Drugs Affecting the Autonomic Nervous System
Pharmacology 49.222Bill Diehl-Jones RN, PhD
Faculty of Nursing and Department of Zoology

Agenda
• A Zen Review• Overview of CNS and ANS• Neurotransmitters and 2nd Messengers• Cholinergic Agonists and Antagonists• Adrenergic Agonists and Antagonists• Movement Disorder Drugs

Organization of the Nervous System:CNS
• Three divisions of brain:– Forebrain
• cerebral hemispheres– Midbrain
• Corpora quadrigemini, tegmentum, cerebral peduncles
– Hindbrain• Cerebellum, pons, medulla
• Brainstem:– Midbrain, medulla, pons– Connects cerebrum, cerebeluum, spinal
cord

Organization of the Nervous System:Reticular Activating System
• Key Regulatory Functions:– CV, respiratory systems– Wakefulness
• Clinical Link:– Disturbances in the RAS are
linked to sleep-wake disturbances Reticular Formation
Ascending Sensory Tracts
Thalamus
Radiation Fibres
Visual Inputs

Organization of the Peripheral Nervous System
• Three major divisions:– Efferent
• Somatic (motor)• Autonomic
– Sympathetic and Parasympathetic
– Afferent• Sensory

Some Basic Plumbing:The Peripheral Nervous System
Sensory
MotorSympathetic
Parasympathetic
Parasympathetic

Preganglionic Nerves
Sympathetic AND Parasympathetic preganglionic fibres release Acetylcholine (ACh)
ACh has two types of receptors:Muscarinic and Nicotinic
Postganglionic nerves have Nicotinic receptors
Sympathetic Parasympathetic
ACh

Postganglionic Nerves
• Sympathetics release Norepinephrine
• Parasympathetics release ACh
• Norepinephrine binds to adrenergic receptors
• ACh binds to Muscarinic receptors
Sympathetic Parasympathetic
ACh
NE

What Happens at the Effectors?
• NE from postganglionic sympathetics binds to Adrenergic Receptors
• ACh from postganglionic parasympathetics binds to Muscarinic Receptors
ACh
MuscarinicReceptor
NE
AdrenergicReceptor
Sympathetic Parasympathetic

Cholinergic Neurons
Na+
Choline
Ca++
Receptor
Acetylcholinesterase
Acetylation

Cholinergic Receptors
• Muscarinic receptors come in 5 flavours– M1, M2, M3, M4, M5– Found in different locations– Research is on-going to identify specific
agonists and antagonists• Nicotinic receptors come in 1 flavour

Cholinergic Agonists
• Acetylcholine• Bethanechol• Carbachol• Pilocarpine

General Effects of Cholinergic Agonists
• Decrease heart rate and cardiac output
• Decrease blood pressure
• Increases GI motility and secretion
• Pupillary constriction

Cholinergic Antagonists
• Antimuscarinic agents– Atropine, ipratropium
• Ganglion blockers– nicotine
• Neuromuscular blockers– Vecuronium,
tubocuarine, pancuronium

Where are some of these drugs used?

Atropine(a cholinergic antagonist)
• Comes from Belladonna– High affinity for muscarinic
receptors– Causes “mydriasis” (dilation of
the pupil) and “cycloplegia”• Useful for eye exams, tmt of
organophosphate poisoning, antisecretory effects
• Side effects?

Scopalamine(also a cholinergic antagonist)
• Also from Belladonna• Peripheral effects
similar to atropine• More CNS effects:
– Anti-motion sickness– amnesiac

Trimethaphan(yet another cholinergic antagonist)
• Competitive nicotinic ganglion blocker
• Used to lower blood pressure in emergencies

Neuromuscular Blockers
• Look like acetylcholine• Either work as antagonists or agonists• Two flavours:
– Non-depolarizing (antagonist)• Eg: tubocurarine• Block ion channels at motor end plate
– Depolarizing (agonist)• Eg: succinylcholine• Activates receptor

Turbocurarine
• Used during surgery to relax muscles– Increase safety of
anaesthetics• Do not cross blood-
brain barrier Na+ ChannelNicotinic Receptor
ACh
CurareNa+

Succinylcholine
• Uses:– endotracheal intubations
• What is this?• Why?
– electroconvulsive shock therapy
• Problem: can cause apnea
+ + + + + + +
- - - - - -
+ + + + + +
- - - - - -
Na+
Na+
Phase I
Phase II

Adrenergic Neurons
Na+
Tyrosine
Ca++
Receptor
MAO
Dopamine
Dopa
Dopamine is converted toepinephrine

Word of the Day:
• SYMPATHOMIMETIC– Adrenergic drug which acts directly on
adrenergic receptor, activating it

Adrenergic Agonists• Direct
– Albuterol– Dobutamine– Dopamine– Isoproteranol
• Indirect– Amphetamine
• Mixed– Ephidrine

Adrenergic Receptors• Two Families:
– Alpha and Beta– Based on affinity to
adrenergic agonists• Alpha affinity:
• epinephrine≥norepinephrine>> isoproteranol
• Beta affinity:• Isoproteranol>epinephrine>
norepinephrine
Epinephrine Norepinephrine Isoproteranol
Epinephrine NorepinephrineIsoproteranol

What do these receptors do?
• Alpha 1– Vasoconstriction, ↑ BP, ↑ tonus sphincter muscles
• Alpha 2– Inhibit norepinephrine, insulin release
• Beta 1– Tachycardia, ↑ lipolysis, ↑ myocardial contractility
• Beta 2– Vasodilation, bronchodilation, ↓insulin release

Adrenergic Angonists
• Direct acting:– Epinephrine: interacts with both alpha and beta
• Low dose: mainly beta effects (vasodilation)• High dose: alpha effects (vasoconstriction)• Therapeutic uses: emerg tmt of asthma, glaucoma,
anaphyslaxis– (what about terbutaline?)

Adrenergic Agonists
• Indirect:– Cause NE release only– Example:
• Amphetamine– CNS stimulant– Increases BP by alpha effect on vasculature, beta effect on heart

Mixed-Action
• Causes NE release AND stimulates receptor• Example:
– Ephedrine:• What type of drug?• Alpha and beta stimulant• Use: asthma, nasal sprays• slower action

Adrenergic Antagonists
• Alpha blockers– Eg: Prazosin
• Selective alpha 1 blocker• Tmt: hypertension
– relaxes arterial and venous smooth muscle– Causes “first dose” response (what is this?)

Adrenergic Antagonists
• Beta Blockers• Example: Propranolol
– Non-selective (blocks beta 1 and beta 2)– Effects:
• ↓ cardiac output, vasodilation, bronchoconstriction

Adrenergic Antagonists
• Eg: Atenolol, Metoprolol– Preferentially block beta 1; no beta effects (why
is this good?)
• Partial Agonists:– Pindolol, acebutolol
• Weakly stimulate beta 1 and beta 2• Causes less bradycardia

Adrenergic Antagonists
• Eg: Nadolol– Nonselective beta blocker– Used for glaucoma
• Eg: Labetolol– Alpha AND beta blocker– Used in treating PIH

Drugs that Affect Uptake/Release
• Eg: Cocaine– Blocks Na+/K+ ATPase– Prevents reuptake of
epinephrine/norepinephrine

Treatment of Movement Disorders

What Regulates Movement?
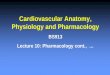
Basal Ganglia are involved

Example: Parkinsons’s Disease
• Symptoms ?

FRONTAL SECTION OF BRAINSherwood, 2001 p 145

BASAL GANGLIA cont’d
• Role of basal ganglia:1. Inhibit muscle tone throughout the body2. Select & maintain purposeful motor activity while suppressing useless/unwanted patterns
of movement3. Coordination of slow, sustained movements
(especially those related to posture & support)
4. Help regulate activity of the cerebral cortex

BASAL GANGLIA SYSTEM
Feedback loops - complex - form direct & indirect pathways
- balance excitatory & inhibitory activities
Neurotransimitters:
Excitatory - ACh Inhibitory - dopamine glutamate GABA

DOPAMINE
• major NT regulating subconscious movements of skeletal muscles
• majority located in the terminals of pathway stretching from the neuronal cell bodies in SNc to the striatum
• generally inhibits the function of striatal neurons & striatal outputs
• when dopamine production is , a chemical imbalance occurs affecting movement, balance and gait

PATHOPHYSIOLOGY OF PARKINSON’S DISEASE
• Major pathological features:1. Death of dopamine producing cells in the SNc
leads to overactivation of the indirect pathway2. Presence of Lewy bodies –small eosinophilic
inclusions found in the neurons of SNcResults in:- degeneration of the nigrostriatal
pathway - decreased thalamic excitation of the
motor cortex

4. Drug of Choice: LEVODOPA
Why is it used? - virtually all pt’s with PD show a response to
levodopa - improves quality of life - in use since 1960’s - easy to administer (non-invasive) - relatively inexpensive - useful in diagnosing PD
• Mechanism of action: is a precursor to dopamine helps restore the balance of dopamine in striatum
–most effective in combo with Carbidopa ( ’s levodopa’s peripheral conversion to dopamine)

5. OTHER APPROACHES TO TREATMENT
• Pharmacological:– Dopamine agonists: ie. Bromocriptine or pergolide
mesylate– Selective inhibitor of type B monoamine
oxidase: ie.Selegiline– Antivirals: ie. Amantadine– Anticholinergics: ie. Trihexyphenidyl– COMT inhibitors: ie. Entacapone

APPROACHES cont’d
• Surgical:• Pallidotomy & Thalotomy:
– microelectrode destruction of specific site in the basal ganglia
• Deep brain stimulation: – electrode implantation with external pacemaker
• Fetal nigral transplantation:– Implantation of embryonic dopaminergic neurons into
the substantia nigra for growth and supply of dopamine
Recommended