Menopause Update:
Focus on Hot Flashes, Atrophic Vaginitis
R. Mimi Secor, MS, M.Ed, FNP-C,
NCMP, FAANP
Onset, Massachusetts
Doctoral Student, Rocky Mountain University
Provo, Utah
Mimi Secor, MS, M.Ed, FNP-C, FAANP • NP 37 years
• Newton Wellesley ObGyn, Newton, Mass
• National Speaker, Consultant
• Doctoral student, Rocky Mountain University, Provo, Utah
• National Certified Menopause Practitioner, (NCMP), from NAMS
• 2013 Lifetime Achievement Award, MCNP/ Massachusetts NP Association
• Coauthor, Fast Facts: The Gyn Exam for NPs, 2012, Springer
• Coauthor, Advanced Health Assessment of Women: Skills & Procedures, 2010
• President Emerita, Senior Advisor, NPACE
• Fellow in the AANP
• Visiting Scholar at Boston College
• Worked in Alaska for 7 years (1992-1999)
• Owned private practice for 12 years in Cambridge, MA. (1984-1996) Secor 2014 copyright
R. Mimi Secor, MS, FNP, FAANP Disclosure
Speaker: GenPath, Shionogi
Secor 2014 copyright 3
Secor 2014 copyright 4
Menopause Update: Objectives
• Describe epidemiology of menopause, Vasomotor Symptoms (VMS) and Vulvovaginal Atrophy (VVA)
15 minutes
• Discuss diagnosis of VMS and Vulvovaginal Atrophy
20 minutes
• Explain options for treatment of VMS and VVA
25 minutes
Secor 2014 copyright 5
Attended NAMs on a Pfizer DNP Scholarship: North American Menopause Society
Secor 2014 copyright 6
Conference Schedule: Day 1
• Pre-Meeting
• Vulvovaginal Health
• NAMs Competency Exam
• Welcome, Introduction
• Plenary Symposium
• President’s Reception
Secor 2014 copyright 7
Keynote Address- Going Full Frontal: Rewiring Frontal Brain Networks
to Restore Cognitive Health
• Sandra Chapman, PhD, Dallas, Texas
• Brains like to be challenged with “big ideas”
• Doesn’t like too much multi-tasking
• Needs rest
http://www.brainhealth.utdallas.edu/about_us/team/sandra_chapman
Secor 2014 copyright 8
Breakfast Sessions: Topic Tables Dr. Diane Pace, NAMS President
Her Menopause Self-Help Table So Many Great Ways to Cool Off
Secor 2014 copyright 9
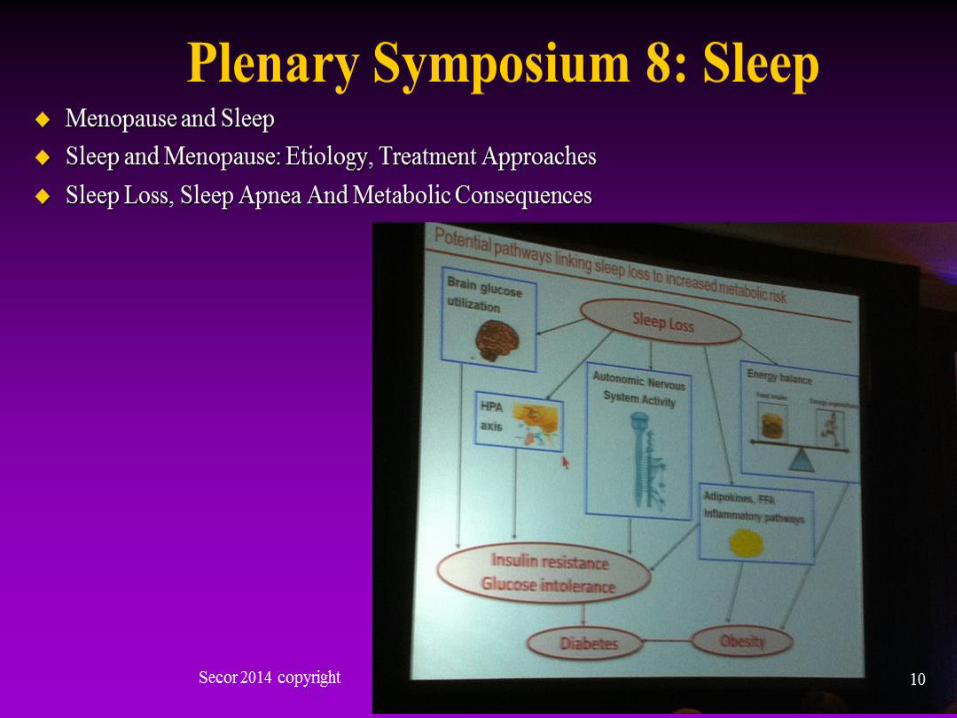
Plenary Symposium 8: Sleep
• Menopause and Sleep
• Sleep and Menopause:
Etiology, Treatment
Approaches
• Sleep Loss,
Sleep Apnea And
Metabolic Consequences
Secor 2014 copyright 10
Plenary Symposium 11 Bioidentical Hormones, What are the Issues?
• What, Why, How?
• Compounded vs FDA Approved: Fact vs Fiction
• Is the Truth About Compounding Knowable?
• Safety, Efficacy, Dosing: unclear!
11
Great Networking too! With Other Menopause NP Experts
Secor 2014 copyright 12
Menopause Diagnosis 52 Million in 2010: 6,000 day
• Average age 50-52 years
• 12 months since FMP (final menstrual period)
• NO labs needed
• FSH over 30 mIU/m
– l week off CHC*, or 1 month if inconclusive
• Estradiol < 20 pg/ml
• Vasomotor symptoms
• Contraception x 12 months after FMP!!!
*CHC/ combination contraceptive contraceptive
Secor 2014 copyright 13
Vasomotor Symptoms (VMS) Epidemiology
• Common
• 75% of perimenopausal women experience these
• Caused by fluctuations in hormones
• BUT exact mechanism unclear
• Duration x 6 months- 2 years, up to 5-12+ years
• 10-25% C/o severe symptoms
• Ethnic variation: African American 46%, Japanese 18%
• Surgical menopause = More severe symptoms
Secor 2014 copyright 14
VMS: Non-Pharmacologic Rx
• Paced respirations
• Dress in cool layers
• Healthy body weight
• Avoid smoking which has some effect on estrogen metabolism and increases risk of flushes
• Avoid personal hot flash triggers (hot drinks, caffeine, spicy foods, ETOH, emotional reactions).
– Devices such as cooling pillows (Chillow Pillow® ), Bed Fan®, wicking clothing/pajamas, wicking sheets/pillow cases
Secor 2014 copyright 15
“Wicked Sheets” for Hot Flashes
Secor 2014 copyright 16

VMS: Non-Pharmacologic Rx
• Exercise
• Yoga
• Acupuncture
• Herbals:
–Remifemin: Studies pending
• Isoflavones: modestly effective
• Progesterone cream: OTC, unclear efficacy, safety, esp. endometrial effects
Secor 2014 copyright 17
Estrogen for VMS? Per NAMS
• Benefits of HT/ET are more likely to outweigh risks for symptomatic women before the age of 60 years or within 10 years after menopause.
Secor 2014 copyright 18
HT* for VMS: Risk per NAMS 2012
• The risk of venous thromboembolism and ischemic stroke increases with oral HT but the absolute risk is rare below age 60 years.
• The dose and duration of HT should be consistent with treatment goals & safety issues & should be individualized
• And for the shortest period of time, lowest dose.
*Hormone therapy = Estrogen, Progesterone/progestin
NAMS. (2012). Position statement: The 2012 HT position statement of the North American Menopause Society. Menopause, 19 (2), 258-271.
Secor 2014 copyright 19
HT for VMS: Risk Breast Cancer
• Risk in women >50 years associated with HT is a complex issue.
• Increased risk is primarily associated w/ addition of progestogen to estrogen therapy and duration of use.
• The risk of breast cancer attributable to HT is small and the risk decreases after treatment is stopped.
• No increase seen in Estrogen-only arm (CEE) of WHI study up to 7.1 years (Anderson et al. (2012). Lancet Oncol, 13 (5), 476-486).
• Increase with EPT group after 3-5 years
(NAMS position statement, 2012).
Secor 2014 copyright 20
Vasomotor Symptoms: Treatments
• Systemic estrogen; Oral, Vaginal, Transdermal
• Estrogen, versus Non-estrogen (Ospemifene)
• Very effective
• Safe in early peri, post-menopause
• Less safe age 70 and over
• Less safe as BMI increases
• Lowest dose for the shortest duration
Per NAMS, www.menopause.org
Secor 2014 copyright 21
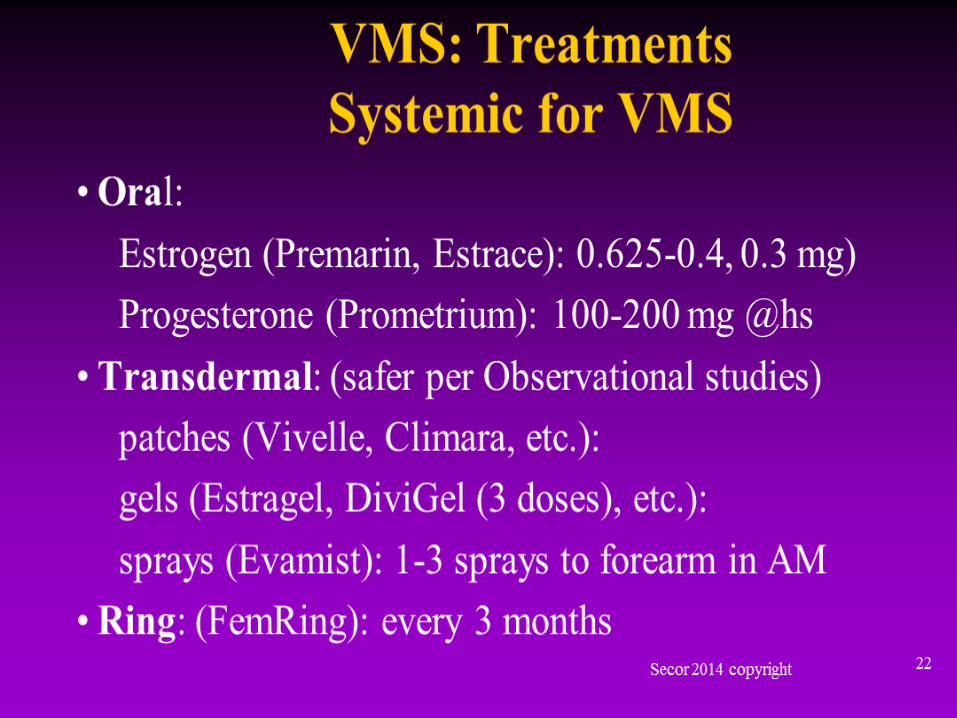
VMS: Treatments Systemic for VMS
–Oral:
Estrogen (Premarin, Estrace): 0.625-0.4, 0.3 mg)
Progesterone (Prometrium): 100-200 mg @hs
–Transdermal: (safer per Observational studies)
patches (Vivelle, Climara, etc.):
gels (Estragel, DiviGel (3 doses), etc.):
sprays (Evamist): 1-3 sprays to forearm in AM
–Ring: (FemRing): every 3 months
Secor 2014 copyright
22
VMS: Non Hormonal Rx
• Non-hormonal pharmacological options such as antidepressants, antihypertensives, and anticonvulsants are available for management of vasomotor symptoms
although…
• Most are not FDA approved for this purpose.
• New non-hormonal drugs for management in menopause did obtain FDA approval in 2013.
Secor 2014 copyright 23
Paroxitene (Brisdelle) Low Dose
• Approved by the FDA for hot flashes
• Dosing 7.5 mg PO daily
• Effective
• Safe
• Few side effects
• Alternative if estrogen contraindicated
• Possible reduced anxiety
Secor 2014 copyright 24
VMS: Patient Education
• Must be thorough, empathetic, resourceful
• Handouts, websites, etc.
Secor 2014 copyright 25
Vulvovaginal Atrophy (VVA)
Algorithm: Vulvar Symptoms Atrophic Vaginitis
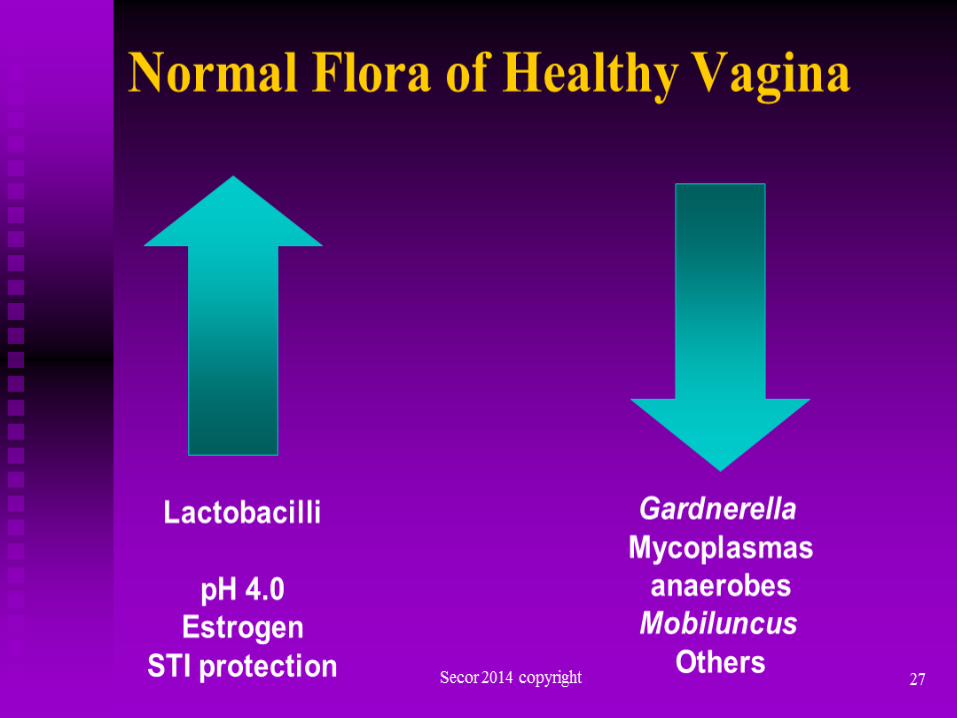
Normal Flora of Healthy Vagina
Secor 2014 copyright 27
Lactobacilli
pH 4.0
Estrogen
STI protection
Gardnerella
Mycoplasmas
anaerobes
Mobiluncus
Others
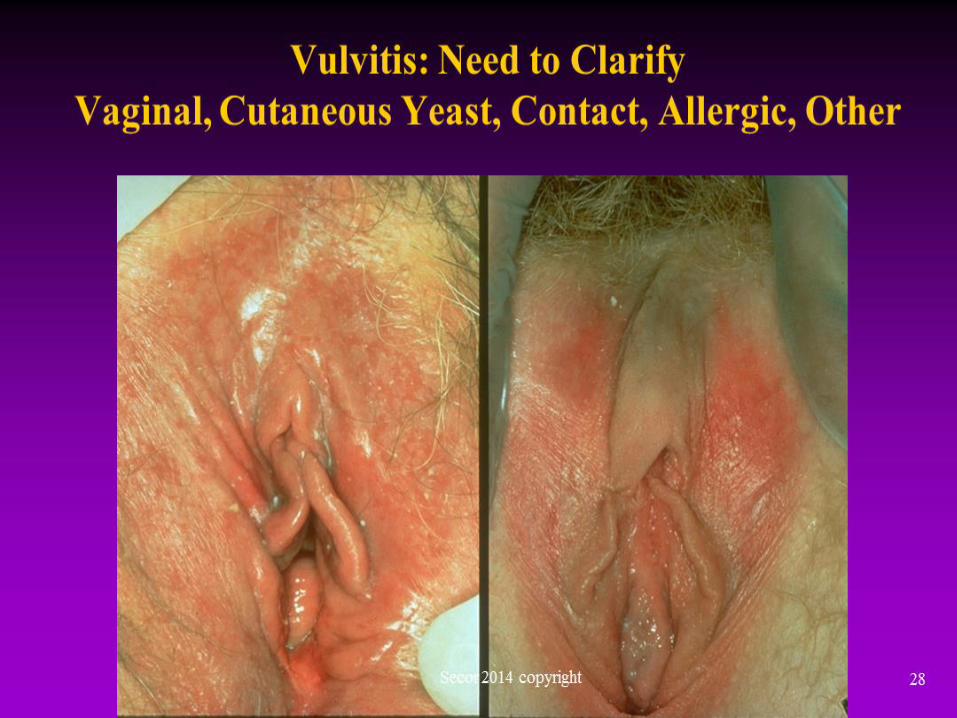
Vulvitis: Need to Clarify Vaginal, Cutaneous Yeast, Contact, Allergic, Other
Secor 2014 copyright 28
Vulvar Symptoms
• Irritants, over cleansing
• Allergens
– Condom allergy is rare
• Infections
– Genital Herpes Type 2
• Skin conditions
– Lichen Simplex Chronicus/ LSC
– Lichen Sclerosis / LS
– Lichen Planus / LP
– Other
• Eczema, atrophy, etc..
Secor 2014 copyright 29
Vulvovaginal Atrophy (VVA)
• 1/3 of menopausal women affected
• Irritation
• Dryness
• Dyspareunia
• Regular sex
• Middlesex.md for vibrators
• Trojan mini-vibrator
• OTC lubricants Secor 2014 copyright 30
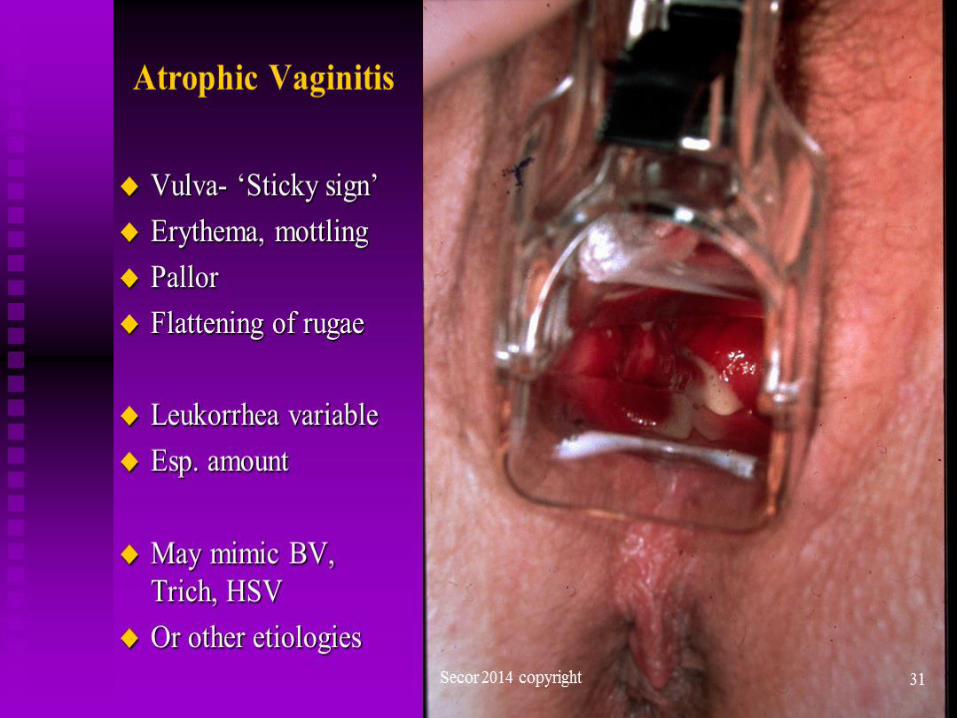
Atrophic Vaginitis
• Vulva- ‘Sticky sign’
• Erythema, mottling
• Pallor
• Flattening of rugae
• Leukorrhea variable
• Esp. amount
• May mimic BV, Trich, HSV
• Or other etiologies
Secor 2014 copyright 31
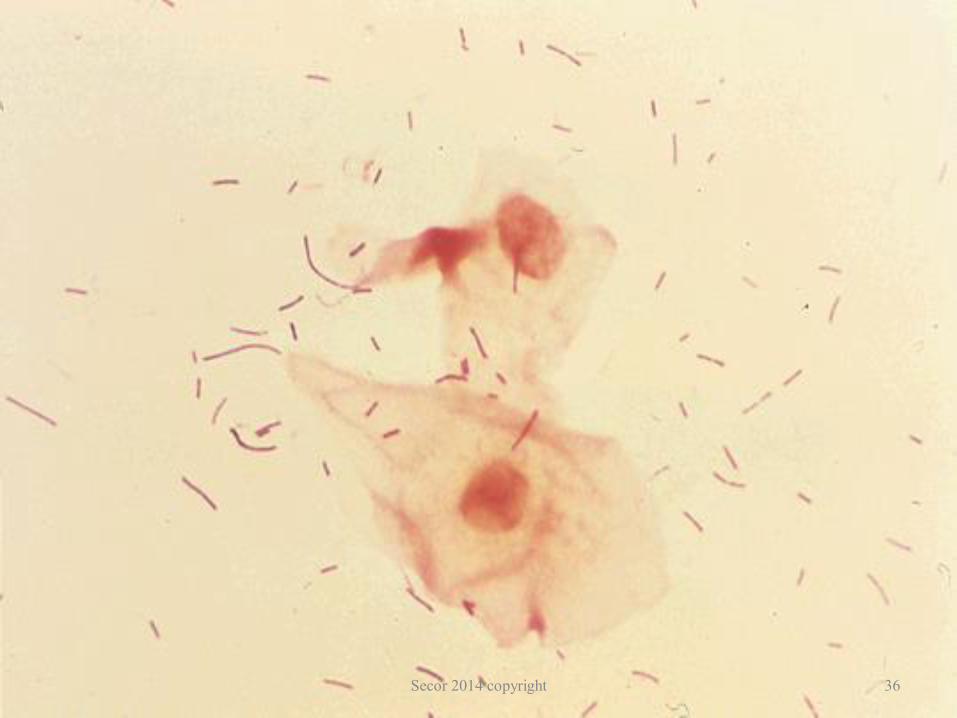
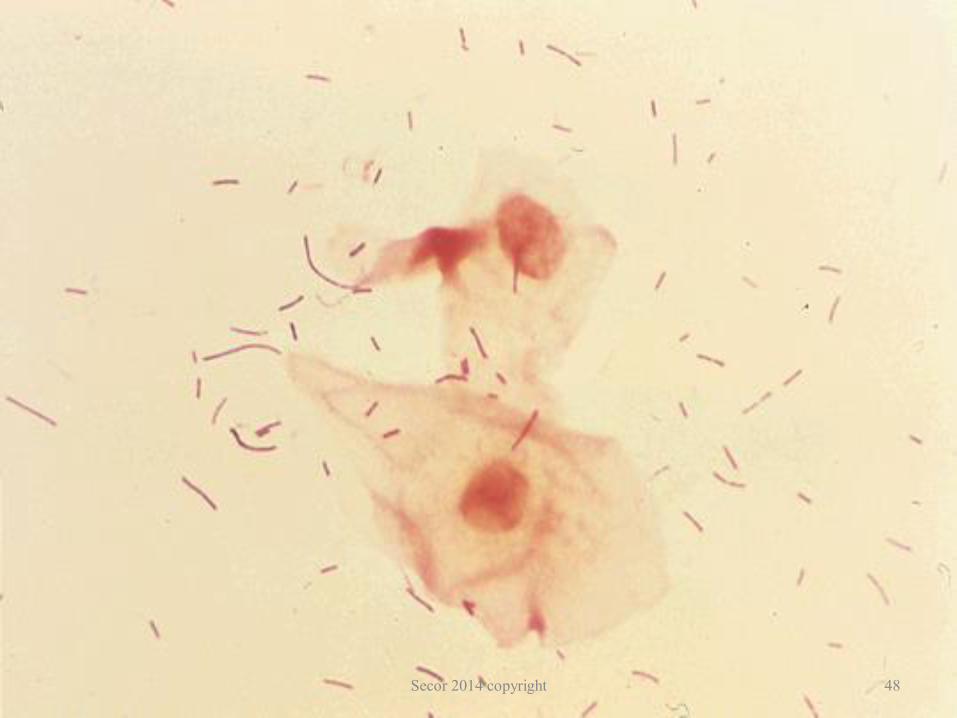
Diagnostic Work up of Atrophic Vaginitis
• Vaginal pH abnormally high > 5
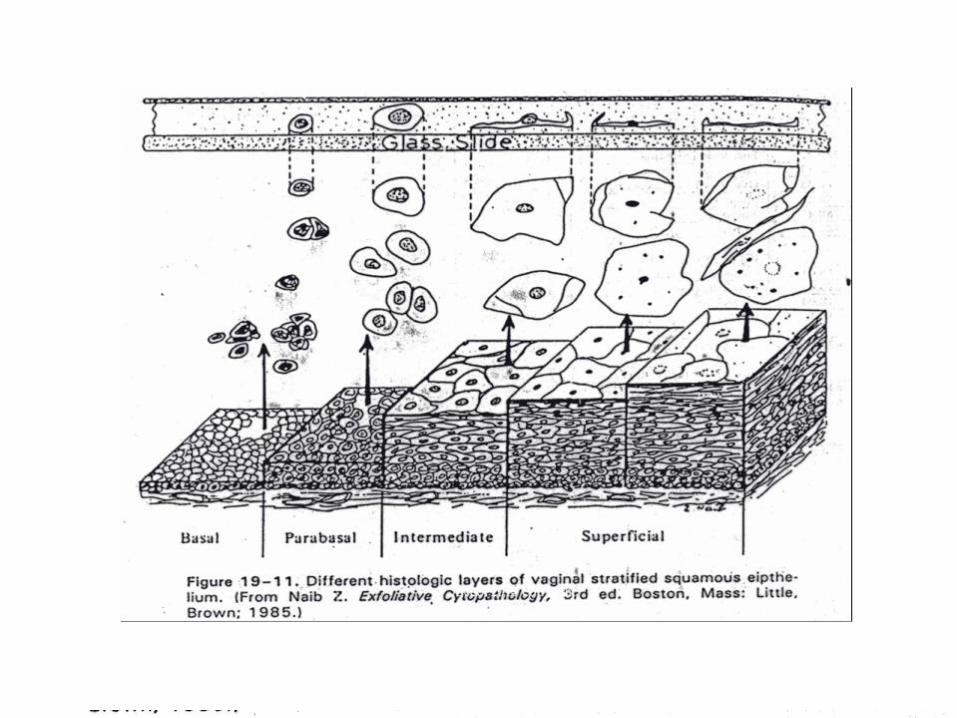
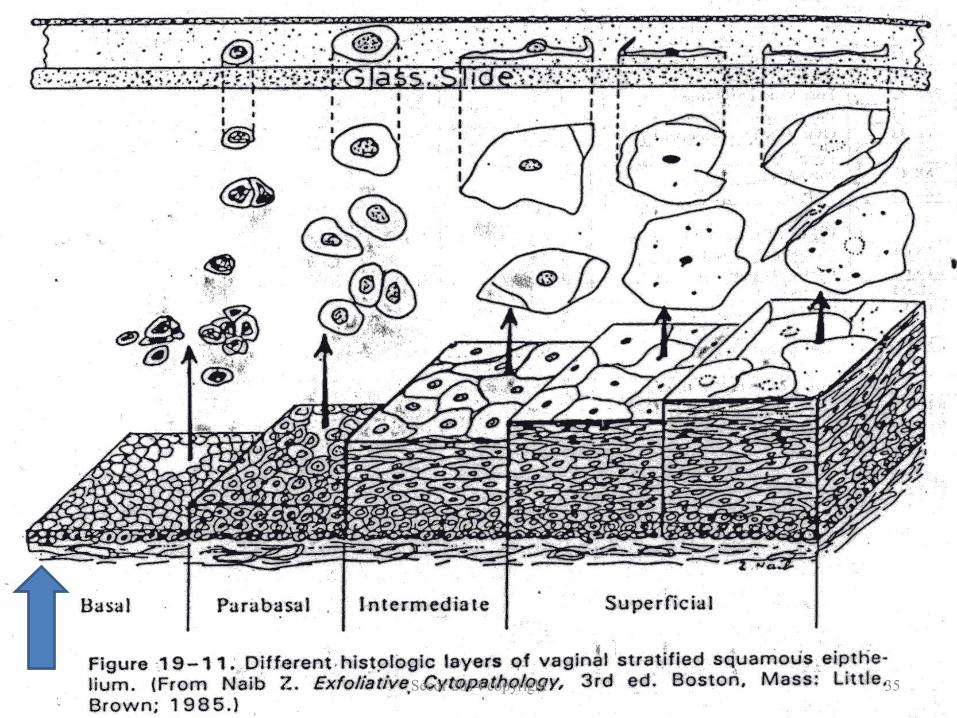
– Proxy test for estrogen levels = maturation index
• Negative Amine KOH ”Whiff “test
• Few Lactobacilli
• Mixed bacteria, grainy epithelial cells
• WBCs variable
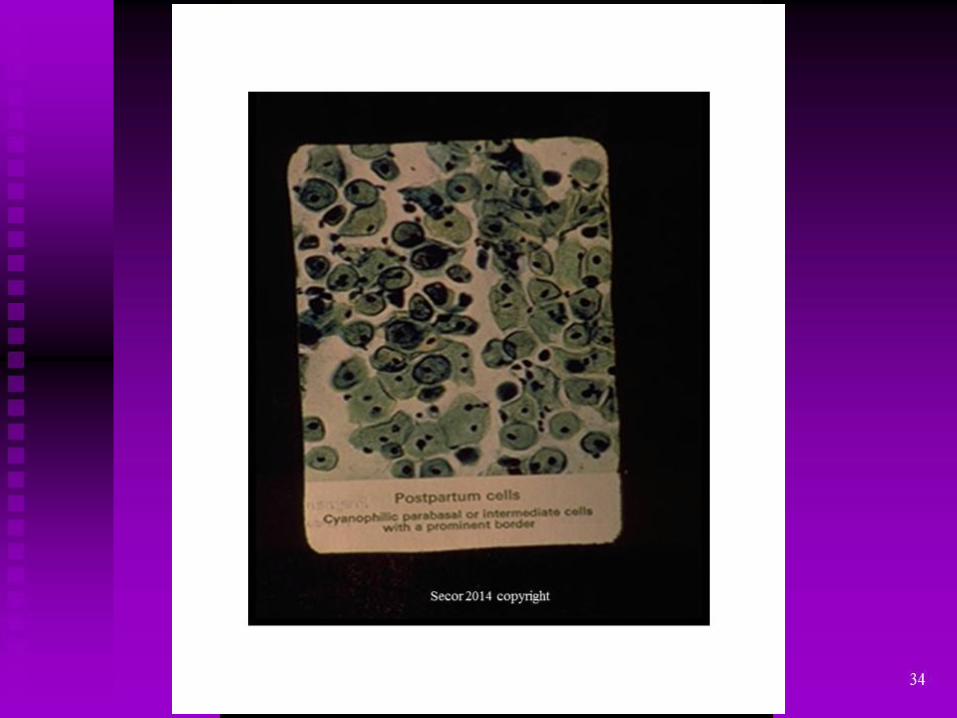
• Immature epithelial cells, maturation index
• Avoid non-specific vaginal cultures, Pap inaccurate
• Test for STIs as appropriate!
Secor 2014 copyright 32
Secor 2014 copyright 33
Secor 2014 copyright 34
Secor 2014 copyright 35
Secor 2014 copyright 36
Atrophic = Abnormal Vaginal pH, CPT code 83986
• pH Range 4.0-7.5
Normal = 4.0-4.5 (proxy for normal estrogen levels)
BV, Trich, Atrophic = > 4.7
• CLIA Waived
• Nitrazine Vaginal pH test “NitraTest”: order by roll
• Requires multiple steps,
• Match color with numerical pH reading (yellow=4.0 normal)
• NEW: Vaginal pH Swab Test “VS-Sense”: 90% accurate
• Rapid results: 10 second test for BV, Trich, Atrophy
• Yellow swab = Normal pH
• Blue swab = Abnormal, elevated pH
Secor 2014 copyright 37
Secor 2014 copyright 38
negative positive
Differential Diagnosis
• BV
• STIs; Trichomoniasis, Herpes, etc.
• Precancers
• Vulvar dermatoses – Lichen sclerosis
– Lichen simplex chronicus
– Lichen planus
– Irritant, allergen, eczema, etc..
Secor 2014 copyright 40
VVA Treatments: Low Dose Rx for VVA Vaginal or Oral (NEW)
– Pt preference, symptoms, safety, efficacy, impact decision to treat
– Do NOT use ORAL estrogen for VVA symptoms only
Secor 2014 copyright 41
Local Vaginal Estrogen Options:
Minimal Systemic Absorption Progestin NOT NEEDED
Sig: Daily for 2-4 weeks, every other day, then twice weekly prn
– Vaginal estrogen creams: 0.5-2 gms pv at bedtime • Conjugated Equine Estrogen /CEE “Premarin” • Estradiol “Estrace”, etc..
– Estradiol vaginal tablet “Vagifem” 10 mcg dose ONLY • If dry atrophy, or introital dyspareunia, less effective?
Bachman et al, Ob Gyn. 2008 jan;111(1):67-76 (RCT) – Vaginal estradiol ring “Estring”: every 3 months
• Effective, convenient, may help OAB as pessary
Secor 2014 copyright 42
Atrophic Vaginitis: Local Vaginal Estrogen Prevent Secondary VVC/Yeast – 50%
Risk!
• Daily for 2 to 4+ weeks; longer if comorbidities
• Twice Weekly maintenance PLUS
• Daily Introital application: KEY (Sticky glove sign)
Probably OK if Breast Cancer history
• Minimal systemic absorption
– Breast tenderness: initially secondary to thin epithelium
– Contraindicated: if breast cancer history BUT
– DUB: EMB and Ultrasound MANDATORY (even 1 drop)
• Sexual rehab: COMPLEX!
– Dilator exercises, regular sex, lubricants, romance, sleep
– Orgasm before intercourse, Manage OAB, Hot flashes, Vv, etc..
Secor 2014 copyright 43
Enhancing the Sexual Experience In Menopause
Clitoral Stimulator
Middlesex MD
Resource for Vibrators, Education, etc..
Secor 2014 copyright 44
Ospemifene (Osphena)
• NEW: Shionogi, www.MyOsphena.com • Non-estrogen, SERM, agonist to vulvar/vagina
• Oral 60 mg tablet
• Daily with food (fatty meal best)
• Similar efficacy to estrogen, 4 week response
• Avoid: Current cancer, CVD, stroke
• Side effects: Hot flashes, incr. vaginal discharge
• Breast or Bone effects: no research
Secor 2014 copyright 45
Top Scoring Abstract Sessions
1. Efficacy of Gabapentin in Rx of VMS in Menopause
2. Transdermal Testosterone Improves SSRI Reuptake Inhibitor-Associated FSD
3. Safety of Oral Ospemifene in Phase 2/3
4. Effects of Stellate Ganglion Block on VMS
Oral Ospemifene, Phase 2/3
Secor 2014 copyright 46
Abnormal Vaginal Bleeding
• For any vaginal bleeding 12 months after FMP
• FMP = final menstrual period
• If after intercourse
• Or just random
• Even if only spotting, 1 time, or 1 drop blood
MUST ORDER:
• Transvaginal ultrasound (Must do with EMB)
• Endometrial biopsy (EMB): > 5 mm Endom. Stripe
Secor 2014 copyright 47
Secor 2014 copyright 48
References
• Freeman, EW, et al. (2011). Duration of VMS and associated risks. Obstet Gynecol, 117 (5),1085-1104.
• Honjo, H., et al. (2009). Low-dose estradiol for climacteric symptoms in Japanese women: A randomized controlled trial. Climacteric, 12(4), 319-328.
• Laliberte, F, et al. (2011). Does route of administration for ET impact risk of VTE? Menopause,18 (10), 1052-1059.
• NAMS. (2013). Position statement: Management of symptomatic VVA. Menopause, 20 (9), 888-902.
• Roach, RE. et al. (2013). The risk of VTE in Women over 50 using oral contraception or postmenopausal hormone therapy. J Thromb Haemost, 11 (1), 124-131.
• Scarabin, PY, et al. (2003). ESTER study group: Oral vs transdermal ET and VTE. Lancet, 362 (9382), 428-432.
Secor 2014 copyright
49
References • Alexander, I. M. & Andrist, L. C. (2013). Menopause. In K. D. Schuiling & F. E.
Likis (Eds.). Women’s Gynecologic Health (2nd ed.) (pp 285-328). Burlington,
MA: Jones & Bartlett Learning.
• De Villiers,T. J., Gass, M. L. S., Haines, C. J., Hall, J. E., Lobo, R. A., Pierroz, D.
D., & Rees, M. (2013). Global consensus statement on menopausal hormone
therapy. Climacteric. 16, 203–204.
• Freeman, et al. (2011). Duration of menopausal hot flushes and associated risk
factors. Obstet Gynecol, 117 (5), 1095-1104.
• North American Menopause Society (NAMS). (2010). Menopause practice: A
clinician’s guide (4th ed.). Cleveland. OH: Author.
• North American Menopause Society (NAMS). (2013). Management of
symptomatic vulvovaginal atrophy: 2013 position statement of The North
American Menopause Society. Menopause: The Journal of The North American
Menopause Society, 20(9), 888-902.
• Stuenkel, C. A., Gass, M. L. S., Manson, J. E., Lobo, R. A., Pal, L., Rebar, R. W., &
Hall, J. E. (2012). A decade after the Women’s Health Initiative-The experts do
agree. Menopause: The Journal of The North American Menopause Society,
19(8).
Secor 2014 copyright
50
Thank You and Good Luck! Questions Welcome
R. Mimi Secor, MS, M.Ed, FNP-C,
NCMP, FAANP
www.MimiSecor.com
Facebook, LinkedIn, Twitter
YouTube, Blog
Secor 2014 copyright 51
Recommended