• No conflict of interest
DECLARATION OF CONFLICT OF INTEREST
Whole body MR-
angiography
Deniz Bilecen, MD, PhD
Kantonsspital Bruderholz, Schweiz ESC 2011
- Motivation: Why Whole body MR angiography ?
- Technical setup: MR scanner and contrast agent
- WB MR-angiography: Some examples
- Take Home Message
- Technical drawbacks
Overview:
Why is a comprehensive assessment of the underlying vascular
pathology required to manage atherosclerotic disease adequately ?
Patients with CAD and PAOD have greater morbidity and mortality
among patients. Patients with CAD and PAOD had a greater risk of cerebral
vascular accidents after myocardial revasculariiation and a 25% increase in
mortality. Higgins TL, et al.JAMA 1992;267:2344-2348.
Peripheral arterial occlusive disease (PAD) in patients with coronary
artery Disease (cAD) compromises the recovery and postoperative (post-
interventional ?) quality of life of patients who undergo myocardial
revascularization). Nikolsky E, et al. Am. J. Cardiol 2004; 93:1536-1539.
Early identification of PAOD by vascular surgens in patients with CAD
is fundamental to reduce morbidity and mortality Eagle KA, et al. J. Am Coll Cardiol 1994
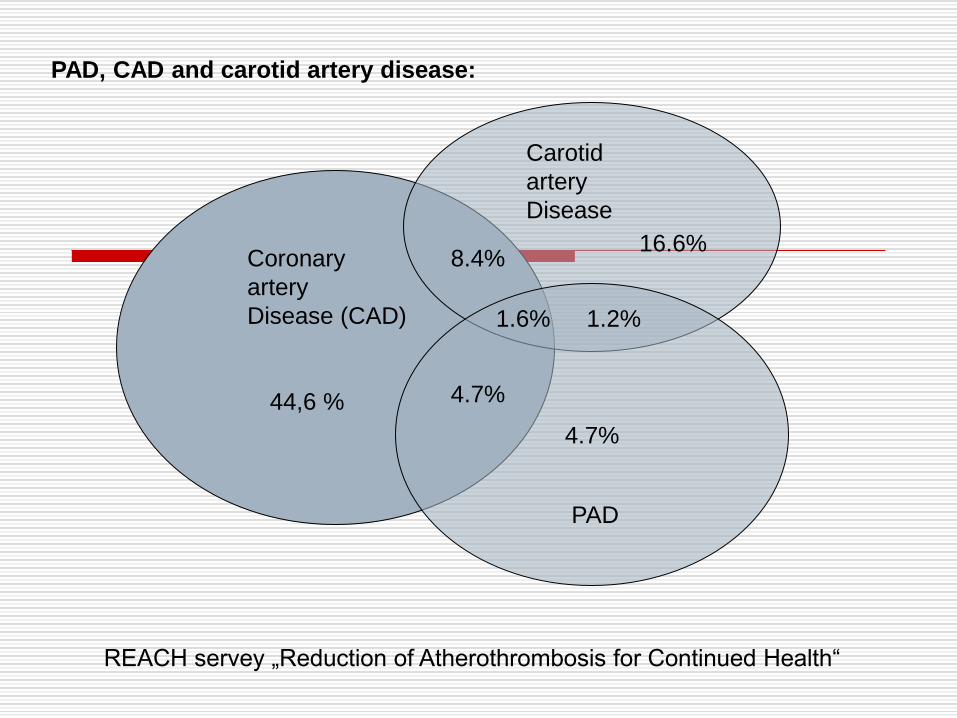
4.7%
44,6 %
16.6%
4.7%
1.2% 1.6%
REACH servey „Reduction of Atherothrombosis for Continued Health“
Coronary
artery
Disease (CAD)
PAD
Carotid
artery
Disease
PAD, CAD and carotid artery disease:
8.4%
4.7%
44,6 %
16.6%
4.7%
1.2% 1.6%
Coronary
artery
Disease (CAD)
PAD
Carotid
artery
Disease
8.4%
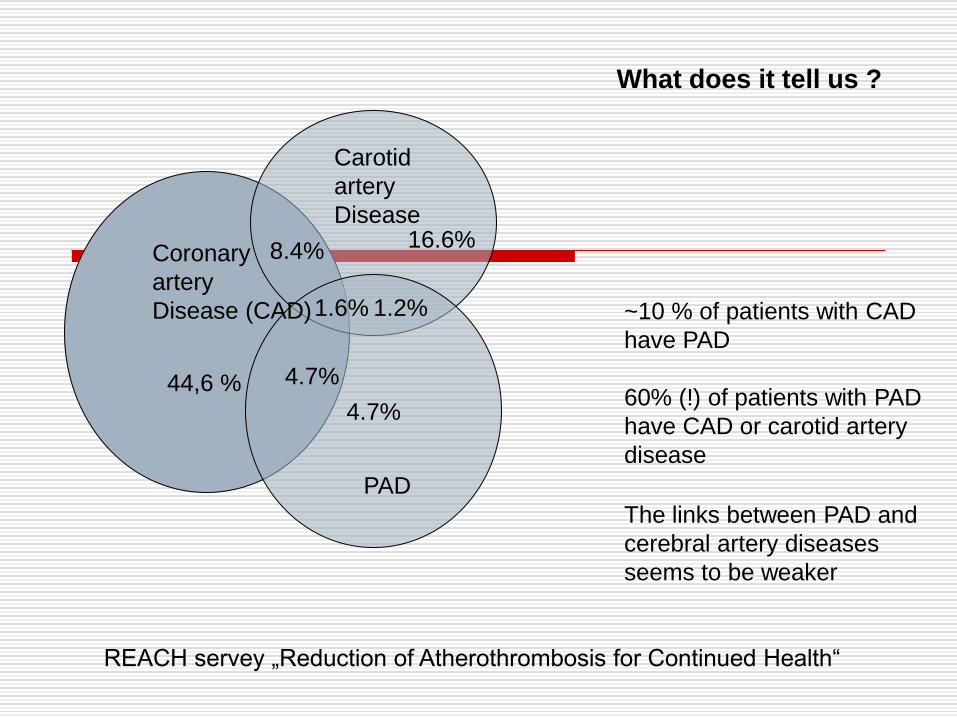
The links between PAD and
cerebral artery diseases
seems to be weaker
What does it tell us ?
~10 % of patients with CAD
have PAD
60% (!) of patients with PAD
have CAD or carotid artery
disease
REACH servey „Reduction of Atherothrombosis for Continued Health“
Imaging modalities für delineation of atherosclerosis for screening
purpose:
-Digital subraction angiography
GOLD standard, catheter technique invasive, high radation exposure.
-Duplex-doppler Sonography
lack of radiation, BUT not all vessel terretories are visible, time consuming,
operator-dependent.
-Whole Body CT angiography
Radiation exposure, BUT not all vessel terretories are visible, nephrotoxic CA.
-Whole Body MR angiography
lack of radiation, overall view - BUT not all vessel terretories are visible, +/-
nephrotoxic CA (NSF)
Whole body MR has been proposed ten years ago by Ruehm et al.
entiteled:
Rapid magnetic resonance angiograpy for detection of athererosclerosis
Lancet 2001 Apr 7;357(9262):1086-91
Whole body MRA enables the delination of the arterial vessel
system from Head to Toe using a multi-step imaging technique
+ iv.contrast agent…
Technical setup: The MR scanner
For Whole Body MR angiography standard scanner are suitable and
available at 1.5 T or 3 T
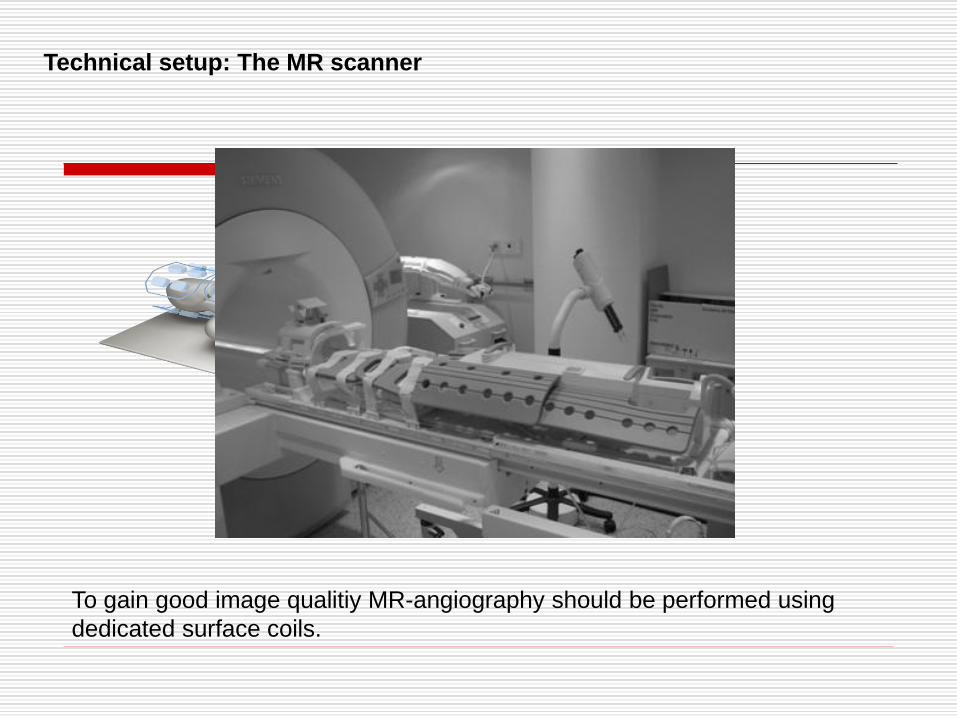
To gain good image qualitiy MR-angiography should be performed using
dedicated surface coils.
Technical setup: The MR scanner
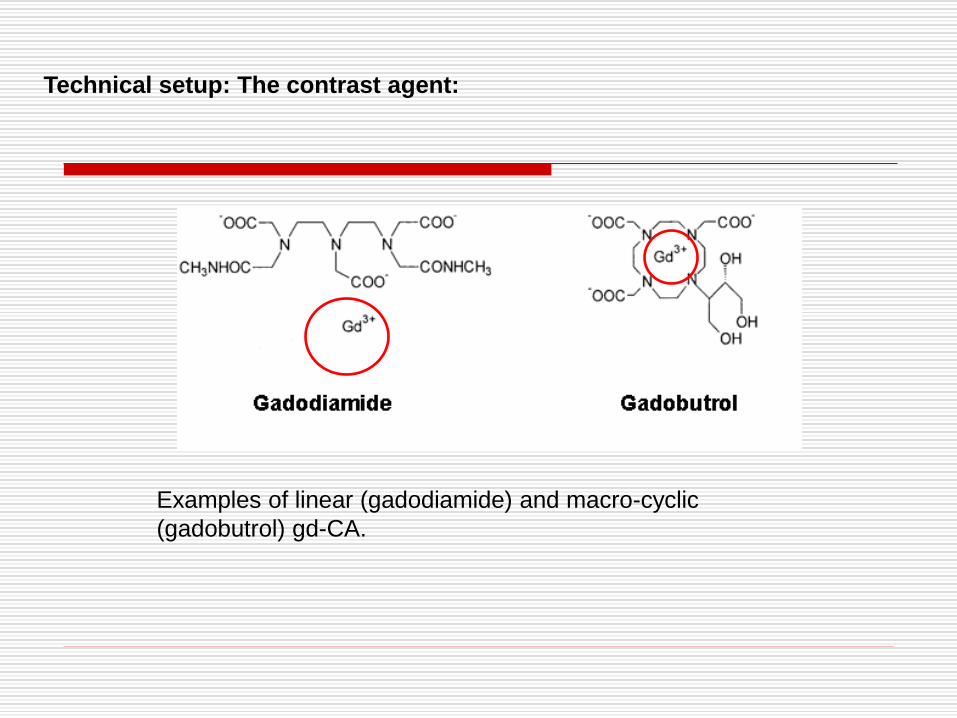
Examples of linear (gadodiamide) and macro-cyclic
(gadobutrol) gd-CA.
Technical setup: The contrast agent:

Contrast agent: CAVE nephrogenic systemic sclerosis (NSF):
NSF is a serious disabling disorder with preciable mortality. rare and serious
syndrome that involves fibrosis of skin, joints, eyes, and internal organs. Its
cause is not fully understood.
However, there is much evidence to suggest that it is associated with
exposure to gadolinium
By far the largest number of cases to date have been associates with severe,
often terminal renal function impairment requiring dialysis.
High risk group in patients with renal insufficiency: patients with eGFR values
< 30 mL/min/173m2
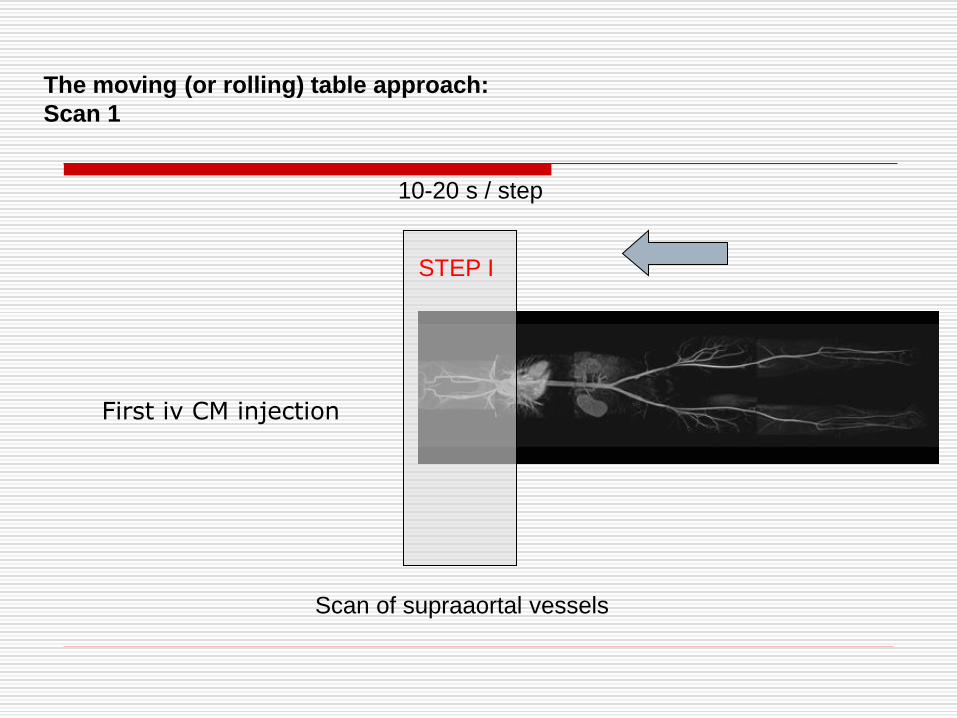
The moving (or rolling) table approach:
Scan 1
STEP I
Scan of supraaortal vessels
10-20 s / step
First iv CM injection
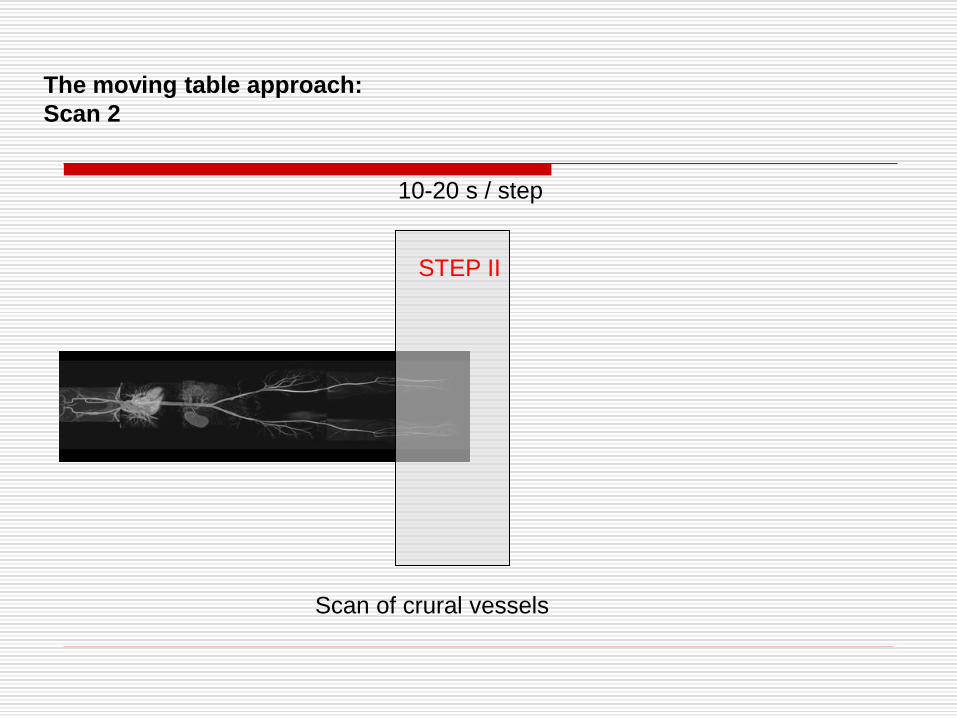
The moving table approach:
Scan 2
STEP II
10-20 s / step
Scan of crural vessels
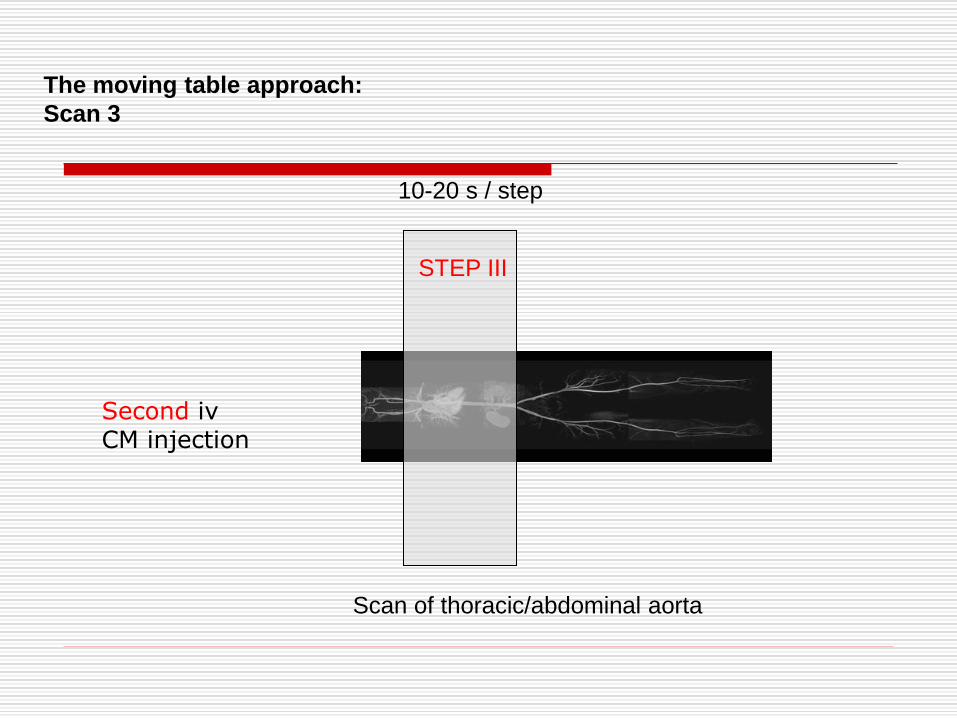
The moving table approach:
Scan 3
STEP III
10-20 s / step
Scan of thoracic/abdominal aorta
Second iv CM injection
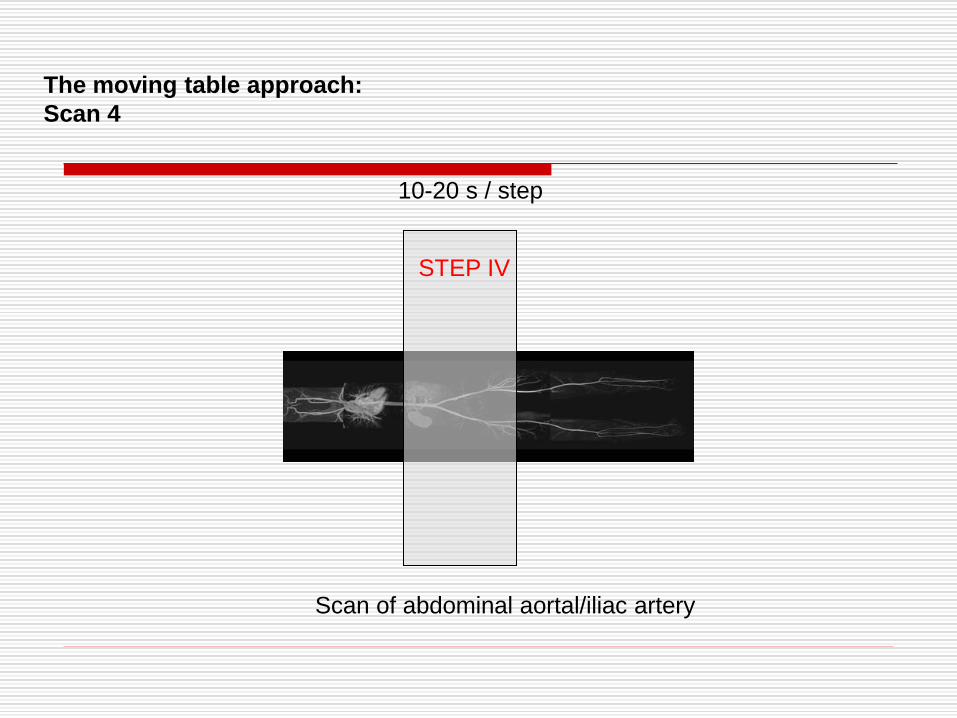
The moving table approach:
Scan 4
STEP IV
10-20 s / step
Scan of abdominal aortal/iliac artery
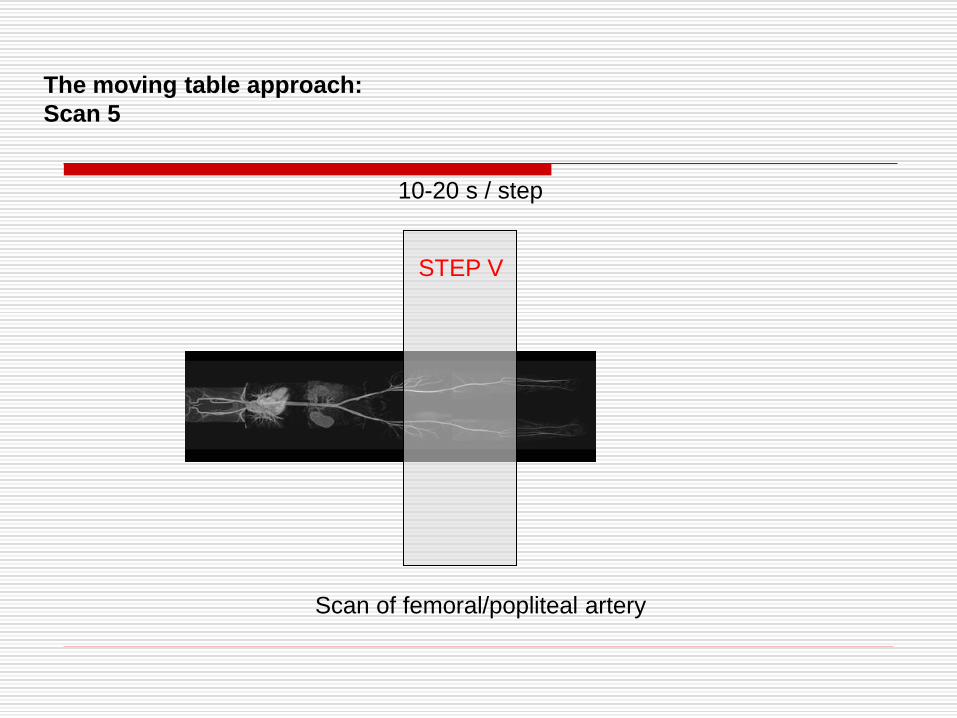
The moving table approach:
Scan 5
STEP V
10-20 s / step
Scan of femoral/popliteal artery
Whole body MRA ist something like riding a „rollercoaster“
1° injection
2° injection
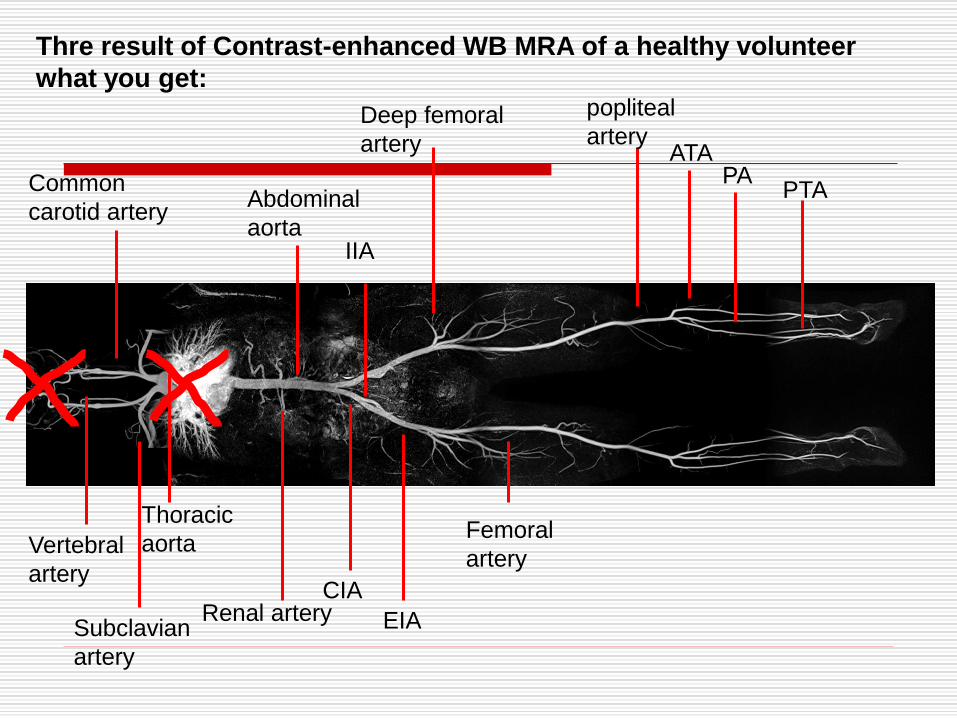
Thre result of Contrast-enhanced WB MRA of a healthy volunteer
what you get:
Common
carotid artery Abdominal
aorta
Renal artery
Deep femoral
artery
popliteal
artery
Vertebral
artery
Subclavian
artery
Thoracic
aorta
CIA
EIA
Femoral
artery
ATA PA
PTA
IIA
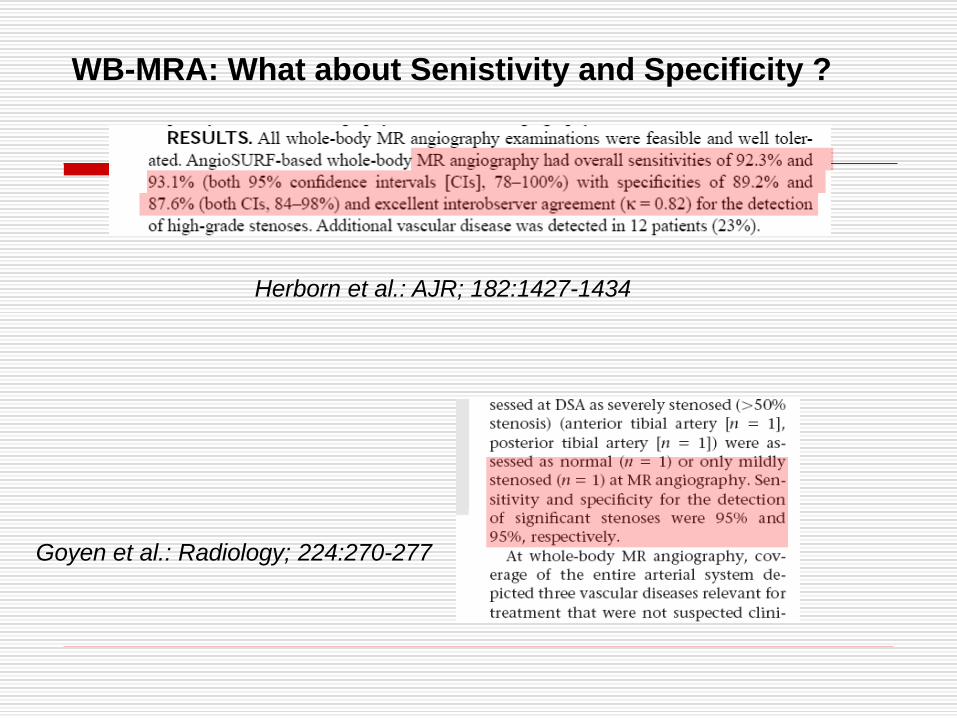
WB-MRA: What about Senistivity and Specificity ?
Herborn et al.: AJR; 182:1427-1434
Goyen et al.: Radiology; 224:270-277
Carotid artery
Thoracic and Abdominal Aorta
Renal arteries
Iliac arteries
Femoral arteries (deep and
superficial)
Crural arteries.
Not (yet)
Coronary arteries
Intracranial arteries
Good imaging quality in WB MR-Angiography is
available for the major vessel territorries of:
Whole Body MRA should provides information about the
A ) Overall burden of atherosclerosis (scoring scheme ? risk management)
B) Delineates arterial stenosis and occlusion of arteries
(+ aneurysms, + variants, roadmap for interventional planning ?)
C) Might provide additional information („overview) of the human body including
organs (kidney, liver), skelettal system etc)
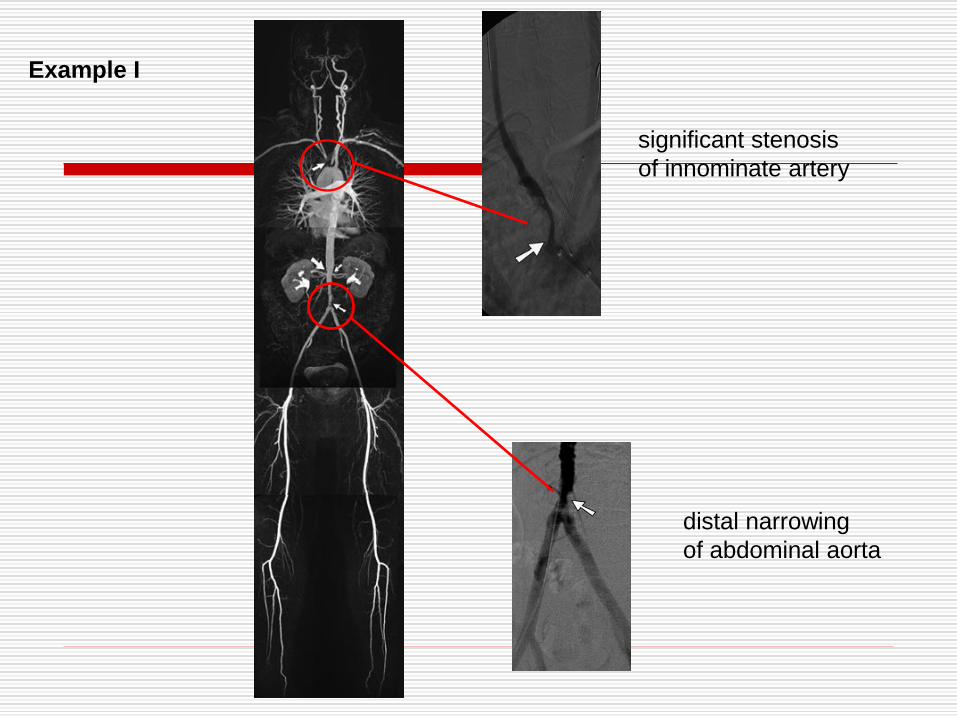
distal narrowing
of abdominal aorta
significant stenosis
of innominate artery
Example I
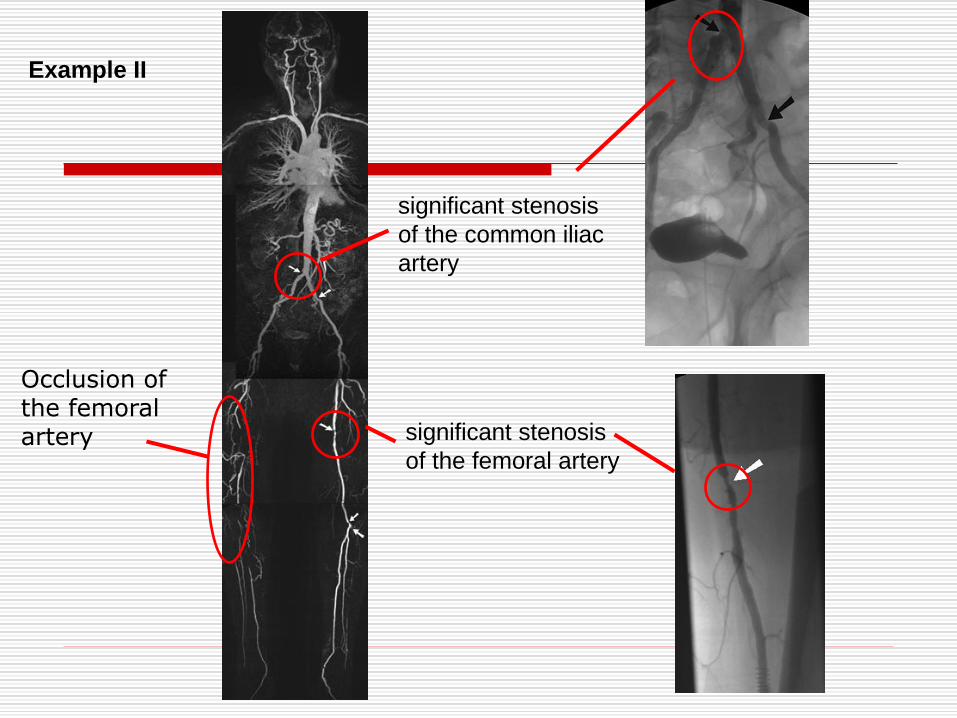
Example II
significant stenosis
of the common iliac
artery
significant stenosis
of the femoral artery
Occlusion of the femoral artery
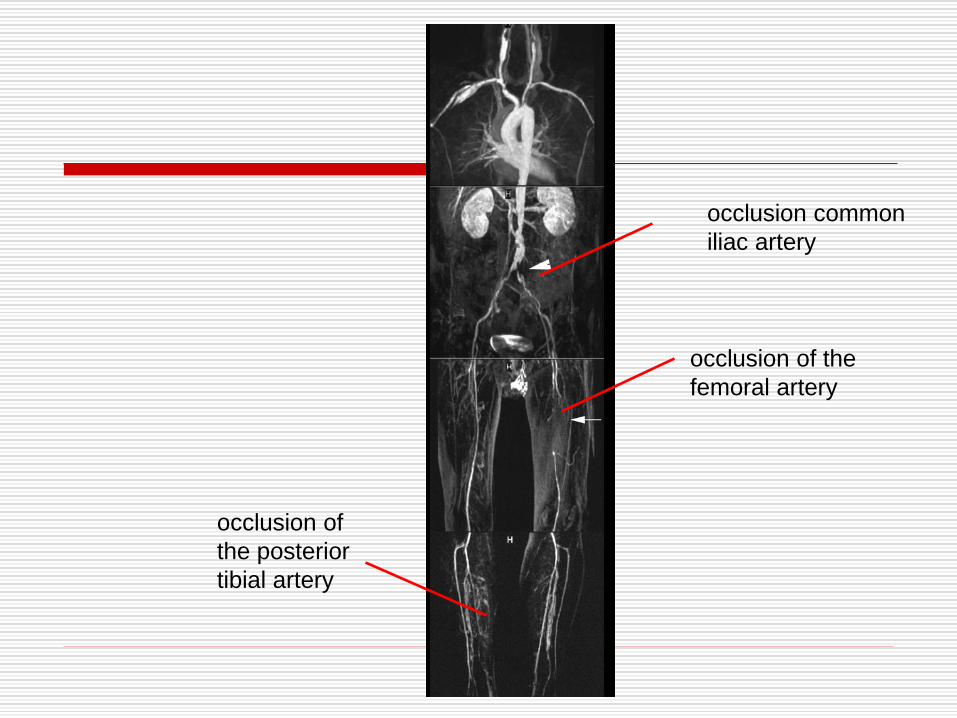
occlusion of the
femoral artery
occlusion of
the posterior
tibial artery
occlusion common
iliac artery
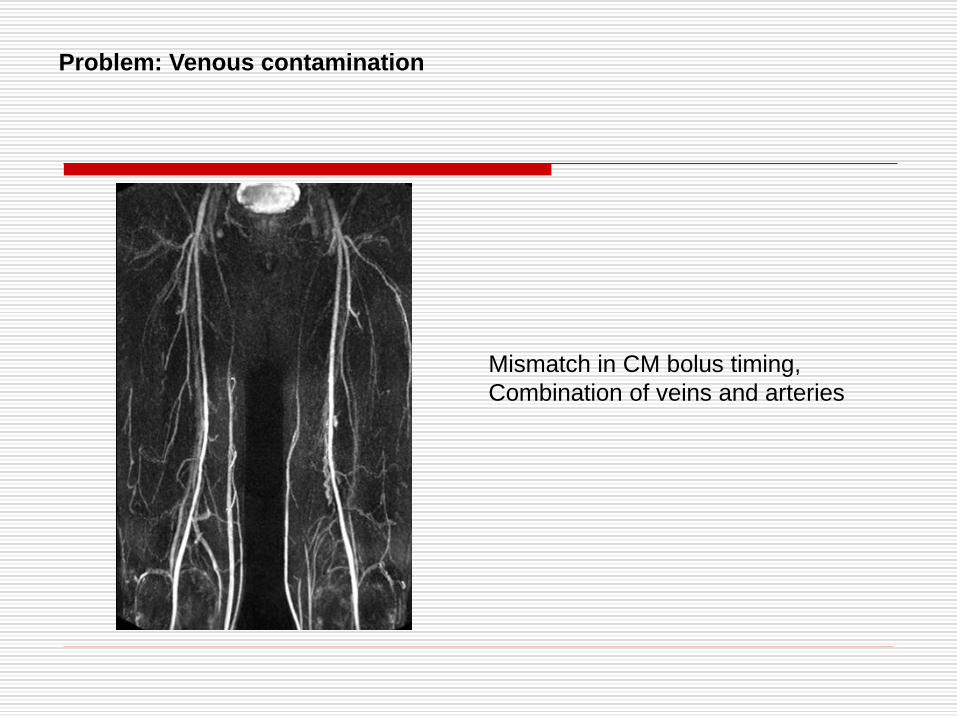
Problem: Venous contamination
Mismatch in CM bolus timing,
Combination of veins and arteries
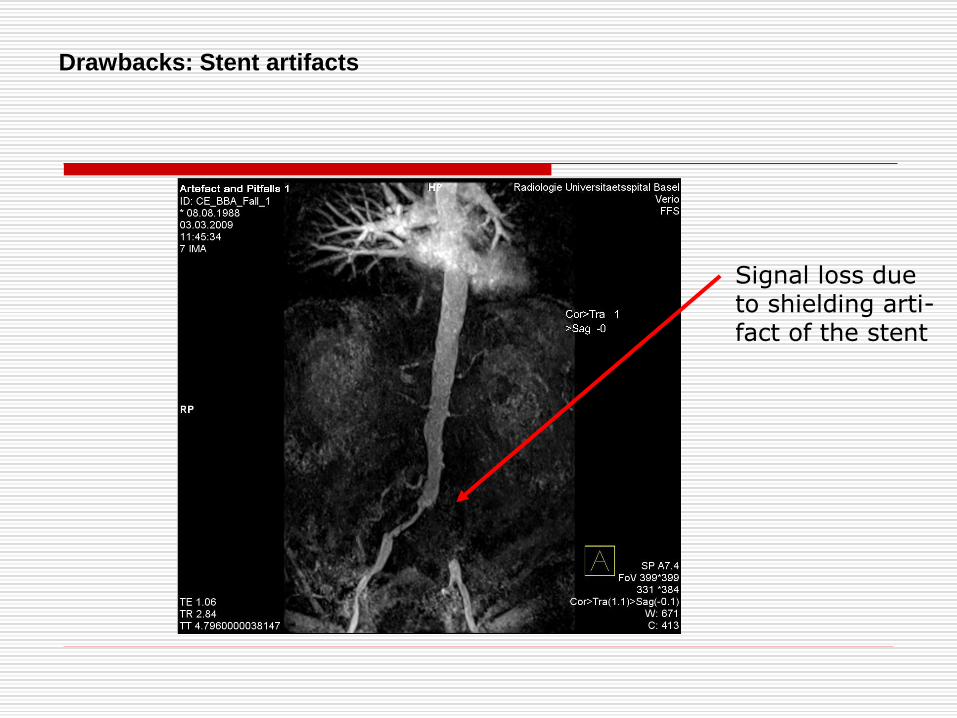
Drawbacks: Stent artifacts
Signal loss due to shielding arti- fact of the stent
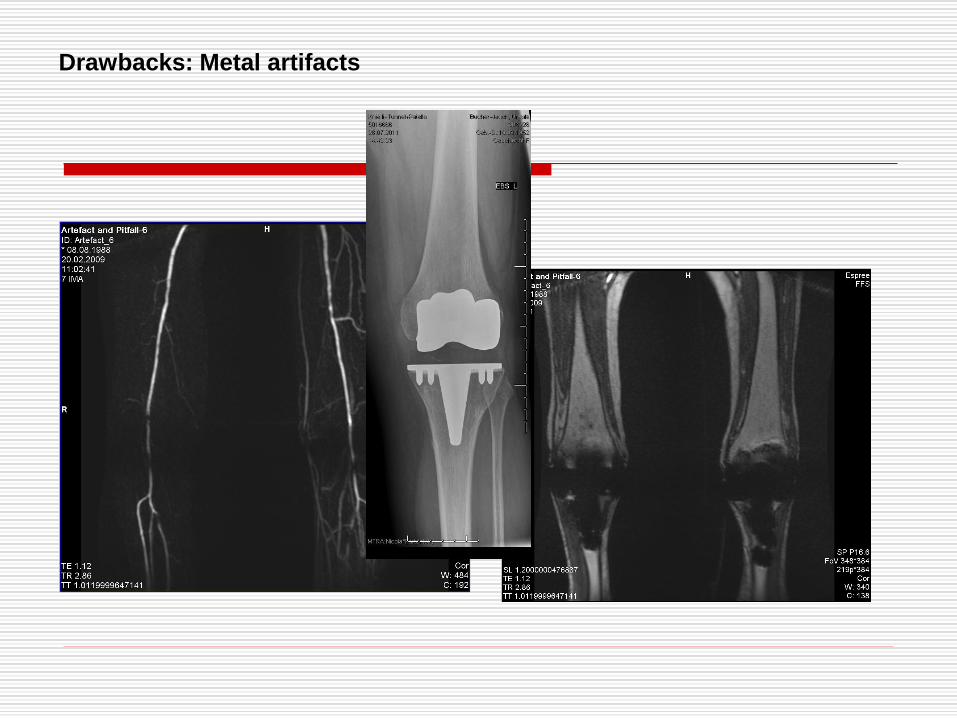
Drawbacks: Metal artifacts
a) Technical equipment (including dedicated suface coils !)
b) Eperienced technicians for precised bolus timing and MR scanning
c) Artifacts due to metal implants
d) Contraindications for MR scanning (e.g. Pacemaker/ICD)
e) Renal insufficiency (cave: nephrogenic systemic sclerosis (NSF))
Why is Whole Body MRA not yet a part of for
clinical routine ?
Whole body MRA enables the evaluation of arterial
stenosis, occlusions, and aneurysms with high
sensitivity/specificity
(= atherosclerotic load scoring of atherosclerosis).
Whole body MRA delineates the arterial system from head to toe
(excluding the intracranial and coronary arteries) in one single
examination.
Whole body MRA provides a „roadmap“ for precise planning of
an interventional procedure.
Take home message:
Thank you for your attention !
Recommended