Nosocomial PneumoniaEpidemiology
Common hospital-acquired infectionOccurs at a rate of approximately 5-10 cases per 1000
hospital admissionsIncidence increases by 6-20 fold in patients being
ventilated mechanically. One study suggested that the risk for developing VAP
increases 1% per dayAnother study suggested, highest risk occur in the first 5
days after intubation

Nosocomial Pneumonia
Copyright © 2001 ican, INC.
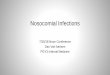
Richards, et al. Crit Care Med. 1999;27:887-892.
Site Distribution in Adult ICUsMajor Types of Infection (NNIS data, 1992-1997)
27%
GI
CVS
Other
Pneu
31%4%
4%
EENT
BSI19%
5%
6%LRTI 4%
UTI
Urinary tract infections (UTI)
Pneumonia (Pneu)
Primary bloodstream infections (BSI)
Gastrointestinal infections (GI)
Cardiovascular system (CVS)
Eye, ear, nose, and throat infection (EENT)
Lower respiratory infections (LRTI) (other than pneumonia)
OtherN = 14,177

Nosocomial PneumoniaEpidemiologyNosocomial pneumonia is the leading cause of
death due to hospital acquired infectionsAssociated with substantial morbidity Has an associated crude mortality of 30-50%Hospital stay increases by 7-9 days per patient Estimated cost > 1 billion dollars/year

Nosocomial PneumoniaHence, the importance of focusing on:
Accurate diagnosisAppropriate treatmentPreventive measures

Nosocomial PneumoniaPathogenesisRisk factorsEtiologic agentsDifferential diagnosisTreatment Prevention

Pathogenesis

Nosocomial PneumoniaMicroaspiration may occur in up to 45% of
healthy volunteers during sleepOropharynx of hospitalized patients is
colonized with GNR in 35-75% of patients depending on the severity and type of underlying illness
Multiple factors are associated with higher risk of colonization with pathogenic bacteria and higher risk of aspiration

Nosocomial PneumoniaPathogenesis
Invasion of the lower respiratory tract by: Aspiration of oropharyngeal/GI organisms Inhalation of aerosols containing bacteria Hematogenous spread


Colonization Aspiration
HAP
MRSA*

Risk Factors

Nosocomial PneumoniaRisk Factors
Host Factors Extremes of age, severe acute or chronic illnesses,
immunosupression, coma, alcoholism, malnutrition, COPD, DM
Factors that enhance colonization of the oropharynx and stomach by pathogenic microorganisms admission to an ICU, administration of antibiotics,
chronic lung disease, endotracheal intubation, etc.

Nosocomial PneumoniaRisk Factors
Conditions favoring aspiration or reflux Supine position, depressed consciousness, endotracheal
intubation, insertion of nasogastric tubeMechanical ventilation
Impaired mucociliary function, injury of mucosa favoring bacterial binding, pooling of secretions in the subglottic area, potential exposure to contaminated respiratory equipment and contact with contaminated or colonized hands of HCWs
Factors that impede adequate pulmonary toilet Surgical procedures that involve the head and neck,
being immobilized as a result of trauma or illness, sedation etc.

Etiologic Agents

Nosocomial PneumoniaEtiologic Agents
S.aureusEnterobacteriaceaeP.aeruginosaAcinetobacter sp.PolymicrobialAnaerobic bacteriaLegionella sp.Aspergillus sp.Viral

Diagnosis

Nosocomial PneumoniaDiagnosis
Not necessarily easy to accurately diagnose HAPCriteria frequently include:
Clinical fever ; cough with purulent sputum,
Radiographic new or progressive infiltrates on CXR,
Laboratorial leukocytosis or leukopenia
Microbiologic Suggestive gram stain and positive cultures of sputum,
tracheal aspirate, BAL, bronchial brushing, pleural fluid or blood
Quantitative cultures

Nosocomial PneumoniaProblems
All above criteria fairly sensitive, but very non- specific, particularly in mechanically ventilated patients
Other criteria/problems include Positive cultures of blood and pleural fluid plus clinical
findings (specific but poor sensitivity) Rapid cavitation of pulmonary infiltrate absent Tb or
cancer (rare) Histopathologic examination of lung tissue (invasive)

Nosocomial pneumonia
Bronchoscopically Directed Techniques for diagnosis of VAP and Quantitative culturesBronchoscopy with BAL/bronchial brushings (10,000 to
100,000 CFU/ml and less than 1% of squamous cells)
Protected specimen brush method (>10³ CFU/ml)
Protected BAL with a balloon tipped catheter (>5% of neutrophils or macrophages with intracellular organisms on a Wright-Giemsa stain)

Nosocomial pneumonia
Multiple studies looked into the accuracy of quantitative culture and microscopic examination of LRT secretions as compared to histopathologic examination and tissue cultures (either lung biopsy or immediate post mortem obtained samples)
Several trials conclude that use of FOB techniques and quantitative cultures are more accurate
At least 4 studies concluded that bronchoscopically directed techniques were not more accurate for diagnosis of VAP than clinical and X-ray criteria, combined with cultures of tracheal aspirate
Therefore no gold standard criteria exist

Nosocomial PneumoniaDifferential diagnosis
ARDSPulmonary edemaPulmonary embolismAtelectasisAlveolar hemorrhageLung contusion

Treatment

Nosocomial PneumoniaAntimicrobial Treatment
Broad spectrum penicillins3rd and 4th generation cephalosporinsCarbapenemsQuinolones AminoglycosidesVancomycinLinezolid

Inadequate
Antibiotic
Therapy
Antibiotic
Resistance

Nosocomial PneumoniaDuration of antimicrobial treatment
Optimal duration of treatment has not been established
Most experts recommend 14-21 days of treatment
Recent data support shorter treatment regimens (8 days)

Prevention

Nosocomial PneumoniaPreventive Measures
Incentive spirometryPromote early ambulationAvoid CNS depressantsDecrease duration of immunosupressionInfection control measuresEducate and train personnel

Nosocomial PneumoniaPreventive Measures
Avoid prolonged nasal intubationSuction secretionsSemi-recumbent position( 30-45°head
elevation)Do not change ventilator circuits routinely
more often than every 48 hoursDrain and discard tubing condensateUse sterile water for respiratory humidifying
devicesSubglottic secretions drainage

Craven, et al. Chest. 1995;108:s1-s16.

Nosocomial PneumoniaPreventive Measures
Remove NGT when no longer neededAvoid gastric overdistentionStress ulcer prophylaxis:
sulcrafate; antacids; H2 receptor antagonistsAcidification of enteral feedingsProphylactic antibiotics
Inhaled antibiotics Selective digestive decontamination
Chlorexidine oral rinsesVaccines ( Influenza; Strep.pneumoniae)
Recommended
















![Nosocomial Pneumonia: [Print] - eMedicine Infectious Diseases](https://img.pdfslide.us/doc/110x75/613cffa50c37c14a830ceb8a/nosocomial-pneumonia-print-emedicine-infectious-diseases.jpg)