Measurement of Pulmonary Artery to Aorta Ratio in Computed Tomography is Correlated
with Pulmonary Artery Pressure, but not with Mortality in Critically Ill Chronic
Obstructive Pulmonary Disease Patients
Ebru Ortaç Ersoy , Mine Durusu Tanriover , Atilla Kara , Serpil Ö cal, LaleOzisik , Meltem Gulsun Akpinar, Arzu Topeli
Hacettepe University Faculty of Medicine
Medical Intensive Care Unit
Ankara, Turkey

Introduction
• Identification of COPD patients at high risk for complications and mortality is important.
• Severe pulmonary hypertension (PHT) may develop as an important complication of COPD.
• Echocardiography for detection of PHT is not optimal, especially in critically-ill patients withunderlying lung diseases because of air trappingand difficulty in optimal positioning of patients.

• Computed tomography (CT) can be used to measure the ratio of the diameter of the pulmonary artery (PA) to the diameter of the aorta (A).
• PA/A ratio was shown to be correlated with pulmonary artery pressure (PAP) in COPD exacerbation.

Aims
• PA enlargement, as shown by PA/A ratio >1 could be associated with a higher risk of mortality in COPD patients admitted to the ICU with acute exacerbation.
• PA/A ratio correlates with PAP.

Patients - Methods
• Medical ICU of a University Hospital in Turkey.
• January 2008 and December 2012
• Acute exacerbation of COPD
• CT scan performed within the last 6 months of
admission

Variables
• Age and gender
• APACHE II scores
• Echocardiographic results as pulmonary artery pressure (PAP) and ejection fraction (EF)
• PaO2, PaCO2
• Computed tomographic calculation of PA and A
• Presence of mechanical ventilation (IMV, NIMV)
• Length of ICU stay
• ICU mortality rate


Statistical Analysis
• Comparisons of data of patients were made between the groups.
• Correlation analysis between PA/A and ICU mortality; PAP and APACHE II; PAP and PA were done.
• Survival analysis was performed by Kaplan Meier curve and significance was assigned with log rank test.
• Logistic regression analysis was used to determine independent risk factors for mortality.

All Patients P/A >1
n=40
P/A ≤1
n=66
p
Age 71.1±9.5 73.1±9.7 69.9±9.4 0.12
Male gender (%) 46 (43) 22 (55) 23 (34.8) 0.04
APACHE II 18±6.2 18.8±5.1 17.2±6.2 0.09
PAP*, mmHg 51±21.3 62.1±23.2 45.3±17.9 0.002
Pulmonary artery diameter, mm 35.3±12.1 41.8±16.5 31.3±5.8 0.001
Aorta diameter, mm 35.8±4.9 34.2±14.23 36.9±5.1 0.01
EF*, percentage 56.6±12.3 57.8±12.5 55.8±12.3 0.33
PaO2, mmHg 68.4±37.8 67.8±44.1 68.8±34.1 0.78
PaCO2, mmHg 56.5±19.2 57.8±12.5 55.9±21.1 0.48
IMV (%) 84 (78.5) 30 (75) 27 (40.9) 0.001
NIMV (%) 57 (53.3) 31 (77.5) 53 (80.3) 0.73
Length of ICU stay, days 13±8.8 12.9±8.2 13.03±9.4 0.74
ICU mortality (%) 45 (42.1) 20 (50) 24 (36.4) 0.16

Died
(n=44)
Survived
(n=62)
p
Age 72.5±9.6 70±9.4 0.20
Male gender (%) 20 (44.4) 26 (41.9) 0.93
APACHE II 18.8±7.7 17.4±4.8 0.35
PAP*, mmHg 53.6±25.5 50±18.8 0.66
Pulmonary artery diameter, mm 35.3±10.6 35.3±13.1 0.56
PA/A >1 (%) 20 (44) 20 (32.3) 0.26
PaO2, mmHg 64.5±28.7 71.3±43.2 0.41
PaCO2, mmHg 55.1±22.1 57.5±17.1 0.16
NIMV (%) 30 (68.2) 54 (87.1) 0.03
IMV (%) 29 (65.9) 28 (45.2) 0.05
Length of ICU stay, days 14.9±10.9 12.1±6.9 0.60


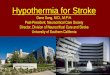
(r=0.51, p=0.001) (r=0.25, p=0.025)

For PHT
• PA diameter (with a cut off value of ≥ 28 mm)
– Sensitivity = 89.2% (79.1-95.1)
– Specificity = 54.5% ( 23.4-83.3)
– AUC = 0.678 (CI 95% = 0.561 -0.780; p=0.104)

Discussion
• Accurate estimation of prognosis in COPD patients with
acute exacerbation is important.
• It is very difficult to measure FEV1 in ICU patients
because of presence of air hunger and respiratory failure.
• Echocardiography has also some limitations.
• CT is a valuable tool in the evaluation of both lung
disease and intrathoracic vasculature in patients with
COPD.

Discussion
• Prior studies have demonstrated that;
– PA/A ratio measured on CT did correlate with PAP
– Wells et al. found a correlation between PA/A >1 and the
risk for development of acute exacerbations of COPD
– PA/A ratio >1 was associated with increased mortality in
COPD patientsWells JM, et al. N Engl J Med 2012, 367:913-921.
Ng CS, et al. J Thorac Imaging 1999, 14:270-278.
Iyer AS, et al . Chest 2014, 145:824-832

Conclusion
• This was the first study performed in an ICU setting.
• PA/A ratio is an easily measured method that can be performed on thoracic CT scans for detectingPHT.
• CT scan measured PA diameter or PA/A ratio can be used to predict PAP and prognosis in COPD patients who are admitted to ICU in respiratoryfailure.
Recommended