Linking Data to Understand Veteran Suicide and Direct Effective Prevention Programs
Claire Hoffmire, PhDDepartment of Veterans AffairsVISN2 Center of Excellence for Suicide Prevention
VETERANS HEALTH ADMINISTRATION
Suicide Mortality Surveillance: The Cornerstone of Suicide Prevention
• Effective surveillance systems:– Inform the development of targeted prevention strategies that have
the potential to meaningfully reduce suicide burden– Help to evaluate the impact of existing and newly implemented
prevention programs.
• National suicide surveillance systems:– National Violent Death Reporting System (NVDRS)– NDI– VA State Mortality Project
• National priority to improve suicide surveillance– 2012 National Strategy for Suicide Prevention goal
• “Increase the timeliness and usefulness of national surveillance systems relevant to suicide prevention and improve the ability to collect, analyze, and use this information for action.”
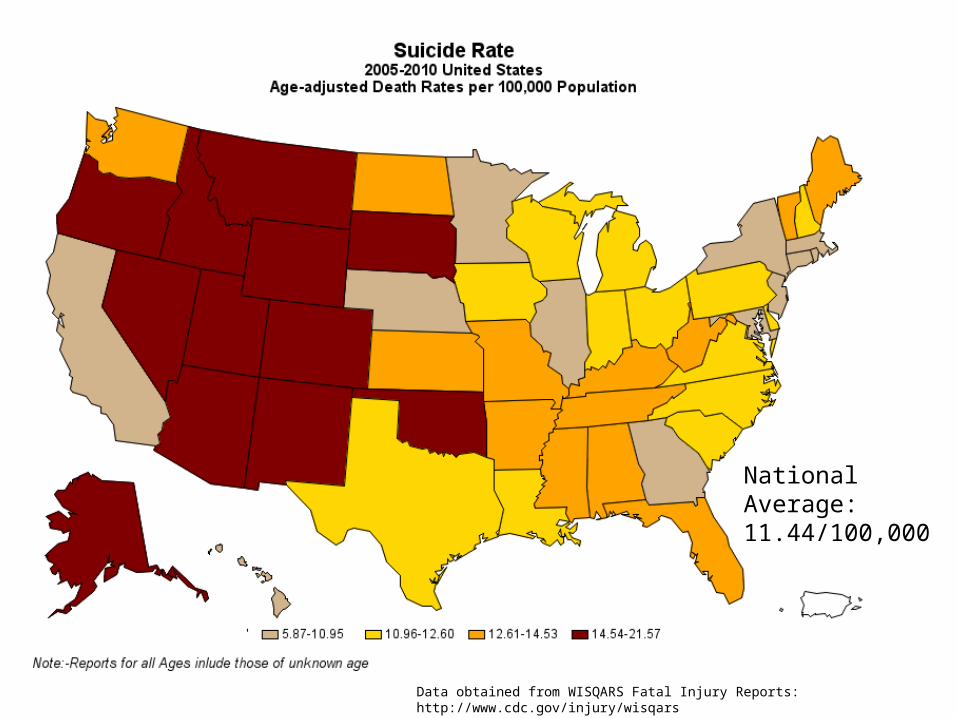
National Average: 11.44/100,000
Data obtained from WISQARS Fatal Injury Reports: http://www.cdc.gov/injury/wisqars
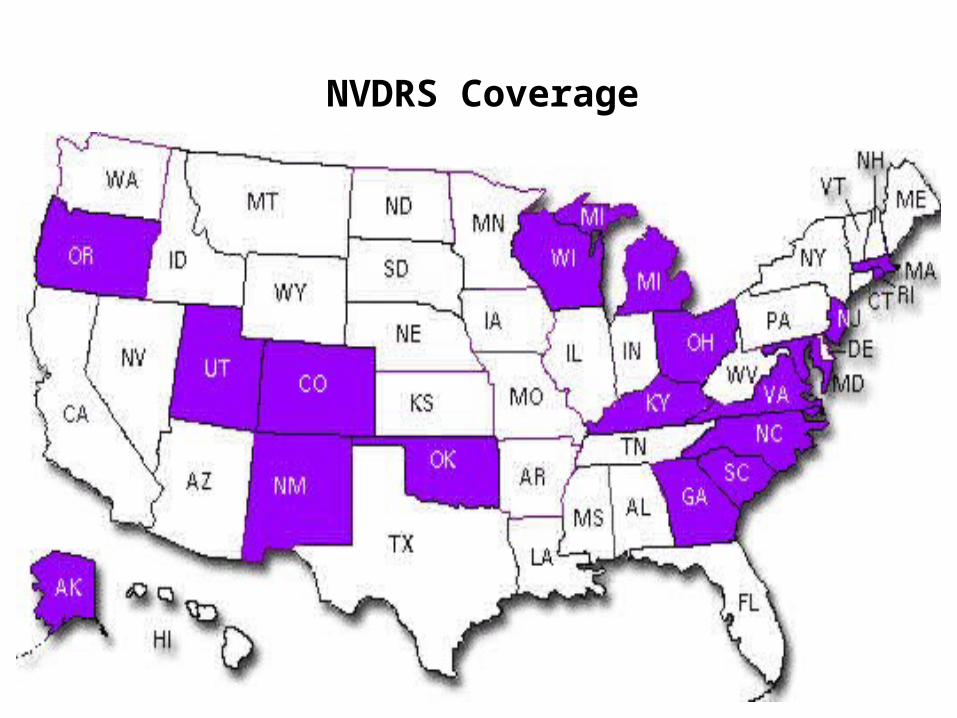
NVDRS Coverage
VETERANS HEALTH ADMINISTRATION
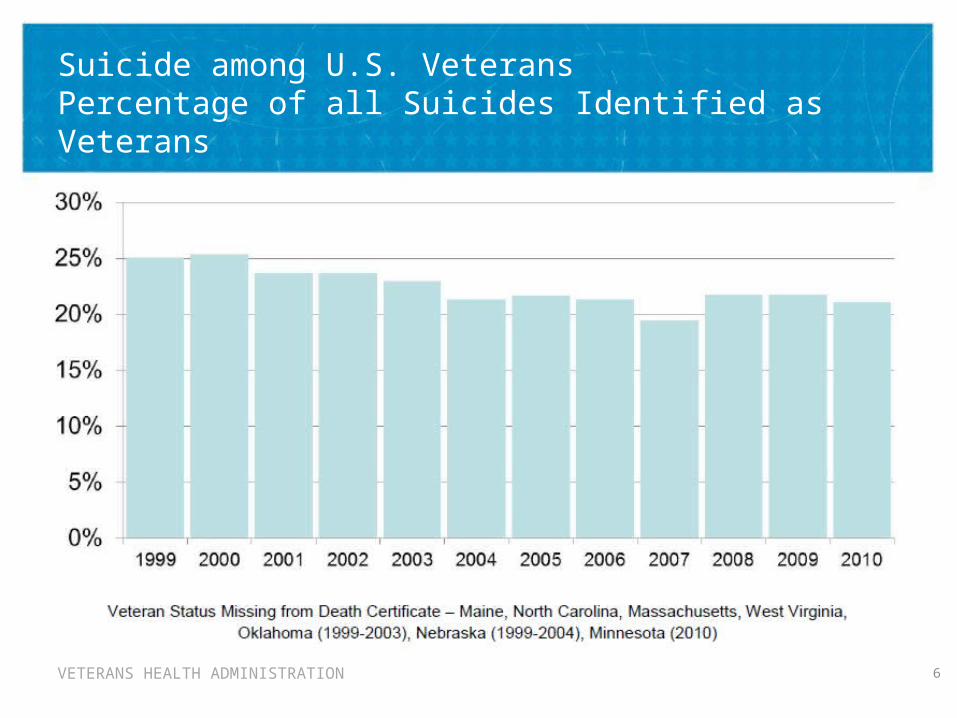
Suicide among U.S. VeteransPercentage of all Suicides Identified as Veterans
6
VETERANS HEALTH ADMINISTRATION
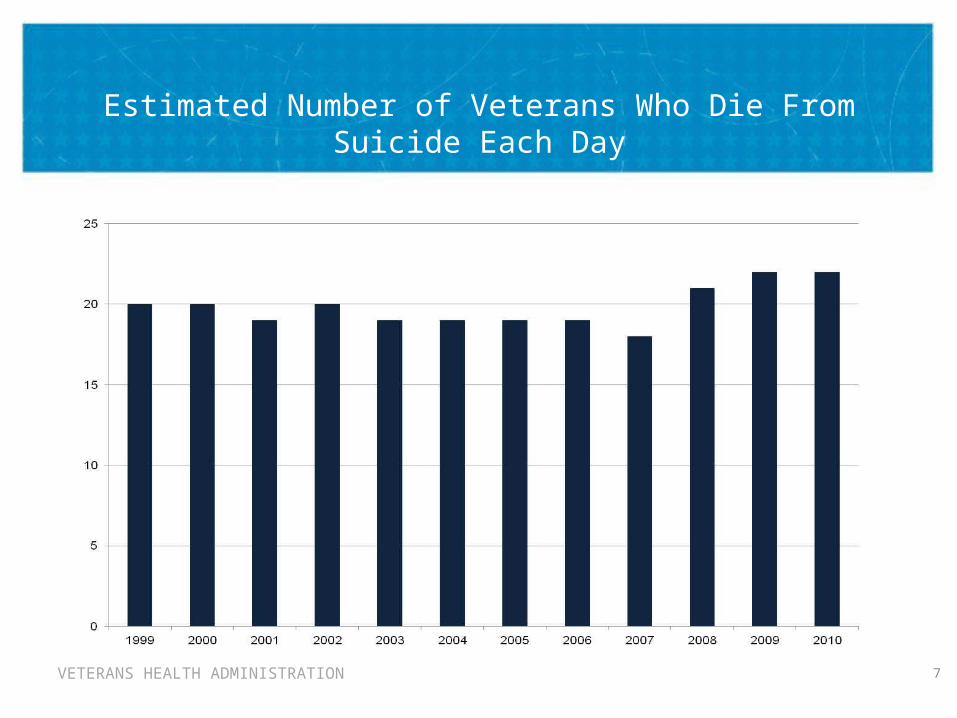
Estimated Number of Veterans Who Die From Suicide Each Day
7
VETERANS HEALTH ADMINISTRATION
The State Mortality Data Project
• “The Department of Veterans Affairs believes that a comprehensive suicide prevention program requires timely and accurate information beyond that acquired from it’s internal patient population.” – 2012 Suicide Data Report
– Overcome delay’s associated with national mortality data– Accurately identify true Veterans– Understand suicide among all Veterans– Evaluate differences and changes in outcomes among VHA utilizing
Veterans
• A State-VA Collaborative Project– In 2010 VA Secretary Shinseki requested collaboration and support from all
U.S states– Data on all known suicides reported from 1999 through 2015 – Will be used, in part, to fulfill Public Law 111.163 to determine the number
of Veterans who died from suicide 1999-2009
VETERANS HEALTH ADMINISTRATION
Project Status: May 2013
• Data Requested from death certificates– SSN, Name, DOB, DOD, Age, Sex, Race/ethnicity, Marital status,
Education, ICD-10 Cause of death, State & County of residence, County of death, Veteran Status, Industry, occupation
• Project Barriers– Inconsistent availability of requested information in all states– State barriers to providing non-resident data – State preference to provide de-indentified data due to conflicting
interpretation of Social security laws
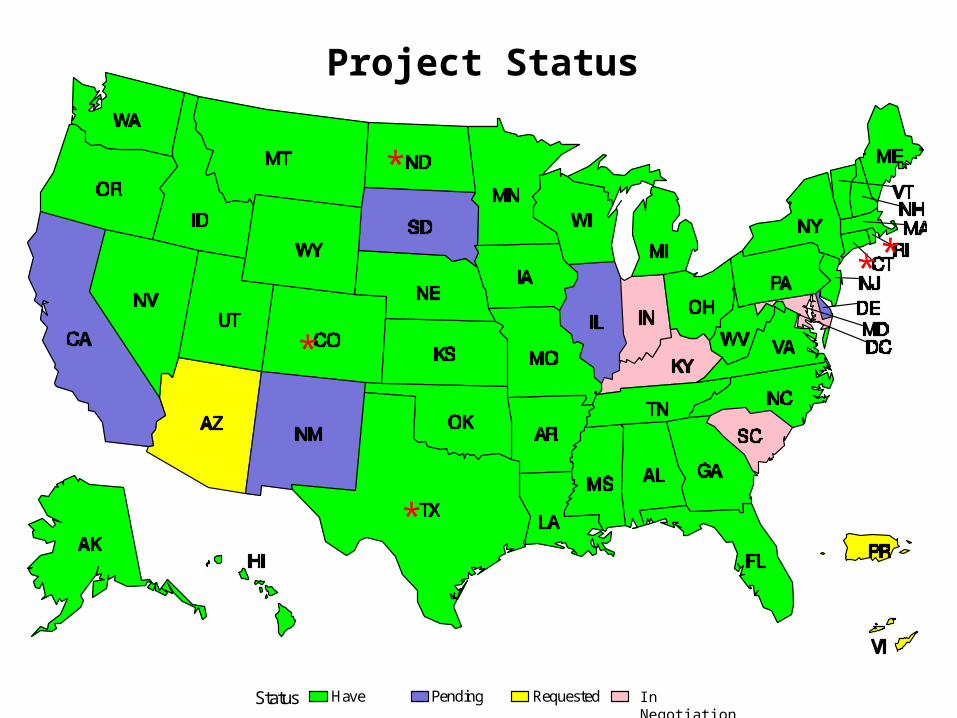
Status Have Pending Requested Denied
Project Status
*
* *
*
*
In Negotiation
VETERANS HEALTH ADMINISTRATION
Linking to VA Data
• Validation of Veteran Status– Partnership with the DOD to accurately identify all Veterans– Preliminary evidence indicates that death certificate misclassification
exists– Improve comparison of Veterans to non-Veterans
• Identification of VHA service utilization– Directly compare VHA & non-VHA Veterans for the first time– Medical information also available for VHA users
• Inclusion of state data in suicide mortality repositories– VA Suicide Data Repository
• State records, annual VA NDI all-cause search, SPAN, VCL, expanded VA-DoD NDI search
– VA-DoD collaborative Data Repository • VA-DoD NDI search, limited DoD service record, DoDSER
VETERANS HEALTH ADMINISTRATION
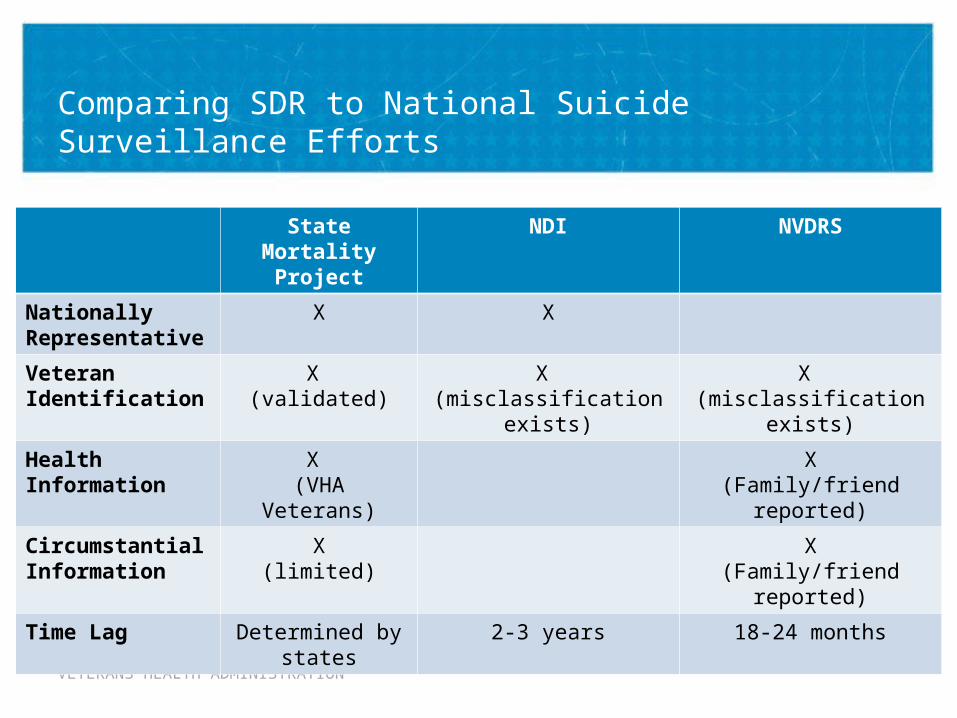
Comparing SDR to National Suicide Surveillance Efforts
State Mortality Project
NDI NVDRS
Nationally Representative
X X
Veteran Identification
X (validated)
X (misclassification
exists)
X (misclassification
exists)
Health Information
X (VHA Veterans)
X(Family/friend
reported)
Circumstantial Information
X(limited)
X(Family/friend
reported)
Time Lag Determined by states
2-3 years 18-24 months
VETERANS HEALTH ADMINISTRATION
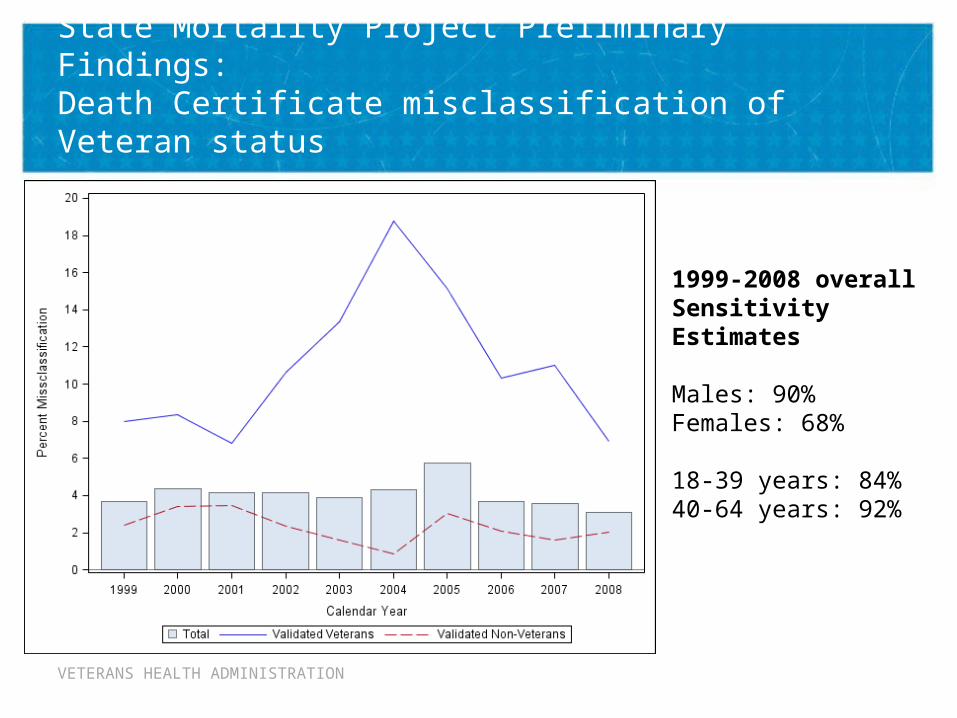
State Mortality Project Preliminary Findings: Death Certificate misclassification of Veteran status
1999-2008 overall Sensitivity Estimates
Males: 90%Females: 68%
18-39 years: 84%40-64 years: 92%
VETERANS HEALTH ADMINISTRATION
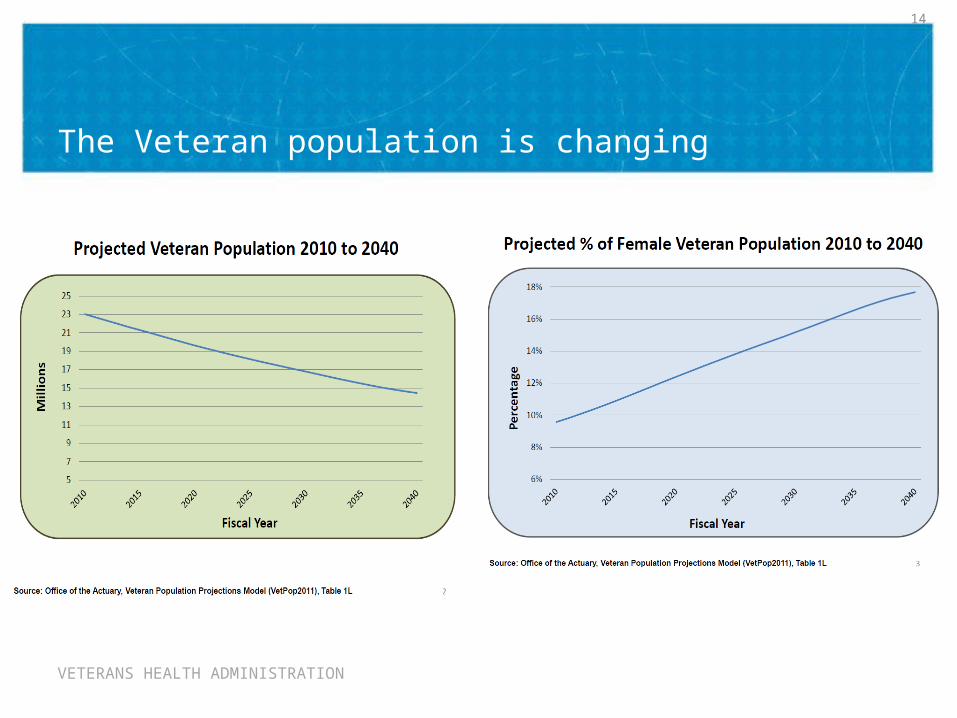
The Veteran population is changing
14
VETERANS HEALTH ADMINISTRATION
Joining Forces to Save Lives:Why initiate or continue State-VA Partnerships?
• The Veteran population is changing making accurate and timely surveillance of Veteran suicide mortality more critical than ever
• Veterans make up nearly 20% of all suicide decedents– Nearly 8,000 Veterans die by suicide every year– In the next 5 years, the NAASP set a goal to save 20,000 lives = 4,000 lives
annually
• Partnering with the VA can greatly improve the accuracy of Veteran status reporting on death certificates
• Coverage far exceeds that of NVDRS and can inform its expansion
• VA and DoD can add critical information to inform prevention
• VA Secretary Shinseki has requested the help of State Health Departments to improve our understanding of Veteran suicide and save lives
VETERANS HEALTH ADMINISTRATION
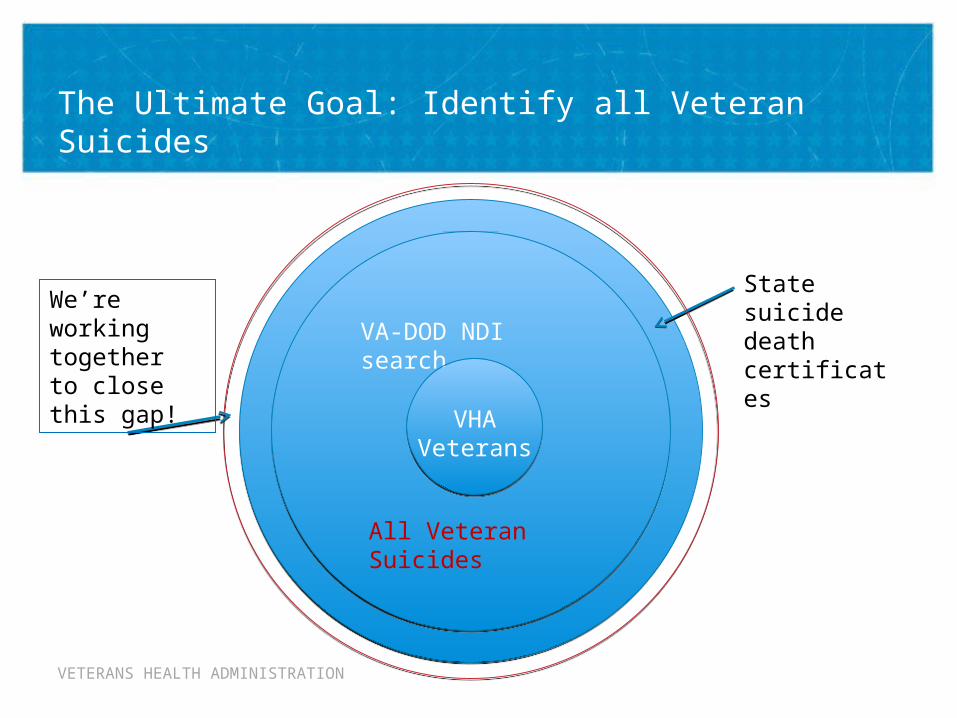
State suicide death certificates
VA-DOD NDI search
The Ultimate Goal: Identify all Veteran Suicides
All Veteran Suicides
VHA Veterans
We’re working together to close this gap!
VETERANS HEALTH ADMINISTRATION
Acknowledgements
• Jan Kemp, RN, PhD – VA National Mental Health Program Director
• Robert Bossarte, PhD – Acting Associate Director, COE• Kenneth Conner, PsyD, MPH – Director, COE• Rebecca Piegari, MS – Statistician, COE• Brady Stephens, MS – Statistician, COE• Heather Shaw, BS – Research Assistant, COE• Janet McCarten, PhD – Health Science Specialist, COE
• Participating State Health Department POCs
Recommended

















