
SM
Making Sense of Managed CareRegulation in CaliforniaNovember 2001
Making Sense ofManaged Care
Regulationin California
November 2001
Prepared for the California HealthCare Foundation
byDebra L. Roth
Deborah Reidy Kelch

476 Ninth Street Oakland, California 94607 Tel: (510) 238-1040 Fax:(510) 238-1388 www.chcf.org
Printed on recycled paper.
Acknowledgments
The authors thank the many individuals who participated in interviews and provided background for thisreport. In addition, the staffs at the Department of Managed Health Care and the Department of Insuranceprovided helpful comments and suggestions. Several people, including individuals from both departments,reviewed this report in draft form. Their feedback was valuable in the editing process. Maureen Sullivan pro-vided planning and research assistance for this project.
About the Authors
Debra L. Roth is an attorney and health care policy consultant with Ruderman & Roth in Sacramento. Herwork includes policy research and advocacy on a range of health care issues, including funding, managed care,and covering the uninsured. She has ten years of experience crafting health care legislation, including eightyears as a policy consultant to the California Legislature. During the 1997-98 session, Ms. Roth served asChief Consultant to the Assembly Health Committee.
Deborah Reidy Kelch, M.P.P.A., is an independent health researcher and president of Kelch AssociatesConsulting. Since 1995, Kelch Associates has published numerous health policy reports and articles, and pro-vides research, consulting, and strategic planning services to nonprofit organizations. Ms. Kelch served as poli-cy and fiscal consultant to the California Legislature for nearly ten years and assisted the Assembly HealthCommittee as policy consultant during staff transition periods in 1997 and 2001.
Copyright © 2001 California HealthCare Foundation
ISBN 1-929008-78-3
Additional copies of this and other publications can be obtained by calling the California HealthCareFoundation’s publications line at 1-888-430-2423 or visiting us online (www.chcf.org).
The California HealthCare Foundation (CHCF) is an independent philanthropy committed to improvingCalifornia’s health care delivery and financing systems. Our mission is to expand access to affordable, qualityhealth care for underserved individuals and communities and to promote fundamental improvements in thehealth status of the people of California.

C O N T E N T S
S e c t i o n 1 5Introduction
S e c t i o n 2 6History of the Knox-Keene Act
S e c t i o n 3 1 2Uncovering the Differences in Regulatory Frameworks
S e c t i o n 4 2 0Understanding the Products in the Health Coverage Marketplace
S e c t i o n 5 2 5Conclusion
Appendices 2 7
Notes 3 9

In California, regulation and oversight of healthinsurance is split between two state departments.The new Department of Managed Health Care(DMHC) primarily regulates health maintenanceorganizations (HMOs), while the CaliforniaDepartment of Insurance (CDI) has jurisdictionover traditional health insurance.
The 1999 legislation establishing the new DMHC(AB 78) transferred regulatory responsibility forHMOs from the Department of Corporations(DOC) to DMHC.1 AB 78 also requires DMHCto report to the Legislature by December 31, 2001on the feasibility of transferring regulatory jurisdic-tion of CDI-regulated health insurers to DMHC.
The two regulatory models, and their deficienciesand strengths, are the result of history, changingpolitical judgments and circumstances, andsweeping marketplace trends over a half-century.While the differences are rooted in distinct statu-tory frameworks and generally apply to discrete
product types, there have been many twists andturns along the way. Today, it can be difficult tounderstand why one regulator rather than anotherhas jurisdiction over a particular product orcompany.
This report considers the political history, currentstatutory and regulatory requirements, and thepredominant types of health insurance productsavailable in today’s market. The goal here is tocontribute to an informed discussion and debate aspolicymakers and stakeholders evaluate the optionswithin the context of the pending AB 78 report.
Research for this report included a review oflegislative history and relevant statutes, review ofmaterials provided by DMHC and CDI, review of other relevant research and reports, and keyinformant interviews with individuals who areparticularly knowledgeable regarding the evolutionand current status of health insurance regulation inCalifornia.
M a k i n g S e n s e o f M a n a g e d C a r e R e g u l a t i o n i n C a l i f o r n i a 5
Introduction 1
The Knox-Keene Health Care Service Plan Act of 1975, the current statutory framework underwhich HMOs and most managed care plansoperate in California, is very directly the result of the history and the times during which it hasevolved. This section provides a brief overview of that history and the evolution of prepaid healthcare and health insurance in California. A detailedchronology appears in Appendix A.
The story of health insurance in California is thestory of two systems developing in parallel: indem-nity health insurance, based on fee-for-serviceprovider payments and broad provider networks,alongside prepaid health plans, or HMOs, providingspecific services for a fixed monthly fee throughmore tightly organized and restrictive networks.2
Until the mid-1970s, Blue Cross, Blue Shield, andcommercial indemnity business, claimed the lion’sshare of the California market.3 Over time, costcontainment concerns yielded much of the marketto the HMOs with their relatively low-cost struc-tures and tighter management of service delivery.
Early Prepaid Health Care
One of the very first prepaid health plans wasestablished in 1929 when the Ross-Loos Clinic, a group practice of physicians, contracted toprovide care for workers in the Los Angeles waterdepartment.4
At about the same time, the Kaiser PermanenteProgram was emerging out of an effort in theMojave Desert to bring medical care to thousandsof workers laboring on the construction of the Los
Angeles Aqueduct. The physician who establishedthe on-site clinic approached Kaiser Industriesproposing to accept a prepaid fixed amount percovered worker to provide medical care for bothon-the-job and non-job related injuries. Theresulting Kaiser model was expanded to otherprojects in California and Washington and wasultimately made available to the public in 1945.
Blue Cross and Blue Shield
In the late 1930s, organized medicine and hospitalassociations around the country helped to establishBlue Cross (hospital coverage) and Blue Shield(coverage for physician services) plans. These plansaimed to shore up revenues dependent on theuncertainties of patient payments and, someobservers report, to block more radical changes in medical care delivery such as government healthinsurance.5
Historians dispute the first place in the countrywhere a Blue Cross plan developed, but many put the origins in Dallas, Texas. The first statutoryauthorization for a California Blue Cross plancame in 1937 legislation creating the new desig-nation of “nonprofit hospital service plan” subjectto regulation by the Insurance Commissioner. As a nonprofit hospital service plan, California BlueCross was exempt from paying the gross premiumstax applicable to other insurers.6
In 1939, the California Medical Association(CMA) founded the California Physicians Service(CPS), the nation’s first statewide, medical-society–controlled, prepaid plan, which would later becalled Blue Shield of California.
6 C a l i f o r n i a H e a l t h C a r e F o u n d a t i o n
2 History of the Knox-Keene Act

In the early 1940s, California’s Insurance Commis-sioner challenged Blue Shield’s contention that itwas not subject to the Insurance Code. In 1946,the California Supreme Court held that BlueShield (and prepaid health plans) are not in thebusiness of insurance and are not subject toregulation by the Insurance Code. The decisionrepresented the first distinction in California lawbetween the “promise to pay” (indemnity healthinsurance) and the “promise to deliver or arrangefor care” (prepaid health care).
According to key informants, Kaiser, Blue Cross,and Blue Shield resisted being regulated by CDI in the same way as commercial insurers for philo-sophical reasons, because they fundamentallybelieved that that they were not in the business of traditional insurance. Several key informantsalso suggested that these companies avoided CDIregulation because they were concerned about thepossibility of having to pay the gross premiums tax.
The Rise of Indemnity Health Insurance
The growth of health insurance (Blue Cross, BlueShield, and commercial indemnity coverage) wasdramatically fueled during World War II whenwages were frozen but benefits were not.7
Organized labor turned its bargaining strategy to benefits instead of wages.
By the early 1950s, health care became a routinebenefit of the workplace, with nearly eight out often workers in the private sector covered throughemployment by some type of voluntary, if limited,health care plan.8 In 1958, nearly two-thirds ofAmericans had coverage for hospital costs, then themost common type of health insurance coverage.
Knox-Mills Act
In 1965, concerned about the lack of any reg-ulatory framework for prepaid health plans inCalifornia, and the increasing potential that therewould be an effort to license them as insurers,Kaiser, Blue Shield, and Ross-Loos actively sup-ported passage of the Knox-Mills registrationprogram. Knox-Mills required “health care serviceplans” to “register” with the Attorney General.Much of the language in Knox-Mills continues in the present day Knox-Keene statute.
Knox-Mills was never considered to be a rigorouslicensing framework by either the plans or otherstakeholders. It was, however, the scandals thatemerged in the early Medi-Cal Prepaid HealthPlan (PHP) program that prompted the Legislatureto consider more substantive regulation of prepaidhealth plans.
Medi-Cal PHP Scandals
In 1971, Governor Ronald Reagan proposedsweeping reforms in the Medi-Cal program, whichincluded a strong emphasis on prepaid health plansas a means of reducing Medi-Cal costs.9
The problems began almost immediately. By mid-1972, the media was reporting misrepresentationsby health plan enrollers, poor quality of care, andfailure to provide promised transportation tomedical offices.10
Many newly organized PHPs were little more than schemes to funnel Medi-Cal dollars through a nonprofit shell to for-profit corporations ownedby the same providers. In some cases, the plansactually sold health plan “shares” to unscrupulousproviders who were hoping to reap huge profits inthe form of provider payments. Plan owners and
M a k i n g S e n s e o f M a n a g e d C a r e R e g u l a t i o n i n C a l i f o r n i a 7
partners siphoned off funds, leaving otherproviders without payment and the PHP shell in financial disarray.
In response to the complaints, the Legislaturepassed the Waxman-Duffy Act, which set regula-tory standards for Medi-Cal PHPs.11 Despite thenew requirements, problems grew.12
State and federal legislative investigations revealedthat California Department of Health Services(DHS) officials had shown favoritism to plansrepresented by former DHS staffers and hadrenewed licenses even where quality of care prob-lems had been documented.13 Investigators alsouncovered financial and/or political ties between a few legislators and plans, where legislators pres-sured DHS to approve new contracts or continueexisting ones despite evidence of potential abuses.A DHS deputy was even accused of impeding aninvestigation by the Los Angeles District Attorney’soffice.14 The written rules had changed, but theunwritten rules had not.
Federal HMO Act
The term “health maintenance organization” wascoined in 1973 with the enactment of the federalHMO Act, an attempt by federal policymakers tostem the “crisis” in health care cost inflation.15
The HMO Act established comprehensive benefits,community rating requirements, administrativeoversight procedures, requirements for financialreserves, annual open enrollments, prohibitions on pre-existing condition limitations, and otherrequirements. The Act recognized several differentmodels of plans and provided federal start-upgrants for nonprofit HMOs to encourage HMOexpansion and development.
Under the HMO Act, plans could choose to applyfor federal qualification and agree to meet therequirements of the Act. In return, HMOs wouldbe eligible for start-up grants and loans and couldmarket the HMO as meeting federal standards and requirements. In addition, the Act originallyrequired employers of more than 25 workers whoalready provided health benefits to offer as onechoice an available federally qualified HMO. Thisrequirement was phased out in the early 1990s. Inthe wake of the HMO Act, the number of HMOsgrew dramatically. By 1987, at least 16 new HMOshad appeared in California.16
The Time Is Right for Knox-Keene
In 1975, Governor Jerry Brown appointed thePrepaid Health Plan Advisory Committee toexamine the Medi-Cal PHP program. Amongother things, the Committee recommended that all Medi-Cal PHPs be required to meet the stan-dards in the federal HMO Act.
At the same time, there was increasing pressure to find a regulatory home for the expandingnonprofit Knox-Mills plans including Blue Shield,Kaiser, and Ross-Loos, which were subject to onlyminimal regulation under Knox-Mills.17
The Knox-Keene Health Care Service Plan Act of 1975 transferred regulatory authority from the Attorney General to the Department ofCorporations and established the basic frameworkfor regulation of health care service plans thatremains today. Knox-Keene was heavily influencedby the failures and inadequacies of the PHP pro-gram and also paralleled many provisions of thefederal HMO Act. The Act set rules for mandatorybasic services, financial stability, availability andaccessibility of providers, review of provider
8 C a l i f o r n i a H e a l t h C a r e F o u n d a t i o n

contracts, administrative organization, and con-sumer disclosure and grievance requirements.
According to key informants, the primary reasonsfor selection of DOC to regulate Knox-Keeneplans were: (1) Department of Health Services was universally viewed as incompetent in the wakeof the PHP scandals, and had a reputation as anunmanageable and unwieldy bureaucracy; (2)Legislative staff and other key stakeholders felt that the Department of Insurance was too friendlyto the interests of insurers; and (3) Stakeholdersbelieved that DOC could bring financial stabilityto the health plan industry, given DOC’s expertisein financial and investment regulation, while thedepartment could contract for or hire the requiredhealth care expertise.
The Act required all Knox-Mills plans to seekKnox-Keene licensure and, according to keyinformants, more than 100 plans applied for andreceived the new license.18 In addition, the new law required Blue Shield to become a Knox-Keeneplan but gave it and several specialized plans(dental and mental health) three years to reduce(but not eliminate) the portion of their businessthat “substantially indemnified subscribers.”19 BlueShield was essentially being told to look more likea prepaid health plan and less like an indemnitycarrier,20 although the company retained the abilityto offer products paying for services delivered bysome providers not under contract.21
Rising HMO Enrollment and the Development of PPOs
In 1982, faced with rising Medi-Cal costs, theLegislature enacted the selective hospital contract-ing program in Medi-Cal. Private insurers arguedthat hospitals would shift costs to the private sector
when their Medi-Cal revenues declined, promptingthe Legislature to repeal the Freedom of Choiceprovisions in the Insurance Code and authorizeinsurers to negotiate and enter into contracts withproviders at “alternative rates of payment.”22 Thestatute provides no further definition or detail onwhat that means. The Act also permitted carriers to limit claims payment to providers charging thealternative rates.
The resulting preferred provider organization(PPO) model of indemnity insurance—whereindividuals have reduced out-of-pocket costs ifthey use providers on the insurer’s preferred list—meant that indemnity carriers could move to bemore price competitive with Knox-Keene licensedHMOs. PPOs implemented utilization review andother cost containment strategies in an effort tocompete with the lower priced HMO plans. By1985, there were 60 PPO plans with nearly 4million covered lives in California.23
California’s health care market became intenselycompetitive. By 1990, there were more than 35HMOs in California with nearly 10 millionenrollees,24 all but six of which had been formedsince passage of the 1973 HMO Act.
HMOs Become Increasingly For-profit
In 1979, the federal HMO Act was amended topermit conversion of nonprofit plans to for-profitstatus. While Knox-Keene permitted both non-profit and for-profit plans since its inception, mostof the HMOs that were developing around thecountry, including in California, were nonprofit.This was primarily because of the availability offederal grants and loans for nonprofit HMOsunder the federal HMO Act. In the early 1980s,
M a k i n g S e n s e o f M a n a g e d C a r e R e g u l a t i o n i n C a l i f o r n i a 9

federal grants and loans were discontinued,prompting many HMOs to pursue for-profitconversions in the search for capital. As a result, awave of conversions of California HMOs occurredthrough the 1980s and into the 1990s.
Blue Cross Moves to Knox-Keene
Blue Cross of California (BCC) continued tooperate as a nonprofit hospital service plan underthe Insurance Code throughout the 1970s and1980s.25 In the early 1990s, a complex combina-tion of political and economic events promptedBCC to seek Knox-Keene licensure. One issue,according to key informants, was the concernamong insurers that BCC’s poor financial condi-tion at the time might result in BCC insolvencyand become a drain on the new health insuranceguarantee fund at CDI. This concern led to therequirement in the legislation establishing theHealth Insurance Guarantee Fund that BCC apply for Knox-Keene licensure by 1991.26
In 1993, BCC obtained multiple Knox-Keenelicenses for health, pharmacy, and dental business.BCC also submitted an initial proposal for“restructuring” of assets that included BCCownership of a large for-profit subsidiary,Wellpoint Health Networks, which in turn owned three nonprofit Knox-Keene licenses.
The ultimate restructuring of BCC was legally and technically complex, controversial, and heavilydebated in legal, legislative, and public forums.After a prolonged legislative and regulatorystruggle, BCC reached agreement with policy-makers and DOC (as its regulator) to dedicatemajor corporate assets to charitable purposes andto maintain a single license as a for-profit healthcare service plan.
BCC was granted specific statutory authorityunder Knox-Keene, similar to the originalauthority provided for Blue Shield, allowing BCC to continue offering PPO products.27
The New Department of Managed Health Care
As providers, consumers, and consumer advocateswitnessed the dramatic changes in health caredelivery precipitated by the growth in managedcare, they increasingly sought legislative andregulatory changes in how HMOs operate and are regulated. Throughout the 1990s, Knox-Keene(and to a large extent the Insurance Code) wasamended to include a series of additional benefitand provider mandates, new provider contractingand claims payment requirements, and changes tocoverage and contract requirements.
In 1997, the statutorily mandated Managed HealthCare Improvement Task Force put forward a seriesof reform recommendations. These included theneed for a new agency to regulate Knox-Keeneplans, and phased-in regulation of other entities,including other health insurance carriers andorganized medical groups.
In 1999, the Legislature passed a series of managedcare reforms, including AB 78, which created thenew Department of Managed (Health) Care. Inaddition, 20 other bills, referred to by consumeradvocates as the “Patient Bill of Rights,” wereenacted in 1999:
■ Guaranteed coverage for second opinions;
■ Time limits on utilization review and mandateddisclosure of the criteria health plans use indenying coverage;
10 C a l i f o r n i a H e a l t h C a r e F o u n d a t i o n

■ Independent external medical review to resolvedisputes related to denials, delays, or modifica-tions of coverage;
■ Improvements in the external review system forcoverage of experimental treatments;
■ Consumer right to sue an HMO for damagesrelated to denials or delays in care;
■ Standards to assure the solvency of medicalgroups under contract with health plans; and
■ Specific mandated benefits, such as mentalhealth parity, contraception, hospice, cancerscreening, and coverage for diabetes supplies.
In July 2000, the new Department of ManagedHealth Care (DMHC) opened its doors. DMHCis currently divided into teams: the HMO Help
Center, Enforcement, Legal Services, Health PlanOversight, Administrative Efficiency, Technologyand Innovation, and Staff Leadership.28
Three boards advise DMHC: the AdvisoryCommittee on Managed Care, the ClinicalAdvisory Panel, and the Financial SolvencyStandards Board. The meetings of these boards and their subcommittees are open to the public.
The Advisory Committee on Managed Care iscurrently considering the regulation of health plansand indemnity insurers in response to the AB 78requirement that DMHC study the feasibility oftransferring the regulation of health insurance from CDI to DMHC. The report is due to theLegislature in December 2001.
M a k i n g S e n s e o f M a n a g e d C a r e R e g u l a t i o n i n C a l i f o r n i a 11

Although both departments regulate carriersproviding health coverage, DMHC and CDIapproach regulation very differently, primarilybecause the various carriers they regulate, and the statutory authority under which they regulate,are very different. At the heart of the distinctionbetween “disability insurers”29 and “health careservice plans”30 is the “promise to pay” versus the“promise to deliver care.”
Under Knox-Keene, health care service plans(commonly referred to as HMOs) actually arrangefor and organize the delivery of health care andservices through contracted or owned providersand facilities. Disability insurers protect against(indemnify) the expenses or charges (losses)associated with illness or injury. A disabilityinsurance policy, or indemnity policy, providescoverage for defined benefits related to the insuredevent—accident, illness, or other covered healthcondition or situation. This is the traditionalconcept of indemnity insurance, and appliesgenerally to all forms of insurance, including ahome destroyed by fire or an automobile destroyedin a collision.
Another inherent difference between a health careservice plan and a disability insurer is the nature of the protection afforded consumers under eachcoverage type. Knox-Keene HMOs assume the riskand pay for all medically necessary covered servicesfor one monthly, prepaid payment; insurers paymedical expenses or a portion of medical expensesaccording to the specific coverage under the con-tract. In effect, under Knox-Keene, consumers arenot financially affected by variations in either costor utilization, outside of specified copayments or
other contract cost-sharing provisions. This isbecause the health plan provides (or contracts for)the services, rather than making payments to covera specific dollar loss (charges), or percentage of theloss, as in indemnity insurance.
Providers may look to their patients with indem-nity coverage to pay costs or charges regardless of whether or how much the insurer indemnifies(reimburses the patient) for the services. However,contracts between Knox-Keene HMOs and pro-viders must specifically prevent the providers fromseeking payment directly from enrollees for coveredservices if the health plan fails to pay.
Marketplace Changes Blur the Distinctions
Over time, the differences between these twomodels of health coverage have been obscured orblurred for many observers and stakeholders. Thereare two primary reasons for this.
First, there have been two significant exceptionsmade in law and regulation in the types of carriersregulated as Knox-Keene plans. Through thehistorical and statutory authorizations describedabove, both Blue Cross and Blue Shield arelicensed as health care service plans, but along with several specialized plans are able to also offerPPO contracts, a type of contract otherwise subjectto CDI licensure and more commonly associatedwith indemnity insurance.31
Second, over the past several decades, theLegislature has authorized both health plans andinsurers to offer new types of policies and contracts
12 C a l i f o r n i a H e a l t h C a r e F o u n d a t i o n
3 Uncovering the Differences in Regulatory Frameworks
that appear more similar than different. Insurershave increasingly offered PPO policies with whatlook like delivery systems, where a published list of “preferred” providers offer their services atdiscounted rates, reducing out-of-pocket costs forconsumers who use the PPO network to obtainhealth care. Health care service plans (HMOs) arenow able to offer point-of-service (POS) contracts,allowing enrollees to receive some services outsideof the network of contracted or employed provid-ers, if they are willing to pay increased out-of-pocket costs for these choices.
Moreover, virtually all health coverage today(whether health plan or disability insurance carrier)has some elements of “managed care” including,for example, prior authorization, coverage limitedto medically necessary care, and utilization review.These hybrid products have in some respectsblurred the distinctions between health plans andinsurers for consumers, policymakers, and otherkey stakeholders.
Key Informant Impressions
Key informants interviewed for this project offeredthe following opinions and observations about thetwo models of health coverage and the respectiveregulation by each department. Appendix E liststhe key informants who were interviewed.
Current System Is Confusing to ConsumersSince the department of jurisdiction for differenthealth insurance products is based in part onhistory and legal technicalities, the differences areinvisible or too complex for consumers to recog-nize. As a result, the dual regulatory system isdifficult for consumers to navigate when they have problems with their health care.
Key informants agreed that DMHC, in existencefor little more than one year, is seen as moreconsumer oriented than the entity that previouslyregulated health plans, the Department ofCorporations. Some key informants also felt that CDI was potentially less consumer friendlybecause CDI’s consumer complaint system isgenerally more limited than DMHC’s system. This is because DMHC has a statutory mandate toreview and resolve complaints related to the qualityof health care services while CDI does not.
Departments Have Different Strengths and WeaknessesEach department regulates in a fundamentallydifferent way. Consequently, key informantsviewed DMHC’s emphasis on insuring quality ofcare as generally more burdensome for health plansin the regulation of adequacy of in-network care,benefit design, consumer complaints, and qualityreview. Virtually all key informants viewed CDI as stricter in the application of financial and claimspayment standards and a more rigorous enforcer offinancial solvency and reserve requirements.
Consumer Recourse Is DifferentThe two types of coverage result in very differentrelationships between consumers and carriers andbetween consumers and providers.
An individual covered by an insurance productindependently selects and deals directly with theprovider, is generally responsible for payment and, if not satisfied, can exercise the option tochange providers. An insured can register com-plaints with CDI, but CDI does not have thestatutory authority to become directly involved in resolving consumer complaints about medicalservices or providers. CDI does enforce laws andregulations related to claims, underwriting, andrating practices. According to CDI, by enforcing
M a k i n g S e n s e o f M a n a g e d C a r e R e g u l a t i o n i n C a l i f o r n i a 13
these requirements, the department is able toensure that consumers are paid for the medicalservices necessary for their treatment.
In contrast, a person covered by an HMO contracthas less flexibility in changing providers, is subjectto greater plan involvement in the delivery ofservices, but can seek assistance from the plan inresolving issues relating to a provider or the qualityof care. Consumers are required to use the healthplan grievance system but can go to DMHC if theplan does not resolve the issue or act in a timelymanner.
Products and Companies Are DifferentCompanies operating health care service plans, as a general rule, have a business focus on healthcoverage. However, for many companies offeringdisability insurance, health is just one smallportion of their overall business, which typicallyalso includes life insurance and may includemultiple other forms of individual and corporateinsurance. Large indemnity insurers with multiplelines of insurance have a different corporate culturethat reflects the business of insurance, not healthcare.
Traditional indemnity health insurance regulatedunder CDI represents a decreasing portion of theoverall health coverage market, with key infor-mants estimating that indemnity represents only 5to 10 percent of the total health coverage market.32
Comparing Statutes and Regulations
This section includes an overview of the statutoryand regulatory differences between disabilityinsurers and health care service plans. Table 1summarizes the differences, which are discussed
more fully below. Appendix B contains a detailedstatutory comparison.
Initial LicensureHealth care service plans apply for and obtain aKnox-Keene license prior to operating in Califor-nia. Disability insurers obtain a certificate ofauthority from the Insurance Commissioner forthe specific line(s) of business they intend to offerprior to conducting insurance business in the state.
In applying for licensure, a health care service plan must submit for review and approval all of the types of plan contracts (policies) it will offer,standard provider contracts and payment methods,proposed advertising and marketing materials,audited financial statements, administrative struc-ture, projections of financial viability, actuarialanalyses, and specific proposed service areas.
The CDI certificate of authority review processinvolves a detailed operational and financial review.The application process includes review of thecompany’s financial stability, available capital andassets, competency and integrity of ownership andmanagement, claims payment procedures, actuarialcertifications, and financial projections. Insurerssubmit their policy forms for review and aresubject to specific “market conduct” (claimshandling) requirements and procedures oftenreferenced as the Fair Claims Practices rules.
While both health care service plans and insurersare required to demonstrate administrative capacityand financial solvency, a health care service planmust also provide a detailed outline of the pro-posed delivery system for in-network care anddemonstrate network adequacy. There is generallylittle or no specific review of the adequacy ofnetworks for insurers, regardless of the type of plan or product they are offering.
14 C a l i f o r n i a H e a l t h C a r e F o u n d a t i o n

M a k i n g S e n s e o f M a n a g e d C a r e R e g u l a t i o n i n C a l i f o r n i a 15
Table 1: Comparing the Functions of CDI and DMHC
Area of Oversight CDI Requirements DMHC Requirements
Primary Focus Ability to pay claims. Ability to deliver care.
Benefits Specific mandated benefits but nominimum benefit package.
Specific mandated benefits plus “basichealth care services.”
Quality No oversight of medical care.
Disclosure and standards for utilizationreview and utilization management.
On-site medical surveys, including on-siteprovider reviews, and mandatory internalquality assurance system.
Disclosure and standards for utilizationreview and utilization management.
ProviderAccessibility
No accessibility standards enforced. Providers must be “readily available andaccessible,” subject to DMHC review.
ProviderPayments
Provider payments limited to fee-for-service and negotiated discount rates.
In addition to fee-for-service and discountrate options, plans may share risk withproviders (e.g., capitation).
ConsumerProtection
Same as those applicable to all lines ofinsurance: consumer disclosure, FairClaims Practices Act (market conduct).Complaints can be filed with CDI.
Independent Medical Review for denials of care.
Consumer disclosure requirements,complaints handled through internal plan grievance system with DMHCintervention if necessary.
Independent Medical Review for denials of care.
FinancialReserves
Reserves based on the greater of: $5million statutory minimum capital or 200 percent of the Risk-Based Capitalstandards developed by the NationalAssociation of Insurance Commissioners.Generally higher than reserverequirements for Knox-Keene plans.
Insurers required to join GuaranteeAssociation. Association will assessmember insurers to pay the claims of an insolvent insurer.
Reserves (tangible net equity) calculatedbased on the greatest of: 2 percent ofpremium revenues; minimum of $1million; or specified percent ofexpenditures.
DMHC can require other plans in an area to assume care of an insolvent plan’senrollees.
Fee and TaxStructures
Licensing fees and other filing fees.
Gross premiums tax (in lieu of othercorporate taxes): 2.35 percent of totalpremiums annually, regardless of profit.
Annual “per enrollee” assessments.
No gross premiums tax. Subject toapplicable corporate taxes.

BenefitsAll health care service plans, including PPOsregulated by DMHC, must offer basic health careservices: physician services, inpatient and outpa-tient hospital services, diagnostic lab and radiology,therapeutic radiology, home health, preventivehealth services, emergency services, and hospicecare. In contrast to Knox-Keene requirements forhealth care service plans, there are no minimum or basic benefits required in the Insurance Code.However, both the Insurance Code and Knox-Keene contain numerous mandatory benefit orcoverage provisions requiring that carriers offer orprovide specific services and/or specific providers.Examples are listed in Appendix C.
Knox-Keene basic health care services can besubject to copayments and deductibles, butDMHC has regulatory authority to review cost-sharing arrangements and other limitations toensure that the contract requirements are “fair,reasonable, and consistent with the objectives ofthe chapter” and are not held to be objectionableby the director.33
By contrast, disability insurers have enormousflexibility to develop alternative benefit packages,with variations on covered services, copaymentsand deductibles, and annual and lifetime maxi-mums. Policies can be written to cover limitedmedical expenses, exclude specific services notmandated in statute, cover primarily catastrophicexpenses, or include significant consumer cost-sharing requirements not subject to regulatoryoversight. In addition, disability insurers are able to develop specialized and supplemental policiessuch as disease-specific coverage, short-term healthinsurance, and coverage for copayments anddeductibles from another policy. These types ofsupplemental policies would not meet Knox-Keenebasic benefit requirements.34
Key informants reported that the flexibility inbenefit design under the Insurance Code is one of the primary reasons that many Knox-Keenelicensed plans also maintain a disability insurancecertificate of authority. Reportedly, the insurancecertificate allows them to respond to purchaser andmarketplace demands for different products, suchas low-cost high-deductible plans, greater choice of out-of-network providers, or lower-cost benefitplans that do not include all of the basic benefitsunder Knox-Keene and are not subject to otherKnox-Keene Act provisions.
For example, instead of offering their point-of-service products35 entirely under their Knox-Keenelicense, some Knox-Keene HMOs offer the equiv-alent of a point-of-service through a combinationof an HMO contract for in-network services and aCDI indemnity “wraparound” for out-of-networkservices.36
Quality Assurance and Quality MonitoringHealth care service plans are required to haveinternal quality assurance and utilization reviewprograms, directed by providers, to document andimprove the quality of care. The regulations requirea written plan, regular meetings of the qualityassurance committee(s), and supervision by a planmedical director. DMHC is required to conducton-site medical surveys of all licensed health plans,including review of patient medical records, at leastevery three years.
Insurers are not subject to comparable qualityassurance requirements. CDI does conduct on-sitereview and regulatory examination of claims,financial records, and rating and underwritingpractices of all licensed insurers.
16 C a l i f o r n i a H e a l t h C a r e F o u n d a t i o n

Utilization Review and Utilization ManagementBoth disability insurers and health care serviceplans are subject to similar statutory requirementsapplicable to their utilization review process.Carriers must have written policies, develop criteriausing health professionals consistent with clinicalprinciples, make decisions within specified time-frames, and disclose the criteria being used. Therequirements apply to approvals, modifications,delays, or denials of services prior to, after, or atthe time of services being rendered.
Health care service plans must designate or employa medical director to set the policies and overseethe decisions, and their programs and policies aresubject to review during the on-site medical survey.Disability insurers must have a medical directoronly if the number of California insureds is 50percent or more of their total national health carebusiness. Violations by either carrier type aresubject to fines and penalties.
Provider AccessibilityHealth care service plans must ensure that servicesare “readily available and accessible to enrollees.”Except for contracts specifically allowing for someout-of-network providers (PPOs, EPOs, and POS),all participating providers must be under contractor employed by the health plan. Regulatory guide-lines include specific physician-enrollee ratios anddistance standards for the location of providers toenrollee residences and workplaces.
As a general rule, disability insurers are not subjectto similar accessibility standards. There are stateinsurance regulations applicable to exclusiveprovider organizations (EPOs)—where payment is limited to providers who have agreed to acceptdiscounted rates—that require consumer disclosureof available providers and contain availability and accessibility standards nearly identical to
Knox-Keene. According to CDI, the regulations donot require that EPOs submit provider contracts oradequacy and accessibility information. Accordingto CDI, the department will inquire into adequacyof provider networks and will “ensure that thepolicy is not inconsistent with standards of goodhealth care.” CDI is not required to and does nottrack the number of EPO policies but concurs withkey informants that there are very few currently inthe marketplace.
Provider PaymentsDisability insurers are limited to paying fee-for-service claims and to negotiating discounted ratesof payment as in a PPO arrangement. Health careservice plans may pay fee-for-service or discountedfee-for-service, and in addition, may executeprovider contracts that pay providers either acapitation payment—a monthly flat rate perenrollee—or some other arrangement where theprovider shares in the risks related to costs andutilization of health services.
While the rates paid to providers contracting with Knox-Keene plans are not subject to DMHCreview and approval, health plans must submit thepayment method. In the case of capitation arrange-ments, plans retain legal responsibility for ensuringthat the provider has the administrative and finan-cial capacity to handle the contract. In addition,the plans must have “a mechanism to detect andcorrect under-service” by providers assumingfinancial risk in treating the plan’s members. In the wake of several highly visible medical groupbankruptcies, DMHC is currently implementingnew provider financial reporting requirements.
Consumer ProtectionHealth care service plans are required to maintainan internal plan grievance system to respond toconsumer complaints. DMHC established the
M a k i n g S e n s e o f M a n a g e d C a r e R e g u l a t i o n i n C a l i f o r n i a 17

“HMO Help Center” (continuing the toll-freeconsumer complaint hotline originally establishedat the Department of Corporations in 1995) andexpanded the hotline hours to 24 hours per day, 7 days per week. After normal business hours, anexternal contractor trained by DMHC responds to hotline calls. The contractor answers basicquestions and is able to send out information,including complaint forms. Help center staff havethe ability to page DMHC staff nurses or consult-ing nurses or physicians, 24 hours per day, forassistance with medical care issues.
There is no similar requirement that insurersmaintain an internal grievance or complaintsystem. CDI also operates a consumer hotline thatpredates the DOC hotline (for all lines of insur-ance, not just health insurance), which is available10 hours per day, 8:00 a.m. to 6:00 p.m. CDI hasvoice mail and email systems allowing consumersto register complaints after hours. CDI staff thenrespond to those complaints during regularbusiness hours.
Both departments are legislatively mandated todevelop an independent medical review (IMR)system where doctors and other professionalsoutside of the health plan or insurer reviewcoverage and medical care decisions made by thecarriers. DMHC contracted with the Center forDispute Resolution to conduct the reviews andCDI agreed to use the same organization forconsistency and clarity across programs.
Financial Reserve RequirementsBoth health care service plans and disabilityinsurers are subjected to financial reportingrequirements, review, and monitoring of theirfinancial capabilities, including on-site reviews, andmust meet specific financial reserve requirements.
Disability insurers are required to maintain reservelevels at the greater of either: (1) a minimum of $5 million or (2) 200 percent of the Risk-BasedCapital standards developed by the NationalAssociation of Insurance Commissioners.Insurance industry representatives report thatreserves under this formula are 50 to 100 percenthigher than the reserves required of Knox-Keenelicensees.
In addition, the Insurance Code requires all lifeand disability insurers to belong to the CaliforniaLife and Health Insurance Guarantee Association.The Guarantee Association is structured so that all insurers share the risk in the event of a carrier’sfinancial insolvency. Assessments on all carriersthen cover the losses (expenses) of people insuredby the insolvent carrier. This system is designed to protect the ability to pay claims.
Under Knox-Keene, health plans are required to maintain financial reserve levels, referred to as tangible net equity (TNE), at the greatest of: (1) a minimum of $1 million; (2) 2 percent ofpremium revenues; or (3) specified percentages of expenditures. In addition, PPO and point-of-service plans are subject to higher TNE require-ments in light of their increased liability fromout-of-network services.
In the event of an insolvent health plan, DMHChas the authority to proportionately assign themembers of the insolvent plan to other Knox-Keene plans in the service area. The neighboringplans are required to assume responsibility fordelivering health care to the assigned members.Under Knox-Keene contracts, providers are notstatutorily protected from the risk of lost paymentsin the event of plan insolvency.
18 C a l i f o r n i a H e a l t h C a r e F o u n d a t i o n

Fee and Tax StructuresHealth care service plans pay an annual assessment,as specified in statute. The amount of the assess-ment is based on the size of the health plan and the specific number of health plan members(enrollees). Health plan assessments support theregulatory and enforcement program at DMHC.By contrast, insurance fees are assessed for eachtype of filing or regulatory request and are not inany way based on the number of people an insurercovers. CDI fees support CDI operations. CDIdoes not track or require insurers to report thenumber of covered lives or insureds.
Knox-Keene plans are subject to all taxes applicableto the particular corporate and tax status of theplan. Insurers pay a gross premiums tax based onthe total dollar amount of premiums sold, regard-less of profit, in lieu of other state or local taxes.
It is difficult to compare and contrast the verydifferent types of assessments and reserve formulasapplicable to each carrier type since they are basedon distinct formulas and requirements. The relativeburden and protection afforded by the reserverequirements, fees, and tax structures betweenhealth care service plans and disability insurers maywarrant further review.
M a k i n g S e n s e o f M a n a g e d C a r e R e g u l a t i o n i n C a l i f o r n i a 19

Much of the confusion about the two differentdepartments and their jurisdictions—and thedriver behind recent interest in possibly combiningor overhauling jurisdictions and regulatory respon-sibilities in some way—results from the overlapand similarities between the products under eachdepartment’s jurisdiction.
Specifically, as indemnity insurers have developednetworks of providers at discounted rates, and ashealth care service plans have developed someproducts where consumers can go out-of-network,it increasingly appears as though both departmentsare regulating the same types of carriers andproducts. One way to begin to organize andanalyze the products in today’s market is to under-stand the prevalence of similar products and theregulatory jurisdiction applicable to these products.
Identifying Products and Regulators
HMOs under Knox-KeeneAs stated earlier, HMOs under Knox-Keeneprovide all services through plan operated orcontracted providers (except for point-of-serviceproducts as discussed below).
There are three models of HMOs: group model,staff model, and independent practice association(IPA) or “network” model plans. In California,Kaiser Permanente is the only group model plan,where one group provides, on an exclusive basis,virtually all of the medical care for plan membersin an area. Staff model plans, where the planemploys the providers, are increasingly rare andprimarily limited to relatively small, nonprofit
community clinic-based or county owned oroperated plans. Most of the HMOs in Californiaare IPA/network model plans, or what the Cali-fornia Association of Health Plans calls “mixedmodel” plans that provide coverage through acombination of large multi-specialty medicalgroups and more loosely organized IPAs—privatephysicians in their own offices who belong to anassociation for contracting purposes.
Unlike insurers, HMOs under Knox-Keene arepermitted to execute provider contracts that shiftsome of the risk to the providers while the healthplan retains legal responsibility to ensure that theproviders have the ability to manage and assumethe risk.
According to the California Association of HealthPlans (CAHP), in 1999 some 73 percent of Knox-Keene plans paid primary care providers by groupor individual capitation, while 19 percent paid
20 C a l i f o r n i a H e a l t h C a r e F o u n d a t i o n
4 Understanding the Products in the Health Coverage Marketplace
Figure 1: PCP Payment ArrangementsAmong Knox-Keene Plans in 1999
Source: California Association of Health Plans 2000 AnnualReport and Profile.
Group orindividualcapitation
73%
Salary3%
Other5%
Fee-for-service or
discountedfee-for-service19%

fee-for-service or discounted fee-for-service, 3 percent salary, and 5 percent other.37 Amongspecialists, 40 percent are paid by capitation and47 percent by fee-for-service. According to keyinformants, in the past two years there has been a gradual erosion of plans paying providers by wayof capitation arrangements.
PPOs and EPOs under Knox-KeeneThe PPO model of health coverage, where thecarrier offers a list of providers who have agreed to accept reduced payment, and the EPO model,where payment is limited to providers on the list,are generally not allowable under or subject to theKnox-Keene Act. However, as discussed, twosignificant exceptions continue to complicateanalysis of the regulatory framework for healthcoverage—Blue Shield and Blue Cross.
According to the California Association of Health Plans, in 2000, approximately 4.6 millionCalifornians, or 20 percent of those enrolled inKnox-Keene plans, were in PPOs, 73 percent inHMOs, and approximately 5 percent in point-of-service plans.38
Both Blue Cross and Blue Shield plans have aspecific statutory or historical exemption from the requirement that all services be delivered by participating providers. Both companies areotherwise subject to the provisions of Knox-Keene,including the requirement to provide all basichealth care services, to establish internal qualitymonitoring systems, to meet availability andaccessibility standards for in-network providers,and to submit plan contracts, advertising, andmarketing materials for prior approval to DMHC.
Historically, DOC, and now DMHC, haveallowed for considerable flexibility in PPOdesign—copayments, deductibles, annual
maximums—so that the Blue Cross and BlueShield PPO products more closely resemble otherPPO products in the marketplace. In addition,out-of-network providers and services, with nodirect affiliation to the plans, are not subject to thesame quality assurance requirements as in-networkproviders. The statutory authorization applicable to the Blue Cross and Blue Shield plans allowsthem to have some portion of their business that“substantially indemnifies subscribers” and bothcompanies also offer limited EPO contracts underthe Knox-Keene license.
Point-of-Service Contracts under Knox-KeeneIn 1992, legislation authorized Knox-Keene healthcare service plans to begin offering plan contractsthat include both an HMO delivery system andthe option for enrollees to choose providers outsideof the plan’s network, for some services. POScontracts are subject to all Knox-Keene standards,except for the providers and services delivered out-of-network. There are statutory limits on thecopayments and deductibles that can be chargedfor out-of-network services, restrictions on theamount of out-of-network care that a health plancan experience, and increased financial reserverequirements. As of 2001, DMHC reports thateight Knox-Keene plans offer point-of-servicecontracts under the POS provisions of Knox-Keene.
Based in part on the statutory constraints applica-ble to Knox-Keene POS contracts, several Knox-Keene plans offer purchasers a POS equivalent thatis regulated under both departments—the previ-ously mentioned HMO contract for in-networkcare, with a disability insurance “wrap-around” forout-of-network care.
M a k i n g S e n s e o f M a n a g e d C a r e R e g u l a t i o n i n C a l i f o r n i a 21

PPOs under the Insurance CodeThe 1982 selective contracting legislation (au-thorizing disability insurers, for the first time, tonegotiate with providers for “alternative rates ofpayment”) was a significant departure for indem-nity health coverage because the Insurance Codehad since 1937 protected the right of an insured to choose any licensed health care provider.
This “alternative payment” language is the basis fordevelopment of what became known as insurancePPOs.39 Key informants in this project consistentlyreported that virtually all of the current indemnitypolicies for full coverage health insurance in Cali-fornia include a PPO network through whichconsumers can access services at reduced cost.
Key informants indicated that many insurers “leaseor rent” PPO networks from corporations that arein the business of organizing the networks, negoti-ating rates, and executing provider contracts. Thesecompanies also make their PPO networks availableto large, self-insured employers. The contractedPPO may also perform other functions such asprior authorization or utilization review foremployers and insurers. The PPO networks and companies themselves are not subject to anylicensing or regulation under California law. PPOnetwork companies are regulated in some otherstates, complicating state-to-state comparisons of how “PPO products” are regulated.
EPOs under the Insurance CodeThe Insurance Code also allows insurers to limitpayment to providers agreeing to alternative rates.Exclusive provider organizations require individualsto receive all services from providers who agree toaccept reduced payments from the insurer.
These products are subject to increased consumerdisclosure regulations monitored through CDI
scrutiny of policy forms. CDI does not track thenumber of EPO policies it approves, but CDIagrees with key informants that there are very fewEPO plans being offered by disability insurers.
Traditional Indemnity Insurance under the Insurance CodeInsurance companies that offer health insuranceunder the Insurance Code may offer an open panelproduct allowing insureds to seek services fromlicensed providers with no network limitation ordiscounted network offering. These products aresubject to statute and regulations applicable todisability insurers generally.
These “traditional” indemnity policies typicallyhave annual deductibles and pay for services whena bill is received. The policies generally coverphysician and hospital services and medical tests.They may cover prescription drugs but are typi-cally limited in coverage of preventive care services.The insurer generally pays a specified percentage of the “usual and customary fees” (often 80percent) while the insured pays the remainingamount, known as “coinsurance.”
Key informants consistently reported that there arevery few “pure” indemnity products remaining intoday’s market. CDI does not track information onthe extent of availability of any product type underits jurisdiction, including traditional indemnitycoverage.
What Is a Health Insurance Product?
Individuals can obtain protection from the costs of health care services through multiple productstrategies, not just traditional health insuranceproducts. The traditional health insurance
22 C a l i f o r n i a H e a l t h C a r e F o u n d a t i o n

products discussed in this report, regulated byDMHC or CDI, constitute a subset of the differ-ent strategies available. Strategies include:
Full coverage health insurance, which generallycovers hospital, medical, and surgical services andmay include coverage for ancillary services. Knox-Keene plans, both HMOs and PPOs, will cover atleast the basic health care services and distinguishproducts primarily by the different levels of patientcost sharing. Among disability insurers, the typesof services covered, including the extent to whichthey cover preventive care, and variation in patientcost-sharing levels, may distinguish products.
Catastrophic or high-deductible health insurance,which covers health care costs above a relatively high fixed-dollar amount and may also includepolicies that cover only high-cost items such asmajor medical or hospitalization. In today’s marketthese policies may be sold in combination with aMedical Savings Account (MSA), a savings accountdedicated for health care expenses and organizedunder federal tax laws establishing MSAs as a tax-deductible option. Both Knox-Keene plans (pri-marily the PPOs) and disability insurers havedeveloped these types of products.
Cash benefit plan, which provides lump sum orperiodic cash payments related to specific eventssuch as hospitalization, accident, defined disability,catastrophic illness, or illness out of the country.These plans do not reimburse for health servicesbut pay cash payments when the insured eventoccurs. The payments can be used to pay for health care or for other expenses. These products
are exclusively offered by disability insurers and are not permissible under Knox-Keene.
Elements of a Health Insurance ProductEach full coverage health insurance product can be viewed as a combination of four key elements:(1) the benefit design—what is covered or insured;(2) the service delivery approach, if any—how andfrom whom the consumer must obtain services toreceive benefits under the contract; (3) the methodof provider payment—how the carrier pays pro-viders; and (4) the specific company or carrier type offering the coverage. Benefit design, whichcontains several elements that are not mutuallyexclusive, is the area of most variability product toproduct. Figure 2 provides an illustration of healthcoverage product components.
What has made the dialogue about health coverageproducts and companies so complicated, and oftenconfusing, is that in the marketplace, products aretypically referred to more by the service deliverytype—HMO, PPO, and POS—than by any otherelement of the product design. And yet there canbe substantial variation among these products and,as the comparison of the two licensing schemesreveals, very different regulatory requirementsdepending on the carrier offering the product.
This section shows that breaking down the com-ponents of any product helps to identify the regu-latory framework and specific requirements thatgovern that product. Appendix D contains anoverview of the different products licensed andregulated in California, which serves to illustratethe complexities inherent in regulation.
M a k i n g S e n s e o f M a n a g e d C a r e R e g u l a t i o n i n C a l i f o r n i a 23

Figure 2: Elements of a Health Insurance Product
These four elements combine to form a health coverage product as sold to purchasers. Consumers may not always befamiliar with or aware of all the elements that make up a health coverage product.
BENEFIT DESIGN
What is covered orinsured by the product
List of services orevents covered
AND
Limits andtimeframes
One visit per year,number of hospitaldays per year, etc.
AND
Copayments,deductibles,co-insurance
SERVICE DELIVERY
How and from whomconsumers need toobtain services
HMO
Closed panel – planowned or contractproviders
OR
PPO
Choose preferred listor any provider
OR
Point-of-Service
Mostly in-network,some out of network
OR
Open panel/TraditionalIndemnity Insurance
Choose any licensedprovider
ABC-XYZ Health Plan Inc.
Subscriber Name: Maria SmithSubscriber ID: 123456789Plan Code: 99Z Copays: $15/$10
PROVIDER PAYMENTMETHOD
How the carrier pays foror reimburses providers
Capitation and risk-pools
Knox-Keene plansonly
OR
Salary
Knox-Keene HMOsonly
OR
Fee-for-service ordiscounted fee-forservice
Knox-Keene HMOs,PPOs, disabilityinsurers, self-insuredplans
BENEFIT PLAN
Covered services andhow much patient paysout-of-pocket
TYPE OF PLAN
Rules and requirementsfor using participatingproviders and/or non-participating providers
PROVIDER INCENTIVES
Applies to primary care,specialists, hospitals,and any other contract-ing provider
CARRIER
Who offers the plan orcoverage
Knox-Keene licensedhealth care serviceplan
OR
Disability insurer
OR
Self-insuredemployer/Trust
APPLICABLE STATUTE AND REGULATIONS
Legal requirements,including consumerprotections
24 C a l i f o r n i a H e a l t h C a r e F o u n d a t i o n
HEALTH COVERAGE PRODUCT AS
SOLD TO PUBLIC

The intent of this report has been to providethe reader with a contextual framework throughwhich to examine the difficult issue of whether theregulation of health coverage in California shouldbe altered or consolidated.
What this report reveals is that public policychoices and shifting political inclinations overmore than a half-century have resulted in two verydifferent statutory and regulatory frameworks. Theexisting differences between the two departments,and their respective regulatory personalities, arefirmly rooted in both history and statute. Thesechoices have also had profound effects on thehealth coverage market in California.
The report also suggests that as long as there are two different departments regulating healthcoverage, and two distinct statutory frameworks,there will be important differences in how carriersare regulated, distinct departmental cultures, anddisparate views of their respective roles and respon-sibilities toward consumers, providers, and carriers.
When properly channeled, and when there is effective collaboration and communicationbetween departments, the differences can serve as learning tools, presenting an opportunity tobuild on success. Many key informants interviewedreported that the information exchange resultingfrom the AB 78 review of the respective depart-ments and frameworks has resulted in many suchdesirable effects. At the same time, it is alsopossible, under dual regulation, for the twodepartments to become competitors vying forrecognition and acknowledgement of the sound-ness of their regulatory performance.
Dual regulation also invites carriers to designproducts to fit within the regulatory structure mostconducive to their business and marketplace needs.Allowing carriers discretion as they develop andlicense products may have the desirable conse-quence of greater flexibility in product design butalso the potentially undesirable consequence ofavoidance of some types of oversight.
Finally, among consumers, stakeholders, andpolicymakers, dual regulation means that there will always be the potential for confusion, mis-understanding, and misinformation.
This project has led the authors to conclude thatany policy change in this area necessitates clearlyarticulated goals and objectives along with opendiscussion of both intended and unintendedconsequences. This means carefully analyzing how statute, regulation, and department styles and strategies may combine such that the actualimpact of various policy choices may ultimatelydiffer from the original intent.
The following questions offer just two examples of possible proposed changes and consequences:
■ If all health coverage were moved to DMHC and made subject to Knox-Keene basic benefitsrequirements, would that reduce or eliminateaffordable options for some consumers?
■ Would consolidating consumer complaint func-tions result in lower levels of expertise or com-petence by complaint handlers who might notunderstand specific statutory and real world dif-ferences among carriers and licensing require-ments? How could that be avoided or mitigated?
M a k i n g S e n s e o f M a n a g e d C a r e R e g u l a t i o n i n C a l i f o r n i a 25
Conclusion 5

A deliberate process has been put in place to studythe ramifications of change, giving policymakersand stakeholders the opportunity to carefullyinvestigate all options before making changes tothe current statutory and regulatory environment.The complexities of the regulatory environment as outlined in this report warrant that level ofthoughtful scrutiny.
Simpler and more understandable regulatoryrequirements, combined with consistent enforce-ment, increase the likelihood that the system willfunction to bring consumers affordable, high-quality care. Given the high number of uninsuredCalifornians, and increasing consumer anxiety overhealth care quality, high-quality care at affordableprices should be the ultimate objective of policychange.
26 C a l i f o r n i a H e a l t h C a r e F o u n d a t i o n

M a k i n g S e n s e o f M a n a g e d C a r e R e g u l a t i o n i n C a l i f o r n i a 27
Appendices
Appendix A: History of the Knox-Keene Health Care Service Plan Act of 1975
1929 Ross-Loos Clinic opens in Los Angeles. First prepaid contract with a group practice of physicians providesmedical care for workers in the city’s water department.
1937 Chapter 11A of the Insurance Code enacted, authorizing first Blue Cross hospital insurance in California as anonprofit hospital service plan subject to the Insurance Code. (Chapter 881, Statutes of 1937)
1938 California Medical Association votes to create California Physicians Service (CPS) (later Blue Shield). CPSprovides coverage for medical and surgical services to employee groups who receive care from “professional[physician] members” of CPS “on a periodic budgeting basis.” CPS does not seek state licensure.
1941 Blue Shield registers as a health service plan under Civil Code Section 593a (legislation sponsored by BlueShield), requiring a service plan to obtain a certificate from the Board of Medical Examiners. Generalsupervision placed with the Attorney General but funds are not budgeted for implementation.
1945 Permanente Health Plan (later Kaiser Permanente) opens public enrollment in the nonprofit prepaid healthplan originally developed for employees of Kaiser Industries. Kaiser Permanente is a group practice modelHMO where a Permanente Medical Group provides services on an exclusive basis to Kaiser enrollees in anarea. The health plan also has an exclusive contract with Kaiser Foundation Hospitals for hospital services.
1946 CPS v. Garrison. California Supreme Court rules that CPS (Blue Shield) (and other prepaid health plans) isnot in the business of insurance and is not subject to the jurisdiction of the Insurance Commissioner.
1954 The local medical society establishes the Foundation for Medical Care in the Stockton/San Joaquin Valleyarea. FMC is an early prototype of the IPA-model HMO, providing health care services through non-exclusive contracts with community physicians, who are paid discounted fees for the services provided.
1959 Congress passes the Federal Employees’ Health Benefits Act, which establishes health coverage as a benefit forfederal employees.
1961 The Family Health Plan (later FHP, Inc.) opens in Southern California as a nonprofit staff-model HMO.Salaried physicians provide health services to enrolled members. FHP owns and operates its own hospitals,pharmacies, and laboratory facilities.
1965 Knox-Mills Health Plan Act requires health care service plans to register with the California Attorney Gene-ral. (Chapter 880, Statutes of 1965) Ultimately more than one hundred plans registered, including specializedplans such as dental and mental health plans, including Kaiser, Ross-Loos, Blue Shield, and FHP.
Kaiser Health Plan enrollment reaches 1 million members.

28 C a l i f o r n i a H e a l t h C a r e F o u n d a t i o n
1972 Innovative Health Systems of Los Angeles signs first non-pilot PHP contract. By December 1972, some 22PHP contracts with 132,668 Medi-Cal enrollees are in effect, mostly in Los Angeles County.
Within months, the public press, most notably the Los Angeles Times, reports serious PHP abuses. The Timesreports enrollment fraud and abuse, substandard care, and lack of physicians available during business hours.
PHP enrollers indicted in Los Angeles for forging the names of Medi-Cal recipients on PHP enrollmentforms. Los Angeles District Attorney initiates criminal investigation into Los Angeles-based PHPs.
Waxman-Duffy Prepaid Health Plan Act sets standards for Medi-Cal PHPs, under the oversight of DHS,including minimum patient-physician ratios, conflict of interest limitations, and onsite reviews. (AB 1496,Chapter 1366, Statutes of 1972)
1973 California Auditor General’s follow-up report documents serious failures in oversight by DHS and violationsof law by some participating PHPs.
Office of the Legislative Analyst issues scathing report on the administration of the PHP program by DHS.Report details financial schemes where “nonprofit” health plans channel Medi-Cal payments into for-profitsubsidiary provider corporations.
Congress passes the Federal Health Maintenance Organization Act of 1973. (42 U.S.C. 300 et seq.) TheHMO Act establishes comprehensive benefits, community rating requirements, administrative procedures,financial reserves, annual open enrollments, prohibitions on pre-existing condition limitations, and otherrequirements, and provides federal grants for start-up of nonprofit HMOs seeking federal qualification. Thephrase “health maintenance organization” is coined for the first time. The Act also requires employers of morethan 25 workers who are already providing health benefits to offer as one choice an available federallyqualified HMO (later repealed).
Assembly Health Committee holds a series of investigatory hearings on PHP abuses. Topics includeenrollment, marketing procedures, and quality of care.
Chapter 11A of the Insurance Code (nonprofit hospital service plans) is amended to allow for developmentand regulation of nonprofit HMOs, and their licensure as nonprofit hospital service plans. Health Net andTake Care are licensed as nonprofit hospital service plan HMOs, originally as subsidiaries of Blue Cross.
1974 Third Auditor General Report reveals that among 15 PHPs investigated (14 in Los Angeles), only 48 percentof funds paid to the plans over a two-year period went for services to Medi-Cal recipients. The remainingfunds went to administrative costs and profits to contractors and subcontractors.
California Attorney General Younger repudiates Knox-Mills, refuses to administer the Act, and urges theLegislature to enact tougher regulation of health plans.
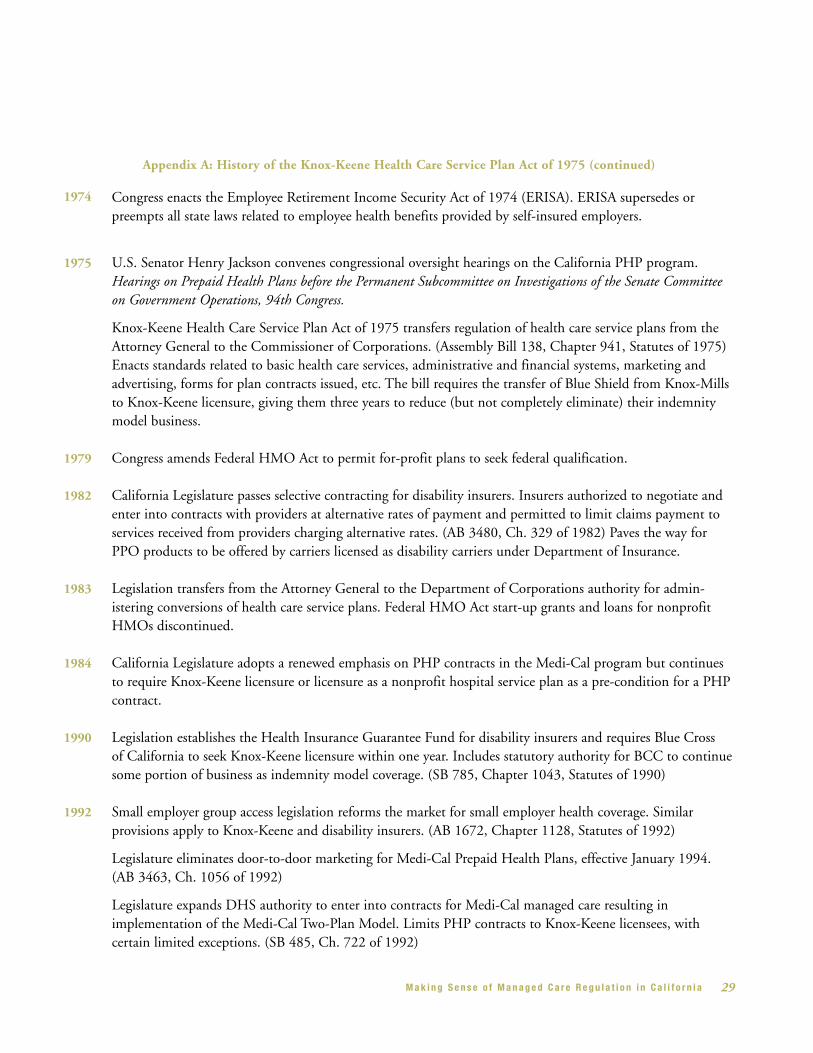
Appendix A: History of the Knox-Keene Health Care Service Plan Act of 1975 (continued)
1971 AB 949, put forward by then Governor Ronald Reagan, enacts significant Medi-Cal reforms, includingauthorizing “prepaid health plans” to serve Medi-Cal beneficiaries, on a capitated basis, under contract withthe Department of Health Services (DHS).
M a k i n g S e n s e o f M a n a g e d C a r e R e g u l a t i o n i n C a l i f o r n i a 29
1975 U.S. Senator Henry Jackson convenes congressional oversight hearings on the California PHP program.Hearings on Prepaid Health Plans before the Permanent Subcommittee on Investigations of the Senate Committeeon Government Operations, 94th Congress.
Knox-Keene Health Care Service Plan Act of 1975 transfers regulation of health care service plans from theAttorney General to the Commissioner of Corporations. (Assembly Bill 138, Chapter 941, Statutes of 1975)Enacts standards related to basic health care services, administrative and financial systems, marketing andadvertising, forms for plan contracts issued, etc. The bill requires the transfer of Blue Shield from Knox-Millsto Knox-Keene licensure, giving them three years to reduce (but not completely eliminate) their indemnitymodel business.
1979 Congress amends Federal HMO Act to permit for-profit plans to seek federal qualification.
1982 California Legislature passes selective contracting for disability insurers. Insurers authorized to negotiate andenter into contracts with providers at alternative rates of payment and permitted to limit claims payment toservices received from providers charging alternative rates. (AB 3480, Ch. 329 of 1982) Paves the way forPPO products to be offered by carriers licensed as disability carriers under Department of Insurance.
1983 Legislation transfers from the Attorney General to the Department of Corporations authority for admin-istering conversions of health care service plans. Federal HMO Act start-up grants and loans for nonprofitHMOs discontinued.
1984 California Legislature adopts a renewed emphasis on PHP contracts in the Medi-Cal program but continuesto require Knox-Keene licensure or licensure as a nonprofit hospital service plan as a pre-condition for a PHPcontract.
1990 Legislation establishes the Health Insurance Guarantee Fund for disability insurers and requires Blue Cross of California to seek Knox-Keene licensure within one year. Includes statutory authority for BCC to continuesome portion of business as indemnity model coverage. (SB 785, Chapter 1043, Statutes of 1990)
Appendix A: History of the Knox-Keene Health Care Service Plan Act of 1975 (continued)
1992 Small employer group access legislation reforms the market for small employer health coverage. Similarprovisions apply to Knox-Keene and disability insurers. (AB 1672, Chapter 1128, Statutes of 1992)
Legislature eliminates door-to-door marketing for Medi-Cal Prepaid Health Plans, effective January 1994.(AB 3463, Ch. 1056 of 1992)
Legislature expands DHS authority to enter into contracts for Medi-Cal managed care resulting inimplementation of the Medi-Cal Two-Plan Model. Limits PHP contracts to Knox-Keene licensees, withcertain limited exceptions. (SB 485, Ch. 722 of 1992)
Congress enacts the Employee Retirement Income Security Act of 1974 (ERISA). ERISA supersedes orpreempts all state laws related to employee health benefits provided by self-insured employers.
1974

30 C a l i f o r n i a H e a l t h C a r e F o u n d a t i o n
Appendix A: History of the Knox-Keene Health Care Service Plan Act of 1975 (continued)
1998 Managed Care Improvement Task Force releases final report. Recommends the creation of a new statedepartment for regulation of health care service plans and phasing in regulation of medical groups and otherprovider entities that bear substantial risk for health care services.
1999 California Legislature passes Patient Bill of Rights. The 21-bill package sponsored and supported byconsumer advocacy groups becomes law. AB 78 creates the new Department of Managed Care and transfersauthority for health care service plans to the new agency.
2000 New Department of Managed Health Care opens for business July 1, 2000. The DMHC constitutes a newAdvisory Committee on Managed Care, a Clinical Advisory Panel, and a Financial Solvency Standards Board,consistent with requirements of AB 78 of 1999.
2001 DMHC contracts with independent consultant for a feasibility study regarding transferring the regulation ofhealth insurance from the California Department of Insurance (CDI) to the new DMHC. Report due to theLegislature December 2001.
1993 Legislature authorizes Knox-Keene plans to develop point-of-service plan contracts. SB 1221, Ch. 987 of1993, allows plans to offer contracts where subscribers can go outside of the plan network for specifiedservices, while incurring higher out-of-pocket costs.
Blue Cross of California licenses four health care service plans, including dental and pharmacy plans, andproposes a controversial corporate restructuring plan.
1995 Consumer hotline enacted. Legislation requires DOC to establish a toll-free number to receive consumercomplaints and inquiries. (SB 689, Ch.789 of 1995)
Blue Cross of California reaches agreement with DOC and the Legislature to dedicate substantial assets tocharity and move forward as a for-profit health care service plan.
1996 Legislature repeals the nonprofit hospital service plan law since there are no remaining licensees. (SB 1866,Ch. 484 of 1996)
Legislation requires DOC to establish HMO Ombudsperson to resolve and respond to consumer complaintsand problems with their health plan. (SB 1936, Ch. 1095 of 1996)
Legislature creates the Managed Health Care Improvement Task Force to report on the status of health carecoverage and the extent to which health care service plans are meeting the goals of cost containment, quality,and access, and to make recommendations on the appropriate role of government in oversight and regulationof managed care. (AB 2343, Ch. 815 of 1996)

M a k i n g S e n s e o f M a n a g e d C a r e R e g u l a t i o n i n C a l i f o r n i a 31
Spec
ializ
ed P
lans
Sec.
740
(a)
Car
rier
s co
veri
ng t
he s
ame
type
s of
serv
ices
are
sub
ject
to
Insu
ranc
ere
gula
tion
but
the
re is
no
spec
ial
cate
gory
of i
nsur
er.
Sec.
134
5(o)
Lice
nses
and
reg
ulat
es s
peci
aliz
edhe
alth
car
e se
rvic
e pl
ans,
tha
t is
,co
ntra
cts
for
heal
th s
ervi
ces
in a
sing
le s
peci
aliz
ed a
rea
such
as
dent
al,
men
tal h
ealth
, or
visi
on.
Oth
er E
ntit
ies
Sec.
742
.20-
742.
44M
ulti
ple
empl
oyer
wel
fare
arra
ngem
ents
(M
EW
As)
mus
t ob
tain
a ce
rtifi
cate
of a
utho
rity
.
1345
, 134
9.1
CC
R §
130
0.43
-130
0.43
.15
Adm
inis
ters
oth
er v
ery
narr
ow a
nd/o
rob
sole
te e
xem
ptio
ns fr
om li
cens
ure
inst
atut
e an
d re
gula
tion
.
App
endi
x B
: Com
pari
son
of S
tatu
tory
and
Reg
ulat
ory
Req
uire
men
tsD
epar
tmen
t of
Man
aged
Hea
lth
Car
e an
d C
alif
orni
a D
epar
tmen
t of
Ins
uran
ce
Activ
ity o
r Fu
nctio
nDe
part
men
t of M
anag
ed H
ealth
Car
eHe
alth
and
Saf
ety
Code
Calif
orni
a De
part
men
t of I
nsur
ance
Insu
ranc
e Co
de
JUR
ISD
ICT
ION
Sec
106:
Def
ines
dis
abili
ty in
sura
nce
as “
insu
ranc
e ap
pert
aini
ng t
o an
inju
ry, d
isab
lem
ent
or d
eath
res
ulti
ngfr
om a
ccid
ents
… o
r si
ckne
ss.”
Reg
ulat
es h
ealth
insu
rers
as
life,
disa
bilit
y an
d pr
oper
ty a
nd c
asua
ltyin
sure
rs.
Car
rier
s co
mm
only
ref
erre
d to
as
“ind
emni
ty”
heal
th in
sure
rs o
rdi
sabi
lity
insu
rers
.
Kno
x K
eene
pla
ns e
xem
pt fr
omre
gula
tion
und
er t
he I
nsur
ance
Cod
eSe
ctio
n 79
1.02
(k).
Pres
umpt
ion
of I
nsur
ance
Dep
artm
ent
juri
sdic
tion
unl
ess
enti
tyis
lice
nsed
by
anot
her
agen
cy.
Sec.
791
.02(
k)
Sec.
740
(a)
Ent
itie
s pr
ovid
ing
cove
rage
for
med
ical
, sur
gica
l, ho
spit
al,
chir
opra
ctic
, phy
sica
l the
rapy
, men
tal
heal
th, d
enta
l, sp
eech
pat
holo
gy,
audi
olog
y, o
ptom
etri
c ..
.
Sec.
101
33.6
Insu
rers
hav
e si
mila
r lim
ited
exem
ptio
n fr
om a
nti-
trus
t. Si
mila
rle
gisl
ativ
e in
tent
. Per
mit
ted
tone
goti
ate
for
“alte
rnat
ive
rate
s of
paym
ent.”
Sec.
134
5(f)
: Hea
lth c
are
serv
ice
plan
s “u
nder
take
to
arra
nge
for
the
prov
isio
n of
hea
lth c
are
serv
ices
, …or
to
reim
burs
e fo
r an
y pa
rt o
f the
cost
of s
ervi
ces,
in r
etur
n fo
r a
prep
aid
or p
erio
dic
char
ge, p
aid
for
by o
r on
beh
alf o
f the
sub
scri
bers
or
enro
llees
.”
Lice
nses
and
reg
ulat
es a
ll “h
ealth
car
ese
rvic
e pl
ans.
”
Reg
ulat
es a
ll H
MO
s an
d tw
oco
mpa
nies
tha
t of
fer
PPO
pla
nsun
der
stat
utor
y an
d/or
reg
ulat
ory
wai
vers
.
Exe
mpt
ions
Sec.
134
3(e)
Incl
udes
oth
er v
ery
narr
ow a
ndsp
ecifi
c ex
empt
ions
.
Sec.
134
3(e)
Sec.
134
3.1
Sec.
134
9.1,
134
9.3
Sec.
134
9.2
Insu
rers
, unl
ess
they
dir
ectly
pro
vide
serv
ices
thr
ough
con
trac
ted
or o
wne
dpr
ovid
ers
and
/or
faci
litie
s.
Life
car
e fa
cilit
ies
for
the
elde
rly
Long
-ter
m c
are
dem
onst
rati
onpr
ogra
ms
Publ
ic a
mbu
lanc
e se
rvic
es
Join
t la
bor
man
agem
ent
trus
ts
Ant
i-tr
ust
Sec.
134
2.6
Lim
ited
sta
te a
nti-
trus
t ex
empt
ion
rela
ted
to p
rovi
der
nego
tiat
ions
.Le
gisl
ativ
e in
tent
sup
port
ing
the
form
atio
n of
gro
ups
or c
ombi
nati
ons
of p
rovi
ders
and
pur
chas
ing
grou
ps.
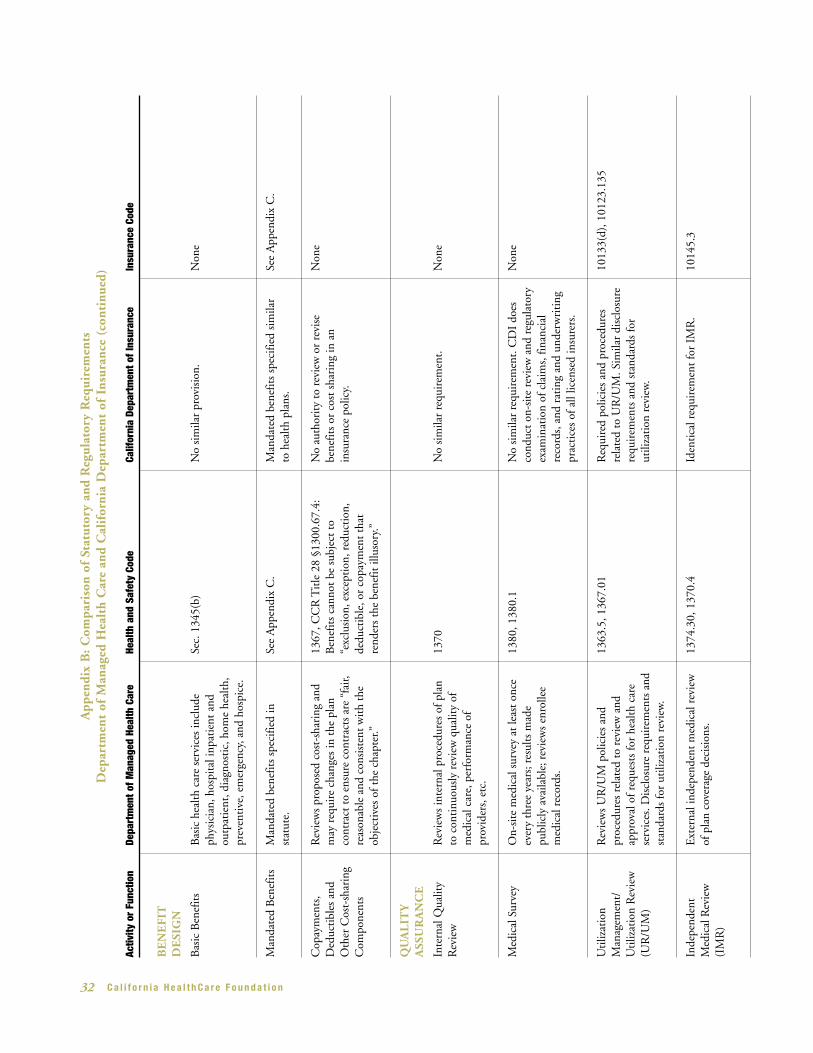
32 C a l i f o r n i a H e a l t h C a r e F o u n d a t i o n
Inde
pend
ent
Med
ical
Rev
iew
(IM
R)
1014
5.3
Iden
tica
l req
uire
men
t fo
r IM
R.
1374
.30,
137
0.4
Ext
erna
l ind
epen
dent
med
ical
rev
iew
of p
lan
cove
rage
dec
isio
ns.A
ppen
dix
B: C
ompa
riso
n of
Sta
tuto
ry a
nd R
egul
ator
y R
equi
rem
ents
Dep
artm
ent
of M
anag
ed H
ealt
h C
are
and
Cal
ifor
nia
Dep
artm
ent
of I
nsur
ance
(co
ntin
ued)
Activ
ity o
r Fu
nctio
nDe
part
men
t of M
anag
ed H
ealth
Car
eHe
alth
and
Saf
ety
Code
Calif
orni
a De
part
men
t of I
nsur
ance
Insu
ranc
e Co
de
BE
NE
FIT
D
ESI
GN
Bas
ic B
enef
its
No
sim
ilar
prov
isio
n.N
one
Man
date
d B
enef
its
See
App
endi
x C
.M
anda
ted
bene
fits
spec
ified
sim
ilar
to h
ealth
pla
ns.
See
App
endi
x C
.M
anda
ted
bene
fits
spec
ified
inst
atut
e.
Bas
ic h
ealth
car
e se
rvic
es in
clud
eph
ysic
ian,
hos
pita
l inp
atie
nt a
ndou
tpat
ient
, dia
gnos
tic,
hom
e he
alth
,pr
even
tive
, em
erge
ncy,
and
hos
pice
.
Sec.
134
5(b)
Cop
aym
ents
,D
educ
tibl
es a
ndO
ther
Cos
t-sh
arin
gC
ompo
nent
s
Non
eN
o au
thor
ity
to r
evie
w o
r re
vise
bene
fits
or c
ost
shar
ing
in a
nin
sura
nce
polic
y.
1367
, CC
R T
itle
28
§130
0.67
.4:
Ben
efit
s ca
nnot
be
subj
ect
to“e
xclu
sion
, exc
epti
on, r
educ
tion
,de
duct
ible
, or
copa
ymen
t th
atre
nder
s th
e be
nefit
illu
sory
.”
Rev
iew
s pr
opos
ed c
ost-
shar
ing
and
may
req
uire
cha
nges
in t
he p
lan
cont
ract
to
ensu
re c
ontr
acts
are
“fa
ir,re
ason
able
and
con
sist
ent
wit
h th
eob
ject
ives
of t
he c
hapt
er.”
QU
AL
ITY
A
SSU
RA
NC
E
Inte
rnal
Qua
lity
Rev
iew
No
sim
ilar
requ
irem
ent.
Med
ical
Sur
vey
Non
eN
o si
mila
r re
quir
emen
t. C
DI
does
cond
uct
on-s
ite
revi
ew a
nd r
egul
ator
yex
amin
atio
n of
cla
ims,
fina
ncia
lre
cord
s, a
nd r
atin
g an
d un
derw
riti
ngpr
acti
ces
of a
ll lic
ense
d in
sure
rs.
1380
, 138
0.1
On-
site
med
ical
sur
vey
at le
ast
once
ever
y th
ree
year
s; r
esul
ts m
ade
publ
icly
ava
ilabl
e; r
evie
ws
enro
llee
med
ical
rec
ords
.
Rev
iew
s in
tern
al p
roce
dure
s of
pla
nto
con
tinu
ousl
y re
view
qua
lity
ofm
edic
al c
are,
per
form
ance
of
prov
ider
s, e
tc.
1370
Non
e
Uti
lizat
ion
Man
agem
ent/
Uti
lizat
ion
Rev
iew
(UR
/UM
)
1013
3(d)
, 101
23.1
35R
equi
red
polic
ies
and
proc
edur
esre
late
d to
UR
/UM
. Sim
ilar
disc
losu
rere
quir
emen
ts a
nd s
tand
ards
for
utili
zati
on r
evie
w.
1363
.5, 1
367.
01R
evie
ws
UR
/UM
pol
icie
s an
dpr
oced
ures
rel
ated
to
revi
ew a
ndap
prov
al o
f req
uest
s fo
r he
alth
car
ese
rvic
es. D
iscl
osur
e re
quir
emen
ts a
ndst
anda
rds
for
utili
zati
on r
evie
w.

M a k i n g S e n s e o f M a n a g e d C a r e R e g u l a t i o n i n C a l i f o r n i a 33
PR
OV
IDE
RN
ET
WO
RK
SN
one
No
sim
ilar
requ
irem
ent.
1351
(k)
Plan
s re
quir
ed t
o re
ceiv
e pr
ior
appr
oval
of n
etw
orks
in e
ach
geog
raph
ic r
egio
n. N
ot a
pplic
able
to
out-
of-n
etw
ork
serv
ices
.
No
sim
ilar
requ
irem
ent.
Non
e
1013
3.5
Acc
essi
bilit
y re
gula
tion
s fo
r E
POs,
no
filin
gs o
f net
wor
ks r
equi
red
and
limit
ed o
vers
ight
bey
ond
polic
ydi
sclo
sure
. EPO
pro
duct
s ra
re o
rno
n-ex
iste
nt.
Sepa
rati
on o
fM
edic
al a
ndA
dmin
istr
ativ
e
1367
(g)
Rev
iew
s pl
an p
roce
ss t
o se
para
tem
edic
al d
ecis
ions
from
fisc
al /
adm
inis
trat
ive
man
agem
ent.
AC
CE
SSIB
ILIT
Y
OF
SE
RV
ICE
S13
67(e
)M
onit
ors
and
revi
ews
spec
ific
guid
elin
es fo
r av
aila
bilit
y an
dac
cess
ibili
ty o
f pro
vide
rs (
i.e.,
1pr
imar
y ca
re p
hysi
cian
for
ever
y2,
000
enro
llees
, pro
vide
r w
ithi
n 30
min
utes
or
15 m
iles)
. Not
app
licab
leto
out
-of-
netw
ork
serv
ices
of K
nox-
Kee
ne P
POs.
App
endi
x B
: Com
pari
son
of S
tatu
tory
and
Reg
ulat
ory
Req
uire
men
tsD
epar
tmen
t of
Man
aged
Hea
lth
Car
e an
d C
alif
orni
a D
epar
tmen
t of
Ins
uran
ce (
cont
inue
d)
Activ
ity o
r Fu
nctio
nDe
part
men
t of M
anag
ed H
ealth
Car
eHe
alth
and
Saf
ety
Code
Calif
orni
a De
part
men
t of I
nsur
ance
Insu
ranc
e Co
de
RE
GU
LA
TO
RY
F
ILIN
GS
Mat
eria
lM
odifi
cati
ons
900,
109
70, 7
17, 1
011,
102
90,
1027
0.9,
102
91.5
(f),
102
93, 1
215-
1215
.16.
CD
I ha
s 30
day
s to
dis
appr
ove
polic
yfo
rms,
rat
ing
chan
ges,
and
oth
erre
quir
ed fi
lings
.
Dis
abili
ty in
sure
rs li
mit
ed t
one
goti
atio
n fo
r “a
ltern
ativ
e ra
tes
ofpa
ymen
t.” A
t-ri
sk p
rovi
der
cont
ract
sno
t pe
rmis
sibl
e.
1013
3
1351
, 135
2, 1
352.
1Pl
ans
mus
t ob
tain
pri
or a
ppro
val f
orpl
an c
ontr
acts
, ser
vice
are
as, a
ndot
her
maj
or c
hang
es.
PR
OV
IDE
R
RE
LAT
ION
SHIP
SA
ND
A
RR
AN
GE
ME
NT
S
Paym
ent
Met
hods
1344
, 137
0, C
CR
Tit
le 2
8 §
1300
.70(
b)(H
)
1348
.6, 1
349.
3, 1
375.
6
Rev
iew
s pr
ovid
er c
ontr
acts
(no
t ra
tes
of p
aym
ent)
and
hea
lth p
lan
polic
ies
and
proc
edur
es fo
r en
suri
ng p
rovi
ders
can
assu
me
risk
of t
he c
ontr
act.
Ris
kco
ntra
cts
wit
h pr
ovid
ers
perm
issi
ble,
subj
ect
to li
mit
atio
ns.
1012
3.36
Sam
e as
Kno
x-K
eene
.E
cono
mic
Pro
filin
g13
67.0
2M
ust
mak
e pu
blic
ly a
vaila
ble
polic
ies
and
proc
edur
es r
elat
ed t
o ec
onom
icpr
ofili
ng—
revi
ewin
g pr
ovid
ers
base
don
cos
ts o
r ut
iliza
tion
.

34 C a l i f o r n i a H e a l t h C a r e F o u n d a t i o n
Prov
ider
Dis
pute
Res
olut
ion
Non
eN
o si
mila
r re
quir
emen
t.13
67(h
)R
evie
ws
plan
pro
vide
r di
sput
ere
solu
tion
sys
tem
.
App
endi
x B
: Com
pari
son
of S
tatu
tory
and
Reg
ulat
ory
Req
uire
men
tsD
epar
tmen
t of
Man
aged
Hea
lth
Car
e an
d C
alif
orni
a D
epar
tmen
t of
Ins
uran
ce (
cont
inue
d)
Activ
ity o
r Fu
nctio
nDe
part
men
t of M
anag
ed H
ealth
Car
eHe
alth
and
Saf
ety
Code
Calif
orni
a De
part
men
t of I
nsur
ance
Insu
ranc
e Co
de
Plan
for
Inso
lven
tC
arri
ers
1067
-106
7.18
Car
rier
s m
ust
belo
ng t
o th
e Li
fe a
ndH
ealth
Ins
uran
ce G
uara
ntee
Ass
ocia
tion
, whi
ch w
ill a
sses
sm
embe
rs t
o pa
y th
e cl
aim
s of
an
inso
lven
t in
sure
r.
1394
.7D
irec
tor
may
ass
ign
enro
llees
of a
nin
solv
ent
plan
to
plan
s in
the
are
aw
ith
suff
icie
nt c
apac
ity
and
finan
cial
reso
urce
s. P
lans
mus
t pr
ovid
e ca
re fo
rtr
ansf
erre
d m
embe
rs.
CO
NSU
ME
R
PR
OT
EC
TIO
NS
Inte
rnal
Gri
evan
cePr
oced
ure
Non
eN
o si
mila
r re
quir
emen
t.
Ope
rate
s co
nsum
er c
ompl
aint
line
for
all l
ines
of i
nsur
ance
wee
kday
s 8
a.m
. unt
il 6
p.m
.
700-
700.
5, 1
0489
.1-1
0489
.95,
730
,73
9-73
9.12
Car
rier
s su
bjec
t to
min
imum
res
erve
san
d N
atio
nal A
ssoc
iati
on o
fIn
sura
nce
Com
mis
sion
ers
(NA
IC)
risk
-bas
ed c
apit
ol r
equi
rem
ents
.R
egul
ar fi
nanc
ial f
iling
s an
d on
-sit
efin
anci
al r
evie
w.
1351
(i),
136
8, 1
370.
2, 1
380(
f)R
evie
ws
plan
’s in
tern
al g
riev
ance
proc
edur
e, r
evie
ws
resu
lts o
n ap
peal
by e
nrol
lee,
rev
iew
s co
nsum
erco
mpl
aint
s du
ring
on-
site
sur
vey.
Toll-
free
Con
sum
erH
otlin
eO
pera
tes
the
HM
O H
elp
Cen
ter,
24ho
urs
per
day,
7 d
ays
per
wee
k. A
fter
-ho
urs
answ
erin
g se
rvic
e ca
n pa
geD
MH
C h
ealth
pro
fess
iona
ls.
FIN
AN
CIA
L
SOLV
EN
CY
1376
, 138
1, 1
382
Plan
s m
ust
mee
t ta
ngib
le n
et e
quit
yre
quir
emen
ts. R
egul
ar fi
nanc
ial
filin
gs a
nd o
n-si
te fi
nanc
ial r
evie
w.
FE
ES
Var
ious
Reg
ulat
ory
filin
g fe
es b
ased
on
type
of fi
ling.
No
asse
ssm
ent
base
d on
num
ber
of in
sure
ds.
1356
Ann
ual a
sses
smen
t ba
sed
on n
umbe
rof
enr
olle
es. P
lans
rei
mbu
rse
cost
of
licen
sing
app
licat
ion.
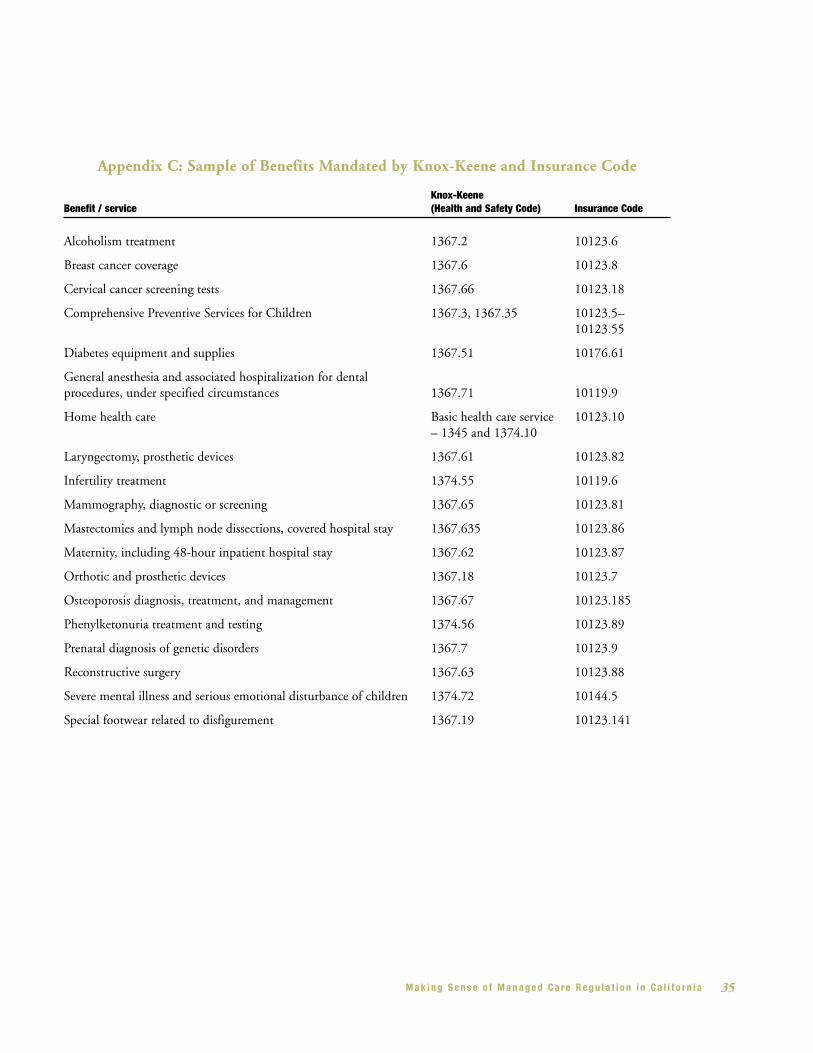
M a k i n g S e n s e o f M a n a g e d C a r e R e g u l a t i o n i n C a l i f o r n i a 35
Appendix C: Sample of Benefits Mandated by Knox-Keene and Insurance Code
Knox-Keene Benefit / service (Health and Safety Code) Insurance Code
Alcoholism treatment 1367.2 10123.6
Breast cancer coverage 1367.6 10123.8
Cervical cancer screening tests 1367.66 10123.18
Comprehensive Preventive Services for Children 1367.3, 1367.35 10123.5–10123.55
Diabetes equipment and supplies 1367.51 10176.61
General anesthesia and associated hospitalization for dental procedures, under specified circumstances 1367.71 10119.9
Home health care Basic health care service 10123.10– 1345 and 1374.10
Laryngectomy, prosthetic devices 1367.61 10123.82
Infertility treatment 1374.55 10119.6
Mammography, diagnostic or screening 1367.65 10123.81
Mastectomies and lymph node dissections, covered hospital stay 1367.635 10123.86
Maternity, including 48-hour inpatient hospital stay 1367.62 10123.87
Orthotic and prosthetic devices 1367.18 10123.7
Osteoporosis diagnosis, treatment, and management 1367.67 10123.185
Phenylketonuria treatment and testing 1374.56 10123.89
Prenatal diagnosis of genetic disorders 1367.7 10123.9
Reconstructive surgery 1367.63 10123.88
Severe mental illness and serious emotional disturbance of children 1374.72 10144.5
Special footwear related to disfigurement 1367.19 10123.141
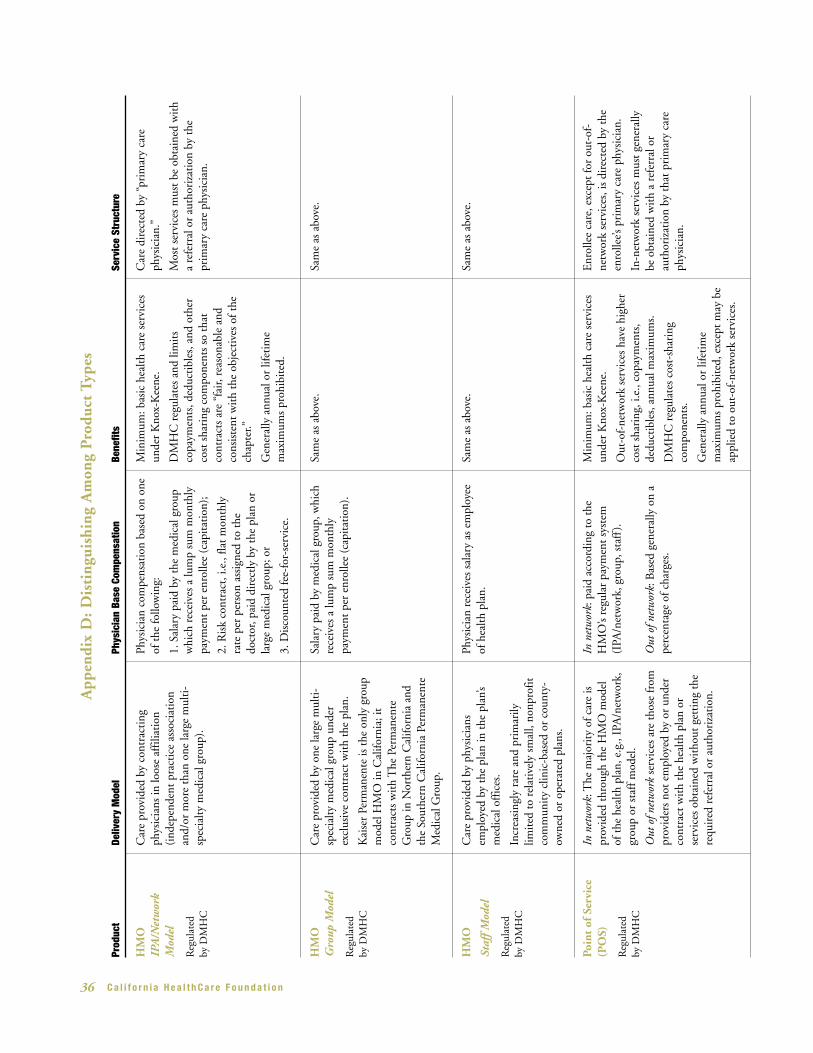
36 C a l i f o r n i a H e a l t h C a r e F o u n d a t i o n
Poin
t of
Ser
vice
(PO
S)
Reg
ulat
ed
by D
MH
C
Enr
olle
e ca
re, e
xcep
t fo
r ou
t-of
-ne
twor
k se
rvic
es, i
s di
rect
ed b
y th
een
rolle
e’s p
rim
ary
care
phy
sici
an.
In-n
etw
ork
serv
ices
mus
t ge
nera
lly
be o
btai
ned
wit
h a
refe
rral
or
auth
oriz
atio
n by
tha
t pr
imar
y ca
reph
ysic
ian.
Min
imum
: bas
ic h
ealth
car
e se
rvic
esun
der
Kno
x-K
eene
.
Out
-of-
netw
ork
serv
ices
hav
e hi
gher
cost
sha
ring
, i.e
., co
paym
ents
,de
duct
ible
s, a
nnua
l max
imum
s.
DM
HC
reg
ulat
es c
ost-
shar
ing
com
pone
nts.
Gen
eral
ly a
nnua
l or
lifet
ime
max
imum
s pr
ohib
ited
, exc
ept
may
be
appl
ied
to o
ut-o
f-ne
twor
k se
rvic
es.
In n
etw
ork:
pai
d ac
cord
ing
to t
heH
MO
’s re
gula
r pa
ymen
t sy
stem
(IPA
/net
wor
k, g
roup
, sta
ff).
Out
of n
etw
ork:
Bas
ed g
ener
ally
on
ape
rcen
tage
of c
harg
es.
In n
etw
ork:
The
maj
orit
y of
car
e is
prov
ided
thr
ough
the
HM
O m
odel
of t
he h
ealth
pla
n, e
.g.,
IPA
/net
wor
k,gr
oup
or s
taff
mod
el.
Out
of n
etw
ork
serv
ices
are
tho
se fr
ompr
ovid
ers
not
empl
oyed
by
or u
nder
cont
ract
wit
h th
e he
alth
pla
n or
serv
ices
obt
aine
d w
itho
ut g
etti
ng t
here
quir
ed r
efer
ral o
r au
thor
izat
ion.A
ppen
dix
D: D
isti
ngui
shin
g A
mon
g P
rodu
ct T
ypes
Prod
uct
Deliv
ery
Mod
elPh
ysic
ian
Base
Com
pens
atio
nBe
nefit
sSe
rvic
e St
ruct
ure
HM
OIP
A/N
etw
ork
Mod
el
Reg
ulat
ed
by D
MH
C
Car
e di
rect
ed b
y “p
rim
ary
care
phys
icia
n.”
Mos
t se
rvic
es m
ust
be o
btai
ned
wit
ha
refe
rral
or
auth
oriz
atio
n by
the
prim
ary
care
phy
sici
an.
Min
imum
: bas
ic h
ealth
car
e se
rvic
esun
der
Kno
x-K
eene
.
DM
HC
reg
ulat
es a
nd li
mit
sco
paym
ents
, ded
ucti
bles
, and
oth
erco
st s
hari
ng c
ompo
nent
s so
tha
tco
ntra
cts
are
“fai
r, re
ason
able
and
cons
iste
nt w
ith
the
obje
ctiv
es o
f the
chap
ter.”
Gen
eral
ly a
nnua
l or
lifet
ime
max
imum
s pr
ohib
ited
.
Sam
e as
abo
ve.
Sam
e as
abo
ve.
Sam
e as
abo
ve.
Sam
e as
abo
ve.
Phys
icia
n co
mpe
nsat
ion
base
d on
one
of t
he fo
llow
ing:
1. S
alar
y pa
id b
y th
e m
edic
al g
roup
whi
ch r
ecei
ves
a lu
mp
sum
mon
thly
paym
ent
per
enro
llee
(cap
itat
ion)
;
2. R
isk
cont
ract
, i.e
., fla
t m
onth
lyra
te p
er p
erso
n as
sign
ed t
o th
edo
ctor
, pai
d di
rect
ly b
y th
e pl
an o
rla
rge
med
ical
gro
up; o
r
3. D
isco
unte
d fe
e-fo
r-se
rvic
e.
Car
e pr
ovid
ed b
y co
ntra
ctin
gph
ysic
ians
in lo
ose
affil
iati
on(i
ndep
ende
nt p
ract
ice
asso
ciat
ion
and/
or m
ore
than
one
larg
e m
ulti
-sp
ecia
lty m
edic
al g
roup
).
HM
OG
roup
Mod
el
Reg
ulat
ed
by D
MH
C
Sala
ry p
aid
by m
edic
al g
roup
, whi
chre
ceiv
es a
lum
p su
m m
onth
lypa
ymen
t pe
r en
rolle
e (c
apit
atio
n).
Car
e pr
ovid
ed b
y on
e la
rge
mul
ti-
spec
ialty
med
ical
gro
up u
nder
excl
usiv
e co
ntra
ct w
ith
the
plan
.
Kai
ser
Perm
anen
te is
the
onl
y gr
oup
mod
el H
MO
in C
alifo
rnia
; it
cont
ract
s w
ith
The
Per
man
ente
Gro
up in
Nor
ther
n C
alifo
rnia
and
the
Sout
hern
Cal
iforn
ia P
erm
anen
teM
edic
al G
roup
.
HM
O
Staf
f Mod
el
Reg
ulat
ed
by D
MH
C
Phys
icia
n re
ceiv
es s
alar
y as
em
ploy
eeof
hea
lth p
lan.
Car
e pr
ovid
ed b
y ph
ysic
ians
empl
oyed
by
the
plan
in t
he p
lan’
sm
edic
al o
ffic
es.
Incr
easi
ngly
rar
e an
d pr
imar
ilylim
ited
to
rela
tive
ly s
mal
l, no
npro
fitco
mm
unit
y cl
inic
-bas
ed o
r co
unty
-ow
ned
or o
pera
ted
plan
s.

M a k i n g S e n s e o f M a n a g e d C a r e R e g u l a t i o n i n C a l i f o r n i a 37
App
endi
x D
: Dis
ting
uish
ing
Am
ong
Pro
duct
Typ
es (
cont
inue
d)
Prod
uct
Deliv
ery
Mod
elPh
ysic
ian
Base
Com
pens
atio
nBe
nefit
sSe
rvic
e St
ruct
ure
Pre
ferr
ed P
rovi
der
Org
aniz
atio
n(P
PO
)
Reg
ulat
ed
by D
MH
C
(by
spec
ific
exem
ptio
n,B
lue
Cro
ss a
nd B
lue
Shie
ld a
re t
he o
nly
DM
HC
pla
nsau
thor
ized
to
offe
r a
PPO
pro
duct
)
No
prim
ary
care
pro
vide
r as
sign
men
t.
Ref
erra
l not
nee
ded
in o
rder
to
see
spec
ialis
t, bu
t so
me
serv
ices
may
be
subj
ect
to p
rior
aut
hori
zati
on b
y th
ehe
alth
pla
n.
Min
imum
: bas
ic h
ealth
car
e se
rvic
esun
der
Kno
x-K
eene
.
DM
HC
reg
ulat
es c
ost
shar
ing
com
pone
nts.
Gen
eral
ly a
nnua
l or
lifet
ime
max
imum
s pr
ohib
ited
but
may
be
appl
ied
to o
ut-o
f-ne
twor
k se
rvic
es.
Phys
icia
ns p
aid
on a
fee-
for-
serv
ice
ordi
scou
nted
fee-
for-
serv
ice
basi
s.
Ris
k co
ntra
cts
wit
h pr
ovid
ers
proh
ibit
ed u
nder
the
Ins
uran
ceC
ode.
Enr
olle
e ca
n re
ceiv
e se
rvic
es fr
om a
nylic
ense
d pr
ovid
er.
Sele
ctin
g pr
ovid
ers
from
the
“pre
ferr
ed p
rovi
der”
list
red
uces
out
-of
-poc
ket
cost
s (c
opay
men
ts,
dedu
ctib
les,
co-
insu
ranc
e).
Ref
ers
to K
nox-
Kee
ne “
full
serv
ice”
(med
ical
) pl
ans.
Inde
mni
tyP
refe
rred
Pro
vide
rO
rgan
izat
ion
(PP
O)
Reg
ulat
ed
by C
DI
No
stat
utor
y m
inim
um s
ervi
ces,
exce
pt s
peci
fic m
anda
ted
bene
fits.
No
regu
lato
ry r
evie
w o
r lim
its
onou
t-of
-poc
ket
cost
s su
ch a
sco
paym
ents
, ded
ucti
bles
, or
annu
alan
d lif
etim
e m
axim
ums.
Trad
itio
nal
Inde
mni
ty P
lan
Reg
ulat
ed
by C
DI
Not
app
licab
le.
No
stat
utor
y or
reg
ulat
ory
min
imum
s or
req
uire
men
ts, e
xcep
tsp
ecifi
c m
anda
ted
bene
fits.
No
regu
lato
ry r
evie
w o
r lim
its
onou
t-of
-poc
ket
cost
s su
ch a
sco
paym
ents
, ded
ucti
bles
, or
annu
alan
d lif
etim
e m
axim
ums.
Typi
cally
a p
erce
ntag
e of
usu
al a
ndcu
stom
ary
fees
.In
sure
d ca
n re
ceiv
e se
rvic
es fr
om a
nypr
ovid
er w
itho
ut n
etw
ork
limit
atio
nor
dis
coun
ted
netw
ork
offe
ring
.
Sam
e as
abo
ve.
Sam
e as
abo
ve.
Sam
e as
abo
ve.

38 C a l i f o r n i a H e a l t h C a r e F o u n d a t i o n
Warren BarnesSupervising CounselDepartment of Managed Health Care
Beth CapellLegislative AdvocateHealth Access
Joe CriscioneSenior ConsultantBlue Shield of California
Emery “Soap” DowellFormer Member, Managed Risk Medical Insurance BoardFormer Vice President of Government AffairsBlue Cross of California
Anne EowanVice PresidentAssociation of California Life and HealthInsurance Companies
Richard FigueroaDeputy Secretary, Legislative AffairsGovernor’s Office
Maureen O’Haren Legislative AdvocateHyde, Miller, Owen & TrostFormer Executive Vice PresidentCalifornia Association of Health Plans
Paul PressFormer Chief ConsultantAssembly Health Committee
Shelley RouillardProgram DirectorHealth Rights Hotline
Herb SchultzDeputy Director for External AffairsDepartment of Managed Health Care
Jeff SheltonVice President, Government Affairs Health Net
Lyle SwallowChief Legal CounselBlue Shield of California
Steve ThompsonVice PresidentCalifornia Medical Association
Barbara YonemuraDeputy Director and Chief CounselDepartment of Health ServicesFormer Legal Advisor to the Office of the DirectorDepartment of Managed Health Care
Steve ZatkinSenior Vice PresidentGovernment RelationsKaiser Permanente
Walter ZelmanPresident and CEOCalifornia Association of Health Plans
Appendix E: Key Informant Interviews
Staff members at the California Department of Insurance and the Department of Managed Health Care providedextensive amounts of background information and materials. CDI was invited to participate in key informantinterviews, but chose instead to respond to written technical questions and to provide extensive written and oralcomments from a team of staff members.

M a k i n g S e n s e o f M a n a g e d C a r e R e g u l a t i o n i n C a l i f o r n i a 39
Notes
1 AB 78, Chapter 525, Statutes of 1999.
2 The Future of California’s Health Care: Solving theSafety Net Puzzle in the New California Context.California Forum for Critical Health Issues,Institute for the Future (IFTF). (1997)
3 Ibid.
4 Ibid.
5 Falkson, JL. HMOs and the Politics of HealthSystem Reform. American Hospital Association.Chicago, Illinois. (1980)
6 In California, separate Blue Cross plans originallyemerged in the north and south, ultimatelybecoming one company.
7 Institute for the Future.
8 Ibid.
9 In the Prepaid Health Plan program, health plansenroll Medi-Cal beneficiaries as members andagree to provide all medically necessary Medi-Calservices for a fixed monthly fee.
10 Ibid.
11 AB 1496, Chapter 1366, Statutes of 1972.
12 Chavrin, DF and Treseder, A. California’s PrepaidHealth Plan Program: Can the Patient Be Saved?Hastings Law Journal. Vol. 28: 685-760. (January1977)
13 Ibid.
14 Ibid.
15 Falkson, JL. HMOs and the Politics of HealthSystem Reform. American Hospital Association.Chicago, Illinois. (1980)
16 Institute for the Future.
17 In his oral history, Howard Hassard (then chiefcounsel to the CMA and counsel for Blue Shield)reported that, as Blue Shield’s membership grew,staff at the Department of Insurance felt increas-ingly uncomfortable with the lack of a regulatoryforum for dealing with consumer complaintsabout the plan. Fifty Years in Law and Medicine:Howard Hassard An Oral History. (1985)
18 Knox-Keene applies to two types of health careservice plans: full-service plans (medical) andspecialized plans such as dental, vision, andmental health. Many of the plans that movedover in the early days were specialized plans. This paper focuses on full-service health careservice plans.
19 AB 138, Chapter 941, Statutes of 1975.
20 This report uses the term “carrier” to refergenerally to entities offering health care coverage,regardless of the license or regulating agency.
21 Except for the limited exceptions of Blue Shield,and a few other specialized plans like DeltaDental, Knox-Keene otherwise requires that allproviders be employed by or under contract withthe health plan.
22 The Full Freedom of Choice Act of 1937provided that insureds with policies underInsurance Department regulation had the right to choose their own health care provider.
23 Institute for the Future.
24 Under Knox-Keene, health plan members arereferred to as enrollees or subscribers, and underthe Insurance Code, as insureds.
25 The only other nonprofit hospital service plansever licensed were two nonprofit HMOs, HealthNet and Take Care, both of which were originally

40 C a l i f o r n i a H e a l t h C a r e F o u n d a t i o n
subsidiary companies of Blue Cross. The non-profit hospital service plan statute was amendedto allow for their licensure and development inthe 1970s. Health Net and Take Care ultimatelybecame Knox-Keene HMOs and later convertedto for-profit status.
26 SB 785, Chapter 1043, Statutes of 1990.
27 California Health and Safety Code §1396.5.
28 Fact Sheet: The California Department of ManagedHealth Care, National Health Law Program,November 28, 2000, obtained online, August2001 (http://www.healthlaw.org).
29 Insurers offering health insurance are oftenreferred to in policy discussions using thecategory of “disability insurer” in the InsuranceCode. According to CDI, insurers of any type(life, property, or casualty) authorized to offer the“class” of disability insurance could offer healthinsurance coverage. For purposes of this report,we use the term disability insurer to refer tocarriers authorized to offer the class of disabilityinsurance.
30 Licensed Knox-Keene plans are legally referred to as “health care service plans.” The phrasehealth maintenance organization (HMO) wascoined in the federal HMO Act, and continues to be the commonly used name for health plansthat provide or deliver services through con-tracted or employed providers, but is generallynot used in California statute. For purposes ofthis report we use the term “health care serviceplan” or “health plan” to refer to Knox-Keenelicensed full-service (medical) plans.
31 Since the PPO lines of business under Knox-Keene are there by special authorization, it issometimes difficult to discuss clearly and easily“Knox-Keene regulation.” Although the twocompanies offering PPOs under Knox-Keene are subject to all relevant Knox-Keene provisions,including providing basic health care services,they do have greater flexibility in product designand out-of-network services are not subject to the
same level of quality assurance and deliverysystem requirements applicable to HMOs lines of business.
32 CDI does not track numbers of insureds or types of policies written by type of coverage,including health insurance, so it is not possible to easily determine exactly how much of thehealth insurance market is insured through CDIregulated policies.
33 Health and Safety Code Section 1367(h) and1367(i). In addition, California Code of Regu-lations, Title 28, §1300.67.2(3)(A) provides thatco-pays and other limitations cannot “render the benefit illusory.” This concept is not furtherdefined in regulation or policy. Several keyinformants report that DMHC has recentlybecome more aggressive in limiting consumercost sharing under this broad regulatoryauthority.
34 However, Knox-Keene plans are specificallyauthorized to (and do) offer Medicare supple-ment products.
35 A point-of-service plan allows consumers to access some services from out-of-networkproviders at higher levels of cost sharing.
36 This allows the plans to avoid the Knox-Keenelimits on cost sharing, out-of-network expenses,and the higher TNE requirements on Knox-Keene plans offering POS.
37 California Association of Health Plans 2000Annual Report and Profile.
38 Ibid.
39 The term “preferred provider” or “preferredprovider organization” (PPO) is generally notused in the Insurance Code but is referenced inone section clarifying that an insurer contractingwith preferred providers is subject to CDIjurisdiction. The product term “PPO” iscommonly used in the marketplace.

Recommended

















