Longitudinal study of caries development from childhood to adolescenceAuthorsMs E. Hall-Scullin1, Consultant in Dental Public Health, NHS Ayrshire & Arran.Miss H. Whitehead2, Dental Professional Lead, Community Dental Service, Salford Royal NHS Foundation Trust.Prof K. Milsom3, Consultant in Dental Public Health, Department of Dental Public Health, Countess of Chester Hospital.Prof M. Tickle4, Professor of Dental Public Health and Primary Care, Division of Dentistry, University of Manchester.Dr T-L Su, Lecturer in Statistics, Division of Dentistry, University of ManchesterDr T. Walsh4, Reader in Biostatistics, Division of Dentistry, University of Manchester.
Address1Public Health Department, NHS Ayrshire & Arran, Afton House, Ailsa Hospital Campus, Dalmellington Road, Ayr, KA6 6AB, UK. 2Community Dental Service, Salford Royal NHS Foundation Trust, Pendleton Gateway, 1 Broadwalk, Salford, M6 5FX, UK. 3Department of Dental Public Health, 1829 Building, Countess of Chester Hospital, Chester, CH2 1UL, UK. 4Division of Dentistry, Faculty of Biology, Medicine and Health, University of Manchester, Oxford Road, Manchester, M13 9PL, UK.
Email Emma Hall-Scullin [email protected] Hilary Whitehead [email protected] Ting-Li Su [email protected] Milsom [email protected] Martin Tickle [email protected] Tanya Walsh [email protected]
Key words (from list provided)Child dentistry, Dental Public health, pediatric dentistry, prevention
Please provide one sentence that describes your article.
Adds to the literature on the longitudinal behaviour (incidence and prevalence) of dental caries in adolescence to inform oral health strategies.
Abstract word count 296 words tbc
Total word count 2882 words tbc
1

Total number of tables/figures 4 tbc
Number of references 18
Abstract
Introduction: The World Health Organization (WHO) has concluded that
globally, dental caries is the most important oral condition. To develop
effective prevention strategies requires an understanding of how this condition
develops and progresses over time, but there are few longitudinal studies of
caries onset and progression in children. Methods: The aim of the study was
to establish the pattern of caries development from childhood into
adolescence and to explore the role of potential risk factors (age, gender,
ethnicity and social deprivation). Of particular interest was the disease
trajectory of dentinal caries in the permanent teeth in groups defined by the
presence or absence of dentinal caries in the primary teeth. Intra-oral
examinations to assess oral health were performed at four time points by
trained and calibrated dentist examiners using a standardized, national
diagnostic protocol. Results: Clinical data were available from 6651 children.
Mean caries prevalence (% D3MFT>0) was 16.7% at the first clinical
examination (ages 7 to 9) increasing to 31.0%, 42.2% and 45.7% at
subsequent examinations. A population-averaged model (generalized
estimating equations) was used to model the longitudinal data. Estimated
mean values indicated a rising D3MFT count as pupils aged (consistent with
new teeth emerging) which was significantly higher (4.49 times, 95% CI 3.90
to 5.16) in those pupils with caries in their primary dentition than in those
without. Conclusion: This study is one of the few large longitudinal studies to
report the development of dental caries from childhood into adolescence.
Children who developed caries in their primary dentition had a very different
caries trajectory in their permanent dentition compared to their caries free
contemporaries. In light of these results, caries free and caries active children
should be considered as two separate populations, suggesting different
prevention strategies are required to address their different risk profiles.
2

Introduction Dental caries was confirmed by the WHO global review on oral health as the
single most important oral condition world-wide (Petersen et al. 2005).
Although caries prevalence is falling in many western countries, the disease
still affects a significant proportion of children. In the United States, NHANES
(2011-2012) reported that over 50% of children aged 6-18 years presented
with caries (Dye et al. 2015). In England, the Children’s Dental Health Survey
(2013) (Pitts et al. 2015) reported 40% of children aged 8 years had caries in
the primary teeth and 10% had caries in their permanent teeth. At age 12
years, prevalence of caries in the permanent teeth had increased to 26% and
to 39% in 15-year-olds. Oral health disparities by ethnicity (Dye et al. 2015)
and deprivation (Pitts et al. 2015) are well established and can persist
throughout the life course (Poulton et al. 2002). The consequences of caries
for children includes pain, swelling, problems eating and communicating,
impact on quality of life; and costs to society related to time off school;
reduced productivity and resources needed to treat the condition
(Casamassimo et al. 2009; Cunnion et al. 2010; Petersen 2005).
To develop effective prevention strategies requires an understanding of how
caries develops and progresses over time, but there have been few, large
longitudinal cohort studies completed in children. Traditionally, observational
caries studies have been cross-sectional in design, which can be suggestive
of risk factors for disease, but are limited in terms of establishing relationships
between exposure and outcome over time. In particular, there have been few
longitudinal cohort studies bridging the transitional period between childhood
and adolescence. This is an important period in the life course in terms of
dental development, with the emergence of the permanent teeth, and social
development as children become more independent.
The primary aim of this study was to describe the prevalence and incidence of
caries in the permanent teeth in a cohort of children over a seven-year period,
with a view to establishing the pattern of caries development. The secondary
aim was to explore the role of potential risk factors (age, gender, ethnicity and
social deprivation) associated with caries. The disease trajectory of the
3

groups defined by the presence or absence of caries (into dentine) in the
primary teeth as a risk factor for caries (into dentine) in the permanent teeth
was of particular interest.
4

Materials and MethodsThis study aimed to clinically examine and follow up all school Year 3 and 4
pupils (aged 7 to 9) who attended any of the 207 state-funded primary schools
in East Lancashire in the North-West of England in February 2006. The
location was chosen for its comparatively high caries prevalence and the
absence of a fluoridated water program (Dental Observatory 2001; 2006). The
study was accepted for inclusion on the NIHR UK Clinical Research Network
Study Portfolio (Ref: 10315) and granted ethical approval by the National
Research Ethics Service (Ref: 11/NE/0006). The study is a human
observational study and conformed to the STROBE guidelines.
Following the invitation to participate, consent was obtained initially at the
school level, followed by parental and child consent. There were four waves of
data collection in the study, bridging the primary and secondary school
systems. Study consent was taken for waves one and two. For waves three
and four consent was separated into consent for a questionnaire of self-
reported risk factors and consent to the intra-oral clinical examination. For the
purpose of this study, only clinical examination data were analyzed. After the
first baseline clinical examination (CE1) at 7-9 years of age, three more
follow-up examinations were conducted when the same cohort reached mean
ages of 11 (CE2), 13 (CE3) and 15 (CE4) years. CE1 and CE2 were carried
out in primary schools; CE3 and CE4 were carried out in secondary (high)
schools.
Schools with less than 10 children in the age group under study were
excluded. All pupils registered in consenting schools in the age group under
study were invited to participate. Throughout the study we followed current
National Health Service guidance on consenting children for observational
studies (Rooney et al. 2010). Before each clinical examination, parents and
potential participants were sent Participant Information Sheets explaining the
study and consent process. In primary schools, participants who did not opt-
out and presented for examination were considered to have provided consent.
In secondary schools, while participants could opt-out, those who presented
were asked to give informed consent.
5

The school provided each pupil’s date of birth, gender and home postcode.
The postcode (geographic area with approximately 15 households) was used
to link to a small area measure of socio-economic position; the Index of
Material Deprivation quintiles 2010 (IMDQ) (IMD, 2010) (Mukund 2011; NPEU
2013). The Index of Multiple Deprivation, commonly known as the IMD, is the
official measure of relative deprivation for small geographical areas in
England. It combines information from seven domains including income,
employment, crime and health. It can be used to rank every small area in
England in quintiles from IMDQ1 (least deprived areas) to IMDQ5 (most
deprived areas). Ethnicity was reported by the parent according to nationally
agreed categories (white, Asian, black, Chinese, Mixed or other) (BASCD
2009). The first recorded gender; ethnicity and home postcode data were
used in the analyses.
At each clinical examination, caries was assessed using a UK national
diagnostic protocol by trained and calibrated dentist examiners (BASCD 2009;
Pine et al. 1997). A dentist recognized nationally as a “gold standard”
provided training and acted as the standard for calibration. The diagnostic
threshold for caries was visual assessment only of frank cavitation into
dentine (d3, D3). Calibration ranges were sensitivity 1.00 to 0.82 and specificity
1.00 to 0.99. Reproducibility for clinical caries scores was assessed using the
Kappa statistic with a re-examination of 10% of participants. Intra-examiner
Kappa was above 0.81 at each time point.
Data were analyzed with STATA 14. A descriptive analysis of pupils’ socio-
demographic characteristics (age, gender, ethnicity and social deprivation)
was carried. The characteristics of consenting and non-consenting pupils
were compared to assess representitivity of the pupils under study and the
potential impact of loss to follow-up.
The number of decayed (d/D), missing (m/M) and filled (f/F) teeth was
summed to calculate individual whole mouth d3mft values for primary and
D3MFT values for permanent dentition separately. D3MFT was recorded for
6

each individual at all four time points and d3mft was recorded for CE1 and
CE2 only. Using these two summary scores separately, each pupil was further
categorized into caries free (d3mft=0, D3MFT=0) and caries active (d3mft>0,
D3MFT>0) groups in order to calculate caries prevalence (percentage of
pupils caries active) and for subgroup analysis.
Caries incidence in the permanent dentition was explored using a population-
averaged (marginal) model with covariates of age, gender, deprivation,
ethnicity and caries absence or presence in the primary dentition. A negative
binomial regression using generalized estimating equations with mean
dispersion variance, unstructured correlation structure, and Huber White
sandwich estimator for standard errors was proposed as a suitable model to
accommodate the over-dispersion and longitudinal nature of the D3MFT count
data. A number of different models were investigated (See Appendix ‘Model
selection’ and Appendix Figure 2). Model fit was assessed through the visual
inspection of residuals, values of information criteria and deviance.
7

ResultsAt CE1 and CE2, 92% (190/207) of primary schools agreed to participate in
the study: Seven schools declined, three were due to close and seven had
fewer than ten pupils in the eligible age-group (See Figure 1). At CE3, 75%
(27/36) of secondary schools and at CE4 67% (24/36) of secondary schools
agreed to participate in the study. One school had closed and the remainder
cited concerns about disruption to academic activities as reasons for declining
to participate.
Figure 1 Study flowchart
The number of pupils providing study consent and consent to intra-oral
examination (CE3 and CE4 only) is summarized in Figure 1. At CE1: 518
pupils were absent from school on the day of examination or had left the
school before the clinical examination and therefore consent could not be
sought; 5470 of 5649 pupils who were present on the day of examination
consented (96.8%) and 179 withheld consent (118 parents and 61 pupils). At
CE2: 908 pupils were absent from school on the day of examination or had
left the school before the clinical examination; 5476 of 5618 pupils (97.5%)
and 142 withheld consent (83 parents and 59 children).
At CE3: 437 pupils were absent from school on the day of examination; 3443
of 3777 pupils (91.2%) consented to the study, with 69 parents and 265
children withholding consent; 3036 (80.4%) consented to the intra-oral exam,
with 69 parents and 672 children withholding consent for this aspect of the
study. At CE4: 756 pupils were absent from school on the day of examination;
3190 of 3295 pupils (96.8%) consented to the study, with 24 parents and 81
children withholding consent; 2733 (82.9%) consented to the intra-oral exam,
with 24 parents and 538 children withholding consent.
The socio-demographic profile of participants is shown in the Appendix Table
1. Due to the small numbers of pupils in some of the ethnic categories the
8

sparsely populated categories of Black (0.18%), Chinese (0.11%), Mixed or
other (0.99%) were combined with the Asian category (22.8%) to form a
binary variable of White (75.9%) and Asian or other (reference category)
(24.1%). A significant number of participants were from more deprived
backgrounds with over 60% of pupils from IMD quintiles 4 and 5.
The socio-demographic characteristics of consenting pupils were similar to
non-consenting pupils (Appendix Table 2). Mean age in years was very
similar for the consented and non-consented groups. For those children who
consented to an intra oral examination, there were slightly more males than
females at each data point. This was reversed in the non-consenting groups.
There were a higher proportion of children recording their ethnicity as ‘White’
in the non-consenting group than in the consenting group.
In line with our secondary aim of exploring the disease trajectory of the groups
defined by the presence or absence of caries (into dentine) in the primary
teeth as a risk factor for caries (into dentine) in the permanent teeth the socio-
demographic characteristics are presented by subgroup in Appendix Table 3.
In total 6651 pupils provided data from at least one clinical examination.
Caries prevalence for primary teeth (d3mft) at CE1 was 73.3% and 49.8% at
CE2; this lower prevalence was due to exfoliated primary teeth. Over the
seven-year period of study, caries prevalence for permanent teeth (D3MFT)
increased from 16.7% at CE1 to 31.0%, 42.2% and 45.7% at CE2, CE3 and
CE4 respectively (Table 1). Caries prevalence increased over time for every
quintile of deprivation (Appendix Figure 1).
The proportion of participants with caries in permanent teeth at every time
point was higher for those who had caries in their primary teeth at baseline
compared with those who were caries-free in their primary teeth at baseline;
and they had a higher mean D3MFT. At CE4, 22.1% of those who were caries
9

free in their primary dentition at baseline had developed caries in their
permanent dentition (mean D3MFT = 0.38, range 0 to 6, n = 606) compared
with 56.1% of those who had caries at baseline (mean D3MFT = 1.78, range 0
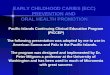
to 13, n = 1523). Figure 2 shows that those that are caries free in the primary
dentition at CE1 are more likely to stay as caries free when they reach
adolescence compared to those who have caries initially.
Figure 2 Distribution of D3MFT by d3mft caries status and clinical examination (CE)
Initial covariates for the regression model included: caries status in the
primary dentition at CE1, ethnicity (White or Asian or other), gender and
IMDQ (Appendix 1 Table 1). We investigated an interaction effect between
age and caries status in the primary dentition at CE1 but this was not
statistically significant (p = 0.09).
Table 1 Results from negative binomial using generalized estimating equation with unstructured correlation structure and mean dispersion variance
The regression analysis model was based on 14,535 records from 5048
pupils who contributed a D3MFT value from at least one of the four clinical
examinations, and values for all covariates in the model. All main effect
covariates were found to be statistically significant. Mean predicted values
indicated a rising D3MFT count as pupils aged (consistent with new teeth
emerging). These values were 4.5 times higher (95% CI 3.90 to 5.16) in those
pupils with caries in their primary dentition at CE1 than in those without. This
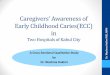
separation of the two trajectories can clearly be seen in Figure 3 where for
illustrative purposes covariates for gender, deprivation and ethnicity have
been fixed at Male, White and most deprived IMDQ. From the adjusted model
(Table 1) White, and Female are associated with higher D3MFT count; D3MFT
count is highly statistically significant with IMDQ (p<0.001) and increased with
increasing levels of deprivation as indicated by IMDQ.
10

Figure 3 Estimated mean D3MFT for Male, White, Index of Material Deprivation quintile 5 (most deprived) subgroup by Clinical Examination 1 d3mft caries status
In Figure 3, for illustrative purposes covariates for gender, ethnicity and
deprivation have been fixed at categories of Male, White and most deprived
IMDQ. Figures corresponding to other combinations of categories can be
plotting using the coefficients provided in Table 1.
11

DiscussionThe main purpose of the study was to describe the development of caries
over seven years in a cohort of children from ages 7 to 16 years. It is the first
of its type in the United Kingdom and one of the largest and longest duration
internationally. It is clear from these results that even in England, which has
the lowest caries rates for 12-year-olds in Europe (Malmo University 2016),
dental caries in disadvantaged areas of the country continues to be a major
public health problem, affecting over 50% of this study population. The
findings support previous studies that caries is significantly associated with
deprivation but that the disparity widens with age with a negative impact on
quality of individual and family life (Ravaghi et al. 2016). A key finding of our
study was the significant association between caries in the primary teeth
(ages 7-9 years) and caries in the permanent teeth. Our data show that the
development of caries in the primary dentition means that children embark on
a very steep and different disease trajectory in their permanent dentition to
children whose primary dentition is caries free.
The main strength of this study was the number of participants recruited and
followed up over a 7-year period. This large study with high quality continuous
data provides information on caries development and progression during a
period of the life course that we know little about. This is an important age
group as children transition from the primary to the permanent dentition and
start to become more independent. The change in social environment
experienced in these years will influence caries risk and have lifelong impact
on oral health. Furthermore, as this was a school-based study, eligibility was
not restricted to children and adolescents registered with or attenders of
general dental practices. This information provided by this whole population
approach improves our understanding of caries development and progression
in underserved populations.
The populations at baseline and follow-up were similar in terms of socio-
demographic values (gender, IMDQ and ethnicity) suggesting loss to follow up
had limited impact on the findings. The socio-demographic profile of the study
cohort was similar to the reference population of the region, with a significant
12

sub-population from an Asian ethnic background and high levels of
deprivation, both associated with increased caries prevalence, which explains
why the caries prevalence in the cohort was higher than national norms (Pitts
et al. 2015). A weakness of the study was loss to follow-up, particularly
between CE2 and CE3. The main reason for loss to follow up was that over
25 per cent of the secondary schools, accounting for more than 40% of pupils
in the study locality did not consent to take part. These schools refusing
access represented the larger schools in the area. Milsom et al (2011)
reported that epidemiological studies in the region showed that children from
larger schools had higher caries prevalence and levels of deprivation
(participation bias) so caries incidence and prevalence may have been under-
estimated in this study.
The caries assessment method used diagnosed caries at a late stage; caries
into dentine. This decision was taken as the study was designed to take a
public health perspective. Cavitated caries requires treatment and therefore
has implications for children and their parents and the healthcare system in
terms of costs and capacity. The caries assessment method we used is the
same method used in local and national disease surveillance programs and
therefore enabled comparison with recent and future cross sectional
epidemiological findings (Pitts et al. 1997). A finer level of caries diagnosis, for
example using the ICDAS stages 2 and 3, would have provided useful
additional information but would have added to the time required to undertake
the assessments and could have compromised recruitment and particularly
retention in secondary schools. Retaining inter-examiner agreement,
particularly in a study of this size, could also pose problems.
The findings of this study have implications for the design of oral health
prevention strategies. Our results show that deprivation remains an important
predictor of future caries, and that children who have caries in their primary
dentition follow a steep disease development trajectory in their permanent
dentition. The key predictor of caries in the permanent teeth was previous
caries experience. Children who have primary dentitions that are caries free
13

and caries active children should be considered as two different populations
for prevention strategies due to their very different risk profiles.
There is a correlation between parental oral health, parental behaviors and
locus of control, which can impact on the oral health risk of young children
(Duijster et al. 2015). Parallel qualitative research on this study population
(need the reference (Hall-Scullin et al. 2015) showed that participants in
adolescence perceived that the example set by their parents in early
childhood was the dominant influence on their oral health. The Dunedin
project (Thomson et al. 2004) reported an association across the life course
between unfavorable dental health beliefs and poorer oral health and
demonstrated that it is possible to change the behaviors between
adolescence and adulthood but these behavioral changes can be unstable.
The study suggests that prevention of caries in early childhood is critically
important to prevent children embarking on a ‘fast train’ disease trajectory,
which will have lifelong consequences, but the evidence base for effective
interventions to instill risk-reducing behavior in very young children is lacking.
This observational study raised two significant research questions; ‘how do
we keep very young children caries free?’ and secondly ‘once a child
develops caries how to we slow down and stop the process?’ The same
interventions may not provide the answers to both questions. For example the
assessment of caries in the primary teeth (caries free or not) could be used to
identify at-risk children for a targeted caries prevention program such as
fissure sealants as soon as permanent teeth erupt.
The findings of this study illustrate the significant long-term consequences of
developing caries in early childhood. The widening of the social gradient of
disease with age also emphasizes the need for dental public health
improvement strategies to address the social determinants of dental disease.
AcknowledgementsThe authors would like to thank the staff and participants at schools in East
Lancashire and Blackburn with Darwen. We also wish to acknowledge the
14

Salaried Dental Service, Lancashire Care NHS Foundation Trust led by
Catherine Morley; Joe Fielding, Uriana Boye, Angela Willesey and Sarah
Procter who acted as Gold Standard examiners for the calibration and training
events; and Janet Neville at The Dental Observatory. This work was
supported by Colgate-Palmolive. Support cost funding was obtained from
Cumbria and Lancashire Comprehensive Local Research Network (CLCLRN).
The authors declare there are no competing interests.
15

ReferencesBASCD. 2009. Oral health survey of 12 year old children in England
2008/2009. National protocol. NHS Dental Epidemiology Programme.
Casamassimo PS, Thikkurissy S, Edelstein BL, Maiorini E. 2009. Beyond the
dmft: The human and economic cost of early childhood caries. Journal
of the American Dental Association. 140(6):650-657.
Cunnion DT, Spiro A, 3rd, Jones JA, Rich SE, Papageorgiou CP, Tate A,
Casamassimo P, Hayes C, Garcia RI. 2010. Pediatric oral health-
related quality of life improvement after treatment of early childhood
caries: A prospective multisite study. Journal of Dentistry for Children
(Chicago, Ill ). 77(1):4-11[abstract only].
Regional dental health 12 year olds 2000/01(England). 2001. [accessed
04/10/2014]. http://www.dental-observatory.nhs.uk/Default.aspx?
crumb=00020007015710E000BB.
Regional dental health 5 year olds 2005/06 (England). 2006. [accessed
04/10/2014]. http://www.dental-observatory.nhs.uk/Default.aspx?
crumb=00020007015610E000BB.
Duijster D, de Jong-Lenters M, Verrips E, van Loveren C. 2015. Establishing
oral health promoting behaviours in children – parents’ views on
barriers, facilitators and professional support: A qualitative study. BMC
Oral Health. 15:157.
Dye BA, Thornton-Evans G, Li X, Iafolla TJ. 2015. Dental caries and sealant
prevalence in children and adolescents in the United States, 2011–
2012. CDC National Centre for Health Statistics.
Hall-Scullin E, Goldthorpe J, Milsom K, Tickle M. 2015. A qualitative study of
the views of adolescents on their caries risk and prevention
behaviours. BMC Oral Health. 15(1):141.
16

Malmo University. 2016. Country oral health profiles who regions table
European Union and European Economic Area (Euro incl. DMFT for
12-year-olds).
Mukund L. 2011. The English Indices of Deprivation 2010. In: Government
CaL, editor.: Department for Communities and Local Government.
NPEU. 2013. IMD postcode search tool. University of Oxford.
Petersen PE. 2005. The burden of oral disease: Challenges to improving oral
health in the 21st century. Bulletin of the World Health Organization.
83(1):3.
Petersen PE, Bourgeois D, Ogawa H, Estupinan-Day S, Ndiaye C. 2005. The
global burden of oral diseases and risks to oral health. Bulletin of the
World Health Organization. 83(9):661-669.
Pine C, Pitts N, Nugent Z. 1997. British Association for the Study of
Community Dentistry (BASCD) guidance on the statistical aspects of
training and calibration of examiners for surveys of child dental health.
A BASCD coordinated dental epidemiology programme quality
standard. Community Dental Health. 14:18.
Pitts N, Chadwick B, Anderson T. 2015. Report 2: Dental disease and
damage in children England, Wales and Northern Ireland. Children’s
Dental Health Survey 2013. Online: National Statistics Office.
Pitts N, Evans D, Pine C. 1997. British Association for the Study of
Community Dentistry (BASCD) diagnostic criteria for caries prevalence
surveys-1996/97. Community Dent Health. 14(Suppl 1):6 - 9.
Poulton R, Caspi A, Milne BJ, Thomson WM, Taylor A, Sears MR, Moffitt TE.
2002. Association between children's experience of socioeconomic
disadvantage and adult health: A life-course study. The Lancet.
360(9346):1640-1645.
17

Ravaghi V, Holmes RD, Steele JG, Tsakos G. 2016. The impact of oral
conditions on children in England, Wales and Northern Ireland 2013. Br
Dent J. 221(4):173-178.
Rooney E, Davies G, Neville J, Robinson M, Perkins C, Bellis M. 2010. NHS
dental epidemiology programme for England oral health survey of 12
year old children 2008/2009. Summary of caries prevalence and
severity reaults.
Thomson WM, Poulton R, Milne BJ, Caspi A, Broughton JR, Ayers KMS.
2004. Socioeconomic inequalities in oral health in childhood and
adulthood in a birth cohort. Community Dentistry & Oral Epidemiology.
32(5):345-353.
18

List of 1 table and 3 figures
Figure 1 Study flowchart
Figure 2 Distribution of D3MFT by d3mft caries status and clinical examination (CE)
Figure 3 Estimated mean D3MFT for Male, White, Index of Material Deprivation quintile 5 (most deprived) subgroup by Clinical Examination 1 d3mft caries status
Table 1 Results from negative binomial using generalized estimating equation with unstructured correlation structure and mean dispersion variance
19

Figure 1 Study flowchart
20

21

Figure 2 Distribution of D3MFT by d3mft caries status and clinical examination (CE)
22

Figure 3 Estimated mean D3MFT for Male, White, Index of Material Deprivation quintile 5 (most deprived) subgroup by Clinical Examination 1 d3mft caries status
Footnote: Illustrative estimated mean D3MFT values for male pupils of self-
reported White ethnicity living in an area of greatest deprivation. Markers (+)
indicate mean observed values at CE1 through CE4.
23

Table 1 Results from negative binomial using generalized estimating equation with unstructured correlation structure and mean dispersion variance
Exponentiated coefficient
Semi robust standard
error§
95% CI
Age 1.27*** 0.01 1.26, 1.28Caries free (d3mft = 0) 1Caries active (d3mft >0) 4.49*** 0.32 3.90, 5.16Asian or other 1White 1.24*** 0.07 1.12, 1.38Male 1Female 1.11* 0.05 1.02, 1.20IMDQ 1 §§ 1IMDQ 2 1.06 0.13 0.83, 1.36IMDQ 3 1.34* 0.17 1.04, 1.72IMDQ 4 1.39** 0.17 1.10, 1.77IMDQ 5 1.77*** 0.21 1.41, 2.23Constant 0.01*** 0 0.00, 0.01
§ Huber/White/sandwich estimator of variance used which produces valid standard errors even if the correlations within group are not as hypothesized by the specified correlation structure and accounts for clustering in the data§§ IMDQ p<0.001* p<0.05, ** p<0.01, *** p<0.001
24

Appendix Title
Longitudinal study of caries development from childhood to adolescenceAuthorsMs E. Hall-Scullin1, Consultant in Dental Public Health, NHS Ayrshire & Arran.Miss H. Whitehead2, Dental Professional Lead, Community Dental Service, Salford Royal NHS Foundation Trust.Prof K. Milsom3, Consultant in Dental Public Health, Department of Dental Public Health, Countess of Chester Hospital.Prof M. Tickle4, Professor of Dental Public Health and Primary Care, Division of Dentistry, University of Manchester.Dr T-L Su, Lecturer in Statistics, Division of Dentistry, University of ManchesterDr T. Walsh4, Reader in Biostatistics, Division of Dentistry, University of Manchester.
Address1Public Health Department, NHS Ayrshire & Arran, Afton House, Ailsa Hospital Campus, Dalmellington Road, Ayr, KA6 6AB, UK. 2Community Dental Service, Salford Royal NHS Foundation Trust, Pendleton Gateway, 1 Broadwalk, Salford, M6 5FX, UK. 3Department of Dental Public Health, 1829 Building, Countess of Chester Hospital, Chester, CH2 1UL, UK. 4Division of Dentistry, Faculty of Biology, Medicine and Health, University of Manchester, Oxford Road, Manchester, M13 9PL, UK.
25

First (Baseline) Clinical Examination 1 (n =
5470)Clinical Examination 2 (n = 5475) Clinical Examination 3 (n = 3036) Clinical Examination 4 (n = 2733)
Median Date 19/03/2006 18/02/2009 10/10/2011 16/05/2013
D3MFT = 0
n (%)
D3MFT > 0
n (%)
D3MFT
Mean (sd)
D3MFT = 0
n (%)
D3MFT > 0
n (%)
D3MFT
Mean (sd)
D3MFT = 0
n (%)
D3MFT > 0
n (%)
D3MFT
Mean (sd)
D3MFT = 0
n (%)
D3MFT > 0
n (%)
D3MFT
Mean (sd)
Caries prevalence
(D3MFT) 4559 (83.35) 911 (16.65)
0.28 (0.73)
[D3MFT > 0
1.70 (0.90)]
3780 (69.04) 1695 (30.96)
0.64 (1.20)
[D3MFT > 0
2.08 (1.29)]
1756 (57.84) 1280 (42.16)
1.04 (1.67)
[D3MFT > 0
2.48 (1.75)]
1484 (54.30) 1249 (45.70)
1.36 (2.08)
[D3MFT > 0
2.98 (2.16)]
Caries status
(d3mft) at
CE1
d3mft = 0 1398 (95.69) 63 (4.31) 0.06 (0.34) 1120 (89.24) 135 (10.76) 0.16 (0.54) 520 (80.12) 129 (19.88) 0.34 (0.80) 472 (77.89) 134 (22.11) 0.38 (0.85)
d3mft > 0 3161 (78.85) 848 (21.15) 0.36 (0.82) 2140 (61.94) 1315 (38.06) 0.81 (1.31) 828 (48.06) 895 (51.94) 1.32 (1.80) 668 (43.86) 855 (56.14) 1.78 (2.27)
Age (years) (SD) 8.04 (0.30) 8.08 (0.31) 10.96 (0.30) 10.97 (0.30) 13.61 (0.34) 13.61 (0.35) 15.20 (0.34) 15.18 (0.34)
Gender Male 2404 (84.29) 448 (15.71) 0.26 (0.70) 2001 (70.31) 845 (29.69) 0.62 (1.18) 917 (59.47) 625 (40.53) 0.97 (1.61) 774 (55.44) 622 (44.56) 1.36 (2.10)
Female 2155 (82.31) 463 (17.69) 0.31 (0.77) 1779 (67.67) 850 (32.33) 0.67 (1.22) 839 (56.16) 655 (43.84) 1.10 ( 1.73) 710 (53.10) 627 (46.90) 1.37 (2.06)
Ethnicity Asian or
other1074 (81.43) 245 (18.57) 0.31 (0.75) 915 (66.64) 458 (33.36) 0.69 (1.21) 475 (55.62) 379 (44.38) 1.11 (1.70) 359 (52.87) 320 (47.13) 1.41 (2.07)
White3484 (83.95) 666 (16.05) 0.28 (0.73) 2849 (69.86) 1229 (30.14) 0.62 (1.19) 1278 (58.76) 897 (41.24) 1.02 (1.65) 1119 (54.83) 922 (45.17) 1.34 (2.08)
Index of
Material
Deprivation
quintiles
2010
(IMDQ)
IMDQ 1 302 (89.61) 35 (10.39) 0.16 (0.57) 279 (80.87) 66 (19.13) 0.37 (0.91) 128 (71.11) 52 (28.89) 0.54 (1.08) 123 (72.78) 46 (27.22) 0.62 (1.32)
IMDQ 2 830 (88.39) 109 (11.61) 0.19 (0.58) 712 (76.48) 219 (23.52) 0.44 (0.98) 360 (69.23) 160 (30.77) 0.63 (1.17) 311 (62.08) 190 (37.92) 0.95 (1.72)
IMDQ 3 503 (84.11) 95 (15.89) 0.28 (0.71) 435 (72.50) 165 (27.50) 0.54 (1.11) 197 (54.27) 166 (45.73) 1.11 (1.68) 176 (54.66) 146 (45.34) 1.29 (2.02)
IMDQ 4 944 (84.59) 172 (15.41) 0.26 (0.70) 760 (69.66) 331 (30.34) 0.59 (1.10) 355 (58.29) 254 (41.71) 1.04 (1.66) 297 (54.50) 248 (45.50) 1.33 (1.97)
IMDQ 5 1933 (79.91) 486 (20.09) 0.35 (0.81) 1559 (63.79) 885 (36.21) 0.80 (1.35) 702 (52.70) 630 (47.30) 1.25 (1.85) 547 (47.94) 594 (52.06) 1.68 (2.30)
Appendix Table 1 Per cent (%) caries free (D3MFT=0) and caries active (D3MFT>0) with mean D3MFT and standard deviation (sd)by clinical and socio-demographic variables at each clinical examination (CE)
26

Clinical Examination (CE)
CE1 N (%) CE2 N (%) CE3 N (%) CE4 N (%)
No consent Consent No
consent Consent No consent Consent No
consent Consent
Age (years)
Mean age (sd) N/A 8.0 (0.3) N/A 11.0
(0.3)13.6 (0.4)
13.6 (0.3)
15.2 (0.4)
15.2 (0.3)
Gender
Male 83 (46.4)
2852 (52.1)
58 (40.8)
2846 (52.0)
365 (49.3)
1542 (50.8)
250 (44.5)
1396 (51.1)
Female 96 (53.6)
2618 (47.9)
84 (59.2)
2630 (48.0)
376 (50.7)
1494 (49.2)
312 (55.5)
1337 (48.9)
Ethnicity
Asian or other
10 (5.7)
1319 (24.1)
14 (9.9)
1373 (25.2)
119 (16.6)
854 (28.2)
71 (12.8)
679 (25.0)
White 164 (94.3)
4150 (75.9)
128 (90.1)
4079 (74.8)
596 (83.4)
2175 (71.8)
483 (87.2)
2041 (75.0)
Index of Material Deprivation quintiles 2010 (IMDQ)
IMDQ 1 19 (10.7)
337 (6.2)
11 (8.0)
345 (6.4)
30 (4.1)
180 (6.0)
12 (2.2)
169 (6.3)
IMDQ 2 41 (23.0)
939 (17.4)
32 (23.3)
931 (17.2)
114 (15.7)
520 (17.3)
74 (13.8)
501 (18.7)
IMDQ 3 23 (12.9)
598 (11.1)
16 (11.7)
601 (11.1)
81 (11.20
363 (12.1)
80 (14.9)
322 (12.0)
IMDQ 4 40 (22.5)
1116 (20.6)
41 (29.9)
1091 (20.2)
152 (21.0)
609 (20.3)
116 (21.6)
545 (20.4)
IMDQ 5 55 (30.9)
2419 (44.7)
37 (27.0)
2444 (45.2)
348 (48.0)
1332 (44.3)
256 (47.6)
1141 (42.6)
Appendix Table 2 Socio-demographic characteristics of consenting and non-consenting pupils
27

First (Baseline) Clinical
Examination
N (%)
d3mft =0 d3mft > 0
Age (years)
Mean age (sd)8.0
(0.29)1461
8.1 (0.30)4009
Gender
Male 83 (46.4)
2852 (52.1)
Female 96 (53.6)
2618 (47.9)
Ethnicity
Asian or other 177 (12.1)
1142(28.5)
White 1284 (87.9)
2866 (71.5)
Index of Material Deprivation quintiles 2010 (IMDQ)
IMDQ 1 157(10.8)
180(4.55)
IMDQ 2 360(24.7)
579(14.6)
IMDQ 3 190(13.1)
408(10.3)
IMDQ 4 279(19.2)
837(21.6)
IMDQ 5 468(32.2)
1951(49.3)
Appendix Table 3 Characteristics of the participants by caries status (d3mft) at first (baseline) clinical examination (CE1)
28

Appendix Figure 1 Graph of caries prevalence (D3MFT) at each data point for each Index of Material Deprivation quintiles (IMDQ)
29

Model selectionVarious modeling approaches were explored including Poisson regression
and Negative Binominal regression (with either mean dispersion variance
(which corresponds to Cameron and Trivedi’s NB2 variance function) or
constant dispersion variance (which corresponds to the NB1 variance
function). All approaches took into account the longitudinal structure of the
data using Generalized Estimating Equations with either independent,
unstructured or exchangeable correlation structures).
Initial covariates for the regression models included all main effects: caries
status in the primary dentition at first (baseline) clinical examination (CE1),
ethnicity (White or Asian or other), gender and IMDQ. We investigated an
interaction effect between age and caries status in the primary dentition at
CE1 but this was not statistically significant (p = 0.09). For improved model fit
and ease of interpretation we removed the interaction term from a final model,
leaving only main effects.
There was statistically significant evidence of over dispersion (mean greater
than variance) in the data, with the estimated dispersion parameter alpha =
1.811 statistically significantly away from zero and indicating that a mean
dispersion variance function was appropriate. Alongside Appendix Figure 2
this provided visual evidence that Negative Binominal demonstrated a
sensible model fit to the data that was superior to the Poisson regression. We
therefore opted for Negative Binominal with Generalized Estimating Equation
as a sensible analysis strategy.
30

Appendix Figure 2 Observed and predicted values from Poisson and Negative Binomial models
31
Recommended