LungCancer2017:It’sComplicated
CraigReynoldsMDFloridaCancerAffiliatesandResearchInstitute
Ocala,Florida

LungCancer—”TheGoodOldDays”• Smallcellhadnochangesanytimerecently• Histologydidn’tmatterinNSCLC• Doubletofchoice(usuallycarboplatinum/paclitaxelintheUS)followedbydocetaxelfollowedbygefitinib orerlotinib
• Nomolecularsubtypesofdisease

LungCancerisNowComplicated
• SCLC—Finallyprogress?• SquamousNSCLC• Nonsquamous NSCLC—Targetedtherapyupdate• ImmunotherapyUpdate

SmallCellLungCancer(SCLC)

SCLC
• Platinum/etoposideisstandardinitialtherapy• Radiationimprovesoutcomesslightlyinlimiteddisease
• Topotecan hasmodestactivityinrelapsed/refractorydiseasebuthastoxicityissues
• Noprogressfortwentyyears,buttwopromisingapproaches

Rovalpituzumab tesirine (Rova-T)
• TargetsDLL3,acancerstemcelltarget• 74patienttrialrelapsed/refractorySCLCreportedatASCO2016,60evaluable
• 68%stabledisease,18%RR• 12patientsreceivedRova T3rd line,with6responses
• Durabilityofresponsesisencouraging• FasttrackbyFDA,shouldhavemoredatawithinayear
Rudin etalASCO2016

ImmunotherapyinSCLC
• Nivolumab andthecombinationofnivolumab andipilumumab havebeenevaluated
• Nivolumab alonehas10%RRwith13%grade¾toxicity
• Nivo/Ipi hashigherresponserates(about20%)with18-19%grade¾toxicity
• Durableresponsesoccur,largerstudiesunderway• ShouldhavegoodcombinationIOdatainSCLCwithinayearAntonioetalLancetOncology20167:883-95

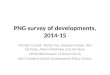
NotMuchProgressinSquamousNSCLCEither
1980s1,2 1990-20053-5 2005-20096-8 2010-20159-10
18
16
14
12
10
8
6
4
2
0
Med
ian
Surv
ival
(Mon
ths)
Single-agent
platinum
Platinum-based
doublets
Platinum-based
doublets
Pem and platinum-triplet (BEV) Platinum-
baseddoublets
Histology-directedtherapy
Oncogene-driventherapy
NSCLC (all histologies)
SqCLC
Non-SqCLC
Pemetrexed and bevacizumab contraindicated in SqCLC histology; No oncogene-directed targeted therapy in squamous histology to date
BEV, bevacizumab; Pem, pemetrexed. 1. Bonomi et al., J Clin Oncol. 1989;7:1602-1613; 2. Eagan et al., J Clin Oncol. 1988;6:5-8; 3. Schiller et al., N Engl J Med. 2002;346:92-98; 4. Sandler et al., J Clin Oncol. 2000;18:122-130; 5. Spira and Ettinger. N Engl J Med. 2004;350:379-392; 6. Sandler et al., N Engl J Med. 2006;355:2542-2550; 7. Scagliotti et al., J Clin Oncol. 2008;26:3543-3551; 8. Scagliotti et al., Oncologist 2009;14:253-263; 9. Socinski et al., J Clin Oncol. 2012;30:2055-2062; 10. Paz-Ares et al., J Clin Oncol. 2013;31:2895-2902.

MolecularTargetsinSquamousNSCLC
Reference Agent Target N(squamous) Study Description PrimaryEndpoint
Scagliotti,2010 Sorafenib RAF, VEGFR 926
(223)
PhaseIIIadvancedNSCLC,includingsquamous(withpaclitaxel/carboplatin) (HRdetrimentinsquamous)
Negative
Novello,2014 Motesanib VEGFR,
PDGFR1450(360)
PhaseIIIadvancedNSCLC,includingsquamous(withpaclitaxel/carboplatin) (unacceptabletoxicityinsquamous)
Negative
Laurie,2014 Cediranib VEGFR,
PDGFR306(39)
PhaseII/IIIadvancedNSCLC,includingsquamous(withcarboplatin/paclitaxel)(haltedforfutility)
Negative
Langer,2014 Figitumumab IGF1R 681
(584)PhaseIIIadvancednon-adenocarcinomaNSCLC(withpaclitaxel/carboplatin) Negative
Sanofi,2013 Iniparib PARP 780
(780)PhaseIIIadvancedsquamousNSCLC(withgemcitabine/carboplatin) Negative
Pirker,2009
Cetuximab(FLEXStudy) EGFR 1125
(377)PhaseIIIadvancedEGFR+NSCLC(withvinorelbine/cisplatin)(HRfavorableinSCCA) Positive

SQUIRETrial

SQUIREResults
GC + N GC
Stratified HR(95%CI) 0.84(0.74,0.96)
Stratified P value(log-rank) 0.01
MedianOS, months(95%CI) 11.5(10.4, 12.6) 9.9(8.9,11.1)
CR, complete response; GC, gemcitabine-cisplatin; N, necitumumab; OS, overall survival; PD, progressive disease; PR, partial response; R, randomization; SD, stable diseaseThatcher et al., Lancet Oncol. 2015;16:763-774.

SQUIREISASQUARE
• Necitumumab didnotsignificantlyimpactpractice• RecentlytakenoutoftheNCCNguidelines• Necitumumab nolongeractivelymarketed

CanWeImprovetheValue?
SQUIRE (EGFR FISH+)1
S0819 (SqCLC-EGFR FISH+)2
FISH, fluorescent in s itu hybridization; GC, gemcitabine and cisplatin; N, necitumumab1. Hirsch et al., WCLC 2015;abstr ORAL32.05; 2. Herbst et al., WCLC 2015;abstr PLEN04.01; 3. Pirker et al., Lancet Oncol. 2012;13:33-42.
FLEX3
aChemotherapy + cetuximabvs chemotherapy

AMAPtoProgressinSquamousNSCLC?
CTBiomarker
profiling (NGS/CLIA) Non-matc
hdrug
Biomarkernon-match
Multiple phase II-III sub-studies with “rolling opening and closure”
Biomarker A
TT A CT
Primary endpointPFS / OS
Biomarker D
TT D+E E
Primary endpointPFS / OS
Biomarker Β
TT B CT
Primary endpointPFS / OS
Biomarker C
TT C+CT CT
Primary endpointPFS / OS
Each sub-study independent of the othersEach sub-study designed for registration of a drug-biomarker combination
Self-sustaining with new sub-studies in planning stages
CLIA, Clinical Laboratory Improvement Amendments; CT, chemotherapy (docetaxel [D] or gemcitabine [G]); E, erlotinib; NGS, next-generation sequencing; OS, overall survival; PFS, progression-free survival; TT, targeted therapy 1. Lung-MAP. Available at: http://www.lung-map.org/healthcare-providers. Accessed February, 2016

MAPInProgress
GDC-0032VsSoC
PalbociclibVsSoc
AZD4547VsSoC
GDC-0032 Palbociclib AZD4547
FGFR1CDK4/6
PI3K
Non-matchSub-studies
Stage1
Stage2
BMN 673VsSoC*
BMN673*
HRD
Nivo/Ipivs
Nivolumab
Checkpoint Naive
MEDI4736/Treme*VsSOC
Checkpoint Refractory
Matched Sub-studies
• Lung-MAP amended to 2nd line therapy & beyond to accommodate Nivolumab approval• Pre-screening added back• Eligibility criteria broadened; *Sub-studies in developmentCDK, cyclin D-dependent k inase; FGFR, fibroblast growth factor receptor; HRD, Homologous
Recombination Defects; Ipi, ipilimumab; PI3K, phosphatidylinositol-4,5-bisphosphate 3-kinase; SoC, standard-of-care1. Lung-MAP. Available at: http://www.lung-map.org/healthcare-providers. Accessed February, 2016

SquamousNSCLCSummary
• Notmuchprogresshereeitherthanimmunotherapy• Necitumumabmightbeconsideredforyounger,motivatedpatients,particularlyifEGFRexpressedathighlevels,thoughaconfirmatorytrialwouldbehelpful
• MAPhasnotfoundtheroadtoprogressyet,butitcontinuesandisanimportanteffort
• Standardapproachisplatinumdoubletchemotherapy(?Withnecitumumab inhighlyselectedpatients)followedbydocetaxelaloneorwithramicurimab andthenafatinib
• We’lltalkaboutimmunotherapylater!

Nonsquamous NSCLC—TargetedTherapy• EGFRmutations—useofliquidbiopsies• ALKmutations—standardofcareischanging• Weareinatargetrichenvironment

EGFRmutatedNSCLC
• Osimertinib isnowapprovedfortheT790Mmutation
• Rebiopsy hasbecomeastandardapproach• Liquidbiopsyisspecificbutnotalwayssensitive,sostandardisliquidbiopsyatprogressionwithtissueifliquidbiopsyisnothelpful
• Rb mutationssuggestsmallcelltransformation,butnotallliquidbiopsiesincludeRb

ALKmutatedNSCLC
• EML-ALKmutationwasdescribedasadrivingmutationinNSCLCin2007
• Crizotinib wasapprovedin2011• TherearenowthreeapprovedALKinhibitorsintheUS—crizotinib,ceritinib,andalectinib

J-ALEX
• Randomizedtrialofalectinib vscrizotinib inALKinhibitornaïveALK-positiveNSCLC
• Japanesetrialof207patientsclosedearlybyDSMB• PFSfavoredalectinib withHR0.34(0.17-0.70,p<.0001)• MedianPFSforalectinib notreachedvs10.2monthsforcrizotinib
• Crizotinib hadmoregrade3-4toxicity• Multinationalconfirmatorytrial(ALEX)willbeatASCO;pressrelaease saysitispositive
• Alectinib islikelythenewstandardinALKpositiveNSCLC
• Alectinib ismuchmoreactiveintheCNSNokihara etalASCO2016abstract9008

OtherTargetsinNonsquamousNSCLC• ROS1• KRAS(sofarnodrugsforthis)• RET• BRAF• METexon14mutations• Morecoming—It’sgettingcomplicated!

TargetedTherapyinNonsquamous NSCLC2017• Rebiopsy isimportant;liquidbiopsiesareusefulbutneedtissueattimes
• UnderstandingofEGFRresistancemutationsisevolvingrapidly
• StandardofcareinALK-positiveNSCLCchangingfromcrizotinib toalectinib
• Newmutations,eachofwhichaccountfor1-2%ofNSCLC,arebeingidentified

ImmunotherapyofNSCLC
• Stateoftheart• Useinfirst-linemetastaticNSCLC• Newapproachesinearlierdisease• Theoreticaldiscussionofvariabilityofresponse

NSCLCImmunotherapy2017
• Threedrugsareapprovedinthesecond-lineandbeyond—pembrolizumab,nivolumab,andatezolizumab
• Useinsecond-linedoesnotrequirePD-L1testingforanyofthesedrugs
• Pembrolizumab isapprovedinfirst-lineNSCLCforpatientswithPD-L1expression>50%

Checkmate017:Nivolumab vs.Docetaxel
Spigel et al., ASCO 2015; abstr 8009.
Brahmer et al., N Engl J Med. 2015;373:123-135.

Checkmate017Results
• Phase III RCT of patients with advanced squamous cell NSCLC in whom disease progressed during or after first-line chemotherapy
• Randomized 272 patients to receive nivolumab 3 mg per kg of body weight every 2 weeks or docetaxel 75 mg/m2 every 3 weeks
•Efficacy of nivolumab was independent of PD-L1 status in this SqCLC trial.•Treatment-related AEs grade 3 or 4 occurred in 7% in the nivolumab group vs 55% in the docetaxel group
Median OS Median PFS
Spigel et al., ASCO 2015; abstr 8009.
Brahmer et al., N Engl J Med. 2015;373:123-135.

PD-L1Expressionin017
No apparent prognostic effect of PD-L1 expression.Survival benefit of nivolumab was independent of PDL1 expression levels.
Spigel et al., ASCO 2015; abstr 8009.
Brahmer et al., N Engl J Med. 2015;373:123-135.

Checkmate057:NonsquamousNSCLC
Borghaei et al., N Engl J Med. 2015;373:1627-1639.

PD-L1ExpressionandOutcomein057
Paz-Ares et al., ASCO 2015, abstr LBA109.
OSbenefitcorrelateswithPD-L1expressioninthisNon-SQ trial.Contrastswithtrial017inSQ.It’scomplicated!

OutcomesofSubgroupsin057
0NIVO DOC
1 2
Paz-Ares et al., ASCO 2015, abstr LBA109.

Immunotherapyin2dLineNSCLCSummary• Datafornivolumab,pembrolizumab,andatezolizumab areallcompellingandfairlysimilar
• Nodirectcomparisonshavebeendoneandlikelyneverwill
• TherewillbesomelimiteddataaboutsequentialIOtherapysoon
• Doublettherapywilllikelymakethismoot

Keynote24:Pembrolizumab in1st-LineNSCLC
R 1:1 N=305
PD / toxicity /
other
PD / toxicity /
other
Key eligibility criteria• Untreated stage IV NSCLC• PD-L1 TPS ≥50%• No activating EGFR mutation or
ALK translocation• No untreated brain metastases Platinum-doublet
chemotherapya
(4-6 cycles) (n=151)
Pembrolizumab 200 mgq3w (35 cycles)
(n=154)
Reck M, et al. Ann Oncol 2016;27(Suppl 6):abstr LBA8_PR
Primary endpoint◆ PFS (RECIST v1.1)
aCarboplatin or cisplatin + pemetrexed, carboplatin or cisplatin + gemcitabine, or carboplatin + paclitaxel, with optional pemetrexed maintenance for nonsquamous NSCLC
Secondary endpoints Exploratory endpoint◆ OS, ORR, safety ♦ DOR
Crossover permitted from chemotherapy to pembrolizumab ifPD

Pembrolizumab vs.ChemotherapyinPD-L1Positive*NSCLC
Reck et al., N Engl J Med. 2016 [Epub ahead of print].
45%
28%
0%
20%
40%
60%
80%
100%
ORR
Pembrolizumab
Chemotherapy
mPFS 10.3 mo
mPFS 6.0 mo
6-mo OS: 80%
6-mo OS: 72%
*PD-L1 expression ≥50%

Keynote24Toxicity
Reck M, et al. Ann Oncol 2016;27(Suppl 6):abstr LBA8_PR
◆ Incidence of treatment-related AE, any severity, was lower with pembrolizumab compared with chemotherapy (73.4 vs 90.0%, respectively).
Exposure and AE summary

Keynote24Summary
• ForpatientswithPD-L1positive(>50%)NSCLC,pembrolizumab improvedOS,PFS,andRRcomparedtochemotherapy
• 44%ofchemotherapypatientscrossedovertopembrolizumab afterdiseaseprogression
• Pembrolizumab hadfeweradverseeventsthanchemotherapy

Keynote21:Chemotherapy+Pembrolizumab
R 1:1
N=123• PD-L1 status (TPS ≥1 vs. <1%)
Key patient inclusion criteria• Untreated stage IIIB / IV
nonsquamous NSCLC• No EGFR mutation or ALK
translocation• Provision of sample for PD-L1
assessment• ECOG PS 0–1• No untreated brain metastases
Pembrolizumab + chemotherapyPembrolizumab 200 mg q3w (2 years)
+carboplatin AUC5 mg/mL/min +
pemetrexed 500 mg/m2 q3w (4 cycles)* (n=60)
Stratification
ChemotherapyCarboplatin AUC5 mg/mL/min +
Pemetrexed 500 mg/m2 q3w (4 cycles)* (n=63)
Secondary endpointsPrimary endpoint◆ ORR (RECIST)central review ♦
PFS, DOR, OS, safety, relationship between anti-tumor activity and PD-L1 TPS
Pembro 200 mg q3w
(2 years)
PD
*Pemetrexed 500 mg/m2 q3w permitted as optional indefinite maintenance therapyLanger C, et al. Ann Oncol 2016;27(Suppl 6):abstr LBA46_PR

Keynote21:KeyResults
Keynote 021 - Key Results and Conclusions
Langer C, et al. Ann Oncol 2016;27(Suppl 6):abstr LBA46_PR; Langer et al, Lancet Oncol. Online Oct 9, 2016.
◆ Pembrolizumab + chemotherapy significantly improved the proportion of patients who achieved an ORR compared with chemotherapy alone (estimated treatment difference 26%)
ORR
, %(9
5%CI
) 10080
60
4020
0 Pembro+ Chemo
Chemo Alone
55%
29%
ConfirmedORR∆26%
p=0.0016
a- alive without subsequent disease progression

Keynote21:KeyResultsKeynote 021 - Key Results and Conclusions
◆ PFS was significantly longer with pembrolizumab + chemotherapy (13.0 mo) compared with chemotherapy alone (8.9 mo) (HR 0.53; p=0.010)
PFS,
%
100
80
60
40
20
00 5 15 2010
Time, months
Pembro + chemo 23
Chemo alone 33
PFS (RECIST v1.1 by Blinded, Independent, Central Review)Events, n HR (95%CI)
0.53
(0.31, 0.91) p=0.0102
Langer C, et al. Ann Oncol 2016;27(Suppl 6):abstr LBA46_PR.

Keynote21:KeyResultsO
RR
,% (9
5%C
I)
ORR by PD-L1 status100
80
60
40
20
0<1% n=21
57% 54% 26% 80% 13% 38% 39% 35%≥1% 1%–49% n=39 n=19
≥50% n=20
<1% n=23
≥1% 1%–49% n=40 n=23
≥50% n=17
Pembrolizumab + chemotherapy Chemotherapy alone
◆ 80% of patients who had a PD-L1 score of ≥50% achieved ORR with pembrolizumab + chemotherapy
Horizontal dotted lines represent the ORR in the total populationLanger C, et al. Ann Oncol 2016;27(Suppl 6):abstr LBA46_PR

Keynote21:KeyResults
Langer C, et al. Ann Oncol 2016;27(Suppl 6):abstr LBA46_PR; Langer et al, Lancet Oncol. Online Oct 9, 2016.
◆ Exposure was 1.6 times longer in the pembrolizumab + chemotherapy group◆ Most treatment-related AEs were mild and grade 1−2 severity
Exposure and AE summary

Keynote21Conclusions
• Pembrolizumab incombinationwithcarboplatinumandpemetrexed hadbetterPFSandRRthanchemotherapyalone
• OSwassimilarbetweentwoarms,butveryimmature
• Safetyprofilewasmanageable• Onlyarandomizedphase2• ConditionalFDAapprovalmaybecomingsoon

First-lineIOSummary
• Pembrolizumab isFDAapprovedforpatientswithPD-L1>50%
• Thechemo/pembro combinationwilllikelygetconditionalapprovalnextmonth
• ThismayhaveanimpactonPD-L1testing• Multipleotherchemo/IOcombinationtrialsareinprogressorhavecompletedaccrual,soawealthofdataiscoming

AndNowForSomethingCompletelyDifferent…

Checkmate026:Nivolumab 1st-LineNSCLC
R 1:1 N=541
Key patient inclusion criteria• Stage IV or recurrent NSCLC• No prior systemic therapy for
advanced disease• No EGFR / ALK mutations sensitive
to targeted inhibitor therapy• PD-L1 expression of ≥1%• CNS mets permitted if adequately trt
at least 2 wks prior to randomization• ECOG PS 0 or 1
Chemotherapy (investigator choice – histology
dependent) for 6 cycles (n=270)
Nivolumab 3 mg/kg IV q2w (n=271)
Primary endpoint◆ PFS (≥5% PD-L1+)
Secondary endpoints◆ PFS (≥1% PD-L1+), OS, ORR
PD / toxicity
PD
Nivolumab (optional)
Stratification
Socinski M, et al. Ann Oncol 2016;27(Suppl 6):abstr LBA7_PR.
• PD-L1 expression (<5% vs. ≥5%)• Histology (squamous vs. nonsquamous)

Checkmate026:Results
Nivolumab
Chemotherapy
Months
PFS,
%
2421181512963 27
100
80
60
40
0
20
0
Primary endpoint (PFS per IRRC in ≥5% PD-L1+)CheckMate 026: Nivolumab vs. chemotherapy in first-line NSCLC
All randomized patients (≥1% PD-L1+): HR 1.17 (95%CI 0.95, 1.43)
Socinski M, et al. Ann Oncol 2016;27(Suppl 6):abstr LBA7_PR
HR 1.15 (95%CI 0.91, 1.45); p=0.2511

Checkmate026:Conclusionsn
Socinski M, et al. Ann Oncol 2016;27(Suppl 6):abstr LBA7_PR
§ Nivolumab did not meet the primary endpoint of superior PFS compared with chemotherapy
§ Safety results were consistent with the known safety profile of nivolumab; there were fewer treatment-related grade 3–4 AEs in the nivolumab vs. chemotherapy arm
§ OS was similar in the nivolumab and chemotherapy arms and both compared favourably with historical controls§ 60.4% of patients in the chemotherapy arm received
subsequent nivolumab

NewfromAACR2017
• Impact of Tumor Mutation Burden (TMB) on the Efficacy of First-Line Nivolumab in Stage IV or Recurrent Non-Small Cell Lung Cancer: An Exploratory Analysis of CheckMate 026
Petersetal,AACR2017

TMBinCheckmate026
• TMBhasbeenshowntobepredictiveofoutcomesinimmuno-oncology(Rizvietal,Science2015348:124-8)
• Anexploratoryanalysisof026wasdonetotestthehypothesisthathighTMBmightpredictbenefitfromnivolumab vs.chemotherapy
• MatchedtumorandgermlineexomesequenceswereperformedforTMBanalysis
• 312patients(58%ofpopulation)hadmatchedsamplesforanalysis
• TMBin026patientsgenerallysimilardistributiontothatseeninpreviousreportofTCGAPetersetalAACR2017

TMBinCheckmate026
• AnalysisofbaselinecharacteristicsverysimilarinoverallpopulationandTMB-evaluable(TMB-E)population
• OSANDPFSweresimilarineacharmforoverallandTMB-E
• Patientsweredividedintothreesubgroupsbasedonnumbersofmutations(<100,100-242,>243)
PetersetalAACR2017

PFSbyTMBTertile inCheckmate026
50
100
90
80
70
60
50
40
30
20
10
00 3 6 9 12
Months15 18 21 24
PFS(%)
High
Low
Medium
Mediumn=49 n=47
3.6(2.7,6.9)
Lown=62
4.2(1.5,5.6)
9.7(5.1,NR)
MedianPFS,months(95%CI)
High Mediumn=53 n=60
6.5(4.3,8.6)
Lown=41
6.9(5.4,NR)
5.8(4.2,8.5)
MedianPFS,months(95%CI)
High100
90
80
70
60
50
40
30
20
10
00 3 6 9 12
Months15 18
High
Low
Medium
21
Nivolumab Chemotherapy
PetersetalAACR2017

PFSandRRbyTMBSubgroupinCheckmate026
OUTCOME HIGH TMB LOW/MED TMB
Nivolumab Chemotherapy Nivolumab Chemotherapy
PFS(months) 9.7 5.8 4.1 6.9
HR0.62(0.38,1.0) HR1.82(1.3,2.55)
RR 47% 28% 23% 33%
PetersetalAACR2017

OSandTMBinCheckmate026
• OSwasnotimpactedbyTMBsubgroup• HighTMBNivo 18.3vChemo18.8mos (HR1.1)(68%crossovertonivo)
• Low/medTMB12.7v13.2mos (HR0.99)(55%crossovertonivo)
PetersetalAACR2017

TMBinCheckmate026
• Current/formersmokershadhigherTMBthannever-smokers
• TherewasnoassociationbetweenTMBandPD-L1expression
PetersetalAACR2017

ORRbyTMBsubgroupandPD-L1Expression
HighTMB Low/Med TMB
PD-L1>50% 75% 34%
PD-L11-49% 32% 16%
HighTMB Low/Med TMB
PD-L1>50% 25% 46%
PD-L11-49% 32% 23%
Nivolumab Chemotherapy
PetersetalAACR2017

PFSbyTMBandPD-L1in026
55
Months
100
75
50
25
0
6 18930 12 15 21Months
100
75
50
25
0
6 1893
PFS(%)
0 12 15 2421
High TMB, PD-L1 ≥50%
High TMB, PD-L1 1–49%
Low/medium TMB, PD-L1 1–49%
Low/medium TMB, PD-L1 ≥50%
Low/medium TMB, PD-L1 ≥50%
High TMB, PD-L1 1–49%
Low/medium TMB,
PD-L1 1–49%High TMB,
PD-L1 ≥50%
Nivolumab Arm Chemotherapy Arm
PetersetalAACR2017

TMBinCheckmate026--Summary
• Nivolumab improvedRRandPFSvschemotherapyinpatientswithhighTMB
• PFSwaslongerinpatientswithhighTMBregardlessofPD-L1status
• PatientswithhighTMBandPD-L1>50%benefitedthemostfromnivolumab
• Patientswithmed/lowTMBhadgreaterbenefitfromchemotherapy
• Thesesubsetsareexploratoryandnumbersaresmall,sothesefindingsshouldbeviewedcautiouslyPetersetalAACR2017

NeoadjuvantNivolumab
Study Design & Endpoints
NewlydiagnosedresectablestageI
(>2cm)/II/IIIANSCLC
Nivolumab3mg/kgIV
onDay-28&Day-14Surgical
resectiononDay0
Standardofcare
postoperative
treatmentSafety
followupfor30days
aftersurgery
TUMOR BIOPSY
BLOOD DRAWS
VIABLE TUMOR
TILS
LYMPH NODE CELLS
BLOOD DRAW
FordeetalESMO2016

StudyEndpoints
Ø Primary Endpoint: Safety and feasibility
Ø Exploratory Endpoints: Correlatives in blood and tumor, percent pathologic response, RFS, OS
Ø Planned enrollment: 6 patient safety & feasibility run-in followed by expansion to enroll up to 20 resected patients.
FordeetalESMO2016

Treatment-relatedAEs
Ø Treatment-related toxicities were consistent with those seen in other studies of nivolumaband there were no treatment-related deaths
Ø One death occurred during the postoperative safety evaluation period that assessed as unrelated to study treatment Data is based on a Sept 15, 2016 database lock
FordeetalESMO2016

AnalysisofResponse(Exploratory)
Tumor pathologic response after neoadjuvant anti-PD-1 (N=17)
Ø 39% (95% CI 20-61% ) of per protocol patients, 7 of 18, had <10% residual viable tumor at resection
Ø 1 patient had a pathologic complete response
0 10 20 30 40 50 60 70 80 901001
4
7
10
13
16
Percent Pathologic Response
Majorpathologicresponse <10% residual viable
tumor cells defines major pathologic response per Pataeret al. JTO 2012
Resected Tumors
FordeetalESMO2016

NeoadjuvantNivolumab Summary
• Neoadjuvantnivolumab didnotinterferewithsurgeryandtherewerenosurprisingsafetyissues
• 39%ofpatientshadamajorpathologicresponsewithtumorinfiltrationbyimmunecells
• ResponseswereseeninPD-L1positiveandnegativepatients
• Verysmallnumbers;Needconfirmationinlargerstudies
FordeetalESMO2016

WhyIsImmunotherapyComplicated?• UnchangeablehostimmunefactorssuchasHLAtype• Changeablehostimmunefactorssuchaslymphocytesubsetscanbeinfluencedbychemotherapyandothertreatment
• Tumorimmunogenicitycanchangeovertimeandcanbeinfluencedbychemotherapyandothertreatment
• Tumorimmunogenicitymayinherentlyvaryaswell(e.g.EGFRmutatedtumorsinnon-smokerswithlowTMB)
• ConcomitantchemotherapyandImmunotherapymayhavesignificantinteractionsspecifictothedrugsused

What’sNextforImmunotherapyofNSCLC?• Combinationsarealreadybeingevaluated(IOandIO,IOandchemo,IOandantibodies)
• Literallythousandsofpotentialcombinationstobestudied
• Broadclinicaltrialparticipationinthecommunityisvitaltomakingprogress!

“Whenpeoplecomplainofyourcomplexity,theyfailtoremembertheymadefunofyoursimplicity.”
--MichaelBassey Johnson
Recommended