MOOD DISORDERSMOOD DISORDERS
HYACINTH C. MANOOD, MD, DPBPHYACINTH C. MANOOD, MD, DPBP
• Mood is a pervasive and sustained feeling tone that is experienced internally and that influences a person's behavior and perception of the world.
• Affect is the external expression of mood.
• A syndrome consisting of a cluster of signs and symptoms sustained over weeks to months, which represent a marked departure from a person’s functioning, and tend to recur, often in periodic or cyclical fashion.
• MAJOR DEPRESSIVE DISORDERS – major depressive episodes only; unipolar depression
• BIPOLAR 1 DISORDER – both manic and depressive episodes or manic episodes alone ( unipolar, pure or euphoric mania)
• BIPOLAR 2 DISORDER – both hypomanic and depressive episodes
• DYSTHYMIC DISORDER – at least 2 years of depressed mood that is not severe enough to fit the diagnosis of MDD
• CYCLOTHYMIC DISORDER – at least 2 years of hypomanic symptoms
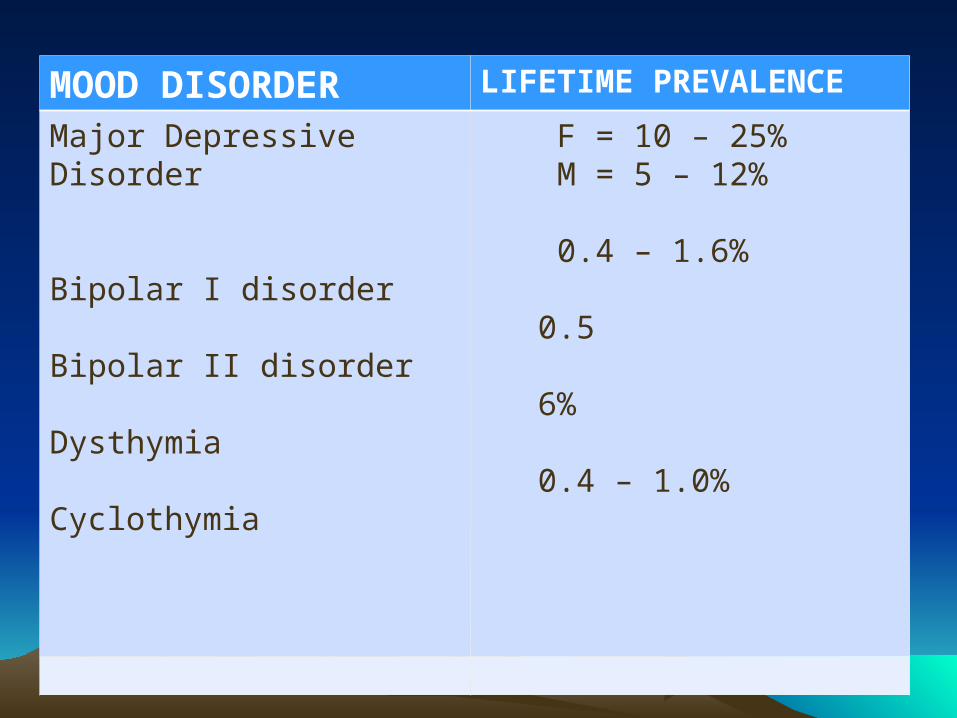
MOOD DISORDER LIFETIME PREVALENCE
Major Depressive Disorder
Bipolar I disorder
Bipolar II disorder
Dysthymia
Cyclothymia
F = 10 – 25% M = 5 – 12%
0.4 – 1.6%
0.5
6%
0.4 – 1.0%
• twofold greater prevalence of major depressive disorder in women than in men.
• bipolar I disorder has an equal prevalence among men and women.
• Manic episodes are more common in men, and depressive episodes are more common in women
• onset of bipolar I disorder is earlier than that of major depressive disorder
• mean age of 30 for bipolar I disorder ; mean age of onset for major depressive disorder is about 40 years
• most often in persons without close interpersonal relationships or in those who are divorced or separated
• higher than average incidence of bipolar I disorder is found among the upper socioeconomic groups;
• increased risk of having one or more additional comorbid Axis I disorders - alcohol abuse or dependence, panic disorder, obsessive-compulsive disorder (OCD), and social anxiety disorder
• Comorbid substance use disorders and anxiety disorders worsen the prognosis of the illness and markedly increase the risk of suicide
ETIOLOGYETIOLOGY
I. Biological FactorsA. Biogenic Amines
1. NOREPINEPHRINE - downregulation or decreased
sensitivity of ß-adrenergic receptors ; presynaptic ß2- receptors
2. SEROTONIN- most commonly associated with depression- depletion of serotonin may precipitate depression
3. DOPAMINE
- reduced in depression; increased in mania; D1 receptors and mesolimbic dopamine pathway.
4. OTHERS
- Abnormal levels of choline
- Reductions of GABA - G proteins or other second messengers. - Hypercortisolema
- elevated basal thyroid-stimulating hormone (TSH) level or an increased TSH response to a 500-mg infusion of the hypothalamic neuropeptide thyroid-releasing hormone (TRH).
- Decreased CSF somatostatin levels have been reported in depression, and increased levels have been observed in mania.
B. Alterations of Sleep Neurophysiology
(1) an increase in nocturnal awakenings, (2) a reduction in total sleep time, (3) increased phasic rapid eye movement (REM) sleep, (4) increased core body temperature
- reduced REM latency
• KINDLING - the electrophysical process in which repeated subthreshold stimulation of a neuron eventually generates an action potential; “kindling in the temporal lobes”;
• NEUROANATOMY:- limbic system, basal ganglia and the hypothalamus
C. Genetic
- if one parent has a mood disorder, a child will have a risk of between 10 and 25 percent for mood disorder.
II. Psychosocial Factors
1. Life Events and Environmental Stress - The life event most often associated with development of depression is losing a parent before age 11.
- The environmental stressor most often associated with the onset of an episode of depression is the loss of a spouse.
2. Personality Factors- Persons with certain personality disorders: OCD, histrionic, and borderline, may be at greater risk for depression
3. Cognitive Theory Aaron Beck postulated a cognitive triad of depression that consists of :(1) views about the self : a negative self-precept;(2) about the environment: a tendency to experience the world as hostile and demanding, and(3) about the future : the expectation of suffering and failure.
4. Learned Helplessness
- internal causal explanations are thought to produce a loss of self-esteem after adverse external events. - cognitive motivational deficit and emotional deficit
DIAGNOSISDIAGNOSIS
• DSM IV – TR CRITERIA
> Mood changes
> Specified period of time
> Change in activity level, cognitive abilities, and vegetative functions;
> Impaired interpersonal, social and occupational functioning
> Exclusion criteria
Major Depressive EpisodeMajor Depressive Episode A. Five (or more) of the following symptoms have been present during
the same 2-week period and represent a change from previous functioning; at least one of the symptoms is either (1) or (2):1. depressed mood most of the day, nearly everyday2. markedly diminished interest or pleasure3. significant weight loss when not dieting or weight gain, or a decrease or increase in appetite nearly everyday.4. insomnia or hypersomnia5. psychomotor agitation or retardation6. fatigue or loss of energy7. feelings of worthlessness or excessive or inappropriate guilt8. diminished ability to think or concentrate, or indecisiveness9. recurrent thoughts of death, recurrent suicidal ideations w/o a specific plan, suicide attempt, or spedific plan for committing suicide
• .
B. The symptoms do not meet criteria for a mixed episode.
C. The symptoms cause clinically significant distress or impairment in social, occupational, or other important areas of functioning
D. The symptoms are not due to the direct physiological effects of a substance (e.g., a drug of abuse, a medication) or a general medical condition (e.g., hypothyroidism).
E. The symptoms are not better accounted for by bereavement, i.e., after the loss of a loved one, the symptoms persist for longer than 2 months or are characterized by marked functional impairment, morbid preoccupation with worthlessness, suicidal ideation, psychotic symptoms, or psychomotor retardation
Manic EpisodeManic Episode A. A distinct period of abnormally and persistently
elevated, expansive, or irritable mood, lasting at least 1 week (or any duration if hospitalization is necessary).
B. During the period of mood disturbance, three (or more) of the following symptoms have persisted (four if the mood is only irritable) and have been present to a significant degree: 1. inflated self-esteem or grandiosity;
2. decreased need for sleep;
3. more talkative than usual or pressure to keep talking;4. flight of ideas or a subjective experience that thoughts are racing;
5. distractability
6. increase in goal – directed activities or psychomotor agitation;7. excessive involvement in pleasurable activities that have a high potential for painful consequences.
C. The symptoms do not meet the criteria for a mixed episode.D. The mood disturbance is sufficiently severe to cause
marked impairment in occupational functioning or in usual social activities or relationships with others, or to necessitate hospitalization
E. The symptoms are not due to the direct physiological effects of a substance or a general medical condition.
Hypomanic EpisodeHypomanic Episode
A. A distinct period of persistently elevated, expansive, or irritable mood, lasting throughout at least 4 days, that is clearly different from the usual non-depressed mood.
B. During the period of mood disturbance, three (or more) of the manic symptoms have persisted (four if the mood is only irritable) and have been present to a significant degree:
C. The episode is associated with an unequivocal change in functioning that is uncharacteristic of the person when not symptomatic.
D. The disturbance in mood and the change in functioning are observable by others.
E. The episode is not severe enough to cause marked impairment in social or occupational functioning, or to necessitate hospitalization, and there are no psychotic features.
F. The symptoms are not due to the direct physiological effects of a substance (e.g., a drug of abuse, a medication, or other treatment) or a general medical condition
MIXED EPISODEMIXED EPISODE
A. The criteria are met both for a manic episode and for a major depressive episode nearly every day during at least a 1-week period.
B. The mood disturbance is sufficiently severe to cause a marked impairment in occupational functioning or in usual social activities and relationships with others, or to necessitate hospitalization;
C. The symptoms are not due to the direct physiological effects of a substance or a general medical condition.
MAJOR DEPRESSIVE DISORDERMAJOR DEPRESSIVE DISORDER
A. If single episode – presence of a single MDE;
If recurrent – 2 or more MDE’s.
B. The MDE is not better accounted for by schizoaffective disorder and are not superimposed on schizophrenia, schizophreniform disorder, delusional disorder, or psychotic disorders NOS;
C. There has never been a manic episode, a mixed episode or a hypomanic episode.
BIPOLAR I DISORDER(single manic BIPOLAR I DISORDER(single manic episode)episode)
A. Presence of only one manic episode and no past MDE.
A. The manic episode is not better accounted for by schizoaffective disorder, and are not superimposed on schizophrenia, schizophreniform disorder, delusional disorder, or psychotic disorders NOS;
BIPOLAR I DISORDERBIPOLAR I DISORDER(most recent episode ________)(most recent episode ________)
A. Currently or most recently in a ________ episode.
B. There has previously been at least one of the other episodes.
C. The mood episodes in A and B are not better accounted for by schizoaffective disorder, and are not superimposed on schizophrenia, schizophreniform disorder, delusional disorder, or psychotic disorders NOS;
BIPOLAR II DISORDERBIPOLAR II DISORDERA. Presence or history on one or more MDE.
B. Presence or history of at least one hypomanic episode.
C. There has never been a manic or mixed episode.
D. The mood episodes in A and B are not better accounted for by schizoaffective disorder, and are not superimposed on schizophrenia, schizophreniform disorder, delusional disorder, or psychotic disorders NOS;
E. The symptoms cause clinically significant distress or impairment in social, occupational, or other important areas of functioning.
DSM-IV-TR Diagnostic Criteria for DSM-IV-TR Diagnostic Criteria for
Dysthymic DisorderDysthymic Disorder A. Depressed mood for most of the day, for more days
than not, as indicated either by subjective account or observation by others, for at least 2 years.Note: In children and adolescents, mood can be irritable and duration must be at least 1 year.
B. Presence, while depressed, of two (or more) of the following: – poor appetite or overeating – insomnia or hypersomnia – low energy or fatigue – low self-esteem – poor concentration or difficulty making decisions – feelings of hopelessness
C. During the 2-year period (1 year for children or adolescents) of the disturbance, the person has never been without the symptoms in Criteria A and B for more than 2 months at a time.
D. No major depressive episode has been present during the first 2 years of the disturbance (1 year for children and adolescents); i.e., the disturbance is not better accounted for by chronic major depressive disorder, or major depressive disorder, in partial remission
E. There has never been a manic episode, a mixed episode, or a hypomanic episode, and criteria have never been met for cyclothymic disorder.
F. The disturbance does not occur exclusively during the course of a chronic psychotic disorder, such as schizophrenia or delusional disorder.
G. The symptoms are not due to the direct physiological effects of a substance (e.g., a drug of abuse, a medication) or a general medical condition (e.g., hypothyroidism).
H.The symptoms cause clinically significant distress or impairment in social, occupational, or other important areas of functioning.
DSM-IV-TR Diagnostic Criteria for DSM-IV-TR Diagnostic Criteria for
Cyclothymic DisorderCyclothymic Disorder
A. For at least 2 years, the presence of numerous periods with hypomanic symptoms and numerous periods with depressive symptoms that do not meet criteria for a major depressive episode. Note: In children and adolescents, the duration must be at least 1 year.
B. During the above 2-year period (1 year in children and adolescents), the person has not been without the symptoms in Criterion A for more than 2 months at a time.
C. No major depressive episode, manic episode, or mixed episode has been present during the first 2 years of the disturbance.Note: After the initial 2 years (1 year in children and adolescents) of cyclothymic disorder, there may be superimposed manic or mixed episodes (in which case both bipolar I disorder and cyclothymic disorder may be diagnosed) or major depressive episodes (in which case both bipolar II disorder and cyclothymic disorder may be diagnosed).
D. The symptoms in Criterion A are not better accounted for by schizoaffective disorder and are not superimposed on schizophrenia, schizophreniform disorder, delusional disorder, or psychotic disorder not otherwise specified.
E. The symptoms are not due to the direct physiological effects of a substance (e.g., a drug of abuse, a medication) or a general medical condition (e.g., hyperthyroidism).
F. The symptoms cause clinically significant distress or impairment in social, occupational, or other important areas of functioning.

TREATMENTTREATMENT
GOALSGOALS
• Patient’s safety must be guaranteed.
• Complete diagnostic evaluation
• Treatment plan addressing not just immediate symptoms but patient’s prospective well-being.
I. Hospitalization– The need for diagnostic procedures– The risk for suicide or homicide– Grossly reduced ability to get food and
shelter– History of rapidly progressing symptoms– Rupture of patient’s usual support system
II. Psychosocial Therapy
1.Cognitive Therapy
2.Interpersonal Therapy
3.Behavior Therapy
4.Psychoanatically-oriented Therapy
5.Family Therapy
III. Pharmacotherapy
A.Major Depressive Disorder
- MAOI’s, TCAC’s, SSRI’s, SNRI’s
B. Bipolar Disorders
- Lithium, anticonvulsants, antipsychotics
Recommended