Leg Assessment and IPCElaine Gibson BSc(Hons) DipN, RGNAspen Medical Europe Tissue Viability Nurse SpecialistEast Kent University Hospitals Foundation Trust
Dr Jon Evans BSc PhD MIET CEngVascular Business Unit ManagerTheresa Hanlon RN DIP HEProduct SpecialistHuntleigh Healthcare
Jane Wigg RGN MScClinical Innovations ManagerHaddenham Healthcare
Trudie Young RGN MScFacilitator
Conference workshops in association with the Leg Club Industry Partners
“Empowering patients through a unique collaboration with industry dedicated to lower limb conditions”

Examination of the arterial patientPast Medical HistoryCardiac: angina; arrhythmias; MIDiabetesHypertensionRenalNeurological: cerebrovascular; peripheralInjuriesArthritis / collagen diseaseClotting abnormalities
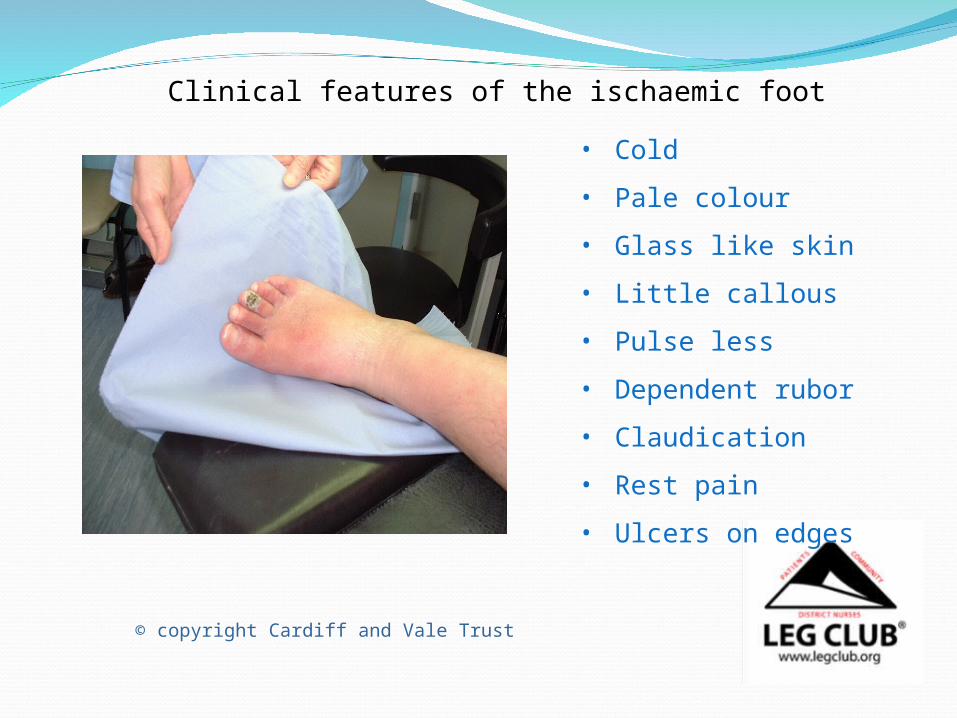
Clinical features of the ischaemic foot• Cold
• Pale colour
• Glass like skin
• Little callous
• Pulse less
• Dependent rubor
• Claudication
• Rest pain
• Ulcers on edges
© copyright Cardiff and Vale Trust

Doppler Assessment
• Doppler probes come in several Frequencies 2-10 MHz
• It is important to use contact gel, use at 45 degree angle
• 8MHz probe is ideal for measuring ABPI
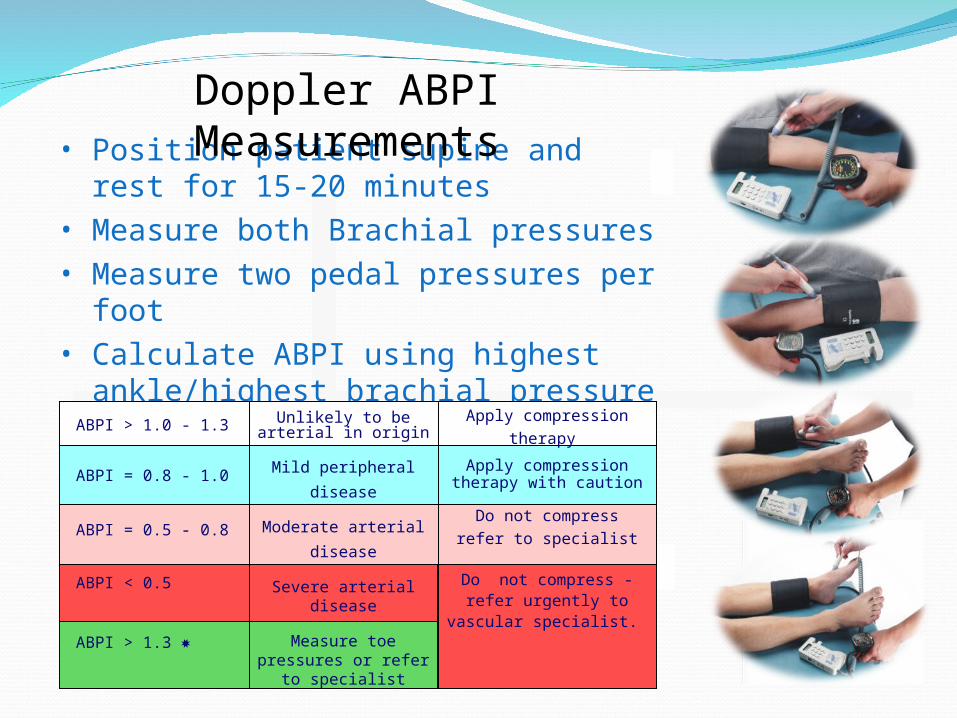
• Position patient supine and rest for 15-20 minutes
• Measure both Brachial pressures• Measure two pedal pressures per foot• Calculate ABPI using highest ankle/highest
brachial pressure
Doppler ABPI Measurements
ABPI > 1.0 - 1.3
ABPI = 0.8 - 1.0
ABPI = 0.5 - 0.8
ABPI < 0.5
ABPI > 1.3
Unlikely to be arterial in origin
Mild peripheral
disease
Moderate arterial
disease
Severe arterial disease
Measure toe pressures or refer to
specialist
Apply compression therapy
Apply compression therapy with caution
Do not compressrefer to specialist
Do not compress - refer urgently to vascular
specialist.

Other useful tests
Waveform assessment (TASC2)
Exercise DopplerSegmental pressuresBuergers testSlow capillary return after blanchingPole testToe pressures (TASC2) Pulse Volume Recording (TASC2)

Pole Test
Pole test for measurement of ankle pressures in patients with calcified vessels: the Doppler probe is placed over a patent pedal artery and the foot raised against a pole that is calibrated in mm Hg. The point at which the pedal signal disappears is taken as the ankle pressure

Triphasic Waveform - Normal Biphasic Waveform – Normal with age
Waveforms provide extra information to confirm clinical findings and ABPI’s
Doppler Waveforms and Sounds

Monophasic Waveform 1 - Abnormal
Doppler Waveforms and Sounds
Toe PressuresDoppler or Photoplethysmography (PPG)
Toe/brachial pressure > 0.7 = normalRest pain usually present in patients with index < 0.15Absolute pressure in the toes of 20-30mmHg is usually
associated with rest pain

Problems with measuring ABPI using Doppler• Difficult to maintain vessel contact during inflation and
deflation
• A reasonable knowledge of anatomy is required
• Difficult to locate vessels
• Typical average time for ABPI is 11mins + 15-20 mins rest (Ipsilon and Get ABI Study 2006)
• Clinicians must be trained and monitored (RCN Guidelines 2006)
• Doppler ABPIs taken by junior doctors disagreed with vascular technicians by 30%. This improved to 15% after formal training (Ray et al 1994)

Specially designed two chamber cuffs are used to detect systolic pressures
Two Chamber Cuffs

An Auto ABI Device
Systolic Pressures and ABI PVR Waveforms

Grade A: NormalSharp systolic peak with prominent dicrotic notch
Pulse Volume Recordings
Grade B: Mildly AbnormalSharp peak, absent dicrotic notch; downslope is bowed away from baseline
Grade C: Moderately AbnormalFlattened systolic peak, upslope and downslope time decreased and nearly equal, absent dicrotic notch.
Grade D: Severely AbnormalLow amplitude or absent pulse wave with equal upslope and downslope time

• Extremely easy to use and fully automatic• Rapid bi-lateral ABI measurement in < 5mins
(Doppler based ABI typically takes 30mins)• No need to rest patient for 15mins• ABI can now be undertaken by less skilled staff• Only have to apply 4 cuffs• Physiologically more accurate• No need to remove socks and tights• Integral printer for documentation of results and
waveforms• Automatic interpretation• Clinically validated (Lewis et al, 2010, 2012)
Advantages of Auto ABI

Uses of IPCDeep veins (Johns et al 2007)Faster muscle recovery (Griffin et al 2007)Increases arterial flow (Morris et al 2002, Eze et al 1996)Wound healing
(Pflzenmaier 2nd,et al 2005, Coleridge-Smith et al 1990)Enhances lymph transport (Baulieu et al 1989)Drainage to functional lymphatics aiding removal
(Brennan and Miller 1998) Oedema Reduction (Partsch, 2008)

Traditional IPC Sequential Cycle
Starts distally and holds pressure in each chamber Releases all chambers togetherUseful for venous and dependency oedemas

Traditional IPC Sequential Cycle
Starts distally and holds pressure in each chamber Releases all chambers togetherUseful for venous and dependency oedemas

Traditional IPCWave cycle
Applies pressure distally and inflates the next progressive chamber whilst releasing the previous
It has a ‘wave’ or peristaltic effect and is useful for palliative, venous and watery oedema

Traditional IPCWave cycle
Applies pressure distally and inflates the next progressive chamber whilst releasing the previous
It has a ‘wave’ or peristaltic effect and is useful for palliative, venous and watery oedema

New machines
‘To date, no mechanical device has been designed to mimic the technique of manual lymphatic drainage, This would essentially
consist of reverse sequential compression’
(Comerota and Aziz, JOL, 2009)
LymphAssist(Flowtron Hydroven 12, developed 2006)

A 12 Chamber IPC Systemwith LymphAssist cycle
Designed for Lymphoedema onlyThe first 12 chamber (overlapping) retrograde
pump with this unique cycleRetrograde flow/ commences proximally5 pulses each chamberBased on MLD (Leduc)Maximum pressure 40mmHgCompletes each cycleCycle 19.6 mins (2 cycles equivalent to MLD)

Advantages
Provides supervised self management/Home useIncreased lymphatic drainage pathways (Furnival-Doran (2012)
Treat the whole /both limbs (full leg garment)Easy to use/ does not required trained therapistCost effective/Time/ resource savingImproved healing timesProblem solvingReduced riskAssists in longevity of roleGood patient experienceEFFECTIVE
Thank YouAny Questions
Recommended