METABOLIC ACIDOSIS
Objectives
Review physiology of acid-base balance Determine gap versus non-anion gap metabolic
acidosis Overview of RTAs Practice with clinical vignettes
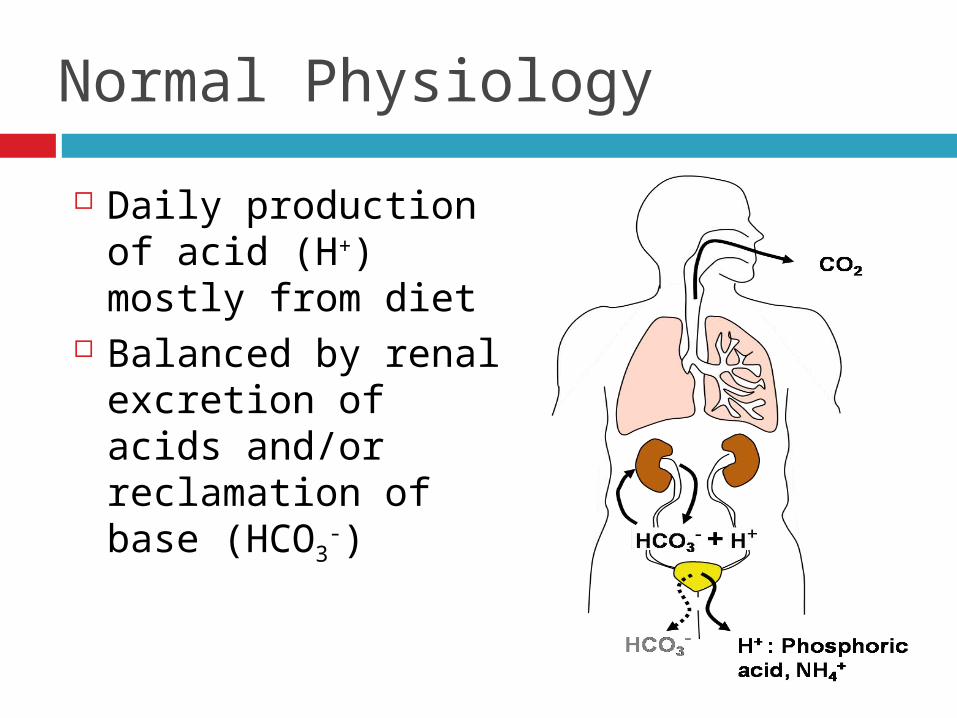
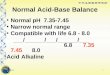
Normal Physiology
Daily production of acid (H+) mostly from diet
Balanced by renal excretion of acids and/or reclamation of base (HCO3
-)
Metabolic Acidosis Disorder
1) Overproduction of acids = ↑H+
2) Increased extra-renal loss of base = ↓ HCO3-
3) Decrease in renal acid secretion = ↑H+
4) Poor renal absorption of base = ↓ HCO3-
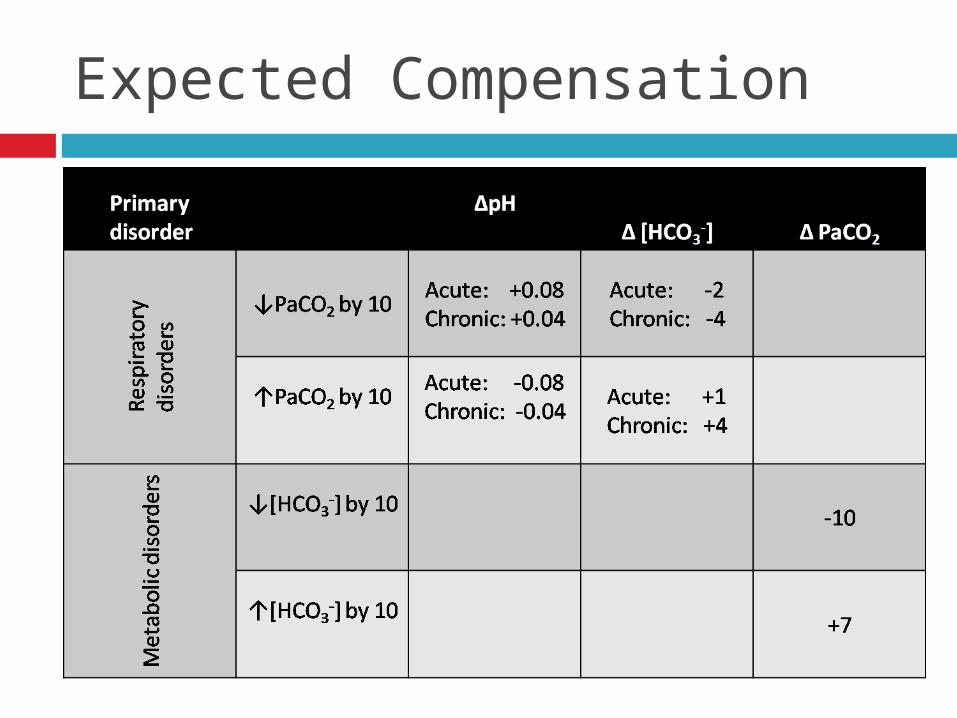
Expected Compensation
Acid/Base Formulas
Winter’s Formula (CO2) = 1.5 [HCO3-] + 8 ± 2
Anion Gap = Na+ – Cl- + HCO3-
Correct for hypoalbuminemia Increase AG by 2.5 for every 1 decrease in albumin
Unmeasured Anions = Lactate, Phosphate, Sulfate ∆ Anion gap / ∆ [HCO3
-]
Elevated Anion Gap (>12)
“MUDPILES” Methanol Uremia Diabetic ketoacidosis / Starvation ketoacidosis Paraldehyde Isoniazid / Iron Lactic acidosis Ethanol / Ethylene glycol Salicylates CO, cyanide, hydrogen sulfide, sulfur, theophylline,
toluene
Non-anion Gap Metabolic Acidosis
“HARD UP” Hyperalimentation Acetazolamide Renal tubular acidosis (RTA) Diarrhea Ureteral diversion Pancreatic fistula
Low Anion Gap (<3)
Increase in unmeasured cations
Hyper-Ca Hyper-Mg Hyper-K Lithium intoxication Paraproteinemia
Decrease in unmeasured anions
Hypoalbuminemia Dilution
Urine Anion Gap
UAG= (UNa + UK + UNH4) – (UCl - UHCO3)
POSITIVE if renal disease NEGATIVE if normal or GI bicarbonate losses
Proximal (type 2) RTA
Impaired proximal tubule HCO3- reabsorption
In steady state distal nephron can accommodate and acidify urine pH < 5.5
Hypokalemia Increased NaHCO3 to the distal tubules Increased aldosterone activity reabsorbing Na+ and
secreting K+
Distal (type 1) RTA
Impaired distal secretion of H+
Causes impairment in regeneration of HCO3-
Unable to acidify urine pH < 5.5 Associated with hypo-K Associated with nephrocalcinosis and
nephrolithiasis Increase in urinary luminal Ca2+ from bone mineral
dissolution for buffering systems High urine pH decreases solubility of Ca2+ phosphate
complexes
Hyperkalemic (type 4) RTA
Decreased H+ and K+ secretion Urine pH < 5.5 Etiology due to mild/moderate CKD, DM,
autoimmune disorders Deficiency of circulating aldosterone Impairment of distal luminal electronegativity in
the cortical collecting duct
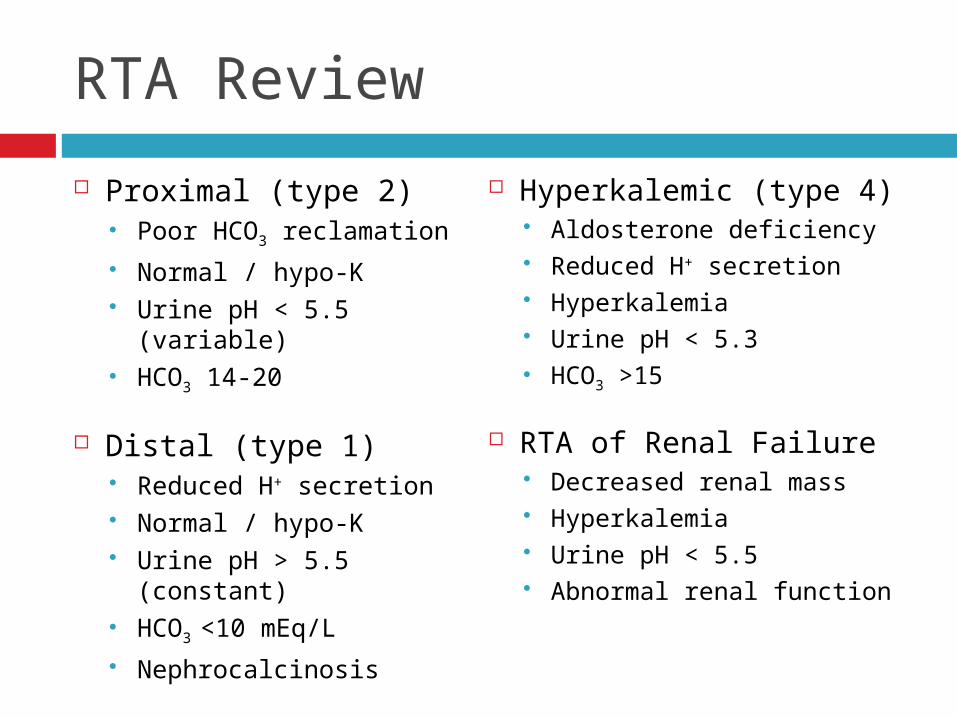
RTA Review
Proximal (type 2) Poor HCO3 reclamation Normal / hypo-K Urine pH < 5.5 (variable) HCO3 14-20
Distal (type 1) Reduced H+ secretion Normal / hypo-K Urine pH > 5.5 (constant) HCO3 <10 mEq/L Nephrocalcinosis
Hyperkalemic (type 4) Aldosterone deficiency Reduced H+ secretion Hyperkalemia Urine pH < 5.3 HCO3 >15
RTA of Renal Failure Decreased renal mass Hyperkalemia Urine pH < 5.5 Abnormal renal function
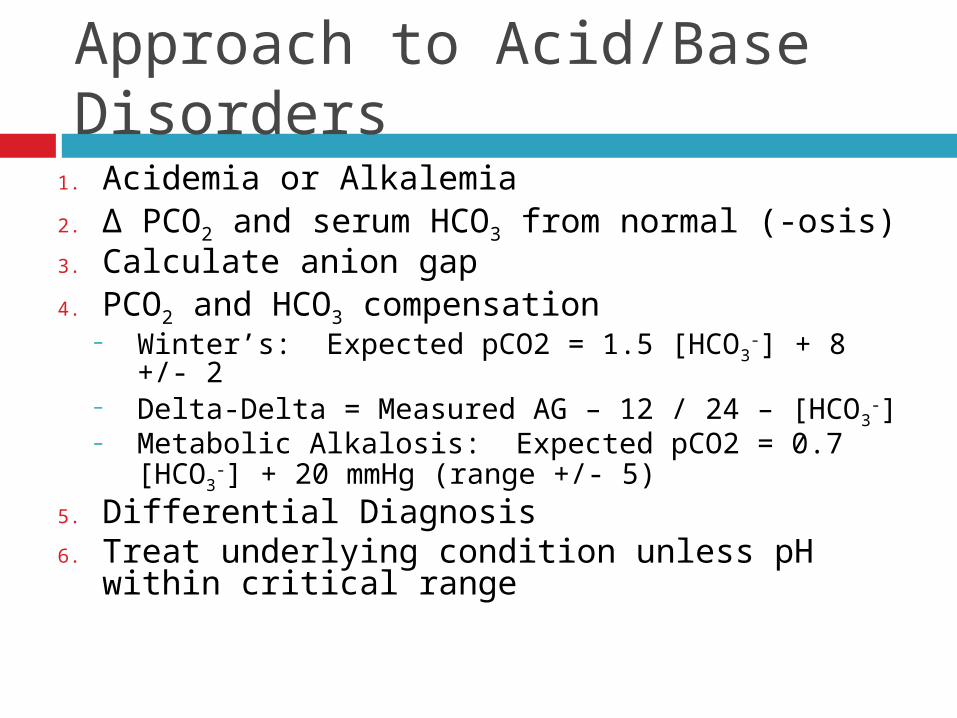
Approach to Acid/Base Disorders
1. Acidemia or Alkalemia2. ∆ PCO2 and serum HCO3 from normal (-osis)3. Calculate anion gap4. PCO2 and HCO3 compensation
– Winter’s: Expected pCO2 = 1.5 [HCO3-] + 8 +/- 2
– Delta-Delta = Measured AG – 12 / 24 – [HCO3-]
– Metabolic Alkalosis: Expected pCO2 = 0.7 [HCO3-] +
20 mmHg (range +/- 5) 5. Differential Diagnosis6. Treat underlying condition unless pH within
critical range
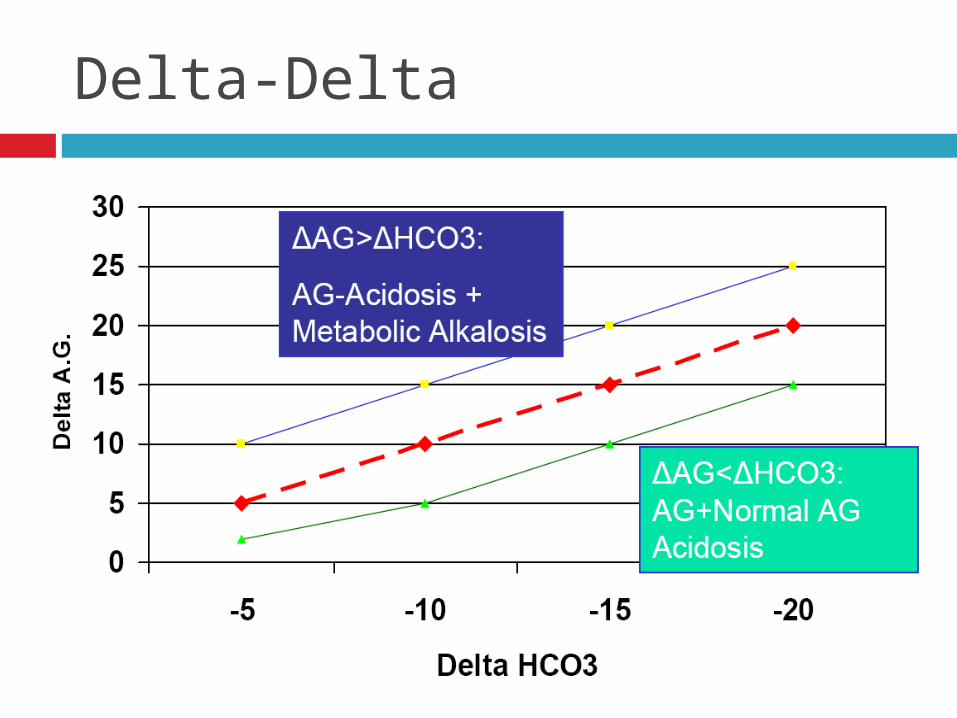
Delta-Delta
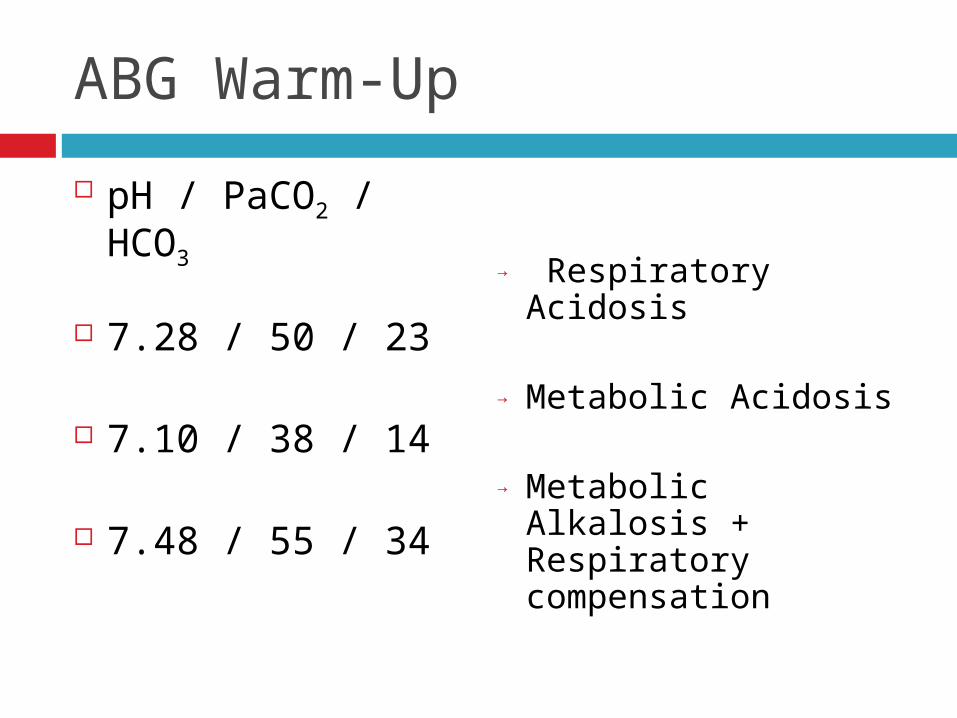
ABG Warm-Up
pH / PaCO2 / HCO3
7.28 / 50 / 23
7.10 / 38 / 14
7.48 / 55 / 34
→ Respiratory Acidosis
→ Metabolic Acidosis
→ Metabolic Alkalosis + Respiratory compensation
Case #1
60 y/o woman with HTN, admitted after 7 days of severe vomiting. Appears ill, hypotensive with tachycardia (+) Rebound tenderness w/ no bowel sounds
BMP – 140/3.2/80/11/90/3<90 ABG – 7.29 / 24
AG Metabolic acidosis + Metabolic alkalosis
Case #2
64 y/o man admitted to ICU for PNA and septic shock. 4 days of SOB and fever Afebrile, BP 85/50, HR 110, RR 22 (+) Crackles and heart murmur, pedal edema
BMP – 135/4.8/103/10/22/1.4<115, Albumin=3.8
ABG – 6.94 / 48 / 51
AG Metabolic acidosis + Respiratory acidosis
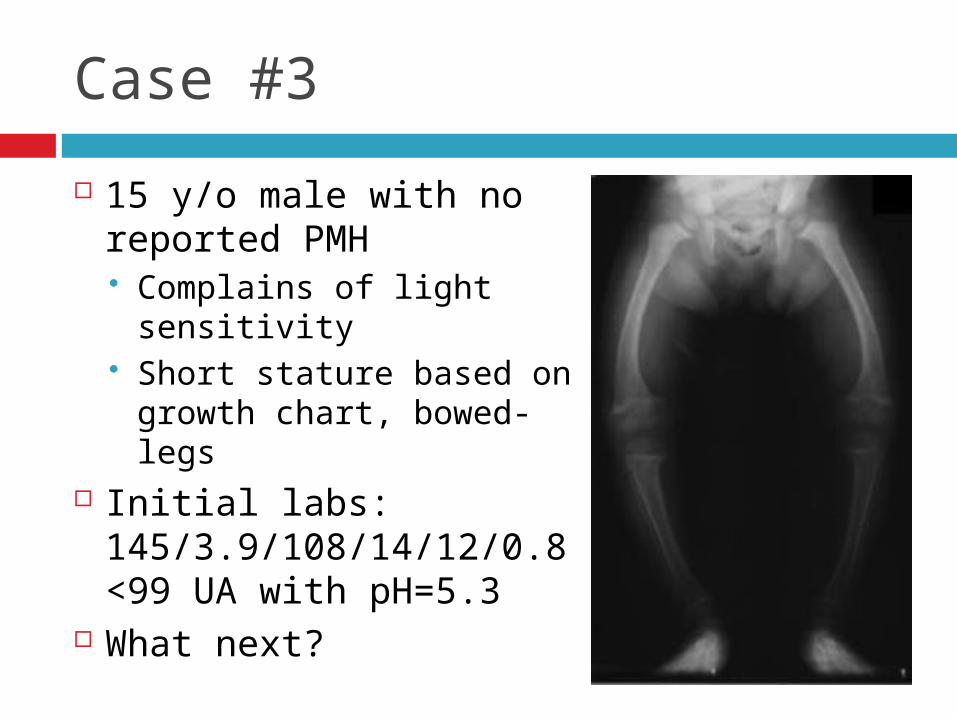
Case #3
15 y/o male with no reported PMH Complains of light sensitivity Short stature based on growth
chart, bowed-legs Initial labs:
145/3.9/108/14/12/0.8<99 UA with pH=5.3
What next?
Case #4
44 y/o female with cirrhosis, HD#2 for fever and abdominal pain Meds: Spironolactone, Lasix, Lactulose Tm=100.8, BP 74/55, HR 72 Appears cachetic Abdomen distended, (+) TTP, 1+ BLE edema
BMP – 128/5.1/104/12/20/1.3<84, Albumin=1.4 ABG – 7.25 / 28 / 78
AG Metabolic acidosis
Case #5
66 y/o man with type II DM, HTN 8 days of diarrhea, abdominal pain, decreased PO Grandson w/ similar symptoms 1 week ago Meds: Enalapril, Atenolol, HCTZ, Metformin Normal vitals, (+) FOBT
BMP – 136/3.9/114/13/21/1.2<128, Albumin=4 Urine pH=6, UNa=32, UK=21, UCl=80 ABG – 7.27 / 30 / 90
Non-anion gap Metabolic acidosis
Metabolic Alkalosis
Metabolic Alkalosis Initiation: Net loss of H+
Net addition of HCO3- (alkali ingestion) External loss of fluid containing Cl- (contraction alkalosis)
Maintenance mechanisms: Cl- depletion K+ depletion Hypercapnea Rarely; primary disorders of specific ion channels in the
Loop of Henle, distal tubule or collecting ducts
Chloride Depletion
Selective Cl- (eg nasogastric suction) produces a major increase in serum bicarbonate
Low urine chloride K+ depletion sustains the metabolic alkalosis
Increases H+ secretion via H+ / K+ ATPase Increase NH4
+ production and excretion
Sources of Cl- responsive alkalosis
Vomiting and NG suction Diarrhea
Congenital Chloride Diarrhea Villous Adenoma
Diuretics Loop diuretics Metolazone Thiazides
Post-hypercapneic state
Chloride-resistant Metabolic Alkalosis
Mineralocorticoid excess 1° hyperaldosternism Adenoma Cushing’s syndrome ACTH tumor Renin tumor Androgenetic syndrome Fludrocortisone
treatment
Apparent excess of mineralocorticoid Licorice or Altoids
(Glycyrrhizic acid) Liddle’s syndrome 11B-Hydroxysteroid
dehydrogenase deficiency
High-dose Glucocorticoids
Normotensive Severe K+ deficiency Bartter’s and Gitelman’s
Exogenous Alkali
Persistent metabolic alkalosis when the body is deficient in K+ or Cl- stores
Hypercalcemia Milk alkali syndrome (Ca2+ containing antacids) Alkali administration Massive pRBC transfusion >10U (Citrate) Refeeding syndrome
Management of Metabolic Alkalosis
Treat underlying condition If severe pH > 7.60 treat with hemodialysis Chloride Responsive
Normal Saline or ½ Normal Saline Rate 50-100 cc/hr over maintenance rate Replete K+
PPIs minimize gastric losses If diuretic induced can use K+ sparing diuretics to limit
alkalosis
Management of Metabolic Alkalosis
Chloride Resistant: In a patient in an edematous state
Acetazolamide Mineralocorticoid excess; restoration of normal
mineralocorticoid activity Surgical Removal K+ sparing diuretics + K+ supplements
Bartter’s and Gitelman’s syndrome K+ sparing diuretics + K+ supplements NSAIDs (Bartter’s)
Recommended