National Public Health Emergency Team
on Carbapenemase Producing Enterobacteriaceae (CPE)
Situational Analysis


National Public Health Emergency Team on CPE Situational Analysis
21 December 2017 1
Table of Contents
List of Tables ........................................................................................................................................... 2
List of Figures .......................................................................................................................................... 2
1. NPHET Chair’s Commentary ............................................................................................................ 3
2. Purpose of the situational analysis ................................................................................................. 4
3. Key NPHET Outputs to Date ............................................................................................................ 4
4. What is CPE ..................................................................................................................................... 4
5. Background to activation of the Public Health Emergency Plan ..................................................... 5
6. National Public Health Emergency Team (NPHET) .......................................................................... 5
7. Expert Group ................................................................................................................................... 6
8. CPE data sources and surveillance figures ...................................................................................... 6
Data sources ........................................................................................................................................ 6
Surveillance ......................................................................................................................................... 7
9. HSE Governance Structures ............................................................................................................ 8
10. HSE Policies, Procedures, Protocols and Guidelines (PPPGs) ......................................................... 9
11. Communications ........................................................................................................................... 10
12. Gaps and Next Steps ..................................................................................................................... 11
Key concepts ......................................................................................................................................... 12
Appendix 1: National Public Health Emergency Team Terms of Reference, Membership and Schedule
of 2017 Meetings .................................................................................................................................. 14
National Public Health Emergency Team Terms of Reference ......................................................... 14
National Public Health Emergency Team Membership .................................................................... 14
Schedule of meetings in 2017 ........................................................................................................... 15
Appendix 2: Hospital Groups (estimated population#) and Hospitals. ................................................. 16
Appendix 3: Community Health Organisations (CHOs) ........................................................................ 18

National Public Health Emergency Team on CPE Situational Analysis
21 December 2017 2
List of Tables Table 1: Key NPHET Outputs to Date ...................................................................................................... 4
HSE Business Intelligence Unit ................................................................................................................ 6
Table 2: Hospital Groups. Newly detected patients with CPE. Numbers. 2016 and 2017 Jan-Nov. ...... 7
Table 3: Hospital Groups. Screening for CPE and newly detected patients with CPE. Numbers.
October 2017 .......................................................................................................................................... 8
Table 4: Hospital Groups and CHOs. Status of IPC and IPC and Antimicrobial Stewardship Committee
9
Table 5: HSE CPE related PPPGs and Target Audience. ........................................................................ 10
Table 6: Gaps and Next steps ................................................................................................................ 11
List of Figures Figure 1: Total number of newly detected patients with CPE 2012-2017 (Jan-Nov).............................. 7

National Public Health Emergency Team on CPE Situational Analysis
21 December 2017 3
1. NPHET Chair’s Commentary
The National Public Health Emergency Plan was activated on 25 October 2017 as response to the
increase and spread of Carbapenemase Producing Enterobacteriaceae (CPE) in Ireland. As a result a
National Public Health Emergency Team was convened and they have been meeting on a weekly
basis since 02 November.
The initial focus of the group has been to gather information to identify current practice in relation
to the surveillance and management of CPE in Ireland. In order to understand the scale of CPE in
Ireland and the HSE’s response capacity, the HSE have been asked to provide information on
governance arrangements, response capacity, surveillance, flows of information and levels of
implementation of action plans and national requirements.
The information gathering process has been slower than anticipated and we are not at a stage yet to
understand the true scale of the problem and the response capacity within the HSE. While some
hospital groups have made progress in 2017 on a number of CPE related issues, including more
screening, this progress has been variable. The HSE have reviewed and strengthened their
governance and implementation oversight arrangements since the National Public Health
Emergency Team was convened. However, quantification of gaps in surveillance and provision of
business cases to respond to these gaps are awaited.
Given the time sensitive nature of this issue, it is of concern to note that we are not in a position to
have a more comprehensive picture of the current situation. In particular, this applies to the actions
the HSE has taken, the impact of those actions, and the plans put in place by the HSE to date in
response to this issue.
- Dr Tony Holohan, Chair of the CPE - National Public Health Emergency Team

National Public Health Emergency Team on CPE Situational Analysis
21 December 2017 4
2. Purpose of the situational analysis The purpose of this situational analysis is to provide an overview of the information gathered via the
National Public Health Emergency Team process to date. It includes the key outputs achieved, the
current CPE figures, governance arrangements, gaps identified and resulting next steps.
Further analysis will be carried out at hospital level to inform the work of NPHET. A situational
analysis report will be published on a monthly basis.
3. Key NPHET Outputs to Date Table 1: Key NPHET Outputs to Date
Key Outputs of NPHET to Date
1 Increased measurement and collation of various data collection bodies related to screening and identification of CPE patients
2 Increased focus on securing timely data from all clinical laboratories on the number of CPE colonised or infected patients
3 Increased communication from HSE to service providers regarding the current national Policies, Procedures, Protocols and Guidance (PPPG)
4 Initial measurement of the implementation of some of those national guidance documents/PPPGs
5 Increased clarity and strengthening of HSE governance arrangements for HCAI/AMR
4. What is CPE Carbapenemase-producing Enterobacteriaceae (CPE) is the newest in a long line of ‘superbugs’ or
bacteria that are hard to kill with antibiotics and are a particular problem in hospital settings. Of all
the superbugs, CPE is the most difficult to kill with antibiotics.
The World Health Organisation (WHO), Centre for Disease Control and the European Centre for
Disease Prevention and Control (ECDC) all identify that infections with CPE are a serious threat to
patient safety due to their resistance to multiple antimicrobials, meaning that there are very few
treatment options for infected patients. Patients infected with CPE experience poorer patient
outcomes, increased morbidity, mortality and have higher associated hospital costs.
The HSE’s National CPE Action Plan (HSE, 2017) identifies several factors that are contributing to the
rise in CPE in Irish health care settings including:
1. Inappropriate antibiotic prescribing in hospitals, primary care, and nursing homes
2. Understaffing and overcrowding in hospitals and other healthcare settings
3. Lack of adherence to standard infection prevention and control practices by healthcare workers in
hospitals, nursing homes and primary care
4. Lack of availability of suitable isolation facilities at ward level and in Emergency Departments
5. Poor infrastructure and design in hospitals

National Public Health Emergency Team on CPE Situational Analysis
21 December 2017 5
6. Suboptimal screening, surveillance and information/IT systems to support timely communication
tracking and flagging of patients with CRE, their contacts and other Multidrug resistant organisms
(MDROs)
7. Shortage of infection control specialists (medical, nursing, pharmacists, medical scientists) at
community, hospital, and national levels
8. Inadequate environmental hygiene and decontamination of patient care equipment
9. Lack of active screening for CPE in a number of hospitals
10. Undefined clarity around indications for screening in non-acute healthcare facilities
11. Lack of awareness in general public and healthcare workers
5. Background to activation of the Public Health Emergency Plan Cases of CPE have been reported throughout the world in recent years. Ireland has seen an increase
in the number of cases year on year. The number of cases almost doubled in 2016 to 282 cases and
is estimated to increase by a third in 2017, (401 in the period from January to November). The
spread of this superbug in hospitals can lead to the closure of beds, wards and units removing
thereby, essential capacity to provide services, to admit patients from Emergency Departments and
to address waiting lists effectively.
International experience indicates that CPE and antimicrobial resistance (AMR) need to be tackled at
a national level. In March 2017, the HSE Leadership Team decided to escalate the increasing CPE risk
and to put in place a national management plan in response. In May, a National Clinical Lead was
appointed and a National Response Team was established and the Director General wrote to
National Directors, Hospital Group CEOs and Community Healthcare Organisation Chief Officers
setting out the national and local response required across the health service. Implementation of
governance and screening requirements commenced with screening levels increasing since then,
however implementation varied nationally.
In October, there was further escalation of the issue from the Director General to the Minister for
Health, Mr Simon Harris, T.D., and from the Health Information and Quality Authority (HIQA) to the
Chief Medical Officer, Dr Tony Holohan. On the advice of the Chief Medical Officer, Dr Tony
Holohan, and in consultation with the National Patient Safety Office the Minister activated the
National Public Health Emergency Plan on 25 October 2017 in response to CPE in Ireland and a
National Public Health Emergency Team was convened as a result.
6. National Public Health Emergency Team (NPHET) The NPHET was convened on 02 November 2017 and have met on a weekly basis. Their role is to
provide advice, guidance, support and direction on the surveillance and management of CPE at
national level; the development and implementation of a strategy to contain CPE and provide
oversight. Membership of the team includes key stakeholders from the Department of Health, the
Health Service Executive (HSE) management with responsibility for public health, surveillance,
operations and quality assurance and patient representatives. Appendix 1 includes their Terms of
Reference, membership and schedule of meetings in 2017.
National Public Health Emergency Team on CPE Situational Analysis
21 December 2017 6
The work of the NPHET to date has been focused on gathering information to inform a situational
analysis including information on levels of screening and number of patients with CPE, policies and
procedures and governance arrangements at national, regional (Hospital Group and Community
Health Organisation) level and in individual facilities. This report provides the current situational
analysis.
7. Expert Group On the direction of NPHET an Expert Group has been convened. This group will monitor and review
national and international research and developments in relation to CPE and provide expert advice
to the NPHET team. This group held their first meeting on 04 December and as a priority they are
assuring the HSE’s screening policy and CPE outbreak management procedure are in line with
current international best practice.
8. CPE data sources and surveillance figures
Data sources
Health Protection Surveillance Centre (HPSC): The HPSC produces a quarterly report which gives
information on the number patients (based on 1st isolate) infected with CPE in Ireland each quarter.
Hospitals are currently not mandated to submit data to the HPSC on their CPE patients. This report
gives specifics as to the organism type of CPE found.
HPSC submits information to the European EARS-Net system biannually. This system collects
laboratory antimicrobial resistance data on the number of blood stream infection from a number of
pathogens including E. coli and Klebsiella pneumoniae (two organisms that in which antimicrobial
resistance, including carbapenem resistance, is of concern). The EARS-Net system was designed to
monitor overall antimicrobial resistance in key pathogens to monitor major trends over time. It was
not designed to collect data in a time frame intended for performance management or to guide
immediate public health action.
CPE Reference Laboratory Service (CPEaRLS): The Reference Laboratory, based at University
Hospital Galway, was established in 2012. CPEaRLS receives isolates from clinical laboratories for
confirmation as CPE and for further typing. The submitted isolates arrive with additional information
on the patient’s clinical details and the patient’s location (long term care facility, hospital, other,
etc). Submitting isolates to CPEaRLS is voluntary but all clinical laboratories submit isolates and
almost all do so in a timely manner. At present the CPE reference laboratory provides monthly
report on the number of new patients (and isolates, including microbiological information on the
type of bacteria).
HSE Business Intelligence Unit: As of August 2017, the BIU collects data relating to CPE in public
hospitals from hospital managers. This includes information on the number of CPE screening tests
done, number of confirmed CPE patients (either infected or colonised), the management/isolation of
CPE patients and the amount of one specific antibiotic (meropenem) used. Hospitals return data on

National Public Health Emergency Team on CPE Situational Analysis
21 December 2017 7
a monthly basis. As this information is at the beginning stages of collection, the quality and
frequency of the data collection from all hospitals is still improving.
This information is helpful to compare to CPEaRLS data, as one gives information on the number of
screening tests done and the other gives information on the number of patients confirmed to have
CPE for the same time periods/frequencies.
Surveillance
Figure 1 shows the number of newly detected patients with CPE from 2012 to 2017 (January to
November). It also provides a breakdown of the different types of CPE identified. OXA-48, KPC and
NDM-1 have been the most frequent type of CPE detected. There has been a year-on-year increase
from five patients in 2012 (October to December only) to 401 in 2017 (January to November only).
This increase is partly attributable to an increase in screening.
Figure 1: Total number of newly detected patients with CPE 2012-2017 (Jan-Nov)
Source: CPE Reference Laboratory Data
Table 2 shows the total number of newly detected patients with CPE in each Hospital Group in 2016
and in 2017 (January to November). Variation across hospital groups may be partly attributable to
the size and type of hospitals in the hospital group, the patient cohort and levels of screening across
the hospitals. See Appendix 2 for a list of all hospitals by Hospital Group.
Table 2: Hospital Groups. Newly detected patients with CPE. Numbers. 2016 and 2017 Jan-Nov.
Hospital Group 2016 Jan-Nov 2017
University Limerick Hospital Group 29 50
Children's Hospital Group 3 4
South/Southwest Hospital Group 22 33
Saolta Hospital Group 41 48
RCSI Hospital Group 9 34
0
50
100
150
200
250
300
350
400
450
2012 2013 2014 2015 2016 2017 (Nov)
IMI
OXA-48
NDM-1
VIM
IMP
KPC
National Public Health Emergency Team on CPE Situational Analysis
21 December 2017 8
Hospital Group 2016 Jan-Nov 2017
Ireland East Hospital Group 28 56
Dublin Midlands Hospital Group 138 143
Other Healthcare Facilities (primarily private hospitals) 13 33
National Total 283 401 Source: CPE Reference Laboratory Data
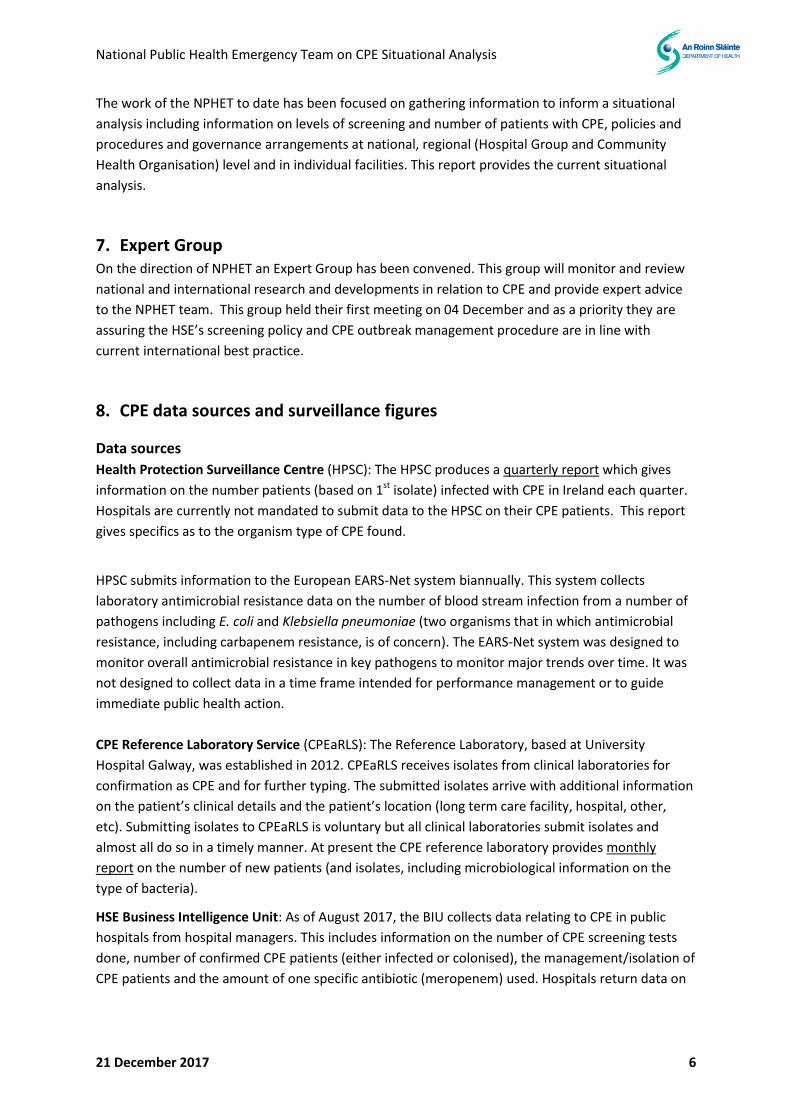
Table 3 shows the total number of CPE screenings that were reported to the HSE’s Business
Intelligence Unit in October (November data was not available at the time of writing this report) and
the total number of newly detected patients with CPE confirmed by the CPE Reference Laboratory
across each of the hospital groups. Variation across hospital groups may be partly attributable to the
size and type of hospitals in the hospital group, the patient cohort and implementation of screening
guidelines across the hospitals within a hospital group.
Table 3: Hospital Groups. Screening for CPE and newly detected patients with CPE. Numbers. October 2017
Hospital Group Reported CPE screening ~
Newly detected patients #
University Limerick Hospital Group 1043 4
The Children’s Hospital Group 383 0
South/South West Hospital Group 381 1
Saolta Hospital Group 1395 6
Royal College of Surgeons Ireland Hospital Group 1078 9
Ireland East Hospital Group 1967 3
Dublin Midlands Hospital Group 3574 13
Total 9821 36 ~ Source: Reported screening HSE Business Intelligence Unit (BIU) data.
# Source: Newly detected patients CPE Reference Laboratory data.
9. HSE Governance Structures The NPHET has been seeking assurances from the HSE in relation to the governance and oversight
for managing CPE.
At a national level, the HSE’s HCAI/AMR National Taskforce was established in 2016, they developed
a CPE Action Plan which was approved by HSE Leadership in March 2017. As a result, a National CPE
Response Team, led by a HCAI/AMR Clinical Lead, was established in May. This group was
responsible for implementation of the CPE Action Plan. In December, the HSE advised the NPHET of
their plans to strengthen this structure to ensure an operational focus. The National Response Team
will be subsumed into an Implementation Team which will include both a Clinical Lead and an
Operational Lead.
At a regional level, the HSE’s HCAI/AMR Clinical Lead has recommended that an Infection Prevention
and Control (IPC) and Antimicrobial Stewardship Committee should be established at Hospital Group
and CHO level to ensure robust governance in relation to CPE and wider healthcare acquired

National Public Health Emergency Team on CPE Situational Analysis
21 December 2017 9
infections (HCAIs) and antimicrobial resistance (AMR). On the direction of NPHET, information was
initially gathered from all Hospital Groups and CHOs on the status of these committees. Table 4
provides an overview of responses from Hospital Groups and CHOs (see Appendix 3 for areas
covered by each CHO). The HSE are in the process of preparing an operational response to the
current governance arrangements.
The next phase of data collection will be focused on governance structures at local level within
individual hospitals. The group will then examine the feasibility of gathering data from long-term
care facilities.
Table 4: Hospital Groups and CHOs. Status of IPC and IPC and Antimicrobial Stewardship Committee
Hospital Group/CHO IPC and Antimicrobial Stewardship Committee currently in place
Dublin Midlands Hospital Group Yes
Ireland East Hospital Group Yes
Royal College of Surgeons Ireland Hospital Group
No (Quality and Patient Safety Committee at group level and IPC Committee at hospital level)
Saolta Hospital Group Yes
South/South West Hospital Group No (plan to establish and first meeting in January 2018)
The Children’s Hospital Group No (Committees at hospital level)
University Limerick Hospital Group Yes
Dublin Midlands Hospital Group Yes
CHO 1 Yes
CHO 2 Yes
CHO 3 No (CHO wide Quality and Patient Safety committee)
CHO 4 Yes
CHO 5 Yes
CHO 6 No (did previously exist, priority to re-establish)
CHO 7 Yes
CHO 8 Yes
CHO 9 Yes
10. HSE Policies, Procedures, Protocols and Guidelines (PPPGs) The HSE have developed a number of CPE related PPPGs in 2017. These documents have been
disseminated within the HSE and published on the HSE’s website. Table 5 includes the CPE related
PPPG documents provided by the HSE to the NPHET.
Screening is required in order to detect, manage and control CPE in a healthcare setting. The HSE
have reported to NPHET that, based on current figures been reported to the HSE’s Business
Intelligence Unit, there is variation in the implementation of the National CPE Screening Policy
across hospital groups and individual hospitals.

National Public Health Emergency Team on CPE Situational Analysis
21 December 2017 10
Table 5: HSE CPE related PPPGs and Target Audience.
Target Audience
PPPG type/name Hospitals Long Term Care Facilities
GPs Public/ Patients
Requirements for screening of Patients for Carbapenemase Producing Enterobacteriaceae (CPE) in the Acute Hospital Sector
●
Out-Patient and Day Care and Hospital Visiting for People Colonised with Antimicrobial Resistant Organisms (AMRO) Including Carbapenemase Producing Enterobacteriaceae (CPE)
● ●
Provisional Guidance relating to Interfacility Transfer of Patients Colonised or Infected with Antimicrobial Resistant Organisms (AMRO) Including Carbapenemase Producing Enterobacteriaceae (CPE)
● ●
Provisional Guidance relating to Healthcare Workers Colonised with CPE
● ●
Response to Requests for Advice on use of Hydrogen Peroxide Vapour and similar technologies for environmental decontamination in the context of Carbapenemase Producing Enterobacteriaceae
● ●
Provisional Guidance relating to CPE for General Practice
●
Provisional Guidance relating to CPE for Long Term Care Facilities (Residential Non Acute Care Settings)
●
You have questions about CPE and CRE? ●
11. Communications The Department of Health have a dedicated webpage on their website where minutes of NPHET
meetings and related documents are published. A press release has been issued after each meeting
to communicate the items discussed and actions agreed. The Department of Health has briefed the
Government Task Force on Emergency Planning and the National Health Threats Coordination Group
on the work of NPHET.
http://health.gov.ie/national-patient-safety-office/patient-safety-surveillance/antimicrobial-
resistance-amr-2/public-health-emergency-plan-to-tackle-cpe/
The HSE have a dedicated HCAI webpage which includes a section on CPE on their website. An
updated version was published on 08 December 2017. The HSE have appointed a HCAI/AMR
Communications Lead.
http://hse.ie/eng/about/Who/healthwellbeing/Our-Priority-Programmes/hcai/resources/cpe/

National Public Health Emergency Team on CPE Situational Analysis
21 December 2017 11
12. Gaps and Next Steps Table 5 provides an overview of the gaps identified to date and the next steps planned.
Table 6: Gaps and Next steps
Gaps Next steps
CPE is not on the list of notifiable diseases therefore reporting in not currently mandatory. This has an impact on the completeness and timeliness of current data.
The Department of Health are preparing an Statutory Instrument to provide for the addition of CPE colonisation to the list of notifiable diseases. The background preparatory work is currently underway by the Health Protection Surveillance Centre.
Variance in implementation of national requirements including national screening policy.
Map requirements, standards and key activities in the various action plans to focus on implementation of interventions. These include:
Ireland’s National Action Plan on Antimicrobial Resistance 2017-2020 (iNAP)
HSE CPE Action Plan
HSE HCAI/AMR Action Plan
HIQA hygiene standards and recommendations in the review of antimicrobial stewardship
Gather data on implementation of requirements from hospitals and CHOs.
Expert Group to assure national screening policy and outbreak management are in line with current international best practice.
Operational response from the HSE.
There is no national IT surveillance system in place. ICNET is not in all hospital. There have been delays in the roll out of MedLIS.
Identify gaps in IT surveillance systems to develop a business case.
Issues in relation to data completeness and timeliness including:
Limited CPE data from long-term care
facilities
Gaps in data on use of resources in hospitals and CHO settings
Multiple data collection streams including the National CPE Reference Laboratory, the Health Protection Surveillance system and HSE’s Business Intelligence Unit.
Gather data from hospitals, Community Health Organisations (CHOs) and long term care facilities (LTCFs) on IPC governance arrangements, use of resources and implementation of requirements.
CPE KPI included in the HSE’s 2018 Service Plan and Scorecard.
Further analysis will be carried out at hospital level to inform the work of NPHET. A situational
analysis report will be published on a monthly basis.

National Public Health Emergency Team on CPE Situational Analysis
21 December 2017 12
Key concepts
What is a public health emergency?
A public health emergency is described as any serious or unexpected event, due to an infectious
disease, which causes, or threatens to cause, death or serious illness to large sections of the
population, an individual region or a specific cohort of individuals and which will have a major
impact on the normal functioning of the health system and on society in general.
What is the Public Health Emergency Plan?
The Department of Health’s National Health Emergency Plan is a plan for activation in the event of a
national/large-scale public health emergency in the event of an infectious disease outbreak or
similar health issue. The purpose of the plan is to assist all health agencies in the State to respond to
a public health emergency in an integrated and co-ordinated manner.
What are Healthcare Associated Infections (HCAIs)?
A healthcare-associated infection is an infection that is acquired after contact with the healthcare
services. This is most frequently after treatment in a hospital, but can also happen after treatment in
outpatient clinics, nursing homes and other healthcare settings. Healthcare-associated infections
that are picked up in hospital are also known as “hospital-acquired infections”.
The five most common HCAIs are:
Surgical site infection
Pneumonia
Urinary tract infection
Bloodstream infection
Gastroenteritis.
What is Antimicrobial Resistance (AMR)?
Antimicrobials are medicines used to treat infections or disease, and are essential in both human
and animal health. Antimicrobial resistance occurs when an antimicrobial that was previously
effective, is no longer effective to treat an infection or disease caused by a microorganism.
The development of resistance is a natural phenomenon that will inevitably occur when
antimicrobials are used to treat disease. The problem at present is that the sheer volume of
antimicrobials being used globally in humans, animals and in other situations is leading to significant
increases in the rate of development of resistance with the result that common infections are
becoming more difficult to treat and microorganisms that are resistant to many antimicrobials, so
called ‘superbugs’, are emerging.
National Public Health Emergency Team on CPE Situational Analysis
21 December 2017 13
What is the difference between antibiotic and antimicrobial resistance?
Antibiotic resistance refers specifically to the resistance developed by bacteria to antibiotics.
Antimicrobial resistance is a broader term, encompassing resistance to drugs to treat infections
caused by other microbes, such as mycobacteria (e.g. M. tuberculosis), parasites (e.g. malaria),
viruses (e.g. HIV) and fungi (e.g. Candida spp. and Aspergillus spp.)
What is Antimicrobial stewardship?
Antimicrobial stewardship is a systematic approach to optimising antimicrobial therapy, through a
variety of structures and interventions. Antimicrobial Stewardship includes not only limiting
inappropriate use but also optimising antimicrobial selection, dosing, route, and duration of therapy
to maximise clinical cure, while limiting the unintended consequences, such as the emergence of
resistance, adverse drug events, and cost.
What is the National Action on Antimicrobial Resistance 2017-2020 (iNAP)?
Ireland’s National Action Plan on Antimicrobial Resistance 2017-2020 aims to implement policies and
actions to prevent, monitor and combat AMR across the health, agricultural and environmental
sectors. Reducing the inappropriate use of antimicrobial medicines, as well as preventing infections
and disease, is vital to stop the development and spread of resistant microorganisms.
It provides an overview for the health, agricultural and environmental sectors. It presents key
strategic interventions for tackling antimicrobial resistance in line with World Health Organisation
(WHO) requirements across the three sectors. These interventions represent Ireland’s commitment
to the development and implementation of a holistic, cross-sectoral ‘One Health’ approach to the
problem of antimicrobial resistance.

National Public Health Emergency Team on CPE Situational Analysis
21 December 2017 14
Appendix 1: National Public Health Emergency Team Terms of Reference,
Membership and Schedule of 2017 Meetings
National Public Health Emergency Team Terms of Reference
1. Oversee and provide expert advice, guidance, support and direction for the overall national
response to CRE, including national and regional and other outbreak control arrangements.
2. Direct the collection and analysis of required data and information and the subsequent reports
to NPHET.
3. Conduct an on-going situational analysis and evaluation having regard to reports received,
expert advice, international guidance and assurance regarding optimal use of resources.
4. Liaise with relevant organisations and stakeholders, to include other Government departments,
statutory and voluntary agencies, international bodies and the relevant regulators.
5. Direct and ensure an effective communications system at local, regional and national levels.
6. Evaluate on an on-going basis the readiness of the health service to manage and sustain the
containment of CPE as part of ordinary operations with a view to standing down the NPHET at
the appropriate time.
National Public Health Emergency Team Membership
Name Job Title Organisation
Dr Tony Holohan (Chair) Chief Medical Officer Department of Health
Dr Kathleen Mac Lellan
Director, National Patient Safety Office (NPSO)
Department of Health
Ms Anna Cunniffe Acute Hospitals Policy Division Department of Health
Ms Sandra Walsh Primary Care Division Department of Health
Ms Bernie O’Reilly Patient Representative Patients for Patient Safety
Ms Brigid Doherty Patient Representative Patient Focus
Mr John Connaghan Chief Operations Officer Health Service Executive
Mr Patrick Lynch National Director, Quality Assurance and Verification Division
Health Service Executive
Professor Martin Cormican HCAI National Clinical Lead Health Service Executive
Mr Tom McGuinness Emergency Management & National Ambulance Service
Health Service Executive
Dr Kevin Kelleher AND Public Health and Director (acting) Health Protection Surveillance Centre (HPSC)
Health Service Executive
Ms Audrey Lambourn
Client Director HCAI/AMR Clinical Programme
Health Service Executive

National Public Health Emergency Team on CPE Situational Analysis
21 December 2017 15
Schedule of meetings in 2017
Meeting number Date of meeting
1. 02 November 2017
2. 09 November 2017
3. 16 November 2017
4. 23 November 2017
5. 30 November 2017
6. 07 December 2017
7. 14 December 2017
8. 21 December 2017

National Public Health Emergency Team on CPE Situational Analysis
21 December 2017 16
Appendix 2: Hospital Groups (estimated population#) and Hospitals.
Hospital Group Hospital name
Dublin Midlands Hospital Group (800,000) Midlands Regional Hospital Portlaoise
Midlands Regional Hospital Tullamore
Naas General Hospital
St James' Hospital
St Luke’s Radiation Oncology Network
The Adelaide & Meath Hospital Tallaght
The Coombe Women & Infant University Hospital
Ireland East Hospital Group (1,000,000) Cappagh National Orthopaedic Hospital
Mater Misercordiae University Hospital
Midland Regional Hospital Mullingar
National Maternity Hospital
Our Lady's Hospital Navan
Royal Victoria Eye and Ear Hospital
St Columcille's Hospital Loughlinstown
St Luke's General Hospital Kilkenny
St Michael's Hospital Dun Laoghaire
St Vincent's University Hospital
Wexford General Hospital
RCSI Hospitals Group (800,000) Beaumont Hospital
Cavan General Hospital
Connolly Hospital Blanchardstown
Louth County Hospital Dundalk
Monaghan Hospital
Our Lady of Lourdes Hospital Drogheda
Rotunda Hospital
Saolta Hospital Group (700,000) Letterkenny University Hospital
Mayo General Hospital
Portiuncula Hospital
Roscommon County Hospital
Sligo Regional Hospital
University Hospital Galway & Merlin Park University Hospital
South/South West Hospital Group (850,000) Bantry General Hospital
Cork University Hospital/Cork University Maternity Hospital
Lourdes Orthopaedic Hospital Kilcreene
Mallow General Hospital
Mercy University Hospital
South Infirmary Victoria University Hospital

National Public Health Emergency Team on CPE Situational Analysis
21 December 2017 17
Hospital Group Hospital name
South Tipperary General Hospital
University Hospital Kerry
University Hospital Waterford
The Children's Hospital Group National Children's Hospital Tallaght
Our Lady's Hospital for Sick Children Crumlin
Temple Street Children's University Hospital
University of Limerick Hospital Group (400,000) Croom Hospital
Ennis Hospital
Nenagh Hospital
St John's Hospital Limerick
University Hospital Limerick
University Maternity Hospital Limerick # Source: The Establishment of Hospital Groups as a transition to Independent Hospital Trusts
(Department of Health, 2013)

National Public Health Emergency Team on CPE Situational Analysis
21 December 2017 18
Appendix 3: Community Health Organisations (CHOs)
CHO name CHO Area
CHO1 Donegal, Sligo/Leitrim/West Cavan and Cavan/Monaghan
CHO2 Galway, Roscommon and Mayo
CHO3 Clare, Limerick and North Tipperary/East Limerick
CHO4 Kerry, North cork, North Lee, South Lee and West Cork
CHO5 South Tipperary, Carlow/Kilkenny, Waterford and Wexford
CHO6 Wicklow, Dun Laoghaire and Dublin South
CHO7 Kildare/West Wicklow, Dublin West, Dublin South City and Dublin South West
CHO8 Laois/Offaly, Longford/Westmeath, Louth and Meath
CHO9 Dublin North, Dublin North Central and Dublin North West
Recommended