HEAD TRAUMA PATHOPHYSIOLOGY, EVALUATIONAND TREATMENT
Martin Young DVM , MS, DACVIM
Mike Higginbotham, DVM, DACVIM
Blackwater Falls

Overview
• Common causes• Pathophysiology• Presenting signs

Common Causes
• Hit by automobile• Falls
Stairs• Kicks• Penetrating
wounds• Bites
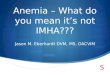
Types of Brain Injury
• Primary injury – initial insult. Function of trauma and forces.
Linear, rotational Coup vs counter coup
www.mdusd.k12.ca.us

Primary Injury
• Concussion Brief loss of consciousness
• Contusion Bruising of parenchyma and secondary edema
• Tissue laceration Physical disruption of the parenchyma
• Intra-axial and extra-axial hematomas

Types of Brain Injury
• Secondary injurycascade of biochemical pathways initiated which lead to further brain injury and increased intracranial pressure (ICP).
• Edema •Vasogenic and cytotoxic vicious cycle of tissue damage

Secondary Injury
• Occurs minutes to hours after initial insult• Series of events that perpetuate and initiate
cellular damage• Driven primarily by cerebral ischemia
Hypotension, hypoxia, and perfusion

Secondary Injury
• Hypotension, hypoxia, and perfusion
• ATP depletion
• Na+ and Ca++ influx
• Cytotoxic edema Depolarization
Other cascades Glutamate

Secondary Injury
Platt & Olby. BSAVA Manual of Canine and Feline Neurology

Intracranial Pressure Dynamics
• Pressure autoregulation MABP
• Chemical autoregulation PaCO2
• Intracranial compliance Monroe-Kelly Doctrine
• CPP = MABP – ICP Volume
Pressure

Fractures

“Tippy”

Intracranial Bleeding
• Epidural
• Subdural / subarachnoid
• Parenchymal

Intracranial Bleeding
Subdural / Subarachnoid

“Piper”

FLAIRT2 image

Herniation

Head Trauma
Assessment

Looking for head trauma
• 25% of trauma patients have head trauma• MGCS – only evaluates BS function• PTE is a common cause of epilepsy 6.8%• 36% of head trauma patients had seizures• DWI - hemorrhage detected by 30 min• MRI is useful for prognostication

Step 1:
• Focus on ABC’s
• Correct hypoxia and hypotension first, will help the brain as well as the rest of the patient and will allow you to better assess your patients neurological status
• Baseline labwork: PCV, TS, CBC, Chem, Urinalysis, and Wt.
• Can’t accurately assess the mentation of a shocky patient!

Postures and respiration
• Postures: decerebrate vs decerebellate vs schiff sherrington
• Respiration: Cheyne-Stokes – deep cerebral and rostral BS –rapid
breathing followed by apnea Central hyperventilation – 25/min – regardless of CO2
content – midbrain to Pons Irregular gasping – caudal BS - terminal

Head Trauma-signs-• Gait and Posture
Paresis, circling, paralysis Normal, opisthotonus, decerebrate rigidity
• Mental status Bright, depressed, stuporous, comatose
• Vestibular signs• Pupils
Size, symmetry, response to light
Decerebrate rigidity

Step 2:
• Part 1 complete. Patient is normovolemic and normotensive and we have established appropriate oxygenation and ventilation
• Assess the rest of the patient: Nervous system, vertebral fractures/ luxation, lungs, abdomen,
musculoskeletal
• Additional Diagnostics: Radiographs: skull, abdomen, thorax Additional bloodwork if indicated MRI/CT, electrodiagnostics

Modified Glasgow Coma Scale
• Published in a 2001 JVIM article by Dr. Simon Platt
• Evaluates the patient using 3 criteria and assigns a severity score from 1-6 to each:
Level of Mentation Motor Function Brainstem Reflexes
• Score assigned from 3-18; higher the score, better prognosis

Basic Levels of Mentation
• Bright, alert, responsive• Obtunded
Dull, depressed but responsive to all manner stimuli
• Semi-coma responsive to stimuli
• Stuporous responsive only to noxious stimuli
• Comatose unconscious, non-responsive to any stimuli

MGCS: Levels of Mentation• 6 - BAR or intermittent periods BAR
• 5 – obtunded – clouded consciousness
• 4 – semi-coma - responsive to visual stimuli
• 3 – semi-coma - responsive to auditory stimuli
• 2 – stuporous – responsive to vigorous stimulation
• 1 - comatose

LOA

Brain Stem Reflexes• 6 - Normal PLR and oculocephalic reflex (OcR)
• 5 - Slow PLR, normal to slow OcR
• 4 - Bilateral unresponsive miosis, normal to slow OcR
• 3 - Pinpoint pupils, reduced to absent OcR
• 2 - Unilateral, unresponsive mydriasis, reduced to absent OcR
• 1 - Bilateral, fixed dilated pupils

Pupil Chart
De Lahunta - Vet Neuroanatomy

Oculocephalic Reflex• AKA - conjugate eye movements
• Pathway between the vestibular system and the extraocular muscles to coordinate eye movements
• Pathway travels through the central brainstem in the medial longitudinal fasciculus before connecting with CN III, IV and VI and exiting the brainstem
• Loss of oculocephalic reflex = Poor Prognosis Denotes severe brainstem damage

MGCS: Motor Assessment• 6 - Normal gait, normal spinal reflexes
• 5 - Hemiparesis, tetraparesis
• 4 - Recumbent, intermittent extensor rigidity
• 3 - Recumbent, constant extensor rigidity
• 2 - Recumbent, constant extensor rigidity w/ opisthotonus (decerebrate rigidity)
• 1 - Recumbent, hypotonia of muscles, depressed/absent spinal reflexes

MGCS Score
• Now, have your MGCS score, what does it mean?
Score 15-18: Good prognosis Score 9-14: Guarded prognosis Score 3-8: Grave prognosis
• A linear association between score during first 48 hours and patient overall prognosis
• Score = 8 in the JVIM paper resulted in 50% mortality

Cushing Reflex• KEY: Decreased mentation, high systemic MAP, low heart rate -
suspect high ICP
Increased ICP results in decreased CBF which regionally increases CO2 concentration
High CO2 sensed by vasomotor center in the brain and triggers a massive sympathetic discharge resulting in a peripheral vasoconstriction
Result is a rise in MAP to maintain CPP
Activates baroreceptors creating the reflex bradycardia

Forebrain
• Can have fewer signs• Seizures• Menace deficit• Behavior changes• Sensory/proprioceptive deficits (contralateral)
• Large circles to the lesion• Altered homeostasis (temperatue, heart rate, blood pressure)

Imaging
• Radiographs Unlikely to reveal additional clinically useful information but may show depressed skull fractures
• Presence of a skull fracture has not been shown to be a negative prognosticator
• Often, CT or MRI warranted to assess for severity of injury, hemorrhage, and herniation
Head Trauma
Treatment

Treating the Head Trauma Patient
• Therapeutic Options:
Mannitol/hypertonic saline
Fluids Anticonvulsants Antibiotics Steroids?
Oxygen Nutrition Analgesia Patient care

Mannitol: MOA Osmotic diuretic: decreases vasogenic cerebral edema and
decreases ICP
Reflex cerebral vasoconstriction as a result of decreased blood viscosity
Free-radical scavenger
Improves microvascular flow; shrinks RBCs by 15% and improves deformation and cell wall flexibility hence improving tissue oxygenation

Hypertonic saline MOA
• Osmotic draw: pulls fluid from interstitial and intracellular space
• Improves: MAP, CBP and CBF
• Volume expansion: not used in dehydration or hypernatremia.
• Can cause vago-reflex – may need atropine

Mannitol/hypertonic saline
• Indications: Clinical indication of increased ICP Progressive decline in neurological status Cushing’s reflex
• Dose: • mannitol 1 to 1.5 g/kg IV over 20 minutes• Hypertonic saline 3-5 ml/kg over 10 minutes
• Effect• Mannitol max effect in 20 min last 2-5 hrs repeat q6-8• Hypertonic saline max effect in minutes, last 1 hour

Mannitol/hypertonic saline
• Do not give if dehydrated/volume depleted
• Monitor electrolytes
• Monitor weight/hydration
• No hypertonic saline if hypernatremic
Maintain Oxygenation
• Evaluate mucous membrane and tongue color, respiratory rate, pattern and thoracic auscultation
Arterial Blood Gas: PaO2 > 90 mmHg Pulse Oximetry: Maintain SpO2 > 95%
• Provide supplemental oxygen Flow-by or mask oxygenation or tent O2 cage does not allow frequent patient assessment Nasal O2 - avoid sneeze induction which increases ICP Intubation / Ventilation

No Corticosteroids
• Are contra-indicated in both veterinary and human medicine for the treatment of head trauma.
• All studies show either no improvement or a worsening of the outcome
• Commonly associated with iatrogenic hyperglycemia and worse prognosis
• Does not help with cytotoxic edema only vasogenic edema• Promote anaerobic metabolism – increase lactate• Increase glutamate levels and neuronal death.

Hyperglycemia and Head Trauma
• Hyperglycemia > 200 mg/dL has been associated with increased mortality in severely brain injured people
• JAVMA, 2001 paper positively correlated degree of hyperglycemia with severity of brain injury
Paper failed to correspond to overall patient prognosis but parallels human papers which correlated higher BG with lower GCS score
• Current guideline: Avoid iatrogenic elevation of blood glucose

Analgesia
• Ideal Analgesic Agent that provides pain relief without inducing respiratory
depression or hypotension
• Options: Opioids – fentanyl Benzodiazepines (reduce anxiety, muscle relaxation) Alpha-2 agonists NSAIDS Gabapentin

Fluid Resuscitation• Goal is to restore normovolemia and normotension
• Fluid Choices: Crystalloids - 90 ml/kg/hr Colloids e.g. hetastarch - 10-20 mL/kg to effect Hypertonic saline - 4-5 mL/kg over 3-5 minutes Blood products if indicated
• No one fluid proven to be better than another, important point is to give to effect, don’t want to create hypertension!
• Ideal MAP = 70 - 90 mmHg, remember, CPP = MAP – ICP! (Minimum CPP 70 mmHg)

Monitoring
• Serial neurological exams necessary as the patient will change, better or worse every 1-2h depending on patient
• Continuous BP, ECG and O2 monitoring recommended
• Serial ABG indicated if patient having difficulty breathing appropriately to determine if ventilation is needed
• Monitor electrolytes, PCV/TS and weight twice daily
Supportive Care
• Circulatory support• Oxygenation• Analgesia• Padded bedding• Rotate patients• Elevation of the head 15-30° above the heart• Lubricated eyes to prevent ulceration• Nutrition• Anticonvulsants if indicated• Avoid jugular compression

BAER test
• Not just an auditory test• Can be a useful assessment of brainstem
function

BAER Tracings
Brainstem damage
Normal

Electroencephalogram

Sequella
• Behavior changes
• Post traumatic epilepsy (weeks to years)
• Persistent deficits
• Ventricular anomalies
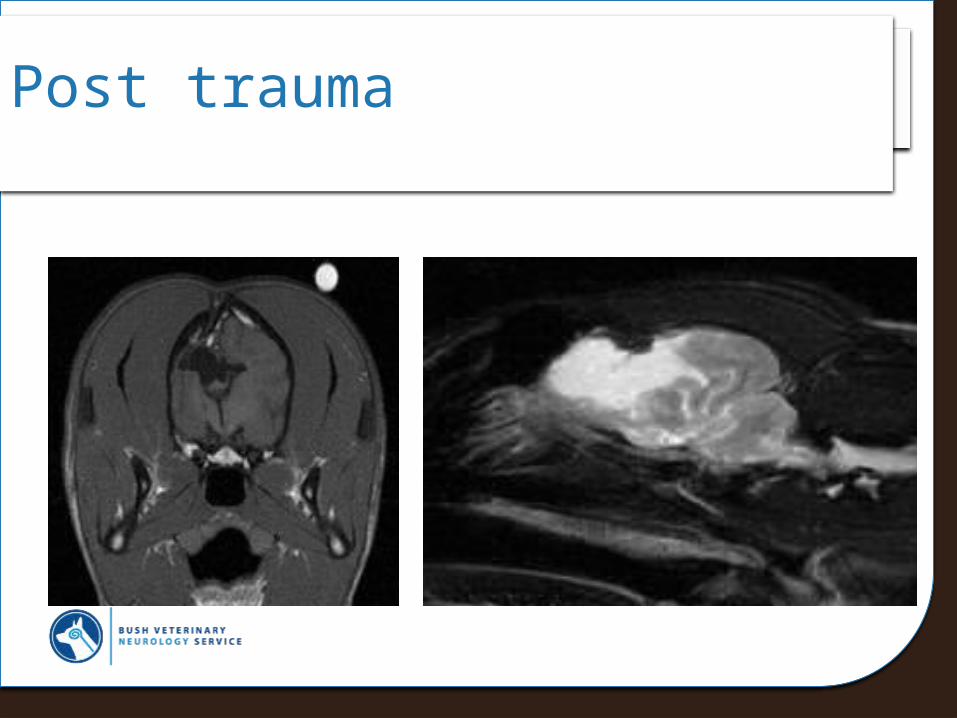
Post trauma

Conclusions
• With time and good supportive care, many head trauma patients can do quite well
• Most important aspect in management is maintaining good MAP and oxygenation

References• Dewey, CW. Emergency Management of the Head Trauma Patient. Veterinary Clinics
of North America: Common Neurological Problems. 2000: 207-25.• Syring RS. Hyperglycemia in dogs and cats with head trauma: 122 cases (1997-1999).
JAVMA. 2001; 218(7): 1124-29.• Syring RS. Assessment and treatment of CNS abnormalities in the emergency patient.
Vet Clin Small Anim. 2005; 35: 343-358.• Platt SR. The Prognostic Value of the Modified Glasgow Coma Scale in Head Trauma
Dogs. JVIM. 2001; 15: 581-84.• Armitage-Chan EA. Anesthetic management of the head trauma patient. JVECC.
2007; 17(1):5-14.• Kalita J. Current Status of osmotherapy in intracerebral hemorrhage. Neurology India.
2003; 51(1): 104-9.• Oliver and Lorenz. Handbook of Veterinary Neuroanatomy.• DeLahunta A. Veterinary Neuroanatomy and clinical neurology. Saunders Elsevier.
2009.
Recommended