New insights for the management of refractory status epilepticus (RSE)
Yi-Chen Lai, M.D.Assistant Professor
Section of Pediatric Critical Care MedicineDepartment of Pediatrics
Baylor College of Medicine

Take home messages•Anesthetic infusions may be associated with worse outcome
•Ketogenic diet may improve seizure control in RSE
• IL-1 receptor antagonist may be beneficial in Febrile-illness related epilepsy syndrome (FIRES)

RSE remains to be a management challenge
•RSE: continuing seizures following 1st & 2nd
lines of anti-epileptic drugs (AED)•No clear recommendation for 3rd line treatment
• Additional intermittent AED• Continuous infusions• Immune modulating agents

Continuous infusions are associated with worse outcomes in adult RSE
Neurology 82:656-664, 2014

Continuous infusions are
associated with worse outcomes in
pediatric RSE
Gainza-Lein, M et al, AES abs# 2.202, 2017

Ketogenic diet improves seizure control in pediatric RSE
Epilepsy Res 144:1-6, 201871% response rate

Febrile-illness related epilepsy syndrome (FIRES)
•A clinical presentation, not a specific diagnosis •Occurs in a previously healthy child•Febrile illness preceding the RSE onset
• Between 2 wks and 24 hrs•Rapidly evolving seizures to prolonged RSE
Epilepsia 59:745-752, 2018

No effective treatments for FIRES
Epilepsia 59:745-752, 2018

Status epilepticus
Ý innate immunity (IL-1b, HMGB, microglia, TLR-4)
ß lower sz threshold
Ý seizures >
>>
>Infection

cytomegalovirus, Epstein–Barr virus, human herpesvirus 6,and CSF herpes simplex virus) and metabolic investigations(including CSF lactate, amino acids, and neurotransmitters)were negative. A comprehensive epilepsy genetics panel(GeneDx, Gaithersburg, MD) was negative, including forPCDH19, POLG, and SCN1A. An extensive serum andCSF autoimmune epilepsy evaluation was also negative,including for antibodies against N-methyl-D-aspartatereceptor, neuronal (V-G) K 1 channel, glutamic acid decar-boxylase 65, c-aminobutyric acidB receptor, and aminohy-droxy methylisoxazole propionic acid receptor (for com-plete list of antibodies tested see www.mayomedicallaboratories.com/test-catalog/Overview/61511). Neuroimaging was initially normal (3T brain mag-netic resonance imaging (MRI) venogram/angiogram (V/A);Fig 3A, C). Despite numerous antiepileptic drugs and a 3-day course of high-dose methylprednisolone, she continuedin super-RSE with a putative diagnosis of FIRES.
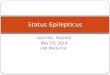
Anakinra Treatment Epoch #1 (Day 6–23)Anakinra commenced on day 6 at 5mg/kg twice daily(total 5 200 mg/day) via subcutaneous injections. After
the start of anakinra, the total number of daily seizuresdecreased from an average of 5.8 seizures/day (days 1–6)to 1.3 seizures/day (days 7–29; p 5 0.009, Mann–Whit-ney test), and her maximum hourly seizure burdendecreased from a mean of 10min/h (days 1–6) to0.75min/h (days 7–29; p< 0.001, Mann–Whitney test).The ketogenic diet was also started on day 6, althoughketosis was very difficult to achieve and her serum beta-hydroxybutyrate levels were not persistently >2mmol/l until day 47, despite aggressive efforts at maintaining a4:1 ratio.
This inability to sustain ketosis was multifactorialbut mostly attributable to developing a severe drug reac-tion with eosinophilia and systemic symptoms (day 22),during which time her survival became quite tenuous.Because the culprit was unclear, many medications werediscontinued including anakinra and phenobarbital (day23). She required prolonged extracorporeal membraneoxygenation support for severe bronchospasm beforeresuming conventional ventilation via her tracheostomytube, and remained seizure-free when cEEG was discon-tinued (day 30).
FIGURE 1: Daily electroencephalographic (EEG) seizure burden and treatment regimen (days 1–65 of pediatric intensive care unit[ICU] admission). Antiseizure medications were uptitrated rapidly to the following maximum daily doses: phenobarbital (20mg/kgbolus, then 5 mg/kg/day), lacosamide (15mg/kg/day), methylprednisolone (mp; 30mg/kg/day), topiramate (15mg/kg/day), propo-fol (60mg/kg/min), felbamate (83mg/kg/day), and ketamine (3mg/kg/h). The ketogenic diet was rapidly escalated to a 4:1 ratio(sustained ketosis was not achieved until day 47), and the patient was successfully weaned on day 98 (not shown). A midazolaminfusion commenced on day 1 (daily infusion rate ranged from 0.01 to 3 mg/kg/h), with a slow wean beginning on day 59 until itwas discontinued on day 88 (not shown). Medications not shown include brief unsuccessful trials of levetiracetam (days 1–5; max-imum 5 63mg/kg/day), fosphenytoin (days 1–2; maximum 5 20mg/kg/day), and ketamine (day 25; 1mg/kg/h). Propofol was usedbriefly to break clusters of seizures (days 2, 4, 8). Clonazepam was added on day 59 to help wean the patient off midazolam.cEEG 5 continuous electroencephalogram; DRESS 5 drug reaction with eosinophilia and systemic symptoms.
ANNALS of Neurology
940 Volume 80, No. 6
Exogenous IL-1ra improves seizure control in a child with FIRES
Ý Day 3 CSF cytokinesIL1-b 218 fg/mlIL-6 252 pg/mlIL-8 4523pg/ml
Ann Neurol 80:939-945, 2016

FIRES may be associated with functional IL-1ra
deficiency
Modified from: Ann Neurol 85:525-537, 2019
FIRES CSF
(pre Tx)
Ex v
ivo
IL-1
rece
ptor
act
ivity
ControlMedia
Control media + IL-1ra
Control CSF + IL-
1ra
FIRES CSF (post Tx)

Exogenous IL-1ra is safe and may be effective for treatment of FIRES
•25 children with FIRES•Median of 20 days to IL-1ra (Anakinra) initiation•No increased infection rate•3 children with drug rash with eosinophilia and systemic symptoms (DRESS)
•Of 15 with available seizure frequency data, 11 (73%) showed reduction in seizures

RSEMidazolam infusion
Pentobarbital infusion
Additional intermittent AED
Wean attempt 24-48 h following seizure control
Seizures recur
Resume pentobarbital infusion
Ketogenic diet
No
Yes
Is acute structural pathology the cause?
infectious autoimmune inflammatory (FIRES)
Manage 1o condition
steroid, IVIG, etcAnakinra
Recommended