Malignant Vascular Endothelial Tumor with Distal Embolization
A New Entity
R. K. WINKELMANN, M.D., Ph.D.
JONATHAN A. VAN HEERDEN,, IM.B., Ch.B. (Cape Town), F.R.C.S. (C)*
PHILIP E. BERNATZ, M.D.
Rochester, Minnesota
From the ‘Mayo Clinic and Mayo Founda- tion, Department of Dermatology and Anatomy, and of Surgery, and from the M.ayo Graduate School of Medicine, Uni- versity of Minnesota, Rochester, Minne- sota. Requests for reprints should be ad- dressed to Dr. R. K. Winkelmann, Mayo Clinic, Rochester, Minnesota 55901. Man- uscript received October 26, 1970.
* Present address: Winchester Surgical Clinic, P.O. Box 854, Winchester, Virginia 22601.
An unusual cause of major arterial obstruction-a vascular endothelial tumor causing aorto-iliac stenosis and distal vascu- lar insufficiency by presumed embolization-is described. In the case reported, there are three distinctive features which imply that this rare syndrome should be recognized as a pattern of vascular disease. (1) There was focal proliferation of cells, similar to neoplastic reticular cells, associated with the endo- thelium of a large vessel. (2) Multiple embolization occurred to peripheral arteries, resulting in gangrene and cutaneous in- flammation. (3) The lesions were recognized in the two levels of the vascular system by use of angiographic technics and skin biopsy.
The usual causes of obstructive disease at the aortic bifurca- tion are advanced atherosclerosis, with or without superimposed thrombosis, and “saddle embolus,” which is usually of intra- cardiac origin.
Distal embolization to the extremities is not uncommon. Its basis is usually atherosclerotic vascular disease, cholesterol emboli, mural thrombi and rarely, fragmentation of intracardiac tumors. Intravascular foreign bodies (for example, bullets) have also, on occasion, embolized distally after entering a large central vessel.
We recently saw a patient who had a massive reticular or endothelial cell proliferation of the abdominal aorta from which multiple emboli to the extremities induced gangrene; we be- lieve that this is a distinct clinical entity related to other intra- vascular reticuloendotheliomas. Among the rare cases of pri- mary aortic tumor are two similar to ours: Sladden’s Case 1 [l] and the case of Staemmler [2]. We believe this syndrome is distinctive and deserves clinical recognition.
692 The American Journal of Medicine

MALIGNANT VASCULAR ENDOTHELIAL TUMOR - WINKEL MANN IET AL.
CASE REPORT
A fifty-six year old whtte man was seen at the Mayo
Clinic in June 1969, having been referred with the diagnosis of Kaposi’s sarcoma of the lower limbs. For a year prior ?o his admission the patient had noticed painful purple spots on both legs. After a cutaneous biopsy performed six months before admission, a diag- nosis of Kaposi’s sarcoma was made and both lower limbs were subjected to irradiation (1,125 rads (R) to the left leg and 375 R to the right leg), with some fad. ing of the lesions. Four weeks prior to admission the patient experienced severe pain in his feet and toes; the pain grew worse with exercise but was present at all times.
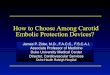
Figure 1. A, multiple linear inflammatory and infarcted
lesions OR the feet at initial examination. B, healing of
lesions after bed rest, bypass surgery and cortisone ther-
apy.
Upon admission, abnormal physical findlngs were confined to the lower extremities. Fran: the middle of the thighs distally, a livedo reticular:s pattern and scattered erythematous macular lesio.ls (about 0.5 cm in diameter) were present. There were severe ischemic lesions on the toes of both feet iFigure IA), and peripheral pulses were decreased (Tab:{? I).
A translumbar aortogram revealed a high degree of aorto-iliac obstruction. The aorta above ti:!s obstruc- tion was smooth, as were the distal iliac and fernoral arteries. A small popliteal aneurysm was present on the left, and there was occlusion (possibly embolic) of the left posterior tibia1 artery (Figure 2).
Biopsy specimens of the skin from the left foot
TABLE I Peripheral Pulses in Patient With Vascular Endothelial Tumor and Distal Embolization
Grade*
Pulse Right Side Left Side
Aorta 4 Femoral 1 3
Popliteal 0 4
Dorsalis pedis 0 0
Posterior tibia1 0 0
* Scale of 0 to 4, 4 being normal.
Figure 2. Aortogram shows marked aorto-iliac obstruc-
tion.
Volume 51, November 1971 693

MALIGNANT VASCULAR ENDOTHELIAL TUMOR - WINKELMANN ET AL.
showed a mass obstructing the muscular vessels of the deep dermis and the connections to the subpapil- lary vessels. The proximal parts of the vessels were filled with large reticular cells that had little cytoplasm and homogeneous nuclei (Figure 3A). The distal parts of the vessels were filled with red blood cells and fibrin clots (Figure 38).
Exploratory surgery was undertaken on June 27, 1969, at which time the diseased aorto-iliac segment was bypassed with a bifurcated, knitted, Dacron graft. The distal aorta and iliac arteries were filled with malig- nant-appearing tissue that seemed more embolic than aortic in origin. Histologically, this tissue was a malig- nant, grade 4 neoplasm of reticulohistiocytic type (Figure 3C). The cells were identical with thDSe ob- served in the lumen of the skin vessels (Figure 3D).
The patient’s postoperative course was essentially uneventful, with continued ischemia of the toes of the
left foot. Angiography undertaken in search of intra- cardiac neoplasia revealed no abnormality. The pa- tient was discharged in the care of his home physician; no specific treatment was prescribed.
On August 11, 1969, prednisone therapy, 5 mg four times daily, was instituted. After one month of therapy, the patient’s condition had improved dra- matically. The mottled rubor had largely disappeared, and although some toenails on the left foot were lost, the pain was gone and the ischemic lesions were sub- stantially healed. The patient continued on this regi- men and by the end of December 1969, he was free of symptoms and had returned full time to his previous occupation. The condition of his feet at this time was much improved (Figure 1B).
In February 1970, eight months after the operation, the patient had an acute relapse and died. Autopsy revealed an extensive intravascular angiosarcoma that
694
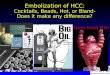
Figure 3. A, specimen of muscular ves- sel from deep dermis obtained by punch biopsy of skin shows syncytium of large reticular cells filling the lumen. Hematoxylin and eosin stain, original magnification x 500. 6, specimen of cutaneous vessel distal to that shown in Figure 2 contains a fibrin and red blood cell thrombus. Hematoxylin and eosin stain, original magnification X 150. C, specimen of tumor mass is composed of layers of fibrin, red blood cells with areas of surrounding necrosis and large reticular cells. Hematoxylin and eosin stain, original magnification x 100. D, close examination of syncyt- ium ‘of cells reveals pale cytoplas’m and homogeneous nuclei with prominent nu- cleoli, suggestive of reticulum cell neo- plasia. Hematoxylin and eosin stain, original magnification x 285.
The American Journal of Medicine

MALIGNANT VASCULAR ENDOTHELIAL TUMOR - WINKELMANN ET AL.
completely occluded the distal portion of the aorta and the right hypogastric artery. In addition, metas- tasrs had occurred to the vessels of both the terminal
part of the ileum (Figure 4A and 4B) and the rectum, causing mucosal ulceration. A skin nodule in the left
inguinal region showed extensive intradermal neo- plastic involvement (Figure 4C and 4D).
COMMENTS
Three distinctive features of this case imply that this rare syndrome should be a recognized pat- tern of vascular disease: (1) There was focal pro- liferation of cells, similar to neoplastic reticular cells, associated with the endothelium of a large vessel. (2) Multiple emboli occurred to peripheral arteries, resulting in gangrene and cutaneous in-
flammation. (3) The lesions were recognrzed in the two levels of the vascular system by ist: of angio- graphic technics and skin biopsy.
Abulafia and associates [3] desc!-rhed a rnaie patient in whom embolism to both upper and lower extremities developed in two abrupt episodes of inflammation and gangrene. No an;:iographic studies were performed, but because of the loca- tion of the emboli, either there were multiple tu- mors in the aorta or there was involvement of the
ascending aorta or the arch of the aorta. Biopsy
specimens of the skin of infarcted areas of both
arms and legs revealed masses of intravascular
reticular cells that produced complete occlusion
of the vessels, identical with that seen in the biopsy specimens from the foot of our patient.
Figure 4. A, specimen shows infiltra- tion of intestinal wall with angiosar- coma. Hematoxylin and eosin stain, original magnification >< 30. B, speci- men shows angiosarcoma with mixtures of large neomorphic cells and poorly formed vascular spaces, fibrosis and inflammation. Hematoxylin and eosin stain, original magnification x 170. C, specimen shows angiosarcoma meta- static to inguinal region. Hematoxylin and eosin stain, original magnification X 30. D, specimen shows ill-defined vascular spaces with large hyperchro- matic cells. Hematoxylin and eosin stain, original magnification x 130.
Volume 51, November 1971 695

MALIGNANT VASCULAR ENDOTHELIAL TUMOR - WINKELMANN ET AL.
TABLE II Types of Primary Tumors of the Aortic lntima Recorded in the Literature
Type Reference Year
Benign (fibromyxoma) Karhoff [5] 1952
Kattus et al. 16) 1960
Malignant
Spindle cell Zeitlhofer et al. [7] 1963
Smeloff et al. [8] 1965
Reticuloendothelial cell Staemmler [2] 1955
Sladden [1] 1964
Abulafia et al. [3] 1969
Winkelmann et al. Unpublished
data
This case was presented as angioendotheliosis proliferans systemisata.
A case that we believe parallels ours closely was reported by Lund [4] who, however, presented it as “metastatic intravascular carcinoma of the skin with secondary necrosis, hemorrhage, and vesiculati,on.” The tumor in his patient, a seventy- three year old man, appeared to be entirely intra- vascular, and the widespread small-vessel tumor emboli seemed identical with those in our patient.
Primary intimal tumors of the aorta are rare and have been reported as both benign and ma- lignant (spindle or endothelial cell) (Table II). In addition to the case of Abulafia et al. [3] two others recorded in the literature are similar to ours. In one, reported by Karhoff [5], there was an ob- structing intralumi~nal tumor mass of endothelial cells with emboli in the celiac artery and its branches, and in the other, Case 1 of Sladden [l], biopsy of the skin demonstrated cutaneous vessels pafcked with embolic malignant cells. The case re- ported by Staemmler [2] and Case 2 of Sladden [l] can be accepted also as involving malignant endo- thelial aot-bc tu’mor without embolus formation. Zeitlhofer and associates [7] described a fibro- myxosarcoma of the aortic intima composed of spindle cells and reticulin, with tumor emboli to the femoral and carotid vessels. The striking case of Kattus et al. [6] emphasized that endothelial aortic tumors may be benign fibromyxomas with foci of cartilage and bone. The symptoms of the benign tumor art! from obstruction of local vessels
only, and in the case of Kattus et al. [6] the tumor was successfully removed at surgery. Tumors in the pulmonary artery and atrial myxoma can present a similar range of endothelial, reticular or spindle cell masses, with or without a reticulin and myxoid stroma and with or without emboli to distant ves- sels.
Systemic proliferating angioendotheliosis was coined as a descriptive term by Tappeiner and Pfleger [9,10] to describe the syndrome in a woman who had rapidly proliferating erythematous plaques of the trunk. Cutaneous biopsy demon- strated proliferation of many open vascular chan- nels in the skin filled with mononuclear cells, which at times appeared related to the endo- thelium. The lesions involuted with cortisone therapy, and Tappeiner and Pfleger [lo] later re- ported that the patient remained in good health. Haber [ll], Braverman and Lerner [12], Midana and Ormea [13] and Maibach [14] reported similar cases. In all instances, many new and dilated vascular channels were packed with large cells. No manifestation of embolism was reccrded. Braverman and Lerner [12] indicated that in their patient, whose condition deteriorated rapidly and who died, invasion of other tissues by the reticular (endothelial or mononuclear) cells occurred and that visceral lesions were observed. They believed that this was a multicentric, potentially lethal, angioendotheliosis.
Our case resembles these principally because the lesions occurred in a similar intravascular location. In our case no vascular dilatation or proliferation was noted: the individual cells were larger and appeared similar to malignant reticular cells, compared to the smaller mononuclear cells observed in Tappeiner and Pfleger’s case. The pattern of tumor mass formation with distal reticu- lar cell embolization is unique. Tappeiner and Pfleger, on reviewing this case with us in 1969, stated that it did not resemble theirs either clini- cally o,r microscopically.
ACKNOWLEDGMENT
Dr. J. R. Marnocha provided follow-up data on this patient.
REFERENCES
1. Sladden RA: Neoplasia of aottic intima. J Clin 3. Abulafia J, Cigorraga J, Saliva J, Molfino JC: Angio- Path 17: 602, 1964. endotheliomatosis proliferante sistemica. Rev
2. Staemmler M: Die Kreislauforgane, Lehrbuch der Derm lberto Lat-Am& 1: 23, 1969. Speziellen Pathologischen Anatomie. vol 1 (Kauf- 4. Lund HZ: Tumors of the skin. Atlas of Tumor Path- mann E, ed), Berlin, Springer-Veriag, l&%5, p 377.
ology, Fast 2, Washington, DC., Armed Forces Institute of Pathology, 1957, p 272.
696 The American Journal of Medicine

MALIGNANT VASCULAR ENDOTHELIAL TUMOR - WINKELMANN ET AL.
5. Karhoff B: Primartumor der Aorta (abstract). Zbl Allg Path 89: 46, 1952.
6. Kattus AA, Jr, Longmire WP, Cannon JA, Webb R, Johnston C: Primary intraluminal tumor of the aorta producing malignant hypertension: success- ful surgical removal. New Eng J Med 262: 694, 19860.
7. Zeitlhofer J, Holzner JH, Krepler P: Primlres Fibro- myxosarkom der Aorta. Krebsarzt 18: 258, 1963.
8. Smeloff EA, Reece JM, Master JA: Primary intra- luminal malignant tumor of the aorta. Amer J Cardiol ‘15: 107, 1965.
9. Pfleger L, Tappeiner J: Zur Kenntnis der systemi- sierten Endotheliomatose der cutanen Blutge- f&se (Reticuloendotheliose?). Hautarzt 10: 359, 1959.
10. Tappeiner J, Pfleger L: Angioendotheliomatosis pro- liferans systemisata: ein klinisch und pathohisto- logisch neues Krankheitsbild. Hautarzt 14: 67, 1963.
11. Haber H: Cited by Tappeiner J, and Pfleger L [lo]. 12. Braverman IM, Lerner AB: Diffuse malignant pro-
liferation of vascular endothelium: a possible new clinical and pathological entity. Arch Derm (Chicago) 84: 22, 1961.
13. Midana A, Ormea F: A propos d’un cas d’ “angio- endotheliomatosis proliferans systematisata” (de Tappeiner et Pfleger). Ann Derm Syph (Paris) 92: 129, 1965.
14. Maibach H: Angioendotheliosis proliferans. Pre- sented at the meeting of the Pacific Dermatologi- cal Society, San Francisco, 19867.
Volume 51, November 1971 697
Recommended