The Real Heart of the Matter
Neurology NewsletterCOLLEGE OF MEDICINE
CALIFORNIA NORTHSTATE UNIVERSITY
June, 2016
From the President 1
Visions of Disease 2
Therapeutic Hypothermia in Stroke Management 3
The Heart and the Brain, CNU Edition 7
Vascular Dementia 8
Etanercept: An Alternative Treatment for Stroke 9
Letter From the Editor 10
From the President: TotheNeurites—CheerstoasuccessfulfirstyearoftheCNU-COMStudentInterestGroupinNeurology.Thesenewsletters,ourinau-guralBrainDayandallthearticlesandstudieswehaveswappedsincethegroup’sinceptionareatestamenttoyourdedicationtoourinterestinneuroscienceandtheschool’sreputationinthebroadermedicalcom-munityandourown.Isincerelythankyouall. Iwouldnowliketoinviteourreaderstoenjoyourlastnewsletteroftheschoolyear,beforeourSIGNpartswaysfortwomonthstoen-joytheproverbial“lastsummer”ofmedicalschool.Becauseweareinthecardiologyblock,thethemeofthisissueisonthecerebrovascula-ture.AsaPhDstudentinthelabofaneurosurgeonwhospecializedintreatingskull-baseaneurysms(areasofweaknesswithinthewallofanarteryleadingtoaballooningeffectandmakingthearterymorepronetoseriousrupture),Icametoappreciatethecomplexityofthissystem.Hewouldfamouslyremark,atleasttomyawe-inspiredears,thatIcouldtakethecerebrovasculaturefromLomaLindatoSanFrancisco—all500milesofit.Well,hereIam—prettyclose,sothankyouDr.WolffKirsch.Healsosuggestedtomethatthesmoothmusclecellsthatmakeupthewallsofthearterialsystemofthebrainareprobablysmarterthantheneuronsthatdoourthinkingandthatwhenthosesmoothmusclecellsaredestroyed,thebrain—anditsneurons—shrinkunderthecrushingpressureofdementia.Fittinglythen,SalilBabbarhasprovidedyouwithanarticleonthespecificsofVasculardementia—anentitysimilartoandatonetimecomparedtoAlzheimer’sdisease.MohammadAzizhasad-ditionallycontributedanarticleonthecontroversialeffectsofhypother-miatreatmentonstrokeoutcomeswithcommentarybyDr.ForshingLui.Lastly,NancyLihasgracedyouagainwithahumorous“neurocomic”,
Page 1

“Vascular dementia is easily preventable if
detected and diagnosed early on, so it’s essential
for clinicians to be able to recognize all the various signs and symptoms of
the disease.“
Page 2
thistimefeaturingTheHeart,andArleenGrewalhaswrittenabeautifulpoemforyourreadingenjoyment. Toclose,IwouldliketothankTrevorTsayfortakingthetimetoformatthesenewsletters—itcouldnotbedonewithouthisefforts.Addi-tionally,thankyoutoourFacultyAdvisor,Dr.ForshingLuiforhissupportandcontributions.Finally,aspecialthanksgoesouttoourreadersandsupportersoutsideoftheSIGN.Wehopeyouenjoyedthefirstiterationofthisepicjourneyweasmedicalstudentshavestarted.Startinginthefallof2016,wewillintroducetoyouanewcropofbuddingneuriteswithourupcomingclassof2020.Fornow,pleaseenjoythisissueofTheNewsletter,courtesyoftheCNUCOMSIGN.
-MatthewZabelPresident,CNUSIGN
visions of diseaseAnx-ray,culture,CT,evenMRI,Allofthesehinttowhere,how,andwhatwentawry.Isithisnose,theleftear,orwasitmid-thigh?Nono,itwasTrachomathatlefthimone-eyed.
ButwhatifIclaimedasimplepaintingbyyou,Couldunveilthewickedplightsofyourvisiontoo?Yousee,thecanvasmaymirroryourtaintedview,Andthereby,ohsoniftilyofferaclue. AFrenchimpressionist,ClaudeMonetwashisname.Sublimedepictionsoflightgavebirthtohisfame.Inhislateseventhdecade,not-so-goodnewscame:“Bilateralcataracts,”thedoctorclaimed.
Farlessvibrant,hispiecesmutedincolor.Hethenwrote“[I]seeacompletefog,”asitwere.Cataractsabsorblightandtodayweinfer,Theystaintheworldwithyellowsandredsinablur.
Fromblue-greentored-yellow,hispaletteshifted.Redsposedasmuddypinks,hecouldnotresistit.Nextenvisionyoursightandmind,too,havedrifted.ThatwhenDoctorsaid“Alzheimer’s,”yourhearttwisted.
ThatwasthefateofoneAmericanartist.WilliamUtermohlen,thoughnotanarcist,Offeredapeakintohismindatitsdarkest,Bypaintingself-portraitsthatslowlylostsharpness.
-Matthew ZabelMS1, CNUCOMPresident, CNU SIGN

Page 3
Diagnosedin’95,atage61.DemiseofWill’sperceptionofdepthhadbegun.Hepaintedforfouryears,loungingunderoursun.Inhislastsevenitcouldnolongerbedone.
Borninthe1830sinParisonenightWasEdgarDegas,wholostdefined,centralsight.Ascotoma,littlebylittlegainedinmight.Ageanddrusenstolehismaculaincoldspite.
Aremarkablepainter,helearnedtoadapt—Replacedoilpaintswithpastelstofeellesstrapped.ThoughnotaMichelangelo,I,too,infactHouseophthalmicmaladiesandacataract.
Atage17,myrighteyenearlywentblind.Butenoughaboutme,fastforwardtorealtime.Tohowexquisitely60livesintertwine,Liketreerootsdrawingclosetogetherinsunshine.
Thankthecolorsandlinesandshapesthatyoucansee.AndCNU,ourhome,wherewe’rehumbledtobe.Reflectingonourgoodgraceeachdayiskey.Forthesepeople,places,andlifewon’talwaysbe.
-Writtenby:ArleenGrewal
-Arleen GrewalMS1, CNUCOM
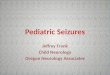
Claude Monet painted “Waterlilly Pond,” in 1899. His vision problems
with cataracts didn’t begin until 1912.
A recent photograph of the bridge.
Current photograph of the same bridge, blurred as it might appear to someone with a moderate cataract.
Details from William Utermohlen’s self-por-traits, the first, made in 1967, the rest from 1996 the year following his diagnosis of Alzheimer’s disease, to 2000, charting his decline. Courtesy of the artist’s estate and GVArt Gallery, London
Oil paint; Dance Class at the Opera, 1872 by Edgar Degas.
Pastels; Ballet Dancers in the Wings, 1900 by Edgar Degas

“Stroke is the fifth lead-ing cause of death in the United States account-ing for one in every 20
deaths. ”
“Two randomized con-trolled trials published in the New England Jour-nal of Medicine in 2002 showed neuroprotective effects of therapeutic
hypothermia”
Page 4
Therapeutic Hypothermia in Stroke Management
StrokeisthefifthleadingcauseofdeathintheUnitedStatesaccountingforoneinevery20deaths.Thevastmajorityofstrokesareischemic(87%)andtheirmanagementrangesfromthrombolyticthera-pytosymptomaticmanagement.Therapyisdirectedatreducingneurondeathduetoischemiaorsubsequentreperfusion.Anewerapproachtocombattingneuronallossistherapeutichypothermia.Therapeutichy-pothermiahasbeenimplementedintothestandardofcareforcardiacarrestpatientsbytheAmericanHeartAssociation,however,itsuseinstrokemanagementremainsmuchmorecontroversial. Cardiacarrestresultsinglobalcerebralischemiaandchancesofreperfusioninjuryareimplicatedinneurologicaldecline.Tworandom-izedcontrolledtrialspublishedintheNewEnglandJournalofMedicinein2002showedneuroprotectiveeffectsoftherapeutichypothermia(32oC-34oC)incomatosepatientsafterout-of-hospitalventricularfibril-lationcardiacarrestwithin2hoursofreturnofspontaneouscirculationandmaintainedfor12-24hours(Kirkmanetal.,2014).Conversely,acuteischemicstrokedoesnotalwaysresultinglobalcerebralisch-emia.Localizedbraininfarctsmaybenefitfromtherapeutichypothermiaattheriskofcompromisingmetabolismincompetentregions.Further-more,returnofcirculationfollowingcardiacarrestistypicallyassociatedwithaccompanyingcerebralreperfusion.Instroke,theaffectedvesselmayremainoccludedfordays,orindefinitely,whichenhancesthesideeffectsofcoolingonotherpartsofthebody.Lastly,unlikecardiacarrestpatients,thoseundergoingacuteischemicstrokearenotusuallycoma-toseorendotracheallyintubatedandriskofshiveringandotherdiscom-fortpresentsanotherchallengefortreatment(Midorietal.,2010).Giventhesetrade-offs,currentclinicalapplicationtakesadvantageofthera-peutichypothermiainsymptomaticmanagementtolowerintracranialpressureandhypertensionwhileclinicaltrialsaregearedatoptimizingprotocolstoextractthemosttherapeuticbenefit. Themechanismsunderlyingtheneuroprotectiveeffectsofther-apeutichypothermiainstrokemanagement,aswellasitsassociatedcomplicationsandproposedmethodsofaccomplishingoptimumtherapywillbediscussedherein.Injury Following an ischemic event Adequatebloodflowdeliversoxygenandglucosetothebraininordertomaintainitsnormalfunction.Normalfunctionrequirestheinteg-rityofionicgradientsmaintainedbytransmembranechannels.Followinganacuteischemicevent,ionichomeostasisisdisrupted,whichleadstoaninfluxofcalciumandtheexcitatoryneurotransmitter,glutamate.Glutamateinducedexcitotoxicityleadstogenerationofreactiveoxygenspecies(ROS)andnitricoxide(NO)thatinduceapoptosisbydamagingcellstructures.Progressivecelldamageleadstodissipationofiongradi-entsestablishedacrossthecellmembrane,whichfurthercontributestoosmoticchangesthatresultincerebraledema.
-Mohammad AzizMS1, CNUCOM

“A 1o C drop in body tem-perature translates into a 6%-7% reduction in
cerebral metabolic rate ”
Neuroprotective Effects,A Multi-pronged Ap-
proach:
1) Decreasing cerebral metabolic demand
2) Modulatory on Glutumate
3) Inhibit Mitochondrial Apoptosis
4) Decrease Reperfusion Injury
Page 5
Cerebraledemacanprogresstoincreasedintracranialpressure(ICP)whichthreatenstocompressvitalstructuresandeventuallyher-niate.Inaddition,anoxiacausesmetabolicalterationswithelevatedlactateleadingtoacidosis.Thelocationandextentofthesechangesaredependentonthenatureofischemiawhichincludeslocation,metabolicdemandandlevelofcollateralbloodsupply.Neuroprotective effects of Hypothermia Cerebralmetabolicrateisdependentontemperature.A1o C dropinbodytemperaturetranslatesintoa6%-7%reductionincerebralmetabolicrate(Polderman,2009).Decreasingcerebralmetabolicratereducesutilizationofoxygenandglucose.Thislessenstheextentofanoxicinjuryfrommetabolicacidosisandlessexcitotoxicitybyloweringmetabolicdemand.Inadditiontoitseffectsintheimmediatestagesofacutestoke,therapeutichypothermiacanlowertheriskofreperfusioninjurybydecreasinginflammationcausedbytheresurgenceinbloodflow. Inearlyglutamateinducedexcitotoxicity,thereisaprotectivefunctionservedbynearbyastrocyteswhichuptakeglutamateviatheGLT-1transporter.Inprolongedischemia,however,thisfunctionrevers-esasinjurytoastrocytesbecomesmorepronounced.TheregurgitationofglutamateunleashesaheavyburdenontheneuronresultinginapotentinflammatoryresponsewithmoreROSrelease.Onelaborato-rystudyshowedareductioninNMDAreceptorphosphorylationandincreaseinGLT-1transporterinastrocytesinnewbornpigletswithinducedhypoxic-ischemicinjuryfollowedbytherapeutichypothermia(Wangetal.,2013). Therapeutichypothermiahasalsobeenshowntoinhibitintrinsic(mitochondrialbased)apoptosisbyloweringpro-apoptoticBCL-2fam-ilymemberssuchasBCL-2associatedX(BAX)andupregulatingan-ti-apoptoticproteinBcl-2,inhibitingcytochromecreleaseandcaspaseactivation(Fukudaetal.,2001,Phanithietal.,2000,Yenarietal.,2002andZhangetal.,2001).Furthermore,thetherapycanpreventendo-plasmicreticulumstressapoptosisthroughsuppressingC-EBP-homolo-gousprotein(CHOP)(Liuetal.,2013). Reperfusionmediatesinjurythroughprovidingoxygenforpro-ox-idantenzymessuchasNADPHoxidasetochurnoutmoreROS(Tangetal.,2011).Thisleadstodisruptionsinthebloodbrainbarrierwhichcanleadtohemorrhage.Hypothermiacanreducethisinflammationandlowertheriskofhemorrhage. Thereareothermechanismsofneuroprotectionmediatedbytherapeutichypothermiathataidneuronalrecoverypostischemia.Theselargelystemfromthepreservationofneuronalfunctionduringtheinitialischemicinsultbypacifyingtheinflammatoryresponseandlimitingdamagetothebraininfrastructure.Complications Thereareconsequencestodepressingthebody’snaturalinflam-matoryresponse;mainlyapropensityfordevelopinginfection.Uptoonethirdofischemicstrokepatientsdevelopinfection(Emsleyand

“There are consequences to depressing the body’s natural inflammatory re-sponse; mainly a propen-sity for developing infec-tion. Up to one third of ischemic stroke patients
develop infection”
“Therapeutic Hypother-mia is a controversial
intervention in the man-agement of acute ischemic stroke... Going forward, research is increasingly
directed towards clinical practice in order to attain
the greatest efficacy of treatment.”
Page 6
Hopkins,2008andMeiseletal.,2005).Asbodytemperatureisloweredto32oC,heartrateisloweredto40-45beats/min(BernardandBuist,2003,DeGeorgiaetal.,2004andStaikouetal.,2011).Cardiaccompli-cationsduetodecreasedheartrateincludeloweredmeanarterialpres-sureandcardiacoutput,arrhythmiasandmyocardialinfarction.Hema-tologically,thecoagulationcascadeisinducedintemperatureslessthan35oC(Polderman,2009).Thisischallengingconsideringstrokeitselfisacoagulation-fibrinolysisdisorder.Othercomplicationsincludeelectro-lytedisorder,hyperglycemia,insulinresistance,colddiuresis,andboweldisorders(Ziplingetal.,2015).Methods of Inducing hypothermia Unliketherapeutichypothermiaforcardiacarrest,therearenosetguidelinesforitsuseinthemanagementofacutestroke.Implementa-tioniscase-dependentandclinicaloutcomeshavenotbeenconsistent.Muchconsiderationisneededtodeterminethetemperatureatwhichtoinducehypothermiaandthedurationoftherapy.Earlyhypothermiawithalongercourseistypicallyassociatedwithbetteroutcomes.Mostinter-ventionshoverintheneighborhoodof32oC-35oC(Ziplingetal.,2015).Rewarmingisperformedslowly,payingcloseattentiontomarkerslikeintracranialpressure.Intermsoflocation,therapycanbelocalizedtothebrainortheentirebody.Optionsareavailableforintra-arterialcoolingandpharmacologicalcoolingaswell.Conclusion TherapeuticHypothermiaisacontroversialinterventioninthemanagementofacuteischemicstroke.Laboratorystudieswithanimalshaveproducedmuchmorepromisingresultsthanclinicalapplication.Currently,ithasbeenusedinconjunctionwithothertacticslikethrombo-lytics,mechanicalthrombectomy,hemicraniectomy,andotherpharma-cologicaltherapytolimitbraininjury.Goingforward,researchisincreas-inglydirectedtowardsclinicalpracticeinordertoattainthegreatestefficacyoftreatment.
-MohammadAziz
References D.Wang,Y.Zhao,Y.Zhang,T.Zhang,X.Shang,J.Wang,Y.Liu,Q.Kong,B.Sun,L.Mu,X.Liu,G.Wang,H.Li.Hypothermiaprotectsagainstoxygen-glucosedeprivation-inducedneuronalinju-rybydown-regulatingthereversetransportofglutamatebyastrocytesasmediatedbyneurons.Neuroscience,237(2013),pp.130–138
MatthewA.Kirkman,MartinSmith,Therapeutichypothermiaandacutebraininjury,Anaesthesia&IntensiveCareMedicine,Volume15,Issue4,April2014,Pages171-175,ISSN1472-0299,http://dx.doi.org/10.1016/j.mpaic.2014.01.021.
YenariMA,HemmenTM.TherapeuticHypotermiaforbrainischemia.Wherehavewecomeandwheredowego?Stroke2010;41(Suppl1):572-74.
Allothercitationsprovidedarefromthisreviewarticle:
ZipingHan,XiangrongLiu,YuminLuo,XunmingJi,Therapeutichypothermiaforstroke:Wheretogo?,ExperimentalNeurology,Volume272,October2015,Pages67-77,ISSN0014-4886,http://dx.doi.org/10.1016/j.expneurol.2015.06.006.

Page 7
-Nancy LiMS1, CNUCOM
The hearT & The Brain
CnU ediTion

“Vascular dementia still remains the second most common cause of demen-
tia amongst elderly in the US and Europe, and the most common form of dementia in some parts of
Asia”
“The 5-year survival rate is 39% for patients with vascular dementia compared with 75% for age-matched controls.”
“Vascular dementia, which is the result of
multiple arterial infarcts and/or chronic ischemia, is the step-wise decline
in cognitive ability with late-onset memory impair-
ment.“
Page 8
Vascular Dementia Whenpeopleheartheword“dementia”theyusuallythinkaboutAlzheimer’sDisease(AD).However,vasculardementiastillremainsthesecondmostcommoncauseofdementiaamongstelderlyintheUSandEurope,andthemostcommonformofdementiainsomepartsofAsia.TheprevalencerateinWesterncountriesisabout1.5%anditaccountsforabout20%ofdementiacasesintheUS.Inpatientswithdementiawhohavehadastroke,theincreaseinmortalityisprofound.The5-yearsurvivalrateis39%forpatientswithvasculardementiacomparedwith75%forage-matchedcontrols.Vasculardementiaiseasilypreventableifdetectedanddiagnosedearlyon,soit’sessentialforclinicianstobeabletorecognizeallthevarioussignsandsymptomsofthedisease. Currently,manysubtypesofvasculardementiahavebeenidentified.Theseformsincludemildvascularcognitiveimpairment,multi-infarctdementia,vasculardementiaduetoastrategicsinglein-farct,vasculardementiaduetolacunarlesions,vasculardementiaduetohemorrhagiclesions,subcorticalvasculardementia,andmixedde-mentia(combinationofADandvasculardementia).Vasculardementia,whichistheresultofmultiplearterialinfarctsand/orchronicischemia,isthestep-wisedeclineincognitiveabilitywithlate-onsetmemoryimpair-ment.Injuriesaccumulateinastepwisemannerwitheveryminorstrokethatoccurs.Mostinfarctsareduetotheformationofathrombusattheparticularsiteofinjuryorathromboembolismmovingtothesiteofinjuryfromadifferentlocation.AnMRIorCTofapersonwithvasculardemen-tiawillshowmultiplecorticaland/orsubcorticalinfarcts,soperforminganMRIorCTisessentialtoconfirmthediagnosis. Inadditiontocognitivedecline,patientswithvasculardementiamayhaveaccompanyingmotororsensorysymptoms,dependingonwheretheinfarctoccursinthebrain.Mostofthetimetheseinfarctsoccurintheparietallobe,cingulategyrus,andotherareasofthebrainsuppliedbytheanteriorcerebralartery.Damagetothecingulategy-rusresultsinchangesinemotionalstate,long-termmemoryformation,olfaction,behavior,andautonomicnervoussystemfunction.Anteriorcerebralarterystrokesoftenresultincontralateralparalysisandsensorylossofthelowerlimbsasitsuppliesthelowerlimbsectionsoftheprima-rymotorcortex(frontallobe)andprimarysomatosensorycortex(pari-etallobe).Vasculardementiacanalsobetriggeredbycerebralamyloidangiopathy,whichinvolvestheaccumulationofbetaamyloidplaquesinthewallsofthecerebralarteries,leadingtothebreakdownandruptureofthesearteries. Ischemicdamageisoftenpermanent,sopreventionoffuturestrokesisveryimportantforpatientsatriskforvasculardementia.Thebestwaytoavoidastrokeisbyloweringhypertension,hyperlipidemia,atrialfibrillation,andmaintainingbloodglucoselevelsinpatientswithdi-abetesmellitus,allofwhicharemajorriskfactorsforstroke.Allofthesefactorsaremajorriskfactorsforstroke.Whenitcomestomedication,aspirinandotherantiplateletagentsliketiclopidineandclopidogrelareusefulinpreventtheformationofnewthrombiandemboli.Forpatientswithatrialfibrillation,whichisanabnormalheartrhythmcharacterizedby
-Salil BabbarMS1, CNUCOM

“Vascular dementia is easily preventable if
detected and diagnosed early on, so it’s essential
for clinicians to be able to recognize all the various signs and symptoms of
the disease.“
Page 9
rapidandirregularbeating,anticoagulationtherapiessuchaswarfarinaremoreeffectiveatpreventingfuturestrokes.Patientswithhyperten-sioncantakeACEinhibitors,Ca2+channelblockers,thiazidediuretics,orβ-blockerstolowertheirbloodpressure,whichwoulddecreasetheirchancesofformingathromboembolism.Additionally,statinshavebeenfoundtoreducetheriskofstrokeinpatientswithcoronaryarterydiseaseandelevatedtotalorlow-densitylipoprotein(LDL)cholesterol. Asthe“babyboomer”generationgetsolder,thenumberofse-niorsages65andolderintheUnitedStatesisexpectedtomorethandoublefrom39millionto89millionin2050.Withthisfactinmind,it’simportantforallfuturephysicians,includinginternists,neurologists,andcardiologiststobeabletorecognizetheearlysignsandsymptomsofvasculardementiainordertoavoidpermanentbraindamageandanearlydeath.Notonlydoesvasculardementiaimpactthepatient,butithasramificationsonthefamilymemberswhotakecareofthatpatient.Thus,everyphysicianneedstobeabletotakeathoroughmedicalhistory(includingfamilyhistoryofdementia),evaluatethepatient’sdailyactivities,obtaininputfromarelativeortrustedfriendofthepatient.Whileathoroughhistoryisimportant,acomprehensiveneurologicalexamisjustasimportantinconjunctionwiththecorrectlaboratorytestsandbrainimaginglikeMRIorCTscans.
-SalilBabbarReferences:Alagiakrishnan,K.,MD.(2015,January12).VascularDementia.RetrievedApril20,2016,fromhttp://emedicine.medscape.com/article/292105-overview#a4
Baskys,A.,&Hou,A.C.(2007).Vasculardementia:Pharmacologicaltreatmentapproachesandperspectives.ClinicalInterventionsinAging,2(3),327–335.
Iemolo,F.,Duro,G.,Rizzo,C.,Castiglia,L.,Hachinski,V.,&Caruso,C.(2009).Pathophysiologyofvasculardementia.Immunity&Ageing:I&A,6,13.http://doi.org/10.1186/1742-4933-6-13
McVeigh,C.,&Passmore,P.(2006).Vasculardementia:preventionandtreatment.ClinicalInter-ventionsinAging,1(3),229–235.
Shelat,A.,DO.(2015,February3).VascularDementia.RetrievedApril20,2016,fromhttps://www.nlm.nih.gov/medlineplus/ency/article/000746.htm
Strub,R.L.(2003).VascularDementia.TheOchsnerJournal,5(1),40–43.
Etanercept: an alternative treatment FOR stroke
InresponsetothearticlepublishedinthisissuebyMohammadAziz,Ihavetopointoutthatresearchershavetriedtostudydifferent“neuroprotective”strategiesforacutestroketreatment.Manyoftheseappearedtobepromisinginin-vitroandanimalstudies.Unfortunatelynone,Iliterallymean“none”hasbeenshowntobebeneficialinclinicalpractice.Thebestmeasurerightnowisstillthe“timeisbrain”concept.Theearlierandmorecompleteonemayopenablockedartery,thebet-tertheoutcomeingeneralhelpedbymodernand“bestsupportiveandnursingcare”. Inflammationhasbeenseenandmayplayanimportantroleinacuteischemicstroke.TNF-alphaisthe“masterregulator”oftheinflam-matory(immune)responseinmanyorgansystems.Autoimmune

Page 10
diseasesarecausedbyanoveractiveimmuneresponse.Etanercept(Enbrel)hasbeenshownandapprovedbyFDAtotreatthesediseasesbyinhibitingTNF-alpha.Thesediseasesincluderheumatoidarthritis,psoriaticarthritisandankylosingspondylitis.Someauthorshypothesizedthattumornecrosisfactor(TNF)mayplayasignificantroleintheme-diationofinflammatorychangesinbrainischemia.Therewereactuallyanumberofstudiespublishedshowingsomeefficacy.TheAmericanAcademyofNeurology(AAN)reviewedtheevidenceofthedataandreleasedareportthisweek. Thefinalconclusionis:Forpatientswithpoststrokedisability,theevidenceisINSUFFICIENTtosupportorrefuteabenefitofEtanerceptforthetreatmentofpoststrokedisability(ClassIVevidenceandlevelUrecommendation). PersonallyIbelieveitisanotherneuroprotectiveagentforstrokethatwillbeforgottenveryquicklybystrokeneurologists.
-ForshingLuiMDReferences:GronsethGSandMesseSR.Practiceadvisory:Etanerceptforpoststrokedisability.ReportoftheGuidelineDevelopment,Dissemination,andImplementationSubcommitteeoftheAAN.Neurolo-gyJune7,2016;86(23):2208-2211
Letter from the editorReadersofNeuroNewsletter, Iwouldliketopersonallyandsincerelythankyouforyourtimereadingthewonderfulnewsletteryouhavebeforeyou.WeweregladtosharewithyouNeuroNewsletters’educationalandentertainingcontent.Thisisourlastnewsletterfortheinaugural2015-2016schoolyear.WewillberestartingthenewsletterinSeptember,2016,andhopefullyshow-casepiecesfromournewclassof2020! Iwouldalsoliketothankthewritersthathavesubmittedanarticleforournewsletter.Itgoeswithoutsayingthatnoneofthiswouldhavebeenpossiblewithoutyourcontributions.Myhopeisthatthisexpe-riencehasbeenbothadevelopingadventureaswellasavehicletodisplayyourwonderfulwritingability.Ifirmlybelievethatthepeoplewhohavesentinarticlesarewellontheirwaytobecomingtalentedwriters,andviatheirstoriesoursocietywillfurtherprogresstoshedlightontheunknown. Theyearof2016bringswithitthestartofthesecondyearofourinauguralclasshereatCaliforniaNorthstateUniveristy,CollegeofMedi-cine,andwithitweareonestepfurtherinourpersonaldevelopmentasphysicians.Ourholisticapproachseekstoadvancenotonlyourmed-icalknowledge,butalsoourpersonality,perspective,andouraptitudeforlife-longlearning.Awonderfulmentorhasoncetoldme,“IfIhadtonameonethingthatmakesagoodphysician...itwouldbetohaveaninquisitivemind...tohaveaninsatiablethirstforknowledge,andperpet-uallyworktoseekoutanswers.”Ihopethatwe,asfuturephysicians,cantakethistoheart,andNeuroNewslettercanbeasmallcoginthemachineaswebecomethebestcitizensonearththatwecanbe.
-TrevorTsay
Neurology Newsletter, a monthly newsletter published by students in the Student Interest Group in Neurology (SIGN) at California Northstate University, College of Medicine (CNUCOM) is meant to bring abreast information in the ever changing field of neuroscience to ultimately provide our patients with excellent medical care and top-notch patient education. Our website can be found at http://cnu-comorgs.wix.com/student-groups . All correspondence should be e-mailed to [email protected]. Chief Editor: Trevor Joel TsayAssistant Editor: Rainy Dae ZhangFaculty Advisor: For-Shing Lui, MD, MRCP(UK), FRCP(Edinburg)
Recommended