Lung biopsy in Lung biopsy in fibrosing ILDfibrosing ILD
Does it have value?Does it have value?
Athol Wells, Royal Brompton Athol Wells, Royal Brompton HospitalHospital, , London UKLondon UK
Biopsy in “IPF”Biopsy in “IPF”RBH dataRBH data
•1978-1989 n=208 1978-1989 n=208 Biopsy rate = 55%Biopsy rate = 55%
•1992-1997 n=212 1992-1997 n=212 Biopsy rate = 15%Biopsy rate = 15%
Data from 160 ILD cases
• Six expert physicians made diagnoses and Six expert physicians made diagnoses and recommendations on managementrecommendations on management
• Surgical biopsies recommended in 40%Surgical biopsies recommended in 40%
• Poor agreement (k=0.26) on whether to Poor agreement (k=0.26) on whether to biopsy (with and without HRCT data).biopsy (with and without HRCT data).
Aziz Z et al. Radiology 2006; 238:725-33Aziz Z et al. Radiology 2006; 238:725-33
This review will cover……This review will cover……
• Is a histological diagnosis truly a Is a histological diagnosis truly a “reference standard” in DILD?“reference standard” in DILD?
• How physicians should think in DILDHow physicians should think in DILD
• How biopsy fits into the diagnostic How biopsy fits into the diagnostic algorithm: a pragmatic viewalgorithm: a pragmatic view
Diagnosis – four Diagnosis – four viewsviews•Suspend thought: biopsy everything
• Suspend thought: biopsy nothing – call Suspend thought: biopsy nothing – call everything “IIP”everything “IIP”
• Suspend thought: CT is truth dataSuspend thought: CT is truth data
• Do not suspend thoughtDo not suspend thought

Part IPart I
Is biopsy truly a Is biopsy truly a diagnostic gold diagnostic gold
standard?standard?
Biopsy is a gold Biopsy is a gold standard: not!standard: not!
•Severe disease, co-morbiditySevere disease, co-morbidity
•Observer variationObserver variation
•““Sampling error”Sampling error”•Indeterminate appearancesIndeterminate appearances
Biopsy in severe disease
•Risk/benefit ratio marginalRisk/benefit ratio marginal
•Risk increases as gas transfer Risk increases as gas transfer falls below 30-35%falls below 30-35%
•Prognostic value lessens as gas Prognostic value lessens as gas transfer falls below 30-35%%transfer falls below 30-35%%
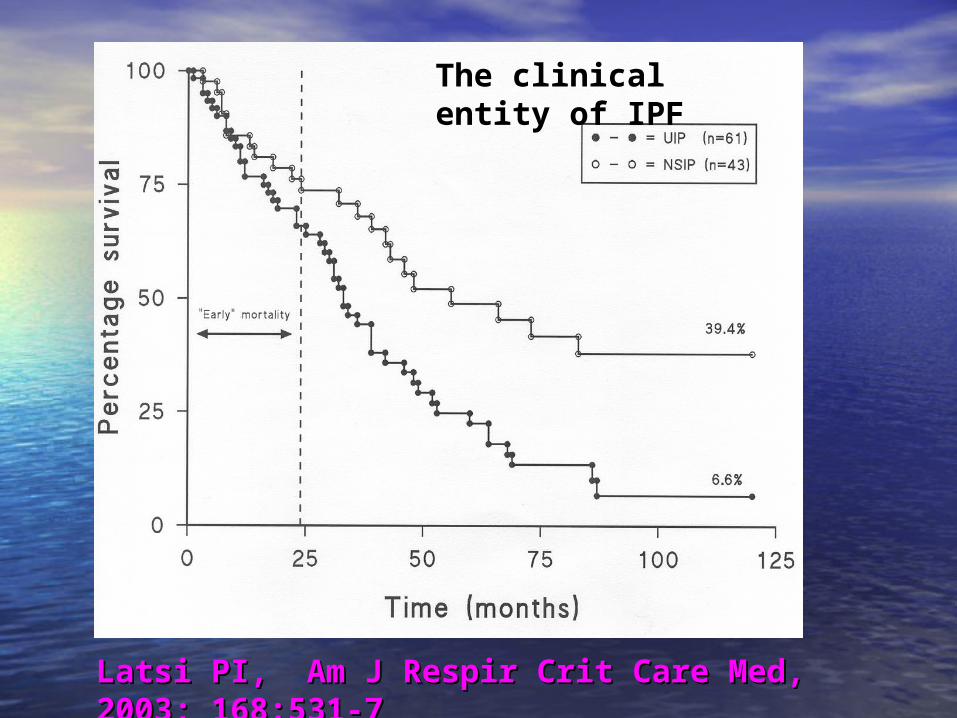
The clinical entity of IPF
Latsi PI, Am J Respir Crit Care Med, 2003; 168:531-7Latsi PI, Am J Respir Crit Care Med, 2003; 168:531-7
Diagnostic variation Diagnostic variation between pathologistsbetween pathologists
•Stated in recent publicationsStated in recent publications
•Historically, a curious paucity Historically, a curious paucity of studies in DILDof studies in DILD
•This may reflect the “iconic This may reflect the “iconic status” of biopsystatus” of biopsy
Inter-observer Inter-observer agreement: agreement: 10 regional UK 10 regional UK
pathologistspathologists
• First choice diagnosis k = 0.38First choice diagnosis k = 0.38
• Confident diagnosis: k = 0.50Confident diagnosis: k = 0.50
• Non-confident diagnosis: k = 0.22Non-confident diagnosis: k = 0.22
• These pathologists were experienced!These pathologists were experienced!
Nicholson AG. Thorax 2004; 59:500-5Nicholson AG. Thorax 2004; 59:500-5
Sampling errorSampling error
• Heterogeneity between biopsiesHeterogeneity between biopsies
• IPF/NSIP cases with two biopsies: IPF/NSIP cases with two biopsies: 50% concordant UIP; 25% 50% concordant UIP; 25% concordant NSIP; 25% discordant concordant NSIP; 25% discordant
• Discordant cases: outcome of IPFDiscordant cases: outcome of IPF
Flaherty KR. Am J Respir Crit Care Med, 2001; 164:1722-27Flaherty KR. Am J Respir Crit Care Med, 2001; 164:1722-27
Sampling error is less of an issue than one might think
Just two comments………Just two comments………
Do not biopsy the tip of Do not biopsy the tip of the middle lobe/lingula the middle lobe/lingula without good reasonwithout good reason
Appearances are often Appearances are often end-stage and non-end-stage and non-specificspecific
•Take two (or more) Take two (or more) biopsies when possiblebiopsies when possible
•Use HRCT to select sites Use HRCT to select sites to sample the full to sample the full morphologic spectrummorphologic spectrum
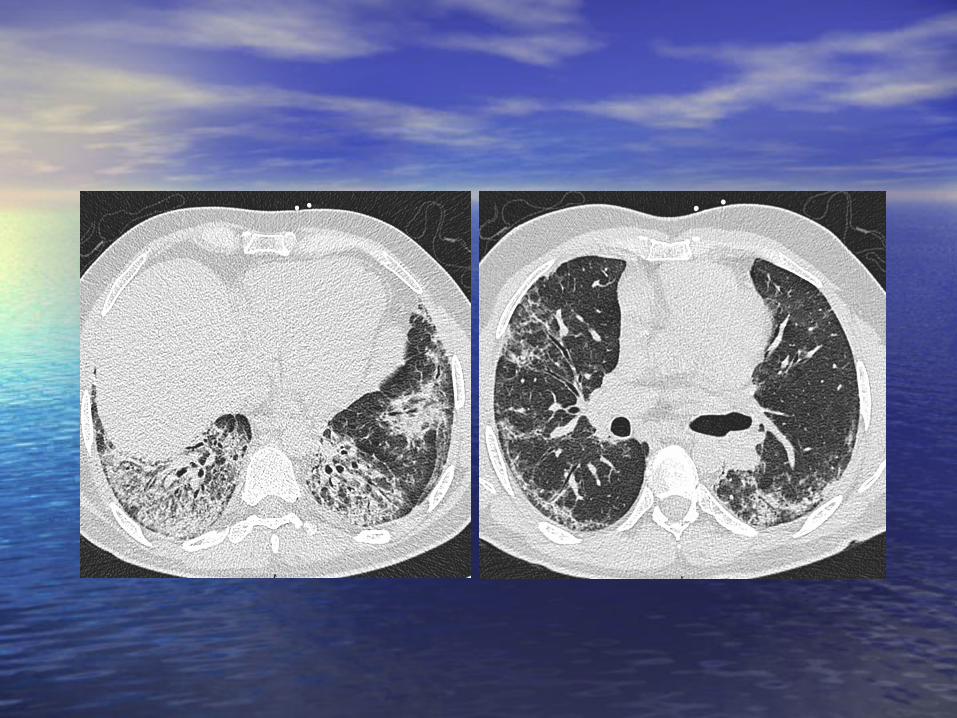
133 biopsies from 82 patients with DILD
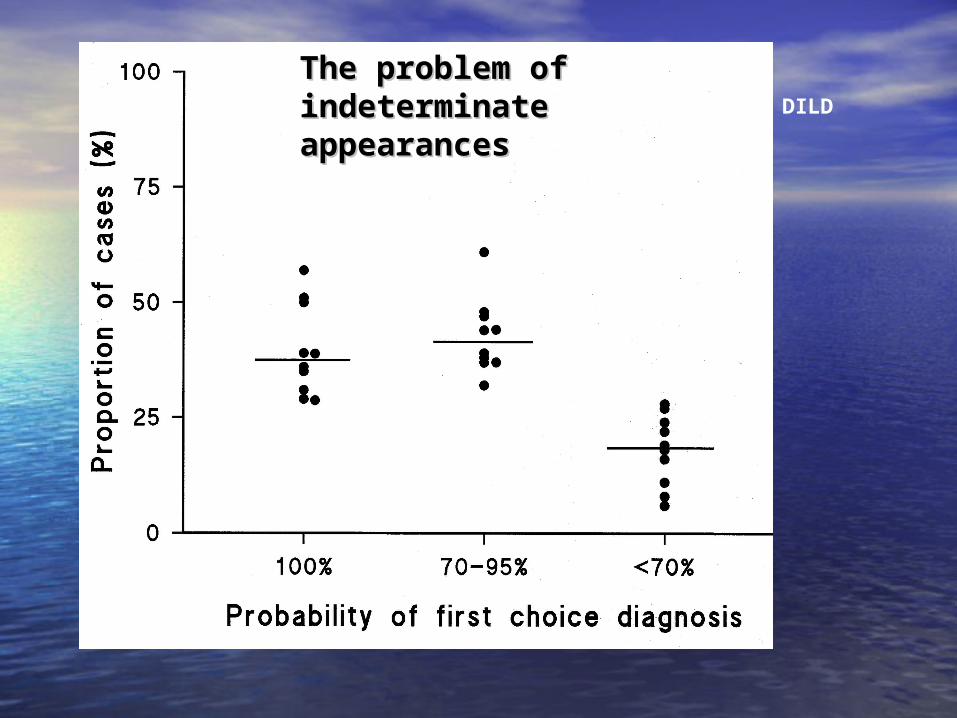
The problem of indeterminate The problem of indeterminate appearancesappearances
For all these reasons, biopsy is no longer a “gold standard”
The diagnostic process in DILD is The diagnostic process in DILD is now more like the Indian fable of now more like the Indian fable of the five blind men and the the five blind men and the elephantelephant
IIP: multidisciplinary diagnosis
• Suspected IIP (n=58) undergoing biopsySuspected IIP (n=58) undergoing biopsy
• Leading clinicians/radiologists/pathologistsLeading clinicians/radiologists/pathologists
• Final consensus diagnosisFinal consensus diagnosis
• Key analysis: clinical/ HRCT diagnosis vs Key analysis: clinical/ HRCT diagnosis vs final diagnosis (with histology integrated).final diagnosis (with histology integrated).
Flaherty KR et al. Am J Respir Crit Care Med 2004; 170:904-910
Multidisciplinary diagnosis
• When pre-biopsy diagnosis IPF, final diagnosis When pre-biopsy diagnosis IPF, final diagnosis virtually always IPFvirtually always IPF
• When pre-biopsy diagnosis not IPF, diagnosis When pre-biopsy diagnosis not IPF, diagnosis changed with biopsy in 50%changed with biopsy in 50%
• Biopsy diagnosis changed 25% of the timeBiopsy diagnosis changed 25% of the time
When the HRCT and clinical When the HRCT and clinical picture are typical of IPF…..picture are typical of IPF…..
• In three good and large studies, a biopsy In three good and large studies, a biopsy virtually never changed the diagnosisvirtually never changed the diagnosis
• The positive predictive value for a pattern The positive predictive value for a pattern of UIP is over 95%, just on HRCT aloneof UIP is over 95%, just on HRCT alone
DO NOT BIOPSY PATIENTS IN THIS CONTEXT
There is no “diagnostic gold standard” in DILD
Clinical, HRCT and histological evaluation are all “silver standards” with biopsy the most argentiferous.
Biopsy is Biopsy is sometimes sometimes invaluable in DILD invaluable in DILD ……… but when?……… but when?
To answer this, we must To answer this, we must understand….understand….
Part IIPart II
How do clinicians How do clinicians actually think in actually think in
diffuse lung diffuse lung disease?disease?
Guidelines for ILD Guidelines for ILD …….…….
““Just one side, please”Just one side, please”
Actually, it ought to be Actually, it ought to be possible to distil the possible to distil the logic of what we do on logic of what we do on just one sidejust one side
But there are difficultiesBut there are difficulties
Major difficulties in Major difficulties in ILDILD
• Multiplicity of disorders – but just a Multiplicity of disorders – but just a few management strategiesfew management strategies
• The terminologyThe terminology
• Problem of patients who do not fit Problem of patients who do not fit exactly into a syndrome: diseases do exactly into a syndrome: diseases do not read medical text-booksnot read medical text-books

Bronchiolitic disordersBronchiolitic disorders
Constrictive bronchiolitis … follicular Constrictive bronchiolitis … follicular bronchiolitis … proliferative bronchiolitis … bronchiolitis … proliferative bronchiolitis … obliterative bronchiolitis … bronchiolitis obliterative bronchiolitis … bronchiolitis obliterans organizing pneumonia … obliterans organizing pneumonia … constrictive obliterative bronchiolitis … constrictive obliterative bronchiolitis … diffuse pan-bronchiolitis … cryptogenic diffuse pan-bronchiolitis … cryptogenic organizing pneumonia … follicular organizing pneumonia … follicular obliterative bronchiolitis ….exudative obliterative bronchiolitis ….exudative bronchiolitisbronchiolitis

BronchiolitisBronchiolitis1 Obliterative bronchiolitisObliterative bronchiolitis (constrictive (constrictive
bronchiolitis, constrictive obliterative bronchiolitis, constrictive obliterative bronchiolitis)bronchiolitis)
2 Cryptogenic organizing pneumoniaCryptogenic organizing pneumonia (bronchiolitis obliterans organizing pneumonia, (bronchiolitis obliterans organizing pneumonia, proliferative bronchiolitis)proliferative bronchiolitis)
3 Follicular bronchiolitisFollicular bronchiolitis
(follicular obliterative bronchiolitis)(follicular obliterative bronchiolitis)
4 Diffuse pan-bronchiolitisDiffuse pan-bronchiolitis (exudative bronchiolitis)(exudative bronchiolitis)
Classification ……Classification ……
• We have histological, radiological, We have histological, radiological, aetiological and other classificationsaetiological and other classifications
• We need as clinicians a simple “what are We need as clinicians a simple “what are you going to do about it?” classification.you going to do about it?” classification.
• Guidelines on just one side – how should we Guidelines on just one side – how should we use multi-disciplinary assessment in use multi-disciplinary assessment in management?management?

Remember why we Remember why we want diagnoseswant diagnoses
•Differences in natural historyDifferences in natural history
•Differences in treatmentDifferences in treatment
•Differences in treated outcomeDifferences in treated outcome
There are a handful of There are a handful of management strategiesmanagement strategies
We need an approach that is We need an approach that is geared to their selectiongeared to their selection
1.1. Observation aloneObservation alone
2.2. Short term steroid trialShort term steroid trial
3.3. Long-term “civilised” regimensLong-term “civilised” regimens
4.4. High dose therapy followed by 3High dose therapy followed by 3
Plus ancillary treatmentsPlus ancillary treatments
Pharmacologic strategiesPharmacologic strategies

A classification based A classification based on pragmatic on pragmatic management ...management ...
• CauseCause
• Predominant morphologic Predominant morphologic abnormalityabnormality
• SeveritySeverity
• Longitudinal behaviourLongitudinal behaviour
IntegrateIntegrate these as follows these as follows
Treatment/monitoring strategies Treatment/monitoring strategies according to:according to:
• Self-limited inflammationSelf-limited inflammation
• Stable fibrotic diseaseStable fibrotic disease
• Major inflammation with variable Major inflammation with variable fibrosisfibrosis
• Inexorably progressive fibrosisInexorably progressive fibrosis
• Severe, rapidly progressive ILDSevere, rapidly progressive ILD
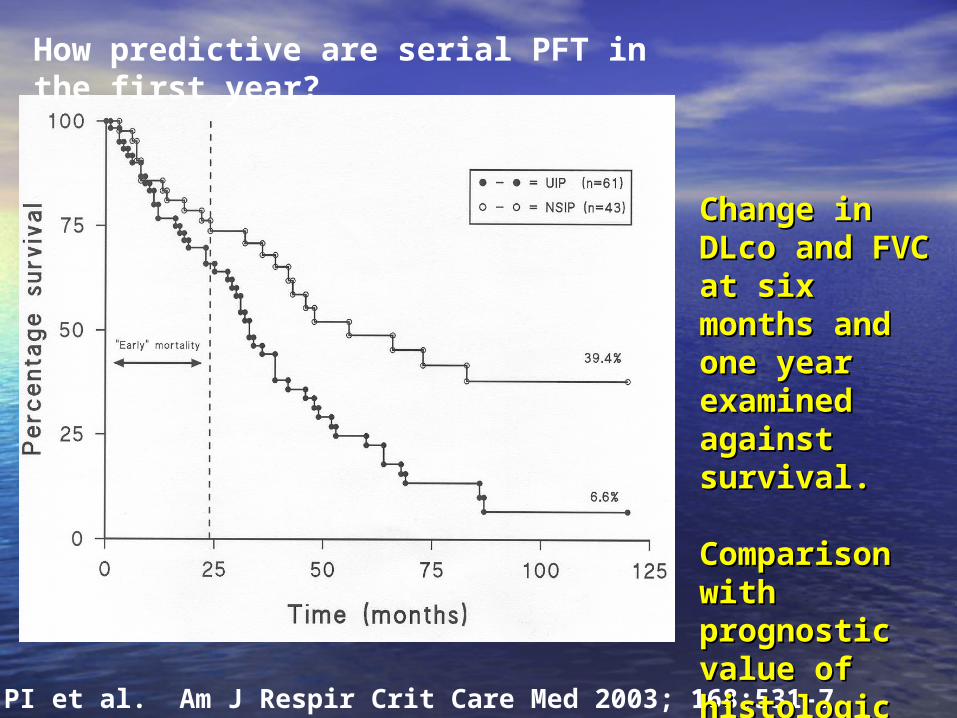
How predictive are serial PFT in the first year?
Latsi PI et al. Am J Respir Crit Care Med 2003; 168:531-7
Change in DLco Change in DLco and FVC at six and FVC at six months and one months and one year examined year examined against survival.against survival.
Comparison with Comparison with prognostic value prognostic value of histologic of histologic diagnosisdiagnosis
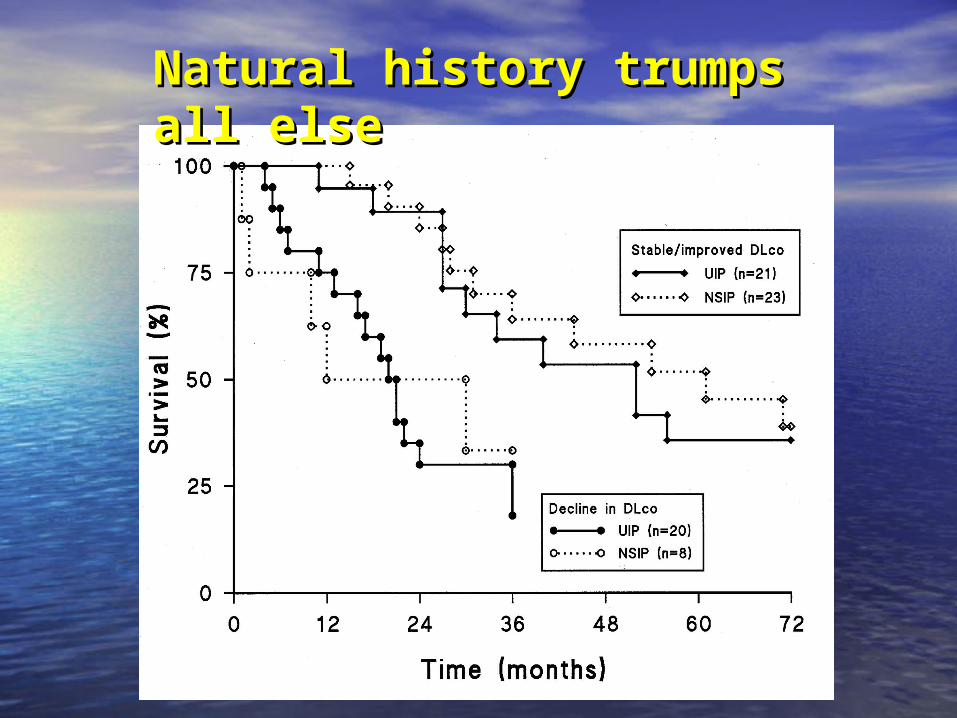
Natural history trumps all elseNatural history trumps all else
Self-limited Self-limited inflammationinflammation• Examples found in HP, sarcoidosis, Examples found in HP, sarcoidosis,
some forms of IIPsome forms of IIP, drug-induced , drug-induced disease …….disease …….
• Outcome goodOutcome good
• Remove the cause Remove the cause
• Not all patients need treatmentNot all patients need treatment
• Monitor to confirm regression of Monitor to confirm regression of diseasedisease
1.1. Observation aloneObservation alone
2.2. Short term steroid trialShort term steroid trial
3.3. Long-term “civilised” regimensLong-term “civilised” regimens
4.4. High dose therapy followed by 3High dose therapy followed by 3
Plus ancillary treatmentsPlus ancillary treatments
Pharmacologic strategiesPharmacologic strategies
Stable/indolent fibrotic Stable/indolent fibrotic diseasedisease
• Examples found in HP, sarcoidosis, Examples found in HP, sarcoidosis, some forms of IIPsome forms of IIP, drug-induced , drug-induced disease….disease….
• Often seen in connective tissue diseaseOften seen in connective tissue disease
• Key is not to over-react: MICO Key is not to over-react: MICO therapy…...therapy…...
““Indolent disease”Indolent disease”
MICO: MICO: Masterful Inactivity Masterful Inactivity with Cat-like Observation with Cat-like Observation
The role of the doctor is to amuse The role of the doctor is to amuse the patient while nature takes its the patient while nature takes its coursecourse
(Voltaire)(Voltaire)
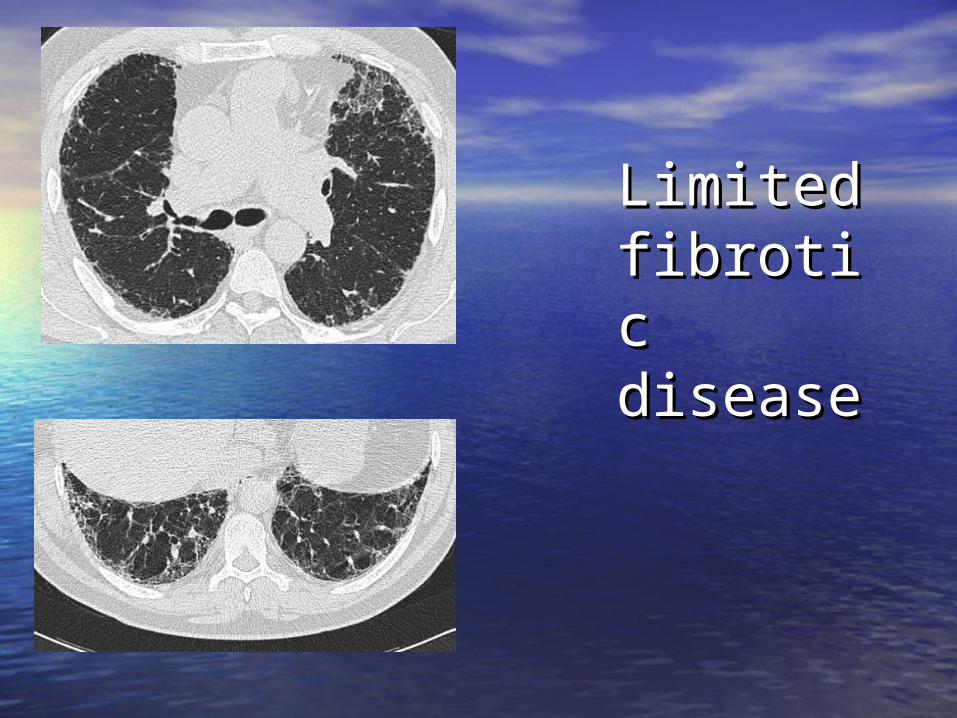
Limited Limited fibrotic fibrotic diseasedisease
100
80
60
40
20
00 20 40 60 80 100 120
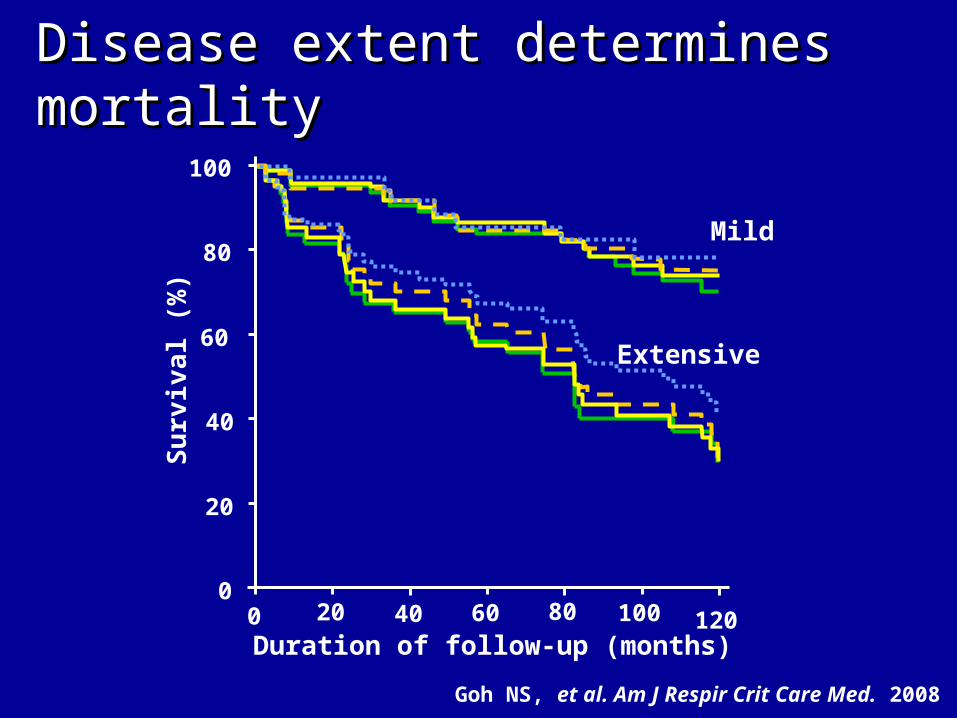
Mild
Duration of follow-up (months)
Extensive
Su
rviv
al (%
)
Disease extent determines Disease extent determines mortalitymortality
Goh NS, et al. Am J Respir Crit Care Med. 2008
1.1. Observation aloneObservation alone
2.2. Short term steroid trialShort term steroid trial
3.3. Long-term “civilised” regimensLong-term “civilised” regimens
4.4. High dose therapy followed by 3High dose therapy followed by 3
Plus ancillary treatmentsPlus ancillary treatments
Pharmacologic strategiesPharmacologic strategies
Major inflammation Major inflammation with variable fibrosiswith variable fibrosis
• Examples in HP, sarcoidosis, Examples in HP, sarcoidosis, some some forms of IIPforms of IIP, drug-induced disease……, drug-induced disease……
• Treat vigourously, reverse any Treat vigourously, reverse any reversible component, then consolidatereversible component, then consolidate
• Monitor initial response and then Monitor initial response and then demonstrate stabilitydemonstrate stability
1.1. Observation aloneObservation alone
2.2. Short term steroid trialShort term steroid trial
3.3. Long-term “civilised” regimensLong-term “civilised” regimens
4.4. High dose therapy followed by 3High dose therapy followed by 3
Plus ancillary treatmentsPlus ancillary treatments
Pharmacologic strategiesPharmacologic strategies
Inexorably progressive Inexorably progressive fibrosisfibrosis• HP, sarcoidosis, HP, sarcoidosis, some forms of IIPsome forms of IIP
• Key to management is to find the right Key to management is to find the right balance between slowing progression balance between slowing progression and poisoning the patientand poisoning the patient
• Thus, crucial to identify any reversible Thus, crucial to identify any reversible component ……….component ……….
1.1. Observation aloneObservation alone
2.2. Short term steroid trialShort term steroid trial
3.3. Long-term “civilised” regimens, Long-term “civilised” regimens, applied with realismapplied with realism
4.4. High dose therapy followed by 3High dose therapy followed by 3
Plus ancillary treatmentsPlus ancillary treatments
Pharmacologic strategiesPharmacologic strategies

Severe, rapidly progressive Severe, rapidly progressive ILDILD
• Some patients with IIPSome patients with IIP, drug-induced , drug-induced disease, simulation of diffuse lung disease, simulation of diffuse lung disease by other disordersdisease by other disorders
• Policy of “treat the treatable”Policy of “treat the treatable”
• Pulsed therapy: IV Methyl Prednisolone Pulsed therapy: IV Methyl Prednisolone versus IV Cyclophosphamideversus IV Cyclophosphamide
1.1. Observation aloneObservation alone
2.2. Short term steroid trialShort term steroid trial
3.3. Long-term “civilised” regimensLong-term “civilised” regimens
4.4. Ultra high dose therapy, then 3Ultra high dose therapy, then 3
Plus ancillary treatmentsPlus ancillary treatments
Pharmacologic strategiesPharmacologic strategies
What clinicians need What clinicians need from a classification….from a classification….
• Captures clusters of disease behaviourCaptures clusters of disease behaviour
• Articulates logical therapeutic goalsArticulates logical therapeutic goals
• Makes approach to monitoring obviousMakes approach to monitoring obvious
Treatment/monitoring strategies Treatment/monitoring strategies according to:according to:
• Self-limited inflammationSelf-limited inflammation
• Stable fibrotic diseaseStable fibrotic disease
• Major inflammation with variable Major inflammation with variable fibrosisfibrosis
• Inexorably progressive fibrosisInexorably progressive fibrosis
• Severe, rapidly progressive ILDSevere, rapidly progressive ILD
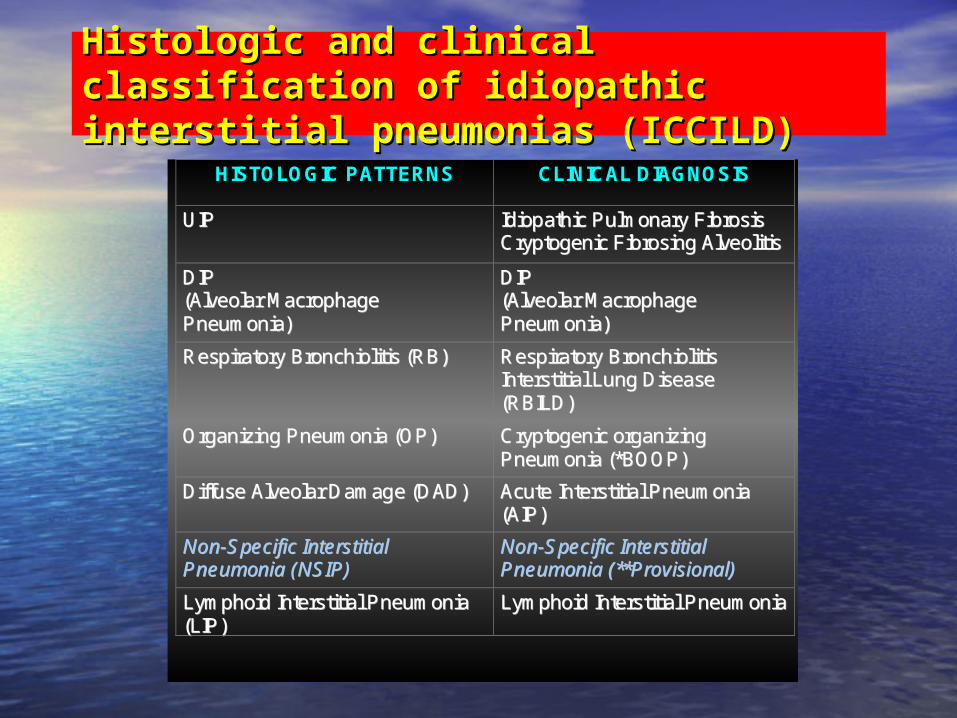
Histologic and clinical classification of Histologic and clinical classification of idiopathic interstitial pneumonias (ICCILD)idiopathic interstitial pneumonias (ICCILD)
HISTOLOGIC PATTERNS CLINICAL DIAGNOSIS
UUIIPP IIddiiooppaatthhiicc PPuullmmoonnaarryy FFiibbrroossiiss CCrryyppttooggeenniicc FFiibbrroossiinngg AAllvveeoolliittiiss
DDIIPP ((AAllvveeoollaarr MMaaccrroopphhaaggee PPnneeuummoonniiaa))
DDIIPP ((AAllvveeoollaarr MMaaccrroopphhaaggee PPnneeuummoonniiaa))
RReessppiirraattoorryy BBrroonncchhiioolliittiiss ((RRBB)) RReessppiirraattoorryy BBrroonncchhiioolliittiiss IInntteerrssttiittiiaall LLuunngg DDiisseeaassee ((RRBBIILLDD))
OOrrggaanniizziinngg PPnneeuummoonniiaa ((OOPP)) CCrryyppttooggeenniicc oorrggaanniizziinngg PPnneeuummoonniiaa ((**BBOOOOPP))
DDiiffffuussee AAllvveeoollaarr DDaammaaggee ((DDAADD)) AAccuuttee IInntteerrssttiittiiaall PPnneeuummoonniiaa ((AAIIPP))
NNoonn--SSppeecciiffiicc IInntteerrssttiittiiaall PPnneeuummoonniiaa ((NNSSIIPP))
NNoonn--SSppeecciiffiicc IInntteerrssttiittiiaall PPnneeuummoonniiaa ((****PPrroovviissiioonnaall))
LLyymmpphhooiidd IInntteerrssttiittiiaall PPnneeuummoonniiaa ((LLIIPP))
LLyymmpphhooiidd IInntteerrssttiittiiaall PPnneeuummoonniiaa
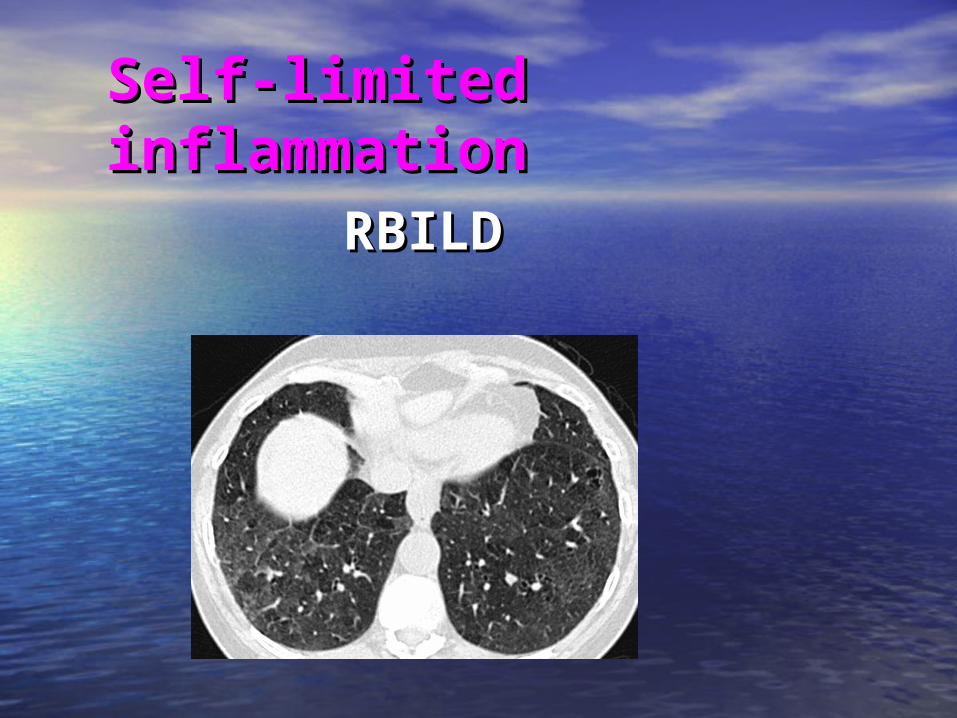
Self-limited Self-limited inflammationinflammation
RBILDRBILD
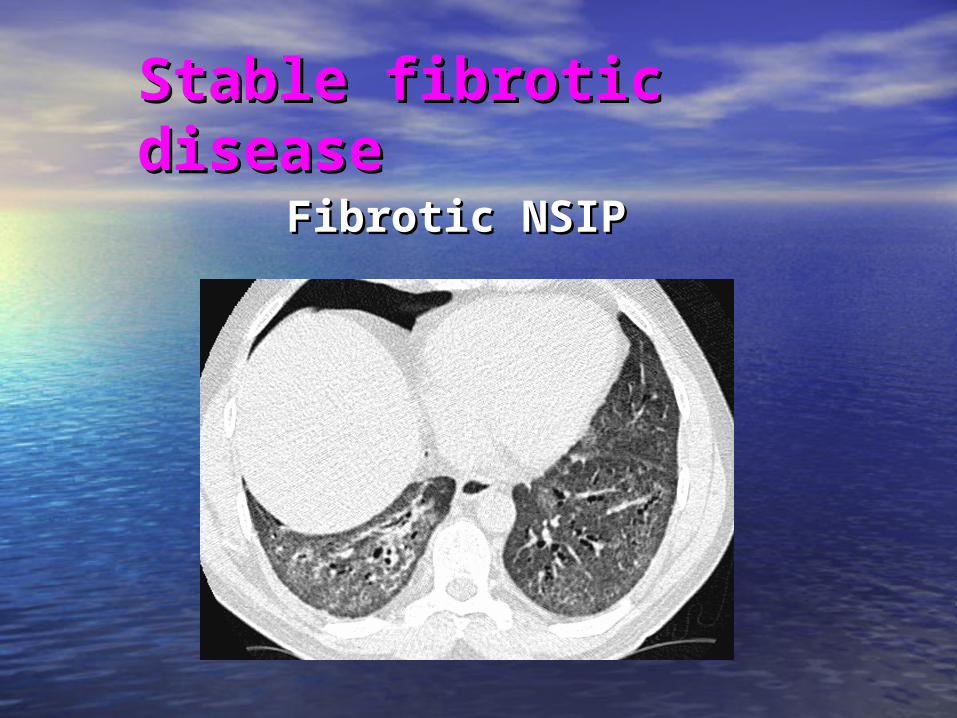
Stable fibrotic Stable fibrotic diseasedisease
Fibrotic NSIPFibrotic NSIP
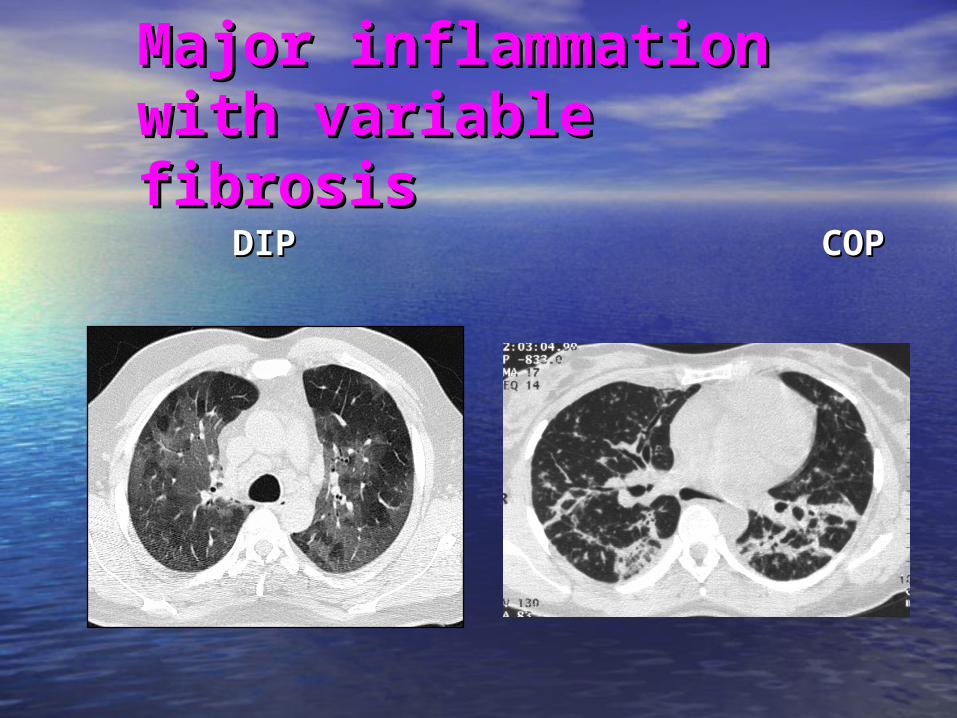
Major inflammation Major inflammation with variable fibrosiswith variable fibrosis
DIP COPDIP COP
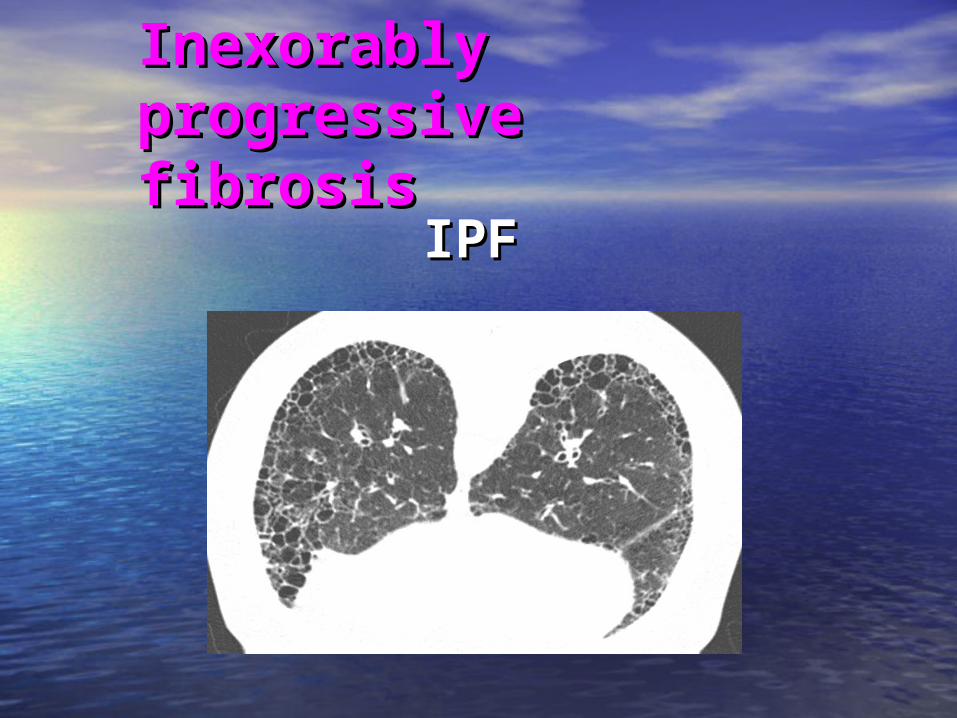
Inexorably Inexorably progressive fibrosisprogressive fibrosis
IPFIPF
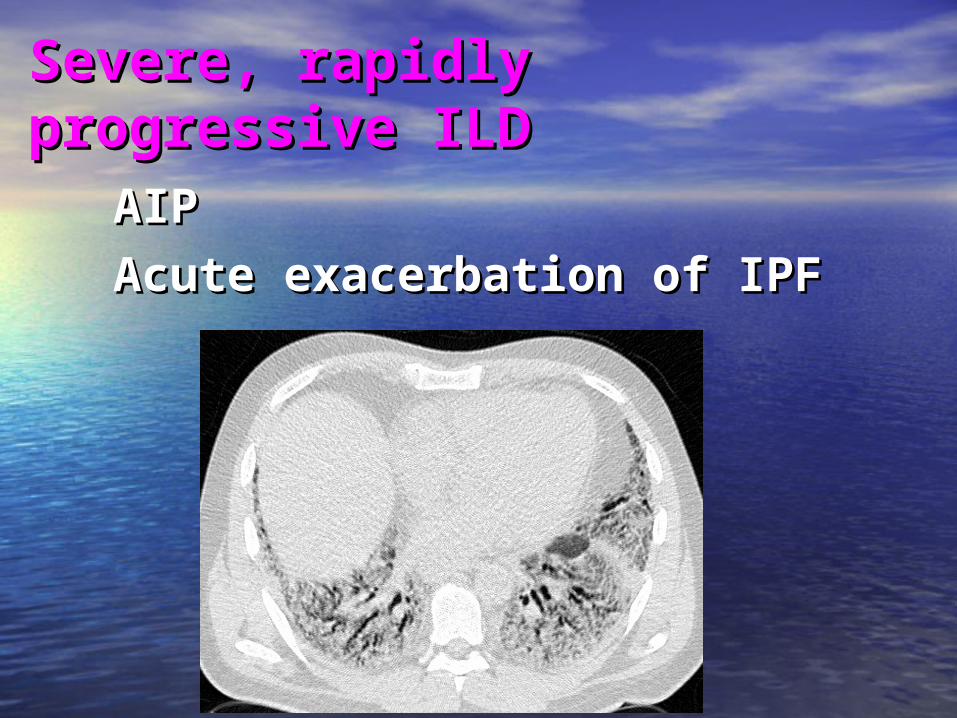
Severe, rapidly progressive Severe, rapidly progressive ILDILD
AIP AIP Acute exacerbation of IPFAcute exacerbation of IPF
Part III
Where does biopsy fit into this?
Treatment/monitoring strategies Treatment/monitoring strategies according to:according to:
• Self-limited inflammationSelf-limited inflammation
• Stable fibrotic diseaseStable fibrotic disease
• Major inflammation with variable Major inflammation with variable fibrosisfibrosis
• Inexorably progressive fibrosisInexorably progressive fibrosis
• Severe, rapidly progressive ILDSevere, rapidly progressive ILD
We investigate in We investigate in order to make these order to make these essential distinctionsessential distinctions
BiopsyBiopsy• The classification informs biopsy The classification informs biopsy
decisions by sharpening risk/benefit decisions by sharpening risk/benefit evaluationevaluation
• It does NOT replace biopsy: system works It does NOT replace biopsy: system works best when the diagnosis is securebest when the diagnosis is secure
• Biopsy decisions themselves need to be Biopsy decisions themselves need to be multidisciplinarymultidisciplinary
The risk/benefit equation
• Physicians can articulate to patients Physicians can articulate to patients exactly why a biopsy is being performedexactly why a biopsy is being performed
• The benefit of the procedure can be The benefit of the procedure can be balanced against the risksbalanced against the risks
• Patients can participate in decision-Patients can participate in decision-makingmaking
Biopsy data informs Biopsy data informs us what patterns of us what patterns of disease behaviour are disease behaviour are possiblepossible
In cases in which we In cases in which we already know this, biopsy is already know this, biopsy is redundantredundant
Selected scenarios: the Selected scenarios: the integration of diagnostic integration of diagnostic datadata
• Pathognomonic HRCT findings: Pathognomonic HRCT findings: biopsy biopsy not requirednot required … IPF … IPF
• Diagnosis and future disease behaviour secure Diagnosis and future disease behaviour secure when HRCT and clinical information combined: when HRCT and clinical information combined: biopsy not required…… RBILDbiopsy not required…… RBILD
• Diagnosis and future disease behaviour Diagnosis and future disease behaviour uncertain after full non-invasive evaluation: uncertain after full non-invasive evaluation: biopsy required unless contraindicatedbiopsy required unless contraindicated
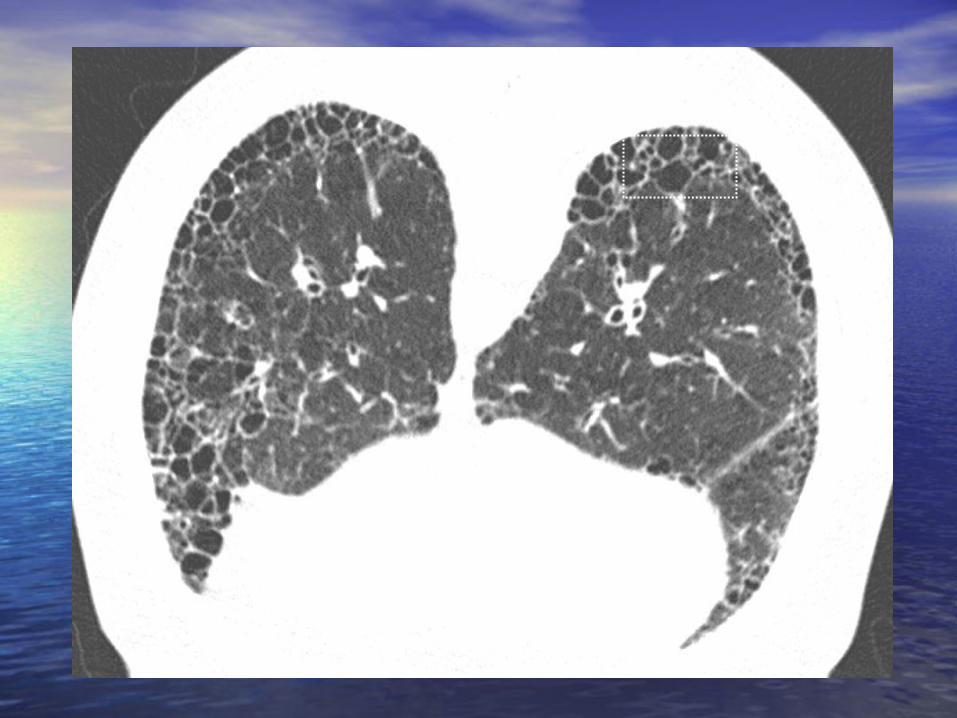
IPF/usual interstitial IPF/usual interstitial pneumoniapneumonia
• Very characteristic HRCT profileVery characteristic HRCT profile
• Now formally incorporated in ATS/ERS Now formally incorporated in ATS/ERS non-invasive diagnostic criterianon-invasive diagnostic criteria
• Cardinal features: predominantly basal Cardinal features: predominantly basal sub-pleural disease; honeycombing; sub-pleural disease; honeycombing; little (or no) ground-glass attenuationlittle (or no) ground-glass attenuation
Raghu G. Chest 1999; 116:1168-Raghu G. Chest 1999; 116:1168-7474
• 59 biopsied patients with new-onset 59 biopsied patients with new-onset ILDILD
• IPF, n=29. Many other disorders, but IPF, n=29. Many other disorders, but fibrotic NSIP not represented fibrotic NSIP not represented
• PPV for IPF, clinicians = 95%PPV for IPF, clinicians = 95%
• PPV for IPF, radiologists = 88% PPV for IPF, radiologists = 88%
Hunninghake GW et al. Am J Respir Hunninghake GW et al. Am J Respir Crit Care Med 2001; 15:193-196Crit Care Med 2001; 15:193-196
• 91 biopsied patients “with suspected IPF”91 biopsied patients “with suspected IPF”
• IPF, n = 54. Mixture of other disorders, IPF, n = 54. Mixture of other disorders, including NSIP (n=6)including NSIP (n=6)
• When diagnosis confident…...When diagnosis confident…... PPV for IPF, core pulmonologists = 87%PPV for IPF, core pulmonologists = 87% PPV for IPF, core radiologists PPV for IPF, core radiologists = 96%= 96% !! !!
Biopsy adds Biopsy adds NO value in NO value in typical IPFtypical IPF
Selected scenarios: the Selected scenarios: the integration of diagnostic integration of diagnostic datadata
• Pathognomonic clinical or HRCT findings: Pathognomonic clinical or HRCT findings: biopsy not requiredbiopsy not required … IPF … IPF
• Diagnosis and disease behaviour secure Diagnosis and disease behaviour secure when HRCT and clinical information when HRCT and clinical information combined: combined: biopsy not required… RBILDbiopsy not required… RBILD
• Diagnosis and future disease behaviour Diagnosis and future disease behaviour uncertain after full non-invasive evaluation: uncertain after full non-invasive evaluation: biopsy required unless contraindicatedbiopsy required unless contraindicated

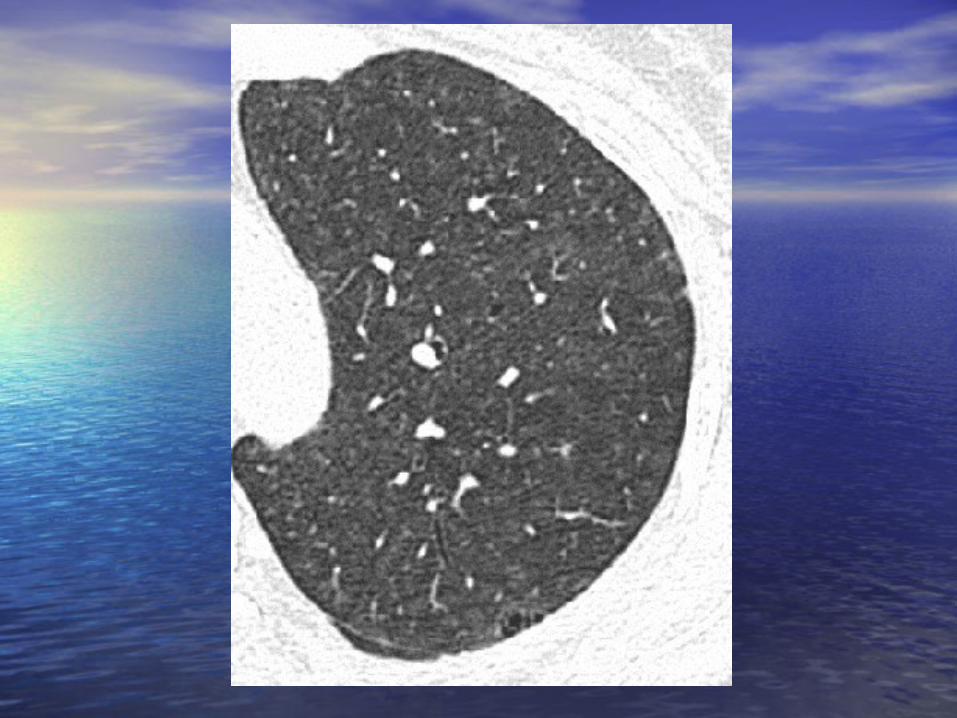
RBILDRBILD
• Exaggerated form of smoking-related Exaggerated form of smoking-related respiratory bronchiolitisrespiratory bronchiolitis
• Generally benign/self limited although Generally benign/self limited although symptoms/functional impairment may symptoms/functional impairment may be significantbe significant
• Is biopsy diagnostically necessary?Is biopsy diagnostically necessary?
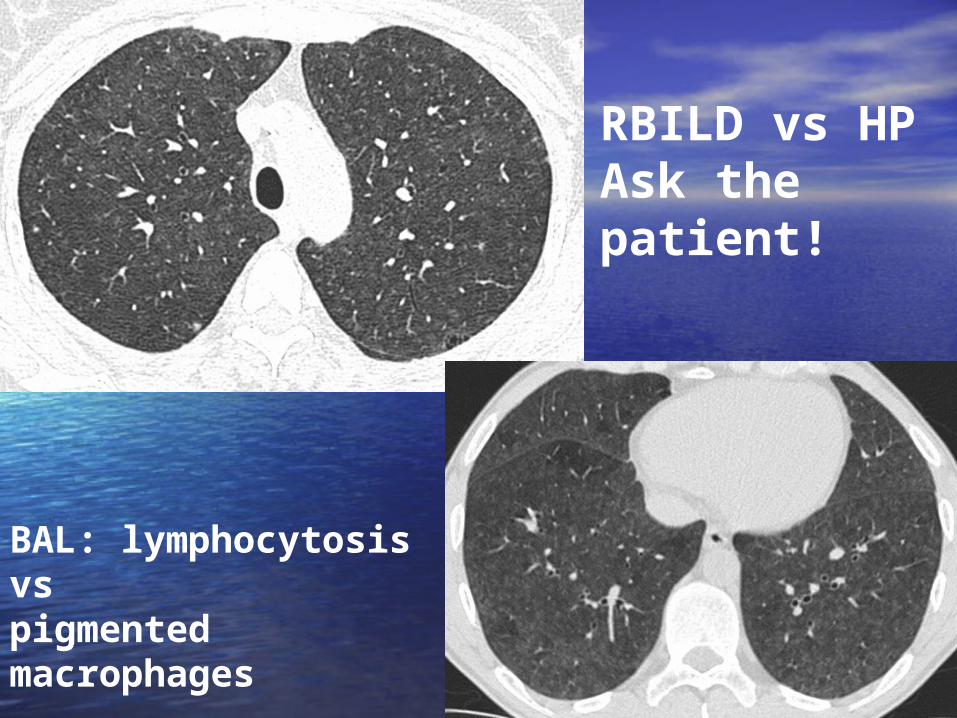
RBILD vs HPAsk the patient!
BAL: lymphocytosis vs pigmented macrophages
If CT and clinical If CT and clinical information are information are conclusive when conclusive when integrated … integrated … biopsy adds NO biopsy adds NO valuevalue
Selected scenarios: the Selected scenarios: the integration of diagnostic integration of diagnostic datadata
• Pathognomonic clinical or HRCT findings: Pathognomonic clinical or HRCT findings: biopsy not requiredbiopsy not required … IPF … IPF
• Diagnosis and future disease behaviour secure Diagnosis and future disease behaviour secure when HRCT and clinical information combined: when HRCT and clinical information combined: biopsy not required…… RBILDbiopsy not required…… RBILD
• Diagnosis and disease behaviour Diagnosis and disease behaviour uncertain after non-invasive evaluation: uncertain after non-invasive evaluation: biopsy required unless contraindicatedbiopsy required unless contraindicated
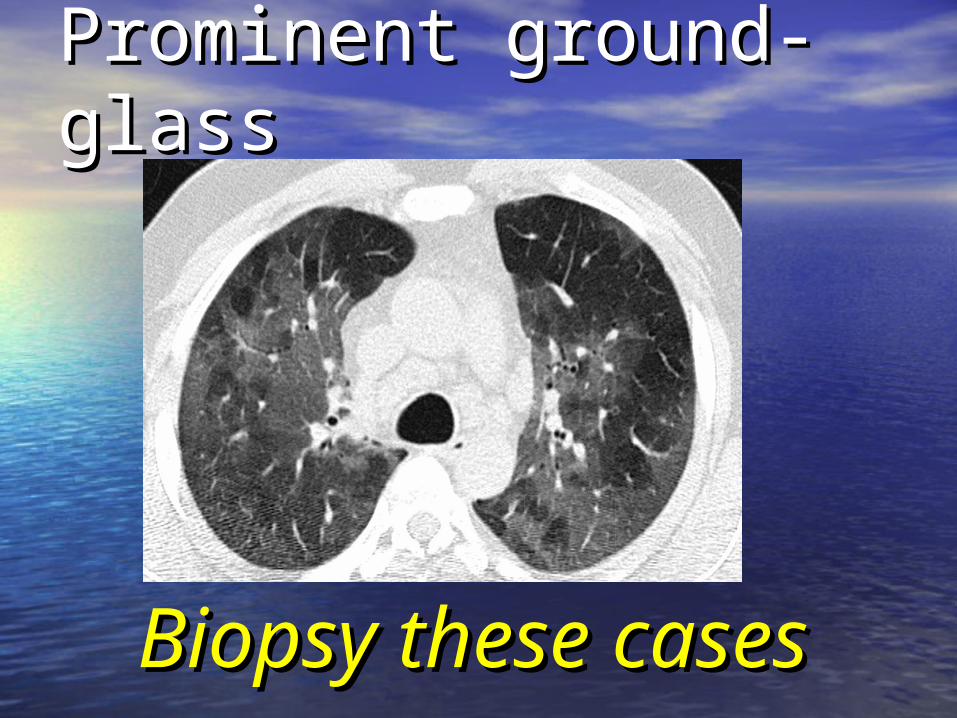
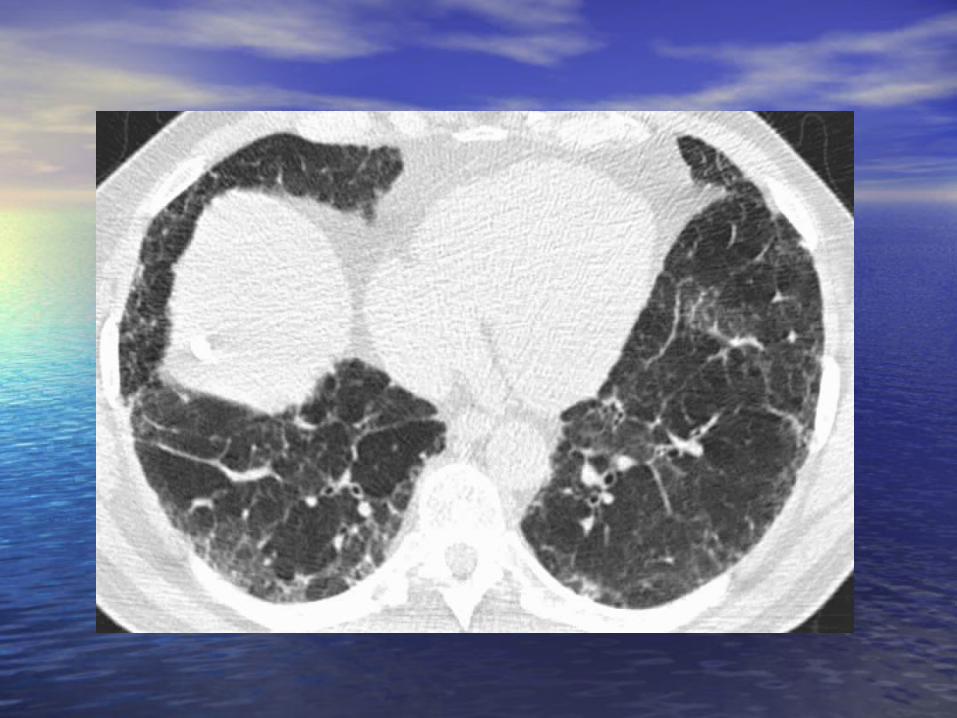
Prominent ground-Prominent ground-glassglass
Biopsy these Biopsy these casescases
HRCT in the diagnosis HRCT in the diagnosis of IPF: the caveatof IPF: the caveat
• Raghu: 20% atypical on HRCTRaghu: 20% atypical on HRCT
• Hunninghake: 20-25% atypical on HRCTHunninghake: 20-25% atypical on HRCT
If appearances are typical, an If appearances are typical, an HRCT diagnosis of IPF is almost HRCT diagnosis of IPF is almost always correctalways correct
The converse is NOT correctThe converse is NOT correct
Atypical appearances Atypical appearances do NOT exclude IPFdo NOT exclude IPF
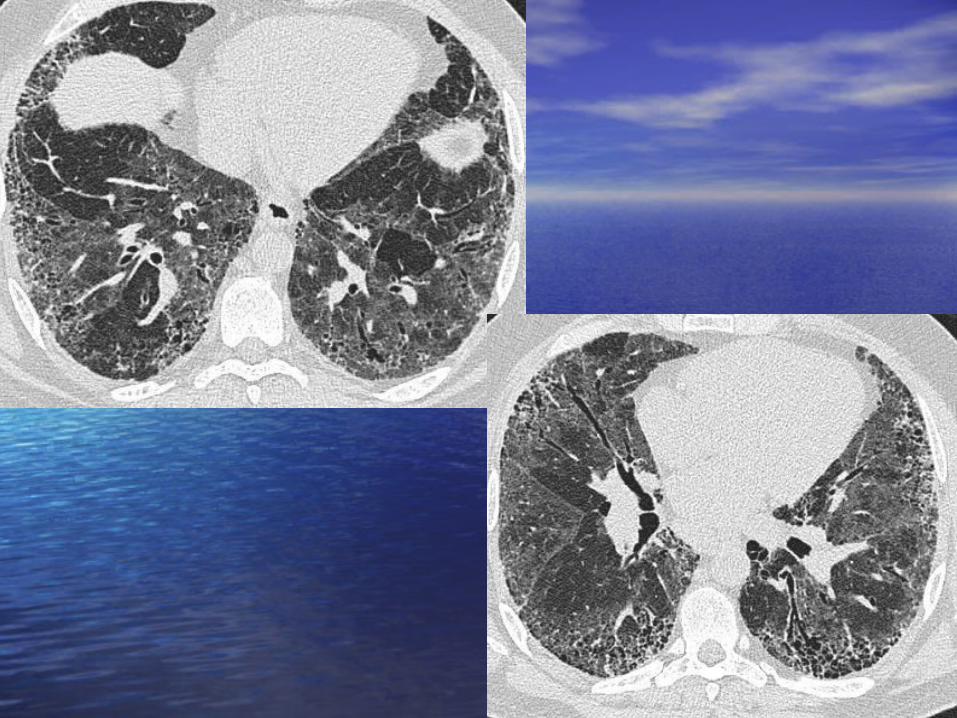
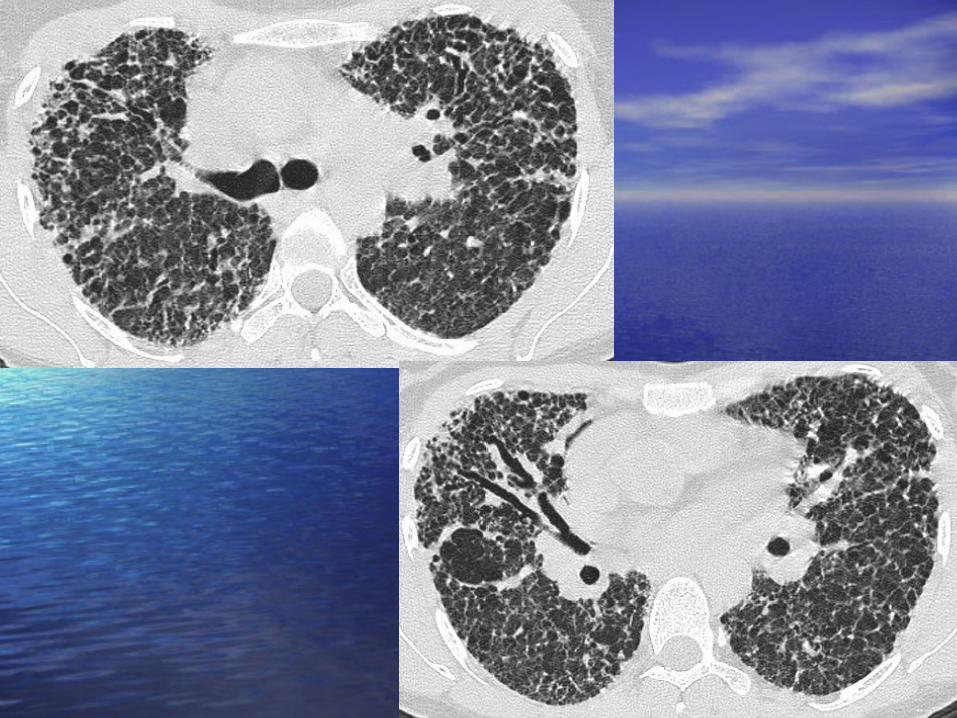
When disease is overtly When disease is overtly progressive despite progressive despite therapy and cannot be therapy and cannot be readily categorised on readily categorised on HRCT, HRCT, always suspect always suspect atypical IPF.atypical IPF.
Biopsy these Biopsy these casescases
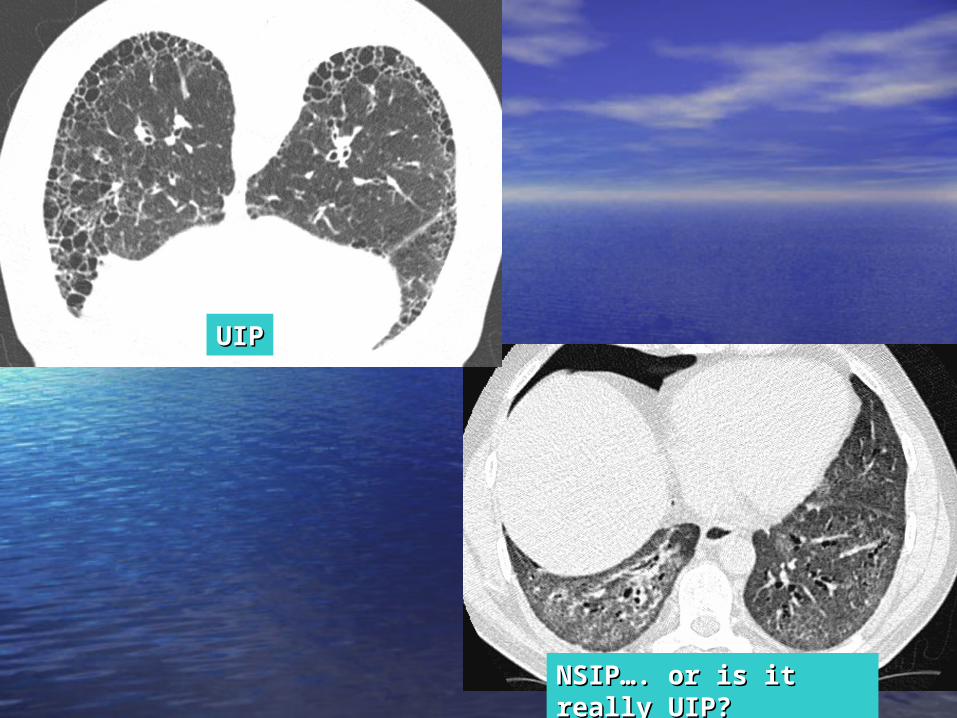
NSIP…. or is it really UIP?NSIP…. or is it really UIP?
UIPUIP
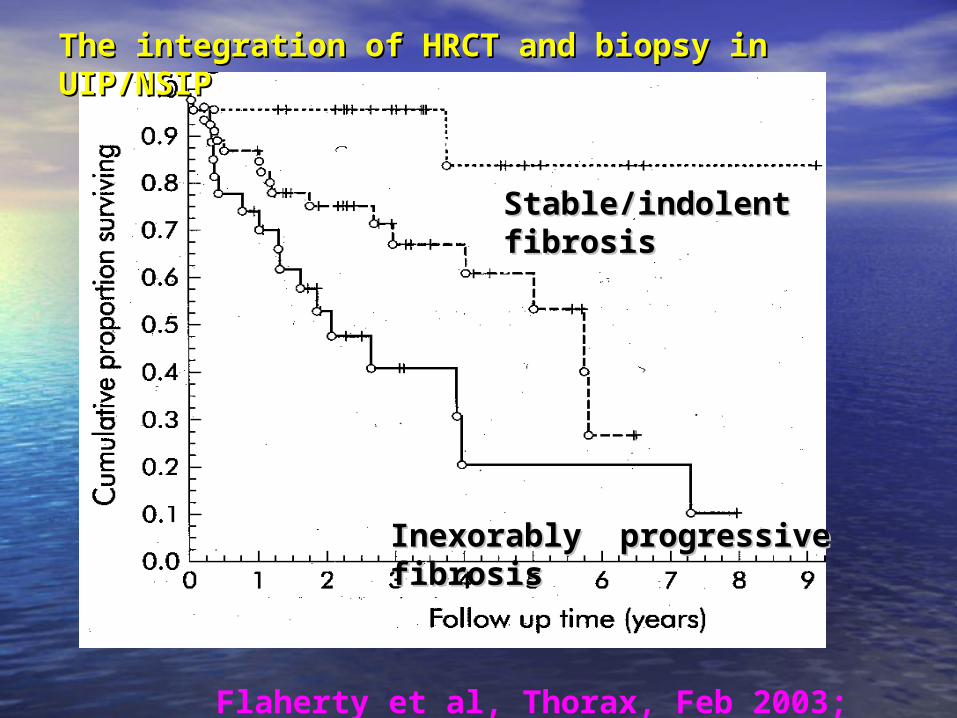
The integration of HRCT and biopsy in UIP/NSIPThe integration of HRCT and biopsy in UIP/NSIP
Flaherty et al, Thorax, Feb 2003; 58:143-8
Biopsy, CT = NSIP
Biopsy = UIP, CT = NSIP
Biopsy, CT = UIP
Stable/indolent fibrosisStable/indolent fibrosis
Inexorably progressive fibrosisInexorably progressive fibrosis
In these scenarios, In these scenarios, biopsy informs our key biopsy informs our key goals goals To prevent major inflammation To prevent major inflammation
(with variable fibrosis) (with variable fibrosis) evolving into progressive evolving into progressive fibrosisfibrosis
To convert inexorably To convert inexorably progressive fibrotic disease progressive fibrotic disease into stable fibrotic diseaseinto stable fibrotic disease
Both these goals are Both these goals are realistic in disorders other realistic in disorders other than IPFthan IPF
Only the second goal Only the second goal applies to IPF and it is not applies to IPF and it is not yet realistic in this diseaseyet realistic in this disease

Biopsy data mayBiopsy data may allow allow full participation by full participation by patients in patients in treatment decisionstreatment decisions
Biopsy data may make Biopsy data may make the logic of the logic of management management transparent, transparent, immediately immediately understoodunderstood by by physicians outside the physicians outside the specialityspeciality
SummarySummary
• Biopsy is no longer a “gold standard”Biopsy is no longer a “gold standard”
• Biopsy has a crucial role when it is Biopsy has a crucial role when it is not possible to broadly predict not possible to broadly predict disease behaviour non-invasivelydisease behaviour non-invasively
• Risk/benefit evaluation is pivotalRisk/benefit evaluation is pivotal
When the decision When the decision to biopsy is a close to biopsy is a close call, the views of the call, the views of the patient should swing patient should swing the decisionthe decision
Recommended