Metastatic Disease to Metastatic Disease to Extraocular Muscles of Extraocular Muscles of Undiscovered Primary Undiscovered Primary Breast CancerBreast Cancer
Maria E. Lim, BS 1
Sergul A. Erzurum, MD, FACS 1, 2
1. Department of Surgery, Northeastern Ohio Universities College of Medicine, Rootstown, OH 44272
2. Section of Ophthalmology in the Department of Surgery at St. Elizabeth Health Center, Youngstown, OH 44501
Authors acknowledge the financial support of the Polena Trust for Ocular Research at the St. Elizabeth Development Foundation, Youngstown, Ohio. Statements are the sole responsibility of the authors. Authors have no financial conflict of interest associated with products described in the report.
57 year old Caucasian 57 year old Caucasian femalefemaleHistory of Present Illness (Feb
2010)Chief complaint: diplopia at
distance x 3-5 weeks◦Resolved when left eye closed
Negative for:◦Orbital/retroorbital pain◦Change in vision
Physical ExamPhysical ExamOD BCVA: 20/20 Tonometry: 20 SLE: NL Fundus:
◦ flame hemmorrhage off disc noted
EOM movement: full in all direction
Hertel: 16 mm◦ base setting 93
PERRL
Neurologic exam Cranial nerve exam,
strength, movement, deep tendon reflexes, sensation, and coordination were all within normal limits.
Lumbar puncture:◦ No malignant cells
OS BCVA: 20/20 Tonometry: 23 SLE: NL Fundus: NL EOM movement:
◦ -3 limitation of abduction ◦ -4 limitation of elevation◦ Distance fixation: 10∆ RHT◦ Near fixation: 1-2∆ intermittent
RHT◦ Right gaze: 8∆ RHT◦ Left gaze: 14∆ RHT, 2∆ XT◦ Upward gaze: approximately
25-20∆ RHT (+) retropulsion Hertel: 16 mm
◦ base setting 93 PERRL
Past Medical HistoryPast Medical History July 2006: Palpable left
axillary lymphadenopathy Nov 2006: Left axillary
lymph node dissection◦ Pathology: poorly
differentiated adenocarcinoma consistent with breast origin
◦ ER (+), PR (-), Her-2/neu (-) in 14/15 nodes
◦ Lymphoproliferative disease markers (-)
◦ Patient received doxorubicin, cyclophosphamide, paclitaxel x 5 months then radiation and anastrozole.
Oct 2007: ↑ CEA & CA 27-29 ◦ PET scan, B/L breast MRI, & CT
abdomen & pelvis◦ All findings benign
May 2008: Bone metastasis, right ovarian metastasis, and retroperitoneal adenopathy◦ Treatment: capecitabine and
pamidronate◦ Right ureteral stent placement
July 2009: Liver metastasis◦ Treatment: gemcitabine and
paclitaxel Jan 2010: Worsening liver
lesions ◦ Treatment: 3 cycles
doxorubicin
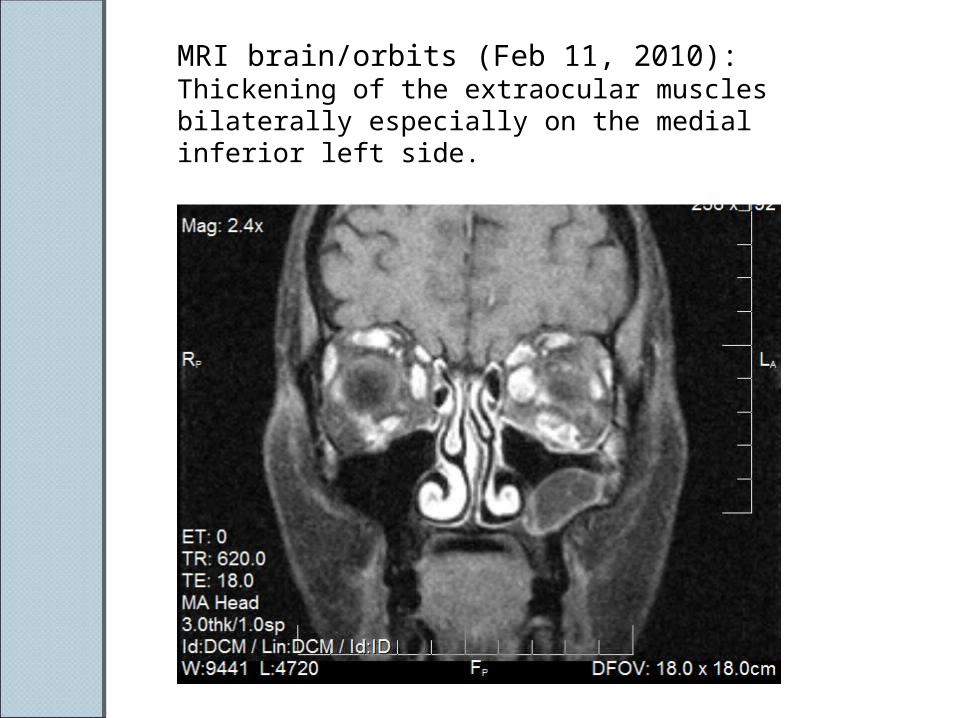
MRI brain/orbits (Feb 11, 2010): Thickening of the extraocular muscles bilaterally especially on the medial inferior left side.
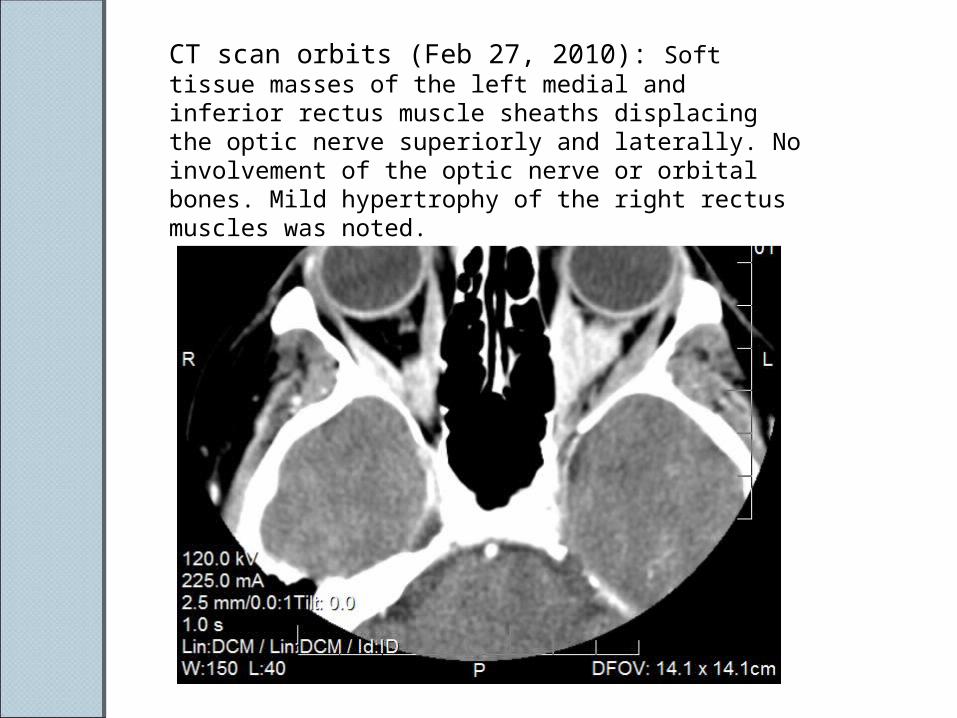
CT scan orbits (Feb 27, 2010): Soft tissue masses of the left medial and inferior rectus muscle sheaths displacing the optic nerve superiorly and laterally. No involvement of the optic nerve or orbital bones. Mild hypertrophy of the right rectus muscles was noted.
Patient CoursePatient CourseTreatment:
◦ Radiation to the left eye and orbit ◦ Continued systemic treatment◦ Developed thrombocytopenia secondary to
therapy. March 2010: admitted to the Medical ICU
for profuse rectal bleeding and hypovolemic shock◦ Received packed red blood cells, platelets,
and IV resuscitation. ◦ Mental status deterioration◦ MRI of the brain: Multi-infarct changes.
After much discussion, the patient and her family opted for Hospice care and she soon passed away.
Metastasis to the OrbitMetastasis to the OrbitPrevalence :1-13% of all orbital
tumors1. Often unilateralTypically involves orbital bone and fatMost common primary origins from
the breast, prostate, lung 2. 9% of all metastatic disease involves
extraocular muscles ◦even fewer involve more than two
muscles 3.
Breast Cancer in the EOMBreast Cancer in the EOMLiterature classically describes
scirrhous type breast cancer ◦presents with enophthalmos from
fibrosis & contracture of invaded tissue◦ localize in orbital fat 4, 5.
75% of breast cancer metastases to the orbit have a primary tumor
Average time between discovery of primary tumor & ophthalmic presentation: 3 years 5.
Mean survival time after orbital manifestation of metastasis: 22 months 6.
Differential DiagnosisDifferential DiagnosisThyroid ophthalmoplegia
◦ Extraocular muscle swelling ◦ Exophthalmos with lid retraction and lid lag◦ Systemic manifestation of hyperthyroidism
Orbital pseudotumor ◦ Acute onset of pain 2
Leptomeningeal or posterior fossa metastasis◦ Typically involves cranial nerves or long nerve
tracts 8
Cranial nerve palsies Lymphoma
◦ 10-15% of orbital lesions 2, 9
◦ Skeletal muscle metastasis commonly harbor leukemia or lymphoma
In ConclusionIn ConclusionPatient presented with left eye limitation of
elevation and abductionNo orbital biopsies, due to patient’s overall
prognosis ◦ Images showed extraocular muscle thickening
bilaterally◦ Metastatic disease was presumed
Patient had a four year course of metastatic spread to the bone, liver, retroperitoneal lymph nodes, and ovaries
While the patient was initially diagnosed with breast cancer from axillary lymph node involvement in 2006, no primary tumor in the breast was found after repeated MRI, mammography, or physical exam.
ReferencesReferences1. Spitzer SG, Bersani TA, Mejico LJ. Multiple bilateral extraocular muscle
metastases as the initial manifestation of breast cancer. J Neuro-Ophthalmol. 2005; 25 (1): 37-9.
2. Lell M, Schulz-Wendtland R, Hafner A, et al. Bilateral orbital tumour as the presentation of mammographically occult breast cancer. Neuroradiology. 2004; 46: 682 – 5.
3. Peckham EL, Giblen G, Kim AK, Sirdofsky MD. Bilateral extraocular muscle metastasis from primary breast cancer. Neurology. 2005; 65 (1): 74.
4. Harnett AN, Kemp EG, Fraser G. Metastatic breast cancer presenting as tolosa-hunt syndrome. Clinical Oncology. 1999; 11: 407-9.
5. Milman T, Pliner L, Langer PD. Breast carcinoma metastatic to the orbit: An unusually late presentation. Ophthal Plast Reconstr Surg. 2008; 24 (6): 480-2.
6. Shields JA, Shields CL, Brothman HK, Carvalho C, Perez N, Eagle RC. Cancer metastatic to the orbit: the 2000 Robert M. Curts Lecture. Ophthalm Plast Reconstr Surg. 2001; 17: 346-354.
7. Luneau K, Falardeau J, Hardy I, Boulos PR, Boghen D. Ophthalmoplegia and lid retraction with normal initial orbit CT imaging in extraocular muscle metastases as the presenting sign of breast carcinoma. J Neuro-Ophthalmol. 2007; 27 (2): 144-6.
8. Heijden A, Twijnstra A, Lamers W, Hupperets P, Freling G. An unusual cause of diplopia in a cancer patient. Eur J Cancer. 1991; 27(1): 1315-6.
9. Weiss R, Grisold W, Jellinger K, Muhlbauer J, Scheiner W, Vesely M. Metastasis of solid tumors in extraocular muscles. Acta Neuropathol. 1984; 65: 168-71.
Recommended