
REGULAR ARTICLE
Mild intellectual disability and ADHD; a comparative study of school agechildren’s adaptive abilitiesIda Lindblad ([email protected])1,2, Leif Svensson3, Magnus Landgren3, Salmir Nasic4, Eva Tideman5, Christopher Gillberg1, Elisabeth Fernell1,3,4
1.Gillberg Neuropsychiatry Centre, Sahlgrenska Academy, University of Gothenburg, Gothenburg, Sweden2.Department of Child and Adolescent Psychiatry, Skaraborgs Hospital, Skovde, Sweden3.Department of Paediatrics, Unit of Neurodevelopmental Disorders, Skaraborg′s Hospital, Mariestad, Sweden4.Research and Development Centre, Skaraborg′s Hospital, Skovde, Sweden5.Department of Psychology, Lund University, Lund, Sweden
KeywordsABAS-II, Adaptive behaviour, Adaptive functioning,ADHD, Mild intellectual disability
CorrespondenceIda Lindblad, Gillberg Neuropsychiatry Centre,Kungsgatan 12, SE-411 19 Gothenburg, Sweden.Tel: +46 31 3425986 |Fax: +46 31 3425979 |Email: [email protected]
Received3 March 2013; revised 7 June 2013;accepted 8 July 2013.
DOI:10.1111/apa.12351
ABSTRACTAim: To compare adaptive functioning in children with mild intellectual disability (MID)
with that of children with attention-deficit/hyperactivity disorder (ADHD).
Methods: Thirty-three children with MID were contrasted with 27 children with ADHD with
regard to adaptive functioning as measured by the Adaptive Behaviour Assessment System
(ABAS-II). The group with MID was population-based, and the group with ADHD was
considered representative of a clinically referred group with that diagnosis. The two groups
were subdivided into those ≤11 years and those ≥12 years.
Results: The group with ADHD had lower adaptive functioning, but differences were not
significant at total group levels. In children 12 years or older, the group with ADHD had
significantly lower adaptive functioning.
Conclusion: Older children with ADHD had poorer adaptive functioning than those with
MID, a finding which should be of interest to school and other authorities mapping out
education and intervention plans for children with special needs.
INTRODUCTIONMild intellectual disability (MID) affects at least onepercent of the general population of school age children(1). Establishing a diagnosis of MID is an important andsometimes difficult clinical task. Particular care is usuallytaken to distinguish MID from ‘borderline intellectualfunctioning’ (BIF) (IQ 70–84). In many countries, MID,but not BIF or other cognitive-behavioural problems, isconsidered a ‘ticket’ to tailored education, intervention andother special needs provisions. To qualify for a diagnosis ofMID, the individual must meet both of the followingcriteria: (i) tested IQ below about 70, and (ii) adaptivefunctioning negatively affected by the low IQ-level.
To facilitate structured information gathering, the use ofstandardized instruments, such as the Vineland AdaptiveBehaviour Scales-II (2) and the Adaptive BehaviourAssessment System (ABAS-II) (3), is often encouraged.‘Adaptive functioning’ refers to an individual’s ability tocope with common demands in life including the degree ofindependence compared with others of similar age andbackground. Adaptive functions include a wide range ofskills, and the tests used measure how well an individualmeets the standards of personal independence and socialresponsibility–at school/work, at home, and more generallyin the community. Examples of adaptive functions include:the ability to respect rules/obey laws, to handle occupa-tional responsibilities, to cope with healthcare, travel/
transportation, schedules/routines, safety and manage theuse of money (4).
Attention-deficit/hyperactivity disorder (ADHD) affectsseveral percent of school-aged children. Epidemiologicalstudies of school age children have shown a prevalencebetween 11.4 and 16.1 in the United States (n = 4), 2.4 and19.8 in other countries (n = 9) (5). ADHD is definedaccording to a specific set of symptoms of attention deficitsand/or hyperactivity–impulsivity problems. Some impair-ment from the symptoms must be present in at least twosettings, and there must be clear evidence of interference
Key notes� In Sweden (through legislation), habilitation and other
specific social and school services are offered toindividuals with certain neurodevelopmental diagno-ses, such as intellectual disability and autism spectrumdisorders.
� ADHD is currently not included among diagnosedconditions that automatically entitle you to specialservices.
� Our results indicate that children with ADHD should begiven more attention with regard to adaptive function-ing and to need for support in daily life.
©2013 Foundation Acta Pædiatrica. Published by John Wiley & Sons Ltd 2013 102, pp. 1027–1031 1027
Acta Pædiatrica ISSN 0803-5253

with developmentally appropriate social, academic oroccupational functioning (6).
Clearly then, the diagnostic criteria both for MID and forADHD include impairments of adaptive functioning. Inclinical diagnostic practice, the requirement for adaptiveimpairment has usually been considered in the case of MIDbut is not always taken specifically into account whenmaking the diagnosis of ADHD (4,6).
MID often co-occurs with ADHD (7–9). In Sweden, MIDis a diagnosis that entails specific legal rights to obtaineducational adjustment at school and support from habil-itation services and society more generally. Children withADHD do not have the same explicit legal rights to supportfrom school and society, and they are not included in thetarget group for habilitation services.
The literature regarding adaptive abilities in children withMID compared to children with ADHD is limited, and wehave not been able to locate a single paper specificallyaddressing this issue. We therefore set out to analyse thelevel of adaptive functioning, as measured by the ABAS-II,in groups of children with these diagnoses. Our hypotheseswere that (1) children with MID would be more impaired inadaptive functioning than those with ADHD (which isgenerally considered a less severe disorder and ‘closer tonormality’ than MID (10), and that (2) older children wouldshow more adaptive impairments than younger children(assuming that in both groups, demands made will increaseover time which would lead to increases in the gap betweenexpectations – socially, academically and behaviourally –and the individual’s ability to live up to these.
PARTICIPANTS AND METHODSMID groupThe children with MID had been recruited in 2009–2010from two representative municipalities in the south-westernhealth-care region of Sweden. Results obtained in the studyof this population-based group have been published in aprevious study dealing with diagnostic validity of MID andcoexisting disorders (9). All the children in the group hadtheir cognitive assessment and test reports scrutinized. Allhad attended a special school/classroom for children withMID. The group consisted of 33 individuals (21 boys and 12girls) with birth years 1993–2002 and a mean age of12.6 years (range 6–16 years) at ABAS-II assessment (seebelow). Among the 33 children with MID, eight had anadditional clinical diagnosis of ADHD, five of whom incombination with yet other disorders; one with autismspectrum disorder (ASD), one with ASD and Tourettesyndrome, one with Tourette syndrome, one with ASD andepilepsy and one with epilepsy. Another three of thechildren with MID had ASD but not ADHD. Theseadditional diagnoses had been established in conjunctionwith the child’s clinical assessment in specialized assess-ment teams within child and adolescent psychiatry orhabilitation services.
The group of children with MID had also been assessedon the Five-to-Fifteen (FTF) parent questionnaire (11,12),
in conjunction with the previously mentioned study (9). TheFTF includes eight domains (motor skills, executive func-tions, perception, memory, language, learning, social skillsand emotion/behaviour problems). The children with MIDscored above the 90th percentile in 55–88% on the eightdomains (10% expected for each domain in Swedishpopulation sample of same-aged children).
ADHD groupThe ADHD group was recruited from a consecutive seriesof patients with ADHD at a specialized paediatric unit inthe same south-western health-care region of Sweden. Tothis unit, schools and general paediatric outpatient clinicsin the region refer children with suspected ADHD forcomprehensive diagnostic assessment and decision aboutintervention. The group referred to this team was consid-ered representative of children with at least moderatelysevere ADHD, in which pharmacological treatment often ispart of the total treatment/intervention plan. As part of thediagnostic assessment, the ABAS-II was used and given toparents and teachers for completion by them. Althoughonly a minority of all the referred children’s teachersactually received the ABAS-II, there was no selection withregard to severity of the child’s ADHD or comorbiditystatus in this procedure. For the purpose of the presentanalyses, children with ADHD who also had MID or ASDwere excluded from the study, as were all children alreadyon pharmacological ADHD treatment before the ABAS-IIquestionnaire had been completed.
In the end, the ADHD group consisted of 27 children (18boys and 9 girls), aged 6–16 years (mean age 12.9 years) atthe time of the teacher ABAS-II assessment. Of the 27children, 26 were diagnosed with combined ADHD, andone was diagnosed with mainly inattentive subtype ADHD.The children’s IQ distribution was as follows: 10 (38%) hadBIF and 17 (62%) had average IQ.
Even though comorbid MID and ASD had been exclu-sion criteria, still 23/27 (85%) had at least one additional‘non-ADHD’ impairment/developmental problem, includ-ing dyslexia, speech and language impairment, oppositionaldefiant disorder (ODD), Tourette syndrome, autistic traits(not meeting full criteria for ASD) and depression.
MeasureThe instrument used for comparison of adaptive function-ing in the two groups was the ABAS-II (3), a validatedquestionnaire for assessment of adaptive behaviour. Thequestionnaire has norm-referenced scaled scores for 10 skillareas (nine included in the three domains for children),with a mean of 10 (SD 1.5) and provides norm-referencedstandard scores for three domains: conceptual domain(CON), social domain (SOC) and practical domain (PRA)and a merged score – general adaptive composite (GAC) –(M 100, SD 15, and 90% and 95% confidence intervals andpercentile ranks). CON includes communication, func-tional academics and self-direction, and SOC includesleisure skills and social skills, and PRA includes communityuse, home/school living, health and safety and self-care.
1028 ©2013 Foundation Acta Pædiatrica. Published by John Wiley & Sons Ltd 2013 102, pp. 1027–1031
Mild intellectual disability and ADHD–adaptive abilities Lindblad et al.
Work skills are also assessed but not included in any of thethree domains. The respondent rates the observedbehaviour frequency of various skills using a four-pointLikert scale, ‘not able’, ‘never’, ‘sometimes’ and ‘always’,and is provided with an option to mark the item as‘guessed’. At the end of each domain, section additionalcomments can be added. Every item is formulated as apositive statement, and high scores indicate good function-ing. Examples are: ‘shows realistic idea of the value ofmoney’ (CON), ‘adapts clothing to weather’ (PRA) and‘treats young children with an understanding of their lowerlevel of maturity’ (SOC).
The ABAS-II includes two separate forms; parent/primary caregiver and teacher/daycare provider and bothare for the ages of 5:0–21:11 years. In the present study,only teacher data were included. In the group of childrenwith MID, we had ABAS-II only from teachers and notfrom parents.
Test–retest and inter-rater reliability of the GAC are all inthe range of 0.89–0.90s. The test–retest reliability coeffi-cients of the 10 skill areas are slightly lower, mainly in0.80s–0.90s and the inter-rater reliability coefficients for theindividual skill areas generally are in the 0.60s and 0.70s(13).
StatisticsDescriptive statistics with medians and quartiles will bepresented for the three ABAS domains and for the GAC.The Mann–Whitney U-test was used for statistical analyses.SPSS v. 20 for Windows (SPSS Inc., Chicago, IL, USA) wasused for all statistical data handling.
EthicsThe studies had been approved by the Regional EthicsCommittee in Gothenburg. Written informed consent wasobtained from parents of children with MID. For theADHD group, ethical approval had been given to analysethe clinically used ABAS-II data for research.
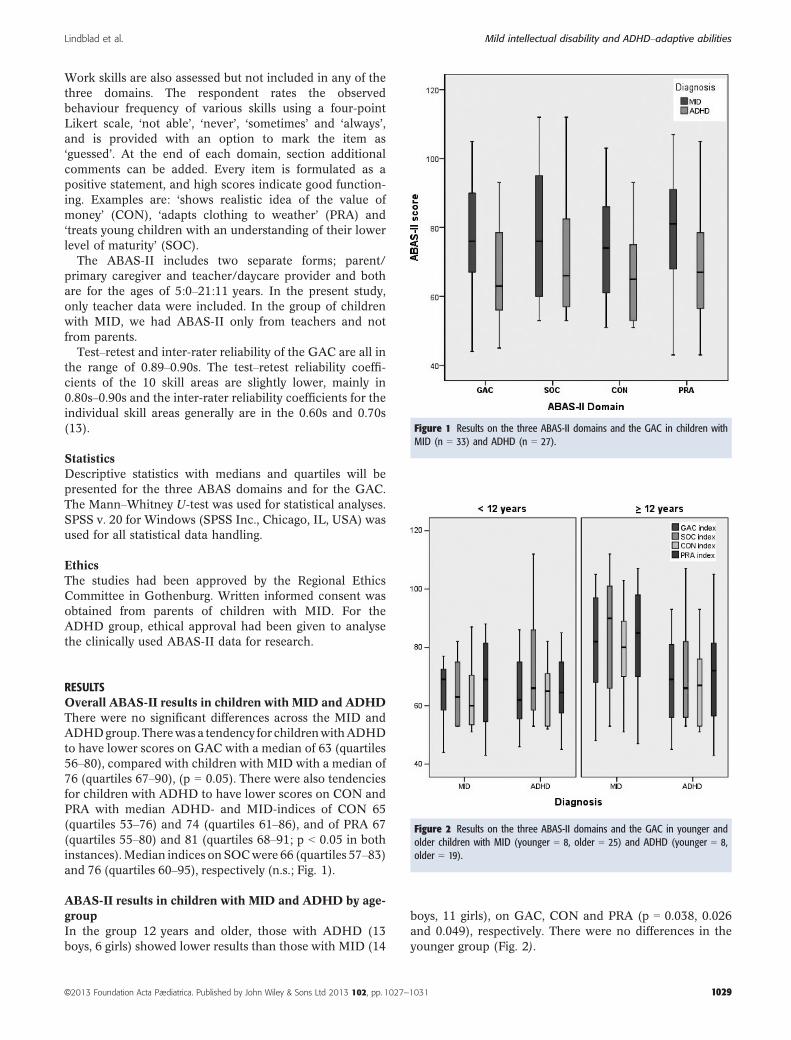
RESULTSOverall ABAS-II results in children with MID and ADHDThere were no significant differences across the MID andADHDgroup.Therewas a tendency for childrenwithADHDto have lower scores on GAC with a median of 63 (quartiles56–80), compared with children with MID with a median of76 (quartiles 67–90), (p = 0.05). There were also tendenciesfor children with ADHD to have lower scores on CON andPRA with median ADHD- and MID-indices of CON 65(quartiles 53–76) and 74 (quartiles 61–86), and of PRA 67(quartiles 55–80) and 81 (quartiles 68–91; p < 0.05 in bothinstances).Median indices onSOCwere 66 (quartiles 57–83)and 76 (quartiles 60–95), respectively (n.s.; Fig. 1).
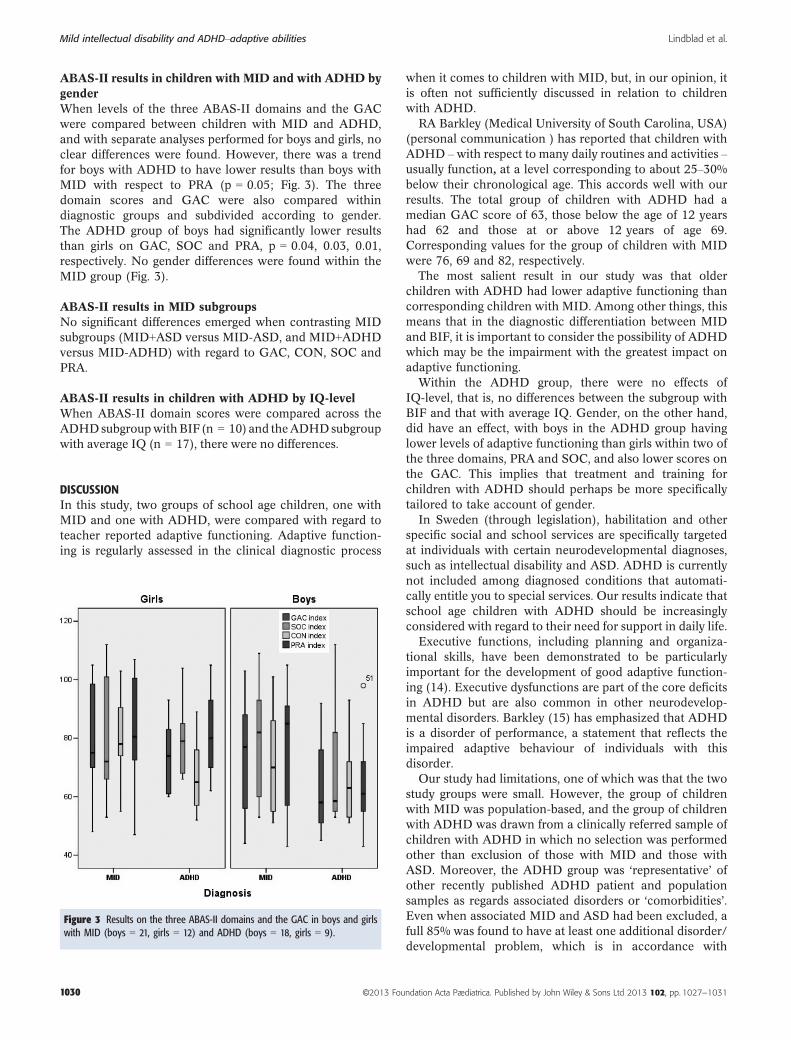
ABAS-II results in children with MID and ADHD by age-groupIn the group 12 years and older, those with ADHD (13boys, 6 girls) showed lower results than those with MID (14
boys, 11 girls), on GAC, CON and PRA (p = 0.038, 0.026and 0.049), respectively. There were no differences in theyounger group (Fig. 2).
Figure 1 Results on the three ABAS-II domains and the GAC in children withMID (n = 33) and ADHD (n = 27).
Figure 2 Results on the three ABAS-II domains and the GAC in younger andolder children with MID (younger = 8, older = 25) and ADHD (younger = 8,older = 19).
©2013 Foundation Acta Pædiatrica. Published by John Wiley & Sons Ltd 2013 102, pp. 1027–1031 1029
Lindblad et al. Mild intellectual disability and ADHD–adaptive abilities
ABAS-II results in children with MID and with ADHD bygenderWhen levels of the three ABAS-II domains and the GACwere compared between children with MID and ADHD,and with separate analyses performed for boys and girls, noclear differences were found. However, there was a trendfor boys with ADHD to have lower results than boys withMID with respect to PRA (p = 0.05; Fig. 3). The threedomain scores and GAC were also compared withindiagnostic groups and subdivided according to gender.The ADHD group of boys had significantly lower resultsthan girls on GAC, SOC and PRA, p = 0.04, 0.03, 0.01,respectively. No gender differences were found within theMID group (Fig. 3).
ABAS-II results in MID subgroupsNo significant differences emerged when contrasting MIDsubgroups (MID+ASD versus MID-ASD, and MID+ADHDversus MID-ADHD) with regard to GAC, CON, SOC andPRA.
ABAS-II results in children with ADHD by IQ-levelWhen ABAS-II domain scores were compared across theADHDsubgroupwithBIF (n = 10) and theADHDsubgroupwith average IQ (n = 17), there were no differences.
DISCUSSIONIn this study, two groups of school age children, one withMID and one with ADHD, were compared with regard toteacher reported adaptive functioning. Adaptive function-ing is regularly assessed in the clinical diagnostic process
when it comes to children with MID, but, in our opinion, itis often not sufficiently discussed in relation to childrenwith ADHD.
RA Barkley (Medical University of South Carolina, USA)(personal communication ) has reported that children withADHD – with respect to many daily routines and activities –usually function, at a level corresponding to about 25–30%below their chronological age. This accords well with ourresults. The total group of children with ADHD had amedian GAC score of 63, those below the age of 12 yearshad 62 and those at or above 12 years of age 69.Corresponding values for the group of children with MIDwere 76, 69 and 82, respectively.
The most salient result in our study was that olderchildren with ADHD had lower adaptive functioning thancorresponding children with MID. Among other things, thismeans that in the diagnostic differentiation between MIDand BIF, it is important to consider the possibility of ADHDwhich may be the impairment with the greatest impact onadaptive functioning.
Within the ADHD group, there were no effects ofIQ-level, that is, no differences between the subgroup withBIF and that with average IQ. Gender, on the other hand,did have an effect, with boys in the ADHD group havinglower levels of adaptive functioning than girls within two ofthe three domains, PRA and SOC, and also lower scores onthe GAC. This implies that treatment and training forchildren with ADHD should perhaps be more specificallytailored to take account of gender.
In Sweden (through legislation), habilitation and otherspecific social and school services are specifically targetedat individuals with certain neurodevelopmental diagnoses,such as intellectual disability and ASD. ADHD is currentlynot included among diagnosed conditions that automati-cally entitle you to special services. Our results indicate thatschool age children with ADHD should be increasinglyconsidered with regard to their need for support in daily life.
Executive functions, including planning and organiza-tional skills, have been demonstrated to be particularlyimportant for the development of good adaptive function-ing (14). Executive dysfunctions are part of the core deficitsin ADHD but are also common in other neurodevelop-mental disorders. Barkley (15) has emphasized that ADHDis a disorder of performance, a statement that reflects theimpaired adaptive behaviour of individuals with thisdisorder.
Our study had limitations, one of which was that the twostudy groups were small. However, the group of childrenwith MID was population-based, and the group of childrenwith ADHD was drawn from a clinically referred sample ofchildren with ADHD in which no selection was performedother than exclusion of those with MID and those withASD. Moreover, the ADHD group was ‘representative’ ofother recently published ADHD patient and populationsamples as regards associated disorders or ‘comorbidities’.Even when associated MID and ASD had been excluded, afull 85% was found to have at least one additional disorder/developmental problem, which is in accordance with
Figure 3 Results on the three ABAS-II domains and the GAC in boys and girlswith MID (boys = 21, girls = 12) and ADHD (boys = 18, girls = 9).
1030 ©2013 Foundation Acta Pædiatrica. Published by John Wiley & Sons Ltd 2013 102, pp. 1027–1031
Mild intellectual disability and ADHD–adaptive abilities Lindblad et al.

general population findings, such as found by Kadesj€o andGillberg (16) several years ago.
The ABAS-II questionnaires were completed by teachersin both groups. The classroom situations of the two studygroups – although we have no hard data to support this –can be assumed to be dissimilar; highly structured for thosewith MID – who attended special classrooms for childrenwith learning problems – and much more variable forthose with ADHD – who often attended mainstreamclassrooms. Another aspect that needs to be taken intoaccount when interpreting the findings is that teachers ofchildren with MID may have other ‘norms’ and possiblytend to overestimate the skills of ‘their child’ when nothaving easy access to comparison with children from thegeneral population. Nevertheless, the ABAS-II items referto very specific situations and abilities demonstrated indaily life, and our conclusion, therefore, is that a compar-ison between the two groups should be valid because theywere both assessed by their teachers, rather than by othertypes of raters.
Given that children with MID in this study were inspecial education classrooms or other special schoolsettings, their disability was well known to their teacher.This is in contrast to the school situation for the vastmajority of children with ADHD who had widely varyingtypes of support and educational adjustments at theirschools.
The higher level of adaptive functioning in the oldergroup with MID – compared with those with ADHD – may,speculatively, and perhaps only to some extent, be attrib-uted to earlier identification of cognitive dysfunctions andsubsequently increased level of support provided for thechildren with MID. Moreover, and also highly speculative,the MID group could have gained adaptive skills because ofthe universally delivered adaptive training in the specialclassrooms that this group attended. The children with MIDmight also have received training in daily living skills athome and in their free time in comparison with the childrenwith ADHD who had no identified diagnosis at the time ofthe ABAS-II assessment.
CONCLUSIONThe results of this study suggest that children and adoles-cents with ADHD should be given more attention withregard to adaptive functioning. Routine structured mea-surement of these functions in daily life should be includedin the assessment procedure not only in children with MID,but also in those with ADHD. More emphasis should bemade on the need for strategies and intervention programsto improve such adaptive skills in ADHD.
ACKNOWLEDGEMENTSTheauthors are grateful to all the teacherswhocompleted theABAS-II questionnaires and to school nurse Annika Johns-son for administrative help. Financial supportwas given from
the Research and Development Centre at Skaraborg′s Hos-pital, and from the Swedish Science Council.
CONFLICT OF INTERESTThe authors declare no conflict of interest.
References
1. Fernell E. Mild mental retardation in schoolchildren in aswedish suburban municipality: prevalence and diagnosticaspects. Acta Paediatr 1996; 85: 584–8.
2. Sparrow S, Cicchetti D, Balla D. Vineland adaptive behaviorscales. 2nd ed. (Vineland-II). San Antonio, TX: PearsonAssessment, 2005.
3. Harrison PL, Oakland T. Adaptive behavior assessment systemmanual. 2nd ed. San Antonio, TX: Harcourt Assessment, 2003.
4. American Association of Intellectual DevelopmentalDisabilities. Washington, DC: AAIDD, 2011 (cited 2011).
5. Faraone SV, Sergeant J, Gillberg C, Biederman J. Theworldwide prevalence of adhd: is it an american condition?World Psychiatry 2003; 2: 104–13.
6. American Psychiatric Association. Diagnostic and statisticalmanual of mental disorders: DSM-IV: prepared by the taskforce on DSM-IV. Washington, DC: American PsychiatricAssociation, 1994.
7. Simonoff E, Pickles A, Wood N, Gringras P, Chadwick O.Adhd symptoms in children with mild intellectual disability.J Am Acad Child Adolesc Psychiatry 2007; 46: 591–600.
8. Fernell E, Ek U. Borderline intellectual functioning in childrenand adolescents - insufficiently recognized difficulties. ActaPaediatr 2010; 99: 748–53.
9. Lindblad I, Gillberg C, Fernell E. ADHD and otherassociated developmental problems in children with mildmental retardation. The use of the “five-to-fifteen”questionnaire in a population-based sample. Res Dev Disabil2011; 32: 2805–9.
10. Gillberg C. The essence in child psychiatry: early symptomaticsyndromes eliciting neurodevelopmental clinical examinations.Res Dev Disabil 2010; 31: 1543–51.
11. Kadesjo B, Janols LO, Korkman M, Mickelsson K, Strand G,Trillingsgaard A, et al. The FTF (five to fifteen): thedevelopment of a parent questionnaire for the assessment ofADHD and comorbid conditions. Eur Child AdolescPsychiatry 2004; 13Suppl 3: 3–13.
12. Trillingsgaard A, Damm D, Sommer S, Jepsen JR, OstergaardO, Frydenberg M, et al. Developmental profiles on the basis ofthe FTF (five to fifteen) questionnaire-clinical validity andutility of the ftf in a child psychiatric sample. Eur Child AdolescPsychiatry 2004; 13Suppl 3: 39–63.
13. Harrison PL, Oakland T. www.pearsonassessments.com. 2012.14. Clark C, Prior M, Kinsella G. The relationship between
executive function abilities, adaptive behaviour, andacademic achievement in children with externalisingbehaviour problems. J Child Psychol Psychiatry 2002; 43:785–96.
15. Barkley RA. Behavioral inhibition, sustained attention, andexecutive functions: constructing a unifying theory of adhd.Psychol Bull 1997; 121: 65–94.
16. Kadesjo B, Gillberg C. The comorbidity of adhd in the generalpopulation of swedish school-age children. J Child PsycholPsychiatry 2001; 42: 487–92.
©2013 Foundation Acta Pædiatrica. Published by John Wiley & Sons Ltd 2013 102, pp. 1027–1031 1031
Lindblad et al. Mild intellectual disability and ADHD–adaptive abilities
Recommended

















