Led by clinicians, accountable to local people
NHS EAST LANCASHIRE CCG GOVERNING BODY
27 January 2014 1 – 3:00pm in Meeting Room 1, Walshaw House
AGENDA
Item Lead Strategic Objective
Report Category Timing
Patient Story – Veterans in Communities 1:00pm
1 Welcome, Introductions & Chair’s Update Chair 1:30pm
2 Apologies
3 Regular Items:
3.1 Governance: Declarations of Interest Quoracy
Chair
1:35pm
3.2 Declarations of Other Business
3.3 Public Questions
3.4 Minutes of the meeting held on 25 November 2013 Action Matrix:
Chair Attached Receipt
3.5 Matters Arising
4 Key Topic for Discussion:
4.1 Three Year Delivery Plans MY/TM All Attached Action 1:45pm
5 Business:
5.1 Chief Clinical Officers Report MI All Attached Receipt 2:15pm
5.2 Keogh Review into ELHT – Position Statement JH 1, 4 Attached Receipt 2:20pm
5.3 Finance & Performance Update MY 2 Attached Receipt 2:30pm
5.4 Communications Progress Report AB All Attached Receipt 2:40pm
5.5 Equality & Inclusion Annual Report AB 2, 3 Attached Receipt 2:50pm
6 Governance:
6.1 Sub Committee Summary AB All Attached Receipt 2:55pm
7 Any Other Business
7.1 Items for inclusion on the Corporate Risk Register 3:00pm
8 Date & Time of Next Meeting
Monday, 24 March 2014, 1pm at Walshaw House
RESOLUTION:
“That representatives of the press and other members of the public be excluded from the remainder of the meeting having regard to the confidential nature of the business
to be transacted, publicity on which would be prejudicial to the public interest.” (Section 1[2] Public Bodies (Admission to Meetings) Act 1960.
PART 2
9 Minutes of the closed meeting held on 25.11.13 Chair Attached 3:05pm
10 Remuneration Committee Minutes : 28.10.13 Chair Attached 3:10pm
11 Cases for Change : Business Cases Financial Details
MY/TM Attached 3:15pm
Page 1 of 10 Approved by DvR : 16.1.14
Agenda Item: 3.4
East Lancashire CCG Governing Body Minutes of the meeting held on Monday, 25 November 2013
1pm, James Hargreaves Suite, Burnley Football Club PRESENT: Di van Ruitenbeek Chair / Lay Advisor - Patient Engagement Steve Allcock Secondary Care Consultant
Dr Fiona Ford GP Lead - Primary Care Development Dr Paul Hartley GP Lead - Acute Commissioning & Contracting Dr Phil Huxley GP Clinical Lead – Pendle Dr Mike Ions Chief Clinical Officer Dr Murthy Motupalli GP Clinical Lead - Hyndburn Dr David White GP Clinical Lead - Burnley
Dr Peter Williams GP Clinical Lead - Rossendale Tom Wolstencroft Lay Advisor - Governance Mark Youlton Chief Finance Officer In Attendance: Steve Dean Director, Healthwatch Lancashire Tim Mansfield Chief Operating Officer
Anne Pietrzak Board Services Manager
Min Ref:
ACTION
13.135 Welcome, Introductions & Chairs Update The Chair welcomed everyone to the meeting and advised the change of venue was to allow more people to attend in relation to the HAC discussion. She reminded attendees this was not a public meeting, but a Governing Body meeting held in public. Any questions would be welcome following the meeting and the Chair would be happy to speak to those individually. Introductions were made. It was with regret that Dr Ions announced that a GP colleague had died. Dr Michael Barsby, GP at Kiddrow Lane, died suddenly following complications. Dr Barsby had been a GP for 16 years and was well respected. He was 43 years old, married with three children. His funeral was taking place that day and Dr Ian Whyte was attending and representing the CCG. Dr Ions wished to record official condolences from the Board and our thoughts are with his family.
13.136 Apologies Apologies were received from Olive Carroll, Dr Ian Whyte and Mike Leaf.
13.137 Governance Issues Declarations of Interest:
- Dr Motupalli, as a Hyndburn GP & employee for ELMS working 2 sessions per month at the HAC.
- Dr White provided ad-hoc occupational health service for ELMS.

Page 2 of 10 Approved by DvR : 16.1.14
- Dr Ford, as a Hyndburn GP and many patients use the facility which would impact on the practice, should the facility close.
- Dr Huxley, as a Pendle GP – the HAC was a significant resource.
It was considered that all GPs should declare an interest in the item relating to the HAC as any decision would impact on all GPs in all 5 localities. The Chair pointed out that if a decision is made regarding the HAC, the issue would be referred to the Remuneration Committee for a final decision. The Chair also highlighted that those declaring an interest would not be involved in the final decision making process. Legal advice had been sought which clarified that this arrangement would deal with any conflict of interest issues as the membership of the Remuneration Committee does not include GP members. Declarations of Other Business: There was no further business
declared. Quoracy: The meeting was quorate.
13.138 Public Questions The Chair advised that one public question had been received from Mr Colin Wills relating to a Specialist Parkinson’s Nurse. Q: If it is decided to appoint a Parkinson’s Nurse:
What will happen next, what will the timetable be, and How long will it be before an appointment is made and the person
appointed starts work? A: Mr Mansfield advised that it was his understanding that recruitment would
be dependent on the Parkinson’s Society releasing the funding for the post and on the length of time to recruit. The item was listed on the agenda and a decision would be made during the meeting.
13.138.1 Petition The CCG had received a petition from Councillor Claire Pritchard relating to services currently provided at the Health Access Centre in Accrington and contained approximately 4665 signatures. The Governing Body were asked to receive the Petition and respond. The Chair formally received the petition on behalf of the CCG. ACTION: Review the policy regarding Petitions.
AB
13.139 Minutes of the meeting held on 28 October 2013 The minutes of the meeting held on 28 October 2013 were presented. 13.120 : Lancashire Health & Wellbeing Board - It was noted there was a missing word in the second paragraph ….. discussions at the last meeting. RESOLVED: that subject to the above amendment, the minutes were approved as an accurate record.
Page 3 of 10 Approved by DvR : 16.1.14
13.140 Action Matrix The Action Matrix was presented and discussed: 13.65 – Integrated Business Report : there were ongoing discussions with the CSU to review the format of the detailed report. More of the detail would be considered when the Head of Quality was in post. 13.96 – Performance : The CSU had advised Ambulance response time data was not available by locality and the CCG was in discussion with Blackpool CCG to consider this going forward. Remain on matrix until data is available. It was reported that Mental Health readmission data was included in the IBR. 13.116 – Towards Transformation : Plans were in place to invite the Area Team to meet with the Governing Body. 13.126 – Lancashire CCG Network – Proposed Governance Arrangements : It was noted the CCG was limited to two amendments each year as required by NHS E. The next opportunity would be June 2014 and with a reminder to the May GB meeting regarding any proposed changes. GB comments had been fed back to Chorley & South Ribble CCG as lead CCG and the final paper would be approved by the CCG network.
AB
13.141 Matters Arising There were no matters arising from the minutes.
13.142 Accrington Victoria Health Access Centre Tim Mansfield, Chief Operating Officer gave a presentation highlighting key issues that the CCG needed to take into consideration when making a decision regarding the future of the Health Access Centre (HAC) in Accrington. An engagement exercise had taken place with patients, the public and local organisations, including Hyndburn Borough Council about the services provided by the HAC. The CCG was very aware of the public interest and emotion associated with the HAC and have been actively listening to the views expressed. The CCG was committed to openness and transparency and it was noted that the level of detail would not have been made available by the previous organisation. The HAC was successful in offering wider access to patients outside GP core hours. The presentation outlined concerns raised by local people and highlighted key challenges for the CCG, particularly the need to deliver the required cost savings of £33m over the next few years, whilst ensuring fairness in GP access across all 5 CCG localities. The contract was initially procured by EL Primary Care Trust and awarded to East Lancashire Medical Services (ELMS), an independently run social enterprise. There were two elements to the Health Access Centre which included access for unregistered patients on a walk-in basis, together with a GP Practice with a list size of 1358. Commissioning responsibility for the GP Practice sat with NHS E and it was expected that a decision regarding this facility would be made in February 2014.

Page 4 of 10 Approved by DvR : 16.1.14
It was reported that the number of attendances at the facility was significantly more than originally anticipated with increased costs and details of locality attendance rates were outlined. A number of options were outlined in the report together with issues that need to be taken into consideration when making a decision regarding the future of the Walk In Centre. It was also recognised that when the engagement exercise commenced, a change to the GP Contract had not been anticipated. Members were asked to express an initial view on the options presented and to consider if there was enough evidence for a final decision to be made at the meeting or defer a decision until the New Year. As Chair, Dr van Ruitenbeek wanted to be confident that sufficient evidence was available to the Governing Body to make a well informed decision at the meeting. Members discussed the options at length and the following points were made:
The majority of members considered there was insufficient information to make an informed decision. [MM & FF felt there was enough evidence to make a decision.]
GP Practices are under pressure, highlighting the need to strengthen primary care to provide a better service. This was an opportunity to improve access for primary care across the patch. Primary care responsibility sits with NHS E and options as they are now could make issues more complicated in terms of access.
It was considered the APMS Practice should be involved in discussions to inform the decision. It was noted this was a separate discussion and there was a need to ensure the CCG is sufficiently engaged with NHS E to ensure decisions are not taken independently.
There was also a need to consider the proposed alternatives outlined in the recent Monitor report, whilst at the same time considering these against the Primary Care Development Strategy.
Options 4 & 5 were identified as being funded at a fixed price. However, a detailed business case was not available outlining costs and benefits of the alternatives.
Healthwatch strongly believed in the need to listen to patients and respond in a positive way. Soft intelligence was consistent with the spirit behind the petition. Consideration should be given to looking wider than the HAC in terms of provision of primary care across the whole of East Lancashire.
There were increasing demands on primary care across all localities with relatively low funding being received within East Lancashire. Winter pressures money had enabled the CCG to pilot different ways of working and build on the quality improvement work ongoing.
The decision would have a direct effect on service users in the Hyndburn area and it was important to work with Hyndburn practices to improve access.
It was also important to have a clinically appropriate model that offers value for money.
There was a request for specific information relating to the percentage of frequent visits and people attending the HAC for a second opinion. It was important to provide the best possible care, balancing want with need and affordability.
Financial consequences associated with deferral of a final decision were considered, noting this could result in 6 months additional activity, creating a potential overspend of £1m which would be managed by non-recurrent funding. Members were advised that details of the
Page 5 of 10 Approved by DvR : 16.1.14
financial allocations for the next two years were expected w/c 16 December and whatever decision is taken, the organisation must be in a sustainable financial position.
Following debate, it was agreed to eliminate the following three options which were amongst those initially being considered:
Keep the status quo and tender a service in its current format; Let the current contract expire without a replacement service; Decommission the GP walk-in service and extend the contract for the
Minor Injuries Unit to include minor illness. Once a decision is made, there would be a need to discuss the impact with the Overview & Scrutiny Committee and if there was likely to be a significant change in service, it would be necessary to go out to formal consultation. In conclusion the Chair thanked everyone for their contributions which highlighted that the majority of members felt there was not enough information to make a decision. It was recognised that in order to make the best decision, greater clarity was required outlining how future models would fit into the whole system, whilst taking account of the financial implications. It was important to have a clear understanding of the primary care development strategy and to ensure the final decision fits with the decisions of NHS E regarding the contract for the GP Practice. It was also important to consider the knock-on effect of this decision on AVCH as a health facility and the wider implications on A&E and Urgent Care Centres. Dr Ions felt the debate was a very accurate summary of the current position. The Chair thanked members of the public for their contributing views to inform this decision, pointing out that the CCG listens to public opinion. She highlighted the importance of understanding that the CCG was making a well considered decision in deciding to defer a final decision until early 2014. RESOLVED: that following in-depth debate, the Governing Body agreed to defer a final decision on the future of the GP walk-in Centre at Accrington Victoria Hospital until early in the new year, to allow more detailed options to be developed.
13.143 Specialist Parkinson’s Nurse for EL Following concerns raised by local people regarding the lack of a Parkinson’s Nurse in East Lancashire, a detailed business case had been developed for a primary care based Parkinson’s Nurse. The post would be pump primed by Parkinson’s UK for two years, on the understanding that this would be mainstreamed by NHS funding thereafter. The nurse would be hosted in primary care and support all five localities, offering home visits and symptom management, therefore reducing the number of emergency admissions and increased length of hospital stay. The Business Case had been considered by the Local Delivery Group with a recommendation to the Governing Body that the CCG support the proposal, which highlighted a good example of responding to patient feedback. Following consideration of the report it was recognised there were a large number of patients with Parkinsons Disease in East Lancashire which was
Page 6 of 10 Approved by DvR : 16.1.14
considered a significant workload for one nurse. This raised the question as to whether the CCG should be commissioning a service rather than a nurse for the number of patients identified. The Chief Nurse was pleased to see the report and agreed with the capacity issues. However, it was important to demonstrate that this role will have an impact on patient experience in terms of reducing the number of admissions and length of stay. It was important to ensure robust support systems are in place together with connectivity with secondary care locally and obtain peer support from neighbouring CCGs. It was considered this was the first step towards helping a group of people improve their quality of life which would produce great benefits. Over the next two years the service should be audited to support the development of a business case for a wider service. The nurse would sit within a Practice in primary care and provide support all five localities. RESOLVED: that the Governing Body support the Business Case and Letter of Intent for submission to Parkinson’s UK by the deadline of 30 November 2013.
TM
In view of timings, the Chair requested precise discussions going forward.
13.144 Keogh Review into ELHT The report provided a position statement relating to the Keogh Assurance Framework in respect of ELHT and the assessment of progress made in the delivery of actions and submission of evidence. Jackie Hanson, Chief Nurse confirmed that the delivery of evidence was now being managed as an on-going process through regular meetings with the Trust and progress was being made in respect of Section 4. It was acknowledged that significant work was underway within the Trust to ensure robust evidence is delivered in a timely manner which is then analysed with further feedback to the Trust. This was an active piece of work, with the aim of having a document that is fully populated before the next Risk Summit, when there would be formal discussion with the TDA and the Trust and progress against the Keogh review would be monitored. Tom Wolstencroft requested significant discussion time at the next meeting to devote to this issue and to ensure there was capacity within the CCGs resource to manage. Dr Ions confirmed the Quality Assurance Framework was the CCGs response to Francis. It was confirmed that concerns regarding the pace of change and embedding of issues throughout the organisation had been articulated with the Trust. More information had been received and it was important to meet the challenge to support the Trust to embed the required changes to improve outcomes and develop a culture demonstrating more care and compassion. It was also reported there had been a number of changes of appointment at ELHT with Interim HR and Communications & Engagement Directors now in post. ACTION:
Allow time for indepth discussion at the next meeting.
Page 7 of 10 Approved by DvR : 16.1.14
Individual points to be raised with Jackie Hanson & Mike Ions outside the meeting.
RESOLVED: that the Governing Body receive the report.
AB MI/JH
13.145 Finance & Performance Update Mark Youlton, Chief Finance Officer presented the financial position statement for the seven month period to 31 October 2013, confirming the forecast outturn position for the organisation remained robust. He reported a slight worsening in the position at ELHT and activity data for other providers identified over-performance at Lancashire Teaching Hospital Hospital and significant under-performance at Pennine Acute. An increase in costs associated with continuing healthcare had resulted in a forecast £3m overspend, noting that a contingency held for this purpose had now been deployed. Prescribing data also identified a £3m overspend against plan. The CCG was in a position to achieve the £10m required surplus, which would be banked for use in the next financial year to support any additional expenditure. However there was non recurrent funding that must be spent in year, the first call on which would be the unidentified QIPP gap, noting that the organisation must not be in this position year on year. Members referred to the challenges of QIPP, the Winter Plan and the Integration Fund and the challenge to work with other organisations. Information was awaited from colleagues in Oldham relating to Affordable Warmth which would lead to reduced admissions at A&E particularly for the frail elderly group and support the CCG to get ready for future years challenges. Concerns were expressed relating to the QIPP £2.9m gap highlighting the need to understand why the target had not been met and to ensure the CCG does not fall into the same position next year. There was a need to change the way services are delivered, highlighting the importance of clinical leadership to support people to keep themselves well at home. The Chair considered it was the responsibility of the whole Governing Body to look for more transformational ways of working to ensure a quality service can be offered in more community based ways. In conclusion the Chair emphasised the need for transformation and creative thinking, recognising that next year will be more financially challenging. RESOLVED: that the Governing Body receive the report.
13.146 Winter Plan Tim Mansfield provided a detailed update in terms of current activities relating to Annual Resilience Planning, specifically relating to winter developments, finances and planning. The system had been under pressure for a long time highlighting a risk if robust services are not in place. It was also recognised that ELHT had received £1.4m to support the winter plan. Tim outlined key points, particularly the strategies and plans that are integral to the overall plan
Page 8 of 10 Approved by DvR : 16.1.14
A Pennine Lancashire Information Campaign had been developed in partnership with the Communications and Engagement Team to provide reassurance to the public and other stakeholders about the ability of the NHS to cope during the winter months. The communications plan was also designed to avoid confusion and help patients to use the most appropriate services. Members received assurance that the organisation was doing as much as possible to ensure robust plans are in place to be confident that services will be available to the public. It was noted there was lengthy discussion at the Senior Clinicians meeting regarding the detail of the ambulatory care pathway, with further discussion at the December meeting. RESOLVED: that the Governing Body receive the report and support the work ongoing to deliver the Annual Resilience Plan 2013/14, confirming there would be further discussion at the Senior Clinicians Meeting in December.
TM
13.147 Integration Transformation Fund Members received correspondence from NHS England outlining the details of the Integration Transformation Fund which confirmed that 3% of the CCGs budget would be made available to promote the development of integrated health and social care services. The budget would sit within the governance arrangements of the Health & Wellbeing Board and details of the funding transfer and how this would impact on East Lancashire was expected on 19 December. The CCG was working with LCC and the Health & Wellbeing Board to develop plans outlining how the funding will be used and submit to NHS E by 15 February 2014, demonstrating engagement with stakeholders and the public, with funding transferring in 2015/16. An Integrated Transformation Board was to be created to take this work forward and a stakeholder event was planned in January 2014 for members of the Patient Participation Groups, together with more detailed discussion at the Health & Wellbeing Partnership in January to sign off the initial plan. Dr Ions reiterated that these were unrealistic timescales to respond to the planning process. The CCG supported the principle of integration and it was important to identify ideas highlighting how we best do this. The Chair requested that voluntary and community group representation was included in the planned events, to influence discussion and priorities and share creative ideas. She also confirmed this was an opportunity to do things differently and demonstrate partnership working. RESOLVED: that the Governing Body receive the report and note the content.
13.148 Procurement Policy The policy was recommended for approval by the Wider Management Team and presented to the Governing Body for ratification. It was an important document to have as an organisation which outlined the procurement process in line with Standing Orders and Prime Financial Policies.
Page 9 of 10 Approved by DvR : 16.1.14
The Chief Finance Officer confirmed the policy was based on a CCG standard and had a clear link with the Conflict of Interest Policy to ensure a robust process was in place. RESOLVED: that the Governing Body ratify the Procurement Policy as presented.
13.149 Sub Committee Summary The report summarised the work of each of the sub-committees of the Governing Body, reporting key decisions and highlighting items for approval. Members attention was drawn to the Audit Committee Terms of Reference which had been revised to clarify the role of the Audit Committee in terms of Emergency Planning and Resilience. Clinicians requested assurance that organisations are working collaboratively and Practices fit in with the arrangements. It was clarified that the CCG was a Category 2 responder and important to ensure the appropriate plans are in place. The sub-committee summary was based on approved minutes of the relevant committees and it was felt that a number of the items listed had been superseded by further discussion. It was also considered that non LDG members would not fully understand the basis of discussions from the summary and that consideration be given to a full set of minutes being included as an appendix. RESOLVED: that the Governing Body receive the report, endorse the decisions taken by the Committees and accept the Audit Committee Terms of Reference.
13.150 Stakeholder Committee Minutes RESOLVED: that the Governing Body receive the following Stakeholder Committee Minutes for information:
Pennine Lancashire Clinical Transformation Board – 2.10.13
13.151 Any Other Business 13.151.1 Corporate Risk Register It was suggested the Health Access Centre be included on the Register in relation to the financial risk from the decision made and organisational reputation risk. 13.151.2 Keogh Review Dr Williams referred to the latest SHMI report for ELHT which identified that mortality rates are as expected, which acknowledged that there had been some progress. It was confirmed that the SHMI rate was in line, however there were some anomalies regarding the HSMR, pointing out that the Keogh concern was not the number of deaths, but the number of deaths not reported.
Page 10 of 10 Approved by DvR : 16.1.14
13.152 Date & Time of Next Meeting The next meeting of the Governing Body would take place on Monday, 27 January 2014, 1pm at Walshaw House. The Chair thanked members of the public for attending.
RESOLUTION:
“That representatives of the press and other members of the public be excluded from the remainder of the meeting having regard to the confidential nature of the business to be transacted, publicity on which would be prejudicial to the public interest.” (Section 1[2] Public Bodies (Admission to Meetings) Act 1960).
Version 14
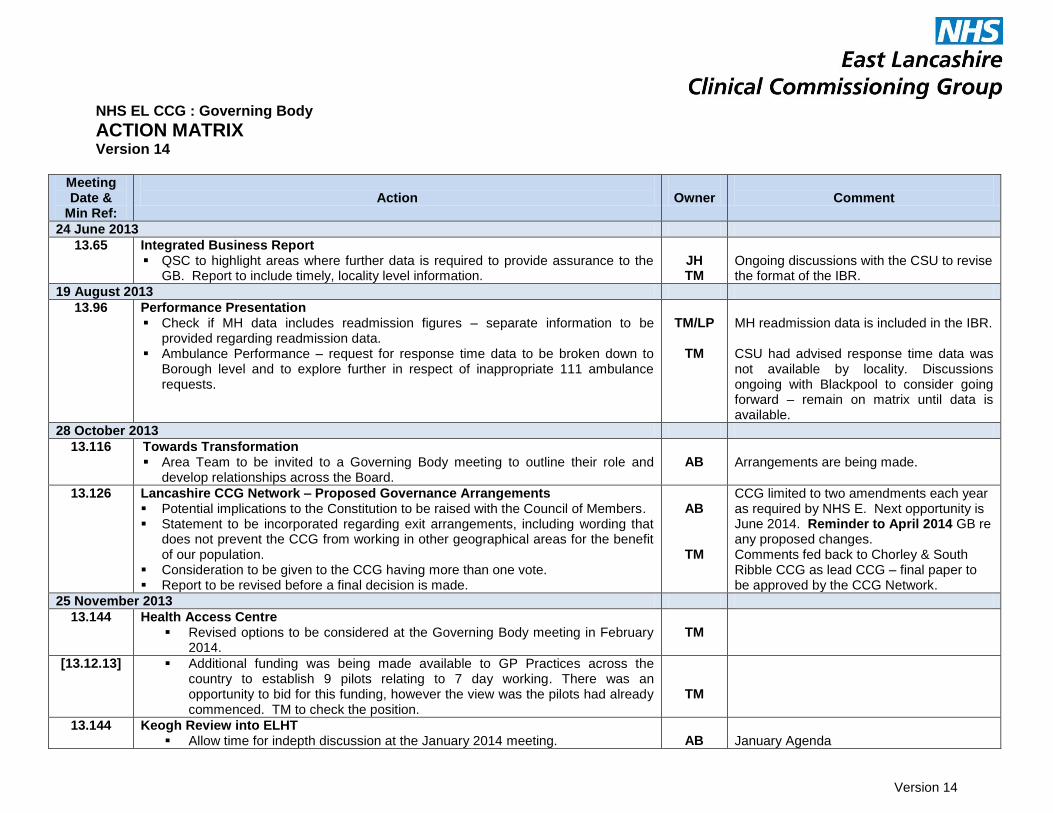
NHS EL CCG : Governing Body
ACTION MATRIX Version 14
Meeting Date &
Min Ref:
Action
Owner
Comment
24 June 2013
13.65 Integrated Business Report QSC to highlight areas where further data is required to provide assurance to the
GB. Report to include timely, locality level information.
JH TM
Ongoing discussions with the CSU to revise the format of the IBR.
19 August 2013
13.96 Performance Presentation Check if MH data includes readmission figures – separate information to be
provided regarding readmission data. Ambulance Performance – request for response time data to be broken down to
Borough level and to explore further in respect of inappropriate 111 ambulance requests.
TM/LP
TM
MH readmission data is included in the IBR. CSU had advised response time data was not available by locality. Discussions ongoing with Blackpool to consider going forward – remain on matrix until data is available.
28 October 2013
13.116 Towards Transformation Area Team to be invited to a Governing Body meeting to outline their role and
develop relationships across the Board.
AB
Arrangements are being made.
13.126 Lancashire CCG Network – Proposed Governance Arrangements Potential implications to the Constitution to be raised with the Council of Members. Statement to be incorporated regarding exit arrangements, including wording that
does not prevent the CCG from working in other geographical areas for the benefit of our population.
Consideration to be given to the CCG having more than one vote. Report to be revised before a final decision is made.
AB
TM
CCG limited to two amendments each year as required by NHS E. Next opportunity is June 2014. Reminder to April 2014 GB re any proposed changes. Comments fed back to Chorley & South Ribble CCG as lead CCG – final paper to be approved by the CCG Network.
25 November 2013
13.144 Health Access Centre Revised options to be considered at the Governing Body meeting in February
2014.
TM
[13.12.13] Additional funding was being made available to GP Practices across the country to establish 9 pilots relating to 7 day working. There was an opportunity to bid for this funding, however the view was the pilots had already commenced. TM to check the position.
TM
13.144 Keogh Review into ELHT Allow time for indepth discussion at the January 2014 meeting.
AB
January Agenda
Version 14
Individual points to be raised with Jackie Hanson & Mike Ions outside the mtg. MI/JH
13 December 2013
13.146 Winter Plan Notes of joint visit with the TDA and Area Team to Urgent Care and the
Medical Assessment Unit to be circulated.
JH
Complete

1
Agenda Item No: 4.1
REPORT TO:
NHS EL CCG Governing Body
MEETING DATE:
27th January 2014
REPORT TITLE:
Cases for Change Business Cases
SUMMARY:
This report outlines the position on the Business Cases and Delivery Plans for the workstreams for Scheduled Care, Unscheduled Care, Integrated Care, Mental Health and Dementia following detailed discussion and recommendations from the LDG
REPORT CATEGORY: Formally Receipt
Tick
Action the recommendations outlined in the report.
Debate the content of the report
Receive the report for information
AUTHOR:
Mark Youlton/Tim Mansfield
PRESENTED BY:
Mark Youlton/Tim Mansfield
COMMITTEES/ GROUPS CONSULTED:
Local Delivery Group (20/1/14)
Which Strategic Objective does the report relate to
Tick
1 Commission the right services for patients to be seen at the right time, in the right place, by the right professional.
2 Optimise appropriate use of resources and remove inefficiencies.
3 Improve access, quality and choice of service provision within Primary Care
4 Work with colleagues from Secondary Care and Local Authorities to develop seamless care pathways
2
Agenda Item No: 4.1
NHS EL CCG Governing Body 27TH January 2014
CASES FOR CHANGE
BUSINESS CASES
1. Introduction 1.1 This report outlines the position on the Business Cases and Delivery Plans for the
workstreams for Scheduled Care, Unscheduled Care, Integrated Care, Mental Health and Dementia following detailed discussion and recommendations from the LDG.
2. Purpose
2.1 Cases for Change have been circulated widely throughout the CCG for the key work-
streams of the CCG. They have been agreed by CCG Members at a QP event, the LDG and the Governing Body. Associated Business Cases and Delivery Plans were agreed at the LDG meeting on 20th January 2014 for recommendation to the Governing Body. We are confident that these will enable the CCG to deliver its QIPP targets in 2014/15 and 2015/16, and the requirements within the planning guidance, Everyone Counts. More detail will be presented to the Governing Body as part of the final planning submission in March.
3. Conclusion
3.1 Scheduled care The recommendations of the LDG are to commission:
- An integrated Skin Service - A consultant led Community Ophthalmology Service - A Community Integrated Rheumatology, MSK and Chronic Pain Management
Service
3.2 Unscheduled Care
The recommendations of the LDG are to commission: – Co-located primary care services within UCC – Ambulatory care pathway within East Lancashire Hospital Trust – Early Action Accident and Emergency Police Liaison Role Pilot – Paediatrics – redesign of Children’s Observation Assessment Unit – Children’s community respiratory service – Children’s physiotherapy service – A review of Bespoke Patient Transport Services

3
– Health Access Centre review – NWAS Intermediate Tier Vehicle Review – Develop a NHS 111 local interface model – Improving access in primary care 3.3 Integrated Transformation
The development of the Business Cases and the Delivery Plan for integrated care is closely aligned with the development of the Better Care Fund and the additional modelling work that the Health economy has commissioned to inform and test the assumptions we have made about the development of community health and care services to facilitate the shift in spending from acute to community services.
The recommendations of the LDG are to commission: – Integrated neighbourhood teams – Safer Transfers of Care – Transitional System redesign – 7 day working in primary and community services – Lead clinician for over 75s 3.4 Mental Health and Dementia The recommendations of the LDG are to commission: - A redesigned Single Point of Access - Further development and expansion of the Counselling programme within IAPT to
widen the numbers of IAPT compliant counsellors and to broaden access to the Primary care MH system.
- A 24/7 A&E MH response through the full year 2014-2015 to allow for re-design of the A&E and Crisis MH system.
- Delivering the Dementia diagnosis gap project and improving management of Dementia within Primary care.
- Local intermediate residential services for people with dementia 4. Recommendations 4.1 Governing Body Members are requested to approve the recommendations
of the LDG as outlined above. 4.2 To note that confirmation of any investment into these work-streams is dependent upon the CCG being able to deliver all its financial targets. Mark Youlton Tim Mansfield Chief Finance Officer Chief Operating Officer

1
Agenda Item No: 5.1
REPORT TO: NHS EL CCG Governing Body
MEETING DATE: 27 January 2014
REPORT TITLE:
Chief Clinical Officer’s Report
SUMMARY:
This report provides an update on both strategic and operational issues of interest to Governing Body members which have taken place since my last update in October 2013.
REPORT CATEGORY: Formally Receipt
Tick
√
Action the recommendations outlined in the report.
Debate the content of the report
Receive the report for information
AUTHOR:
Angela Brown, Head of Corporate Affairs
PRESENTED BY:
Mike Ions, Chief Clinical Officer
COMMITTEES/ GROUPS CONSULTED:
Which Strategic Objective does the report relate to
Tick
1 Commission the right services for patients to be seen at the right time, in the right place, by the right professional.
√
2 Optimise appropriate use of resources and remove inefficiencies. √
3 Improve access, quality and choice of service provision within Primary Care √
4 Work with colleagues from Secondary Care and Local Authorities to develop seamless care pathways
√
2
Agenda Item No: 5.1
NHS East Lancashire CCG GOVERNING BODY
27 January 2014
Chief Clinical Officer’s Report
1. Introduction 1.1 This report provides an update on both strategic and operational issues of interest
to Governing Body members which have taken place since my last update in October 2013. In this report I will refer to the following:
Keogh Review
Planning Guidance
NHS Choices: Publication of GP Data
Personal Health Budgets
Tobacco Free Lancashire: Revised Tobacco Free Strategy and Terms of
Reference
CCG Assurance: Quarter 2
ELHT
Governing Body Members o Appointment of Lay Advisor
Rossendale Steering Group Elections
Stakeholder Engagement
Policies and Procedures
2 Keogh Review
2.1 The second CCG listening event was held in Pendle on 16th January at Colne Library. The event was well attended with approximately 60 people attending, all conveying their views on the services provided to the Pendle residents. There was representation from the CCG, East Lancashire Hospitals NHS Trust, Airedale Foundation Trust, Pendle Overview and Scrutiny Committee and Health Watch. 2.2 The listening event was positive and feedback from the public suggests that future events would be welcomed. Themes and comments have been collated and these will be used to identify and address any issues and inform the commissioning of services going forward.
2.3 A date has also been set for the Burnley listening event, and this will be held on Saturday 1st February.
3
3 Planning Guidance 3.1 NHS England has published its framework within which commissioners will need to
work with providers and partners in local government to develop strong, robust and ambitious five year plans to secure the continuity of sustainable high quality care for all, now and for future generations.
3.2 Everyone Counts: Planning for Patients 2014/15 to 2018/19 describes NHS
England’s ambition for the years ahead and its ongoing commitment to focus on better outcomes for patients. It describes the vision for transformed, integrated and more convenient services, set within the context of significant financial challenge. The planning guidance is accompanied by a suite of support tools intended to assist commissioners with their planning considerations to maximise the best possible outcomes for their local communities.
3.3 The planning guidance seeks:-
Strategic plans covering a five year period, with first two years at operating plan level
An outcomes focused approach, with stretching local ambitions expected of commissioners, alongside credible and costed plans to deliver them
Citizen inclusion and empowerment to focus on what patients want and need
More integration between providers and commissioners
More integration with social care – cooperation with Local Authorities on Better Care Fund planning
Plans to be explicit in dealing with the financial gap and risk and mitigation strategies. No change not an option
3.4 NHS England has also published the funding allocations that Clinical
Commissioning Groups (CCGs) will receive over the next two years (2014/15 and 2015/16). The allocations contain a new funding formula that will more accurately reflect population changes and include a specific deprivation measure.
3.5 Funding for NHS commissioners will rise from £96bn to £100bn over the next two
years so, despite wider public sector budget cuts, the NHS is being protected from inflation. The changes follow an extensive review into funding allocations and all CCGs will receive a funding increase matching inflation in the next two years while the most underfunded areas, and those with fast-growing populations, will receive even more.
3.6 work is underway within the CCG to develop and populate the required
documentation. 3.7 The framework and funding allocations can be accessed at: Everyone Counts: Planning for Patients 2014/15 to 2018/19 Funding Allocations for CCGs 4 NHS Choices: Publication of GP Outcomes Data 4.1 As part of NHS England’s drive for more transparency and public participation,
increased information about the standards and performance of primary care was published on the NHS Choices website on 6th December.
4.2 The information, which is a data set of GP outcome standards and high level
indicators, includes screening rates, Quality Outcomes Framework measures, prescribing items and patient survey data. The new ‘accountability view’ published

4
by NHS Choices pulls together a total of 201 indicators across GP practices, hospitals, local authorities and clinical commissioning groups. 40 of these indicators are newly-available on NHS Choices, although they have been in the public domain via other sources, but this is the first time they have been brought together in an easy-access way. The information is also presented in a “below average” “average” and “above average” manner and highlights regional variations in practices.
4.3 National statics on unplanned hospitalisation and full outcomes data can be accessed
via the NHS Choices Website at: http://www.nhs.uk/Service-Search/Accountability
5 Personal Health Budgets – April 2014 Right to Ask
5.1 From April 2014 people who are have a long term condition or are in receipt of continuing health care will have the right to ask for a personal health budget; this will then move to a right to have a Personal Health budget by October 2014. 5.2 The CCG has made the following progress towards achieving this NHS Mandate:
The CCG have begun to develop systems and processes with the Lancashire CSU to ensure that people can access Personal Health Budgets by April 2014
The CCG is working with the Local Authority to scope out the potential for joint health and social care budgets, and this may be as part of the Integrated Transformation Fund.
6 Tobacco Free Lancashire: Revised Tobacco Free Strategy and Terms of Reference 6.1 Tobacco Free Lancashire (TFL) is a collaborative programme which has been in place in Lancashire since 2002, when it was known as the Smokefree Cumbria and Lancashire Partnership. A revised Tobacco Free Strategy and Terms of Reference
have been developed in partnership with a wide range of stakeholder organisations and agencies interested in working together to reduce the devastating impact that tobacco has in Lancashire. The strategy has been endorsed by Tobacco Free Lancashire. 6.2 The final versions will be signed off at the next Tobacco Free Lancashire Alliance Meeting on 5th February 2014, and members of the Governing Body are asked to support this work.
Tobacco Free Lancashire Strategy v2 (revised at 19 12 2013).pdf
Tobacco Free Lancashire Terms of Reference (revised at 19 12 2013).pdf
7 CCG Assurance 7.1 Further to my last update, East Lancashire Clinical Commissioning Group has had its second checkpoint meeting with NHS England on Tuesday 3rd December. Following the meeting, the CCG submitted a populated Quarter 2 action plan on 10th December which detailed the actions required for each domain. These will be continually monitored and progress reported to the NHS England Local Area Team (LAT).
5
8 East Lancashire Hospitals Trust 8.1 On 6th December 13, Mark Brearley stood down from his post as Chief Executive of
East Lancashire Hospitals NHS Trust. Jonathan Wood, Director of Finance has been acting Chief Executive and the Trust has since announced the appointment of Jim Birrell as interim Chief Executive from 6th January 2014.
The Trust Development Agency (NHS TDA) has also confirmed the appointment of
Professor Eileen Fairhurst as the new Chair of ELHT from 1st February 2014. 9 Governing Body Members 9.1 At its meeting in October 13 the Governing Body supported the proposal to appoint an additional Lay Advisor with an interest in Patient Engagement and Quality. The appointment process is now underway and interviews will take place on 4th February. 10 Rossendale Steering Group Elections 10.1 The election of GP Member representatives on the Rossendale Locality Steering Group has now concluded. A total of 29 responses were received out of a distribution of 39 ballot papers, representing a 74% response rate. 10.2 All five of the candidates listed below have been elected to serve on the Steering Group formally from 1 March 2014, and our congratulations go to those individuals. Dr J. Cowdery Dr A. Mannan – re elected Dr T. Mackenzie – re elected Dr J. O’Malley Dr Z. Sykes – re elected 11 Stakeholder Engagement 11.1 As part of the CCG’s proactive programme of engagement with our key
stakeholders, the following meetings have taken place since my last update:
11th November – Meeting with Gordon Birtwistle MP for Burnley
12th November – Meeting with Mark Hindle, CEO Calderstones
14th November - Lancashire Health & Wellbeing Board Development Day
23rd December – Meeting with Mike Leaf, Director of Public Health
21st January – Meeting with Airedale Executive Team
11.2 Actions from these meetings will be handled through the embedded CCG business
processes.
12 Policies and Procedures 12.1 The following policies have been approved and disseminated in line with the policy ‘An Organisation wide Policy for the Development and Management of Policy and Procedural Documents’:

6
Procurement Policy
Local Emergency Planning and Resilience Policy
13 Recommendations 13.1 Members are requested to:
Support the work of Tobacco Free Lancashire
Note the updates within the report
Dr Mike Ions Chief Clinical Officer
1
Agenda Item No: 5.2
REPORT TO:
Governing Body
MEETING DATE:
27th January 2014
REPORT TITLE:
Keogh Review CCG Quality Assurance Framework – positional statement
SUMMARY:
This report is provided to the Governing Body, as a position statement, in relation to the evidence submitted by East Lancashire Hospitals Trust (ELHT) and the wider Health Economy against the CCG Keogh Quality Assurance Framework (QAF).
REPORT CATEGORY: Formally Receipt
Tick
x
Action the recommendations outlined in the report.
Debate the content of the report
Receive the report for information
AUTHOR:
Mrs Jackie Hanson Chief Nurse
PRESENTED BY:
Mrs Jackie Hanson Chief Nurse
COMMITTEES/ GROUPS CONSULTED:
Quality Surveillance Group (ELHT) EL CCG Quality & Safety Committee
Tick
1 Commission the right services for patients to be seen at the right time, in the right place, by the right professional.
x
2 Optimise appropriate use of resources and remove inefficiencies.
3 Improve access, quality and choice of service provision within Primary Care
4 Work with colleagues from Secondary Care and Local Authorities to develop seamless care pathways
x
2
Agenda Item No: 5.2
Governing Body Meeting 27 January 2014
Keogh Review – CCG Quality Assurance Framework positional update
1. Introduction 1.1 This report is provided to the Governing Body, as a position statement, in relation to the
evidence submitted by East Lancashire Hospitals Trust (ELHT) and the wider Health Economy against the CCG Keogh Quality Assurance Framework (QAF).
1.2 Following the publication of the Keogh Review Report in July 2013, East Lancashire
Clinical Commissioning Group (CCG), as lead commissioner for ELHT, along with colleagues from Blackburn with Darwen Clinical CCG, NHS England Lancashire Area Team and ELHT have worked in close collaboration to develop a CCG QAF.
1.3 This Framework is designed to provide Commissioners with the level of assurance
required to be confident that appropriate action is being taken by the Trust to address the issues and concerns raised by the Keogh Team.
2. Purpose of the Quality Assurance Framework. 2.1 As previously reported the Keogh report highlighted a number of areas where
improvements can be made and the CCGs have been committed to working with ELHT to ensure that these are implemented so that all services provided by ELHT become highly regarded and trusted by the people of East Lancashire and beyond
2.2 The framework focuses on 4 key themes identified in the Keogh review report which
are:
Governance & Leadership
Alignment of Strategies Organisational Development, Values & behaviours Patient Experience
2.3 Within each of these areas the specific key lines of enquiry (KLOE) have been
identified from the Keogh review report and then best practice outcomes have been described against each area in order to articulate the expected level of attainment to be achieved by ELHT.
2.4 Furthermore, the framework specifies the overarching and detailed evidence required
to give assurance to the CCG that the appropriate action is being taken, with clear timescales and underpinning key performance indicators that will be monitored to provide further information on progress and impact.
3
3. Delivery of Evidence
3.1 The scrutiny of evidence submitted by ELHT in line with the QAF requirements is currently being managed across the CCGs and the Lancashire Commissioning Support Unit (LCSU) with a collaborative approach with ELHT adopted.
3.2 Whilst it was noted and reported that initial evidence submitted by ELHT provided very
limited assurance, significant work has taken place within the Trust to ensure robust evidence is delivered to the CCG in a timely manner. It has been noted that the quantity of the evidence provided has increased over the last month, but there are concerns about the quality of the evidence in some areas, leading to an ability to provide full assurance.
3.3 Following the submission of evidence colleagues from LSCU and the CCG have
undertaken an intensive review to establish a positional update on the level of assurance obtained and progress made by ELHT against the best practice outcomes.
3.4 The positional update summary as of December 2013 was discussed and agreed at
the CCG Quality and Safety Committee held on the 15th January 2014 and is available at member’s request.
3.5 The positional update has been shared with East Lancashire NHS Hospital Trust and they have confirmed that they agreed with the assessment provided
4. Quality Surveillance Group 4.1 The information attached was provided to the Quality Surveillance Group (ELHT),
organised by Lancashire Area Team which was held on the 11th December 2013. East Lancashire CCG and Blackburn with Darwen CCG were represented alongside the Care Quality Commission, Trust Development Authority and the Area team.
4.2 The Clinical Commissioning Groups have not received the formal minutes from this
meeting yet, however the following points were identified within the discussion:
a) The Trust had engaged with the Quality Assurance Framework process and there was evidence of change in all areas identified. There was agreement by all agencies that progress had been made in addressing all the areas identified, but in some areas pace of change was still slow and the impact on patient experience could not yet be fully demonstrated therefore the level of assurance in all four key areas with judged as being limited.
b) The areas identified within the Quality Surveillance Group for priority action by ELHT were identified as;
Complaints handling – in particular understanding the impact on patient experience from the changes to the complaints handling system,
Safeguarding – particularly in relation to the training rates across all divisions.
Performance in key areas such as A&E, Cancer and Stroke pathways
Quality and Governance leadership. Concern was expressed in relation to the lack of capacity in the current structure due to staff vacancies, which could lead to the organisation not being sighted on the key risks and issues.
4.3 The key points identified above have all been discussed through with the Trust and action has been initiated or enhanced to address the issues in a timely fashion. The impact of these changes will be included in the next update of the Quality Assurance Framework, which will take place at the end of January 2014.
4
4.4 It has been noted by all agencies concerned that the Trust is completing multiple
evidence submissions to both the Trust Development Agency and the Clinical commissioning Group as well as responding the regulatory requirements from the CQC, and although there has been some progress in aligning the information, there are opportunities to do this further, therefore reducing the burden on the Trust and ensuring that the analysis of this is done collaboratively with key agencies.
4.5 The CCG Chief Clinical Officer and Chief Nurse have had brief discussions with the
Improvement Director appointed by the Trust Development Authority(TDA) to work with East Lancashire NHS Hospitals Trust,-(Mrs Marie-Noelle Orzell) The discussion centred on streamlining the TDA and CCG reporting requirements in relation to Keogh. Where possible it was envisaged that the Trust would provide evidence against one framework that focussed on priority actions for the next 30, 60 and 90 day periods, shows impact on patient & staff experience and identifies where monitoring arrangements can now be included in the usual quality meetings within the CCG. These discussions are at an early stage and further reports will be provided to the Governing Body at future meetings on the feasibility of achieving this joint approach that is able to maintain a focus on providing the level of assurance to the CCG as detailed in the current Quality Assurance Framework
5. Recommendations 5.1 Members are asked to:
- Receive the report - Note the current position in relation to evidence submitted and discuss the
subsequent assessment of assurance provided. - Note the potential changes to the Assurance Framework process and discuss the
potential impact on gaining the required assurance.
Mrs Jackie Hanson Chief Nurse

Agenda Item 5.3 Appendix 1
NHS East Lancashire CCG Governing Body
27 January 2014
Accident and Emergency 4 hour Standard Performance Briefing
1. Purpose
The purpose of this briefing is to update the governing body on the current performance for East Lancashire hospitals Trust against the national 95% 4 hour standard for Accident and Emergency patients 2. Background The operational standard for A&E (95% of patients admitted transferred or discharged within 4hours).is a national operational standard and is designed to deliver patients’ rights’ under the NHS constitution. 3. Current Position East Lancashire Hospitals Trust (ELHT) has only achieved the 95% in the first quarter of the year to date and has failed to meet the standard in Quarter 2 and Quarter 3 (93.23 and 91.89% respectively). The current year to date position is 93.15%. Using the daily situation report figures up to and including the 31st December 2013 it would appear that the 2013-14 4hr target maximum number of breaches has been surpassed and ELHT will be unable to recover the position to meet the standard by 31st March 2014. A Performance Trajectory for Quarter 4 is currently being reviewed and will be shared and monitored weekly, ELHT report to the National Trust Development Authority (NTDA) on a weekly basis and provide a Root Cause Analysis for any week where the 95% standard isn’t achieved this is supported by an action plan. 4. Health Economy Actions Since April 2013, the Clinical Commissioning Groups (CCG) and ELHT have worked together to support the achievement of the standard by revising the role, membership and function of the Pennine Lancashire Unscheduled Care Group in line with national recommendations – this group is now known as the Pennine Lancashire Access and Flow Group and has key links with the Integrated Care Agenda. Close liaison with the Lancashire Area Team has also been a key feature with the Director of Operations and Delivery attending the meeting monthly. To support the delivery and subsequent achievement of the 4 hour standard a Health Economy Action plan has been developed and this is monitored through the Pennine
Lancashire Access and Flow Group this is also reported to both East Lancashire and Blackburn CCG’s. The Annual Resilience Plan has been reviewed and a joint Health and Social Care Economy winter plan has been developed with a clear Trigger and Escalation plan in place which identifies clear responsibilities and agreed action from all organisations. Central Winter Investment funds were made available to the Health Economy and these have been utilised in 4 key areas:
Primary Care Access – including the extension of a Primary Care Pathway in Urgent Care.
Ambulatory Care Pathway Pilot
Increased capacity across Health and social Care for 7 day provision of support services, to improve weekend and bank holiday discharges.
Review of the pathway for Continuing Health Care. The impact of these schemes are being monitored and reported to NHS England Local Area team on a monthly basis. Weekly Teleconferences are held with the Director of Operations ELHT, Chief Operating Officer East Lancashire CCG, Head of Unscheduled Care Pennine Lancashire CCG’s and Director of Operations and Deliver NHS England Lancashire Area Team. The teleconference reviews weekly performance, reviews the action plan and also the Performance Trajectory. 5. Next Steps The CCG and key partners from across the health economy will work with EHLT to deliver sustainable improvement on current performance for the Accident and Emergency 4 hour standard. The CCG will liaise with NHS England in relation to the next steps and how the recognition that failure to achieve the 4 hour standard at year end will impact on the health economy. 6. Recommendation The East Lancashire Governing Body is requested to:
Note the contents of this briefing
Acknowledge the actions undertaken
Agree to receive a further update Tim Mansfield Chief Operation Officer

FOR THE NINE MONTH PERIOD TO 31 DECEMBER 2013
&
FORECAST OUT-TURN TO 31 MARCH 2014
FINANCIAL REPORT TO THE
GOVERNING BODY
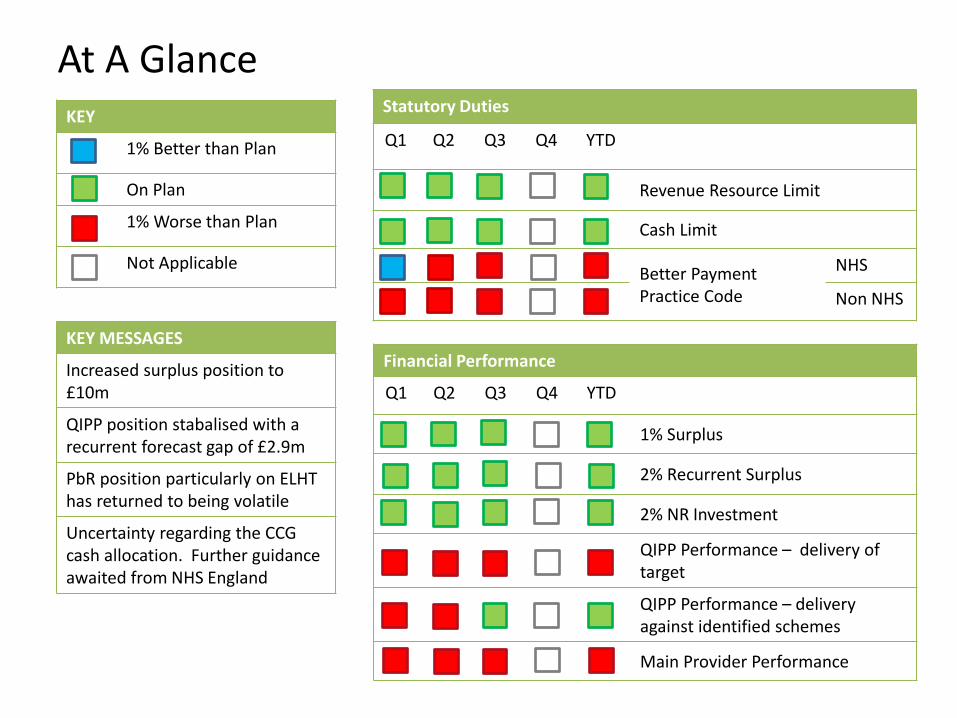
At A Glance KEY
1% Better than Plan
On Plan
1% Worse than Plan
Not Applicable c
Statutory Duties
Q1 Q2 Q3 Q4 YTD
Revenue Resource Limit
Cash Limit
Better Payment Practice Code
NHS
Non NHS
c
c
c
Financial Performance
Q1 Q2 Q3 Q4 YTD
1% Surplus
2% Recurrent Surplus
2% NR Investment
QIPP Performance – delivery of target
QIPP Performance – delivery against identified schemes
Main Provider Performance
KEY MESSAGES
Increased surplus position to £10m
QIPP position stabalised with a recurrent forecast gap of £2.9m
PbR position particularly on ELHT has returned to being volatile
Uncertainty regarding the CCG cash allocation. Further guidance awaited from NHS England
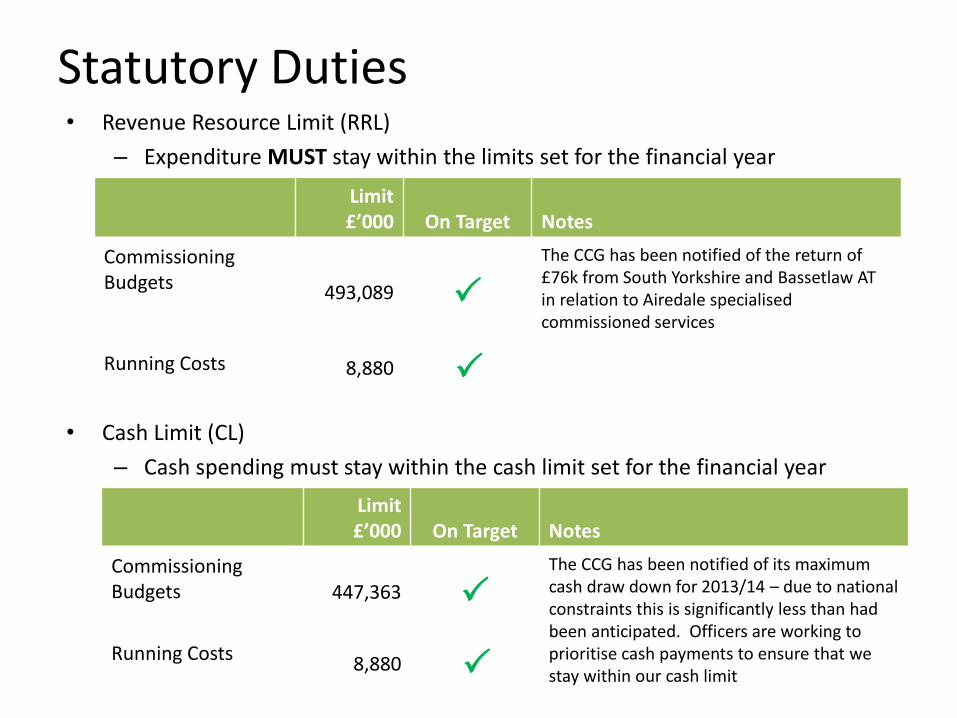
Statutory Duties • Revenue Resource Limit (RRL)
– Expenditure MUST stay within the limits set for the financial year
• Cash Limit (CL)
– Cash spending must stay within the cash limit set for the financial year
Limit £’000 On Target Notes
Commissioning Budgets 493,089 P
The CCG has been notified of the return of £76k from South Yorkshire and Bassetlaw AT in relation to Airedale specialised commissioned services
Running Costs 8,880 P
Limit £’000 On Target Notes
Commissioning Budgets 447,363 P
The CCG has been notified of its maximum cash draw down for 2013/14 – due to national constraints this is significantly less than had been anticipated. Officers are working to prioritise cash payments to ensure that we stay within our cash limit
Running Costs 8,880
P
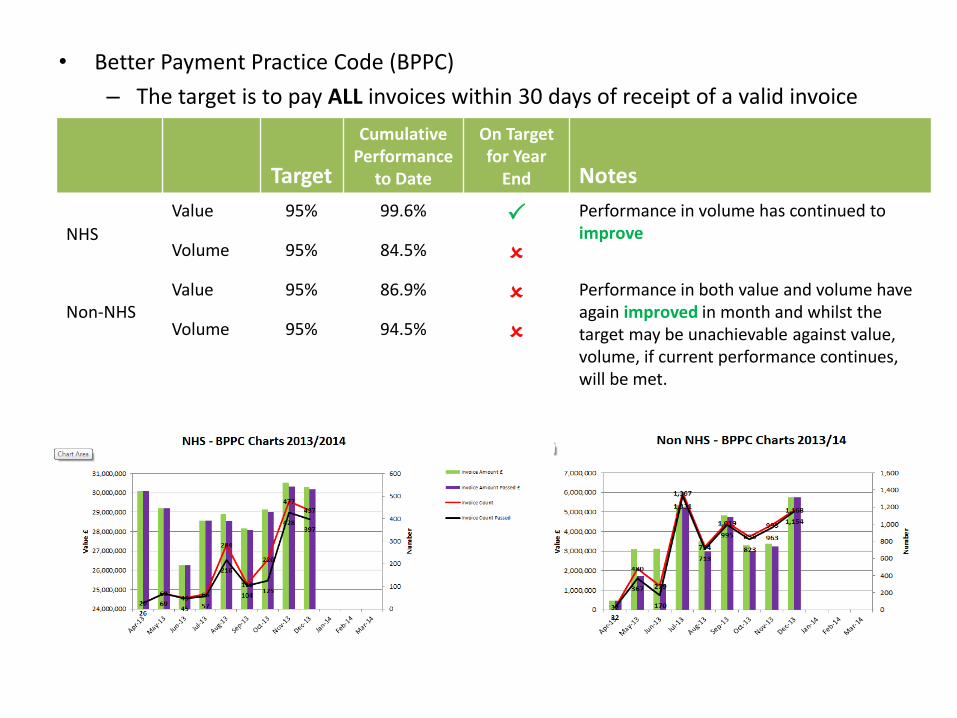
Target
Cumulative Performance
to Date
On Target for Year
End Notes
NHS
Value 95% 99.6% P Performance in volume has continued to improve
Volume 95% 84.5% O
Non-NHS
Value 95% 86.9% O Performance in both value and volume have again improved in month and whilst the target may be unachievable against value, volume, if current performance continues, will be met.
Volume 95% 94.5% O
• Better Payment Practice Code (BPPC)
– The target is to pay ALL invoices within 30 days of receipt of a valid invoice
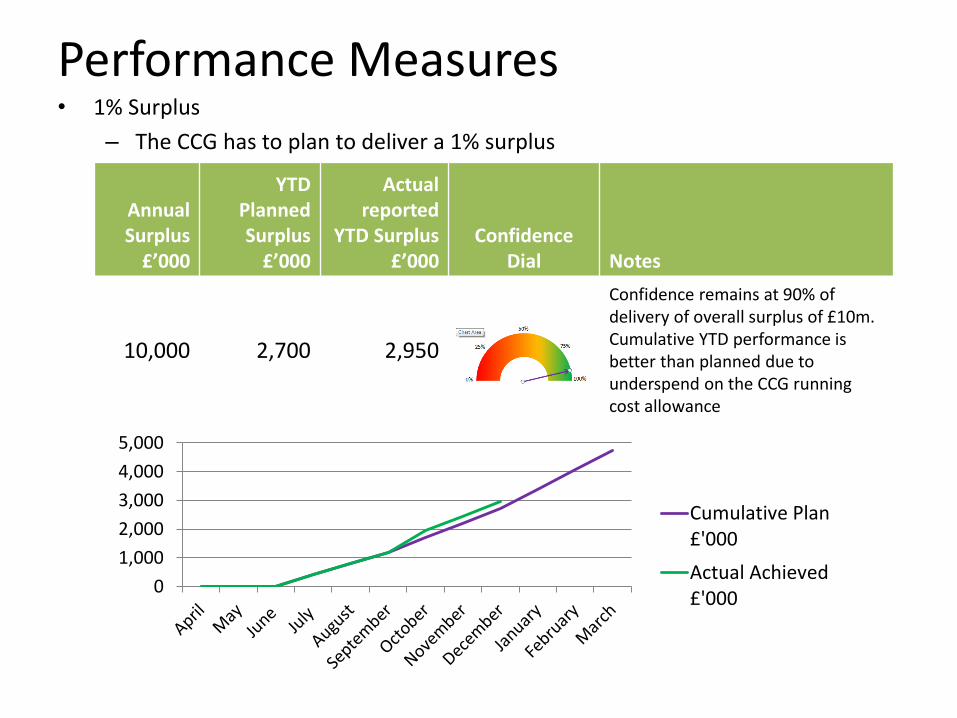
Performance Measures • 1% Surplus
– The CCG has to plan to deliver a 1% surplus
Annual Surplus £’000
YTD Planned Surplus £’000
Actual reported
YTD Surplus £’000
Confidence Dial Notes
10,000 2,700 2,950
Confidence remains at 90% of delivery of overall surplus of £10m. Cumulative YTD performance is better than planned due to underspend on the CCG running cost allowance
0
1,000
2,000
3,000
4,000
5,000
Cumulative Plan£'000
Actual Achieved£'000

• 2% Recurrent Surplus
– The CCG has to keep in reserves 2% of its recurrent resource. This is to be invested non-recurrently
• 2% Non-recurrent investment – The CCG has to invest its 2% recurrent reserve on a non-recurrent basis in
order to lever transformational change and deliver the QIPP programme
2% Surplus £’000 Confidence Dial Notes
9,740
The 2% has to be retained on a recurrent basis and is used as a performance measure of organisational sustainability. Recurrent pressures can be absorbed without utilising the 2% reserve
Annual budget £’000
YTD Planned
Expenditure £’000
Actual reported
YTD Expenditure
£’000 Confidence
Dial Notes
9,740 6,390 6,390
The uncommitted balance forms part of the CCGs current planning to invest non-recurrent funding to pump prime delivery of 2014/15 QIPP

• Total QIPP Schemes – Achievement of target
• QIPP Scheme Delivery
– Analysis of identified QIPP schemes and delivery against savings plans to date
Identified Schemes
£’000
YTD Planned Savings £’000
Actual reported
Savings £’000
Confidence Dial Notes
7,137 4,870 4,870
The confidence level of achieving the £7.1m QIPP savings through identified schemes has improved further this month
Total QIPP
Target £’000
Identified schemes
£’000 QIPP Gap
£’000 Confidence
Dial Notes
10,000 7,100 2,900
There is very little confidence that tthe gap of £2.9m will be met by ssavings schemes. The gap will be ccovered by contingencies, slippage aand reserves from elsewhere in the CCG budget
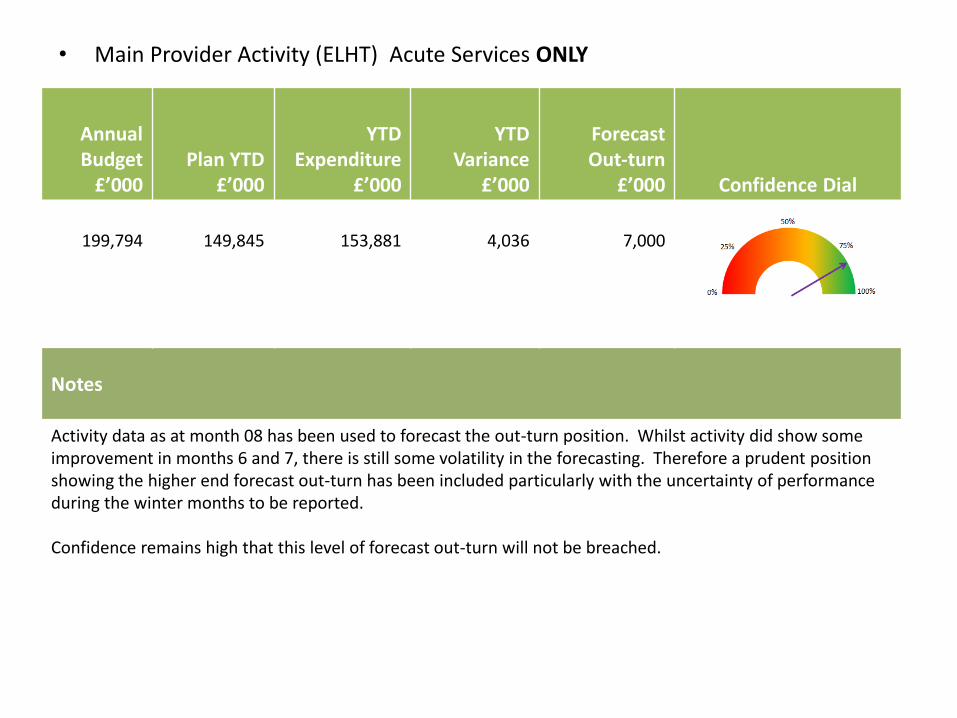
• Main Provider Activity (ELHT) Acute Services ONLY
Annual Budget £’000
Plan YTD £’000
YTD Expenditure
£’000
YTD Variance
£’000
Forecast Out-turn
£’000 Confidence Dial
199,794
149,845
153,881
4,036
7,000
Notes
Activity data as at month 08 has been used to forecast the out-turn position. Whilst activity did show some improvement in months 6 and 7, there is still some volatility in the forecasting. Therefore a prudent position showing the higher end forecast out-turn has been included particularly with the uncertainty of performance during the winter months to be reported. Confidence remains high that this level of forecast out-turn will not be breached.
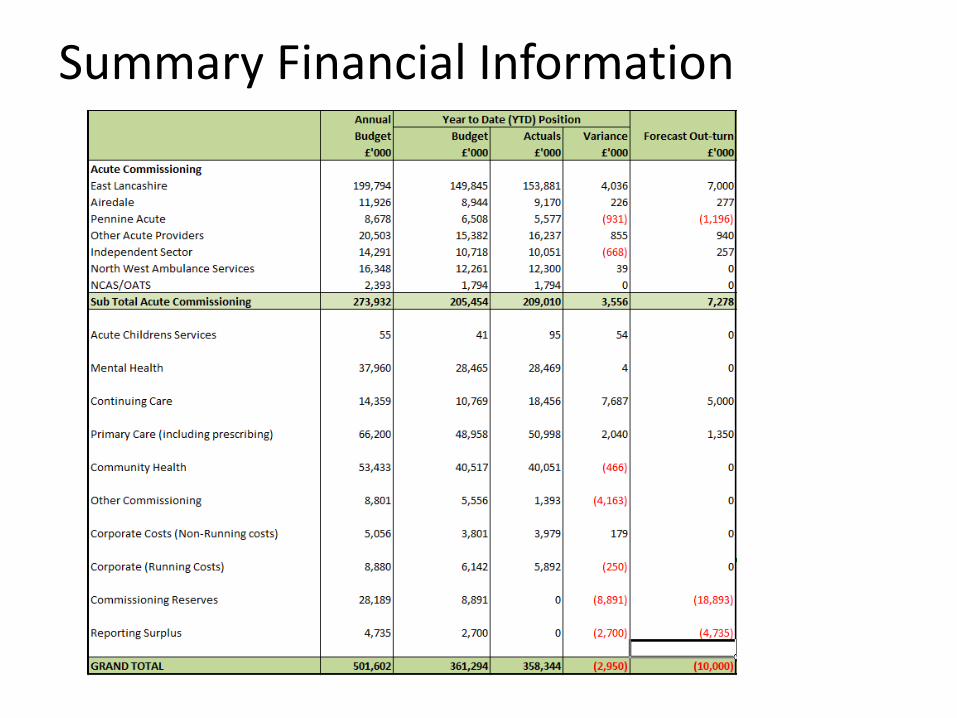
Summary Financial Information
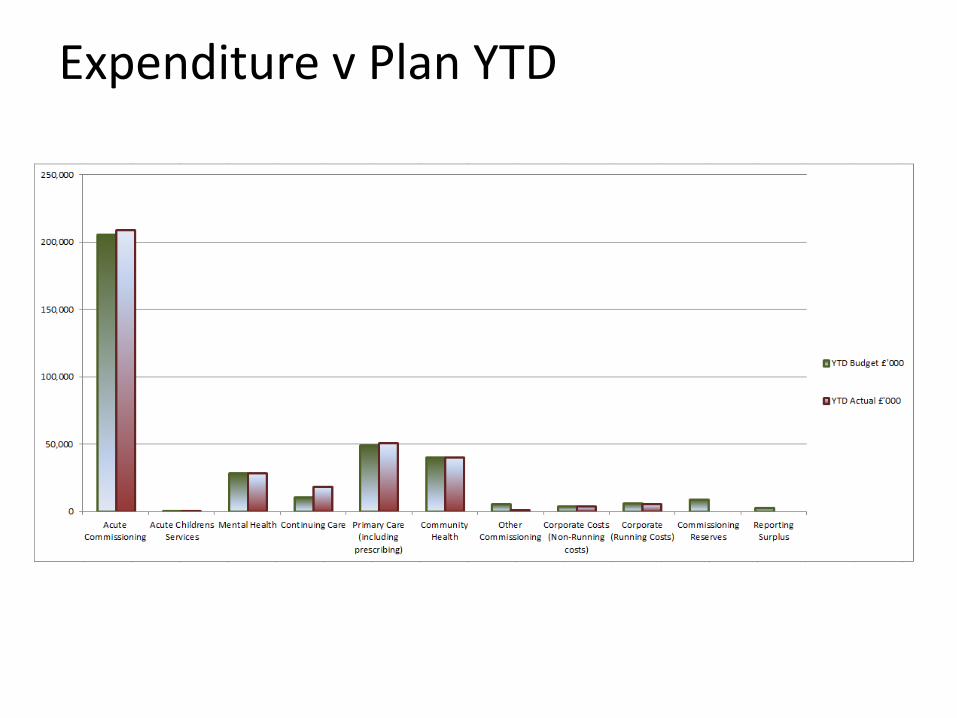
Expenditure v Plan YTD
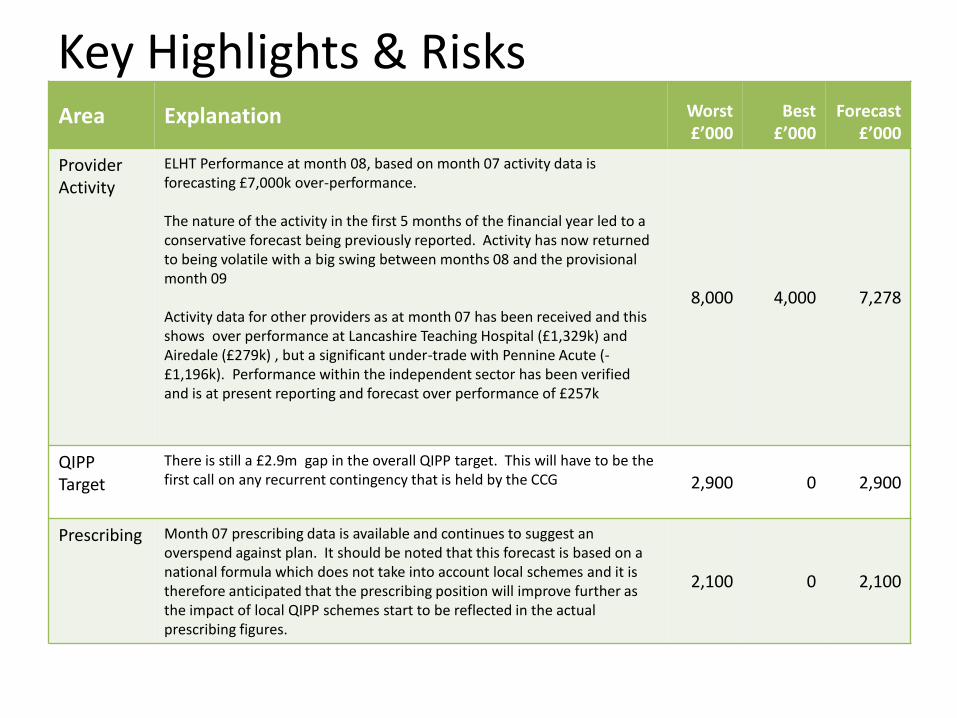
Key Highlights & Risks Area Explanation Worst
£’000 Best £’000
Forecast £’000
Provider Activity
ELHT Performance at month 08, based on month 07 activity data is forecasting £7,000k over-performance. The nature of the activity in the first 5 months of the financial year led to a conservative forecast being previously reported. Activity has now returned to being volatile with a big swing between months 08 and the provisional month 09 Activity data for other providers as at month 07 has been received and this shows over performance at Lancashire Teaching Hospital (£1,329k) and Airedale (£279k) , but a significant under-trade with Pennine Acute (-£1,196k). Performance within the independent sector has been verified and is at present reporting and forecast over performance of £257k
8,000 4,000 7,278
QIPP Target
There is still a £2.9m gap in the overall QIPP target. This will have to be the first call on any recurrent contingency that is held by the CCG 2,900 0 2,900
Prescribing Month 07 prescribing data is available and continues to suggest an overspend against plan. It should be noted that this forecast is based on a national formula which does not take into account local schemes and it is therefore anticipated that the prescribing position will improve further as the impact of local QIPP schemes start to be reflected in the actual prescribing figures.
2,100 0 2,100

Area Explanation Worst £’000
Best £’000
Forecast £’000
IPA Up to date figures from the Broadcare system suggest an over performance of £5m, this is a significant worsening of the position over the previously reported out-turn. This would represent a 28% increase in expenditure on CHC, IFR, Complex cases and nursing homes. It excludes the impact of any retrospective restitution cases which are for accounted for on balance sheet. Colleagues are working with members of the CSU to understand this swing in position and to ensure that the database is accurately reflecting the financial position. For prudence the whole of the estimated overspend has been included in the forecast position.
5,000 0 5,000
Reserves & contingencies
As directed, the CCG is holding a 1% recurrent contingency. The first call on this would need to be the unidentified QIPP gap, followed by over-performance 0 (2,368) 0
Allocation issues
There are no outstanding allocation issues at present 0 0 0
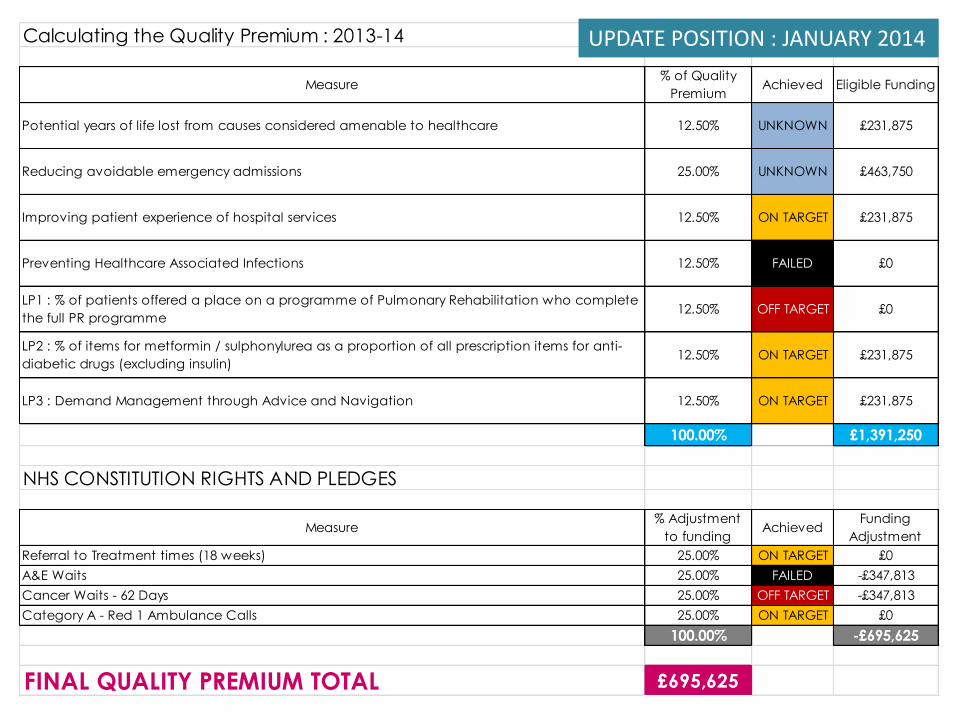
Calculating the Quality Premium : 2013-14
Measure% of Quality
PremiumAchieved Eligible Funding
Potential years of life lost from causes considered amenable to healthcare 12.50% UNKNOWN £231,875
Reducing avoidable emergency admissions 25.00% UNKNOWN £463,750
Improving patient experience of hospital services 12.50% ON TARGET £231,875
Preventing Healthcare Associated Infections 12.50% FAILED £0
LP1 : % of patients offered a place on a programme of Pulmonary Rehabilitation who complete
the full PR programme12.50% OFF TARGET £0
LP2 : % of items for metformin / sulphonylurea as a proportion of all prescription items for anti-
diabetic drugs (excluding insulin)12.50% ON TARGET £231,875
LP3 : Demand Management through Advice and Navigation 12.50% ON TARGET £231,875
100.00% £1,391,250
NHS CONSTITUTION RIGHTS AND PLEDGES
Measure% Adjustment
to fundingAchieved
Funding
Adjustment
Referral to Treatment times (18 weeks) 25.00% ON TARGET £0
A&E Waits 25.00% FAILED -£347,813
Cancer Waits - 62 Days 25.00% OFF TARGET -£347,813
Category A - Red 1 Ambulance Calls 25.00% ON TARGET £0
100.00% -£695,625
FINAL QUALITY PREMIUM TOTAL £695,625
UPDATE POSITION : JANUARY 2014
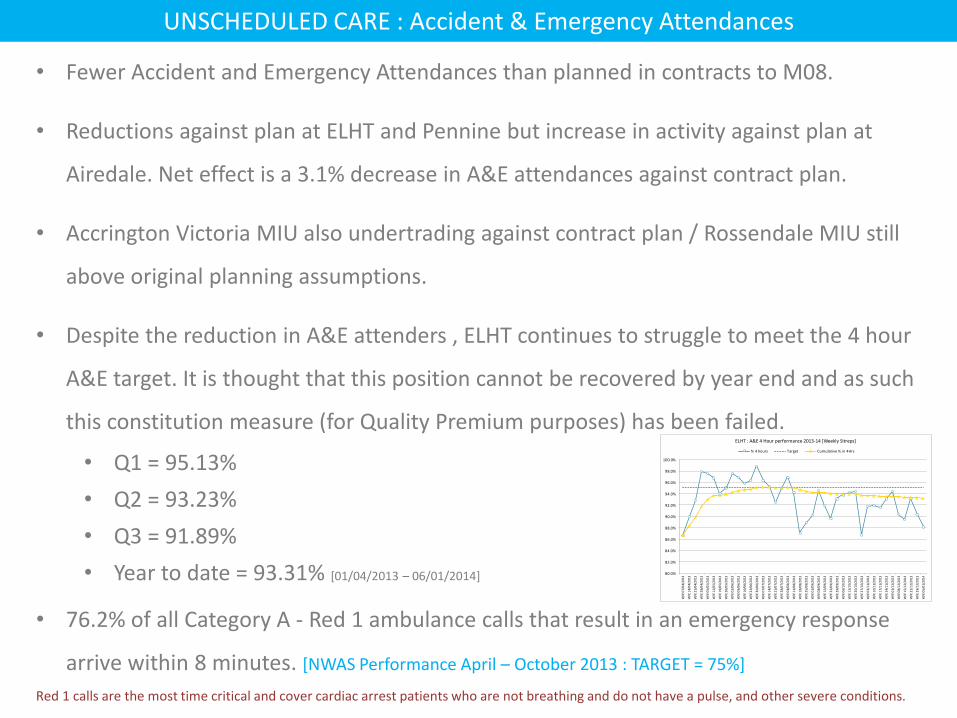
UNSCHEDULED CARE : Accident & Emergency Attendances
• Fewer Accident and Emergency Attendances than planned in contracts to M08.
• Reductions against plan at ELHT and Pennine but increase in activity against plan at
Airedale. Net effect is a 3.1% decrease in A&E attendances against contract plan.
• Accrington Victoria MIU also undertrading against contract plan / Rossendale MIU still
above original planning assumptions.
• Despite the reduction in A&E attenders , ELHT continues to struggle to meet the 4 hour
A&E target. It is thought that this position cannot be recovered by year end and as such
this constitution measure (for Quality Premium purposes) has been failed.
• Q1 = 95.13%
• Q2 = 93.23%
• Q3 = 91.89%
• Year to date = 93.31% [01/04/2013 – 06/01/2014]
• 76.2% of all Category A - Red 1 ambulance calls that result in an emergency response
arrive within 8 minutes. [NWAS Performance April – October 2013 : TARGET = 75%]
Red 1 calls are the most time critical and cover cardiac arrest patients who are not breathing and do not have a pulse, and other severe conditions.
80.0%
82.0%
84.0%
86.0%
88.0%
90.0%
92.0%
94.0%
96.0%
98.0%
100.0%
W/E
07/
04/
201
3
W/E
14/
04/
201
3
W/E
21/
04/
201
3
W/E
28/
04/
201
3
W/E
05/
05/
201
3
W/E
12/
05/
201
3
W/E
19/
05/
201
3
W/E
26/
05/
201
3
W/E
02/
06/
201
3
W/E
09/
06/
201
3
W/E
16/
06/
201
3
W/E
23/
06/
201
3
W/E
30/
06/
201
3
W/E
07/
07/
201
3
W/E
14/
07/
201
3
W/E
21/
07/
201
3
W/E
28/
07/
201
3
W/E
04/
08/
201
3
W/E
11/
08/
201
3
W/E
18/
08/
201
3
W/E
25/
08/
201
3
W/E
01/
09/
201
3
W/E
08/
09/
201
3
W/E
15/
09/
201
3
W/E
22/
09/
201
3
W/E
29/
09/
201
3
W/E
06/
10/
201
3
W/E
13/
10/
201
3
W/E
20/
10/
201
3
W/E
27/
10/
201
3
W/E
03/
11/
201
3
W/E
10/
11/
201
3
W/E
17/
11/
201
3
W/E
24/
11/
201
3
W/E
01/
12/
201
3
W/E
08/
12/
201
3
W/E
15/
12/
201
3
W/E
22/
12/
201
3
W/E
29/
12/
201
3
W/E
05/
01/
201
4
ELHT : A&E 4 Hour performance 2013-14 [Weekly Sitreps]
% 4 hours Target Cumulative % in 4Hrs
UNSCHEDULED CARE : Emergency Admissions [1]
• Volume of emergency admissions (contracted providers) is lower than planned levels to
November 2013 (-650 spells)
• Most providers are reporting fewer emergency admissions than planned for, including
ELHT and Pennine Acute.
• It is important to note that in most instances the plan for emergency admissions was set
at last years outturn levels. National benchmarking identifies that the CCG has higher
than expected emergency admissions in several specialties, especially Paediatrics.
• Excess Bed Day costs for patients admitted as an emergency are significantly higher
than planned (+£807k). The majority of this is being reported @ ELHT.
• The seasonal activity increase starting in October has started to be observed but at
levels lower than those seen in 2012-13.
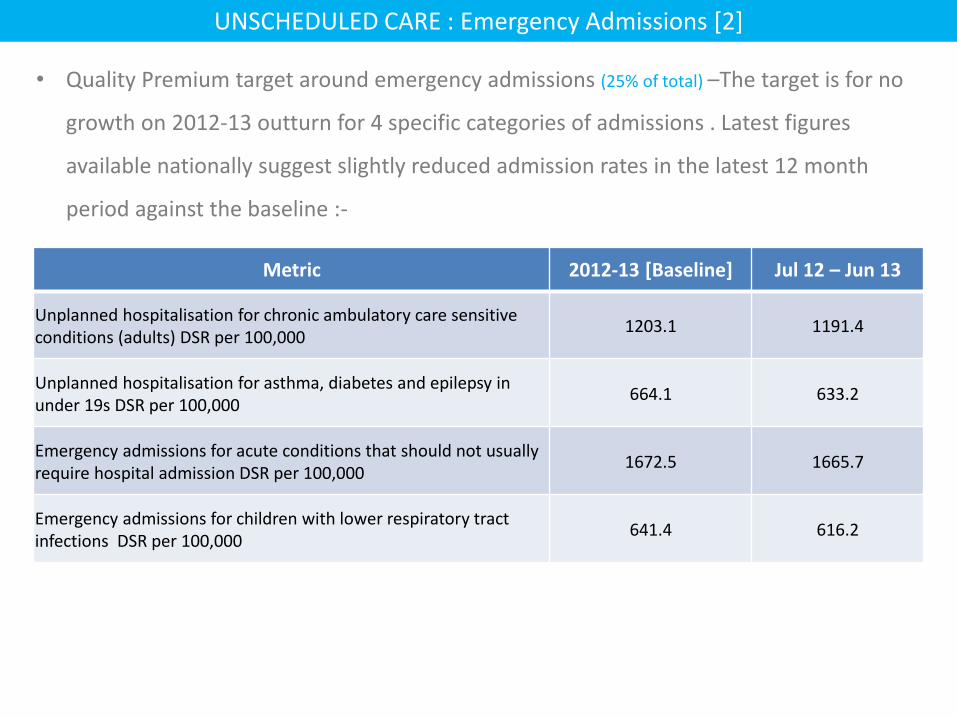
UNSCHEDULED CARE : Emergency Admissions [2]
• Quality Premium target around emergency admissions (25% of total) –The target is for no
growth on 2012-13 outturn for 4 specific categories of admissions . Latest figures
available nationally suggest slightly reduced admission rates in the latest 12 month
period against the baseline :-
Metric 2012-13 [Baseline] Jul 12 – Jun 13
Unplanned hospitalisation for chronic ambulatory care sensitive conditions (adults) DSR per 100,000
1203.1 1191.4
Unplanned hospitalisation for asthma, diabetes and epilepsy in under 19s DSR per 100,000
664.1 633.2
Emergency admissions for acute conditions that should not usually require hospital admission DSR per 100,000
1672.5 1665.7
Emergency admissions for children with lower respiratory tract infections DSR per 100,000
641.4 616.2
-1,000
0
1,000
2,000
3,000
4,000
1 2 3 4 5 6 7 8 9 10 11 12
Act
ivit
y
Month
Activity Chart
Cumulative Var Plan Actual
UNSCHEDULED CARE : Emergency Admissions [3]
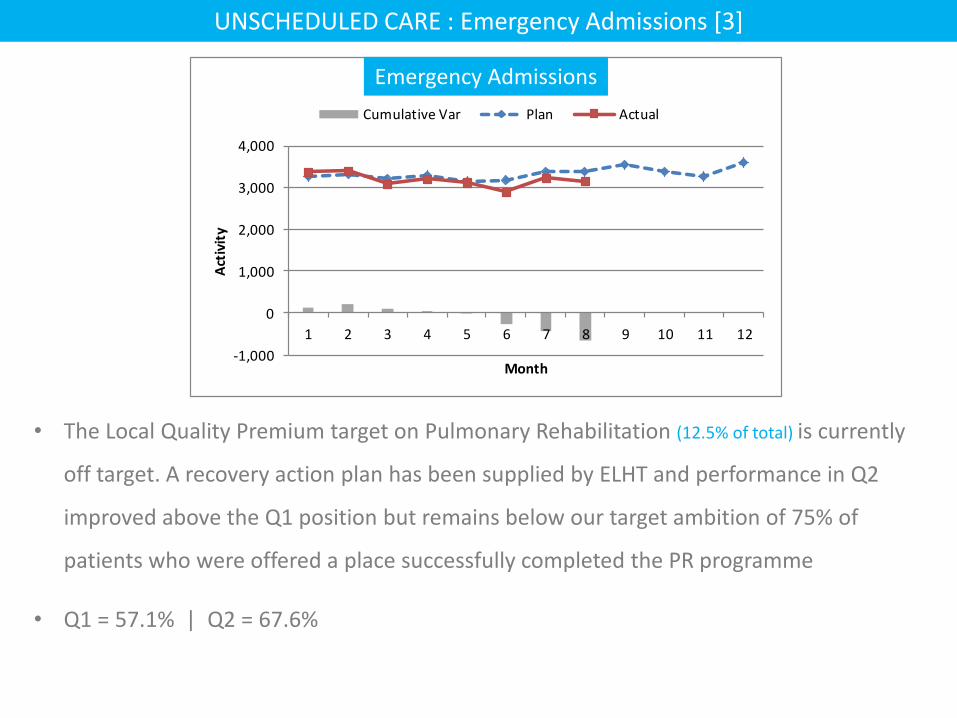
• The Local Quality Premium target on Pulmonary Rehabilitation (12.5% of total) is currently
off target. A recovery action plan has been supplied by ELHT and performance in Q2
improved above the Q1 position but remains below our target ambition of 75% of
patients who were offered a place successfully completed the PR programme
• Q1 = 57.1% | Q2 = 67.6%
Emergency Admissions
SCHEDULED CARE : Referrals & Outpatients [1]
• GP referrals to ELHT are slightly lower than last year (based on working days in the month –
approx. 0.6 fewer referrals per day)
• There have been reductions in ‘Urgent’ GP referrals and an increase in ‘2-week rule’
suspected cancer referrals.
• ELHT have reported increases in first OP attendances across several specialties including
Cardiology, Surgery, Orthopaedics and ENT.
• Pennine Acute is reporting fewer first OP attendances in Orthopaedics.
• Non-Admitted 18 week referral to treatment times are being maintained well within
threshold levels. Neurology poses the greatest challenge (YTD position= 89.73% against
a 95% target) and this is mainly through activity at Lancashire Teaching Hospitals.
SCHEDULED CARE : Referrals & Outpatients [2]
• Advice and Navigation scheme now available to all localities . This is focused on the key
specialties of Orthopaedics, Dermatology and General Surgery. Utilisation of this
scheme and anticipated ‘deflection’ activity is currently ‘On Target’ to deliver against
the local Quality Premium measure (12.5% of total) .
• Outpatient procedures are significantly overtrading against plan, particularly at ELHT.
• Dermatology OPPROCs are 39% higher than planned (+2,867 attendances / +£351k)
across all providers with the bulk of this being driven by HRG : JC14Z – Skin Therapies
Level 2.
• Dermatology Outpatient follow-ups have reduced by a similar volume (but at a lower
unit price) (-2,755 attendances / -£196k)
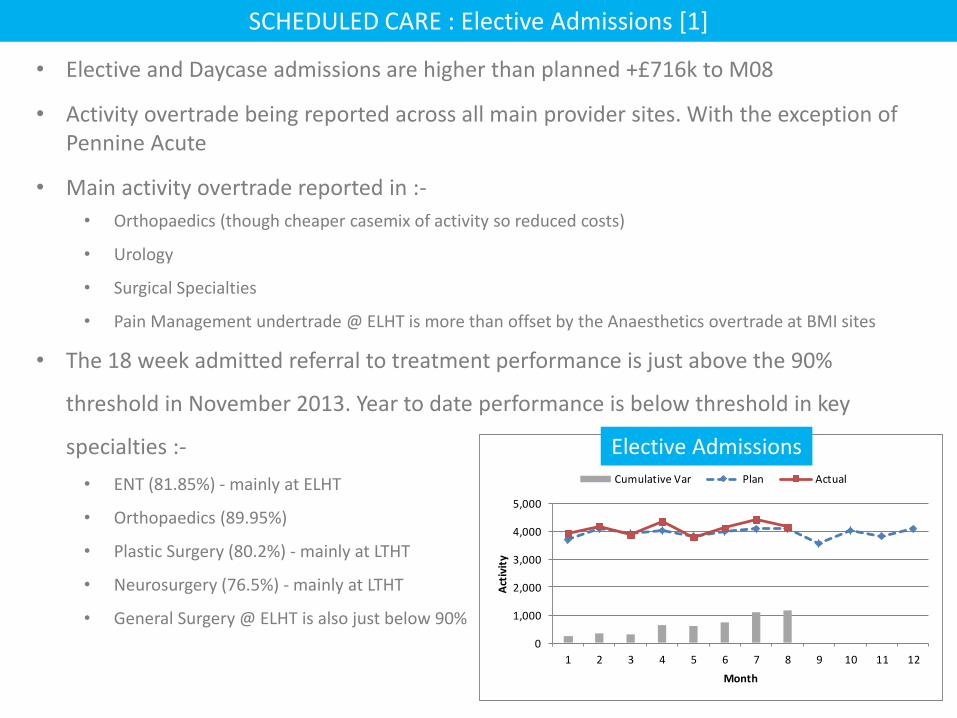
• Elective and Daycase admissions are higher than planned +£716k to M08
• Activity overtrade being reported across all main provider sites. With the exception of Pennine Acute
• Main activity overtrade reported in :-
• Orthopaedics (though cheaper casemix of activity so reduced costs)
• Urology
• Surgical Specialties
• Pain Management undertrade @ ELHT is more than offset by the Anaesthetics overtrade at BMI sites
• The 18 week admitted referral to treatment performance is just above the 90%
threshold in November 2013. Year to date performance is below threshold in key
specialties :-
• ENT (81.85%) - mainly at ELHT
• Orthopaedics (89.95%)
• Plastic Surgery (80.2%) - mainly at LTHT
• Neurosurgery (76.5%) - mainly at LTHT
• General Surgery @ ELHT is also just below 90%
SCHEDULED CARE : Elective Admissions [1]
0
1,000
2,000
3,000
4,000
5,000
1 2 3 4 5 6 7 8 9 10 11 12
Act
ivit
y
Month
Activity Chart
Cumulative Var Plan Actual
Elective Admissions
SCHEDULED CARE : Elective Admissions [2]
• ENT activity is running slightly above plan @ ELHT yet the waiting list position and
delivery of 18 weeks continues to be challenging. It is worth noting that there is an
increasing undertrade against this specialty @ BMI Gisburne Park which would suggest
there is some capacity in the system to support managing these patients
• Delivery against the 18 week Incomplete Pathways measure is currently at 95.12% (YTD)
against a target of 92% and is therefore ‘on target’ for Quality Premium payments.
• 30 patients have been waiting longer than 36 weeks at the end of November 2013.
• 9 of these are at LTHT for Plastic Surgery (5) and Neurosurgery(3)
• 14 patients are waiting at Central Manchester, the majority for Specialist Paediatrics
0.0%
2.0%
4.0%
6.0%
8.0%
10.0%
12.0%
14.0%
16.0%
18.0%
0.00
10.00
20.00
30.00
40.00
50.00
60.00
April 2013 May 2013 June 2013 July 2013 August 2013 September2013
October2013
November2013
% R
esp
on
se R
ate
Ne
t P
rom
ote
r Sc
ore
Friends and Family Test : A&E
ELHT - Net Promoter Score National - Net Promoter Score
ELHT - Response Rate National - Response Rate
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
60.00
62.00
64.00
66.00
68.00
70.00
72.00
74.00
76.00
78.00
80.00
April 2013 May 2013 June 2013 July 2013 August 2013 September2013
October2013
November2013
% R
esp
on
se R
ate
Ne
t P
rom
ote
r Sc
ore
Friends and Family Test : INPATIENTS
ELHT - Net Promoter Score National - Net Promoter Score
ELHT - Response Rate National - Response Rate
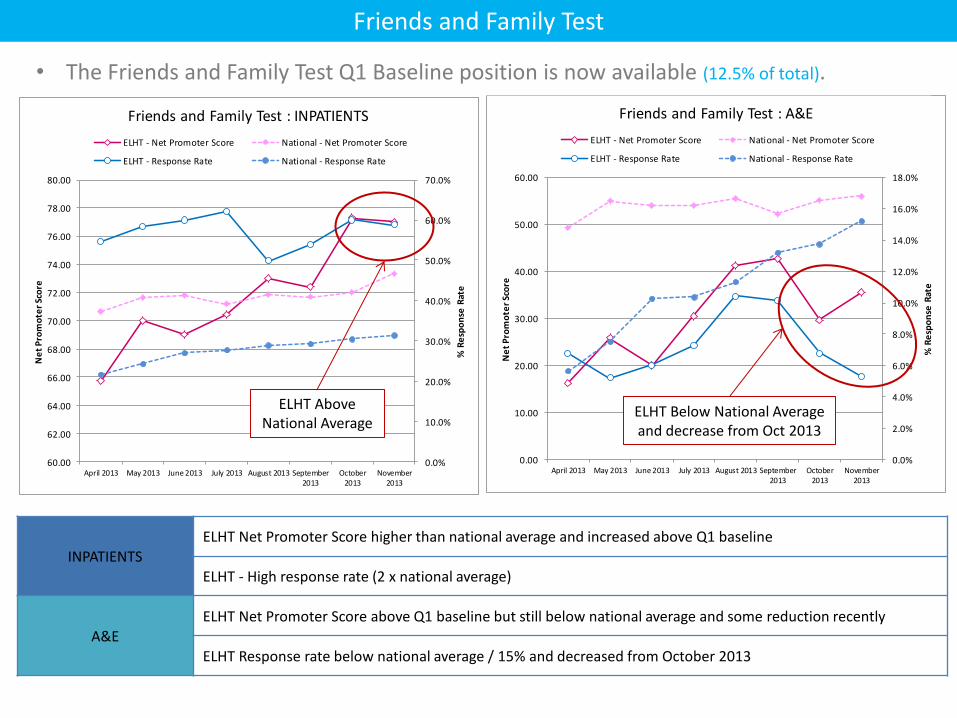
Friends and Family Test
• The Friends and Family Test Q1 Baseline position is now available (12.5% of total).
INPATIENTS ELHT Net Promoter Score higher than national average and increased above Q1 baseline
ELHT - High response rate (2 x national average)
A&E ELHT Net Promoter Score above Q1 baseline but still below national average and some reduction recently
ELHT Response rate below national average / 15% and decreased from October 2013
ELHT Above National Average
ELHT Below National Average and decrease from Oct 2013

OTHER
• The Healthcare Acquired infections aspect of the Quality Premium has been failed (12.5%
of total) . Although the number of C.Diff cases is within the profiled annual trajectory,
there have been 6 reported MRSA cases against a zero case threshold.
• The latest update on the local quality premium metric around anti-diabetic drug
prescribing (12.5% of total) shows that we are edging very close to the national position
which we had set as the aspirational target.
• The year-to-to date position against the 62-day wait from urgent GP referral to first
definitive treatment for cancer is lower than the required threshold (84.77% against a
target of 85%). Performance has been improving over the past few months .
• More patients are being reported with rehabilitation bed days than planned for.
Agenda Item No: 5.4
REPORT TO:
NHS EL CCG Governing Body
MEETING DATE:
27 January 2014
REPORT TITLE:
COMMUNICATION AND ENGAGEMENT : April – December 2013
SUMMARY:
The report outlines progress against the communication and engagement agenda during the period April – December 2013.
REPORT CATEGORY: Formally Receipt
Tick
Action the recommendations outlined in the report.
Debate the content of the report
Receive the report for information
AUTHOR:
CSU Communications
PRESENTED BY:
Angela Brown Head Of Corporate Affairs
COMMITTEES/ GROUPS CONSULTED:
Which Strategic Objective does the report relate to
Tick
1 Commission the right services for patients to be seen at the right time, in the right place, by the right professional.
2 Optimise appropriate use of resources and remove inefficiencies.
3 Improve access, quality and choice of service provision within Primary Care
4 Work with colleagues from Secondary Care and Local Authorities to develop seamless care pathways

Agenda Item: 5.4
EAST LANCASHIRE CLINICAL COMMISSIONING GROUP (CCG)
27 January 2014
Communication and Engagement: April – December 2013
1. Introduction
This report provides a summary of communication and engagement activity over the period April – December 2013. Communication and engagement refers to activities, which seek to build the relationships and reputation of the CCG and to use the intelligence from such activities to inform clinical commissioning and quality monitoring. The purpose of this report is to evidence progress and inform activity for the coming three to six months.
The report provides information concerning key aspects of communication support to the CCG: PR, media relations and marketing, Freedom of Information (FoI) requests, social media and web based communication. It also provides information concerning key aspects of engagement support to the CCG including: complaints, compliments, concerns and comments, as well as engagement, market research and insight undertaken. The CCG has lead officers responsible for specific areas covered in this report, namely the Head of Corporate Affairs, Corporate Communications (including staff, stakeholder, FOI’s, website). Chief Operating Officer– Patient and member engagement. An agreed CCG communication and engagement strategy and work plan are the key drivers for most of the activity described.
A forward look highlighting main areas of activity and development is also included.
2. Overall assessment
Since April 2013, the CCG has steadily built its communications and engagement activities and raised its profile within the East Lancashire area. The focus of communications and engagement activity has been around:
- The gathering of qualitative information and soft intelligence about service provision and quality, including the development of the ‘Connect’ initiative and listening events.
- Communications and engagement/patient education on a range of strategically important issues, including urgent care demand management
- Engagement and, where required, formal consultation on developments including the review of the Rossendale Minor Injuries Unit (MIU) contract, the review of the service at the Accrington GP walk-in centre and Lancashire-wide dementia services review.
- Media relations to support operational objectives, such as the winter campaign and minor illnesses and self-care.
- Support for GP engagement through production of the corporate brief and building links to locality groupings through locality managers and steering
groups. - Support for stakeholder engagement via health summits and planning for
engagement in relation to service changes. Media relations has been increased, with additional opportunities identified and
additional proactive work, in addition to reactive responses to major issues such as East Lancashire Hospitals NHS Trust being in special measures and reactions to the review of the provision of the Accrington GP walk-in centre.
3 4 5
Context This report provides information concerning communication and engagement activities supported by the communication and engagement team of NHS Staffordshire and Lancashire Commissioning Support Unit (CSU). Communication activities include: media management, marketing, website and social media, and FOI management. Engagement activities include insight and market research, complaints management, patient and public involvement and membership. Communications: overview This has been a period of positioning the CCG to achieve more prominence in the media and building relationships with stakeholders. One of the challenges for the CCG has been the scale of media interest and coverage of the acute trust with significant issues, particularly around Keogh. This has clouded perceptions of the NHS in Pennine Lancashire. The positioning of the CCG in this environment has been to convey leadership, reassurance and assurance of scrutiny and stewardship. In recognition of this environment, a significant amount of work has been done in relation to reputation and issues management. Communications and engagement links across Pennine Lancashire, in particular between both CCGs have been developed. A Pennine Lancashire communications group has been established, led by the head of locality for communication and engagement for East Lancashire and BwD CCGs. Membership includes the council, county council, acute trust and mental health trust. This is helping to ensure co-ordinated, consistent and coherent communication occurs. As a result of this additional strategic activity, there has been a notable increase in print and radio coverage. Web and social media: overview The CCG now has a vibrant and actively functioning website which is building a regular following of users. Similarly the number of followers to the CCG Twitter account is growing. These channels will be actively promoted to build a larger following and encourage these platforms as a means to engage with the CCG further. The CCG has agreed that the website and an extranet/intranet will be hosted in-house from April 2014. Work is ongoing to design a process for developing this work.
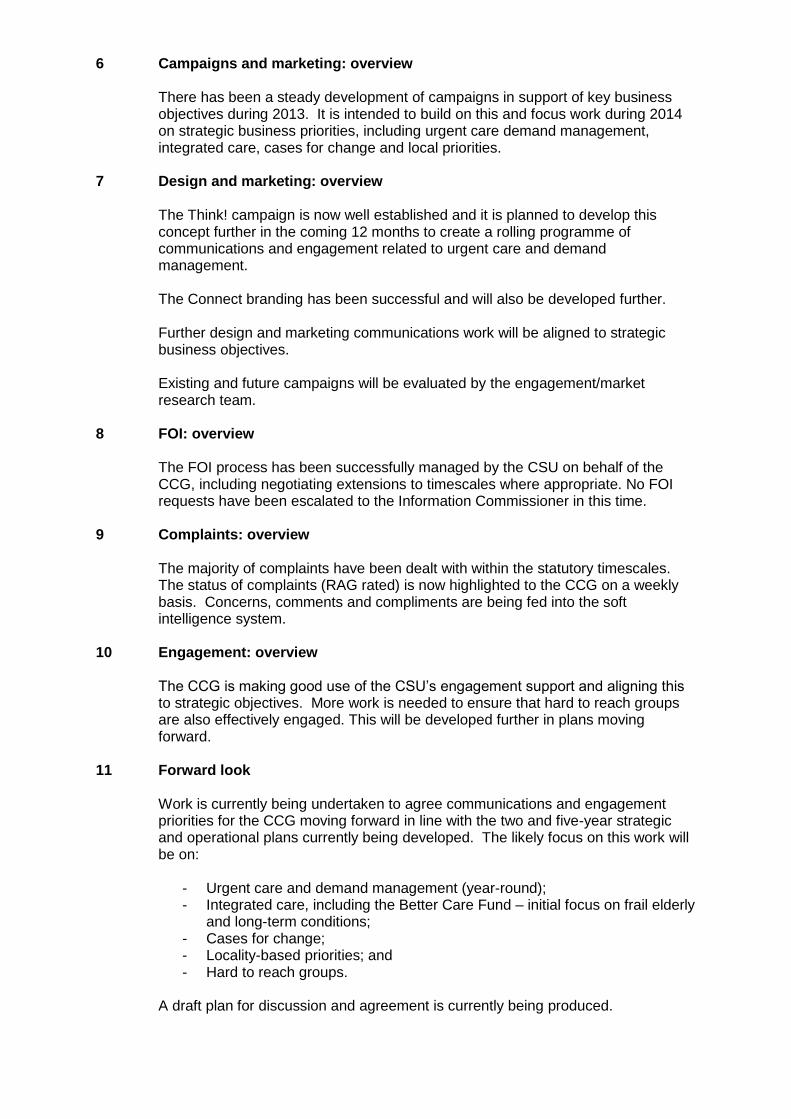
6 7 8 9 10 11
Campaigns and marketing: overview There has been a steady development of campaigns in support of key business objectives during 2013. It is intended to build on this and focus work during 2014 on strategic business priorities, including urgent care demand management, integrated care, cases for change and local priorities. Design and marketing: overview The Think! campaign is now well established and it is planned to develop this concept further in the coming 12 months to create a rolling programme of communications and engagement related to urgent care and demand management. The Connect branding has been successful and will also be developed further. Further design and marketing communications work will be aligned to strategic business objectives. Existing and future campaigns will be evaluated by the engagement/market research team. FOI: overview The FOI process has been successfully managed by the CSU on behalf of the CCG, including negotiating extensions to timescales where appropriate. No FOI requests have been escalated to the Information Commissioner in this time. Complaints: overview The majority of complaints have been dealt with within the statutory timescales. The status of complaints (RAG rated) is now highlighted to the CCG on a weekly basis. Concerns, comments and compliments are being fed into the soft intelligence system. Engagement: overview The CCG is making good use of the CSU’s engagement support and aligning this to strategic objectives. More work is needed to ensure that hard to reach groups are also effectively engaged. This will be developed further in plans moving forward. Forward look Work is currently being undertaken to agree communications and engagement priorities for the CCG moving forward in line with the two and five-year strategic and operational plans currently being developed. The likely focus on this work will be on:
- Urgent care and demand management (year-round); - Integrated care, including the Better Care Fund – initial focus on frail elderly
and long-term conditions; - Cases for change; - Locality-based priorities; and - Hard to reach groups.
A draft plan for discussion and agreement is currently being produced.
12
Conclusion There has been a solid and steady programme of communications and engagement work from April 2013 onwards. Aligning this work with strategic and operational priorities moving forward will enable the CCG to build on this foundation and provide increased evidence of effective communications and engagement to inform commissioning decisions, service quality monitoring and service review and development.
13 Recommendations The Governing Body is asked to:
- Note the content of the report. - Note the work completed from April to December 2013
David Rogers Senior Executive – Communication and Engagement, SLCSU Colette Booth Head of Locality Communications and Engagement, East Lancashire CCG/ SLCSU

Appendix
Communications
The CCG has a growing media presence in local print and radio.
There were a total of 107 stories in print media in the first six months of the year, the majority
of these were favourable (see Figure 1, below)
Of the 107 articles, 68 were positive, 25 neutral and 14 negative.
Media interest has been focused on: (1) Changes to services/commissioning decisions and
discussions (e.g. Accrington and Rossendale) (2) General proactive health messages, e.g.
winter and self-care. (3) Issues at East Lancashire Hospitals NHS Trust, of which ELCCG is
the lead commissioner.
The CCG has achieved a significant level of broadcast media interest. In particular, there
has been radio and TV interest in the Health Access Centre developments, and dementia
services, as well as the Keogh review. All have been potentially contentious issues, but the
CCG position was presented well, in a balanced way.
Over the last six months, the balance of media engagement has shifted towards more
proactive media responses as the CCG has evolved and developed its plans. This in turn
has led to more proactive media engagement.
A total of 47 media releases have been researched, written and issued and 34 reactive
media enquiries dealt with. In addition to this, working relationships with key journalists,
notably on the Lancashire Telegraph, BBC Radio Lancashire and the Rossendale Observer
have been developed and strengthened.
Media and stakeholder briefings and support
A considerable amount of support has been provided in the form of advice and briefings to
support the Keogh and post-Keogh interest in the acute trust. Close liaison with the acute
trust communications team has ensured that the CCG has been fully informed and involved
in the Trust’s media and stakeholder communication. A Pennine Lancashire Communication
group was established to ensure consistency and coherence of communication across the
health economy. This has proved useful in planning for winter messages and anticipated
pressures in urgent care.
Media coverage
Positive
Neutral
Negative

Media briefings and/or statements have been prepared and distributed in relation to several
major issues in addition to queries around ELHT, including CQC involvement in
Calderstones, reactions to national announcements and other areas.
Weekly reporting and Horizon Scanning
The CSU communication and engagement team have provided the CCG with a weekly
‘reputation and relationship’ tracker which provides data and regular analysis of
communication and engagement metrics. This also provides the CCG with a high level
analysis of ‘hot issues’, and an update of work that the communication and engagement
team have undertaken for the CCG in the last week, with plans for the following week. In
addition to this, the communication and engagement team provide the core team with a
weekly horizon scanning document which brings together important policy, guidance, news
and information.
Web and social media
The communication and engagement team built and content managed the website for the
new CCG. Over the last six months the website has been reviewed, given a refresh and
updated. The newly revised content can be viewed here:
http://www.eastlancsccg.nhs.uk/ The website includes a carousel of prominent news features,
and contacts for all GP practices. It also includes an updated news section. Twitter is
integrated with the website.
Since the website was launched in April 2013, it has attracted 15,074 visitors, including
9,340 unique visitors. There have been almost 60,000 page views (59,786) and the average
number of pages viewed by each visitor was just under 4 (3.97).
The top 5 website pages viewed are (1) Who we are (2) Contact us (3) Key documents (4)
Governing body: member profiles; and (5) What we do.
The CCG Twitter account is integrated with the CCG website. The CCG has 1028 followers
– a significant and growing following. We have tweeted more than 300 health and related
messages. There were 185 retweets – where Twitter messages are sent to others with
similar or larger followings, and the CCG was mentioned in the tweets of 198 other Twitter
followers. This reflects a growing penetration of the Twitter ‘sphere’ enabling the CCG to
bypass traditional media and convey its messages to residents and stakeholders in a more
direct way.
The communication and engagement team have tweeted about a wide range of topics,
including amplification of national campaigns (such as dementia awareness week, world
diabetes week and self-care week), and more localised tweets (such as promoting local
Think! messages and demand management and supporting local authority public health
initiatives). There has been a significant increase in localised tweets towards the end of the
year, with the support of the CSU digital team.
Approval of the social media policy (to be discussed, January 2014) will enable the CCG to
further develop its social media presence, including on Facebook.
Campaigns and marketing
Think!
The “Think!” campaign was developed using patient engagement for use in urgent care
demand management and successfully launched in September 2013. The aim of this
ongoing campaign is to encourage residents, patients and public to think about how they
access health care. It includes a focus on minor illnesses and self-care and a range of
channels to deliver messages about how, where and when to access appropriate care.
The campaign was developed using focus groups and insight from the experiences of
patients, and was created in partnership with both Pennine Lancashire CCGs and East
Lancashire Hospitals NHS Trust. Materials included posters, leaflets and banners.
Feedback from the public has been positive, particularly in relation to the newsletter which
gave details of health care access points and the distribution of forehead thermometers
designed to be used for children. It is clear, however, that communications to support
demand management needs to be developed into a year-round campaign which can be
delivered on an ongoing basis.
Minor illnesses
In line with the Think! campaign, a series of 10 leaflets, plus posters and other materials
were developed aimed at directing patients to self-care and pharmacies where they were
suffering from routine minor illnesses. Patient information was designed to be handed out by
GPs and practice staff in preference to a prescription. The material was also distributed to
pharmacies. In East Lancashire, this will be further developed to cover the Minor Ailments
Scheme in due course.
Team Winter
Building on the Think! campaign, a Team Winter campaign was developed to reinforce and
make seasonal demand management and urgent care messages. The campaign was
launched in December and included radio advertisements across the Pennine Lancashire
area, including 2BR, print media advertisements, posters and a proactive schedule of media
releases on key healthcare topics.
The daily teleconference on winter pressures is supported by the CSU, as is out of hours
communications cover to deal with urgent issues as winter pressures increase.
Design and marketing support
Connect Campaign – Branding/Poster/Advert/Postcard/Banner
Think! campaign materials for launch, including thermometers, newsletters and other materials
Team Winter Campaign – Logo/Newspaper adverts/Web banners/Posters/Leaflets
Minor illness – 10 leaflets plus posters and other materials.
Patient Guide to Urgent Care Leaflet
CCG Corporate Briefing – Issue 1-3
Your Views Poster
Improving Health Flyer
Patient Pro Forma
In addition the design team have carried out and integrated design work into the CCG
website to support its development as a user friendly site.
Freedom of Information (FOI)
It has been an exceptionally busy period for Freedom of Information requests. From April to
December 2013 the CCG received 132 FOI requests.
All information that was requested was provided in 103 (83%) of cases. Where information
was not provided (19 cases, 14%), it was because the CCG did not hold this information.
In all, 114 (86%) of FOIs were responded to within the timeframe. In 15 (11%) cases, a
response was not made within the time frame, but a mutually acceptable time-frame was
negotiated with the requestor. No FOIs were escalated to the Information Commissioner in
this period.
The majority of the FOIs related to queries about the CCG, services that it commissions and
expenditure (see below). The remaining cases (4) remain open.
Complaints, concerns, compliments and comments
Since April, there have been 51 formal complaints, of which,11 are ongoing and open at the
present time. There have been two breaches against the statutory time frame in the
management of the formal complaints over this time period.
The majority of these complaints have been about NHS continuing and funded healthcare
(18, 35%).
Where the complaints relate to services provided by organisations other than the CSU, e.g.
Acute Trusts, GPs, the complainant’s/patient’s consent is obtained to forward the complaint
to the responsible service provider for investigation and response.
We received 132 concerns/enquiries Five of these are currently open and ongoing.
Again, where the concerns relate to services provided by organisations other than the CSU,
they are forwarded to the relevant organisation for attention. The remainder of the
concerns/enquiries have been dealt with satisfactorily.
We received six compliments during this period.
The compliments were shared with the relevant teams, and where possible the an
acknowledgement and thank you sent to the sender.
Engagement, Insight and Market Research
There has been a broad range of engagement support provided by the CSU to the CCG
during 2013.
The Head of Locality and communication and engagement team have supported a number
of engagement events and used the opportunity to gain insights and feedback from the
public and other stakeholders, including councils and the voluntary sector. Appendix 1,
Table 1, below evidences the engagement activities undertaken from April to December
2014.
The focus of engagement has been around four key areas as guided by the CCG: (1) urgent
care (2) appropriate use of service (3) Specific service reviews, such as Rossendale MIU
and Accrington walk-in centre and (4) Feedback on services and service quality in the
‘Connect’ listening events.
1
Agenda Item No: 5.5
REPORT TO:
NHS EL CCG Governing Body
MEETING DATE:
27 January 2014
REPORT TITLE:
Equality & Inclusion Annual Report
SUMMARY:
This is the first Equality & Inclusion Annual Report for EL CCG setting out how the organisation is meeting its commitment to taking equality, diversity and human rights into account when commissioning services, employing people, developing policies and communicating with or engaging local people in its work.
REPORT CATEGORY: Formally Receipt
Tick
√
Action the recommendations outlined in the report.
Debate the content of the report
Receive the report for information
AUTHOR:
Jules Wall Head of Equality & Inclusion, LCSU
PRESENTED BY:
Angela Brown Head of Corporate Affairs
COMMITTEES/ GROUPS CONSULTED:
Which Strategic Objective does the report relate to
Tick
1 Commission the right services for patients to be seen at the right time, in the right place, by the right professional.
2 Optimise appropriate use of resources and remove inefficiencies. √
3 Improve access, quality and choice of service provision within Primary Care √
4 Work with colleagues from Secondary Care and Local Authorities to develop seamless care pathways
2
Agenda Item No: 5.5
NHS East Lancashire CCG GOVERNING BODY
27 January 2014
Equality & Inclusion Annual Report
1. Introduction This is East Lancs CCG first Equality and Inclusion Annual Report. This report sets out how the CCG has been demonstrating its due regard to meeting the aims of the Public Sector Equality Duty. 2. Background
The report contains a summary of the activities and progress which have evidenced the CCGs endeavour to meet its statutory duty of compliance with the requirements set out in the Equality Act (2010), namely
eliminate discrimination, harassment, victimisation and other unlawful acts
advance equality of opportunity between people who share a protected characteristic and those who don’t share it
foster good relations between people who share a protected characteristic and those who don’t share it
Page 13 of the report contains a summary of the recent ‘grading’ event, where the CCG invited a diverse range of members of the public to review evidence of its working practices, decisions, and commissioning intentions, against a range of measures to provide a baseline of our progress. Our intention during 2014 is to build on those areas highlighted within the grading summary as ‘developing’ and members will be informed of progress at regular intervals. Our staff have received additional specialised training in addition to the mandatory training requirements, to ensure that they are best placed to embed the requirements of the Equality agenda into all that they do. Governing Body members will recall a development session held in December 2013 which provided an overview of the Equality and Inclusion agenda in addition to highlighting Corporate responsibilities of the GB. 3. Recommendation
The GB are requested to formally receive the Equality and Inclusion Annual Report ANGELA BROWN Head of Corporate Affairs
Led by clinicians, accountable to local people
East Lancashire Clinical Commissioning Group: Equality & Inclusion Annual Report
2 | P a g e
East Lancashire Clinical Commissioning Group
Led by clinicians, accountable to local people
Foreword 3
Introduction and Aims of the Report 4
Commissioning Intentions 4
Our Population 5
Compliance with the Public Sector Equality Duty 6
Meeting Statutory Human Rights Requirements 7
Meeting our Equality Pledges 8
Outcomes of our Equality Objectives 10
Engagement with Local People 10
Monitoring NHS Healthcare Providers 11
The Way Forward 13
Conclusions 15
Equality Objectives Action Plan Progress Report 16
Share Your Views 21
Contact Our Customer Care Team 22

3 | P a g e
East Lancashire Clinical Commissioning Group
Led by clinicians, accountable to local people
Foreword We are pleased to present our first Equality and Inclusion Annual Report for East Lancashire
Clinical Commissioning Group. This document sets out how the CCG is meeting our
commitment to taking equality, diversity and human rights into account in everything we do
whether that’s commissioning services, employing people, developing policies,
communicating with or engaging local people in our work.
The Clinical Commissioning Group has a designated Board level lead that is responsible for
ensuring the Governing Body consider Equality, Diversity and Human Rights. The Board
level lead is supported by an external source providing high level experience, knowledge
and skills on a shared basis with other local Clinical Commissioning Groups.
The people in our community are the experts of their own conditions, their personal
characteristics or the needs of the people they care for. Empowering patients and the public
to become our partners within the new landscape as we move forward will ensure a world
class service for all.
The CCG will also involve local people in the continuing development and monitoring of this
strategy to ensure that we buy the right health care services, reduce health inequalities and
provide well trained staff to deliver services and ensure our providers meet the equality
duties set out in the Equality Act 2010 and promote people’s rights.
Dr Mike Ions Dr Di Van Ruitenbeek
Accountable Officer CCG Chair
The CCG is committed to putting the patient at the heart of
what we do; through effective engagement and
involvement of local people in decision making, buying
healthcare to meet the identified needs of the population of
East Lancashire, improving health outcomes and eliminating
health inequalities
4 | P a g e
East Lancashire Clinical Commissioning Group
Led by clinicians, accountable to local people
Introduction and Aims of the Report
This is the Clinical Commissioning Groups (CCG) first annual Equality & Inclusion Report.
The report will set out how the CCG has been demonstrating ‘due regard’ to the Public
Sector Equality Duty’s three aims and will provide evidence
for meeting the specific equality duty, which requires all
public sector organisations to publish their equality
information annually.
This means that the CCG has given detailed consideration to
issues of equality and discrimination before making any
policy decision. That is an essential requirement that is seen
as an integral and important part of the mechanisms for ensuring the fulfilment of the aims of
anti-discrimination legislation set out in the Equality Act 2010 and the Human Rights Act
1998.
Commissioning Intentions
The Clinical Commissioning Group (CCG) buys a range of health care to meet the needs of
the people of East Lancashire. The CCG develops plans every year setting out what it will
buy these are called the Commissioning Intentions.
Commissioning Intentions form part of the annual planning cycle which commences
development in the summer and finishes with agreed and signed contracts with providers by
the 31st March of the following year. The major part of the planning cycle is the development
of an integrated plan which responds to the requirements of the NHS Operating Framework
which is published each year.
The CCG considers equality information, including health data provided by Public Health,
England on health inequalities when developing its commissioning plans, undertaking
service design and redesign, equality analysis and strategic developments. Equality
analyses are being carried out as part of the development of the 2014/15 Commissioning
Intentions to ensure that equality is at the heart of the process.
“We will make equality core
to our business
planning”
5 | P a g e
East Lancashire Clinical Commissioning Group
Led by clinicians, accountable to local people
Our Population
East Lancashire CCG comprises the five boroughs of Burnley, Hyndburn, Pendle, the Ribble
Valley (excluding Longridge), and Rossendale.
The population the CCG serves is estimated at 371,443 people from diverse backgrounds.
The population is an ageing population in the sense that the numbers of people over 75
years has increased and is projected to continue to do so. At the same time, the numbers of
children and young people in the population is higher than average, this means that the CCG
will need to consider both ends of the age spectrum, when buying health services. The
south Asian ethnic community makes up over 11% of the registered population and has a
much younger age structure than the white British community.
Health status
Life expectancy in East Lancashire has improved,
but there are wide health inequalities within our
CCG area, and between the East Lancashire region
and the national figure. These inequalities are a
result of relatively high early death rates from the
“big killers”, CVD, cancers and respiratory disease,
but also by a small number of deaths occurring at a
markedly young age e.g. accidents, chronic liver
disease, suicides and infant deaths. Early deaths
from cancer, in particular, make an important
contribution to overall early death rates, and there
is evidence that the local premature cancer death rate has increased over recent years.
Our ‘Strategic Plan 2013 – 2018’ sets out our assessment of where we are now
based on what we know about our local population, we firmly believe that the ‘NHS
belongs to the people’ and in partnership with you we will focus on equality,
integration, compassion and care, genuine patient engagement and tackling health
inequalities across East Lancashire.
‘Improving the
health and wellbeing
outcomes for
patients and the
local population shall
be our central goal.
6 | P a g e
East Lancashire Clinical Commissioning Group
Led by clinicians, accountable to local people
Compliance with the Public Sector Equality Duty
The CCG has worked to show due regard to the aims of the Public Sector General Equality
Duty as set out in the Equality Act as set out below:
Aim 1 Eliminate unlawful discrimination, harassment and victimisation
Aim 2 Advance equality of opportunity between different groups
Aim 3 Foster good relations between different groups
This means that the CCG must work to prevent discrimination, harassment and victimisation
from happening in the first place, take steps to meet the health needs of people with certain
protected characteristics as set out in the Equality Act 2010 e.g. age, disability, gender
reassignment, religion and belief, sexual orientation, sex, race, pregnancy and maternity,
marriage and civil partnership, where these differ from the needs of the wider population and
encourage people with certain protected characteristics to participate in public life or
decisions making where their participation is disproportionately low.
The CCG has adopted the NHS Equality Delivery System (EDS) as its performance
management tool which allows the CCG to demonstrate to local people how the CCG is
meeting the three aims of the Equality Duty
by ensuring that employees consider
equality and human rights when
undertaking their work.
The EDS grading against the 4 EDS goals
provides the Clinical Commissioning Group
Governing Body with an assurance
mechanism for compliance with the
Equality Act 2010 and enables local people
to co-design the Clinical Commissioning
Groups equality objectives to ensure improvements in the experiences of patients, carers,
employees and local people.
During October 2012 whilst in shadow form, the CCG undertook a self-assessment against
the 4 goals and 16 outcomes. Over the past twelve months the CCG has produced further
evidence for a self-assessment which was graded by local people and employees in October
2013. Grading will take place annually to ensure progress against our objectives and aims.
The four EDS goals are:
1. Better health outcomes for all
2. Improved patient access and experience
3. Empowered, engaged and included staff
4. Inclusive leadership at all levels
The grades for EDS are as follows:
Undeveloped – Red
Developing – Amber
Achieving – Green
Excelling – Purple
7 | P a g e
East Lancashire Clinical Commissioning Group
Led by clinicians, accountable to local people
The CCG has adopted the Pre-PEAR Toolkit which provides a framework for undertaking
equality analysis; privacy impact assessments and human rights screening which enables
the CCG the show due regards to the three aims of the general equality duty.
Commissioning staff are currently developing their commissioning intentions and are
undertaking engagement and equality analysis and human rights screening as part of the
development process.
Meeting Statutory Human Rights Requirements
The Human Rights Act 1998 sets out a range of rights which have implications for the way
the CCG buys services and manages our workforce. In practice this means that we must:
Act compatibly with the rights contained in
the Human Rights Act in everything we do
Recognise that anyone who is a ‘victim’
under the Human Rights Act can bring a
claim against the CCG (in a UK court,
tribunal, hearing or complaints procedure)
Wherever possible existing laws, guidance
and directives that the CCG as a public
body deals with, must be interpreted and
applied in a way that fits with the rights in the Human Rights Act 1998.
The CCG is committed to promoting and protecting the rights of people living in East
Lancashire when undertaking decision making. In 2013 the CCG carried out human rights
screening as part of the planning process for the development of its annual commissioning
intentions and has undertaken screening on its decision making, including commissioning
and decommissioning and service redesign programmes.
The CCG is supported by the Equality & Inclusion Team at the Commissioning Support Unit
(CSU) who provide specialist support to CCG staff undertaking human rights screening.
Staff from the CCG have also attended training provided by the Equality & Inclusion Team
during 2013, to ensure that they understand their roles in promoting and protecting people’s
human rights and are able to effectively undertake human rights screening.
The NHS is founded on a
common set of principles and
values that bind together the
communities and
people it serves

8 | P a g e
East Lancashire Clinical Commissioning Group
Led by clinicians, accountable to local people
Meeting our Equality Pledges
Pledge 1 Ensure we talk to local people across East Lancashire from a range of
protected groups, to involve them as much as possible in our decision making
processes.
Progress in 2013
The CCG has held several listening events throughout the year offering
patients and their families, cares and members of the public the opportunity to
share their experiences of NHS services locally and to influence service
development.
One example was the Rossendale Locality Listening Event which was
attended by local people who were asked to give their views across three main
themes which were identified with the objective of patients giving their
comments in relation to services at either a Rossendale locality, East
Lancashire or wider perspective and were as follows:-
a) What do you think is good / working well
b) What areas of improvement are there
c) What do you think works less well / needs improving
The above three themes were subdivided into further sections with the
opportunity to express comments across any of the following:-
a) GP Services
b) Dental, Optical or Pharmacy
c) Burnley Hospital
d) Blackburn Hospital
e) Community Services
f) Mental Health
Local people were also involved in grading the CCG against the NHS Equality
Delivery System in October 2013.
Pledge 2 Ensure that all policies and processes carried out by the CCG or on behalf of
the CCG are based on a robust review of equality information and are based
on the needs of the all the people we serve.
Progress in 2013
The CCG utilises a range of information including the Joint Strategic Needs
Assessment (JSNA) and public health profiles amongst a few. The CCG has
also adopted the Pre-PEAR Toolkit which provides a framework to support the
CCG in undertaking equality analysis and human rights screening of all
decisions including what health care to buy or not to buy (Commissioning
Intentions). CCG staff have used the toolkit to undertake equality analysis on
a number of work programmes during 2013 e.g. Chronic Pain Management
service redesign & Respiratory Service Redesign.
9 | P a g e
East Lancashire Clinical Commissioning Group
Led by clinicians, accountable to local people
Pledge 3 Ensure all staff including Governing Body members undertake equality,
diversity and human rights training & development at a level related to their
role.
Progress In 2013
Equality training is provided for all staff of the CCG, this is provided in a range
of ways to ensure all staff receive the training they require e.g. mandatory
equality training utilising the Skills for Health e-learning modules;
Overview
This course provides the broad
based-knowledge of Equality &
Diversity needed by all staff working
in the health sector today.
It is made up two sections with 8
modules in total including:
Module 1: General awareness
Module 2: Age
Module 3: Disability
Module 4: Gender and gender
reassignment
Module 5: Race & ethnicity
Module 6: Religion & belief
Module 7: Sexual orientation
Module 8: Pregnancy and maternity.
Assessment
Each module is followed by an
assessment with a pass mark of
70%. Progress can be tracked by
managers for internal audits and
learners can keep a certificate of
completion for CPD.
Accreditations & Endorsements
The course was initially developed
by the e-learning development team
in Liverpool Community Health
Trust, commissioned by NHS North
West. The material in the course
has since been revised for national
use with the support of Skills for
Health and E-Learning for Health.
Duration: 2 hours 30 minutes
approx. Board training took place in
December 2013 and additional
enhance training for managers.
Pledge 4 Use the NHS Equality Delivery System (EDS) to inform local people of how
the CCG is performing and ensure that any health care providers
commissioned by the CCG are also using EDS.
Progress in 2013
The CCG uses the published EDS outcomes to monitor its performance and
outcomes of both the CCGs processes and that of their providers. An annual
review by patients and public/residents is carried out every October the results
of the 2013 grading can be found on page 14.
10 | P a g e
East Lancashire Clinical Commissioning Group
Led by clinicians, accountable to local people
Outcomes of our Equality Objectives
East Lancashire Clinical Commissioning Group prepared and published its equality
objectives in October 2012 whilst in shadow form. These objectives further the aims of the
general equality duty, and will be refreshed annually following the grading of the CCG
against the four goals of the Equality Delivery System and revised every four years. (See
the action plan on page 16 for the annual progress report).
Engagement with Local People
The CCG wants to actively involve local people in decision making to support this across the
organisation it has put in place a Communication and Engagement Strategy which will work
in partnership with the Equality Strategy. The CCG will also engagement with local people
and staff when undertaking its annual review of performance and outcome delivery against
the four goals of the Equality Delivery System, this engagement will inform the CCG on its
performance and will form part of the annual reporting mechanisms.
The CCG is also embedding engagement and
involvement in to its commissioning processes
through its ‘Listening Events’ e.g. the Rossendale
Locality Listening Event which was attended by
local people who were asked to give their views
across three main themes which were identified
with the objective of patients giving their comments
in relation to services at either a Rossendale
locality, East Lancashire or wider perspective and
were as follows:-
a) What do you think is good / working well
b) What areas of improvement are there
c) What do you think works less well / needs improving
The CCG firmly believes that
the ‘NHS belongs to the
people’ and in partnership
with you we will focus on
equality, integration,
compassion and care, genuine
patient engagement and
tackling health inequalities
across East Lancashire.
11 | P a g e
East Lancashire Clinical Commissioning Group
Led by clinicians, accountable to local people
Monitoring our NHS Healthcare Providers
The CCG through its contracts with providers ensures that those providers’ organisations are
compliant with Equality legislation. All the NHS providers which the CCG contracts with
undertake the annual equality performance review using the NHS Equality Delivery System
(EDS).
NHS Provider Equality
Objectives
Published
Equality
Information in
2013
Undertaken EDS
Grading 2013/14
East Lancashire
Hospital Trust
Lancashire Care
Foundation Trust
Calderstones
Partnership NHS
Foundation Trust
Due early 2014
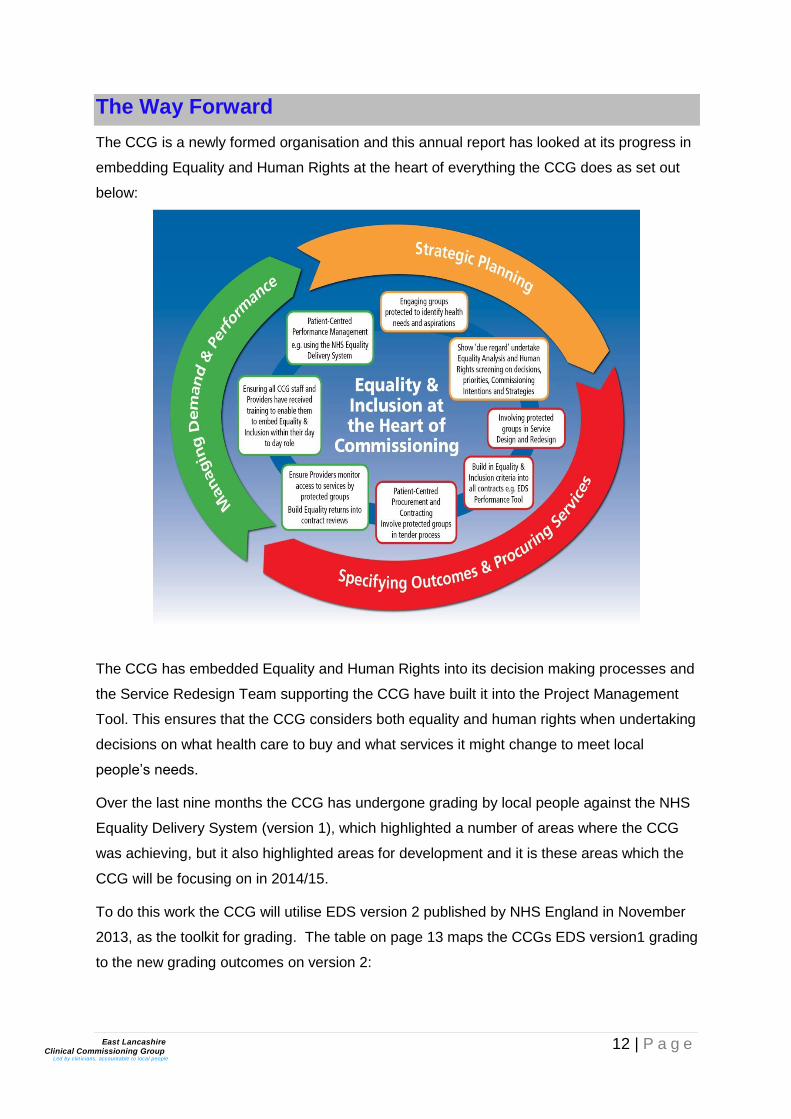
12 | P a g e
East Lancashire Clinical Commissioning Group
Led by clinicians, accountable to local people
The Way Forward
The CCG is a newly formed organisation and this annual report has looked at its progress in
embedding Equality and Human Rights at the heart of everything the CCG does as set out
below:
The CCG has embedded Equality and Human Rights into its decision making processes and
the Service Redesign Team supporting the CCG have built it into the Project Management
Tool. This ensures that the CCG considers both equality and human rights when undertaking
decisions on what health care to buy and what services it might change to meet local
people’s needs.
Over the last nine months the CCG has undergone grading by local people against the NHS
Equality Delivery System (version 1), which highlighted a number of areas where the CCG
was achieving, but it also highlighted areas for development and it is these areas which the
CCG will be focusing on in 2014/15.
To do this work the CCG will utilise EDS version 2 published by NHS England in November
2013, as the toolkit for grading. The table on page 13 maps the CCGs EDS version1 grading
to the new grading outcomes on version 2:
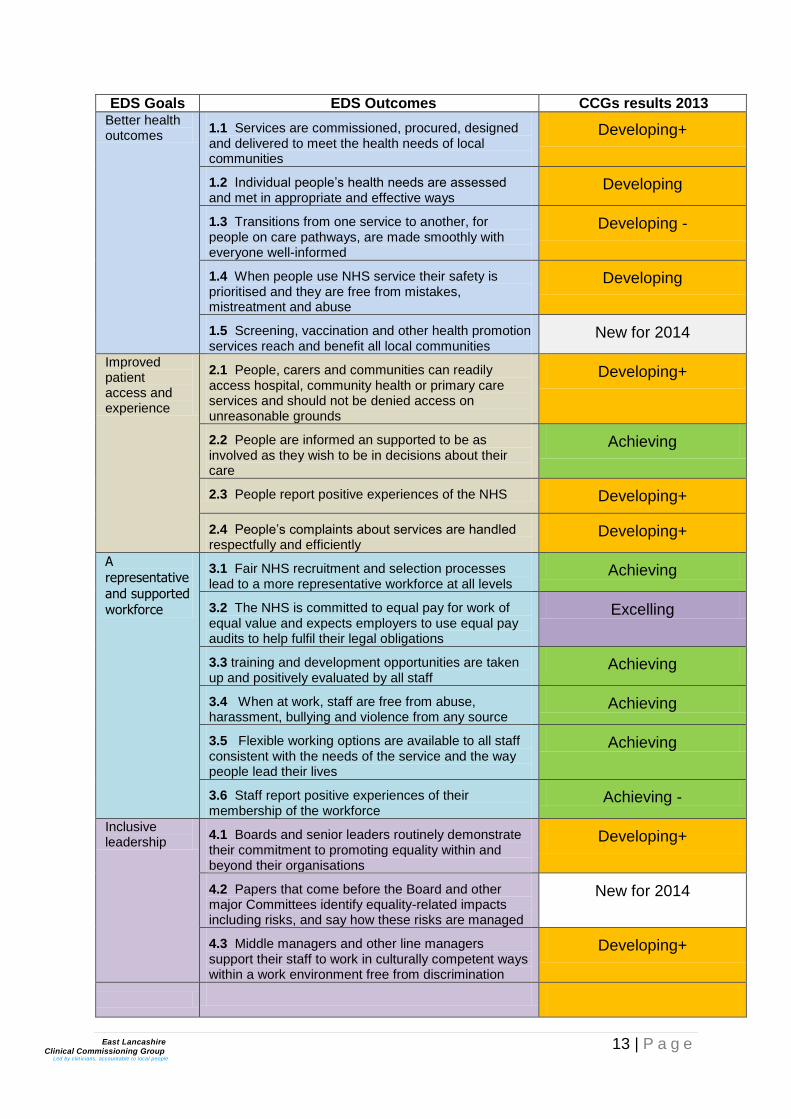
13 | P a g e
East Lancashire Clinical Commissioning Group
Led by clinicians, accountable to local people
EDS Goals EDS Outcomes CCGs results 2013 Better health outcomes
1.1 Services are commissioned, procured, designed and delivered to meet the health needs of local communities
Developing+
1.2 Individual people’s health needs are assessed and met in appropriate and effective ways
Developing
1.3 Transitions from one service to another, for people on care pathways, are made smoothly with everyone well-informed
Developing -
1.4 When people use NHS service their safety is prioritised and they are free from mistakes, mistreatment and abuse
Developing
1.5 Screening, vaccination and other health promotion services reach and benefit all local communities
New for 2014
Improved patient access and experience
2.1 People, carers and communities can readily access hospital, community health or primary care services and should not be denied access on unreasonable grounds
Developing+
2.2 People are informed an supported to be as involved as they wish to be in decisions about their care
Achieving
2.3 People report positive experiences of the NHS Developing+
2.4 People’s complaints about services are handled respectfully and efficiently
Developing+
A
representative
and supported workforce
3.1 Fair NHS recruitment and selection processes lead to a more representative workforce at all levels
Achieving
3.2 The NHS is committed to equal pay for work of equal value and expects employers to use equal pay audits to help fulfil their legal obligations
Excelling
3.3 training and development opportunities are taken up and positively evaluated by all staff
Achieving
3.4 When at work, staff are free from abuse, harassment, bullying and violence from any source
Achieving
3.5 Flexible working options are available to all staff consistent with the needs of the service and the way people lead their lives
Achieving
3.6 Staff report positive experiences of their membership of the workforce
Achieving -
Inclusive leadership
4.1 Boards and senior leaders routinely demonstrate their commitment to promoting equality within and beyond their organisations
Developing+
4.2 Papers that come before the Board and other major Committees identify equality-related impacts including risks, and say how these risks are managed
New for 2014
4.3 Middle managers and other line managers support their staff to work in culturally competent ways within a work environment free from discrimination
Developing+

14 | P a g e
East Lancashire Clinical Commissioning Group
Led by clinicians, accountable to local people
Conclusion
The CCG was established as a statutory body on the 1st of April 2013 as set out in the
Health and Social Care Act 2012, this meant that the CCG is responsible for showing ‘due
regard’ to the Public Sector Equality Duty as set out in section 149 of the Equality Act 2010.
Prior to 1st April 2013 the CCG had been in shadow form and during the shadow period,
set out its vision around Equality & Inclusion in its Equality, Diversity and Human Rights
Strategy, which was refreshed following the EDS grading outcomes of 2013.
The CCG undertook a self-assessment against the 4 goals of the Equality Delivery System
in October 2012. At the time the CCG graded itself as ‘Developing’ against 16 outcomes
considered across the four goals.
The grading was then redone in October 2013 and this was carried out by local people and
employees (the panel) of the CCG on evidence gathered in the 12months since the self-
assessment. This grading confirmed that 9 of the 16 outcomes graded as ‘Developing’ at
self-assessment were still at ‘Developing’ although there was a consensus across the
graders that they could see progress in all 9 areas. 6 of the outcomes that were ‘Developing’
at self-assessment were graded by the panel at ‘Achieving’ and one outcome went from
‘Developing’ to ‘Excelling’.
The CCG’s Senior Management Team and Governing Body are encouraged by this positive
outcome from the first grading by the panel and are committed to continuous development
against all 4 goals.
There were some developmental areas for the CCG in relation to the grading, as this was
the first time that employees and local people had been involved in this type of assessment
and there are plans in place to ensure that the evidence collection and grading are much
smoother in 2014.
Author: Jules Wall Role: Head of Equality & Inclusion NHS Staffordshire and Lancashire
Commissioning Support Unit
Date: December 2013
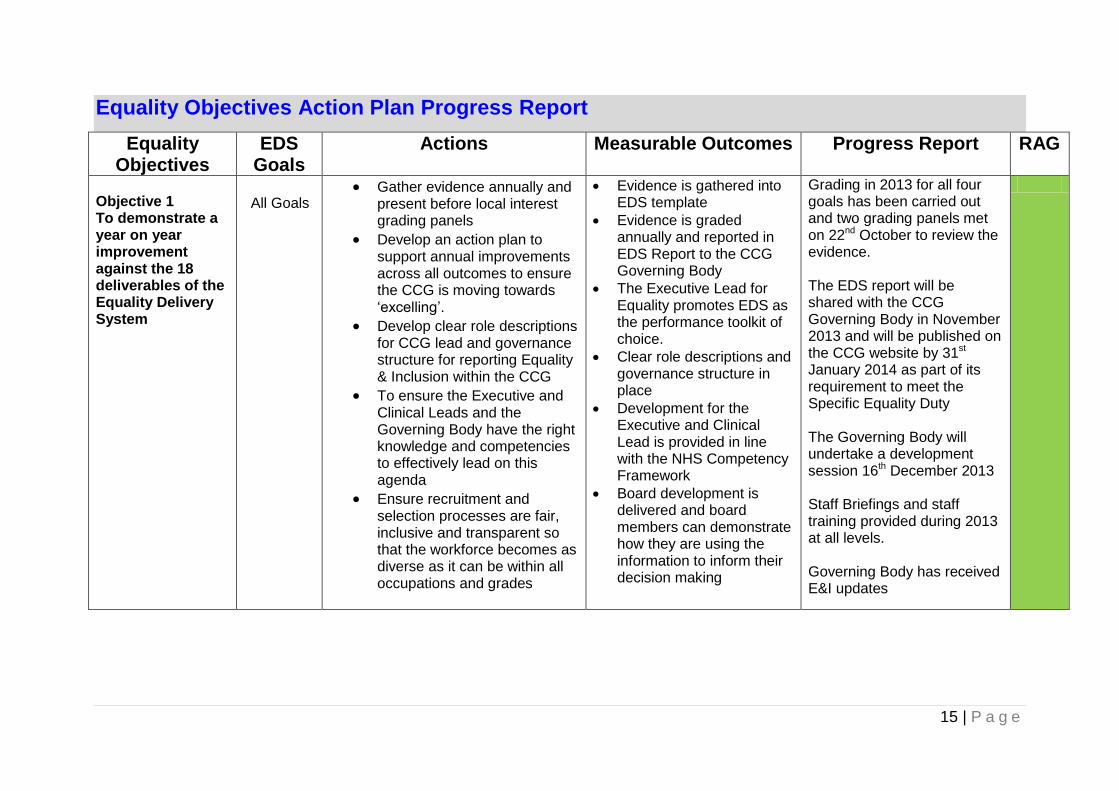
15 | P a g e
Equality Objectives Action Plan Progress Report
Equality Objectives
EDS Goals
Actions Measurable Outcomes Progress Report RAG
Objective 1 To demonstrate a year on year improvement against the 18 deliverables of the Equality Delivery System
All Goals
Gather evidence annually and present before local interest grading panels
Develop an action plan to support annual improvements across all outcomes to ensure the CCG is moving towards ‘excelling’.
Develop clear role descriptions for CCG lead and governance structure for reporting Equality & Inclusion within the CCG
To ensure the Executive and Clinical Leads and the Governing Body have the right knowledge and competencies to effectively lead on this agenda
Ensure recruitment and selection processes are fair, inclusive and transparent so that the workforce becomes as diverse as it can be within all occupations and grades
Evidence is gathered into EDS template
Evidence is graded annually and reported in EDS Report to the CCG Governing Body
The Executive Lead for Equality promotes EDS as the performance toolkit of choice.
Clear role descriptions and governance structure in place
Development for the Executive and Clinical Lead is provided in line with the NHS Competency Framework
Board development is delivered and board members can demonstrate how they are using the information to inform their decision making
Grading in 2013 for all four goals has been carried out and two grading panels met on 22nd October to review the evidence. The EDS report will be shared with the CCG Governing Body in November 2013 and will be published on the CCG website by 31st January 2014 as part of its requirement to meet the Specific Equality Duty The Governing Body will undertake a development session 16th December 2013 Staff Briefings and staff training provided during 2013 at all levels. Governing Body has received E&I updates
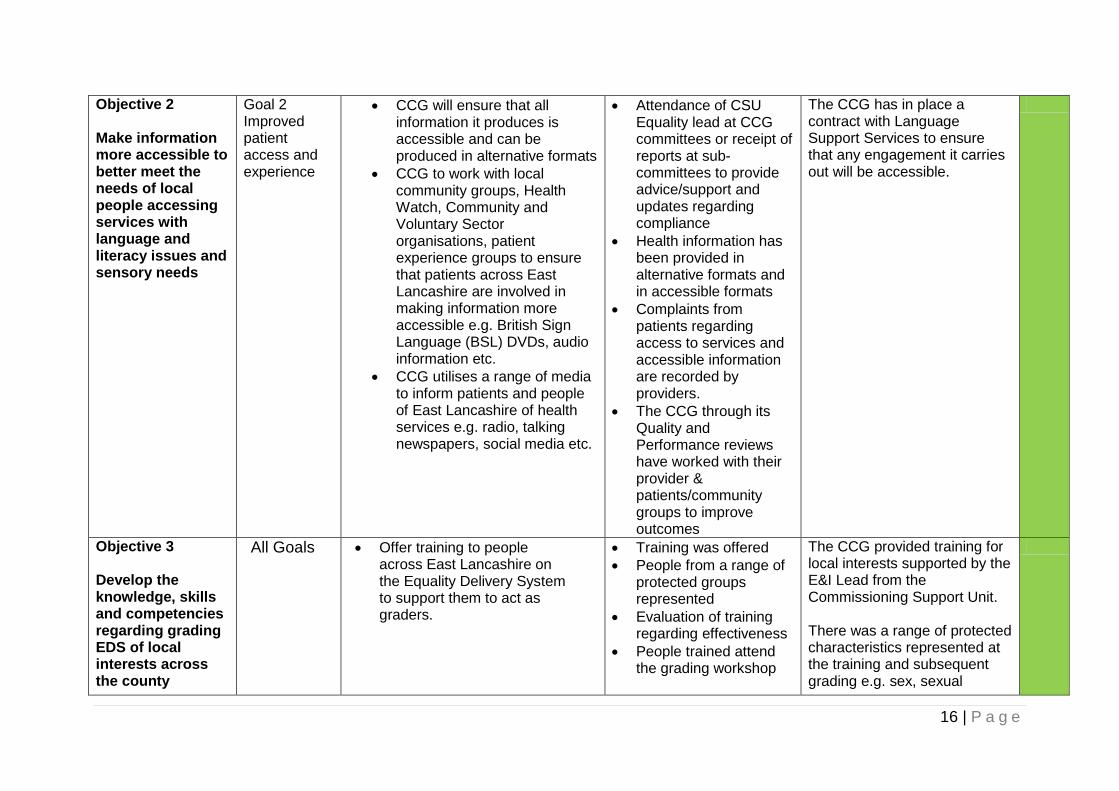
16 | P a g e
Objective 2 Make information more accessible to better meet the needs of local people accessing services with language and literacy issues and sensory needs
Goal 2 Improved patient access and experience
CCG will ensure that all information it produces is accessible and can be produced in alternative formats
CCG to work with local community groups, Health Watch, Community and Voluntary Sector organisations, patient experience groups to ensure that patients across East Lancashire are involved in making information more accessible e.g. British Sign Language (BSL) DVDs, audio information etc.
CCG utilises a range of media to inform patients and people of East Lancashire of health services e.g. radio, talking newspapers, social media etc.
Attendance of CSU Equality lead at CCG committees or receipt of reports at sub-committees to provide advice/support and updates regarding compliance
Health information has been provided in alternative formats and in accessible formats
Complaints from patients regarding access to services and accessible information are recorded by providers.
The CCG through its Quality and Performance reviews have worked with their provider & patients/community groups to improve outcomes
The CCG has in place a contract with Language Support Services to ensure that any engagement it carries out will be accessible.
Objective 3 Develop the knowledge, skills and competencies regarding grading EDS of local interests across the county
All Goals
Offer training to people across East Lancashire on the Equality Delivery System to support them to act as graders.
Training was offered
People from a range of protected groups represented
Evaluation of training regarding effectiveness
People trained attend the grading workshop
The CCG provided training for local interests supported by the E&I Lead from the Commissioning Support Unit. There was a range of protected characteristics represented at the training and subsequent grading e.g. sex, sexual

17 | P a g e
orientation, religion and belief, race, disability, gender reassignment, age
18 | P a g e
Objective 4 To ensure the Executive and Clinical Leads and the Board have the right knowledge and competencies to effectively lead on this agenda
Goal 4 & Goal 3
Identify an executive lead/senior manager within the CCG for Equality and Inclusion
Identify a clinical lead for Equality & Inclusion within the CCG Governing Body
E&I is embedded into Governing Body agenda as a standing item.
All papers requiring a decision must have an equality analysis and Governing Body members are developed to understand their roles and responsibilities.
Executive and Clinical Lead is identified
Equality & Inclusion is a standard agenda item at CCG board meetings
The CCG Governing Body receive assurances that the CCG and the CSU are compliant with all equality legislation
Employees at all levels including the Governing Body receive Equality & Inclusion development appropriate to their role.
The Governing Body and Senior Management promote Equality & Inclusion as a positive cultural requirement of the CCG
The CCG has identified the Executive, Senior Management and Clinical Lead for Equality. The CCGs Chair actively supports Equality & Inclusion within her role. The Senior Manager Lead meets regularly with the E&I Strategic Lead who supports the CCG, and promotes Equality & Inclusion at all levels within the organisation. The Senior Manager, Clinical Lead and Chair recently supported the EDS Training of graders and the actual grading of the CCGs evidence showing clear senior management promotion of Equality & Inclusion within the CCG. The CCG has supported staff to attend equality analysis training and scored ‘achieving’ and ‘excelling’ across outcomes in goals 3 & 4 of the Equality Delivery System
19 | P a g e
Objective 5 We will improve access to all health care services for the most vulnerable groups and we will support carers and family members.
Goal 1 Better health outcomes for all Goal 2 Improved patient access and experience
Utilise principles of proportionate universalism when developing contracts and service specifications to ensure proactive engagement of members of the population who experience the worst health outcomes, based on health profiles for the CCG footprint.
Ensure commissioning and contracting staff are trained in mandatory equality and diversity awareness (as part of organisational development programme and personal development process) and in Equality Analysis techniques
Routinely collect and publish data on CCG website regarding Equality information relating to the people who live in East Lancashire as they are the people affected by the CCG’s policies and practices when buying or not buying health and social care services.
Link the Equality function with the Governance, Safety and Quality functions within the CCG. (Commonalities include: Serious Untoward Incidents (SUIs), policies, safeguarding, risk management, equality
CCG commissions services to meet the health needs of local communities, promote well-being, and reduce health inequalities
Patients, carers and communities can readily access services, and should not be denied access on unreasonable grounds
Patients are informed and supported so that they can understand their diagnoses, consent to their treatments, and choose their places of treatment
Grading against goal 1 and 2 show improving outcomes year on year.
Patients’ health needs are assessed, and resulting services are provided, in appropriate and effective ways
The CCG in year 1 of undertaking grading against the four goals of the Equality Delivery System achieved a ‘developing’ grade for goals 1 & 2 with come outcomes gaining achieving – the CCG is committed to buying health care which is meeting the needs of local people and have undertaken a range of engagement activities and are carrying out Equality Analysis to ensure that services they buy are accessible and fit for purpose. In 2014 the CCG will be working on specific areas highlighted through the EDS grading to demonstrate the commitment to continuous improvement.
20 | P a g e
analysis, compliance, reporting)
21 | P a g e
East Lancashire Clinical Commissioning Group
Led by clinicians, accountable to local people
Share Your Views
Patient involvement is a top priority for all CCGs in order to effectively commission (buy) and
oversee local services that meet the needs of local people. We ensure we can listen to you
in order to reflect those needs in our commissioning activities through a variety of different
forums.
Healthwatch Lancashire
Healthwatch Lancashire is the local consumer champion for healthcare services. The branch
is one of 152 community-focussed organisations in the national Healthwatch network set up
in October 2012.
We are working alongside your Healthwatch representatives to further understand the needs
and opinions of local people.
You have the right to be involved in decisions about your health and social care services and
Healthwatch provides that opportunity. By sharing your experiences and ideas with
Healthwatch you can influence the way services are run.
Listening to our patients and public
Our CCG has a dedicated patient and public engagement lay member. They work in local
communities to explain the work of the CCG and open a two-way dialogue.
Patient participation groups
Another way we engage with local people is through patient participation groups.
These offer patients interested in health and healthcare the opportunity to get involved with
their local GP practice and support its work. Most groups also include members of practice
staff. They meet at regular intervals to decide the ways and means of adding value to the
services and facilities offered to patients.
22 | P a g e
East Lancashire Clinical Commissioning Group
Led by clinicians, accountable to local people
If you need this leaflet in another format or language, please contact the customer care team on freephone:
Freephone: 0800 032 2424 Telephone: 01772 777 952
Textphone: 01772 227 005
Email: [email protected]
Contact our Customer Care Team
Page 1 of 5 Approved by TW : 6.1.13
Audit Committee Minutes of the meeting held on
Monday, 9 December 2013, 12:30-13:30pm, at Walshaw House PRESENT: Tom Wolstencroft Lay Advisor – Governance – Chair Jackie Hanson Chief Nurse Dr Phil Huxley GP Clinical Lead - Pendle
Dr Murthy Motupalli GP Clinical Lead - Hyndburn - from 12:45pm Dr Steve Alcock Secondary Care Consultant In Attendance: Mark Youlton Chief Finance Officer
Simon Hardman Audit Manager, Grant Thornton Fiona Blatcher Associate Director, Grant Thornton Kirsty Hollis Deputy Chief Finance Officer David Swift Internal Audit Manager, ANW Lisa Warner Internal Audit
Anne Pietrzak Board Administration Manager - Minutes
Min No: ACTION
13.130 Welcome, Introductions & Chairs Update The Chair welcomed everyone to the meeting, particularly Lisa Warner, Internal Audit Manager, Audit NW and introductions were made. He also congratulated Anne Pietrzak on her achievement of working 35 years within NHS service and passed on the thanks from her colleagues for all her support, encouragement and hard work.
13.131 Apologies Apologies were received from Angela Brown and Lucille Hinnigan.
13.132 Governance Declarations of Interest - None received Quoracy – The meeting was quorate
13.133 Minutes of the meeting held on 11 November 2013 13.126 – Learning from Others : there was a request to amend the wording to read ….. the locality view was that on occasions the timing of the learning events impacted on access, due to the number of Practice closedowns. Subject to the above amendment, the minutes were approved as an accurate record.
13.134 Action Matrix The Action Matrix was presented and discussed: 13.114 - Half Year Financial Review : Allocations for the next two years were due 19 December 2013. Remove from the Matrix.
Page 2 of 5 Approved by TW : 6.1.13
13.121 - Patient Confidential Data :This was an ongoing issue, access was now being received to expedite the process and the position would be monitored. 13.127 - Public Involvement : Management of GP complaints to be raised with the Area Team.
JH
13.135 Quality & Safety Committee Minutes of 13 November 2013 Jackie Hanson, Chief Nurse and Chair of the QSC referred to discussions at the last meeting relating to the Slaidburn Practice and confirmed she had asked for this issue to be placed on the Risk Register. She presented the minutes of the QSC of 13 November and highlighted key points. Exception reports had been requested relating to Stroke performance and members debated whether actions taken had made a difference. Slight improvement was noted and details of further challenge had been requested regarding the robustness of the response. Concerns were expressed that CQUIN data submitted for Q1 from ELHT was two months late and Q2 data remained outstanding. This had now been actioned by ELHT and a productive meeting had taken place with the Trust when it was confirmed that the number was small in terms of those areas not being achieved. A robust discussion had taken place in respect of the financial impact of Keogh on ELHT and further discussion would take place at the next meeting. With reference to infection control, it was reported there were a number of pre and post 48 hour MRSA cases within the system which had affected the CCGs quality premium, together with an increase in CDI cases. It was considered there was a fragmented system regarding infection control, with lack of support in primary care and a specific specialist in the CCG. A Pennine Lancashire strategic meeting had been convened on 21 November to consider HCAI with collaboration to improve the system going forward. Quarterly meetings were planned and a workplan had been drafted providing reassurance that plans are now in place to support primary care. Serious Incident reporting had been an area of concern regarding robustness, however the CCG was now receiving weekly reporting from the CSU and Interim Support was in place to manage this. An Action Plan would be presented to the next QSC meeting. Reflecting on the first six months, Tom Wolstencroft considered the tone of discussions had moved towards engagement which provided reassurance that support systems are now in place and becoming embedded in the organisation. There was a need to consider quoracy of the QSC as this was a recurring issue together with timings for discussion. Members were reassured that an infection control strategy was in place and it was agreed that CDiff should be included on the risk register.
Page 3 of 5 Approved by TW : 6.1.13
13.136 Risk Management There were currently twenty one risks on the Risk Register and sixteen on the Board Assurance Framework. Four new risks had been added to the register in October and seven had closed during November, details of which were included in the report. In considering the report, Members felt the report did not highlight what is being done to mitigate the risks, requesting more detail in future reports to identify what action has been taken. It was also noted that a number of issues have not changed and remained a high risk, highlighting the need to know what the escalation process is to manage. It was agreed that high level risks would be considered at the QSC and referred to the Governing Body where necessary. ACTION:
Further discussion outside the meeting with the Head of Corporate Affairs to ensure more detail was included behind each risk outlining actions taken.
TW/AB
13.137 Internal Audit – Progress Report David Swift, Senior Internal Audit Manager reported on progress against the audit plan to mid November confirming that work was progressing well. Final reports had been completed in respect of Partnerships and Practice Development and both received a high assurance rating with good systems in place. In relation to Communications & Engagement, significant assurance was received with two medium rated recommendations relating to policies which required updating, noting these had now been addressed. Regarding the future arrangements of Audit NW, the Board had proposed that Mersey Internal Audit Agency will be the preferred supplier going forward. Lisa Warner would take on the role of Senior Internal Audit Manager following the retirement of David Swift on 31 January 2014.
13.138 External Audit – Progress Report Simon Hardman, Audit Manager presented a report summarising the position to date, confirming that work would commence in January 2014 and continue until late June, by which time the audit of the 2013-14 financial statements would be available. The scope of the work to inform the 2013-14 VfM conclusion would commence in December. Details of emerging issues and developments were also provided and Members attention was drawn to the section relating to Alternative Therapy, which outlined key messages and good practice regarding financial control, together with guidance relating to the Integration Transformation Fund. It was also noted that Sophia Iqbal had recently joined the Grant Thornton Team, bringing many years of public sector audit experience and would work closely with Fiona and Simon.
Page 4 of 5 Approved by TW : 6.1.13
Kirsty Hollis provided feedback following attendance at a workshop in Manchester led by NHS E highlighting key issues relating to year-end closedown. She confirmed work was in the planning stages to understand who will be doing what throughout the process, with a dry run in Month 9. A draft plan was in place and final reporting guidance was awaited. The initial submission to NHS E and Auditors was due by 23 April 2014. External Auditor would then have 5 weeks to conclude the audit and report to the Audit Committee. ACTION:
Check timing of the Audit Committee to coincide with final accounts reporting.
Guidance relating to the new requirements of Audit Committees to be circulated to members.
AP
13.139 External Audit – Value for Money Update Fiona Blatcher presented a paper outlining the VFM approach. The Audit Commission had issued guidance to enable auditors to focus on local issues and risks in the CCG’s first year of existence. The guidance also reflected the key things that CCGs will need to develop and it was important that the CCG has adequate arrangements in place to respond. Further discussions would take place outside the meeting and Fiona would be pleased to receive any views from Members. It was agreed there was no right way in the first year of reporting, but important to identify common messages to help raise the profile.
13.140 Locality Issues This item was to be deferred to the next meeting.
13.141 Resilience & Emergency Planning Ryan Catlow was in attendance for this item. Ryan confirmed that Tim Mansfield was the accountable officer for Emergency Planning & Resilience, whilst he supported the operational work. The CCG requirements were lighter than those for the PCT and it was important to ensure that contracts with providers have emergency plans in place and work was ongoing with the contracting team. NHS E would work with providers to deliver this agenda. The CCG would support the Area Team in the event of a major incident and plans were in place to identify those requirements. A Major Incident Plan and Business Continuity Plan were also in place which sat under the Emergency Planning Policy approved by the Governing Body in October and an On Call system spans both Blackburn with Darwen and East Lancashire CCGs. In terms of assurance, the Area Team would undertake an assurance review of emergency planning requirements next year.
Page 5 of 5 Approved by TW : 6.1.13
All documents had been shared with Area Team and would be reviewed annually which was recognised as best practice. Members felt the arrangements in place were robust in terms of escalation. The Plan addressed key issues and linked with the annual resilience work regarding winter planning. It was reported the Emergency Plan was tested during the summer, involving the CCG and partner agencies. However there was a need to test the CCGs arrangements and agree how this will be done. Lancashire wide discussions were ongoing to consider whether there was a requirement for a senior management on call presence within each CCG. There was also a need to take into consideration the Area Team emergency plans and a copy would be requested. ACTION:
Request sight of the Area Team Emergency Plan. The Chair thanked Ryan for attending and providing an update to the Audit Committee.
TM
13.142 Any Other Business 13.142.1 New Items for the Risk Register Concerns regarding the C Diff data being below trajectory to be included. 13.142.2 Counter Fraud Clare Ward, Local Counter Fraud Specialist to be invited to a future meeting.
13.143 Date of Next Meeting The next meeting was scheduled for Monday, 13 January 2014, 12:30pm in Meeting Room 1.
Page 1 of 5 Approved by TW : : 27.11.12
AUDIT COMMITTEE Minutes of the meeting held on
Monday, 11 November 2013, 12:30-13:30pm, at Walshaw House PRESENT: Tom Wolstencroft Lay Advisor, Governance - Chair Jackie Hanson Chief Nurse Dr Phil Huxley GP Clinical Lead - Pendle
Dr Murthy Motupalli GP Clinical Lead - Hyndburn In Attendance: Angela Brown Head of Corporate Affairs Mark Youlton Chief Finance Officer Kirsty Hollis Deputy Chief Finance Officer David Swift Internal Audit Manager, ANW Mohammed Kothiya Assistant Management Accountant Marianne Rintoul Locality Lead – Provider Relationship Management, LCSU
Anne Pietrzak Board Administration Manager - Minutes
Min No: ACTION
13.117 Welcome, Introductions & Chairs Update The Chair welcomed everyone to the meeting. Mohammed Kothiya was attending as an observer and introductions were made.
13.118 Apologies Apologies were received from Steve Allcock, Fiona Blatcher, Simon Hardman and Lucille Hinnigan.
13.119 Governance Declarations of Interest – None received. Quoracy – The meeting was quorate.
13.120 Minutes of the meeting held on 14 October 2013 The minutes of the previous meeting were approved as an accurate record.
13.121 Action Matrix v7 The Action Matrix was presented and discussed: 13.46 - Terms of Reference: This was covered on the agenda. 13.82 - Patient Confidential Data: EMIC system was not working as smoothly as intended. The CCG was working with the CSU to ensure invoices are paid within a timely manner. 13.113 - Grant Thornton Survey: The questionnaire had been reissued to the Chief Finance Officer. 13.114 - Allocations: MY confirmed feedback had been received, advising that deprivation was reflected in the mortality figures. Reference was also made to an article in the BMJ which highlighted a very clear link to deprivation & mortality in the
KH
Page 2 of 5 Approved by TW : : 27.11.12
debate regarding allocations. Notification of allocations was due in December and any change would happen over a period of time.
13.122 Matters Arising 13.122.1 Updated ToR With reference to Section 9.9 of the Terms of Reference, clarity had now been received regarding the role of the CCG and the Audit Committee in respect of Emergency Planning and Resilience. Lead responsibility sat within the portfolio of the Chief Operating Officer and Tim Mansfield would attend the December meeting to provide clarity. It was noted the formatting of the document required updating in respect of paragraph numbering.
AP
AP
13.123 Quality & Safety Committee Minutes – 16 October 2013 Jackie Hanson, Chief Nurse and Chair of the QSC presented the draft minutes and highlighted key points. Discussions were ongoing outside the Committee to understand the infection control procedures, as lead responsibility had transferred to Public Health. MRSA rates with the local provider identified high numbers and in conjunction with the TDA, a high level meeting was taking place on 21 November to consider responsibility across the health economy. A Francis update had not been provided and it was acknowledged this was due to a lack of capacity within the system which had been included on the risk register at level 20. This was considered a significant risk for the CCG going forward regard internal capacity and the CCG had agreed to fund a Head of Quality post which had now been advertised. Discussions were also ongoing with the CSU regarding capacity within their team and members would be updated regarding their intentions to support this agenda going forward. The Quality Assurance Framework was a major area where the CCG was focusing attention. Fortnightly meetings were taking place with ELHT to consider evidence against the specific sections and a detailed analysis would be presented to the next meeting of the Governing Body. Jackie had also met with the TDA to consider how evidence would be shared. The Rossendale Listening Event was very successful and a second listening event was to be held in the Pendle locality. The CQC Inspection Report relating to Royal Blackburn Hospital had been shared and members discussed the enforcement notice and actions required. Monitor and the CQC were completing investigations into specific issues at Calderstones and the CCG had a very positive quality meeting with Calderstones. In response to members concerns, Jackie confirmed that due to a lack of capacity and strategic level leadership at ELHT regarding a number of issues, the CCG had developed the QAF following the Keogh Review and was providing a level of input and support to obtain assurance going
Page 3 of 5 Approved by TW : : 27.11.12
forward. It was important to work with the Trust, but the CCG was not there to operationally manage what is happening in the Trust. It was also confirmed that the Chris Cason had been appointed Chief Nurse at ELHT and was due to commence in January 2014. Members discussed the soft intelligence system, particularly the breadth of the review. Jackie confirmed that information captured in the system relating to patient feedback is considered on a weekly basis and themed to identify trends and issues are raised with ELHT. It was considered that the issue relating to the Slaidburn Practice should this be on the Risk Register and this would be addressed at the next meeting. Members discussed the wider impact of MPIG on primary care, noting that responsibility and accountability sat with NHS England.
JH
13.124 Waivers / Financial Contracts Proforma Marianne Rintoul was in attendance for this item. Members were reminded that a proforma had been developed and presented to a previous meeting when it was considered that more detailed contract information should be incorporated into the proforma. Marianne advised that the CSU Contract Management Team held a contract depository which provided an indication of the terms of individual contracts, when these are due for review and outlined any issues that are likely to go to procurement. The CSU also looked at shared contracts across the region to co-ordinate where there are several contracts in place. It was considered that as this information was already available, it would address the requirements of the proforma and would be shared with the Audit Committee. Clinicians felt it would also be useful to receive contract information in primary care, outlining what is working well and when contracts are due for review. This would provide the overall picture and create an opportunity to influence decisions going forward. The Audit Committee also had a duty to look at Waivers. The process for quotations and tendering was outlined and it was agreed that when contracts that are due for renewal or procurement and the process does not fit within the formal procurement criteria, the issue should be raised through the Audit Committee. ACTION:
Circulate guidance regarding quotes required. Provide a positive declaration that waivers are not accepted.
KH/AP
13.125 Locality Issues The Head of Corporate Affairs confirmed there was good engagement at the Risk Management Committee with Locality Managers which provided positive assurance that risks are being identified and addressed.
Page 4 of 5 Approved by TW : : 27.11.12
13.126 Learning from Others Members were advised that a programme of training had been provided during the first year of the CCG. A Conflict of Interest training session was planned for CCG staff which was relevant to commissioning managers when drawing up contracts. Staff had been invited to identify training needs to fulfill their role and programmes of development had been arranged to meet their requirements. Dr Huxley provided feedback from the locality advising that the view was there was that on occasions the timing of the learning events impacted on access due to the number of Practice closedowns. This was a reflection of how much work was ongoing, providing opportunities to develop, but it was also important to consider the impact on Practices. There was reference to the 38 Degrees campaign regarding gagging clauses, noting the Constitution had been amended to positively reflect specific comments. There was also a need to be conscious that 38 Degrees will be asked to check CCGs locally that actions had been taken.
13.127 Public Involvement & Engagement Dr Di van Ruitenbeek, CCG Chair & Lay Advisor for Public Involvement and Engagement was in attendance for this item to update the committee on the work ongoing within the organisation. Di referred to the new system for collecting soft intelligence, noting the CCG was receiving patient stories and feedback that was not previously received which was encouraging. The data would be used to identify trends to raise with providers. The process had been developed following the Keogh review to ensure the CCGs response to Francis is open, transparent and robust. Di welcomed thoughts on how this process is working. In relation to timescales, it was noted the system should acknowledge automatically, followed by a review of issues identified and feedback to practices and patients. It was highlighted that a significant amount of time was spent on complaints within the practice and clinicians felt the process was confusing for patients as complaints are managed by NHS E rather than the CCG or CSU. Concerns would be raised the Area Team at the next meeting. Jackie had expressed interest in the CSU IT system that could assist in streamlining our current system, which identified soft intelligence alongside complaints. This system was working well in Staffordshire and it was important to review thoroughly and ensure a managed transition, should any changes take place. The CCG held its first Listening Event in Rossendale, which was the first in a series of events across the localities, the next event being in Pendle on 16 November. Approximately 70 people attended the Rossendale event, which was run in the style of World Café , with comments on post in notes and opportunities to speak in groups or in private. It was important to demonstrate that points raised by the public are addressed and Andy Laverty had produced a detailed account of the feedback together
JH

Page 5 of 5 Approved by TW : : 27.11.12
with planned actions. Rossendale residents had raised concerns regarding the lack of a specialist Parkinson Nurse. Following this a business case was prepared for submission to LDG and the GB for approval in November, highlighting that the organisation is listening and consider what has to be done, fulfilling the You Said We Did approach. Di highlighted the need for better use of the website and to consider better ways of communicating, particularly with hard to reach groups. A recent visit to the Health Access Centre had identified concerns that some people cannot access email, websites and phones. All engagement activities need to be co-ordinated to ensure the correct information is issued at the right time. When dealing with highly controversial issues, it is important to demonstrate that we listen, are open and transparent and views are taken into account. Di considered that the CCG had not until recently been tested in this way and it was important to recognise controversial issues and work smarter to manage the message. It was also important to make the distinction about speaking as individual GPs or as CCG clinical leads Di confirmed that the Remuneration Committee had agreed to the appointment of a second Lay Advisor with a key interest in Patient Engagement and Quality. The role would enhance the quality agenda and continue the patient engagement work. The Chair thanked Dr van Ruitenbeek for outlining the work ongoing across the organisation in respect of patient engagement.
13.128 Any Other Business Risk Register There were no additional items inclusion on the Corporate Risk Register.
13.129 Date of Next Meeting The next meeting would take place on Monday, 9 December 2013 at 12:30pm.
Draft minutes approved for circulation by Dr Mike Ions, (Chair) on 23 December 2013
PENNINE LANCASHIRE CLINICAL TRANSFORMATION BOARD
Wednesday 4 December 2013 at Walshaw House, Nelson 4.30pm – 6.00pm
M I N U T E S v review draft
Present: Dr Mike Ions Chair ELCCG Dr Warren Larkin LCFT
Dr Chris Clayton BwD CCG Dr Murthy Motupalli ELCCG Dr Alan Crowther ELHT Ms Maire Morton ELHT Dr John Dean ELHT Dr Bob Palmowski ELMS Dr Paul Hartley ELCCG Dr Ian Stanley ELHT Mark HIndle Calderstones FT Dr Amanda Thornton LCFT Dr Gifford Kerr PH BwD
In Attendance: Jackie Hanson ELCCG
Tim Mansfield EL CCG Debbie Nixon BwD CCG Alex Walker ELCCG CI Justin Srivastava Lancashire Constabulary Jillian Wilde Pennine Lancs CCGs Elizabeth Houghton EL CCG ( note taker)
13.101. Welcome and Introductions The Chair welcomed Chief Inspector Srivastava, Jillian Wilde, Jackie Hanson Mark HIndle and members to the meeting, introductions followed
13.102 Apologies These were received and noted from: Dr Arokia Antonysamy Val Bertenshaw, Kathy Blacker, Mark Brearley, Dr Simon Hill Martin Hodgson Prof. Max Marshall, Malcolm Ridgway, Mrs Rinecke Schram, Steve Tingle
13.103 Presentation
Jillian Wild and CI Srivastava spoke to a presentation (copy attached) which summarised the background and case for a proposal to initiate 12 month pilot a co-ordinated and integrated police support role within A&E by co –locating two Police Officers within the A&E department at Royal Blackburn.. Officers would work with stakeholders to address the needs of a cohort of ‘chaotic’ patients s who present at A&E with:
• challenging behaviour • alcohol and substance misuse issues
Pennine Lancashire Hospital Early Action Team CTB Presentation 4th Dec 13 v3.pptx
Page 2 of 8
• people who do not have a clear mental health diagnosis • frequent attenders with all of the above
Information relating police calls to RBI A&E September 2012/September 2014 was presented as follows
• There were a total of 1230 calls – an average of 100 calls per month • 305 calls were in respect of Concerns for Safety (24.7% of the total
calls) • 65 calls related specifically to missing persons (5.3% of the total) • By the very nature of the missing person calls, a significant number are
graded as high risk • 120 incidents that related to nuisance (9.7% of the total) • 181 incidents related to sudden death (14.7% of the total) • When looking solely at ASB incidents there have been 63 calls in the
past 180 days. • The next nearest demand is 27 incidents which relate to a House of
Multiple Occupation. The proposal to pilot an Early Action Police Liaison Role within the A&E Department at Royal Blackburn Hospital for a 12 month period would aim
• to provide a more co-ordinated and integrated police support role within A&E
• to share data to identify frequent flyers across health and social care • to develop a Memorandum of Understanding and a Risk Sharing
Protocol between organisations in order to reduce demand and multiple hand-offs
• to facilitate early referral into targeted services to improve outcomes for individuals and families and potentially reduce demand
and would support Two Police Officers co-located within the A&E department (Monday – Thursday daytime and Thursday – Sunday overnight) who will work with stakeholders to address the needs of individuals with:
challenging behaviour alcohol and substance misuse issues people who do not have a clear mental health diagnosis frequent attenders with all of the above
This would enable
• A single risk assessment will be undertaken as per the Memorandum of Understanding
• Appropriate individuals will be signposted into an Early Action intervention.
• Training, Development and Support for staff within ELHT The pilot would build on the experience of a similar model in Leighton –which has reported a 15 % reduction in concerns for safety, 9% reduction in sudden deaths reported and 46% reduction in anti-social behaviour it is anticipated that a PL pilot would demonstrate inter alia the following benefits
establish whether frequent flyers are common to all agencies • streamline pathways and reduce demand on staff and organisations by
minimising multiple hand-offs
Page 3 of 8
• reduce unnecessary police attendance in A&E Department • reduce unnecessary aggression against hospital staff • increase patient access into early action services and measure whether
this reduces unnecessary attendances at A&E The business case would be developed and put forward to the CCG Boards There followed discussion including these points
o PL Information sharing Agreement already exists - based on revolution
project – challenge now to use it – need to use and make work o The project would present the opportunity to build evidence for co-
locating MH crisis workers. o The importance of encouraging greater input from mental health
services and the opportunity to make a first diagnosis which wold be followed up in primary care
o There is a level of support from ELHT for this project o It would provide valuable experience of building multi - agency teams o There is a similar – if not the same cohort of patients presenting in
primary care o Not all patients are ill – they do have adversity – there was reference to
the US system of using an ‘A’ score which could be incorporated into the pilot – rather than medicalising all presentations
o Governance process – the case which would involve multi-agency funding is being put to each CCG, the Access and Flow group both Local Authorities and the Police Authority
o The groups attention was drawn to the recently published Design Council information relating to how design of eg signs, information and ‘wall messages’ in A&E departments helps to reduce violence and aggression in the area – it was estimated that an amount of £20K could be identified to align this as part of the exit strategy ( similar to the Enhancing the Environment project)
In conclusion it was agreed that the PLCTB supported the pilot proposal including the action, which it has been proposed to include in the exit strategy, and would welcome further information as the project develops
13.104 Governance
Declarations of Interest – Drs Crowther, Motupalli and Palmowski declared financial interests in the discussion about Community hospital provision under agenda item 6.2 minute 13.111
Quoracy - the meeting was declared quorate
13.105 Minutes of previous meeting Held on 6 November 2013 were received, reviewed and agreed as an accurate record;, subject to the duplication p4/5 being corrected
13.106 Matters Arising including review of Action Matrix - Re 13.084 Tim Mansfield (TM) confirmed that ELCCG board had supported the bid for a Parkinson’s Disease Nurse and that a bid for financial support was being submitted to the Parkinson’s Society, discussions relating to the possibility of sharing the service with BwD would be held outside this meeting
TM
Page 4 of 8
Re 13.091 TM confirmed that the Winter Escalation Plan was aligned with the CCGs on call rota for the period RE 13.079 Debbie Nixon (DN) requested a correction to the action matrix to indicate that action is to bring collective action plans/shared learning as part of collective Transformation Fund proposals to the January meeting of the PLCTB Other Matrix Review items followed either on this or subsequent meeting agenda
Corporate Admin/DN
13.107 Action Matrix Re 13.099 Appointment of Chair of Palliative Care & EoL Steering Group TM reported that whilst it had been agreed previously that this would be a GP, he would act as chair on an interim basis Re 13.090 Post Discharge Mortality Review Jackie Hanson Reported that a first meeting of the review grop had been held on 28/11 to scope the review – there was no previous model available so PL needs to develop its own process, to clarify the focus around whether to review deaths by diagnosis or risk or where GPs identified cases of concern a mix was probable and ta secondary review – triggered by findings emerging from the primary review and seeking to identify preventative actions would follow; it was noted that there was intention to involve GPs in the scope of the review – the next meeting will be held in January 2014 and a report to the February meeting will follow
JH
13.108 Keogh Update and CCG QAF Jackie Hanson noted that previous versions of the QAF had been available to all members of the PLCTB, Version 18 had been circulated prior to today’s meeting. She reported: that at this stage evidence was being collated and added to an evidence template with particular reference to patient experience and organisational development; that initial progress had been slow but now gathering pace; that the CCGs had provided robust feedback to the Trust and had added particular challenges around the Trust’s complaint handling; that evidence was being aligned with experience at different organisational and service levels that the next iteration would be the following Monday For the Trust Dr Ian Stanley reported that evidence was now being provided in different format for this process and for the weekly reports to the TDA- the level of detail is high and that it has not always been possible to provide it as required, but that this was changing slowly. IS reported that there had been a fruitful meeting between the Trust and the Newcastle Team earlier in the day which had been helpful in particular with gathering information from patients, engagement and with governance In acknowledging the general sense of frustration and pressures, MI indicated that it is now understood that progress has been achieved to a point in a number of areas. Dr Chris Clayton(CC) reported that at the earlier BwD Board Meeting ,the CCG had been held to account by lay members of the Board and public present- he continued that it was difficult to provide public assurance, and that we need to simplify the language we use – he suggested that the risk plan could be
Page 5 of 8
annotated with eg ○ we support, ○ support with concerns , ○ don’t support
MI reported that it would seem that the second risk summit – originally expected in September would not take place in December and that at that meeting there would be an expectation that improvements for the population could be reported. JH advised that these matters would be taken forward in the course of the next meeting of the Keogh Review Group and should be in place by Christmas as Dr Clayton had requested It was agreed that on-going report of the QAF would be made to the January meeting and that this be a standing item on future agenda of the CTB
JH Corporate Admin
Executive Officers’ Group – report Debbie Nixon reported that the most recent meeting of the EOG had been cancelled and that members had been asked to prioritise a future meeting, there followed discussion about the need to review membership of the group to ensure that it was fit for future purpose (qv presentation Agenda 6.2 programme management) and The Chair referred to the expectation that it was the group which undertook the work remitted by or on behalf of the CTB.
13.109 Winter Plan – update Papers circulated prior to the meeting, Debbie Nixon reported that the PL winter planning meeting which CC chaired had been held earlier in the week-. Confirmed Actions are as follows
winter plan has now been signed off by all partners signed off
escalation plan signed off
monitoring the A&E recovery plan is ingoing The Desk-top exercise had been successful , there were remaining concerns relating to (a) the co-location of Ambulatory Care and GP OoHrs services within former GUM Clinic – date for start of this arrangement is now confirmed as 15 December and to (b) the inevitably high level of scrutiny of A&E Recovery Plan not least given that this is a high profile system under pressure and additional NHS funding TM advised that there had been internal discussions within ELCCG and that clarity was still needed around Ambulatory Care Pathway – CC agreed that a wider understanding of the issues was required – needs to be ‘sold’ to partners in this Pathway this was being requested through the contract mechanism Dr John Dean advised that he, David White and Sakthi Karunanithi had been present at the meeting and that this would be taken forward as an action point Dr Clayton sought assurance as to where the systematic scrutiny of the A&E Recovery plans would occur. TM responded that it rests with the Executive Officer Group – a weekly telephone call is introduced with Val Bertenshaw, ELHT and NHS England Jillian Wild would capture the status and actions in the Recovery Plan Dr Ions queried who would take the actions which would arise should the plan
Dr John Dean
Page 6 of 8
be underperforming or not delivering and was there a real-time reporting mechanism to the Urgent Care group or the ELCCG as lead commissioner. Dr John Dean indicated that organisations should ensure that the ‘call makers’ referred to earlier should be the people who have the authority to effect action within their organisations A report would be made to the January Meeting of the CTB
13110 Pursuing the Perfect Week –update Alex Walker spoke to a presentation – copy attached– and reported the actions taken since the previous meeting to progress/accelerate those Actions which had arisen from the ‘first’ Perfect Week- he noted that this had proved more problematical than anticipated, the main issue being governance arrangements.. Work was ongoing against a check-plan which would identify ‘Quick wins’ in terms of process, timing, adjustments to ways of working and timescales for action which could make a difference to when discharge can occur, but he advised that it was unrealistic to deliver the associated and significant behavioural or cultural changes in the intervening month. He reported that governance structures were proposed which clarified programmes of work and that Integrated Care Systems and Integrated Neighbourhood Teams are clearly CCG led pieces of work but linked back to safer transfer work and future planning. The PL Integrated Care Delivery Group of key managers was now scheduled to meet regularly and would report to CCG Boards via EOG and the CTB. He assured the CTB that an Action plan would be agreed by December 14 2013 and a stakeholder event was planned for January 2014 The second presentation ( copy attached) identified and summarised the key themes which emerged and the proposed next steps from a follow up to the Perfect Week exercise in East Lancashire which included a review of two intermediate care resources jointly funded by ELCCG and LCC ( didn’t include two CHs) It was noted that BWD had commissioned external scrutiny to look at proposal how for build capacity of intermediate care services to manage complexity with particular reference to dementia – potentially to have a step-up facility which doesn’t currently exist in PL. Pennine Lancashire Dr Chris Clayton responded that at the Winter Planning Meeting, held on the previous Monday there was a clear view that a unified discharge arrangement should be agreed and in place in four weeks, there followed discussion and the points noted were
o An in principle agreement of a single set of criteria for intermediate care could be reached in the meeting but that for a range of practical reasons, it would not be possible to deliver the full working arrangements in four weeks
o There are real differences in the on – the ground services in East Lancs and BwD which at this point would not enable a fused model
o Such agreements could be signed up in principle at a Clinical Lead or CTB level but that in practice significant intra and cross- organisational cultural shifts were required for implementation
o A discussion had been held to discuss, determine and agree the terms of complex and simple discharge
Perfect Week 1 November.pptx
Perfect Week 2.pptx
Page 7 of 8
o Need to sort multiple assessments / multiple teams involved in discharge
o Should be clearer re known complex cases – current practice does not set up the process of case management straight away but close to discharge when it is difficult to put in place supports which are known to take months or longer to coordinate
o Once patients with complex needs are well case-managed through the system this will be the key to successful discharges
o If a single set of criteria for discharge to Community Hospitals were to be agreed - with Commissioner’s support, transfers could be achieved more easily
It was agreed that an action plan would be developed within 7 days and that
Alex Walker will outline the required outcomes
ELHT ( lead organisation) will respond with what needs to be in place and what level of support is required from each organisation
ELHT will identify the Pilot Lead
Each partner organisation will identify the key link
All partner organisations will commit fully to providing the best support possible throughout this initial period and prepared to escalate to the highest level to enable progress
A preliminary report will be presented to the January meeting of the CTB and a Key Topic discussion will form part of the agenda at the February meeting
13.111 Pennine Lancashire Quality Improvement & Learning Forum – proposal and TORs Jackie Hanson reported that the initial draft which had been circulated was based on the pledges which had been agreed earlier in the year and that it had been deemed necessary to establish a forum which focusses on quality and improvement ,which was attended by all the partner organisations’ Quality Leads The paper proposed a core membership – it was noted that this could be extended at a later date but that it was important to begin the work which would address priorities in the whole health economy thematically – ie how key information is conveyed from meetings, how soft intelligence is captured and an external focus on work of organisations such a AQuA which had local impact. It was stressed that this was learning into action group not an assurance group. The Group would be facilitated by the CCGs as Commissioners would meet bi-monthly and that the chair would rotate to ensure all organisations were fully involved. The next meeting would be held in February an, minutes could be circulated for information. It was proposed and agreed that a first formal report would be made to the CTB in March There followed discussion referring to Dr Dominic Harrison’s proposal about investing collectively in an independent information officer who would support such a group. Dr Gifford Kerr advised that the next step would be to discuss the matter with Dr Sakthi Karunanithi and that the outcome of that discussion could also be brought to the March meeting Support was expressed for the idea that a Quality and Improvement Faculty could be developed within the Health Economy
JH Corporate Admin Dr Gifford Kerr
Page 8 of 8
13.112 Integration Transformation Fund ( ITF) Tim Mansfield reported that the governance context for the |Integration and Transformation Fund(ITF) was set out in a slide within an earlier presentation ( copy attached) This indicated that in the East of the county Health & Wellbeing partnership, comprising 5 districts, ,county council, voluntary sector and CCG would play a significant role- the next meeting of this group would be around 26 January 2014 A stakeholder event including all service providers was proposed for the 8 January 2014 at Turf Moor to develop working proposals for the Fund A similar event was to be held in BwD, facilitated by Peter Colclough to develop an agreed level of ambition for transformation and integration – modelling the impact on ELHT beds and community services. Debbie Nixon noted that it would be necessary to review the combined impact of the proposals which emerged from the two events prior to submitting these in February It was proposed and agreed that the review of ITF submission would be a Key Topic and allocated one hour’s discussion at the February meeting of the CTB.
IC accountability DRAFT v6 26.11.13.odp
13.113 Pennine Lancashire Strategic HCAI Group – scoping, draft TOR’s and Membership Jackie Hanson reported that this group had been established to address issues relating to HCAI given that the level of eg MRSA affected Quality Premia and that there were concerns around the system relating to infection control Jackie is coordinating the group with representation from TDA LA primary care, medicines management. Draft TORs and proposed membership to be circulated when they are available. There followed discussion about the allocation of incidences of MRSA it is noted that Dr Chris Clayton intends to raise the concern at a national level and there was general agreement that this is a whole community concern rather than a specific provider – specialist advice is required.
Jackie Hanson
AOB Re Oncology Dr Alan Crowther advised that there would be three oncologists in post by the end of January 2014 the Oncology Steering Group was concerned that tit had not yet received the final commissioning specification from Lynn Scott and Neil Smith Agreed action : TM would take this forward
TM
Date & Time of next meeting This was proposed and agreed as Wednesday 8 January 2013
4.30pm in Meeting Room 1
at NHS East Lancashire, Walshaw House, Nelson

Page 9 of 8
NAME REPRESENTING Julie Cooper – in the Chair Burnley Council Mike Banks LCC Pam Barton Hyndburn BC Tony Beckett Pendle Council Mark Brearley East Lancs Hospitals NHS Trust Mick Cartledge Burnley Council Ian Clark Together Housing Group Dianne Gardner LCC Terry Hephrun Burnley, Pendle & Rossendale CVS Bridget Hilton Ribble Valley BC Colin Hirst Ribble Valley BC Paul Hussey LCC Mike Ions East Lancs CCG Tim Mansfield East Lancs CCG Mick McHugh Philip Mousdale Pendle Council Clare Pritchard Hyndburn BC Steve Tanti Hyndburn Council Kelly Taylor East Lancs CCG Di Van Ruitenbeek East Lancs CCG Mike Wedgeworth Third Sector Lancashire Imelda Grady Burnley Council
37. Apologies
Apologies were received from Councillor Azhar Ali, Ian Clark, Mike Hammond, Mike Leaf, Councillor McInnes and Fiona Meechan,
38. Minutes
The minutes of the meeting held on 30th September 2013 were confirmed as a correct record.
39. Joint Strategic Needs Assessment Summary
Mick McHugh gave a presentation on the new joint strategic needs assessment (JSNA) for children and young people in Lancashire. This new
MINUTES OF THE EASTLANCASHIRE HEALTH AND WELLBEING PARTNERSHIP
held at Burnley Football Club
Monday 25 th November 2013 @ 3.30pm
JSNA gave a refreshed analysis of the data available in five key stages from pre-natal through to young people aged 16 to 19, and also on emerging issues such as measles, safeguarding pressures, child sexual exploitation, missing children and austerity measures. The presentation showed that poverty and deprivation remained a common thread across all stages.
The presentation outlined the positive differences that had been made to date through the Children and Young People’s Plan in areas such as traffic accidents, teenage pregnancies, offending rates, exclusions from school, educational attainments and young people choosing not to drink alcohol or smoke.
The new JSNA would be published by the end of March 2014 and district profiles would be available soon.
In response to a question about district levels of MMR vaccinations, Mick McHugh agreed to provide this information.
Councillor Beckett said that it would be useful to have the district profiles broken down further so that resources could be better targeted to needs, however Mick MCHugh said that the data set might not always drill down to this level.
Mike Wedgeworth said that poverty and deprivation needed to be addressed and referred to a welfare rights campaign in Wyre and Fylde which had seen an increase in the take up of benefit entitlements up to £1m and suggested that this could be done elsewhere.
Tim Mansfield referred to the Marmot report’s key messages on the need to intervene early to address health inequalities and Kelly Taylor confirmed that work was continuing with children’s centres to provide these early interventions.
Mick Cartledge said the district councils were focusing on longer term benefits through investment in the local economy and education which, although not direct health measures , would impact on the health wellbeing of residents by providing better employment opportunities and housing.
Di Van Ruitenbeek said that the Integration Transformation Fund, which was to be considered later in the agenda, could offer an opportunity to address issues in a more innovative way.
40. Health Access Centre – Hyndburn
Tim Mansfield informed members that the CCG Governing Body had agreed to defer a decision on future of the Health Access Centre in Hyndburn until February/March 2014.
The engagement exercise had shown that there was a clear demand for a walk-in service but this had to be set in the context of the savings that the CCG had to meet over the next three years. The CCG could not continue
with a contract where it had no control over costs.
The options now being considered were provision of a walk-in-service at a fixed cost rather than a fee per attendance or increased access to GP’s surgeries with in-day appointments, extended hours and with some walk- in provision.
Tim said that the deferral of a decision would mean extending the current contract which would have a financial cost to the CCG but confirmed the service would not be withdrawn until there was a robust plan in place for alternative provision.
Members discussed issues associated with accessing primary care and considered different ways in which urgent care might be accessed, all of which would be taken into account before a final decision on the Health Access Centre was taken.
It was noted that further more detailed costed opti ons would be developed which could then be considered by the CCG and the Partnership.
Tim Mansfield
41. Keogh Review – East Lancashire Hospitals NHS T rust
Mark Brearley, Chief Executive of East Lancs Hospitals NHS Trust, updated members on 5 key areas of concern that had been identified by the Keogh Review and outlined the steps that were being taken to address them. The 5 areas were staffing levels, the complaints system, maternity unit processes, operating capacity/demand levels and governance.
He said that external scrutiny had been commissioned to look at staffing levels and as a result more staff had been recruited to deliver care. The complaints procedure had been improved to provide for face to face meetings with the clinical teams early in the complaints process. The maternity unit processes had been examined and more close observation beds and staff made available.
In response to a question on the high number of still births recorded in March 2013 Mark said that the Keogh team had found no systematic process to make the Board aware of the situation and this had now been addressed.
In response to a question on staff morale, Mark indicated that the staff would prefer a more balanced coverage of the NHS in the media.
In response to a question on basic care and day to day nursing Mark said that extra health care assistants had been employed on each shift to support patients, senior staff would now visit patients to identify their care needs and a 24 hour helpline for patient and relatives was proposed.
Mark agreed to report back to the Partnership in Ja nuary 2014.
42. Health and Wellbeing Strategy Delivery Plan
Tim Mansfield presented information on the Health and Wellbeing Strategy Delivery Plan showing the actions and planned activity against the overarching goals to
• improve healthy life expectancy and reduce inequalities • improve experience of people receiving health and social care • reduce hospital admissions, readmissions and permanent
admissions to residential and nursing homes
The national and county outcome figures for October 2013 were also presented.
The East Lancs CCG had fed in its planned activity and actions into the plan.
The Partnership agreed that it would be useful for each partner organisation to complete a proforma setting out the ir top 5 contributions to address health inequalities in the ir areas. This information would be collated and evaluated at the next meeting to identify if there were any gaps and enable the part nership to focus on key areas that needed to be addressed .
Mick Cartledge/Dianne Gardner
43. Integration Transformation Fund
Tim Mansfield gave a presentation on Integration Transformation Fund which informed of a £3.8bn pooled budget to be spent locally on health and social care through joint arrangements between CCGs and local authorities.
There was £15m allocated to East Lancashire and Tim advised that half of this had already been committed and that a decision would need to be taken on how the rest would be spent in a way which would achieve the objectives and satisfy the national conditions attached to the grant.
The CCG and local authorities needed to agree the formula for distribution and a template with a costed and deliverable 2 year plan needed to be completed by February 2014.
The creation of an Integration Board had been agreed with County and the next steps would be to engage stakeholders and the public. The representatives of patient participation groups would be consulted in January.
It was agreed that the CCG and LCC be asked to arra nge an engagement event, externally facilitated, on 8 th January 2014 at 9.30 a.m. – 1.30 p.m.
CCG/LCC
44. Building Individual and Community Resilience
Dianne Gardner spoke regarding 2 successful business cases which had secured PCT non-recurrent funding early 2013 and had now been joined together into the Building Resilience Asset project. The project aims to tackle low level mental health needs. The steps proposed to achieve this included commissioning asset mapping work across the five districts to capture the assets that exist within those communities and then to utilise the funding to build upon these assets to build community and individual resilience. There would be a robust governance structure in place and a service specification and procurement process would be announced in the New Year with events organised to communicate the aims of the project to the third sector. It was suggested that the Partnership oversee the allocation of the funding to ensure an open and transparent process and that the bidding process should be similar to that applied to the Veterans funding allocation, although there was no consensus on this proposal.
45. East Lancs Re;Fresh
Mick Cartledge updated member on progress with the proposed re;Fresh initiative for the four districts.
The project based on the Blackburn with Darwen model had been worked up to give a standardised offer across the four districts. A launch date of April 2014 was proposed however Mick said that there was no point in moving to the costings stage unless funding was made available by next March.
Dianne Gardner said there was a need to look at how this project integrated with other health initiatives and Terry Hephrun pointed out that the third sector already delivered some of the components and that this expertise could be used.
Steve Tanti said that Hyndburn was supportive of the initiative.
It was agreed that
a) Dianne Gardner would discuss with Public Health colleagues the likelihood of any LCC public health funding bec oming available in 2014
b) A meeting of the five council lead officers and Public Health be held to progress this.

Dianne Gardner/Mick Cartledge
46. Telephone charges to GP surgeries
Tim Mansfield said that he would follow up this issue with the area teams and report back.
Tim Mansfield
47. CCG commissioning sub-group minutes
The minutes of the meeting held on 16th September 2013 were received for information.
48. Dates of future meetings
A special meeting with stakeholder to consider the integration transformation fund be held on Wednesday 8th January 2014 at 9.30 a.m. – 1.30 p.m. at Burnley Football Club.
The date of the next ordinary meeting would be held on Monday 20th January 2014.
Future dates were agreed as
31 March 2014 May meeting to be confirmed 21 July 2014 29 September 2014 17 November 2014 All meetings to commence at 2.30 p.m. and be held at Walshaw House, Nelson.
CCG meeting 28 November 2013 Page 1 of 3
Meeting held on Thursday 28 November 2013, 10.00 am
Between Lancashire CCGs Network Meeting room 1, Conference Suite, Floor 1, Preston Business Centre,
Watling Street Road, Fulwood, Preston PR2 8DY Present: In attendance: Dr Chris Clayton (chair) - Blackburn with Darwen Dr Gora Bangi - Chorley & South Ribble Dr Ann Bowman - Greater Preston Dr Tony Naughton – Fylde & Wyre Dr Mike Ions – East Lancashire Dr Amanda Doyle – Blackpool Dr John Caine – West Lancashire In attendance: Mrs Jennifer Butterworth, Strategic Engagement Lead, Aqua (item 12) Mrs Cath Hill, Director, Aqua (item 12) Professor Donal O’Donoghue, Chairman, Strategic Clinical Networks & Senate (item 13) Mrs Juliette Kumar, Senate Manager, Strategic Clinical Networks & Senate (item 13) Dr Julia Simon, Head of CCG Strategic Support NHS England
Mrs Debbie Nixon - Blackburn with Darwen Mrs Jan Ledward - Greater Preston/Chorley & South Ribble Mr Mike Maguire – West Lancashire Mr Peter Tinson – Fylde & Wyre Mr David Bonson – Blackpool Mr Gary O’Neil – Lancashire North Mr Mike Barker – Chorley & South Ribble Mrs Jill Truby – Network
1. Apologies for absence Apologies for absence were received from Dr Alex Gaw, Mr Tim Mansfield and Mr Andrew Bennett. 2. Declarations of interests There were no declarations of interests in relation to agenda items. 3. Minutes of meeting held on 31 October 2013 The minutes of the meeting held on 31 October 2013 were agreed as a correct record. 4. Matters arising and action sheet Dr Clayton reported that discussions around winter planning were ongoing with the area team. The action sheet was updated. 5. SRO leader role and work definition Following comments received at the Network meeting on 26 September a revised copy of the document on the role of the CCG SRO and CSU Collaborative Service Redesign Team Collaborative Work Programmes was presented and noted. 6. IPA update The Network noted the briefing paper from the IPA Programme Board.
CCG meeting 28 November 2013 Page 2 of 3
7. Independent sector mental health update Mrs Nixon explained that the process to pass on the lead role for mental health from Lancashire North to Blackburn was in a transition stage. It was agreed that Mrs Nixon/Mr Parr/Mr Bennett take forward. Mrs Nixon reported that Blackburn had engaged expert support to work around rehabilitation and will write a strategy and proposal to be submitted to CAG and the Network early next year. Dr Clayton emphasised that Blackburn would not take over the procurement lead until there was clarity on what they were taking over before submitting to their governing body for approval. Resolved: Mrs Nixon/Messrs Parr and Brown to take forward 8. CAG feedback Mr Tinson reported on the recent collaborative arrangement workshops that had taken place. From these workshops a work programme for 2014 was being produced for agreement by all CCGs. Mr Ashworth would attempt to visit all CCGs to showcase the outcomes of the workshop together with the proposed work programme. It was hoped that some operational work programmes could be passed over to other functions within the CSU which would allow the collaborative team to concentrate on supporting strategic collaboration. 9. Feedback Network Governance Mr Barker reported that examples of scenarios of levels A & B would be circulated next week for those CCGs still waiting to take the paper to their respective governing bodies. Other members of the Network fed back comments from their respective governing bodies. Some amendments were proposed and accepted. For those CCGs who expressed concern it was agreed to take the scenarios back to their governing bodies to offer a better understanding of the issues that the Network may be asked to agree on a Lancashire wide basis. 10. Non-emergency transport NHS responsibilities A copy of an early draft on Non-emergency transport NHS responsibilities had been previously circulated for comments which had been considered at the Lancashire Ambulance Commissioning Group meeting held on the 27 November. Mr Bonson summarised some of these comments. The paper outlined the NHS responsibilities towards patient transport for those who met eligible criteria. There was a general consensus by Network members that the NHS is not responsible for, and is unable to fund, transport for patients relatives or carers but is committed to working with partner organisations such as local authorities and voluntary sector organisations to signpost/identify the support available. Mr Bonson reported that he would seek legal advice before presenting the final version to the December meeting. Resolved: Mr Bonson to provide final version to the December network. 11. Aqua – advancing quality Members received a presentation from Mrs Jennifer Butterworth, Strategic Engagement Lead and Mrs Cath Hill, Director of Aqua – advancing quality. Areas highlighted during the presentation included: Improving Outcomes, Achievements, Summary Proposition, and The benefit of AQ – feedback from the providers. In summary of the presentation, AQ contributes to the delivery of CCG outcomes and quality requirements. AQ will continue to review and update systems and processes to reduce costs. In response to a question Mrs Butterworth confirmed that the cost which was for data collection and analysis was based on CCGs population footprints. Following discussion it was suggested that it would be useful to have a CCG précis from AQUA covering the following areas: cost and rationale for cost, evidence assurance, the part AQUA plays amongst other strategies, and assurance to governing bodies around this investment. Dr Clayton thanked Mrs Butterworth and Mrs Hill for an informative presentation. Resolved: Mrs Butterworth and Mrs Hill to write précis for all CCGs 12. Strategic Clinical Networks & Senate A presentation was received from Professor Donal O’Donoghue, Chair, and Mrs Juliette Kumar, Senate Manager to introduce Strategic Clinical Networks & Senate. Prof O’Donoghue explained that Senates had been established to be a source of independent, strategic advice and guidance to commissioners and other stakeholders and were non statutory bodies. He outlined the key
CCG meeting 28 November 2013 Page 3 of 3
relationships and membership of the Senate Council. He opened up a discussion on what the Senate could do to help CCGs. Dr Clayton thanked Professor O’Donoghue and Mrs Kumar for an informative introduction to the Senate. 13. Minutes of meetings The minutes of the Collaborative Arrangements Group meeting held on 12 November were noted. 14. Any other business Dr Bowman drew attention to the need for a representative to attend the Clinical Development Group. As this group was NWAS related Dr Doyle volunteered to write out to all CCGs seeking volunteers. 15. Next meeting: 19 December 2013, meeting room 1, Conference Suite, Floor 1, Preston Business Centre, Watling Street Road, Fulwood, Preston PR2 8DY.
CCG meeting, 31 October 2013 Page 1 of 3
Meeting held on Thursday 31 October 2013, 9.00 am
Meeting room 1, Conference Suite, Floor 1, Preston Business Centre, Watling Street Road, Fulwood, Preston PR2 8DY
Present: In attendance: Dr Chris Clayton (chair) - Blackburn with Darwen Dr Gora Bangi - Chorley & South Ribble Dr Ann Bowman - Greater Preston Dr Tony Naughton – Fylde & Wyre Dr Mike Ions – East Lancashire In attendance: Mr Mark Youlton – East Lancashire Mr Gary Raphael – Blackpool Mr Kevin Parkinson – North Lancashire Mr Iain Stoddart – Wyre & Fylde
Mrs Debbie Nixon - Blackburn with Darwen Mrs Jan Ledward - Greater Preston/Chorley & South Ribble Mr Tim Mansfield – East Lancashire Mr Mike Maguire – West Lancashire Mr Iain Fletcher – Blackburn with Darwen Mr Mike Barker – Chorley & South Ribble Mrs Jill Truby – Network
Mr Matt Gaunt – Chorley & South Ribble
1. Apologies for absence Apologies for absence were received from Dr John Caine, Dr Alex Gaw, Mr Andrew Bennett, Mr Peter Tinson, Mr Iain Crossley, Mr Roger Parr and Mr Paul Kingan. 2. Declarations of interests There were no declarations of interests in relation to agenda items. 3. Minutes of meeting held on 26 September 2013 The minutes of the meeting held on 26 September 2013 were agreed as an accurate record subject to the following amendments: Remove Dr Ions’ name from those present. Add Dr Amanda Doyle to those present. A correction was requested to minute 8 “Mr Jude presented an updated draft model for the North West Medical Emergency Response Incident Team arrangements. Following discussion it was agreed that Mr Bonson provides further cost details and Mr Jude agreed to circulate further details to accountable officers. “ 4. Matters arising and action sheet 4.1 Minute 8 NWAS, Mr Bonson agreed to re-circulate the document and to discuss the issue further with Mr Tinson. 4.2 Agreed to receive regular verbal updates on the IPA programme. 4.3 Dr Clayton gave an update on the quality surveillance group and the need for an understanding of the functions the group carries out. Concern around the process of agreeing reports at this forum was raised. Mrs Nixon and Mrs Ledward to write to the area team with their concerns. 4.4 Dr Bowman reported that unfortunately Greater Preston/Chorley & South Ribble CCGs had not been successful in their Health Economy bid to become a pioneer site for Health & Social Care Integration. 5. Review of working arrangements/network business case A detailed and lengthy discussion took place on the working arrangements of the network and it was agreed to arrange a 1-day facilitated event to take forward. Resolved to: Arrange a 1-day facilitated event.
CCG meeting, 31 October 2013 Page 2 of 3
6. Chief Finance Officers (CFOs) proposal for working together The network team was pleased to note that the Lancashire CFOs and area team Director of Finance had managed to claw back into Lancashire CCGs funding that had originally been allocated to the Specialist Commissioning Team or NHS England (for public health). In addition, it was noted that in view of the acknowledged problems in being able to justify how the original SCT allocation adjustments had been made and their differential impact on Lancashire CCGs, the CFOs had taken a pragmatic approach to risk sharing across Lancashire. This ensured that all the CCGs were able to plan to achieve their financial objectives in 2013/14, albeit that some CCGs were required to make substantial compromises on their original service plans and that the recurring positions of some CCGs had not been rectified. The network team noted the verbal report from CFOs and discussed the ways in which general risk share arrangements could best be organised more formally, while keeping the flexibility required to deliver results quickly. It was agreed that a number of CCGs in Lancashire needed to consider how they may raise formally with NHS England the effect of the original SCT allocation reductions to CCGs and seek to resolve the recurring financial problems caused by these changes. 7. Interventions of limited clinical priority The Pan Lancashire Review of Commissioning Policies was mandated by the Collaborative Working Group as a Level 3 QIPP initiative. It has resulted in a revised local NHS “offer” based on systematic application of agreed principles. During the transition process the CCGs adopted the policies which had been implemented in Tranches 1 and 2. However development work on the subsequent policies was ‘put on hold’ pending a review of the impact of implementing Tranche 1 and 2 policies. Dr Bowman reported that evidence of the benefits of tranche 1 and 2 policies had been requested. No savings had been identified or how it impacted on financial planning. The network agreed that this was an important piece of work but did not wish to roll out with tranches 3 and 4 until further scoping work had been undertaken on tranches 1 and 2. Resolved that: Dr Ions to take forward with the collaborative arrangement group. 8. NWAS Patient Transport Service extension Mr Maguire asked members for their thoughts on the PTS contract. Mr Bonson reported that this should have been discussed at the recent ambulance group but the meeting was cancelled. He agreed to send out the paper that was circulated. The core services would go out to tender and there was consensus that any extended hours were to fit in with the contract. Mr Alan Jude had been tasked with taking forward with NWAS. 9. Primary Care Quality Mrs Ledward reported that both Greater Preston and Chorley & South Ribble CCGs had signed off the letter and sent out to all practices. Dr Bangi emphasised that performance management was the responsibility of the area team and quality improvement the responsibility of CCGs. Dr Clayton confirmed that this was also the approach from Blackburn with Darwen. Dr Ions reported on the system they used at East Lancashire whereby the CCG collects all the information, goes into practices and offers support. Dr Bowman stated that sometimes failure was due to circumstances outside of practices control such as premises, investment, succession planning and support. Dr Doyle suggested that each CCG responded separately. Dr Doyle reminded members to ensure that practices had adequate “out of hours” cover during Christmas and New Year Eves and not to put calls through to 111 before 6.30 pm. 10. Minutes of meetings The minutes of the meeting of Collaborative Arrangement Group held on 4 October was noted. 11. Any other business 11.1 TIA Mrs Ledward reported that the procurement of telestroke was to be linked into the work of TIA. The Senate was redesigning this work and looking for support.
CCG meeting, 31 October 2013 Page 3 of 3
11.2 Reciprocal assurance Mrs Ledward raised the issue of checkpoint assurance. It was agreed that Dr Bangi would write to the local area team. Mr Raphael reported that this had also been discussed at a recent specialist commissioning oversight group meeting where it had been agreed to develop proposals for consideration by CCGs. Dr Clayton agreed to write to the Specialist Commissioning group to obtain further information. Resolved that: Dr Bangi to write to the local area team Dr Clayton to write to the specialist commissioning group 11.3 Dementia Services Outcome Following the recent option appraisal of specialist dementia inpatient services, Mrs Nixon produced a progress report and final recommendation. It set out the decisions of all of the 8 CCG Governing Bodies across Lancashire. In summary, 7 CCGs have supported the recommendations. West Lancashire CCG has deferred the decision until November 2013, whilst they explore all local options. The West Lancashire number of patients is unlikely to have a material adverse financial impact on the inpatient scheme. A number of CCGs commented on their own local discussions, which included issues about access and requiring a detailed plan from LCFT regarding the roll out of the specialist community services. The CCGs also recognised that patients and their families would always be able to exercise choice about hospital admission, and in some instances may chose not to go to the Harbour. In summary the network agreed to support the recommendations of the Specialist Dementia Committee. Dr Bangi took over as chair for the following item only: 11.4 Review of Commissioning / Contracting arrangements Lancashire wide LCFT mental health contract Mrs Nixon reported that Blackburn with Darwen has continued to lead on the LCFT mental health contract. This was a legacy agreement and was agreed as part of the CCGs network discussions in 2011/12. The network was now being asked to consider re-designing the CSU support. There was also a requirement to identify a lead to provide overall programme management and co-ordination across the various stakeholders. Following discussion it was agreed that Mrs Nixon and Mr Maguire would put together a proposal for taking forward with the CSU. Resolved that: Mrs Nixon/Mr Maguire to put together a proposal Dr Clayton took over as chair 11.5 On call arrangements Dr Clayton reported that a meeting had taken place to discuss Lancashire’s “on call” arrangements and a proposal had been submitted based on a two tier arrangement. An “on call pack” would be produced detailing responsibilities with examples of scenarios. Resolved that: Dr Clayton/Mrs Ledward to take forward 12. Next meeting Next meeting: 28 November 2013, meeting room 1, Conference Suite, Floor 1, Preston Business Centre, Watling Street Road, Fulwood, Preston PR2 8DY.
Page 1 of 6
Agenda Item No: 6.1
REPORT TO:
NHS EL CCG Governing Body
MEETING DATE:
27 January 2014
REPORT TITLE:
Sub Committee Summary
SUMMARY:
This report summarises each sub-committee meeting of the Governing Body and full copies of all minutes are available from the Board Secretary on request. This report identifies: Items requiring approval from the Governing Body; Advises on delegated decision taken; Reports on key decisions; Highlights items of particular interest or potential risk.
REPORT CATEGORY:
Formally Receipt
Tick
√
Action the recommendations outlined in the report.
Debate the content of the report
Receive the report for information
AUTHOR:
Anne Pietrzak, Board Administration Manager
PRESENTED BY:
Angela Brown, Head of Corporate Affairs
COMMITTEES/ GROUPS CONSULTED:
Which Strategic Objective does the report relate to
Tick
1 Commission the right services for patients to be seen at the right time, in the right place, by the right professional.
2 Optimise appropriate use of resources and remove inefficiencies.
3 Improve access, quality and choice of service provision within Primary Care
4 Work with colleagues from Secondary Care and Local Authorities to develop seamless care pathways

Page 2 of 6
Agenda Item 6.1 NHS EL CCG Governing Body
27 January 2014
SUB COMMITTEE SUMMARY OF BUSINESS
1. INTRODUCTION
1.1 This report summarises each sub-committee meeting of the Governing Body and full copies of all minutes are available from the Board Secretary on request. This report identifies: Items requiring approval from the Governing Body; Advises on delegated decision taken; Reports on key decisions; Highlights items of particular interest or potential risk.
2. SUB COMMITTEES:
2.1 AUDIT COMMITTEE : 11 November & 9 December 2013 : Chair - Tom Wolstencroft
The minutes of 14 November & 9 December 2013 are attached in full at Appendix A.
2.2 LOCAL DELIVERY GROUP : 18 November & 23 December 2013 Chair - Dr Mike Ions
The Group discussed issues relating to the following areas:
a. Items requiring approval from the Governing Body:
Health Access Centre, Accrington Victoria Community Hospital
Following an engagement exercise, Members considered a paper outlining options relating to the future of the Walk In Centre and made a recommendation to the Governing Body that the following two options be removed:
Keep the status quo and tender a service in its current format
Let the current contract expire without a replacement service. The CCG had also met with Hyndburn Council when the options were considered. It was noted that NHS England would not make a decision on the preferred option for the registered list until February 2014. The Governing Body would consider the options at a future meeting.
Parkinson’s Nurse Proposal
A proposal to develop a primary care based Parkinson’s Nurse would be pump primed by Parkinson’s UK for two years on the understanding that the CCG would continue the funding. Members supported the proposals and made a recommendation to the Governing Body to support the Business Case and submit the letter of intent to the Parkinson’s UK Funding Panel.
Integrated Transformation :
Stroke Pathway Review Members received a business case for a revised Stroke Pathway to improve the rehabilitation and discharge element, allowing more patients to be rehabilitated at home and the remainder of patients being treated on one site with a maximum length
Page 3 of 6
of stay of six weeks. The revised pathway will improve patient outcomes and enable investment in an enhanced 7 day community stroke team. Dementia Local Service Model Members received detailed proposals to support the enhanced delivery of the national Direct Enhanced Service for dementia, including additional elements to provide a comprehensive local service, enabling a more robust post-diagnosis system in primary care. The paper proposed a Local Improvement Scheme be developed to ensure delivery of targeted case findings and screening, closure of diagnosis gaps at practice level and an improved annual review process. This would support the CCG priority to close the diagnosis gap and reduce the prescribing of anti-psychotics. Rossendale Hospice at Home Service A proposal to enter into a Section 75 Agreement with LCC was considered, which would allow the promotion of integration in end of life care on a wider footprint for the CCG, enabling the Hospice at Home service to continue to be delivered by the Rossendale Hospice and align with existing services. Pendle Community Diabetes A contract improvement notice was served on ELHT in order to allow the Trust sufficient time to implement the Diabetes Service as per the current service specification. Members reviewed a number of options and associated risks and agreed to support a recommendation to the Governing Body to approve the decision to serve notice on ELHT for the Community Diabetes Service. However viable options were to be provided to the next LDG to ensure an affordable option is available for consideration by the Governing Body.
b. Delegated decisions taken, requiring ratification by the GB.
Telemedicine
Members received a presentation from Airedale NHS Foundation Trust relating to Telemedicine, with the aim of providing a patient centred integrated service by using technology to support patients in their own homes, preventing admissions and reducing A&E attendances. Members supported a proposal to install 50 boxes into the highest admitting nursing homes for a trial period which would be funded non-recurrently this year. A robust evaluation would be carried out and patient feedback would be obtained. ELHT would also be advised of the intention to work with Airedale in relation to Telemedicine.
c. Reporting on key decisions: Cases for Change
Members received a presentation outlining the agreed process for the development of the commissioning intentions for 2013-16 and provided an overview of the key themes of the Cases for Change in respect of Urgent Care, Integrated Care, Scheduled Care & Demand Management and Dementia and outlined key priorities. A robust process had been put in place with clear timescales for completion. Members approved the Cases for Change.
Planning Guidance 2014-16
Members received planning guidance for 2014-16 which confirmed that strategic plans are produced covering a five year period. The first two years would be at operating plan level covering the cases for change and delivery plans, whilst the five year plan would include both a Lancashire wide and health economy plan. Allocations for the next two years were also presented. The first submission on plans was scheduled for 14 February and Governing Body approval of the plans was required prior to the deadline of 31 March 2014. Additional resources to support planning had been announced and a bid had been submitted.

Page 4 of 6
Finance, QIPP & Performance Members received a presentation outlining the month 8 financial position, progress against QIPP delivery and performance update, highlighting particular issues relating to referrals at ELHT and A&E performance.
Public Health Commissioning
Members received an overview of the Public Health priorities and associated services commissioned by LCC in East Lancashire and summarised commissioning intentions and plans for 2014 onwards.
Urgent Care :
Annual Resilience Planning 2013/14 – Winter Update Members received an update in respect of developments, finances and planning undertaken to support Winter 2013/14, highlighting key areas. The Trigger & Escalation Plan was now live and a three week plan had been implemented to cover the Christmas and New Year period. Additional Government funding of £1.43m to support the 4 hour standard had been confirmed for Pennine Lancashire. The Communications & Engagement Plan had been launched and daily teleconferences were taking place to monitor performance. Unscheduled Care Highlight Report The report provided a high level overview of current and planned work of the Pennine Lancashire Unscheduled Access & Flow Group, highlighting the position in respect of A&E Performance, Out of Hours Co-location BGH & RBH, Acute GP Visiting Scheme and the Early Action/Police A&E Liaison Role.
Primary Care :
Primary Care Foundation Support The proposal had previously been considered by the Remuneration Committee when Members requested confirmation from LDG members that the proposal represented value for money. Following discussion, Members agreed the proposal represented good value for money.
Medicines Optimisation :
Progress Report
Members received a detailed report outlining progress against the Medicines Management Work Plan, the Incentive Scheme and the Local Quality Premium Performance Prescribing Indicator. In collaboration with member practices, the work plan was on track to deliver the proposed £691,785 of efficiency savings. The CSU had been advised of the CCGs decision to transfer employment of the Medicines Management Team back to the CCG from April 2014, which was fully supported by Members.
Palliative Care Service Specification The aim of the service was to increase the availability of palliative care drugs to patients in East Lancashire and Blackburn with Darwen by improving access and continuity of supply, together with up to date information for patients, carers and healthcare professionals. Members supported the specification.
2.3 QUALITY & SAFETY COMMITTEE : 13 November & 11 December 2013 Chair - Jackie Hanson
The Committee discussed items relating to the following areas:
Page 5 of 6
a. Items requiring approval from the Governing Body: The 11 December meeting was not quorate and it was therefore necessary to obtain Governing Body approval in respect of the following two time critical items. CQUIN Update
Following discussion at previous Quality meetings with ELHT, tight deadlines had been set for the receipt of data, on the understanding that if not received, CQUIN payment would be withheld. Recovery plans had been put in place and ELHT had demonstrated increased levels of engagement and ownership of the CQUIN process, noting that compliance with data submission timescales had improved significantly, as had the quality of those submissions. Following discussion, members recommended full payment for Q1 and Q2 with the exception of Advancing Quality re Stroke. Payment would be released if stroke performance improved.
GB Decision : Members approved the proposal as outlined.
Financial Impact of Keogh
This item had been considered at the November and December QSC meetings. The level of external scrutiny on the Trust had incurred significant additional costs across a number of areas and it was therefore proposed that the CCG provide a non-recurrent contribution to support the cost of the Keogh work. Following discussion it was proposed to provide the additional funding on a 40:60 basis. The 40% payment would be made as soon as possible and the remaining 60% would be paid subject to a number of conditions being demonstrated.
GB Decision : Members agreed to support the proposal to pay 40% immediately and up to 60% being totally dependent on specific conditions being demonstrated, including reaching clinical targets.
b. Delegated decisions taken requiring ratification by the GB: None
c. Reporting on key decisions:
Stroke Performance
Members received an update following concerns regarding a drop in performance at ELHT, which confirmed that internal special measures had been introduced by the provider to improve performance and progress was being monitored. A number of actions were agreed and challenges would be put into the system to understand the clinical issues and pathways.
Soft Intelligence System
A system had been developed to enable the co-ordinated and systematic escalation of service concerns originating in General Practice or by members of the public in relation to commissioned services. Members received a presentation which provided an overview of the type of information being received, which was RAG rated and reviewed on a weekly basis to identify trends and escalate issues to the provider.
Risk Management
The Corporate Risk Register was received which outlined changes to the Register during October. There were currently twenty five risks on the Register, the management of which were regularly monitored and reviewed by the Risk Management Group.
Infection Control
The bi-monthly report provided an update in relation to healthcare acquired infections and the work ongoing to address the same. Q2 data indicated that five MRSA cases had been assigned to the CCG. CDiff data was below trajectory and the CCG continued to see a reduction on last year’s cases. A number of MSSA acute and non
Page 6 of 6
acute cases had been reported and a root cause analysis had been undertaken for each case. A high level meeting had taken place during November to adopt a health economy approach to infection control.
Serious Incident Reporting
The report provided a brief overview of the internal management of serious incidents, confirming the Lancashire CSU had been commissioned to undertake this role on behalf of the CCG.
Protocol for Quality Monitoring Provider Visits
A visiting programme was to be established which would provide the opportunity to review the quality of services within commissioned provider services and to explore the views of staff in respect of services provided. Proposals for visits during the 2013/14 contract were agreed and would take place both during the day and evenings.
Patient Insight Report
The report provided a summary of formal complaints, concerns and enquiries received relating to NHS services in the EL area.
Safeguarding Dashboard The report provided an overview of the quality issues within the safeguarding arrangements and highlighted key points
Locality Issues : Clitheroe Community Hospital Members were advised that GPs in the Ribblesdale locality provide medical cover in-hours at Clitheroe Hospital, traditionally looking after their own patients. Concerns were expressed that GPs were frequently asked to look after non RV patients, creating an increased workload and additional concerns as the GPs do not know the patient or their families. The complexity of patients being discharged had also increased and concerns had also been expressed by ELMS, as the Out of Hours provider. Work was ongoing with ELHT to address these issues.
2.4 REMUNERATION COMMITTEE : 16 December 2014 : Chair – Di van Ruitenbeek
The Remuneration Committee minutes will be received under Part 2 of the agenda.
2.5 LOCALITY STEERING GROUP SUMMARIES : Chair – GP Clinical Leads Locality summaries are attached at Appendix B.
3. STAKEHOLDER COMMITTEES
The following Stakeholder Committee minutes are attached at Appendix C for information. Pennine Lancashire Clinical Transformation Board : 4 December 2013 Health & Wellbeing Partnership : 25 November 2013 CCG Network : 31 October & 28 November 2013
4. Recommendations
Members are asked to: a. Ratify and endorse the delegated decisions taken by the Sub-Committees; b. Receive the monitoring information on key decisions; c. Be advised of the items of particular interest or risk. d. Receive the Stakeholder Committee minutes for information.
ANGELA BROWN Head of Corporate Affairs
Recommended

















