Nirali H. Patel, MDPediatric Emergency Medicine
Children’s Hospital Medical Center of Akron

4 years of Medical School 1 year of Research 3 years of Pediatric Residency 1 year of Pediatric Chief Resident 2 years of Pediatric Emergency Fellowship
Total: 11 Years of Medical Experience
Estimate 80 hours work week (conservative!)
80 hrs x 52 weeks/yr x 11 yr
45,760 hours
A: 0-10 hours
B: 11-20 hours
C: 21-30 hours
D: 31-40 hours

Article published May 2010 in Western Journal of Emergency Medicine◦ Surveyed 34 EM residents and 22 EM attendings
regarding overall comfort of billing and coding
◦ 91% of Residents and 95% of Attendings felt that their jobs will require knowledge in billing & coding
◦ Only 26% and 29% felt they had adequate education in billing and documentation during residency

According to a 2004 Article in Emergency Medicine Clinics of North America, surgical and diagnostic procedures performed in the ED are considered separate services for coding purposes.
A billable service is one listed in the CPT manual that is performed as described.
Includes orthopaedic procedures, laceration repairs, foreign body removals, CPR.
Uses◦ Support and protect injured bones and soft tissue.◦ Reduce pain, swelling, and muscle spasm.◦ Decrease movement◦ Provide support and comfort through stabilization
of an injury. ◦ Secure nonemergent injuries to bones until they
can be evaluated by orthopaedics.
Advantages & Disadvantages◦ Unlike casts, splints are noncircumferential and
often preferred in the emergency department setting, since injuries are often acute and continued swelling can occur.
◦ Splints or "half-casts" provide less support than casts. However, splints can be adjusted to accommodate swelling from injuries easier than enclosed casts.
Methods◦ Custom Made: especially if an exact fit is
necessary.
◦ Ready-made splint: Off-the-shelf splints Variety of shapes and sizes Easier and faster to use Easy to adjust, and to put on and take off due to
velcro straps
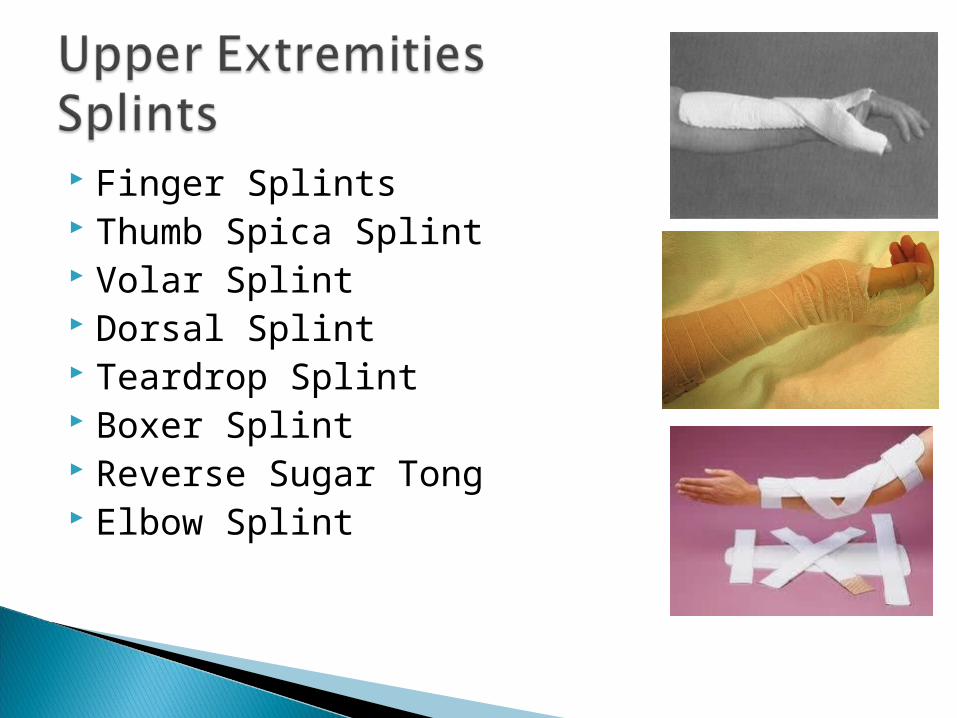
Finger Splints Thumb Spica Splint Volar Splint Dorsal Splint Teardrop Splint Boxer Splint Reverse Sugar Tong Elbow Splint

Knee Immobilizer Ankle Stirrup Posterior Ankle Posterior Leg

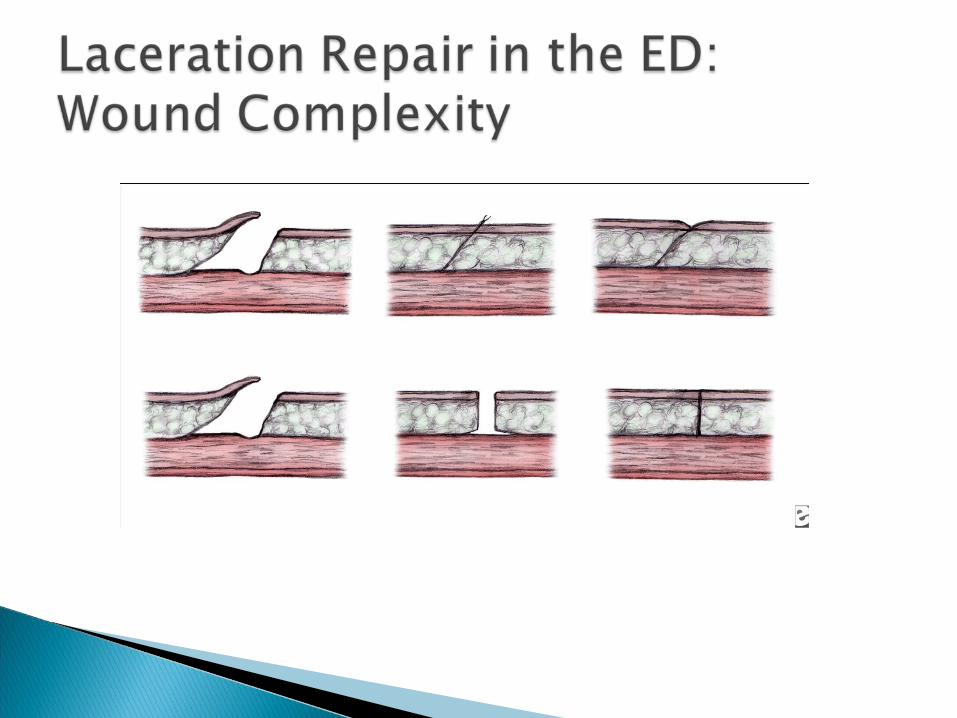
Laceration coding depends on three variables◦ Repair complexity
◦ Wound location
◦ Wound size
CPT groups laceration repairs broadly into three categories, by extent of repair.◦ Simple
◦ Intermediate
◦ Complex
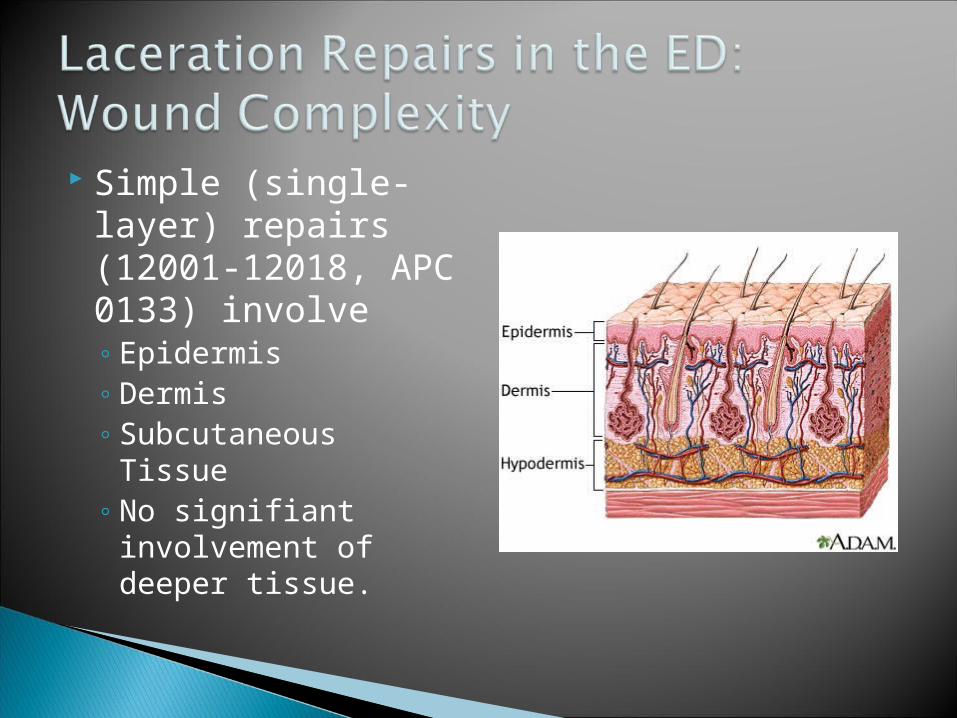
Simple (single-layer) repairs (12001-12018, APC 0133) involve◦ Epidermis◦ Dermis◦ Subcutaneous Tissue◦ No signifiant
involvement of deeper tissue.
Intermediate repairs (12031-12057, APCs 0133 and 0134) involve
◦ Deeper layers Subcutaneous tissue Superficial (non-muscle) fascia Skin (epidermal and dermal) closure.
◦ Layered closure.
◦ Heavily contaminated wounds requiring extensive cleaning may qualify as an intermediate repair, even if single layer sutures.

Complex repairs (13100-13153, APCs 0134 and 0135)◦ Involve more than layered closure
Extensive undermining Stents Retention sutures
◦ Extensive revision or repair of traumatic lacerations
◦ Avulsions
◦ Reconstructive or creation of a defect to be repaired (scar excision with subsequent closure).

Within each level of repair, CPT categorizes wounds by anatomic location.
For example, simple repair codes 12001-12007 apply to wounds of the neck, axillae, external genitalia, trunk, and/or extremities (including hands and feet).
Determine code choice according to repair complexity and anatomic location for each wound
Then select final code according to the size of the repaired wound(s).

Multiple Wounds◦ CPT treats all repairs of the same severity and
within the same anatomic classification as a single, “cumulative” wound
◦ Choose one code only to describe two or more repairs of the same severity in the same anatomic category.

Example◦ Surgeon repairs lacerations on both hands (3 cm and 5 cm) and
the left arm (9 cm).
◦ All repairs qualify as intermediate because the physician must remove particulate matter from the wounds, in addition to simple closure.
◦ To report repair of the hand wounds, add together the individual 3-cm and 5-cm lacerations for a total size of 8 cm
◦ Report 12044: Repair, intermediate, wounds of neck, hands, feet and/or external genitalia; 7.6 cm to 12 cm
◦ For the arm wound, select 12034 Repair, intermediate, wounds of scalp, axillae, trunk and/or extremities [excluding hands and feet]; 7.6 cm to 12.5 cm

Traumas or Cardio respiratory Arrests
Chaotic Documentation
Includes ◦ Intubations◦ Central Lines◦ Intraosseous Lines◦ Thoracocentesis and Thoracotomy Tubes

In the ED, will not be an elective intubation.
Emergent intubation usually preceded by Rapid Sequence Intubation (RSI)

Endotracheal intubation, emergency (CPT 31500) ◦ Use this code in emergency or crisis situations, not for
elective intubation
◦ Documentation should support an emergent need through appropriate coding
Critical care codes◦ Intubations are considered separately billable
procedures from critical care services
◦ Must subtract the time you spend on these procedures from the time you bill for critical care services

Multiple Sites
Requires Sterile Site
Associated with more risks and complications
Usually requires a specialist
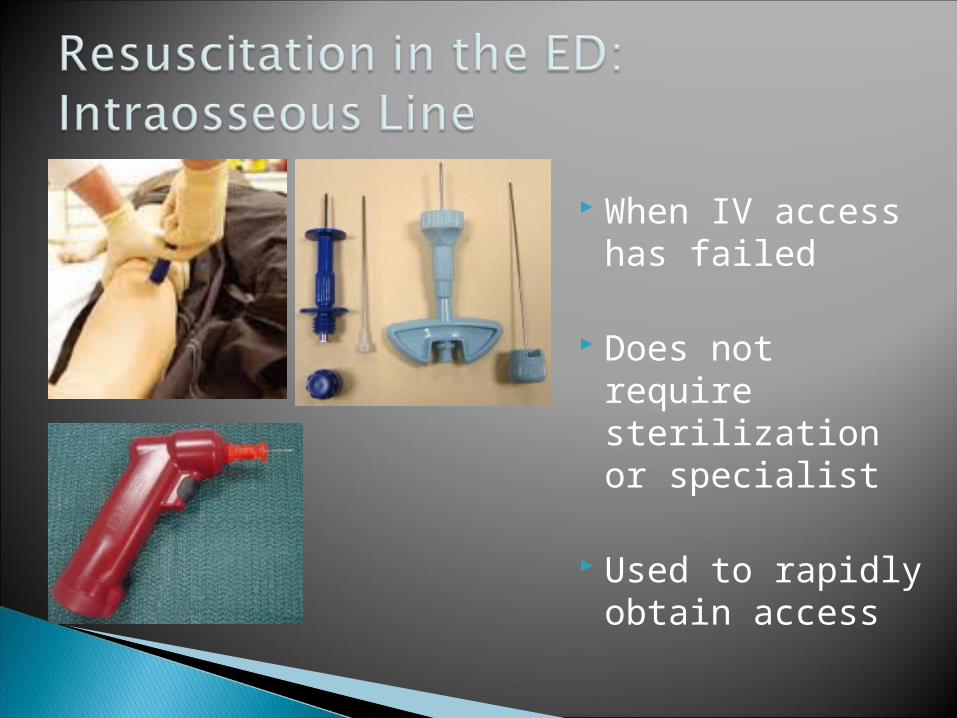
When IV access has failed
Does not require sterilization or specialist
Used to rapidly obtain access
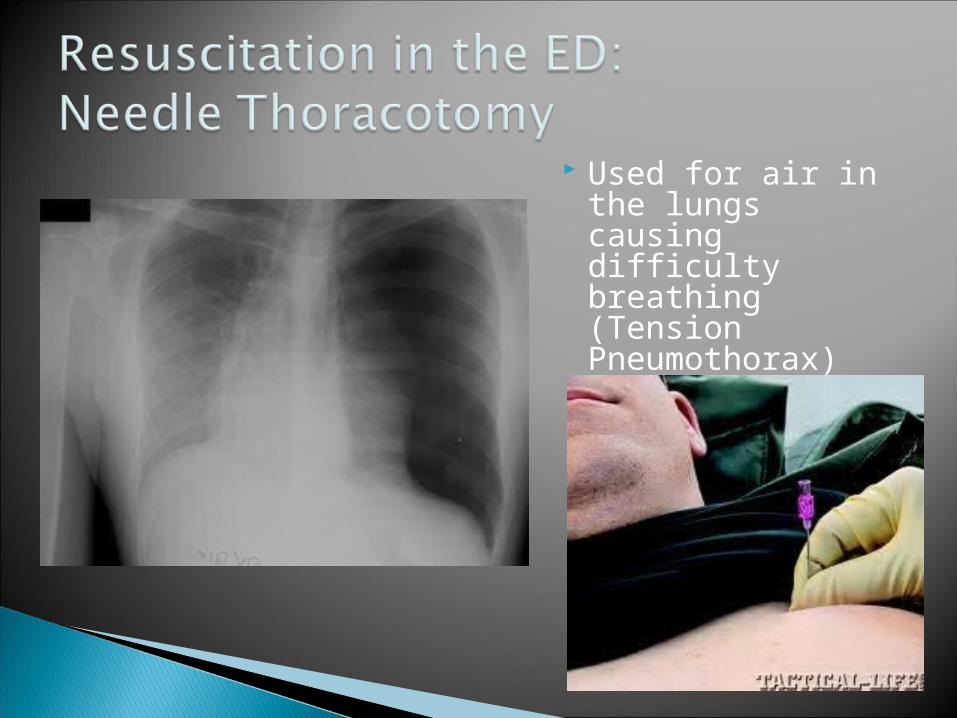
Used for air in the lungs causing difficulty breathing (Tension Pneumothorax)
For blood or fluid in the lungs or lung lining (hemothorax, pleural effusion) or large pneumothorax
Sterile procedure
May be done under conscious sedation in stable patients or while patient is intubated during resuscitation


Recommended