Neoplasms of the Gastrointestinal Tract
Dr. M JeffersConsultant HistopathologistAMNCH, Tallaght
AMNCH Tallaght
Objectives: GI tumour pathology
tumour nomenclature and classification
tumour aetiology and pathogenesisprecursor lesionsmechanisms of carcinogenesis in different tissuespotential points for prevention / modification
tumour growth and behaviourinvasionmetastasis
tumour stagingstaging systemsprognostic factors

AMNCH Tallaght
Useful links
http://medstat.med.utah.edu/WebPath/webpath.html
www.bmj.com : collected resources
ABC of colorectal cancerABC of the upper gastrointestinal tract: cancer of the stomach and pancreas
AMNCH Tallaght
Neoplasms
Definition
Epidemiology, Aetiology, Pathogenesis
Morphology: Gross / Microscopic
Clinical presentation and outcome
Prognosis
AMNCH Tallaght
Nomenclature and Classification
Nomenclature / Classification by histogenesis:
Epithelial
Mesenchymal
Neuroendocrine
Haematolymphoid
Melanocytic

AMNCH Tallaght
Nomenclature and Classification
Epithelial tumours:
Benign: “adenoma”
Malignant: “carcinoma”
Adenocarcinoma Squamous carcinoma Small cell carcinoma

AMNCH Tallaght
Nomenclature and Classification
Neuroendocrine tumours:
Benign: “carcinoid”
Malignant: neuroendocrine carcinomasmall cell carcinoma

AMNCH Tallaght
Nomenclature and Classification
Mesenchymal tumours:
Benign: (tissue)oma lipoma, leiomyoma etc
Malignant: (tissue)sarcoma liposarcoma, leiomyoma etc
Gastrointestinal stromal tumour (GIST): benignlow malignant potentialmalignant

AMNCH Tallaght
Nomenclature and Classification
Haematolymphoid tumours:
Bone marrow neoplasm (+/- circulating cells): leukaemia
Lymph node / extranodal lymphoid cell tumour: lymphoma

AMNCH Tallaght
Neoplasms of the Gastrointestinal Tract
Concepts:
Carcinogenesis: Metaplasia/Dysplasia/Carcinoma sequenceAdenoma/Carcinoma sequence
Differentiation
Invasion and Metastasis
Tumour staging
AMNCH Tallaght
Tumour Aetiology and Pathogenesis: Carcinogenesis
Various mechanisms operative in carcinogenesis in the GI tract:
Intraepithelial neoplasia – Dysplasia – Carcinoma
Metaplasia – Dysplasia - Carcinoma
Adenoma - Carcinoma sequence
Replicator error phenotype

AMNCH Tallaght
Intraepithelial neoplasia – carcinoma sequence
Multistage process of carcinogenesis from
normal through low grade intra-epithelial neoplasia (dysplasia) (RR 2.2) through high grade intra-epithelial neoplasia (dysplasia) (RR >60) to invasive carcinoma.
Progressive development of architectural and cytological abnormalityProgressive increase in relative risk of invasive carcinoma
Useful model is squamous cell carcinoma of oesophagus.

AMNCH Tallaght
Intraepithelial neoplasia – carcinoma sequence: Oesophageal cancer
Morphologic abnormality in dysplasia –carcinoma sequence in oesophageal mucosa reflects underlying genetic abnormality.
p53 mutationlow grade
LOH 3p14 (FHIT) fragile histidine triad, tumour suppressor gene
Cyclin D1 overexpression (11q13), 3p21 LOH
C-myc, EGFR, HST1 overexpression invasive carcinoma

AMNCH Tallaght
Intraepithelial neoplasia – carcinoma sequence
Normal oesophageal squamous mucosa
High grade squamous dysplasia (carcinoma in-situ)
Invasive squamous cell carcinoma
p53 mutation FHIT LOH CYD1 c-myc, EGFR, HST1

AMNCH Tallaght
Metaplasia – Dysplasia – Carcinoma Sequence
Multistage process of carcinogenesis from
Normal throughMetaplastic columnar epithelium throughDysplasia in metaplastic epithelium
low gradehigh grade to
Invasive carcinoma
Useful model is adenocarcinoma of oesophagus

AMNCH Tallaght
Metaplasia – Dysplasia – Carcinoma sequence:Oesophageal cancer
Barrett’s oesophagus = columnar lined oesophagus
Replacement of the squamous lining of the distal oesophagus by glandular mucosa in response to injury, most frequently gastro-oesophageal refluxmetaplasia to gastric and intestinal type epithelium
Stepwise progression of dysplasia in metaplastic epithelium leads to invasive malignancy: architectural and cytological abnormalities develop.
Morphologic changes reflect underlying molecular genetic / cell cyle regulatory abnormalities

AMNCH Tallaght
Metaplasia – Dysplasia – Carcinoma sequence:Oesophageal cancer
Normal
MetaplasiaFHIT alterations, CDKN2A hypermethylation
Dysplasiarab11 abnormalities
Low gradeKi67 abnormality
High grade APC mutation
p53 mutation (different to scc)
Invasive carcinoma c-erbB2, EGFR

AMNCH Tallaght
Metaplasia – Dysplasia – Carcinoma sequence:Oesophageal cancer
Normal oesophageal squamous mucosaBarrett’s oesophagus: metaplastic columnar and intestinal mucosa

AMNCH Tallaght
Metaplasia – Dysplasia – Carcinoma sequence:Oesophageal cancer
Barrett’s oesophagus: low grade dysplasia
Barrett’s oesophagus: high grade dysplasia
Invasive adenocarcinoma
FHIT Ki67 p53 APC

AMNCH Tallaght
The metaplasia dysplasia sequence: significance
Intestinal metaplasia in the oesophagus is a marker of increased adenocarcinoma risk
Risk of carcinoma is greatest with high grade dysplasia: concurrent carcinoma in up to 50%
Many cases of high grade dysplasia will progress to invasive carcinoma over time
Diagnosis of high grade dysplasia: rebiopsy to exclude invasion consider surgery
Diagnosis of metaplasia: treat underlying conditions (GORD)surveillance endoscopy to identify dysplasiaaiming to prevent cancers / detect cancer early

AMNCH Tallaght
Metaplasia – Dysplasia – Carcinoma sequence:Gastric cancer
Chronic atrophic gastritis is a major risk factor for gastric carcinoma (intestinal type)
Risk of malignant transformation is strongly linked to intestinal metaplasia and intra-epithelial neoplasia (dysplasia)
Variety of processes may lead to atrophic gastritis:Helicobacter gastritisAuto-immune gastritis
Metaplasia – dysplasia sequence acts as a final common pathway in development of malignancy
AMNCH Tallaght
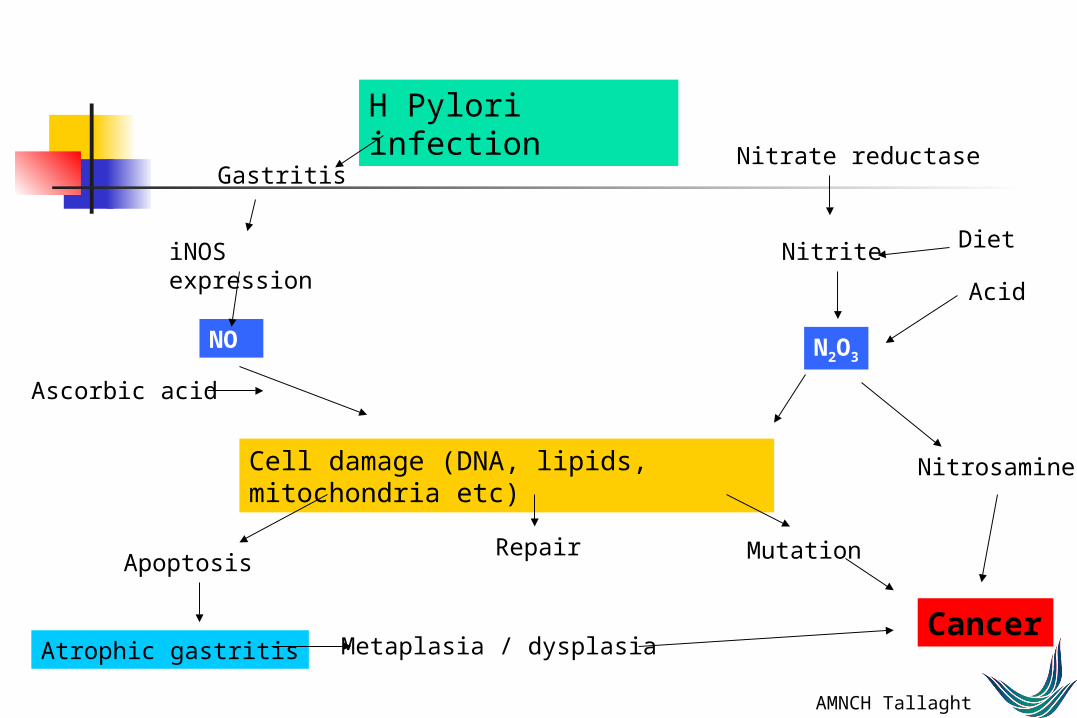
H Pylori infection
Gastritis
iNOS expression
NO
Cell damage (DNA, lipids, mitochondria etc)
Apoptosis
Atrophic gastritis
Ascorbic acid
Nitrate reductase
Nitrite Diet
Acid
N2O3
Nitrosamines
Mutation
Cancer
Repair
Metaplasia / dysplasia
AMNCH Tallaght
Metaplasia – Dysplasia – Carcinoma sequence:Gastric cancer
Chronic gastritis
Intestinal metaplasia
Dysplasia
low grade
high grade
Invasive carcinoma

AMNCH Tallaght
Metaplasia – dysplasia - carcinoma sequence in the stomach
Stomach: normalStomach: chronic gastritis
Stomach: atrophy and intestinal metaplasia

AMNCH Tallaght
Metaplasia – dysplasia - carcinoma sequence in the stomach
Stomach: low grade dysplasia Stomach: high grade dysplasia
Stomach: invasive adenocarcinoma

AMNCH Tallaght
The metaplasia dysplasia sequence: significance
Most intestinal type gastric cancers develop on a background of atrophy, metaplasia and dysplasia.
Predisposing factors for atrophy and metaplasia are known:chronic HP gastritis, auto-immune gastritis etc.
Treatment of predisposing conditions, endoscopic surveillance of patients with documented metaplasia: strategies to reduce risk, detect cancer early.
AMNCH Tallaght
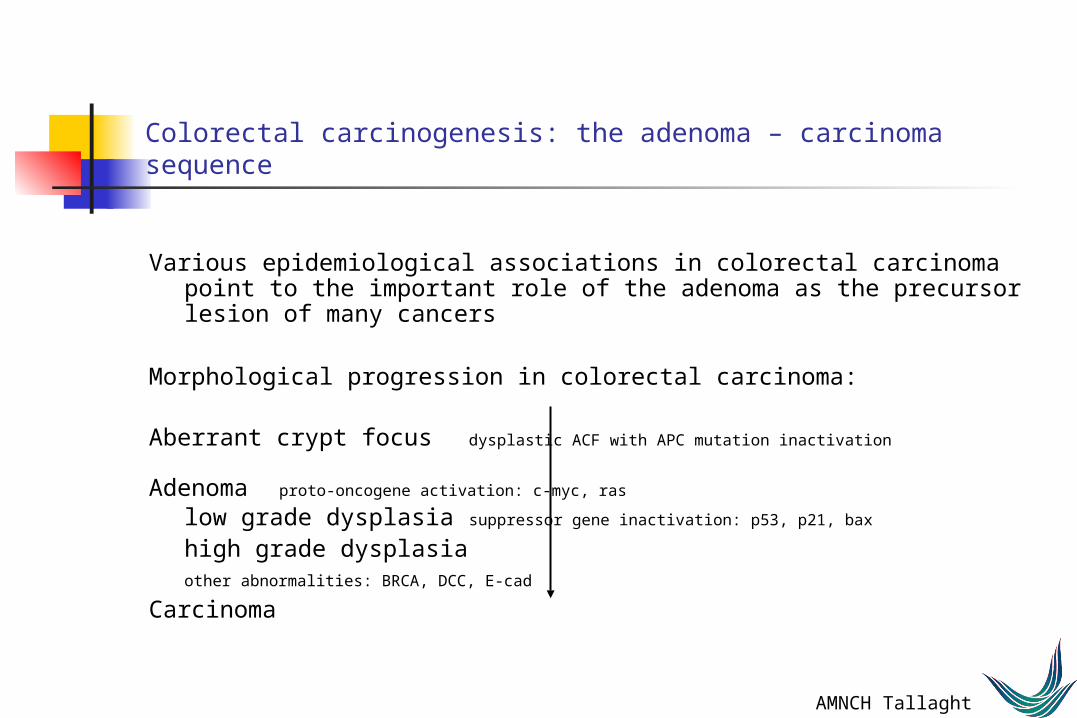
Colorectal carcinogenesis: the adenoma – carcinoma sequence
Various epidemiological associations in colorectal carcinoma point to the important role of the adenoma as the precursor lesion of many cancers
Morphological progression in colorectal carcinoma:
Aberrant crypt focus dysplastic ACF with APC mutation inactivation
Adenoma proto-oncogene activation: c-myc, ras
low grade dysplasia suppressor gene inactivation: p53, p21, bax
high grade dysplasiaother abnormalities: BRCA, DCC, E-cad
Carcinoma

AMNCH Tallaght
Normal Epithelium
Early Adenoma
Intermediate
Adenoma
Late
Adenoma
Carcinoma
CarcinomaMSI +
Metastasis
Methylation Defect
APC
K-Ras Smad4 p53
Mismatch repair defectTGF, BAX
Genetic Model for Sporadic Colorectal Carcinogenesis
??
??

AMNCH Tallaght
Adenomatous polyps of the colon
Neoplastic polyps, precursors of carcinoma
Architectural patterns:Tubular/Villous/Tubulovillous
Gross presentation:sessile/pedunculated/flat adenoma
Risk of malignancy size (ras), architecture, dysplasia

AMNCH Tallaght
Colon: tubular adenoma

AMNCH Tallaght
normal epithelium adenomatous epithelium

AMNCH Tallaght
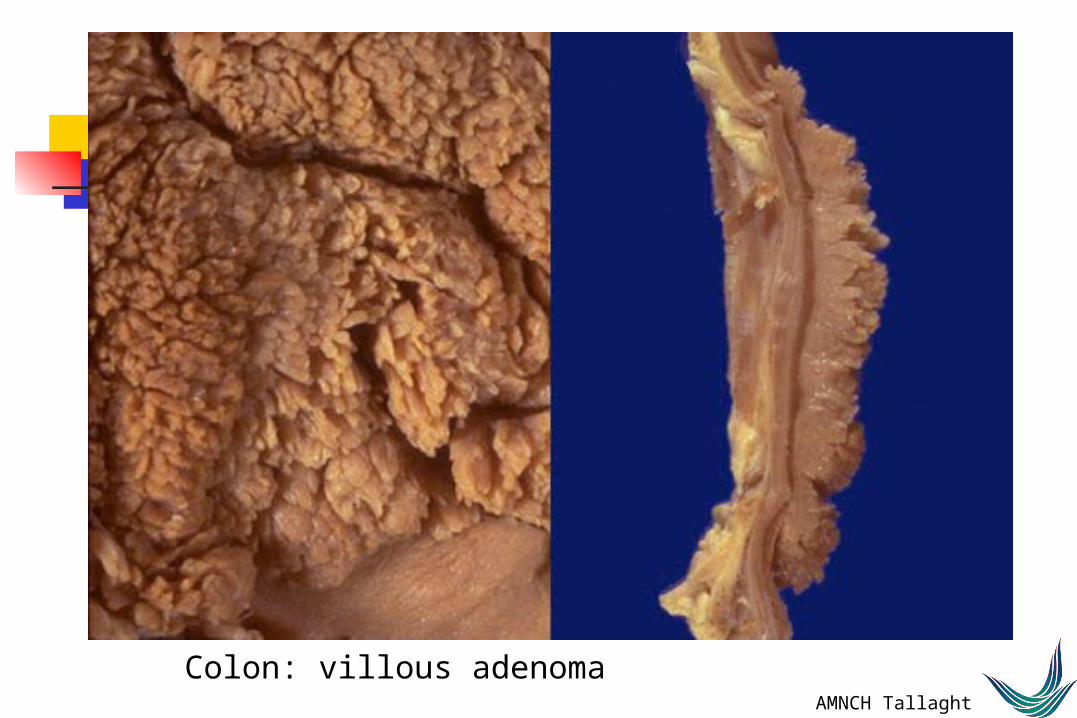
Colon: villous adenoma

AMNCH TallaghtColon: villous adenoma

AMNCH Tallaght
Polyposis syndromes
Sydromes characterised by multiple polyps in colorectum +/- elsewhere in GIT
FAP: 5q21 defect, multiple polyps, 100% lifetime risk of carcinoma
HNPCC: MSH gene defect, fewer polyps, typical pattern of tumours
Gardner: variant of FAP with skin and other lesions
Turcot: association with CNS neoplasms
AMNCH Tallaght
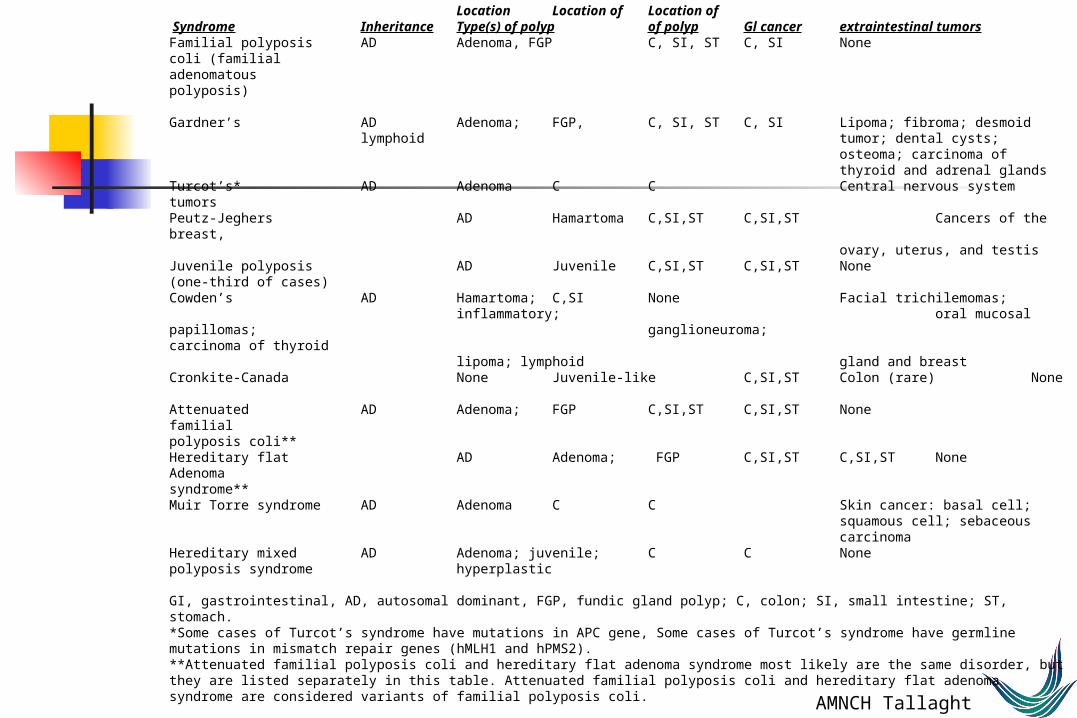
Table 1. Intestinal polyposis syndromes Location Location of Location of Syndrome Inheritance Type(s) of polyp of polyp Gl cancer extraintestinal tumorsFamilial polyposis AD Adenoma, FGP C, SI, ST C, SI Nonecoli (familial adenomatous polyposis) Gardner’s AD Adenoma; FGP, C, SI, ST C, SI Lipoma; fibroma; desmoid lymphoid tumor; dental cysts; osteoma; carcinoma of thyroid and adrenal glandsTurcot’s* AD Adenoma C C Central nervous system tumorsPeutz-Jeghers AD Hamartoma C,SI,ST C,SI,ST Cancers of the breast, ovary, uterus, and testis Juvenile polyposis AD Juvenile C,SI,ST C,SI,ST None(one-third of cases) Cowden’s AD Hamartoma; C,SI None Facial trichilemomas; inflammatory; oral mucosal papillomas;
ganglioneuroma; carcinoma of thyroid lipoma; lymphoid gland and breastCronkite-Canada None Juvenile-like C,SI,ST Colon (rare) None
Attenuated AD Adenoma; FGP C,SI,ST C,SI,ST Nonefamilial polyposis coli** Hereditary flat AD Adenoma; FGP C,SI,ST C,SI,ST NoneAdenoma syndrome** Muir Torre syndrome AD Adenoma C C Skin cancer: basal cell;
squamous cell; sebaceous carcinomaHereditary mixed AD Adenoma; juvenile; C C Nonepolyposis syndrome hyperplastic GI, gastrointestinal, AD, autosomal dominant, FGP, fundic gland polyp; C, colon; SI, small intestine; ST, stomach. *Some cases of Turcot’s syndrome have mutations in APC gene, Some cases of Turcot’s syndrome have germline mutations in mismatch repair genes (hMLH1 and hPMS2). **Attenuated familial polyposis coli and hereditary flat adenoma syndrome most likely are the same disorder, but they are listed separately in this table. Attenuated familial polyposis coli and hereditary flat adenoma syndrome are considered variants of familial polyposis coli.
AMNCH Tallaght
Familial adenomatous polyposis (FAP)
Autosomal dominant condition characterised by numerous adenomatous polyps and high risk of progression to adenocarcinoma
Germline mutation in APC gene (5q21-22) which encodes a 2843 aa polypeptide which acts as a negative regulator in the Wnt signalling pathway, regulates cellular -catenin concentration
Lack of functional APC leads to accumulation of -catenin and consititutive expression of c-myc and cyclin D1
AMNCH Tallaght
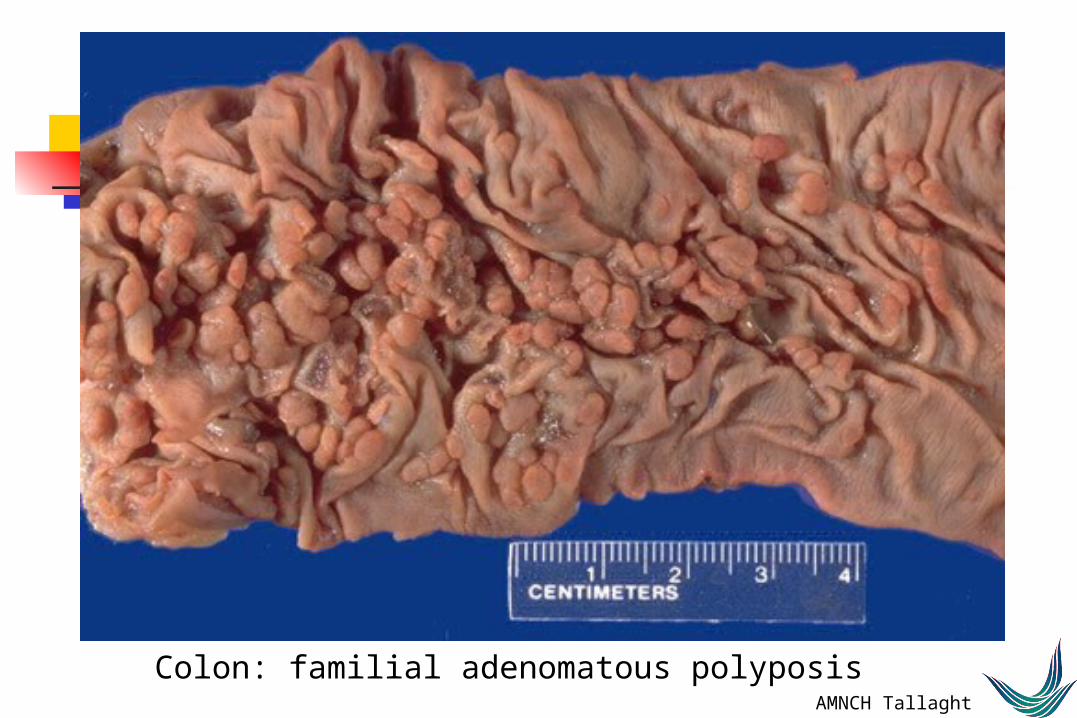
Colon: familial adenomatous polyposis

AMNCH Tallaght
Adenoma carcinoma sequence: significance and implications
Mechanism underlying most colorectal carcinomas
Identifiable precursor lesions in many cases: early detection of precursor lesions has obvious implications for early treatment and prevention of invasive disease
Identification of families with germ-line mutations and significant polyposis syndromes offers significant preventive opportunities
Tumour pathogenesis has direct implications on cancer management and prevention
AMNCH Tallaght
Colorectal carcinogenesis: the mismatch repair defect pathway
Mechanism of carcinogenesis distinct from the adenoma – carcinoma sequence
Tumours characterised by extensive nucleotide insertions / deletions in repeated sequences in tumour DNA: microsatellite instability (MSI) / DNA replication error (RER)
Tumours with MSI are classified as MSI high-frequency (MSI-H) or MSI low frequency (MSI-L)
These tumours arise through defects in the DNA mismatch repair mechanism, defects which may be sporadic or inherited
Some sporadic tumours are MSI-H but most MSI-H tumours characteristic of hereditary non-polyposis colorectal carcinoma (HNPCC)

AMNCH Tallaght
HNPCC
HNPCC: a syndrome characterised by inherited defects in DNA repair due to germline mutations of the relevant genes: (hMLH1, hMSH2)
High frequency of colorectal carcinomaExtracolonic tumours in endometrium, stomach, ovary, brain, skin, small
bowel
Criteria for classification as HNPCC: Amsterdam criteria (+ revisions)
Classical tumour characteristics: right sided, large, mucinous, low stage
AMNCH Tallaght
Hereditary Non-polyposis Colorectal Cancer
Criteria:At least 3 relatives with a HNPCC associated cancer (colorectum/endometrium/small bowel/ureter/renal pelvis)
Ones should be first degree relative of other two
At least 2 successive generations involved
At least one tumour diagnosed before 50 yrs of age
Familial adenomatous polyposis should be excluded
Tumours should be verified by histopathological examination

AMNCH Tallaght
MSI in colorectal cancer: diagnosis
hMSH2: normal hMSH2: tumour
Normal tissue: hMSH2 expression Loss of expression in MSI-H tumour

AMNCH Tallaght
Replicator error phenotype: implications
Identification of MSI-H tumours confers a high probability of an inherited cancer
Cancers can be screened for MSI status, confirmation of germ-line status required for definition of syndrome
Careful family history combined with tumour characteristics can identify at-risk groups
Early intervention and prevention opportunities
Tumour pathogenesis impacts directly on patient management and prognosis.

AMNCH Tallaght
Carcinogenesis: review of mechanisms
Various mechanisms operative in carcinogenesis in the GI tract:
Intraepithelial neoplasia – Dysplasia – Carcinoma
Metaplasia – Dysplasia - Carcinoma
Adenoma - Carcinoma sequence
Replicator error phenotype
Various mechanisms implicated at different sites
Significance in terms of identification of precursor lesions, treatment and prevention of cancer

AMNCH Tallaght
AMNCH Tallaght
Differentiation
Differentiation refers to the degree of maturation of tumour cells / tissues:
what cell type / tissue type does the tumour grow in ?
how closely does the tumour reproduce normal tissue architecture ?
Tumours are described as: well differentiatedmoderately differentiatedpoorly differentiated
Differentiation is closely related to tumour grade:
well differentiated – low gradepoorly differentiated – high grade
AMNCH Tallaght
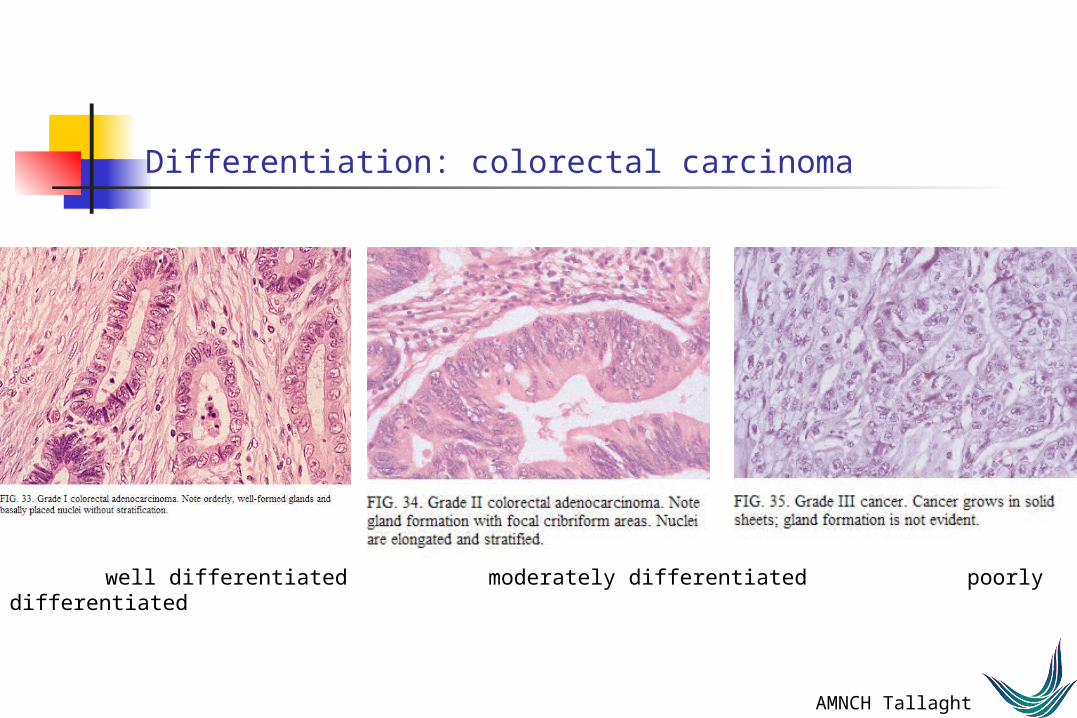
Differentiation: colorectal carcinoma
well differentiated moderately differentiated poorly differentiated

AMNCH Tallaght

AMNCH Tallaght
Neoplasms of the Gastrointestinal Tract
Classification of tumours:
Anatomical Location
Origin (Primary/Secondary)
Behaviour (benign/uncertain/malignant)
Histogenesis (epithelial/stromal/lymphoid etc)

AMNCH Tallaght
Tumours of the oesophagus
Benign tumours rare:
Leiomyoma
Most are malignant and most are carcinomas
Squamous cell carcinomaAdenocarcinoma

AMNCH Tallaght
Oesophageal carcinoma
Approx 6% of GIT cancers
1996 Irish Cancer Registry data:
299 cases (1.4% of all cancers)
303 deaths (4.1% of all cancer deaths)

AMNCH Tallaght
Oesophageal carcinoma
Histological types:
Squamous cell carcinomaAdenocarcinoma (a/w Barrett’s oesophagus)Others
Relative proportion of squamous and adenocarcinoma varies with geography
Adenocarcinoma increasing incidence

AMNCH Tallaght
Oesophageal carcinoma
Squamous carcinoma:
Alcohol, Tobacco, Food, HPVArise on background of dysplasia / in-situ carcinomaVarying differentiation
well - poorly differentiated

AMNCH Tallaght

AMNCH Tallaght
Normal Oesphagus

AMNCH Tallaght
Oesophageal squamous carcinoma

AMNCH Tallaght
Squamous cell carcinoma

AMNCH Tallaght
Oesophageal carcinoma
Adenocarcinoma:
Majority arise on a background of Barrett’s oesophagus.Metaplasia - Dysplasia - Carcinoma sequenceSequential acquisition of genetic abnormalities, oncogene activation,
TSG inactivation Majority are intestinal type adenocarcinoma

AMNCH Tallaght

AMNCH Tallaght

AMNCH Tallaght
Oesophageal carcinoma
Invasion through submucosa, muscularis and into soft tissueMetastasis to regional nodes, distant sites
Most are advanced at diagnosis5 year survival is poor (<30%)Early diagnosis improves outcome
AMNCH Tallaght
Tumours of the stomach
Benign tumours are rare:
Leiomyomas etc
Malignant tumours:
carcinoma >> lymphoma, stromal tumours, carcinoid tumours

AMNCH Tallaght
Gastric carcinoma
Irish Cancer Registry Data 1996:
482 cases (2.3% of total cancers)399 deaths (5.4% of total cancer deaths)
Male : female 1.5:1
18 lymphomas in same time period

AMNCH Tallaght
Gastric carcinoma
Pathogenesis:
Chronic gastritis - metaplasia - dysplasia(H Pylori)
Dietary factors, smokingGenetic factors (HNPCC)
Dysplasia is a final common pathway in intestinal type tumours

AMNCH Tallaght
Gastric carcinoma
Tumour pathology: 2 major types:
Intestinal: Bulky masses / ulcers, glandular pattern
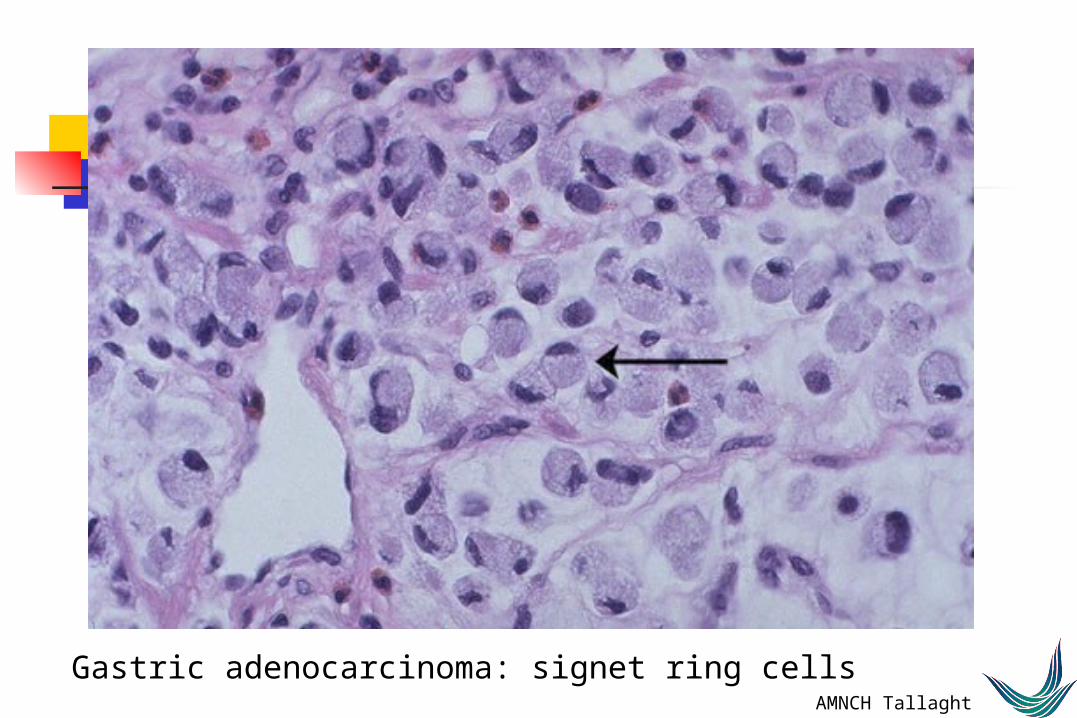
Diffuse: infiltrative lesions, “signet-ring” cells

AMNCH Tallaght
Gastric tumour

AMNCH Tallaght
Gastric cancer: Linitis Plastica

AMNCH Tallaght
Normal stomach mucosa

AMNCH Tallaght

AMNCH Tallaght
Gastric adenocarcinoma: diffuse type
AMNCH Tallaght
Gastric adenocarcinoma: signet ring cells
AMNCH Tallaght
Gastric carcinoma
Late presentation is typical
6% present in stage I, 30% stage IV(of those staged)
Prognosis is poor:
Cumulative probability of survival34% @ 1yr20% @5yrs

AMNCH Tallaght
Gastric carcinoma
Importance of Pathologic Staging:
Early gastric carcinoma is disease limited to mucosa and submucosa, irrespective of nodal involvement
5ys is >90% with surgical resection
Advanced gastric carcinoma is disease which invades the muscularis propria
5ys is <20% regardless of treatment

AMNCH Tallaght
Gastric carcinoma
Patterns of disease spread:
Direct invasion: stomach wall, adjacent structures
local/regional/distant nodal metastases: lesser/greater curve, porta hepatis
haematogenous dissemination: liver, lungs
peritoneal spread (Krukenberg tumour of ovaries)
AMNCH Tallaght
Adenocarcinoma of the oesophago-gastric junction
Adenocarcinoma which crosses the junction of oesophagus and stomach, regardless of where the tumour bulk lies
(entirely above ogj: oesophageal carcinoma entirely below ogj: gastric carcinoma)
Typically a tumour of older malesIncreasing in frequency (gastric carcinoma decreasing)
Principal predisposing factor is GERD (not diet or HP gastritis)
Typically present late

AMNCH Tallaght
Other tumours of the stomach
Lymphoma:Low grade B cell MALT lymphoma
clonal B cell process related to chronic H Pylori infectionHigh grade B cell lymphoma
Carcinoid tumours
Stromal neoplasmstumours of muscle/nerve/vascular etc phenotype
Metastases

AMNCH Tallaght
Stomach: large B cell lymphoma
AMNCH Tallaght
Carcinoid tumours of stomach
1. Atrophic gastritis / Pernicious anaemiahypochlorhydria, antral G cell hyperplasia, Gastrin ,
ECL cell
2. Sporadic (G cell or ECL) not a/w hypochlorhdyria
3. Fundic ECL tumours in patients with Zollinger-Ellison syndrome
4. Poorly differentiated small cell carcinoma

AMNCH Tallaght

AMNCH Tallaght
Tumours of the small intestine
Small bowel: 75% of GIT, 6% of GIT tumours
Adenomas:majority occur in region of ampulla of Vaterprecursor of carcinoma in this location
AMNCH Tallaght
Tumours of the small intestine: Carcinoma
Adenocarcinoma:
Most occur in duodenum and jejunum
Most probably arise from precursor adenoma
Typical intestinal type adenocarcinomas
May obstruct/perforate/bleed/spread

AMNCH Tallaght
Ampullary carcinoma
AMNCH Tallaght
Tumours of the small intestine: Carcinoid Tumour
Carcinoid tumour:
origin from endocrine (APUD/Kultchitsky cells)
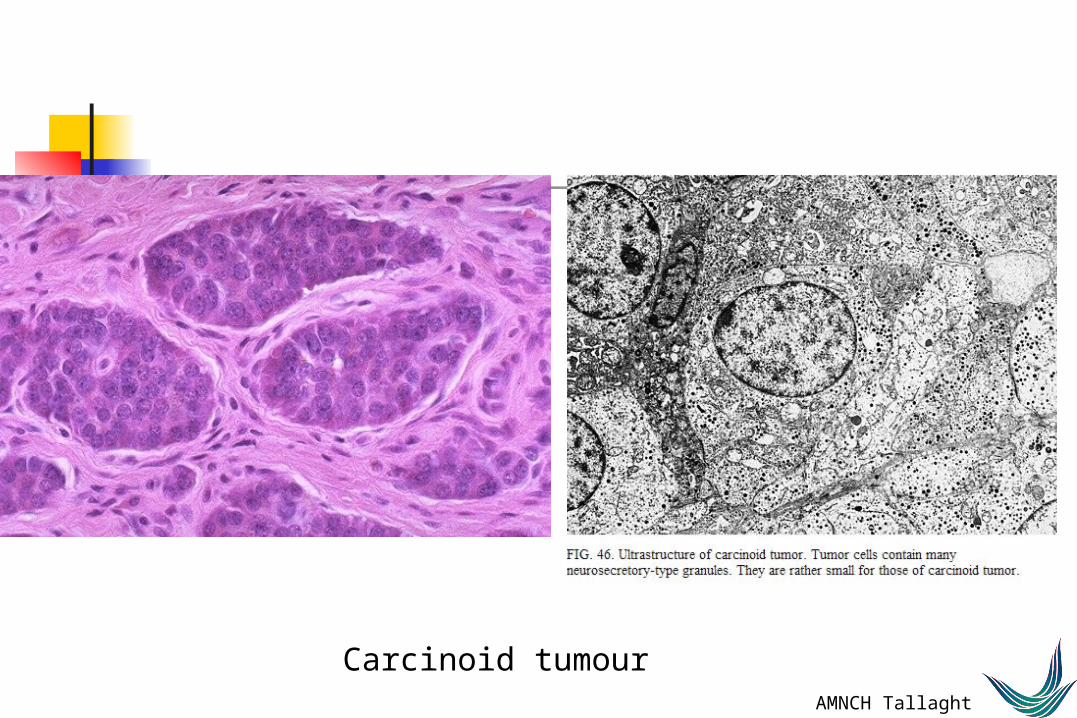
cells are neuroendocrine type, contain neurosecretory granules
may produce hormone and cause carcinoid syndrome
behaviour depends on depth of infiltration intra-mural: good prognosis, peritoneal involvement: poor prognosis

AMNCH Tallaght
Small intestinal carcinoid tumour
AMNCH Tallaght
Carcinoid tumour
AMNCH Tallaght
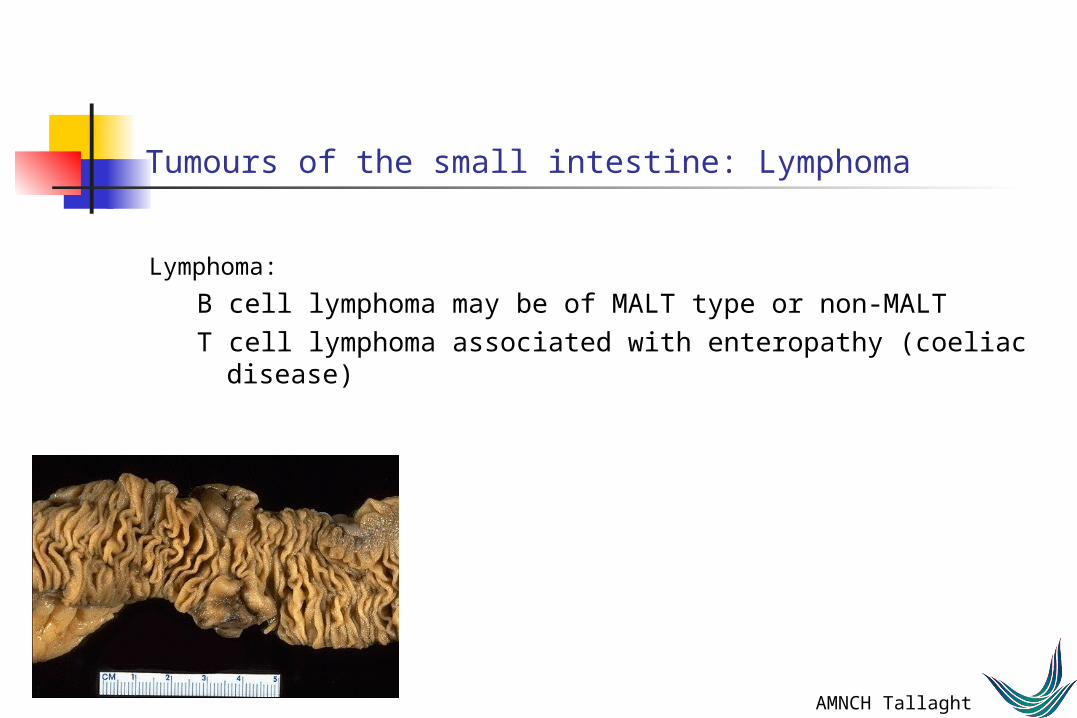
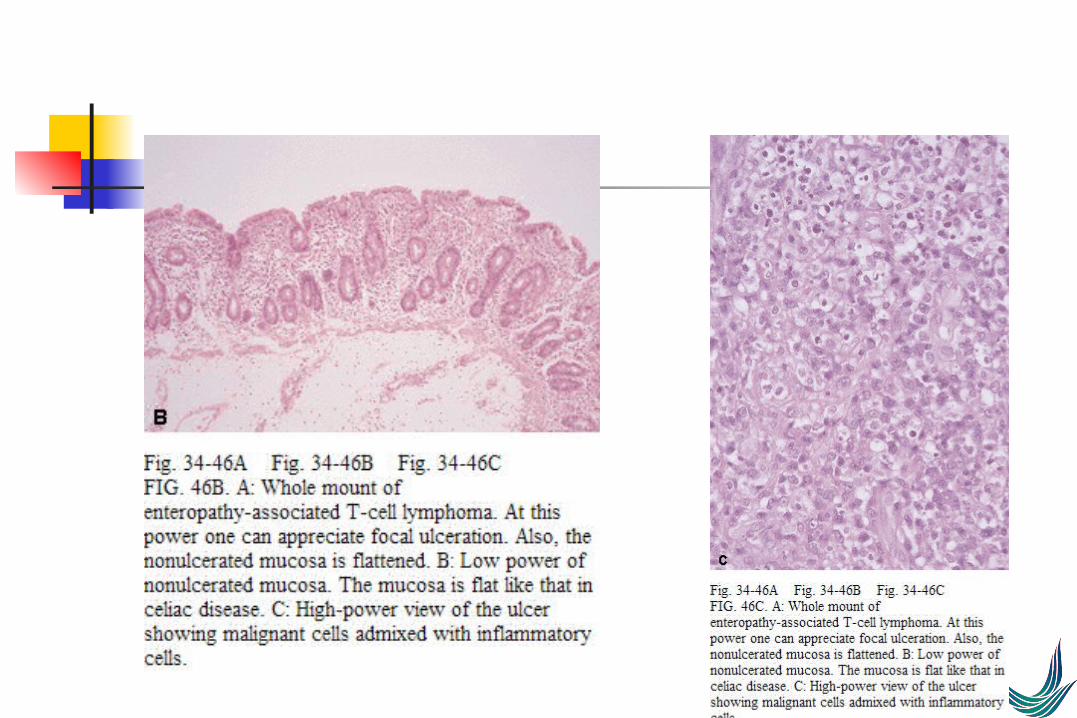
Tumours of the small intestine: Lymphoma
Lymphoma:
B cell lymphoma may be of MALT type or non-MALTT cell lymphoma associated with enteropathy (coeliac disease)
AMNCH Tallaght
AMNCH Tallaght
Tumours of the small intestine: Stromal tumours
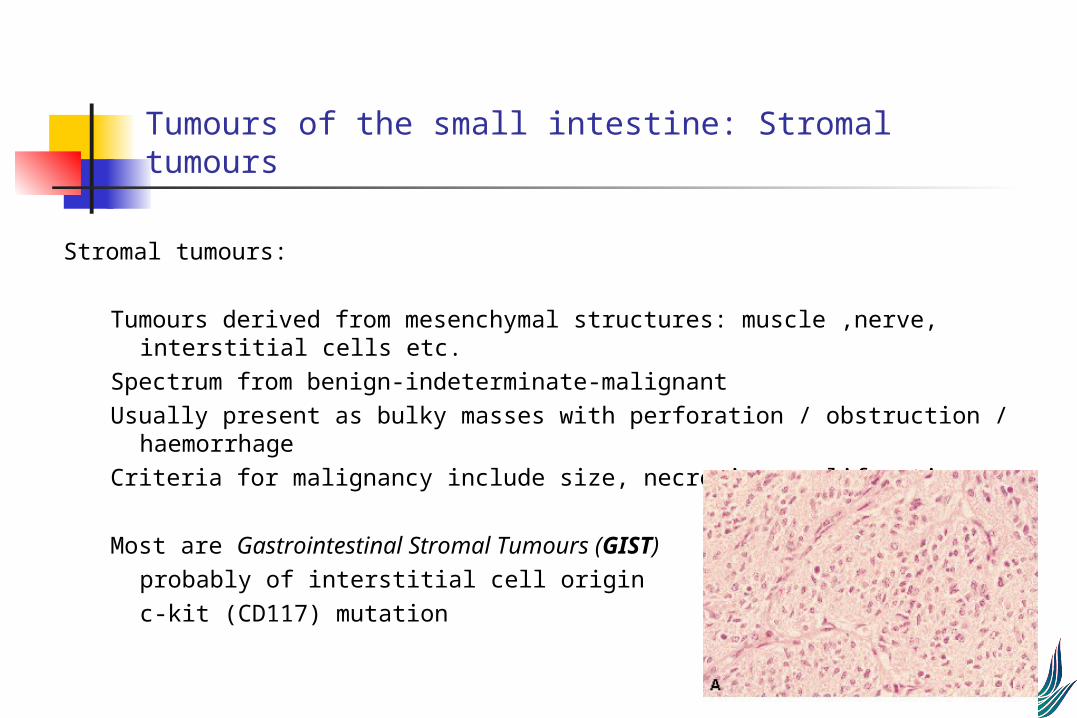
Stromal tumours:
Tumours derived from mesenchymal structures: muscle ,nerve, interstitial cells etc.
Spectrum from benign-indeterminate-malignantUsually present as bulky masses with perforation / obstruction /
haemorrhageCriteria for malignancy include size, necrosis, proliferation
Most are Gastrointestinal Stromal Tumours (GIST)probably of interstitial cell originc-kit (CD117) mutation

AMNCH Tallaght
Tumours of the appendix
Carcinoid tumour:
small, often at tip of appendixtypical carcinoid / goblet cell carcinoid
Mucinous neoplasms:
mucinous cystadenomamucinous cystadenocarcinomaMay be associated with Pseudomyxoma Peritoneii
AMNCH Tallaght
Colorectal Tumours
Polyps:
Hyperplastic (metaplastic)Inflammatory, Juvenile, Hamartomatous
AdenomatousSporadic / Hereditary syndromes

AMNCH Tallaght
Colorectal cancer
Risk factors / associations:Geography: industrialised societiesObesity, inactivityDiet: meat and refined carbohydratesfamily historyadenomatous polyps (sporadic/familial syndromes)ulcerative colitis
AMNCH Tallaght
Colorectal Carcinoma
>70% arise from adenomasadenoma incidence is ~ 30 -40%immediate family of affected patient: risk x 2-3
~ 2% arise on a background of ulcerative colitis
different genetic pathways to neoplasia:(1) adenoma - carcinoma sequence(2) hereditary non-polyposis mechanism(3) UC associated neoplasia

AMNCH Tallaght
Adenomatous polyps of the colon
Neoplastic polyps, precursors of carcinoma
Architectural patterns:Tubular/Villous/Tubulovillous
Gross presentation:sessile/pedunculated/flat adenoma
Risk of malignancy size (ras), architecture, dysplasia

AMNCH Tallaght
Colon: tubular adenoma

AMNCH TallaghtColon: adenomatous epithelium
AMNCH Tallaght
Colon: villous adenoma

AMNCH TallaghtColon: villous adenoma

AMNCH Tallaght
Colitis-associated neoplasia
UC increases risk x 2-8
Risk increased with - duration of disease - extent of disease
- presence of dysplasia
neoplasm evolves from dysplasia rather than adenoma
bcl-2 overexpression less frequent in UCAN
APC gene mutations much less frequent in UCAN
E-cadherin mutations more frequent in UCAN
AMNCH Tallaght
Colorectal carcinoma: Pathology
Virtually all are adenocarcinomas
Irish Cancer Registry 1996:
1784 cases (8.6% of all cancers, largest group apart from skin cancer), close to European average
Crude incidence 40% > in malesAge standardised incidence 75%> in males

AMNCH Tallaght
Colorectal carcinoma
Left > right side
Left side tend to be annular obstructing lesionsRight side tend to be polypoid exophytic
Intestinal type adenocarcinomas, range of differentiation: well- moderate –poor
+/- mucinous, neuroendocrine differentiation
Mucinous differentiation more common in right sided tumours, HNPCC association

AMNCH TallaghtColon: carcinoma

AMNCH Tallaght
Colon: carcinoma

AMNCH Tallaght
Colon: carcinoma

AMNCH Tallaght
Colon: adenocarcinoma

AMNCH Tallaght
Colorectal carcinoma
Infiltrate into and through wallmetastasize to regional nodesdisseminate through blood to liver, distant sites
prognosis is primarily dependent on stageStaging: Dukes’ A B C
Dukes’ variantsTNM
Accurate staging depends on pathological examination of resected specimen in conjunction with clinical and radiological information

AMNCH TallaghtColon cancer: staging
Dukes’ A
Dukes’ B

AMNCH TallaghtColon cancer: staging
Dukes’ C

AMNCH Tallaght
Colorectal carcinoma
Stage at diagnosis:Stage 1: <20%Stage 4 >20%
Cumulative survival probability: 1 yr 69%, 3yrs 51%
1yr: stage 1 90%, stage 4 30%3yr: stage 1 80%, stage 4 10%
AMNCH Tallaght
Objectives: GI tumour pathology
tumour nomenclature and classification
tumour aetiology and pathogenesisprecursor lesionsmechanisms of carcinogenesis in different tissuespotential points for prevention / modification
tumour growth and behaviourinvasionmetastasis
tumour stagingstaging systemsprognostic factors
Recommended