8/22/2016
1
Lung Cancer 101 and ASCO 2016 Highlights Dr. Jennifer Garst with ASCO slides by Dr. Jared Weiss Duke Cancer Institute at Duke Cancer Center Raleigh
8/20/2016
Build Hope. Take Action. End Lung Cancer.
…..To save lives and provide support to those affected by lung cancer through research,
awareness, education, and access programs across North Carolina.
Mission

8/22/2016
2
A Major Public Health Problem
• Estimated 1.6 million deaths each year worldwide from lung cancer
• In 2015:
– Estimated 221,200 new cases of lung cancer expected to be diagnosed in US
– 158,000 Americans expected to die from lung cancer
• Leading cause of cancer-related deaths in US men and women
– More deaths from lung cancer than breast, prostate, colon, liver, melanoma, and kidney cancers combined
• Need for better thought out, patient-driven studies
Torre LA, et al. CA Cancer J Clin. 2015;65(2):87-108.
Siegel RL, et al. CA Cancer J Clin. 2015;65(1):5-29.
USA Distribution

8/22/2016
3
Lung cancer is an uncontrolled growth of abnormal cells that starts in the lungs.
Cancer can develop with a mutation or error in the lung cell’s DNA.
DNA mutations can be caused by the normal aging process and through exposure to toxins
like smoke, viruses, radon, and other environmental factors.
What is lung cancer?
Cigarette Smoke

8/22/2016
4
• Current or past H/O smoking or second hand smoke exposure
• Radon exposure
• Previous cancer
• Lung disease, COPD, pulmonary fibrosis
• Toxic exposures: arsenic, chromium, asbestos, nickel,, cadmium, beryllium, silica, diesel fumes, viruses
• Genetic risks
Lung Cancer Risk Factors
It likely takes a series of mutations to create a lung cancer cell. Cells may be pre-cancerous
due to some mutations but continue to function like normal lung cells. As these cells divide, the mutations are passed down and can become
augmented from other toxic exposures until the cells do not behave like normal lung cells and take on the characteristics or “hallmarks” of
cancer.
What is lung cancer?

8/22/2016
5
Hanahan D, et al. Cell. 2000;100(1):57-70.
Self-sufficiency in growth signals
Evading
apoptosis
Sustained
angiogenesis
Limitless replicative potential
Insensitivity to
antigrowth signals
Tissue invasion
and metastasis
The Hallmarks of Cancer: New Targets
• 228,190 new cases of lung cancer
• 159,480 deaths due to lung cancer
Men
Lung and bronchus 28%
Prostate 10% Colon and rectum 9% Pancreas 6% Leukemia 5%
Women
Lung and bronchus 26%
Breast 14%
Colon and rectum 9%
Pancreas 7%
Ovary 5%
Leading Sites, United States, 2013 Estimates
Siegel R, et al. CA Cancer J Clin. 2013;63(1):11-30.
Cancer-Related Deaths

8/22/2016
6
Common causes of US cancer deaths, 2008
Rudin CM, et al. Clin Cancer Res. 2009;15(18):5622-5625.
Ever-Smokers
Never-Smokers
Types of Lung Cancer
• Non-Small Cell Lung Cancer – Adenocarcinoma
Squamous cell carcinoma
– Large cell
• Small Cell Lung Cancer

8/22/2016
7
NSCLC Stages at Presentation
Subramanian J, et al. J Thorac Oncol. 2010;5: 23–28.
Stage I:
•≤ 5cm; no lymph nodes involved
Stage II:
•≤ 7cm, if ipsilateral hilar lymph nodes involved
•>7cm, or local invasion, or multiple nodules in same lobe if no lymph nodes involved
Staging: NSCLC

8/22/2016
8
Stage III:
•Has not spread beyond lymph nodes in chest
•May have metastases within ipsilateral lung
•May have local invasion of major structures
Stage IV:
•Metastatic disease or disease with pleural effusion
Staging: NSCLC

8/22/2016
9
Less Invasive Lung Cancer Staging
EndoBronchial Ultrasound (EBUS) Mediastinoscopy
Use of an ultrasound-guided camera to biopsy lymph nodes around the airway with needle aspiration
Surgical removal of lymph nodes from around the main airway
ENDOBRONCHIAL ULTRASOUND
EBUS is done under general anesthesia
Angled, balloon-tipped ultrasound bronchoscope allows simultaneous endoscopic and ultrasound views
Endoscopic view
Ultrasound view EBUS probe in the main airway

8/22/2016
10
Current State of NSCLC • NSCLC: ~ 85% of lung cancers
• Histology-directed therapy
– Non-squamous: bevacizumab, pemetrexed
– Squamous: nab-paclitaxel, nivolumab
• Biomarker-directed therapy
– Erlotinib, afatinib, gefitinib, crizotinib, ceritinib
• Immunotherapy
• Overcoming resistance
– EGFR and ALK resistance
More Choices = More Decisions
patients, providers, payers
Strategies to Improve Outcome of Lung Cancer Patients
• Move away from approaching lung cancer as one disease
• Develop treatment strategies for different subsets of lung cancer
• Treatment improvements based on
– Histology
– Oncogenic alterations
– Proteomics

8/22/2016
11
First-line Second-line Third-line Maintenance Not approved
1970 1980 1990 2000
Median OS
(mos)
12+
~ 6 ~ 2–4
BSC Single-agent platinum Doublets Bevacizumab + PC
Carboplatina 1989
Erlotinib Pemetrexed
2004
Docetaxel 1999
Paclitaxel Gemcitabine
1998
Vinorelbine 1994
Docetaxel 2002
Bevacizumab 2006
Gefitinib 2003
Standard Therapies aLabel does not include NSCLC-specific indication. BSC = best supportive care; PC = paclitaxel/carboplatin; OS = overall survival. Adapted from Shrump, et al. Non-small cell lung cancer. In: Cancer: Principles and Practice of Oncology. 7th ed. Philadelphia, PA: Lippincott Williams & Wilkins:2005.
Pemetrexed 2008/2009
Histology-directed therapy
Cisplatina 1978
History of Therapy in Advanced NSCLC: FDA Approval Dates 1970-2010
2010
Erlotinib 2010
~ 8–10
Maintenance Therapy
Targeted Therapy ALK Translocation EGFR Mutation
2011 2013
History of Therapy in Advanced NSCLC: FDA Approval Dates 2011-2013
Crizotinib 2011
Erlotinib 2013
Afatinib 2013
Median OS
(mos)
Targeted Therapy
20-30+ months

8/22/2016
12
Lung Cancer Mutation Consortium: Incidence of Driver Mutations
ROS-1 1%
Kris MG, et al. JAMA. 2014;311:1998-2006.
Lung Adenocarcinoma Mutations
Rudin CM, et al. Clin Cancer Res. 2009;15(18):5646-5661.

8/22/2016
13
MATCH trial
EGFR Signaling
Adapted from Ciardiello F, Tortora G. N Engl J Med. 2008;358:1160-1174.
gefitinib erlotinib

8/22/2016
14
EGFRMUT Disease Progression on an EGFR TKI
Molecular:
• Unknown (other pathways)
• EGFR T790M (exon 20)
• MET amplification
• PIK3CA
• SCLC
Clinical PD appearance:
• Rapid disease PD globally
• Slow growth globally
• Growth in several areas, but not all T790M
~ 40-55%
T790M +
EGFR amp
~ 10%
Other
EGFR mut
1-2%
SCLC w/
PI3K
~ 4%
SCLC
~ 6%
PIK3CA
~ 1-2%
MET amp
~ 5%
BRAF
~ 1%
HER2 Amp
~ 8-13%
EMT
~ 1-2%
Unknown
~ 15-20%
Camidge DR, et al. Nat Rev Clin Oncol. 2014;11(8):473-481.
Osimertinib activity in patients with leptomeningeal disease from non-small cell lung cancer: <br />updated results from the BLOOM study
Presented By James Yang at 2016 ASCO Annual Meeting

8/22/2016
15
Changes in EGFRm DNA copy number in CSF <br />with osimertinib treatment
Presented By James Yang at 2016 ASCO Annual Meeting
Phase I study (BLOOM) of AZD3759, a CNS penetrable EGFR inhibitor, for the treatment of non-small-cell lung cancer (NSCLC) with brain metastasis (BM) and leptomeningeal
metastasis (LM)
Presented By Myung-Ju Ahn at 2016 ASCO Annual Meeting

8/22/2016
16
Third Generation EGFR TKIs
“3rd” Generation N RR* T790M-
RR T790M+
PFS Toxicity
Rociletinib (CO-1686)
256 37% 53% ~ 8.0 mo Hyperglycemia
AZD9291 253 21% 61% ~ 8.2 mo Diarrhea
HM61713 (800 mg)
62 12% (300 mg)
55% NR Dyspnea/rash
EGF816X* 53 60% NR Rash
ASP8273* 47 ~ 33% 61% NR Hyponatremia/ diarrhea
Sequist L, et al. J Clin Oncol. 2015;33(suppl). Abstract 8001; Jänne PA, et al. N Engl J Med. 2015;372(18):1689-
1699; Park K, et al. J Clin Oncol. 2015;33(suppl). Abstract 8084; Tan DS-W, et al. J Clin Oncol. 2015;33(suppl).
Abstract 8013; Goto Y, et al. J Clin Oncol. 2015;33(suppl). Abstract 8014.
Multiple other agents earlier in development *T790M subgroups are very small.
RR, response rate; PFS, progression-free survival.
ALK Fusion Oncogenes and Downstream Signaling
Shaw AT, Solomon B. Clin Cancer Res. 2011;17:2081-2086.

8/22/2016
17
Alectinib versus Crizotinib in ALK Inhibitor Naïve ALK-Positive Non-Small Cell Lung Cancer:<br /> Primary Results from the J-ALEX Study
Presented By Hiroshi Nokihara at 2016 ASCO Annual Meeting
J-ALEX Phase III Study Design
Presented By Hiroshi Nokihara at 2016 ASCO Annual Meeting

8/22/2016
18
Primary Endpoint: PFS by IRF (ITT Population)
Presented By Hiroshi Nokihara at 2016 ASCO Annual Meeting
Brigatinib in Patients With Crizotinib-Refractory ALK+ Non–Small Cell Lung Cancer: First Report of Efficacy and Safety From a Pivotal Randomized Phase 2 Trial (ALTA)
Presented By Dong-Wan Kim at 2016 ASCO Annual Meeting

8/22/2016
19
PFS by Arm
Presented By Dong-Wan Kim at 2016 ASCO Annual Meeting
Survival by Arm
Presented By Dong-Wan Kim at 2016 ASCO Annual Meeting

8/22/2016
20
ROS1 Rearrangement in Lung Cancer
Jänne PA, et al. J Clin Oncol. 2012;30(8):878-879.
Safety and Efficacy of Lorlatinib (PF-06463922) From the Dose Escalation Component of a Study in Patients With Advanced ALK+ or ROS1+ Non-Small-Cell Lung Cancer
Presented By Benjamin Solomon at 2016 ASCO Annual Meeting

8/22/2016
21
Phase I Design and Patient Population <br />of an Ongoing Phase I/II Study
Presented By Benjamin Solomon at 2016 ASCO Annual Meeting
Clinical Activity: <br />Progression-Free Survival in ALK+ Patients
Presented By Benjamin Solomon at 2016 ASCO Annual Meeting

8/22/2016
22
Majority of ROS1 Patients Had a <br />Decrease in Target Lesion Size*
Presented By Benjamin Solomon at 2016 ASCO Annual Meeting
CNS Responses in ALK/ROS1+ Patients<br />with Measurable Disease
Presented By Benjamin Solomon at 2016 ASCO Annual Meeting

8/22/2016
23
Other Drugs That Target ALK and/or ROS-1 • 1st-generation ALK
Crizotinib( plus ROS-1)
• 2nd-generation ALK Inhibitors
‒ Ceritinib (LDK378)( plus ROS-1)
‒ Alectinib (CH5424802)( no ROS-1 activity)
• ALK/EGFR/ROS-1 Inhibitors
‒ Brigatinib (AP26113)(nearing approval process)
Promising Others ALK/ROS-1: Lorlatinib, Ensartinib (X-396) in clinical trials
Resistance: Cabozantinib (FDA approved med thyroid/renal), TPX-0005 (ALK/SRC) in clinical trials
Response of An ROS1+ Patient
Baseline 12 Weeks Crizotinib
Bergethon K, et al. J Clin Oncol. 2012;30(8):863-870.

8/22/2016
24
Antitumor Activity and Safety of Crizotinib <br />in Patients with Advanced MET Exon 14-Altered <br />Non-Small Cell Lung Cancer
Presented By Alexander Drilon at 2016 ASCO Annual Meeting
Slide 11
Presented By Alexander Drilon at 2016 ASCO Annual Meeting

8/22/2016
25
An Open-Label Phase 2 Trial of Dabrafenib in Combination With Trametinib in Patients With Previously Treated BRAF V600E–Mutant Advanced <br />Non-Small Cell Lung Cancer
(BRF113928)
Presented By David Planchard at 2016 ASCO Annual Meeting
Progression-Free Survival
Presented By David Planchard at 2016 ASCO Annual Meeting

8/22/2016
26
Slide 1
Presented By D. Camidge at 2016 ASCO Annual Meeting
Antibody Drug Conjugate: Sacituzumab Govitecan (IMMU-132)
Presented By D. Camidge at 2016 ASCO Annual Meeting

8/22/2016
27
Progression-Free Survival and Overall Survival <br />(8 or 10 mg/kg; median of 3 prior therapies)
Presented By D. Camidge at 2016 ASCO Annual Meeting
Immunotherapy in NSCLC
• Immunotherapy
• Vaccines
• Check-point inhibitors:
• Preliminary evidence of activity with CTLA-4 and chemotherapy
• Preliminary evidence of activity with PD-1 or PD-L1
Lynch TJ, et al. J Clin Oncol. 2012. Genova C, et al. Expert Opin Biol Ther 2012. Brahmer JR et al NEJM
2012, Topalian S et al NEJM 2012

8/22/2016
28

8/22/2016
29
PD-1, PD-L1 Antibodies
Target Agent
PD-1 Nivolumab (BMS-936558)
Pembrolizumab (MK-3475)
Pidilizumab (CT-011)
AMP-224
PD-L1 BMS-936559
Durvalumab (MEDI4736)
Atezolizumab (MPDL-3280A)
Davies M. Cancer Manag Res. 2014;6:63-75; Brahmer JR. J Clin Oncol. 2013;31(8):1021-1028;
Rizvi NA, et al. J Clin Oncol. 2014;32(suppl 15). Abstract 8007;
Brahmer JR, et al. J Clin Oncol. 2014;32(suppl 15). Abstract 8021.
PD-1, programmed death receptor-1; PD-L1, programmed death-ligand 1.
CheckMate 012: Safety and Efficacy of First‐line Nivolumab and Ipilimumab in Advanced NSCLC
Presented By Matthew Hellmann at 2016 ASCO Annual Meeting

8/22/2016
30
Nivolumab Plus Ipilimumab in First-line NSCLC:<br />Summary of Efficacy
Presented By Matthew Hellmann at 2016 ASCO Annual Meeting
Nivolumab Plus Ipilimumab in First-line NSCLC:<br />Efficacy Across All Tumor PD-L1 Expression Levels
Presented By Matthew Hellmann at 2016 ASCO Annual Meeting

8/22/2016
31
• Immune responses are dynamic and evolve.
• A single biomarker may not be the complete answer.
• “Mutational Load” is a very important factor and may be a better predictor of response to a single PD-1 blockade.
• Micro-environment influences responses to PD-1 blockade…....hypoxia, metabolism, genetics.
Immunotherapy Conclusions:

8/22/2016
32
Small cell lung cancer
Safety and efficacy of single agent rovalpituzumab tesirine (SC16LD6.5), a delta-like protein 3 (DLL3)-targeted antibody-drug conjugate (ADC) in recurrent or refractory small cell
lung cancer (SCLC)
Presented By Charles Rudin at 2016 ASCO Annual Meeting

8/22/2016
33
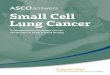
SCLC Kaplan-Meier Overall Survival
Presented By Charles Rudin at 2016 ASCO Annual Meeting
Favorable Comparison vs. Existing 2L and 3L CTX
Presented By Charles Rudin at 2016 ASCO Annual Meeting

8/22/2016
34
Local Consolidative Therapy (LCT) Improves Progression-Free Survival (PFS) in Patients with Oligometastatic Non-Small Cell Lung Cancer (NSCLC) who do not Progress after
Front Line Systemic Therapy (FLST): Results of a Multi-Institutional Phase II Randomized Study
Presented By Daniel Gomez at 2016 ASCO Annual Meeting
Trial Design
Presented By Daniel Gomez at 2016 ASCO Annual Meeting

8/22/2016
35
Trial Design
Presented By Daniel Gomez at 2016 ASCO Annual Meeting
Prognostic Factors for PFS
Presented By Daniel Gomez at 2016 ASCO Annual Meeting

8/22/2016
36
Improved Overall Survival in Lung Cancer Patients <br />using a Webapplication-mediated Follow-up compared to Standard Modalities: <br />Results of a Phase III Randomized
Trial
Presented By Fabrice Denis at 2016 ASCO Annual Meeting
Phase 3 multi-centric randomized study
Presented By Fabrice Denis at 2016 ASCO Annual Meeting

8/22/2016
37
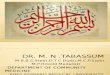
Overall Survival Improvement
Presented By Fabrice Denis at 2016 ASCO Annual Meeting
Other « intensive » clinical follow-up studies
Presented By Fabrice Denis at 2016 ASCO Annual Meeting

8/22/2016
38
Challenges for the Next Decade
• Expanding biomarker-directed therapy
– Transitioning to multiplex testing
– BRAF, Exon 14 MET, HER2
• Defining role of immunotherapy
• Squamous histology-directed therapy
• Small cell lung cancer
• Maintenance ‒ what surrogate can we use?
Figure 6
Source: Cell , Volume 144, Issue 5, Pages 646-674 (DOI:10.1016/j.cell.2011.02.013)
Copyright © 2011 Elsevier Inc. Terms and Conditions

8/22/2016
39
Trends Continuing as Screening for Lung CA Evolves
• Earlier Detection
– NLST Results finding survival benefit with CT screening
• Earlier Diagnosis
– Navigational Bronchoscopy
• More Treatment Options
– Early stage Lung CA improved prognosis, more flexibility with treatment options tailored to patient

8/22/2016
40
Duke Raleigh Hospital Cancer Center Multidisciplinary Lung Cancer Care Team
Standing: Brenda Wilcox , RN; Dr. Jennifer Garst; Lisa Dowd, NP; Dr. Albert Chang Seated: Dr. Catherine Chang, Dr. David White, Katherine Gillis, PA-C
Radiation Fields

8/22/2016
41
Referral: Fast and Appropriate
• Medical oncologists – appropriate for every lung cancer patient
• Thoracic surgeons – role in treatment for all stage patients – Best results from centers that do higher
number of thoracic surgeries

8/22/2016
42
Clinical Trials: The Road to New Therapeutic Advances
• With the advances being made in lung cancer treatment, clinical trials are an attractive therapy option
• The family physician is often the most trusted – your advice carries a lot of weight!
• You don’t need to know that there is a trial available, just plant the seed!
Trends in Management of Lung CA
HOPE
Image Guidance
Less invasive
Better Outcomes
Targeted Therapy
Earlier Detection

8/22/2016
43
• We all need a team of support:
• Family and friends
• Advocacy groups like LCI
• Social media/blogs/ carebridges
• Local medical team
• Consulting medical team
• Spiritual support and more…...
Team HOPE
Our “A” team: Jonathan Choe, PA-C, Vereterrica Rushdan, RMA,
Jennifer Mizelle, RN, Elattmont Spiller, patient care coordinator

8/22/2016
44
Heather Hooper, Executive Director
Thank You to Our Staff!
Lynne Ritter, Director of Finance
Khaki Stelten, Communications & Development Manager
Jenni Danai Programs Manager
Parker Shields Administrative & Program Assistant
Cynamon Frierson, Communication & Marketing Manager
We are very much looking forward to partnering with you in the cause and making lung cancer awareness and
research a priority.
Together, there’s always something we can do!

8/22/2016
45
Recommended