to the target consonant with possible lsquoreplayrsquo and lsquoreviewrsquo of
A Harding and P Grunwell350
their own production Frequent stimulation of cognitive alertness to the targetconsonant can develop awareness without confronting the child with errors orrisking hisher failure The child is then free to attempt to repair hisher ownrealization to continue to re ect and to silently rehearse the adult realizationTraditional articulation therapy is thus combined with development of metaphonol-ogical skills ie the ability to re ect upon onersquos own speech production The resultshould be that new target realizations will be more phonologically stable thanexclusively production-based articulation therapy might have facilitated
Stabilizationgeneralization
Procedures to ensure stabilization and generalization of new target consonantswould be as described by Grunwell (1992) Success may be constrained by theconsiderable articulatory eVort sometimes required to maintain pressure consonantproduction in spontaneous speech (Harding and Grunwell 1993)
Conclusions
In speech assessment it is helpful to distinguish between errors which are cleft-type and non-cleft type and those which are part of active versus passive processesThe active and passive processes have been de ned and their phonological implica-tions discussed Focus on active and passive processes has facilitated focus on thephonological consequences of cleft palate on speech development In the futureawareness of the likely eVect of a cleft palate on normal phonological developmentcould avoid extended periods of unsuccessful clinical intervention Furthermoresensitivity to the relationship between phonological processes and structural con-straints should facilitate theoretically based management decisions Incidences suchas the case of CP in which nasal realizations were thought to indicate VPI but weresubsequently unaVected by surgery might be avoided if phonological analysiscontributes to management decisions
Surgery did improve hypernasal resonance and eliminated passive processes buthad little eVect on active processes Active processes in younger subjects werethought to require therapeutic intervention but in the longer term the oldersubjects showed few cleft-type processes Whilst it is possible that active cleft-typeprocesses may resolve with increasing age the implication for the future is thatactive cleft-type processes should be treated with skilled therapeutic interventionnot surgery Therapy which addresses the phonological consequences of cleft palateon speech development by combining metaphonologicalphonologicalarticulatoryapproaches is likely to be successful
References
Albery E 1991 Consonant articulation in the diVerent types of cleft lip and palate UnpublishedMPhil thesis Leicester Polytechnic
Albery E and Grunwell P 1993 Consonant articulation in diVerent types of cleft palate InP Grunwell (Ed) Analysing Cleft Palate Speech (London Whurr)
Ferguson C A 1978 Fricatives in child language acquisition In V Honsa and M Hardmann-Battista (Eds) Papers on Linguistics and Child Language (Mouton The Hague)
Fletcher S G 1985 Speech production and oral motor skill in an adult with an unrepaired palatalcleft Journal of Speech and Hearing Disorders 50 254ndash261
Active versus passive cleft-type speech characteristics 351
Golding-Kushner K J 1995 Treatment of articulation and resonancne disorders associated withcleft palate management and VPI In R Shprintzen (Ed) Cleft Palate Speech Management AMultidisciplinary Approach (St Louis Mosby)
Grundy K and Harding A 1995 Developmental speech disorders In K Grundy (Ed) Linguisticsin Clinical Practice (2nd edition) (London Whurr)
Grunwell P 1985 Phonological Assessment of Child Speech (Windsor NFER-Nelson)Grunwell P 1987a Clinical Phonology (2nd edition) (London Croom Helm)Grunwell P 1987b PACS Pictures Language Elicitation Materials (Windsor NFER-Nelson)Grunwell P 1991 Processes of phonological change in developmental speech disorders Clinical
Linguistics and Phonetics 6 101ndash122Grunwell P 1992 Principled decision making in the remediation of children with phonological
disorders In P Fletcher and D Hall (Eds) Specic Speech and Language Disorders in Children(London Whurr)
Grunwell P and Harding A 1995 PACSTOYS A Screening Assessment of Phonological Development(Windsor NFER-Nelson)
Grunwell P and Harding A 1996 A note on describing types of nasality Clinical Linguistics andPhonetics 10 157ndash161
Harding A 1993 An Investigation into the Relationship Between Timing of Cleft Palate Repairand Speech Development Unpublished PhD thesis
Harding A and Grunwell P 1993 The relationship between speech and timing of hard palaterepair In P Grunwell (Ed) Analysisng Cleft Palate Speech (London Whurr)
Harding A and Grunwell P 1996 Characteristics of cleft palate speech European Journal ofDisorders of Communication 31 331ndash358
Henningsson G and Isberg A M 1986 Velopharyngeal movement patterns in patients alternatingbetween oral and glottal articulation A clinical and cineradiographicical study Cleft Palate Journal23 1ndash9
Hewlett N 1990 Processes of development and production In P Grunwell (Ed) DevelopmentalSpeech Disorders (Edinburgh Churchill Livingstone)
Hotz M M Gnoinski W M Nussbaumer H and Kistler E 1978 Early orthopaedics in CLPcases guidelines for surgery Cleft Palate Journal 15 405ndash411
Hutters B and Brondsted K 1987 Strategies in cleft palate with special reference to DanishCleft Palate Journal 24 127ndash136
Isshiki N and Ringel R 1964 Airow during the production of selected consonants Journal ofSpeech and Hearing Research 7 233ndash244
Kummer A W Curtis C Wiggs M Lee L and Strife J L 1992 Comparison of velopharyngealgap size in patients with hypernasality hypernasality with nasal emission and nasal emissionor nasal turbulence (rustle) as the primary speech characteristic Cleft-palate-Craniofacial Journal29 152ndash156
Lancaster G and Pope L 1989 Working with Childrenrsquos Phonology (Oxford Winslow)Morley M E 1970 Cleft Palate and Speech (7th edition) (Edinburgh Churchill Livingstone)Russell V J 1991 Speech Development in Children with Cleft Lip and Palate Unpublished PhD
thesis Leicester PolytechnicRussell V J and Grunwell P 1993 Speech development in children with cleft lip and palate In
P Grunwell (Ed) Analysing Cleft Palate Speech (London Whurr)Sell D A and Grunwell P 1990 Speech results following late palatal surgery in previously
unoperated Sri Lankan adolescents with cleft palate Cleft Palate Journal 27 162ndash168Sell D Harding A and Grunwell P 1994 GOSSPASS A screening assessment of cleft palate
speech European Journal of Disorders of Communication 29 1ndash15Sell D Harding A and Grunwell P 1998 GOSSPASSrsquo98 An assessment for speech disorders
associated with cleft palate andor velopharyngeal dysfunction International Journal of Languageamp Communication Disorders ( in press)
Shorter E 1995 A spectographic analyis of child homophones Unpublished honours project DeMontfort University Leicester
Stenglehoffen J 1989 Nature and causes of communication diYculties In J Stengelhofen (Ed)Cleft Palate Nature and Remediation of Communication Problems (Edinburgh Churchill Livingstone)
Trost J E 1981 Articulatory additions to the classical description of the speech of persons withcleft palate Cleft Palate Journal 18
Trost-Cardamone J E 1990 The development of speech assessing cleft palate misarticulationsIn D A Kernahan and S N Rosenstein (Eds) Cleft Lip and Palate A System of Management(Baltimore Williams amp Wilkins)
A Harding and P Grunwell352
Appendix Active passive analysis of cleft palate speech

Active versus passive cleft-type speech characteristics 347
Diagnostic implications
Passive versus active nasal fricatives
The important management consideration related to this distinction is that an activenasal fricative is an established phonological process which is unlikely to be directlyaVected by surgery alone Therapy would be necessary to destabilize nasal realizationsof oral consonants In contrast passive nasal fricatives may be eliminated by surgeryOf particular relevance is diVerential diagnosis between passive and active nasalfricatives in surgical and therapeutic management When hypernasality co-occurswith nasal air ow during consonant production which can be redirected by nose-holding passive nasal fricatives are diagnosed These would be transcribed as [(sk)n
deg]
passive alveolar nasal fricatives [(Wk)mdeg
] bilabial nasal fricatives or [(fk)Iacutedeg ] labiodentalnasal fricatives Full VPI investigations would be recommended to diagnose thenature of the structural or functional de ciency and distinguish between velopharyn-geal incompetence and velopharyngeal mislearning
It is highly likely that plosive targets would be aVected by reduced intra-oral airpressure such that plosives would either be realized by nasal counterparts eg bd[ [m n] or [b d] may be nasalized and weak Voiceless plosives may be eitheraccompanied by nasal emission [p t k] or realized as glottal fricative [h]
Production of the target sentence lsquoI saw Sam sitting on a busrsquo might be
[aI (sk)ndeg O~ (sk)n
degaelig~m (sk)n
deg IhIn Aacute~n mouml~(sk)ndeg] passive processes and
[aI xO xaeligm xIkIIcirc AacuteIcirc goumlx] active processes
Contribution to surgical management decisions
Passiveactive interpretation of clinical assessments might facilitate surgical manage-ment decisions If noseholding does not facilitate correct production of targetconsonants then it is likely that an alternative articulatory pattern has becomephonologically established ie particular realizations for one or more targets areconsistently distributed in the phonological system These realizations may haveevolved because of initial diYculty producing articulatory targets and subsequentlystabilized within the phonological system Grundy and Harding (1995) refer to thisphenomenon as an lsquoarticulatory disorder with phonological consequencesrsquo
Therapy
Where obvious structural defects or diagnosed dysfunction exists clinicians fre-quently defer therapeutic intervention until surgery has been undertaken Theexpectation would be that normal structure and function is essential for normalspeech However pre-operative therapy may facilitate oral consonant productionwhich may serve to reduce hypernasal resonance Hence therapy prior to surgerymay avoid unnecessary surgery or reduce the extent of surgery required All activeprocesses are likely to require therapy
Principled selection of targets for therapy
Speech patterns frequently evidence a mixture of apparently passive and activeprocesses which complicates decisions about target selection Target selection can
A Harding and P Grunwell348
be based on assessment of which consonant targets can be most easily elicted inisolation (stimulability) This may lead to a sequence of target selection which isopposite to the sequence of consonant acquisition in normal development Forexample where reduced intra-oral pressure is present in a passive pattern [T] maybe easier to elicit in imitation than more nely grooved [s] or [S] Therapy maytarget [T] followed by [S ] and nally [s] As in non-cleft phonological therapywhere a class of consonants is aVected by the cleft then it is helpful to target theentire class The following decision-making process can be applied for both activeand passive processes
Decision making procedure for target selection
(1) Voiced versus voiceless targets(2) Front versus back placements(3) Syllable initial versus syllable nal targets(4) Plosives versus fricative targets
Voiceless plosives and fricatives are produced with an open glottis whichfacilitates topping up of air ow from the lungs hence voiceless plosive and fricativetargets are frequently more successful than voiced counterparts (Isshiki and Ringel1964) Front targets usually cause more diYculty than back particularly where analveolar defect or stula exists Contrary to normal development back targets maybe targeted before front Word- nal targets generally require less oral air pressurethan word initial targets and similarly fricatives may be more easily elicited thanplosives Fricatives do require a greater volume of air than plosives (Fletcher 1985)but in the presence of nasal escape weak fricative production appears to be morereadily achieved than weak plosive production Since nal fricatives would normallybe acquired in advance of word-initial fricatives (Ferguson 1978) targeting word- nal fricatives is frequently a productive starting point for therapy
Principles of therapy for passive processes
(1) Use of soft attack similar to gentle whisper for all target models ensuresminimal articulatory eVort (Harding and Grunwell 1993) and requires min-imal intra-oral air pressure It may be appropriate to gradually increase thearticulatory attack when the articulatory posture and evidence of intendedoral air ow have been established
(2) Slightly stretched duration of segment transitions in models of consonantto vowel (CndashV) or vowel to consonant (VndashC) facilitates review of motorplanning and extends the available time for execution of the new motorprogrammer whilst maintaining control of the oral airstream
(3) Noseholding can be used to provide exclusively oral air ow Gradual releaseof the nostrils during production of sustained [VVVVVf ] or [hhhhh ] allowsthe child to attempt to sustain an oral consonant despite increasing nasalemission This maximizes the use of available oral air ow Procedures forusing noseholding are described in some detail by Golding-Kushner (1995)
Principles of therapy for active processes
This is more like phonological therapy and can follow Grunwellrsquos (1991) processesfor phonological change and principled decision-making (Grunwell 1992) Some
Active versus passive cleft-type speech characteristics 349
examples are given here by way of illustration of ways to eVect the rst twoprocesses of change which may need to be approached diVerently in cleft palateversus non-cleft speech disorders DiVerent approaches may also be appropriate formodifying active versus passive cleft-type processes
Innovation production of new targets Some useful principles
(1) Introduction of new lsquonon-speech likersquo targets in sound play using a conson-ant sound segment model such as [ph ] note not a syllable like [p] whichis the type of pronunciation used when target sounds are presented as lettersfor reading Target [s] might be introduced as a lsquoTrain Slowing Down Noisersquo[ts ts ts tssssssss]
(2) lsquoNew consonantsrsquo can later be modelled and elicited in soft productions ofsyllable structure [tssssndashi] [ indashtssss] which can subsequently be identi ed assimilar to words lsquosearsquo and lsquoeatsrsquo
(3) lsquoDeferring responsibilityrsquo transfers responsibility or lsquoblamersquo for errors fromthe child and attributes it to the articulators eg lsquoyour tongue is havingtrouble with hellip rsquo lsquoLetrsquos show your tongue how to hellip rsquo
(4) New targets can be modelled repeatedly and recorded on audio or videotape which can be listened to at home
(5) Targeting classes of consonants (eg alveolars t d s n l voiceless fricativesf s S perhaps with aVricate T avoids phonological confusion whichmight occur if production ofsis achieved whilst other alveolar targetsremain backed The risk is that s might not integrate into the phonologicalsystem unless all backed alveolar consonants are destabilized
(6) Increased eye contact during auditory and production work can be invaluablein holding visual and auditory attention and ensures that visual informationabout the sound has been processed This is easily achieved by the clinicianlifting any focus of the childrsquos attention close to hisher mouth at theprecise moment when the target is modelled
Stimulation of non-speech related sounds such as a lsquoTrain Slowing DownNoisersquo [ts ts tsss] con rms that target [s] is physically achievable whether or not[ssss] can be imitated Some children continue to access [s] through the lsquoTrainSlowing Down Noisersquo throughout therapy until it is occurring spontaneouslywithout conscious planning This can be an eVective means of underminingestablished motor programmers (Hewlett 1990) for active cleft-type processes
Destabilizing active processes
As it is likely that children will be unaware of each occurrence of their alternativearticulatory pattern for speci c consonant errors it is preferrable to destabilizeactive processes with minimal conscious eVort by the child As children becomeaware of their mismatches they frequently add the newly acquired target realizationto their existing production eg target word tu childrsquos old realization [ku] childrsquoscorrected realization [t-ku] Destabilization can be achieved with minimal consciouseVort through input therapy techniques such as auditory bombardment (Lancasterand Pope 1989) auditory decision-making such as lsquowhich bear says this wordproperlyrsquo Red Bear says lsquotworsquo or Blue Bear says lsquocoorsquo This type of strategy oftenprecipitates attention to the target consonant with possible lsquoreplayrsquo and lsquoreviewrsquo of
A Harding and P Grunwell350
their own production Frequent stimulation of cognitive alertness to the targetconsonant can develop awareness without confronting the child with errors orrisking hisher failure The child is then free to attempt to repair hisher ownrealization to continue to re ect and to silently rehearse the adult realizationTraditional articulation therapy is thus combined with development of metaphonol-ogical skills ie the ability to re ect upon onersquos own speech production The resultshould be that new target realizations will be more phonologically stable thanexclusively production-based articulation therapy might have facilitated
Stabilizationgeneralization
Procedures to ensure stabilization and generalization of new target consonantswould be as described by Grunwell (1992) Success may be constrained by theconsiderable articulatory eVort sometimes required to maintain pressure consonantproduction in spontaneous speech (Harding and Grunwell 1993)
Conclusions
In speech assessment it is helpful to distinguish between errors which are cleft-type and non-cleft type and those which are part of active versus passive processesThe active and passive processes have been de ned and their phonological implica-tions discussed Focus on active and passive processes has facilitated focus on thephonological consequences of cleft palate on speech development In the futureawareness of the likely eVect of a cleft palate on normal phonological developmentcould avoid extended periods of unsuccessful clinical intervention Furthermoresensitivity to the relationship between phonological processes and structural con-straints should facilitate theoretically based management decisions Incidences suchas the case of CP in which nasal realizations were thought to indicate VPI but weresubsequently unaVected by surgery might be avoided if phonological analysiscontributes to management decisions
Surgery did improve hypernasal resonance and eliminated passive processes buthad little eVect on active processes Active processes in younger subjects werethought to require therapeutic intervention but in the longer term the oldersubjects showed few cleft-type processes Whilst it is possible that active cleft-typeprocesses may resolve with increasing age the implication for the future is thatactive cleft-type processes should be treated with skilled therapeutic interventionnot surgery Therapy which addresses the phonological consequences of cleft palateon speech development by combining metaphonologicalphonologicalarticulatoryapproaches is likely to be successful
References
Albery E 1991 Consonant articulation in the diVerent types of cleft lip and palate UnpublishedMPhil thesis Leicester Polytechnic
Albery E and Grunwell P 1993 Consonant articulation in diVerent types of cleft palate InP Grunwell (Ed) Analysing Cleft Palate Speech (London Whurr)
Ferguson C A 1978 Fricatives in child language acquisition In V Honsa and M Hardmann-Battista (Eds) Papers on Linguistics and Child Language (Mouton The Hague)
Fletcher S G 1985 Speech production and oral motor skill in an adult with an unrepaired palatalcleft Journal of Speech and Hearing Disorders 50 254ndash261
Active versus passive cleft-type speech characteristics 351
Golding-Kushner K J 1995 Treatment of articulation and resonancne disorders associated withcleft palate management and VPI In R Shprintzen (Ed) Cleft Palate Speech Management AMultidisciplinary Approach (St Louis Mosby)
Grundy K and Harding A 1995 Developmental speech disorders In K Grundy (Ed) Linguisticsin Clinical Practice (2nd edition) (London Whurr)
Grunwell P 1985 Phonological Assessment of Child Speech (Windsor NFER-Nelson)Grunwell P 1987a Clinical Phonology (2nd edition) (London Croom Helm)Grunwell P 1987b PACS Pictures Language Elicitation Materials (Windsor NFER-Nelson)Grunwell P 1991 Processes of phonological change in developmental speech disorders Clinical
Linguistics and Phonetics 6 101ndash122Grunwell P 1992 Principled decision making in the remediation of children with phonological
disorders In P Fletcher and D Hall (Eds) Specic Speech and Language Disorders in Children(London Whurr)
Grunwell P and Harding A 1995 PACSTOYS A Screening Assessment of Phonological Development(Windsor NFER-Nelson)
Grunwell P and Harding A 1996 A note on describing types of nasality Clinical Linguistics andPhonetics 10 157ndash161
Harding A 1993 An Investigation into the Relationship Between Timing of Cleft Palate Repairand Speech Development Unpublished PhD thesis
Harding A and Grunwell P 1993 The relationship between speech and timing of hard palaterepair In P Grunwell (Ed) Analysisng Cleft Palate Speech (London Whurr)
Harding A and Grunwell P 1996 Characteristics of cleft palate speech European Journal ofDisorders of Communication 31 331ndash358
Henningsson G and Isberg A M 1986 Velopharyngeal movement patterns in patients alternatingbetween oral and glottal articulation A clinical and cineradiographicical study Cleft Palate Journal23 1ndash9
Hewlett N 1990 Processes of development and production In P Grunwell (Ed) DevelopmentalSpeech Disorders (Edinburgh Churchill Livingstone)
Hotz M M Gnoinski W M Nussbaumer H and Kistler E 1978 Early orthopaedics in CLPcases guidelines for surgery Cleft Palate Journal 15 405ndash411
Hutters B and Brondsted K 1987 Strategies in cleft palate with special reference to DanishCleft Palate Journal 24 127ndash136
Isshiki N and Ringel R 1964 Airow during the production of selected consonants Journal ofSpeech and Hearing Research 7 233ndash244
Kummer A W Curtis C Wiggs M Lee L and Strife J L 1992 Comparison of velopharyngealgap size in patients with hypernasality hypernasality with nasal emission and nasal emissionor nasal turbulence (rustle) as the primary speech characteristic Cleft-palate-Craniofacial Journal29 152ndash156
Lancaster G and Pope L 1989 Working with Childrenrsquos Phonology (Oxford Winslow)Morley M E 1970 Cleft Palate and Speech (7th edition) (Edinburgh Churchill Livingstone)Russell V J 1991 Speech Development in Children with Cleft Lip and Palate Unpublished PhD
thesis Leicester PolytechnicRussell V J and Grunwell P 1993 Speech development in children with cleft lip and palate In
P Grunwell (Ed) Analysing Cleft Palate Speech (London Whurr)Sell D A and Grunwell P 1990 Speech results following late palatal surgery in previously
unoperated Sri Lankan adolescents with cleft palate Cleft Palate Journal 27 162ndash168Sell D Harding A and Grunwell P 1994 GOSSPASS A screening assessment of cleft palate
speech European Journal of Disorders of Communication 29 1ndash15Sell D Harding A and Grunwell P 1998 GOSSPASSrsquo98 An assessment for speech disorders
associated with cleft palate andor velopharyngeal dysfunction International Journal of Languageamp Communication Disorders ( in press)
Shorter E 1995 A spectographic analyis of child homophones Unpublished honours project DeMontfort University Leicester
Stenglehoffen J 1989 Nature and causes of communication diYculties In J Stengelhofen (Ed)Cleft Palate Nature and Remediation of Communication Problems (Edinburgh Churchill Livingstone)
Trost J E 1981 Articulatory additions to the classical description of the speech of persons withcleft palate Cleft Palate Journal 18
Trost-Cardamone J E 1990 The development of speech assessing cleft palate misarticulationsIn D A Kernahan and S N Rosenstein (Eds) Cleft Lip and Palate A System of Management(Baltimore Williams amp Wilkins)
A Harding and P Grunwell352
Appendix Active passive analysis of cleft palate speech

A Harding and P Grunwell348
be based on assessment of which consonant targets can be most easily elicted inisolation (stimulability) This may lead to a sequence of target selection which isopposite to the sequence of consonant acquisition in normal development Forexample where reduced intra-oral pressure is present in a passive pattern [T] maybe easier to elicit in imitation than more nely grooved [s] or [S] Therapy maytarget [T] followed by [S ] and nally [s] As in non-cleft phonological therapywhere a class of consonants is aVected by the cleft then it is helpful to target theentire class The following decision-making process can be applied for both activeand passive processes
Decision making procedure for target selection
(1) Voiced versus voiceless targets(2) Front versus back placements(3) Syllable initial versus syllable nal targets(4) Plosives versus fricative targets
Voiceless plosives and fricatives are produced with an open glottis whichfacilitates topping up of air ow from the lungs hence voiceless plosive and fricativetargets are frequently more successful than voiced counterparts (Isshiki and Ringel1964) Front targets usually cause more diYculty than back particularly where analveolar defect or stula exists Contrary to normal development back targets maybe targeted before front Word- nal targets generally require less oral air pressurethan word initial targets and similarly fricatives may be more easily elicited thanplosives Fricatives do require a greater volume of air than plosives (Fletcher 1985)but in the presence of nasal escape weak fricative production appears to be morereadily achieved than weak plosive production Since nal fricatives would normallybe acquired in advance of word-initial fricatives (Ferguson 1978) targeting word- nal fricatives is frequently a productive starting point for therapy
Principles of therapy for passive processes
(1) Use of soft attack similar to gentle whisper for all target models ensuresminimal articulatory eVort (Harding and Grunwell 1993) and requires min-imal intra-oral air pressure It may be appropriate to gradually increase thearticulatory attack when the articulatory posture and evidence of intendedoral air ow have been established
(2) Slightly stretched duration of segment transitions in models of consonantto vowel (CndashV) or vowel to consonant (VndashC) facilitates review of motorplanning and extends the available time for execution of the new motorprogrammer whilst maintaining control of the oral airstream
(3) Noseholding can be used to provide exclusively oral air ow Gradual releaseof the nostrils during production of sustained [VVVVVf ] or [hhhhh ] allowsthe child to attempt to sustain an oral consonant despite increasing nasalemission This maximizes the use of available oral air ow Procedures forusing noseholding are described in some detail by Golding-Kushner (1995)
Principles of therapy for active processes
This is more like phonological therapy and can follow Grunwellrsquos (1991) processesfor phonological change and principled decision-making (Grunwell 1992) Some
Active versus passive cleft-type speech characteristics 349
examples are given here by way of illustration of ways to eVect the rst twoprocesses of change which may need to be approached diVerently in cleft palateversus non-cleft speech disorders DiVerent approaches may also be appropriate formodifying active versus passive cleft-type processes
Innovation production of new targets Some useful principles
(1) Introduction of new lsquonon-speech likersquo targets in sound play using a conson-ant sound segment model such as [ph ] note not a syllable like [p] whichis the type of pronunciation used when target sounds are presented as lettersfor reading Target [s] might be introduced as a lsquoTrain Slowing Down Noisersquo[ts ts ts tssssssss]
(2) lsquoNew consonantsrsquo can later be modelled and elicited in soft productions ofsyllable structure [tssssndashi] [ indashtssss] which can subsequently be identi ed assimilar to words lsquosearsquo and lsquoeatsrsquo
(3) lsquoDeferring responsibilityrsquo transfers responsibility or lsquoblamersquo for errors fromthe child and attributes it to the articulators eg lsquoyour tongue is havingtrouble with hellip rsquo lsquoLetrsquos show your tongue how to hellip rsquo
(4) New targets can be modelled repeatedly and recorded on audio or videotape which can be listened to at home
(5) Targeting classes of consonants (eg alveolars t d s n l voiceless fricativesf s S perhaps with aVricate T avoids phonological confusion whichmight occur if production ofsis achieved whilst other alveolar targetsremain backed The risk is that s might not integrate into the phonologicalsystem unless all backed alveolar consonants are destabilized
(6) Increased eye contact during auditory and production work can be invaluablein holding visual and auditory attention and ensures that visual informationabout the sound has been processed This is easily achieved by the clinicianlifting any focus of the childrsquos attention close to hisher mouth at theprecise moment when the target is modelled
Stimulation of non-speech related sounds such as a lsquoTrain Slowing DownNoisersquo [ts ts tsss] con rms that target [s] is physically achievable whether or not[ssss] can be imitated Some children continue to access [s] through the lsquoTrainSlowing Down Noisersquo throughout therapy until it is occurring spontaneouslywithout conscious planning This can be an eVective means of underminingestablished motor programmers (Hewlett 1990) for active cleft-type processes
Destabilizing active processes
As it is likely that children will be unaware of each occurrence of their alternativearticulatory pattern for speci c consonant errors it is preferrable to destabilizeactive processes with minimal conscious eVort by the child As children becomeaware of their mismatches they frequently add the newly acquired target realizationto their existing production eg target word tu childrsquos old realization [ku] childrsquoscorrected realization [t-ku] Destabilization can be achieved with minimal consciouseVort through input therapy techniques such as auditory bombardment (Lancasterand Pope 1989) auditory decision-making such as lsquowhich bear says this wordproperlyrsquo Red Bear says lsquotworsquo or Blue Bear says lsquocoorsquo This type of strategy oftenprecipitates attention to the target consonant with possible lsquoreplayrsquo and lsquoreviewrsquo of
A Harding and P Grunwell350
their own production Frequent stimulation of cognitive alertness to the targetconsonant can develop awareness without confronting the child with errors orrisking hisher failure The child is then free to attempt to repair hisher ownrealization to continue to re ect and to silently rehearse the adult realizationTraditional articulation therapy is thus combined with development of metaphonol-ogical skills ie the ability to re ect upon onersquos own speech production The resultshould be that new target realizations will be more phonologically stable thanexclusively production-based articulation therapy might have facilitated
Stabilizationgeneralization
Procedures to ensure stabilization and generalization of new target consonantswould be as described by Grunwell (1992) Success may be constrained by theconsiderable articulatory eVort sometimes required to maintain pressure consonantproduction in spontaneous speech (Harding and Grunwell 1993)
Conclusions
In speech assessment it is helpful to distinguish between errors which are cleft-type and non-cleft type and those which are part of active versus passive processesThe active and passive processes have been de ned and their phonological implica-tions discussed Focus on active and passive processes has facilitated focus on thephonological consequences of cleft palate on speech development In the futureawareness of the likely eVect of a cleft palate on normal phonological developmentcould avoid extended periods of unsuccessful clinical intervention Furthermoresensitivity to the relationship between phonological processes and structural con-straints should facilitate theoretically based management decisions Incidences suchas the case of CP in which nasal realizations were thought to indicate VPI but weresubsequently unaVected by surgery might be avoided if phonological analysiscontributes to management decisions
Surgery did improve hypernasal resonance and eliminated passive processes buthad little eVect on active processes Active processes in younger subjects werethought to require therapeutic intervention but in the longer term the oldersubjects showed few cleft-type processes Whilst it is possible that active cleft-typeprocesses may resolve with increasing age the implication for the future is thatactive cleft-type processes should be treated with skilled therapeutic interventionnot surgery Therapy which addresses the phonological consequences of cleft palateon speech development by combining metaphonologicalphonologicalarticulatoryapproaches is likely to be successful
References
Albery E 1991 Consonant articulation in the diVerent types of cleft lip and palate UnpublishedMPhil thesis Leicester Polytechnic
Albery E and Grunwell P 1993 Consonant articulation in diVerent types of cleft palate InP Grunwell (Ed) Analysing Cleft Palate Speech (London Whurr)
Ferguson C A 1978 Fricatives in child language acquisition In V Honsa and M Hardmann-Battista (Eds) Papers on Linguistics and Child Language (Mouton The Hague)
Fletcher S G 1985 Speech production and oral motor skill in an adult with an unrepaired palatalcleft Journal of Speech and Hearing Disorders 50 254ndash261
Active versus passive cleft-type speech characteristics 351
Golding-Kushner K J 1995 Treatment of articulation and resonancne disorders associated withcleft palate management and VPI In R Shprintzen (Ed) Cleft Palate Speech Management AMultidisciplinary Approach (St Louis Mosby)
Grundy K and Harding A 1995 Developmental speech disorders In K Grundy (Ed) Linguisticsin Clinical Practice (2nd edition) (London Whurr)
Grunwell P 1985 Phonological Assessment of Child Speech (Windsor NFER-Nelson)Grunwell P 1987a Clinical Phonology (2nd edition) (London Croom Helm)Grunwell P 1987b PACS Pictures Language Elicitation Materials (Windsor NFER-Nelson)Grunwell P 1991 Processes of phonological change in developmental speech disorders Clinical
Linguistics and Phonetics 6 101ndash122Grunwell P 1992 Principled decision making in the remediation of children with phonological
disorders In P Fletcher and D Hall (Eds) Specic Speech and Language Disorders in Children(London Whurr)
Grunwell P and Harding A 1995 PACSTOYS A Screening Assessment of Phonological Development(Windsor NFER-Nelson)
Grunwell P and Harding A 1996 A note on describing types of nasality Clinical Linguistics andPhonetics 10 157ndash161
Harding A 1993 An Investigation into the Relationship Between Timing of Cleft Palate Repairand Speech Development Unpublished PhD thesis
Harding A and Grunwell P 1993 The relationship between speech and timing of hard palaterepair In P Grunwell (Ed) Analysisng Cleft Palate Speech (London Whurr)
Harding A and Grunwell P 1996 Characteristics of cleft palate speech European Journal ofDisorders of Communication 31 331ndash358
Henningsson G and Isberg A M 1986 Velopharyngeal movement patterns in patients alternatingbetween oral and glottal articulation A clinical and cineradiographicical study Cleft Palate Journal23 1ndash9
Hewlett N 1990 Processes of development and production In P Grunwell (Ed) DevelopmentalSpeech Disorders (Edinburgh Churchill Livingstone)
Hotz M M Gnoinski W M Nussbaumer H and Kistler E 1978 Early orthopaedics in CLPcases guidelines for surgery Cleft Palate Journal 15 405ndash411
Hutters B and Brondsted K 1987 Strategies in cleft palate with special reference to DanishCleft Palate Journal 24 127ndash136
Isshiki N and Ringel R 1964 Airow during the production of selected consonants Journal ofSpeech and Hearing Research 7 233ndash244
Kummer A W Curtis C Wiggs M Lee L and Strife J L 1992 Comparison of velopharyngealgap size in patients with hypernasality hypernasality with nasal emission and nasal emissionor nasal turbulence (rustle) as the primary speech characteristic Cleft-palate-Craniofacial Journal29 152ndash156
Lancaster G and Pope L 1989 Working with Childrenrsquos Phonology (Oxford Winslow)Morley M E 1970 Cleft Palate and Speech (7th edition) (Edinburgh Churchill Livingstone)Russell V J 1991 Speech Development in Children with Cleft Lip and Palate Unpublished PhD
thesis Leicester PolytechnicRussell V J and Grunwell P 1993 Speech development in children with cleft lip and palate In
P Grunwell (Ed) Analysing Cleft Palate Speech (London Whurr)Sell D A and Grunwell P 1990 Speech results following late palatal surgery in previously
unoperated Sri Lankan adolescents with cleft palate Cleft Palate Journal 27 162ndash168Sell D Harding A and Grunwell P 1994 GOSSPASS A screening assessment of cleft palate
speech European Journal of Disorders of Communication 29 1ndash15Sell D Harding A and Grunwell P 1998 GOSSPASSrsquo98 An assessment for speech disorders
associated with cleft palate andor velopharyngeal dysfunction International Journal of Languageamp Communication Disorders ( in press)
Shorter E 1995 A spectographic analyis of child homophones Unpublished honours project DeMontfort University Leicester
Stenglehoffen J 1989 Nature and causes of communication diYculties In J Stengelhofen (Ed)Cleft Palate Nature and Remediation of Communication Problems (Edinburgh Churchill Livingstone)
Trost J E 1981 Articulatory additions to the classical description of the speech of persons withcleft palate Cleft Palate Journal 18
Trost-Cardamone J E 1990 The development of speech assessing cleft palate misarticulationsIn D A Kernahan and S N Rosenstein (Eds) Cleft Lip and Palate A System of Management(Baltimore Williams amp Wilkins)
A Harding and P Grunwell352
Appendix Active passive analysis of cleft palate speech

Active versus passive cleft-type speech characteristics 349
examples are given here by way of illustration of ways to eVect the rst twoprocesses of change which may need to be approached diVerently in cleft palateversus non-cleft speech disorders DiVerent approaches may also be appropriate formodifying active versus passive cleft-type processes
Innovation production of new targets Some useful principles
(1) Introduction of new lsquonon-speech likersquo targets in sound play using a conson-ant sound segment model such as [ph ] note not a syllable like [p] whichis the type of pronunciation used when target sounds are presented as lettersfor reading Target [s] might be introduced as a lsquoTrain Slowing Down Noisersquo[ts ts ts tssssssss]
(2) lsquoNew consonantsrsquo can later be modelled and elicited in soft productions ofsyllable structure [tssssndashi] [ indashtssss] which can subsequently be identi ed assimilar to words lsquosearsquo and lsquoeatsrsquo
(3) lsquoDeferring responsibilityrsquo transfers responsibility or lsquoblamersquo for errors fromthe child and attributes it to the articulators eg lsquoyour tongue is havingtrouble with hellip rsquo lsquoLetrsquos show your tongue how to hellip rsquo
(4) New targets can be modelled repeatedly and recorded on audio or videotape which can be listened to at home
(5) Targeting classes of consonants (eg alveolars t d s n l voiceless fricativesf s S perhaps with aVricate T avoids phonological confusion whichmight occur if production ofsis achieved whilst other alveolar targetsremain backed The risk is that s might not integrate into the phonologicalsystem unless all backed alveolar consonants are destabilized
(6) Increased eye contact during auditory and production work can be invaluablein holding visual and auditory attention and ensures that visual informationabout the sound has been processed This is easily achieved by the clinicianlifting any focus of the childrsquos attention close to hisher mouth at theprecise moment when the target is modelled
Stimulation of non-speech related sounds such as a lsquoTrain Slowing DownNoisersquo [ts ts tsss] con rms that target [s] is physically achievable whether or not[ssss] can be imitated Some children continue to access [s] through the lsquoTrainSlowing Down Noisersquo throughout therapy until it is occurring spontaneouslywithout conscious planning This can be an eVective means of underminingestablished motor programmers (Hewlett 1990) for active cleft-type processes
Destabilizing active processes
As it is likely that children will be unaware of each occurrence of their alternativearticulatory pattern for speci c consonant errors it is preferrable to destabilizeactive processes with minimal conscious eVort by the child As children becomeaware of their mismatches they frequently add the newly acquired target realizationto their existing production eg target word tu childrsquos old realization [ku] childrsquoscorrected realization [t-ku] Destabilization can be achieved with minimal consciouseVort through input therapy techniques such as auditory bombardment (Lancasterand Pope 1989) auditory decision-making such as lsquowhich bear says this wordproperlyrsquo Red Bear says lsquotworsquo or Blue Bear says lsquocoorsquo This type of strategy oftenprecipitates attention to the target consonant with possible lsquoreplayrsquo and lsquoreviewrsquo of
A Harding and P Grunwell350
their own production Frequent stimulation of cognitive alertness to the targetconsonant can develop awareness without confronting the child with errors orrisking hisher failure The child is then free to attempt to repair hisher ownrealization to continue to re ect and to silently rehearse the adult realizationTraditional articulation therapy is thus combined with development of metaphonol-ogical skills ie the ability to re ect upon onersquos own speech production The resultshould be that new target realizations will be more phonologically stable thanexclusively production-based articulation therapy might have facilitated
Stabilizationgeneralization
Procedures to ensure stabilization and generalization of new target consonantswould be as described by Grunwell (1992) Success may be constrained by theconsiderable articulatory eVort sometimes required to maintain pressure consonantproduction in spontaneous speech (Harding and Grunwell 1993)
Conclusions
In speech assessment it is helpful to distinguish between errors which are cleft-type and non-cleft type and those which are part of active versus passive processesThe active and passive processes have been de ned and their phonological implica-tions discussed Focus on active and passive processes has facilitated focus on thephonological consequences of cleft palate on speech development In the futureawareness of the likely eVect of a cleft palate on normal phonological developmentcould avoid extended periods of unsuccessful clinical intervention Furthermoresensitivity to the relationship between phonological processes and structural con-straints should facilitate theoretically based management decisions Incidences suchas the case of CP in which nasal realizations were thought to indicate VPI but weresubsequently unaVected by surgery might be avoided if phonological analysiscontributes to management decisions
Surgery did improve hypernasal resonance and eliminated passive processes buthad little eVect on active processes Active processes in younger subjects werethought to require therapeutic intervention but in the longer term the oldersubjects showed few cleft-type processes Whilst it is possible that active cleft-typeprocesses may resolve with increasing age the implication for the future is thatactive cleft-type processes should be treated with skilled therapeutic interventionnot surgery Therapy which addresses the phonological consequences of cleft palateon speech development by combining metaphonologicalphonologicalarticulatoryapproaches is likely to be successful
References
Albery E 1991 Consonant articulation in the diVerent types of cleft lip and palate UnpublishedMPhil thesis Leicester Polytechnic
Albery E and Grunwell P 1993 Consonant articulation in diVerent types of cleft palate InP Grunwell (Ed) Analysing Cleft Palate Speech (London Whurr)
Ferguson C A 1978 Fricatives in child language acquisition In V Honsa and M Hardmann-Battista (Eds) Papers on Linguistics and Child Language (Mouton The Hague)
Fletcher S G 1985 Speech production and oral motor skill in an adult with an unrepaired palatalcleft Journal of Speech and Hearing Disorders 50 254ndash261
Active versus passive cleft-type speech characteristics 351
Golding-Kushner K J 1995 Treatment of articulation and resonancne disorders associated withcleft palate management and VPI In R Shprintzen (Ed) Cleft Palate Speech Management AMultidisciplinary Approach (St Louis Mosby)
Grundy K and Harding A 1995 Developmental speech disorders In K Grundy (Ed) Linguisticsin Clinical Practice (2nd edition) (London Whurr)
Grunwell P 1985 Phonological Assessment of Child Speech (Windsor NFER-Nelson)Grunwell P 1987a Clinical Phonology (2nd edition) (London Croom Helm)Grunwell P 1987b PACS Pictures Language Elicitation Materials (Windsor NFER-Nelson)Grunwell P 1991 Processes of phonological change in developmental speech disorders Clinical
Linguistics and Phonetics 6 101ndash122Grunwell P 1992 Principled decision making in the remediation of children with phonological
disorders In P Fletcher and D Hall (Eds) Specic Speech and Language Disorders in Children(London Whurr)
Grunwell P and Harding A 1995 PACSTOYS A Screening Assessment of Phonological Development(Windsor NFER-Nelson)
Grunwell P and Harding A 1996 A note on describing types of nasality Clinical Linguistics andPhonetics 10 157ndash161
Harding A 1993 An Investigation into the Relationship Between Timing of Cleft Palate Repairand Speech Development Unpublished PhD thesis
Harding A and Grunwell P 1993 The relationship between speech and timing of hard palaterepair In P Grunwell (Ed) Analysisng Cleft Palate Speech (London Whurr)
Harding A and Grunwell P 1996 Characteristics of cleft palate speech European Journal ofDisorders of Communication 31 331ndash358
Henningsson G and Isberg A M 1986 Velopharyngeal movement patterns in patients alternatingbetween oral and glottal articulation A clinical and cineradiographicical study Cleft Palate Journal23 1ndash9
Hewlett N 1990 Processes of development and production In P Grunwell (Ed) DevelopmentalSpeech Disorders (Edinburgh Churchill Livingstone)
Hotz M M Gnoinski W M Nussbaumer H and Kistler E 1978 Early orthopaedics in CLPcases guidelines for surgery Cleft Palate Journal 15 405ndash411
Hutters B and Brondsted K 1987 Strategies in cleft palate with special reference to DanishCleft Palate Journal 24 127ndash136
Isshiki N and Ringel R 1964 Airow during the production of selected consonants Journal ofSpeech and Hearing Research 7 233ndash244
Kummer A W Curtis C Wiggs M Lee L and Strife J L 1992 Comparison of velopharyngealgap size in patients with hypernasality hypernasality with nasal emission and nasal emissionor nasal turbulence (rustle) as the primary speech characteristic Cleft-palate-Craniofacial Journal29 152ndash156
Lancaster G and Pope L 1989 Working with Childrenrsquos Phonology (Oxford Winslow)Morley M E 1970 Cleft Palate and Speech (7th edition) (Edinburgh Churchill Livingstone)Russell V J 1991 Speech Development in Children with Cleft Lip and Palate Unpublished PhD
thesis Leicester PolytechnicRussell V J and Grunwell P 1993 Speech development in children with cleft lip and palate In
P Grunwell (Ed) Analysing Cleft Palate Speech (London Whurr)Sell D A and Grunwell P 1990 Speech results following late palatal surgery in previously
unoperated Sri Lankan adolescents with cleft palate Cleft Palate Journal 27 162ndash168Sell D Harding A and Grunwell P 1994 GOSSPASS A screening assessment of cleft palate
speech European Journal of Disorders of Communication 29 1ndash15Sell D Harding A and Grunwell P 1998 GOSSPASSrsquo98 An assessment for speech disorders
associated with cleft palate andor velopharyngeal dysfunction International Journal of Languageamp Communication Disorders ( in press)
Shorter E 1995 A spectographic analyis of child homophones Unpublished honours project DeMontfort University Leicester
Stenglehoffen J 1989 Nature and causes of communication diYculties In J Stengelhofen (Ed)Cleft Palate Nature and Remediation of Communication Problems (Edinburgh Churchill Livingstone)
Trost J E 1981 Articulatory additions to the classical description of the speech of persons withcleft palate Cleft Palate Journal 18
Trost-Cardamone J E 1990 The development of speech assessing cleft palate misarticulationsIn D A Kernahan and S N Rosenstein (Eds) Cleft Lip and Palate A System of Management(Baltimore Williams amp Wilkins)
A Harding and P Grunwell352
Appendix Active passive analysis of cleft palate speech

A Harding and P Grunwell350
their own production Frequent stimulation of cognitive alertness to the targetconsonant can develop awareness without confronting the child with errors orrisking hisher failure The child is then free to attempt to repair hisher ownrealization to continue to re ect and to silently rehearse the adult realizationTraditional articulation therapy is thus combined with development of metaphonol-ogical skills ie the ability to re ect upon onersquos own speech production The resultshould be that new target realizations will be more phonologically stable thanexclusively production-based articulation therapy might have facilitated
Stabilizationgeneralization
Procedures to ensure stabilization and generalization of new target consonantswould be as described by Grunwell (1992) Success may be constrained by theconsiderable articulatory eVort sometimes required to maintain pressure consonantproduction in spontaneous speech (Harding and Grunwell 1993)
Conclusions
In speech assessment it is helpful to distinguish between errors which are cleft-type and non-cleft type and those which are part of active versus passive processesThe active and passive processes have been de ned and their phonological implica-tions discussed Focus on active and passive processes has facilitated focus on thephonological consequences of cleft palate on speech development In the futureawareness of the likely eVect of a cleft palate on normal phonological developmentcould avoid extended periods of unsuccessful clinical intervention Furthermoresensitivity to the relationship between phonological processes and structural con-straints should facilitate theoretically based management decisions Incidences suchas the case of CP in which nasal realizations were thought to indicate VPI but weresubsequently unaVected by surgery might be avoided if phonological analysiscontributes to management decisions
Surgery did improve hypernasal resonance and eliminated passive processes buthad little eVect on active processes Active processes in younger subjects werethought to require therapeutic intervention but in the longer term the oldersubjects showed few cleft-type processes Whilst it is possible that active cleft-typeprocesses may resolve with increasing age the implication for the future is thatactive cleft-type processes should be treated with skilled therapeutic interventionnot surgery Therapy which addresses the phonological consequences of cleft palateon speech development by combining metaphonologicalphonologicalarticulatoryapproaches is likely to be successful
References
Albery E 1991 Consonant articulation in the diVerent types of cleft lip and palate UnpublishedMPhil thesis Leicester Polytechnic
Albery E and Grunwell P 1993 Consonant articulation in diVerent types of cleft palate InP Grunwell (Ed) Analysing Cleft Palate Speech (London Whurr)
Ferguson C A 1978 Fricatives in child language acquisition In V Honsa and M Hardmann-Battista (Eds) Papers on Linguistics and Child Language (Mouton The Hague)
Fletcher S G 1985 Speech production and oral motor skill in an adult with an unrepaired palatalcleft Journal of Speech and Hearing Disorders 50 254ndash261
Active versus passive cleft-type speech characteristics 351
Golding-Kushner K J 1995 Treatment of articulation and resonancne disorders associated withcleft palate management and VPI In R Shprintzen (Ed) Cleft Palate Speech Management AMultidisciplinary Approach (St Louis Mosby)
Grundy K and Harding A 1995 Developmental speech disorders In K Grundy (Ed) Linguisticsin Clinical Practice (2nd edition) (London Whurr)
Grunwell P 1985 Phonological Assessment of Child Speech (Windsor NFER-Nelson)Grunwell P 1987a Clinical Phonology (2nd edition) (London Croom Helm)Grunwell P 1987b PACS Pictures Language Elicitation Materials (Windsor NFER-Nelson)Grunwell P 1991 Processes of phonological change in developmental speech disorders Clinical
Linguistics and Phonetics 6 101ndash122Grunwell P 1992 Principled decision making in the remediation of children with phonological
disorders In P Fletcher and D Hall (Eds) Specic Speech and Language Disorders in Children(London Whurr)
Grunwell P and Harding A 1995 PACSTOYS A Screening Assessment of Phonological Development(Windsor NFER-Nelson)
Grunwell P and Harding A 1996 A note on describing types of nasality Clinical Linguistics andPhonetics 10 157ndash161
Harding A 1993 An Investigation into the Relationship Between Timing of Cleft Palate Repairand Speech Development Unpublished PhD thesis
Harding A and Grunwell P 1993 The relationship between speech and timing of hard palaterepair In P Grunwell (Ed) Analysisng Cleft Palate Speech (London Whurr)
Harding A and Grunwell P 1996 Characteristics of cleft palate speech European Journal ofDisorders of Communication 31 331ndash358
Henningsson G and Isberg A M 1986 Velopharyngeal movement patterns in patients alternatingbetween oral and glottal articulation A clinical and cineradiographicical study Cleft Palate Journal23 1ndash9
Hewlett N 1990 Processes of development and production In P Grunwell (Ed) DevelopmentalSpeech Disorders (Edinburgh Churchill Livingstone)
Hotz M M Gnoinski W M Nussbaumer H and Kistler E 1978 Early orthopaedics in CLPcases guidelines for surgery Cleft Palate Journal 15 405ndash411
Hutters B and Brondsted K 1987 Strategies in cleft palate with special reference to DanishCleft Palate Journal 24 127ndash136
Isshiki N and Ringel R 1964 Airow during the production of selected consonants Journal ofSpeech and Hearing Research 7 233ndash244
Kummer A W Curtis C Wiggs M Lee L and Strife J L 1992 Comparison of velopharyngealgap size in patients with hypernasality hypernasality with nasal emission and nasal emissionor nasal turbulence (rustle) as the primary speech characteristic Cleft-palate-Craniofacial Journal29 152ndash156
Lancaster G and Pope L 1989 Working with Childrenrsquos Phonology (Oxford Winslow)Morley M E 1970 Cleft Palate and Speech (7th edition) (Edinburgh Churchill Livingstone)Russell V J 1991 Speech Development in Children with Cleft Lip and Palate Unpublished PhD
thesis Leicester PolytechnicRussell V J and Grunwell P 1993 Speech development in children with cleft lip and palate In
P Grunwell (Ed) Analysing Cleft Palate Speech (London Whurr)Sell D A and Grunwell P 1990 Speech results following late palatal surgery in previously
unoperated Sri Lankan adolescents with cleft palate Cleft Palate Journal 27 162ndash168Sell D Harding A and Grunwell P 1994 GOSSPASS A screening assessment of cleft palate
speech European Journal of Disorders of Communication 29 1ndash15Sell D Harding A and Grunwell P 1998 GOSSPASSrsquo98 An assessment for speech disorders
associated with cleft palate andor velopharyngeal dysfunction International Journal of Languageamp Communication Disorders ( in press)
Shorter E 1995 A spectographic analyis of child homophones Unpublished honours project DeMontfort University Leicester
Stenglehoffen J 1989 Nature and causes of communication diYculties In J Stengelhofen (Ed)Cleft Palate Nature and Remediation of Communication Problems (Edinburgh Churchill Livingstone)
Trost J E 1981 Articulatory additions to the classical description of the speech of persons withcleft palate Cleft Palate Journal 18
Trost-Cardamone J E 1990 The development of speech assessing cleft palate misarticulationsIn D A Kernahan and S N Rosenstein (Eds) Cleft Lip and Palate A System of Management(Baltimore Williams amp Wilkins)
A Harding and P Grunwell352
Appendix Active passive analysis of cleft palate speech

Active versus passive cleft-type speech characteristics 351
Golding-Kushner K J 1995 Treatment of articulation and resonancne disorders associated withcleft palate management and VPI In R Shprintzen (Ed) Cleft Palate Speech Management AMultidisciplinary Approach (St Louis Mosby)
Grundy K and Harding A 1995 Developmental speech disorders In K Grundy (Ed) Linguisticsin Clinical Practice (2nd edition) (London Whurr)
Grunwell P 1985 Phonological Assessment of Child Speech (Windsor NFER-Nelson)Grunwell P 1987a Clinical Phonology (2nd edition) (London Croom Helm)Grunwell P 1987b PACS Pictures Language Elicitation Materials (Windsor NFER-Nelson)Grunwell P 1991 Processes of phonological change in developmental speech disorders Clinical
Linguistics and Phonetics 6 101ndash122Grunwell P 1992 Principled decision making in the remediation of children with phonological
disorders In P Fletcher and D Hall (Eds) Specic Speech and Language Disorders in Children(London Whurr)
Grunwell P and Harding A 1995 PACSTOYS A Screening Assessment of Phonological Development(Windsor NFER-Nelson)
Grunwell P and Harding A 1996 A note on describing types of nasality Clinical Linguistics andPhonetics 10 157ndash161
Harding A 1993 An Investigation into the Relationship Between Timing of Cleft Palate Repairand Speech Development Unpublished PhD thesis
Harding A and Grunwell P 1993 The relationship between speech and timing of hard palaterepair In P Grunwell (Ed) Analysisng Cleft Palate Speech (London Whurr)
Harding A and Grunwell P 1996 Characteristics of cleft palate speech European Journal ofDisorders of Communication 31 331ndash358
Henningsson G and Isberg A M 1986 Velopharyngeal movement patterns in patients alternatingbetween oral and glottal articulation A clinical and cineradiographicical study Cleft Palate Journal23 1ndash9
Hewlett N 1990 Processes of development and production In P Grunwell (Ed) DevelopmentalSpeech Disorders (Edinburgh Churchill Livingstone)
Hotz M M Gnoinski W M Nussbaumer H and Kistler E 1978 Early orthopaedics in CLPcases guidelines for surgery Cleft Palate Journal 15 405ndash411
Hutters B and Brondsted K 1987 Strategies in cleft palate with special reference to DanishCleft Palate Journal 24 127ndash136
Isshiki N and Ringel R 1964 Airow during the production of selected consonants Journal ofSpeech and Hearing Research 7 233ndash244
Kummer A W Curtis C Wiggs M Lee L and Strife J L 1992 Comparison of velopharyngealgap size in patients with hypernasality hypernasality with nasal emission and nasal emissionor nasal turbulence (rustle) as the primary speech characteristic Cleft-palate-Craniofacial Journal29 152ndash156
Lancaster G and Pope L 1989 Working with Childrenrsquos Phonology (Oxford Winslow)Morley M E 1970 Cleft Palate and Speech (7th edition) (Edinburgh Churchill Livingstone)Russell V J 1991 Speech Development in Children with Cleft Lip and Palate Unpublished PhD
thesis Leicester PolytechnicRussell V J and Grunwell P 1993 Speech development in children with cleft lip and palate In
P Grunwell (Ed) Analysing Cleft Palate Speech (London Whurr)Sell D A and Grunwell P 1990 Speech results following late palatal surgery in previously
unoperated Sri Lankan adolescents with cleft palate Cleft Palate Journal 27 162ndash168Sell D Harding A and Grunwell P 1994 GOSSPASS A screening assessment of cleft palate
speech European Journal of Disorders of Communication 29 1ndash15Sell D Harding A and Grunwell P 1998 GOSSPASSrsquo98 An assessment for speech disorders
associated with cleft palate andor velopharyngeal dysfunction International Journal of Languageamp Communication Disorders ( in press)
Shorter E 1995 A spectographic analyis of child homophones Unpublished honours project DeMontfort University Leicester
Stenglehoffen J 1989 Nature and causes of communication diYculties In J Stengelhofen (Ed)Cleft Palate Nature and Remediation of Communication Problems (Edinburgh Churchill Livingstone)
Trost J E 1981 Articulatory additions to the classical description of the speech of persons withcleft palate Cleft Palate Journal 18
Trost-Cardamone J E 1990 The development of speech assessing cleft palate misarticulationsIn D A Kernahan and S N Rosenstein (Eds) Cleft Lip and Palate A System of Management(Baltimore Williams amp Wilkins)
A Harding and P Grunwell352
Appendix Active passive analysis of cleft palate speech

A Harding and P Grunwell352
Appendix Active passive analysis of cleft palate speech
Recommended