Neuroanatomy and
Neurophysiology
Sensory Motor• Afferent
• Vision• Kinesthesia• Olfaction• Hearing• Taste• Pain• Temperature• Touch• Balance
• Efferent• Glands• Muscle• Organs
• Circulation• Digestion• Respiration• Excretion• Reproduction
,Viscera
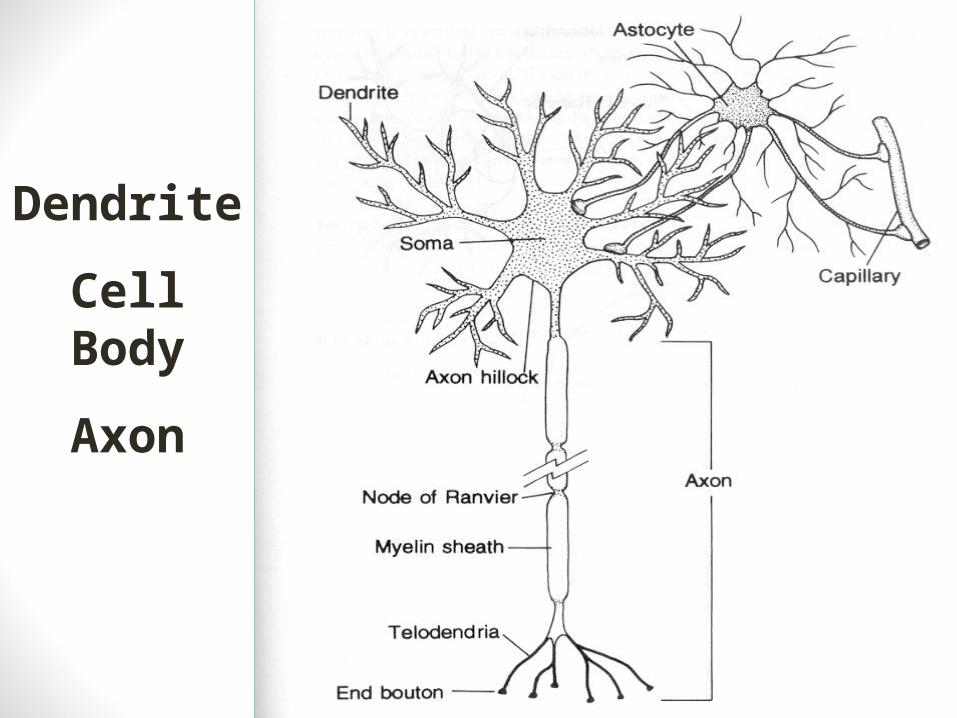
Dendrite
Cell Body
Axon
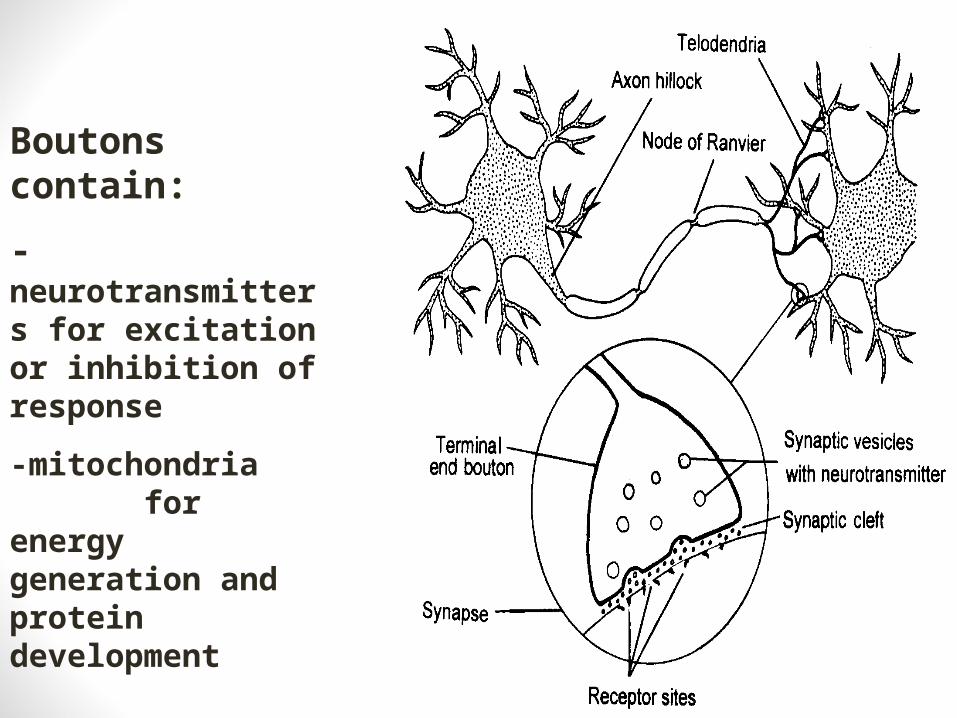
Boutons contain:
-neurotransmitters for excitation or inhibition of response
-mitochondria for energy generation and protein development
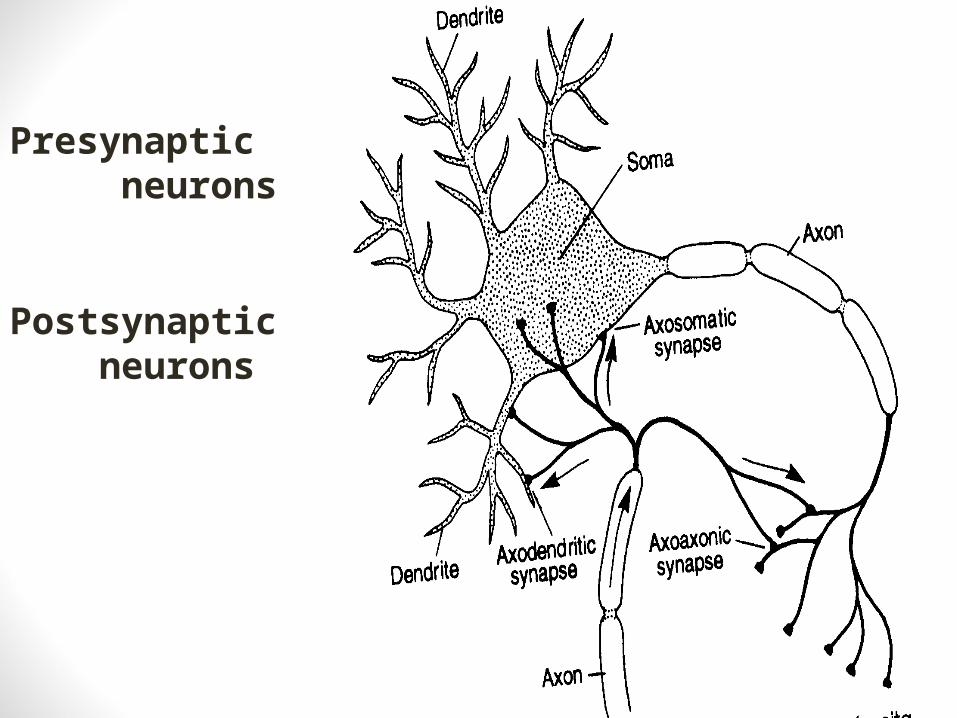
Presynaptic neurons
Postsynaptic neurons
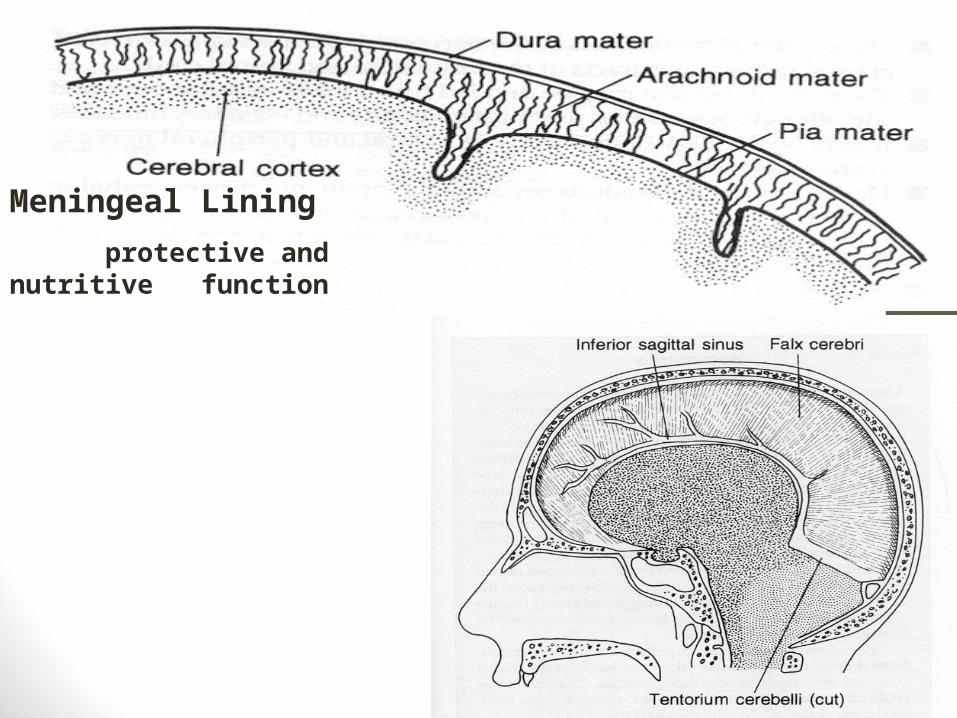
Meningeal Lining
protective and nutritive function
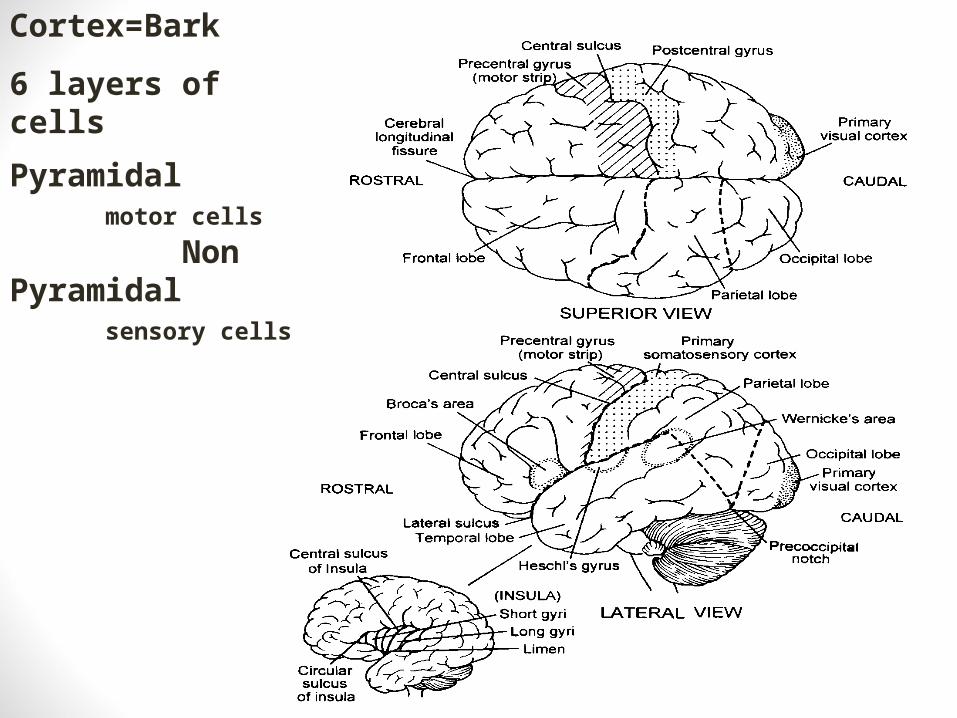
Cortex=Bark
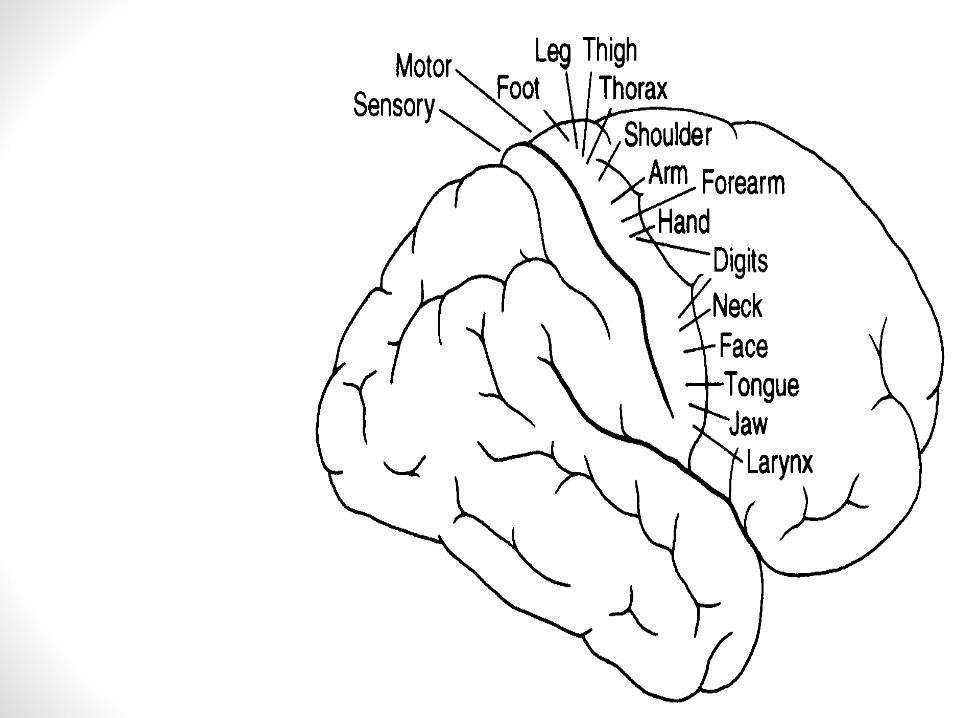
6 layers of cells
Pyramidal motor cells
Non Pyramidal sensory cells
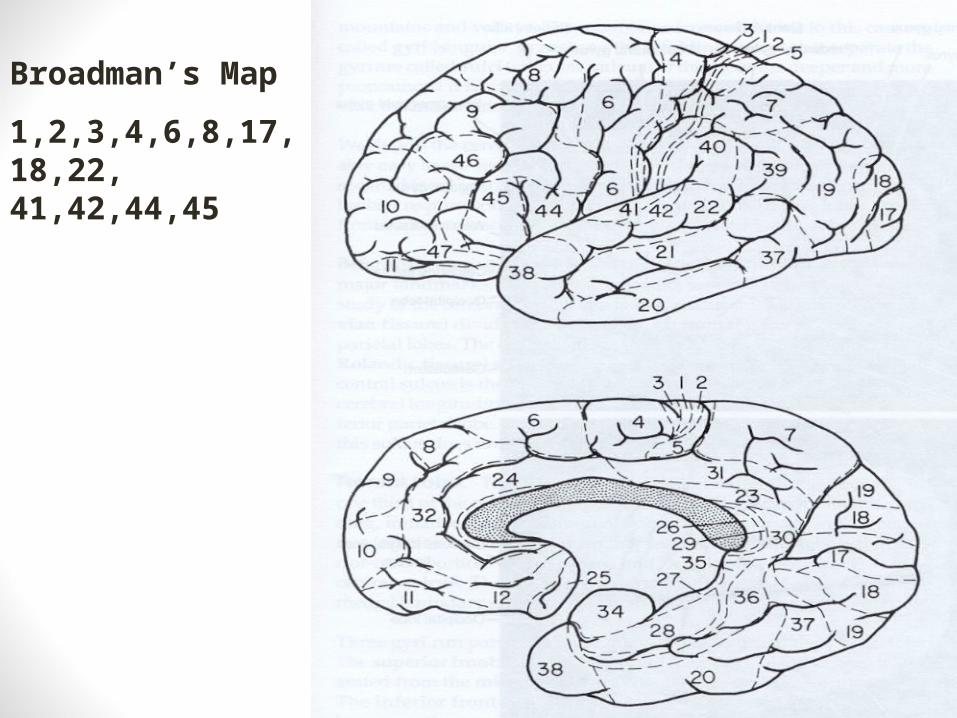
Broadman’s Map
1,2,3,4,6,8,17,18,22, 41,42,44,45
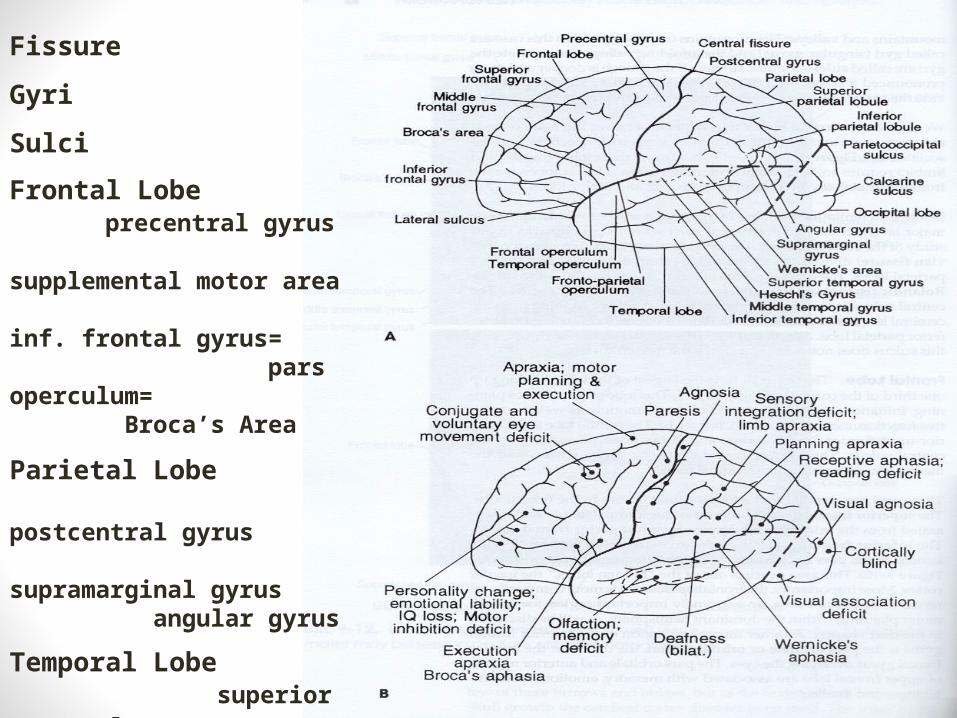
Fissure
Gyri
Sulci
Frontal Lobe precentral gyrus supplemental motor area inf. frontal gyrus= pars operculum= Broca’s Area
Parietal Lobe postcentral gyrus supramarginal gyrus angular gyrus
Temporal Lobe superior temporal gyrus
Heschl’s Gyrus Wernicke’s Area
Occipital Lobe calcarine sulcus
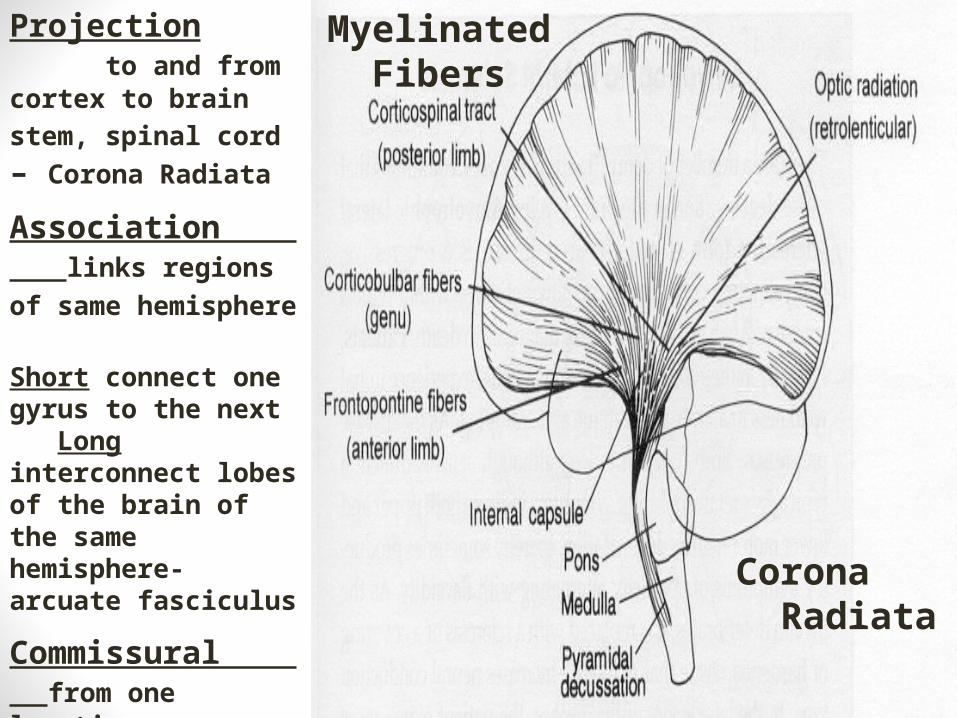
Corona Radiata
Myelinated Fibers
Projection to and from cortex to
brain stem, spinal cord – Corona Radiata
Association links regions of same
hemisphere Short connect one gyrus to the next Long interconnect lobes of the brain of the same hemisphere- arcuate fasciculus
Commissural from one location on one hemisphere to the corresponding location in the other –corpus callosum
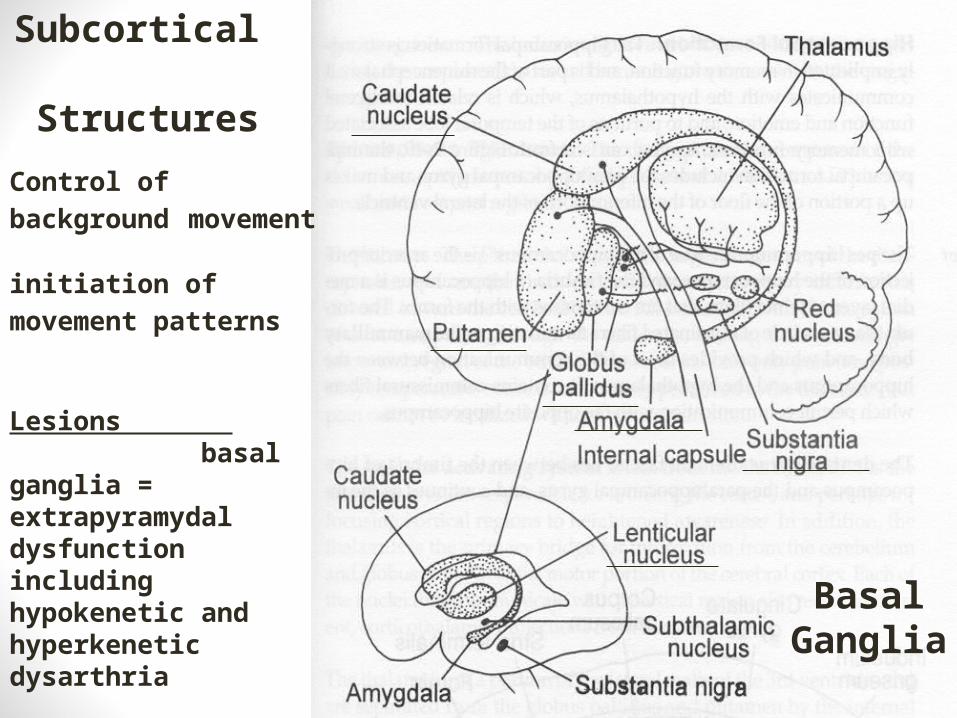
Subcortical Structures
Basal Ganglia
Control of background movement initiation of movement
patterns
Lesions basal ganglia = extrapyramydal dysfunction including hypokenetic and hyperkenetic dysarthria
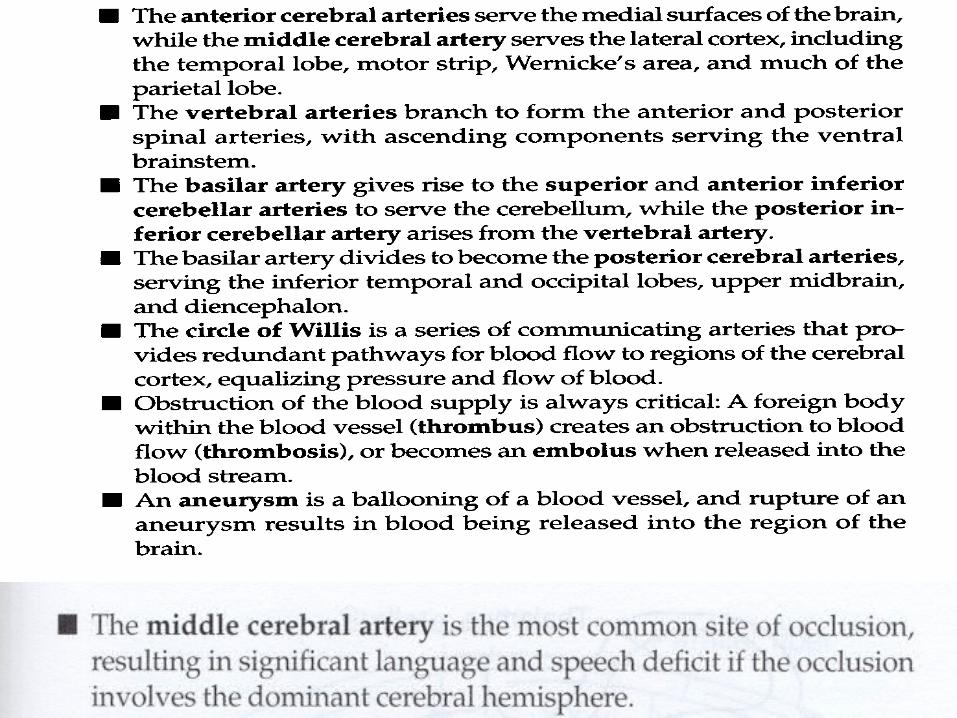
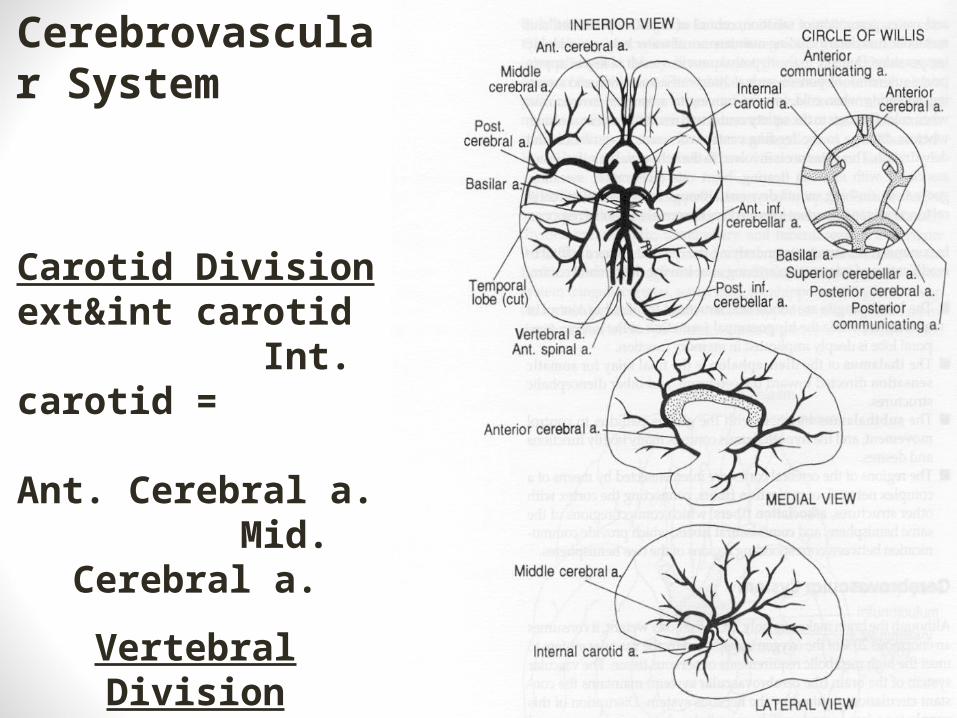
Cerebrovascular System
Carotid Division ext&int carotid Int. carotid = Ant. Cerebral a. Mid. Cerebral
a.
Vertebral Division ant&post spinal a.
basilar arteries = sup/ant cerebellar a. post cerebral a.
Cerebralvascular Obstruction• Thrombosis is a stationary obstruction• Embolus is a traveling clot that obstructs• Aneurysm is a dilation or ballooning of a vessel wall which can
cause a rupture into surrounding space• Congenital, AVM• Trauma• CVA, TIA
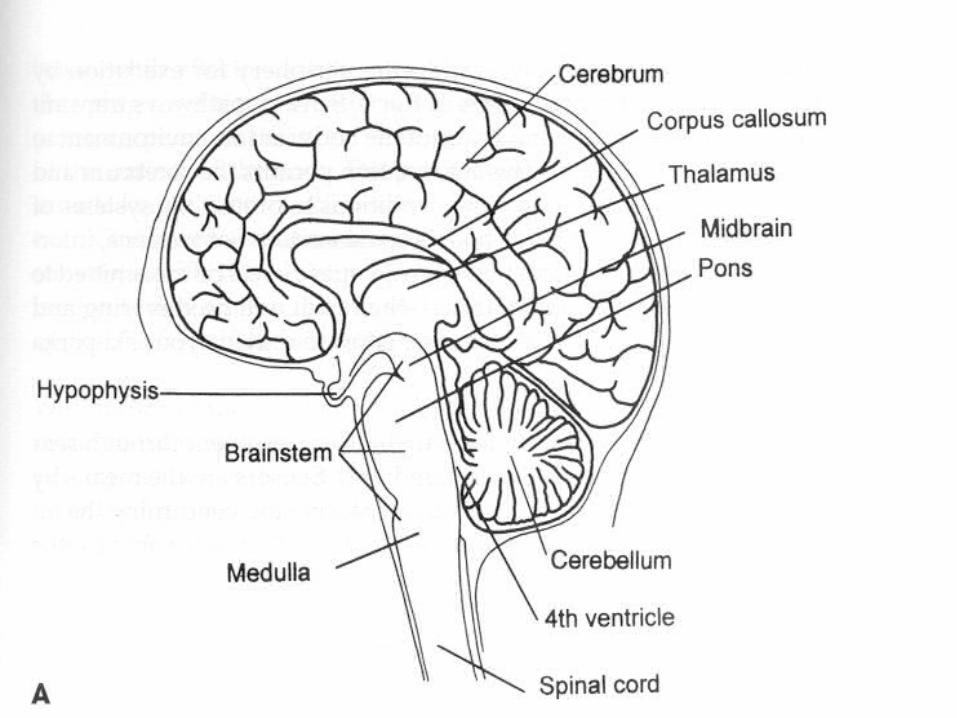
Anatomy of the Brainstem
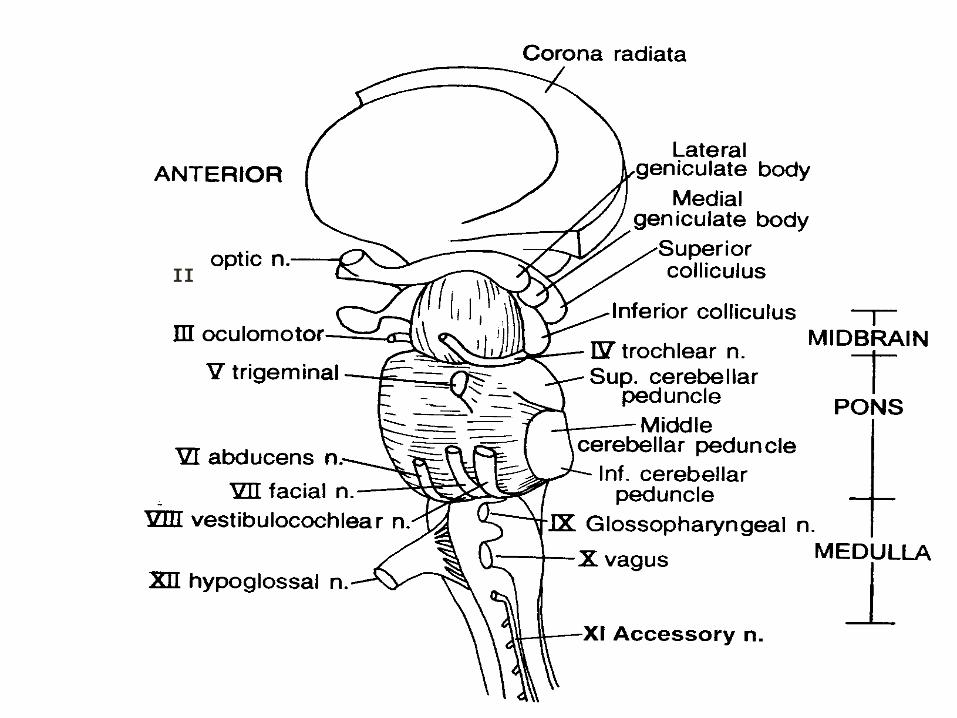
II
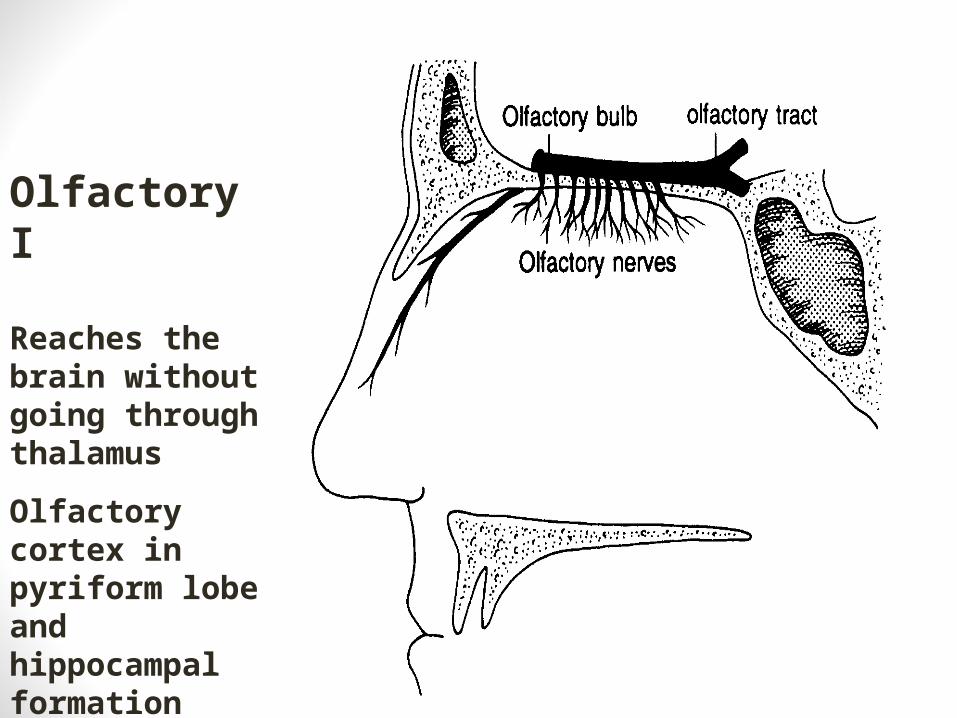
Olfactory I Reaches the brain without going through thalamus
Olfactory cortex in pyriform lobe and hippocampal formation
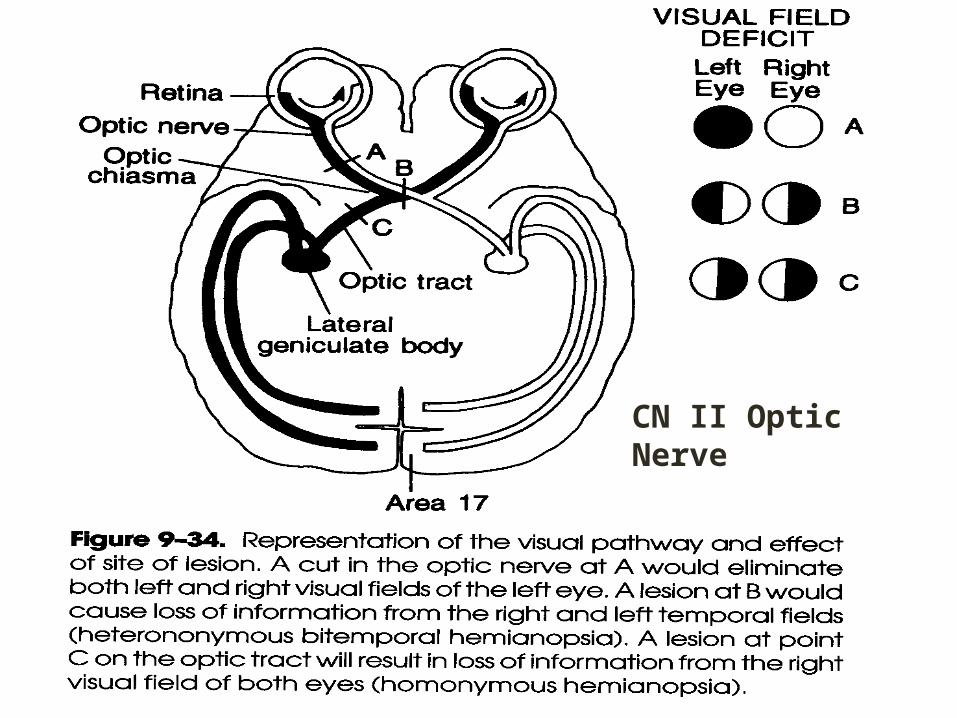
CN II Optic Nerve
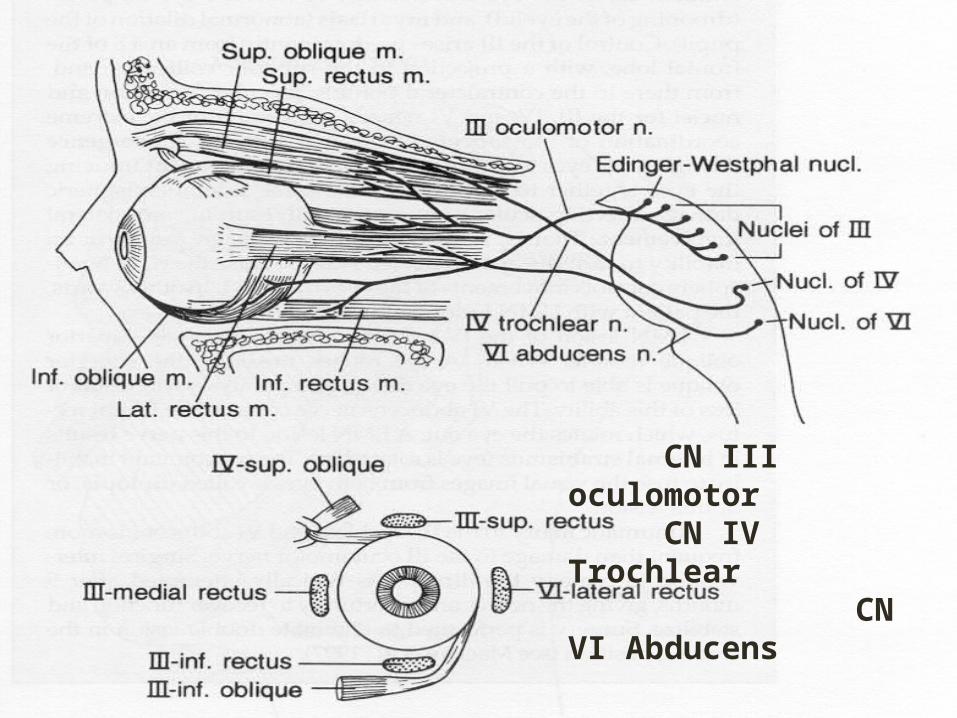
CN III oculomotor CN IV Trochlear CN VI Abducens
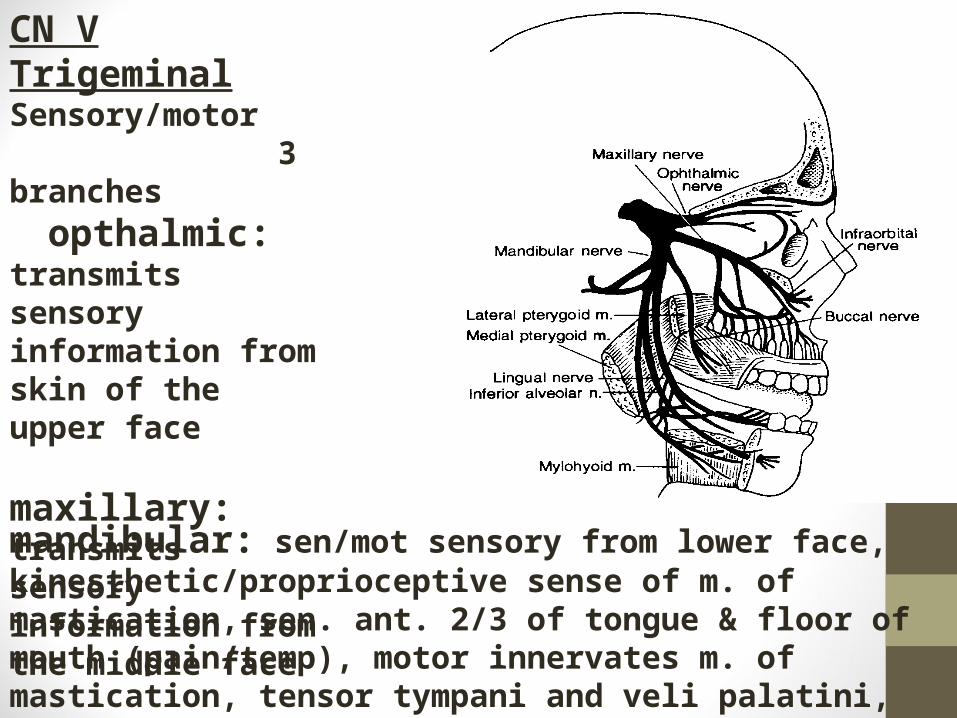
CN V Trigeminal Sensory/motor 3 branches opthalmic: transmits sensory information from skin of the upper face maxillary: transmits sensory information from the middle face
mandibular: sen/mot sensory from lower face, kinesthetic/proprioceptive sense of m. of mastication, sen. ant. 2/3 of tongue & floor of mouth (pain/temp), motor innervates m. of mastication, tensor tympani and veli palatini, mylohyoid, ant. belly of digastric
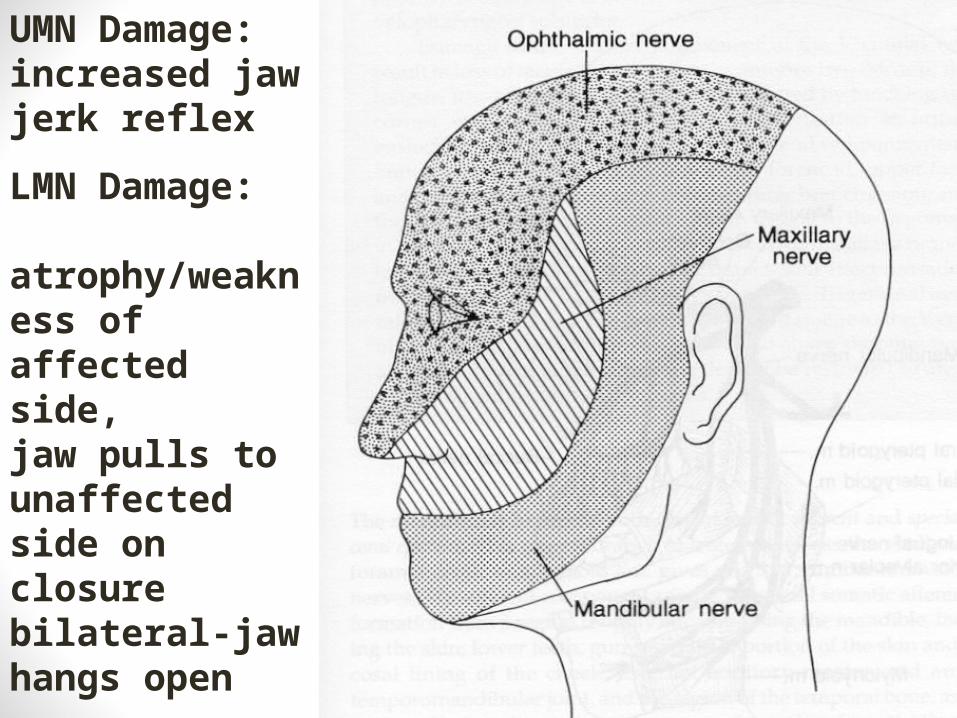
UMN Damage: increased jaw jerk reflex
LMN Damage: atrophy/weakness of affected side, jaw pulls to unaffected side on closure bilateral-jaw hangs open
TVP damage: hypernasality
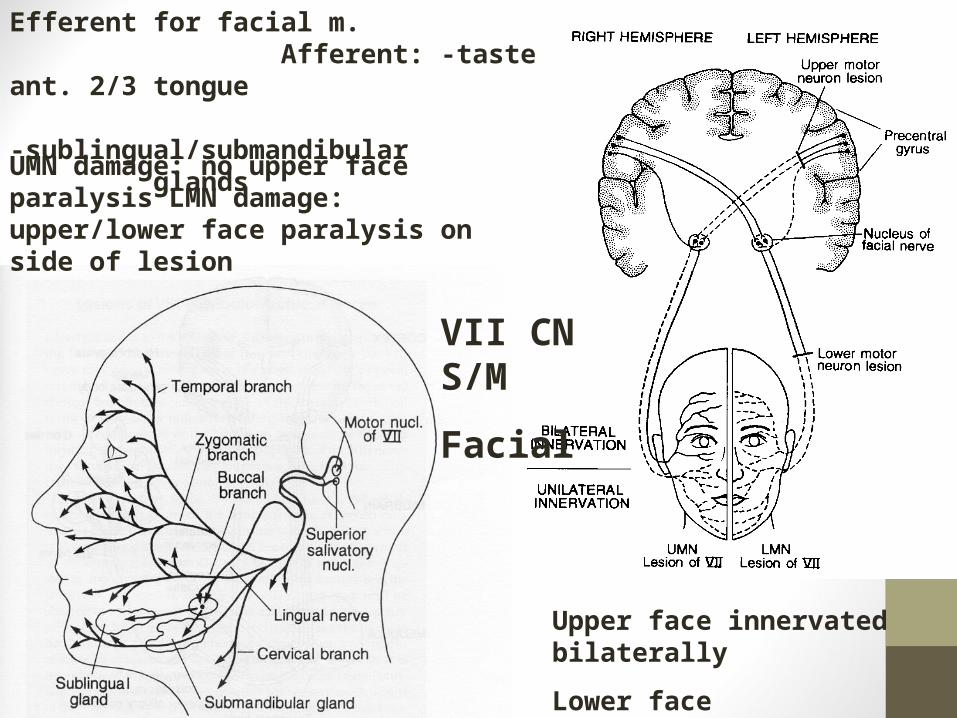
Upper face innervated bilaterally
Lower face contralateral
Efferent for facial m. Afferent: -taste ant. 2/3 tongue
-sublingual/submandibular glands
UMN damage: no upper face paralysis LMN damage: upper/lower face paralysis on side of lesion
VII CN S/M
Facial
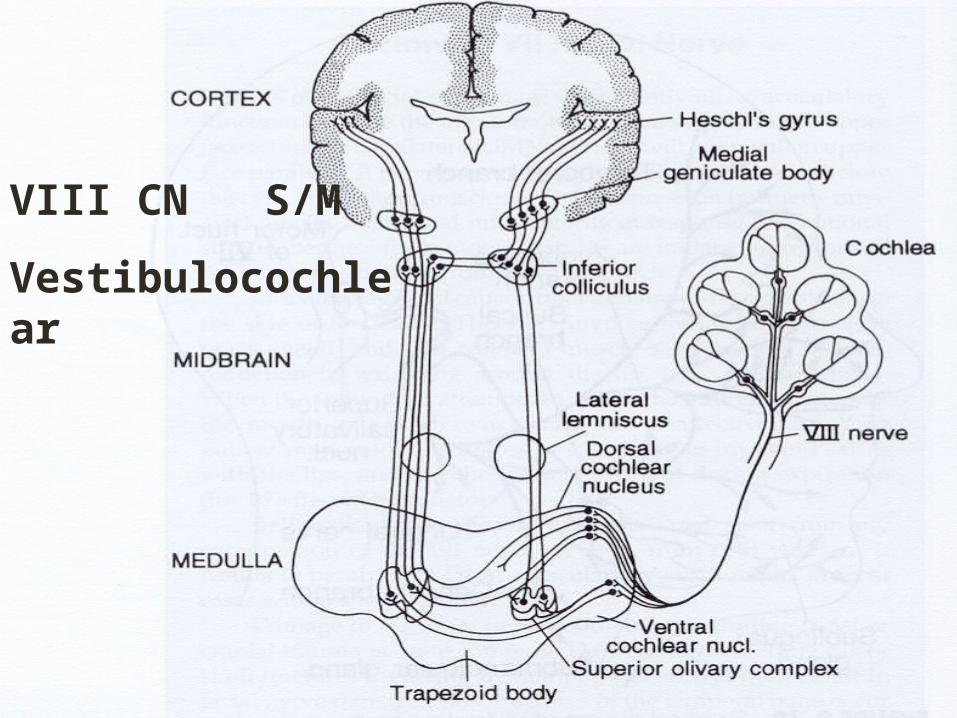
VIII CN S/M
Vestibulocochlear
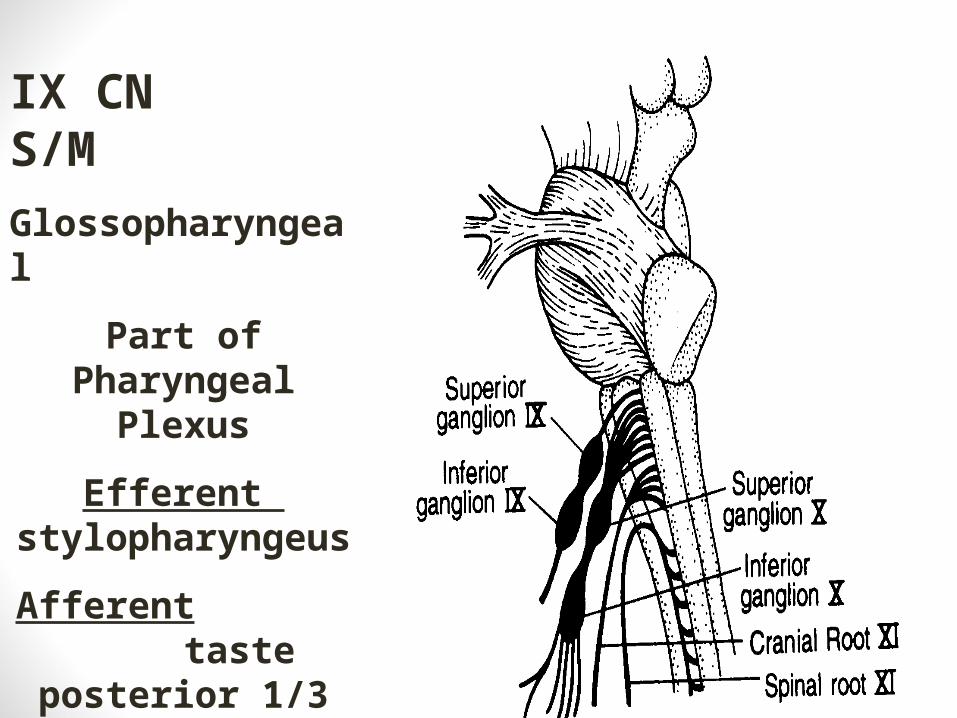
IX CN S/M
Glossopharyngeal
Part of Pharyngeal Plexus
Efferent stylopharyngeus
Afferent taste posterior 1/3 tongue, soft palate
Pain, temp., touch posterior 1/3
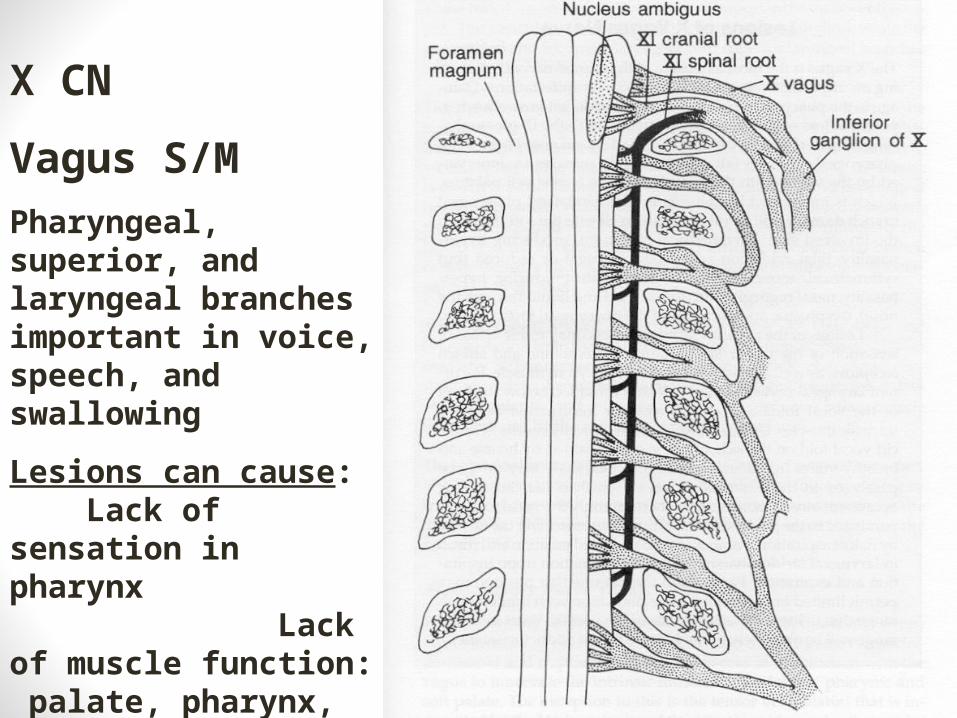
X CN
Vagus S/M
Pharyngeal, superior, and laryngeal branches important in voice, speech, and swallowing
Lesions can cause: Lack of sensation in pharynx Lack of muscle function: palate, pharynx, vocal fold, esophagus
Large autonomic role
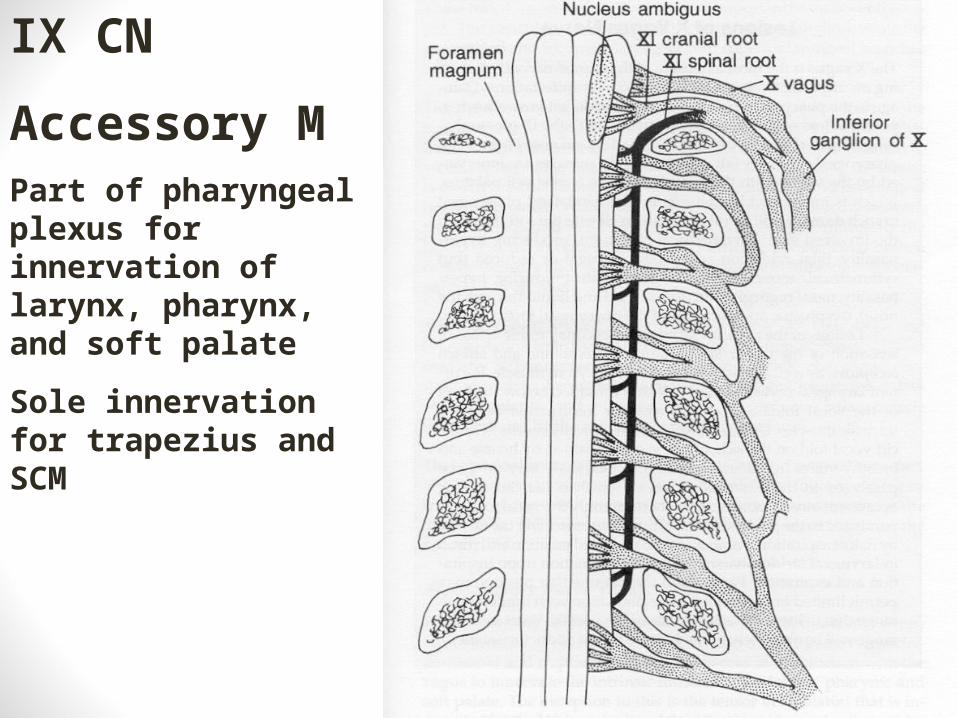
IX CN
Accessory MPart of pharyngeal plexus for innervation of larynx, pharynx, and soft palate
Sole innervation for trapezius and SCM
XII CN
Hypoglossal MInnervation for the motor function of the tongue
Each hypoglossal nucleus served by contralateral corticobulbar tract (L) UMN damage = (R) tongue weakness (L) LMN damage = (L) tongue weakness
Fibers of the Corticobulbar Tract decussate prior to reaching the hypoglossal nucleus, therefore (L) UMN damage/ (R) LMN damage = (R) tongue weakness
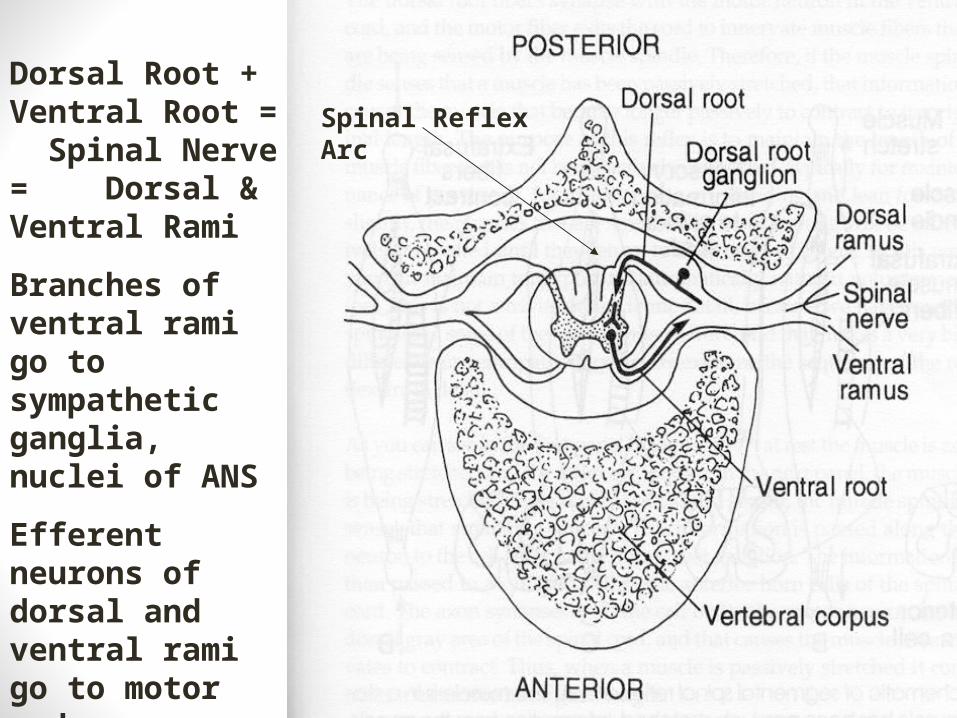
Dorsal Root + Ventral Root = Spinal Nerve = Dorsal & Ventral Rami
Branches of ventral rami go to sympathetic ganglia, nuclei of ANS
Efferent neurons of dorsal and ventral rami go to motor end plates/muscle synapse
Spinal Reflex Arc
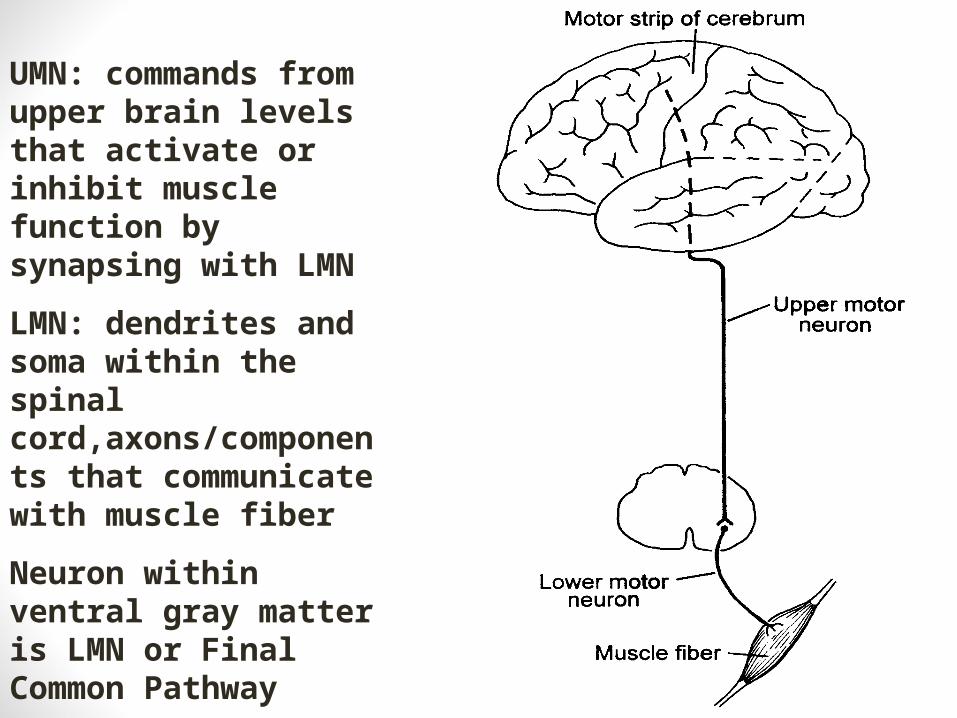
UMN: commands from upper brain levels that activate or inhibit muscle function by synapsing with LMN
LMN: dendrites and soma within the spinal cord,axons/components that communicate with muscle fiber
Neuron within ventral gray matter is LMN or Final Common Pathway
UMN/LMN• LMN Damage: muscle weakness or complete paralysis,
reflexes not intact• UMN Damage: muscle weakness or complete paralysis,
reflexes intact because a spinal arc reflex is a LMN process
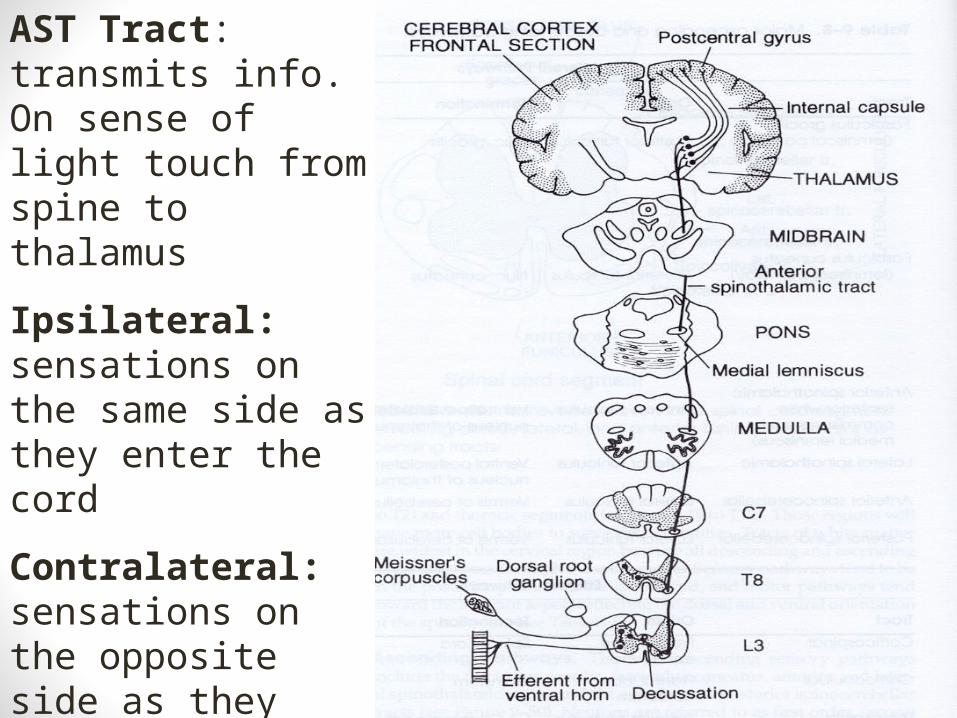
AST Tract: transmits info. On sense of light touch from spine to thalamus
Ipsilateral: sensations on the same side as they enter the cord
Contralateral: sensations on the opposite side as they enter the cord
Decussate: cross the midline
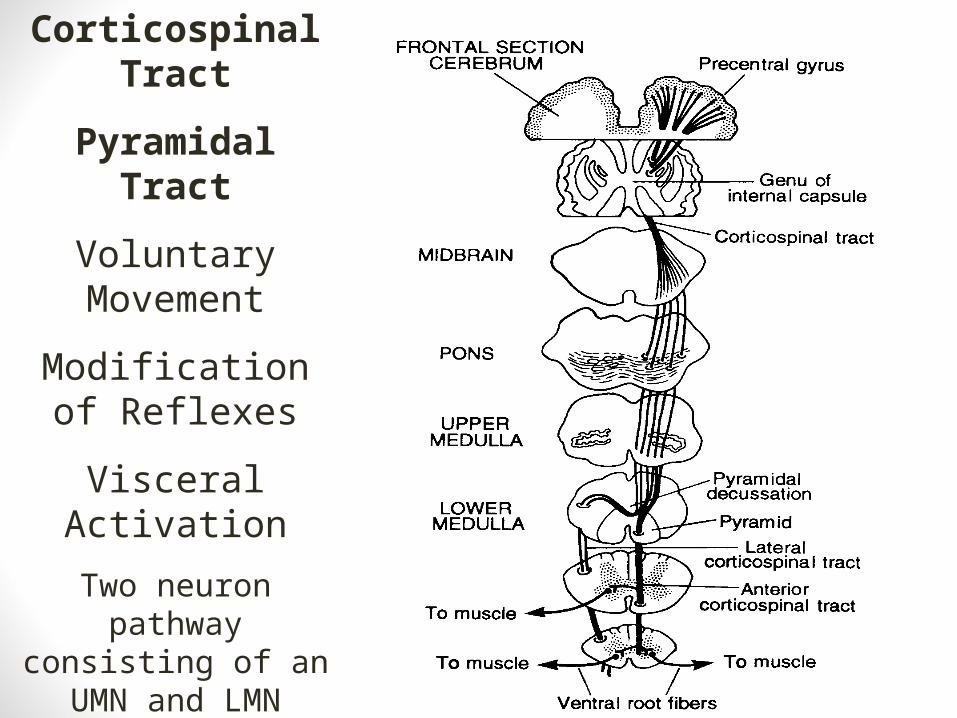
Corticospinal Tract
Pyramidal Tract
Voluntary Movement
Modification of Reflexes
Visceral Activation
Two neuron pathway consisting of an UMN
and LMN
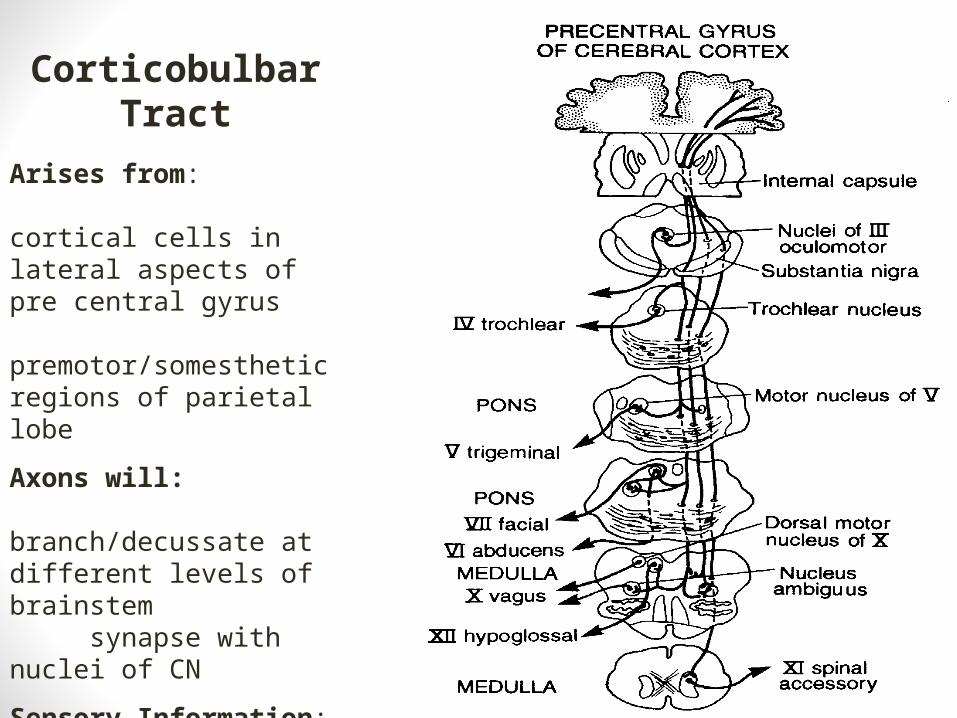
Corticobulbar Tract
Arises from: cortical cells in lateral aspects of pre central gyrus premotor/somesthetic regions of parietal lobe
Axons will: branch/decussate at different levels of brainstem synapse with nuclei of CN
Sensory Information: facilitate/inhibit transmission to thalamus
Serves: CN for speech
Higher Functioning• Primary activity areas: receive information from senses,
extract info.• Adjacent higher order areas of processing (secondary,
tertiary,quaterary): info. compared to other info. received and stored associated with modality
• Association areas: highest level of cognitive processing
Motor Function• Identify target: tongue tip to alveolar ridge
• Spacial orientation: integration of information of body parts in space
• Posterior parietal lobe receives information from thalamus, cerebellum, basal ganglia
• Develop plan to achieve target behavior• Premotor region, area 6, anterior to motor strip plans the action,
receives info from areas 1,2,3 re location of muscles and joints• SMA, area 6 sup. & med., preparatory speech act, initiation of
speech act
• Execute plan: muscle movement with accurate timing force and rate• Area 4 execution of voluntary movement
Motor System Lesions• Dysarthria: speech disorder arising from paralysis, muscular weakness,
and dyscoordination of speech musculature
• Flaccid Dysarthria: LMN damage of CN, dysphonia due to VF paralysis, fasciculations, hypotonia, reflexive responses reduced or absent
• Spastic Dysarthria: UMN bilateral damage to pyramidal or extrapyramidal tracts, hyper-reflexia, hypertonia• UUMN: less devastating than bilateral
Motor System Lesions• Ataxic Dysarthria: Damage to the cerebellum &/or brainstem
vestibular nuclei• Loss of coordination, unable to achieve articulatory target,
problems in coordination of rate, range, and movement• Dysdiadochokinesia• Dysprosody
Motor System Lesions• Hypokenetic Dysarthria: paucity of movement, inhibited initiation of
movement, reduced ROM, rigidity, pill rolling hand tremor• Damage to BG &/or substantia nigra (SN)
• SN produces Dopamine (DA) which balances acetylcholine (Ach), decreased DA results in inhibited initiation of motor function
• Speech rushed, reduced duration of speech sounds, monopitch, monoloudness
Motor System Lesions• Hyperkenetic Dysarthria:Extraneous involuntary movement caused by BG
circuit damage• Subthalamic N. damage: inhibition to GP is lost resulting in Ballism (uncontrolled
flailing)• BG damage: if Ach is decreased and DA increased choreiform, involuntary
twitching and movements, result• Tics: rapid movements of small groups of muscle fibers• Tremors: rhythmic contractions• Athetosis: slow, writhing movements• Dystonia: involuntary movement to a posture, posture held briefly
Motor System Lesions
• Mixed Dysarthria: Damage to more than one of the controlling systems• S/F: found in ALS, disease of UMN & LMN• S/A: found in MS, UMN and cerebellum • S/A/hypo: Wilson’s disease (hepatolenticular
degeneration)
Motor System Lesions• Apraxia/Dyspraxia: A dysfunction of motor planning in the absence of
muscular weakness or dysfunction• SMA damage: difficulty in initiating speech• Dominant insular cortex damage: verbal dyspraxia (loss of fluency and groping
behavior, ability to contract musculature voluntarily is impaired) • Oral apraxia: inability to perform non speech oral gestures
• Supramarginal Gyrus damage: verbal apraxia affecting long and complex sentences
Hemispheric Specialization
• Left Hemisphere• Lateral Fissure is longer• Planum Temporale (HG) is larger• Generally functional dominance for L/S• Processes consonant transitions and stop consonant
bursts in (R) handed • Process of analysis, favored discrete, sequential, brief
duration or rapidly changing information• Spoken/written language perception & production
Hemispheric Specialization
• Right Hemisphere• Spatial and holistic elements
• Face recognition• Speech intonation• Melody, tonal information• Perception of form• Intention of speaker
Lesion Studies• Speech and Language Areas
• Wernicke’s Area (22): receptive or fluent aphasia• Relatively normal flow of speech• Has syntax • Does not understand what is said • Verbal paraphasias (substitution of words)• Neologisms (new word), jargon, word salad• Cannot repeat
Lesion Studies• Broca’s Aphasia: lesions to 44,45, operculum of frontal-
parietal, insula, supramarginal gyrus of parietal lobe• Difficulty with the planning of speech• Non fluent aphasia• Expressive abilities severely limited• Usually retain auditory and visual input
Lesion Studies• Global Aphasia: Damage to both Wernicke’s and Broca’s
Area and some sub cortical structures• Both receptive and expressive functions are severely impaired
Lesion Studies• Conduction Aphasia: lesion of arcuate fasiculus connecting Broca’s and
Wernicke’s area• problem with repetition of words
• Anomia: difficulty naming objects• Thalamic damage, cortical and subcortical structures
Lesion Studies• Dyspraxia: : inability to program the articulators for
voluntary speech and non speech movements• Frontal lobe insular cortex damage: difficulty producing simple
gestures with articulators (executive dyspraxia)• Supramarginal gyrus damage: difficulty sequencing more
complex articulatory gestures ( planning dyspraxia)
Lesion Studies• TBI/Right Hemisphere Damage
• Decision making• Problem solving• Judgment• Response inhibition• Pragmatics• Emotional lability• Personality characteristics• Communication of emotion, intent, humor• Abstract information• Frontal- response inhibition
Lesion Studies
• Parahippocampal region• Learning complex tasks• Remembering information received through sensory
modalities
• Hippocampus• Bilateral produce profound short term memory
deficit• Unilateral produce milder deficit• Removal of (L) difficulty remembering verbal
information
Recommended