
Lean Six Sigma in NICU Healthcare
What can NICU nurses learn from industry practices?
Lynn E. Bayne, PhD, APRN, NNP-BC Neonatal Nurse Practitioner Nursing Research Facilitator
Disclosure Disclaimer
“I have no relevant financial relationships to disclose.”
On the other hand, I do work for 2 great facilities!
Objectives
Learner will be able to: Identify key databases for comparing your
institution’s NICU to others. List six keys steps in successfully
identifying, conducting, and completing a quality improvement project.
Name three improvement opportunities in their NICU amenable to QI methods to achieve better outcomes.
Begin to formula a project plan that you want to tackle starting now!
Critical Concepts
Things have changed! Patients are customers… Families do matter…
What matters in 2015 and beyond Transparency Translational science Accountability
So how does one get started?
Getting Started
Benchmarking Internal
Day vs night shift NICU vs. PICU
External Local Regional National
Reasons Hospitals Need Benchmarking
Useful for: Making recommendations for creating safe
staffing and scheduling. Guiding decisions about how best to
allocated workforce and capital resources. Providing a structured approach where
hospitals can learn from one another. From Josie’s Story….. http://www.hopkinsmedicine.org/armstrong
_institute/

More Reasons Hospitals Need Benchmarking
Useful for: Helping to cultivate a practice environment
conducive to evidence-based practice and quality improvement.
Fostering transparency such that external benchmarks disclosed and institutions competitive advantages or weaknesses.
Sharing best practices associated with favorable outcomes.
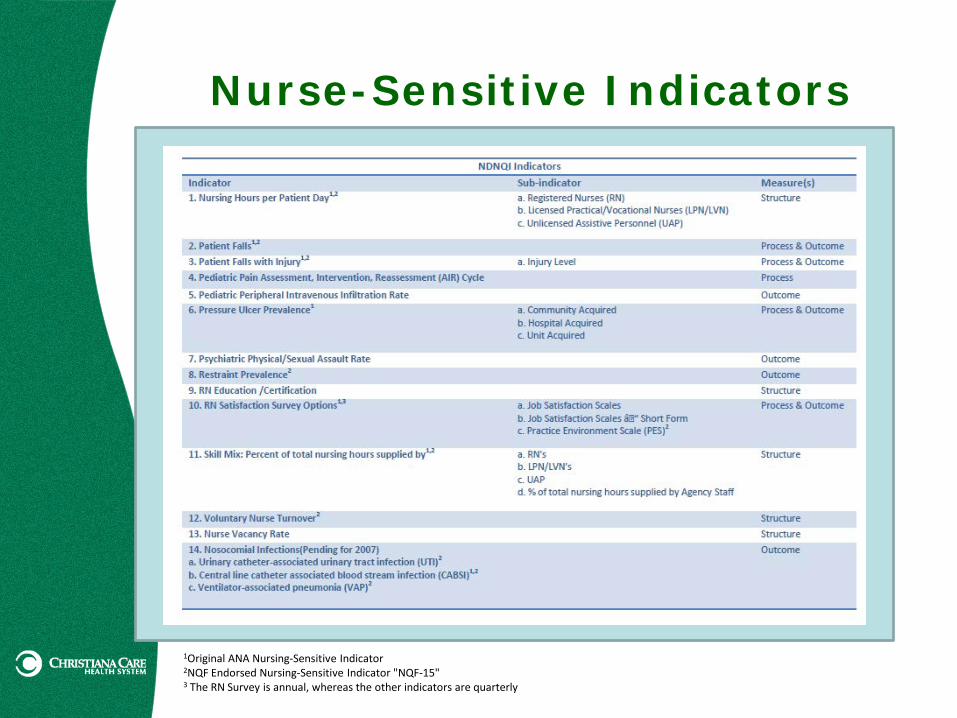
Nurse-Sensitive Indicators
1Original ANA Nursing-Sensitive Indicator 2NQF Endorsed Nursing-Sensitive Indicator "NQF-15" 3 The RN Survey is annual, whereas the other indicators are quarterly
IOM Six Aims for 21st Century Health Care System
The six aims are to: Achieve the highest level of patient safety Ensure integration of EBP into clinical care Promote reliable and valid measurement of
core measures and performance outcomes Guarantee timely accessibility of all
healthcare services Support efficiency of care Eliminate healthcare disparities in
provision of care
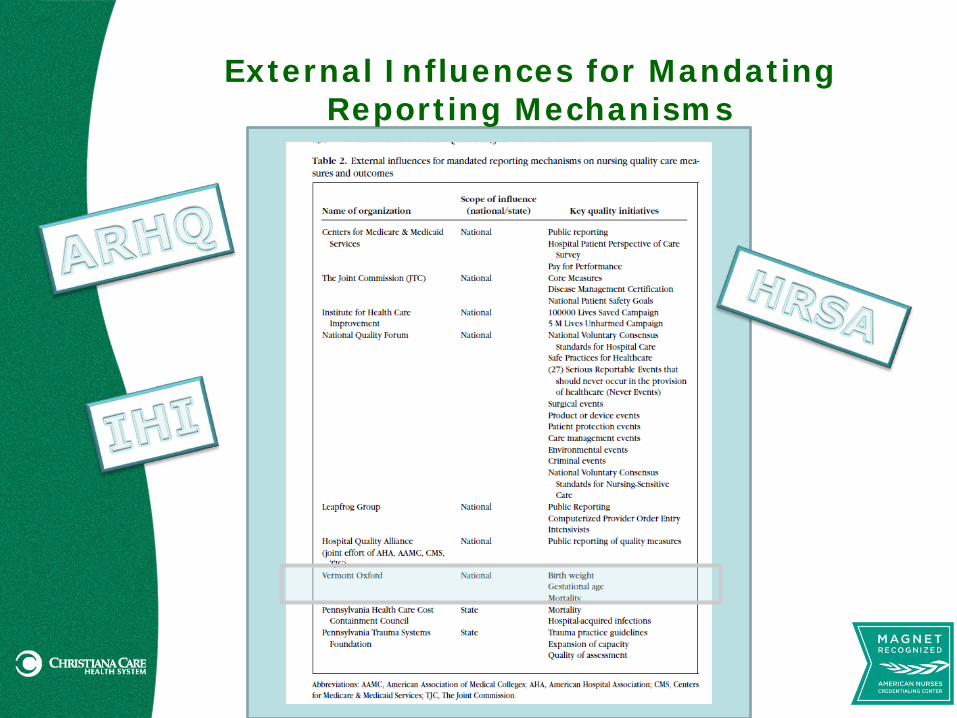
External Influences for Mandating Reporting Mechanisms
NICU-specific Benchmarking
Vermont-Oxford Network (VON) https://public.vtoxford.org/
California Perinatal Quality Care Collaborative https://www.cpqcc.org/
Children’s Hospitals Association (CHA) Formerly known as National Association of
Children’s Hospitals and Related Institutions (NACHRI)
https://www.childrenshospitals.org/
Benchmarking in the NICU
CPQCC 132 member
hospitals; 90% neonates in CA NICUs
Initiatives: HAI Breastmilk
Nutrition DR
Management
VON 909 member
hospitals in US; > 1000 member hospitals globally
VON booklet 2015 VON
Patient Data Booklet

So how does one start this journey?
(And how do you set priorities?)
Getting Better….
Reducing admission hypothermia Reducing unplanned extubations Reducing LOS for NAS Reducing door-to-drug
antibiotics Reducing HAI
CLABSI 40,000 pediatric patients/year ~ 100 die of sepsis
Optimizing appropriate use of oxygen through SpO2 targeting

In Search of Excellence
Improving compliance with procedural sedation during emergent intubation
Improving use of nonpharmacological interventions during procedures
Improving breast milk administration Use of BrM in general MBM Commitment to post-hospital BrF
NO Complications Increasing timeliness of
immunization(s) Reducing noise in the NICU Reducing time-to-first parental
hold Improving neonatal
transport/standardized handoff Condition, lines/tubes, medication Both sides of transport
Referring & accepting facilities
Improving discharge processes Decreasing re-admission rates
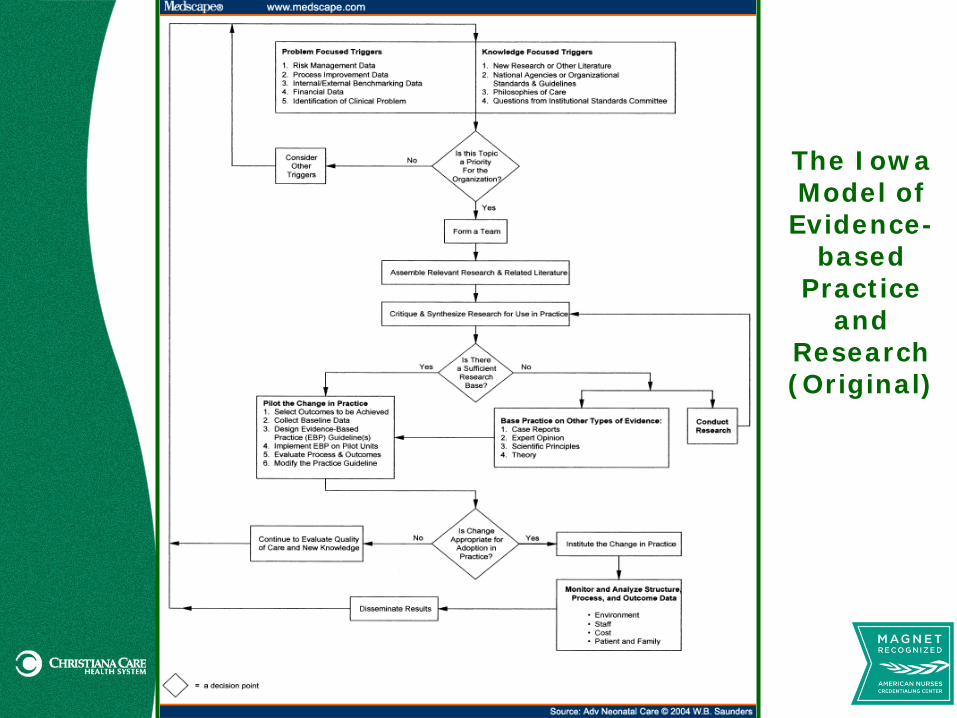
The Iowa Model of
Evidence- based
Practice and
Research (Original)
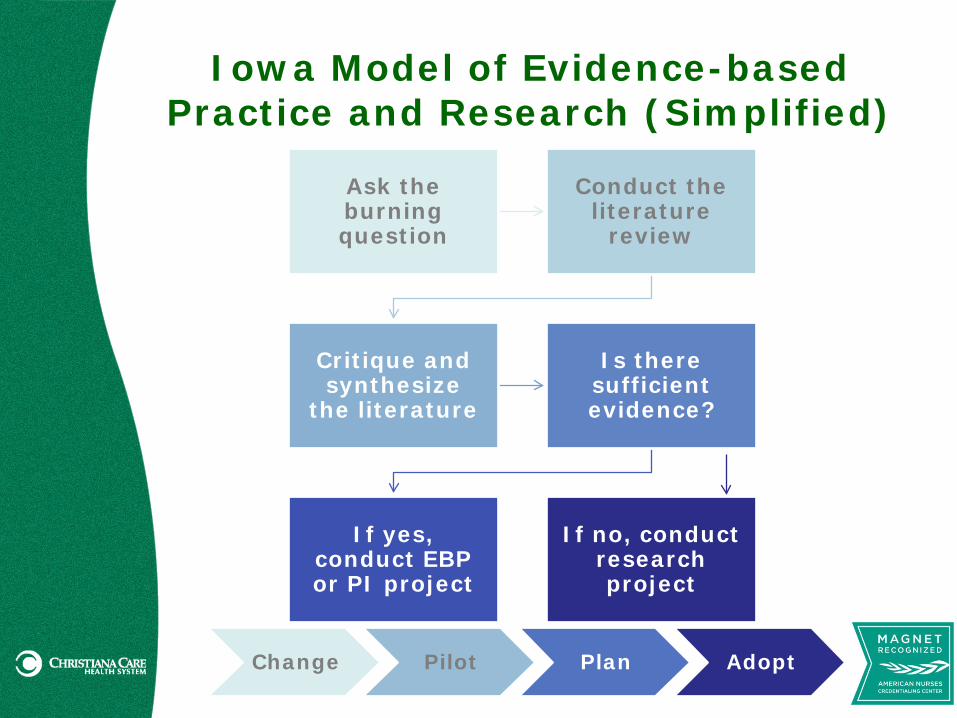
Iowa Model of Evidence-based Practice and Research (Simplified)
Ask the burning question
Conduct the literature
review
Critique and synthesize
the literature
Is there sufficient evidence?
If yes, conduct EBP or PI project
If no, conduct research project
Change Pilot Plan Adopt

QUALITY IMPROVEMENT: TOOLS & METHODS
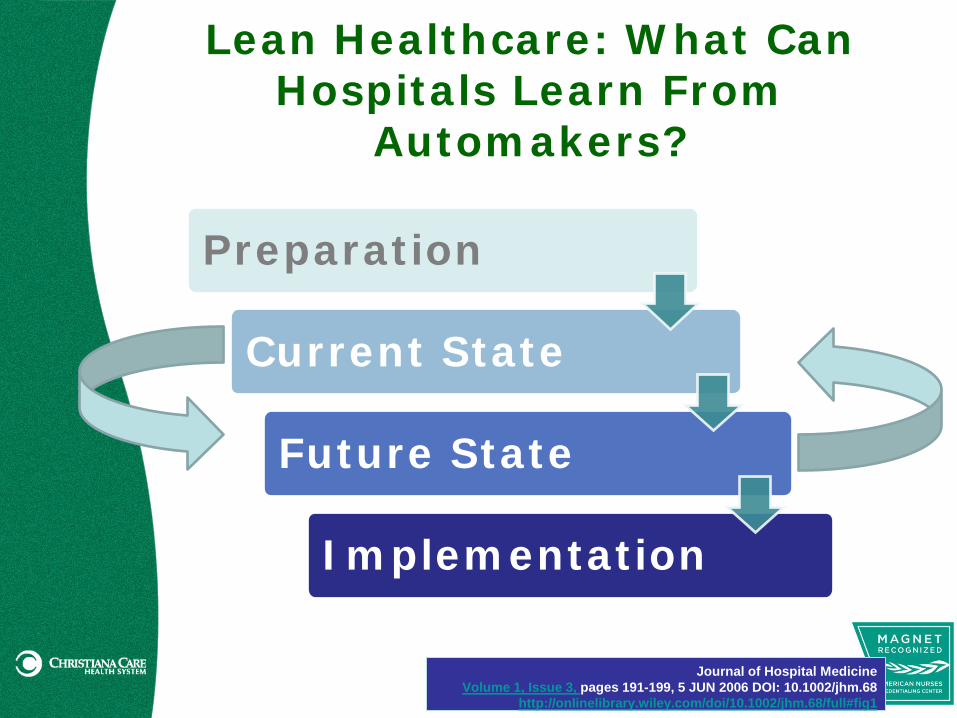
Lean Healthcare: What Can Hospitals Learn From
Automakers?
Preparation
Current State
Future State
Implementation
Journal of Hospital Medicine Volume 1, Issue 3, pages 191-199, 5 JUN 2006 DOI: 10.1002/jhm.68
http://onlinelibrary.wiley.com/doi/10.1002/jhm.68/full#fig1
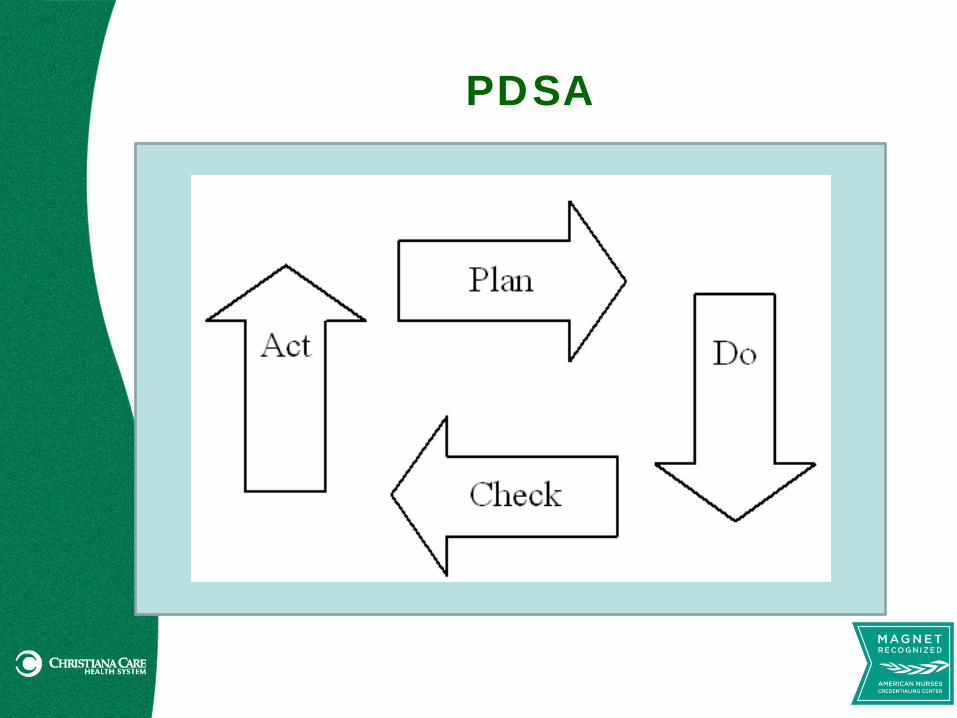
PDSA
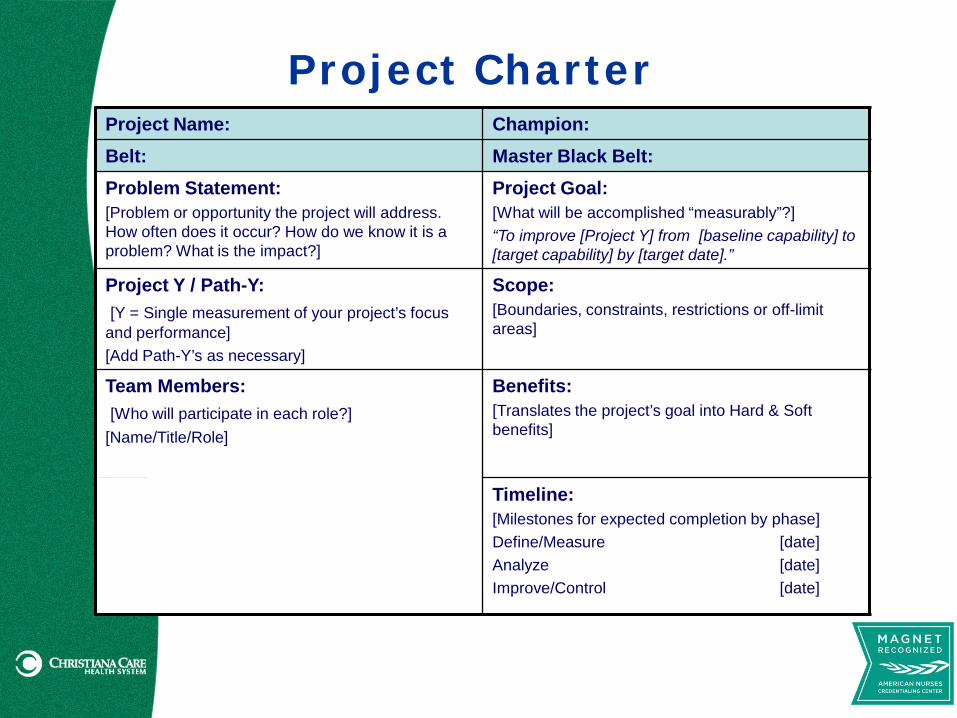
Project Charter Project Name: Champion: Belt: Master Black Belt: Problem Statement: [Problem or opportunity the project will address. How often does it occur? How do we know it is a problem? What is the impact?]
Project Goal: [What will be accomplished “measurably”?] “To improve [Project Y] from [baseline capability] to [target capability] by [target date].”
Project Y / Path-Y: [Y = Single measurement of your project’s focus and performance] [Add Path-Y’s as necessary]
Scope: [Boundaries, constraints, restrictions or off-limit areas]
Team Members: [Who will participate in each role?] [Name/Title/Role]
Benefits: [Translates the project’s goal into Hard & Soft benefits]
Timeline: [Milestones for expected completion by phase] Define/Measure [date] Analyze [date] Improve/Control [date]
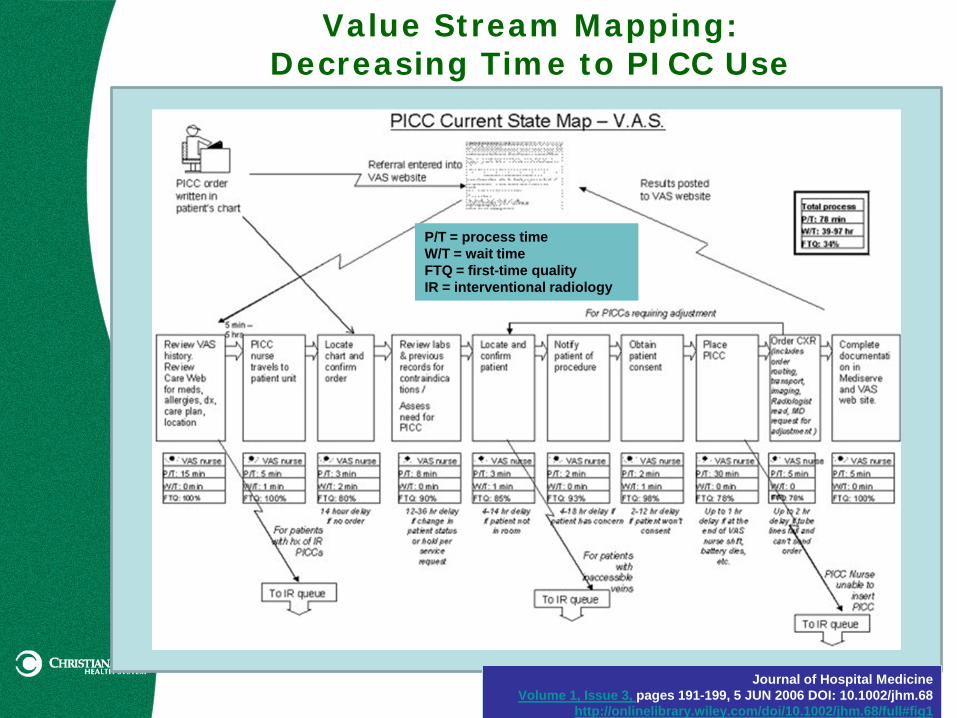
Value Stream Mapping: Decreasing Time to PICC Use
Journal of Hospital Medicine Volume 1, Issue 3, pages 191-199, 5 JUN 2006 DOI: 10.1002/jhm.68
http://onlinelibrary.wiley.com/doi/10.1002/jhm.68/full#fig1
P/T = process time W/T = wait time FTQ = first-time quality IR = interventional radiology
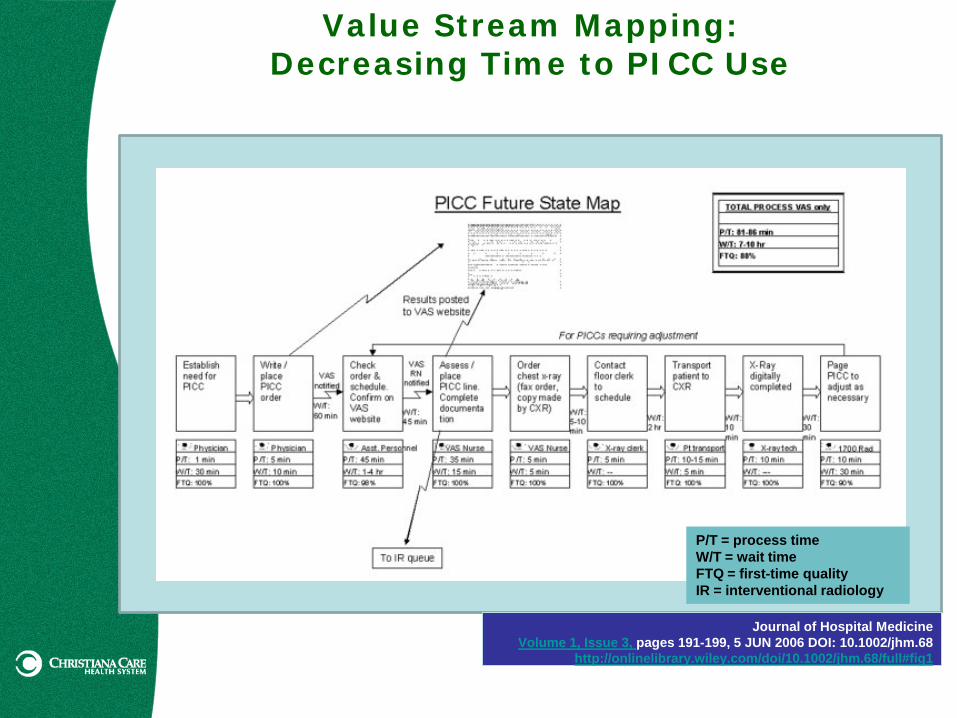
Value Stream Mapping: Decreasing Time to PICC Use
Journal of Hospital Medicine Volume 1, Issue 3, pages 191-199, 5 JUN 2006 DOI: 10.1002/jhm.68
http://onlinelibrary.wiley.com/doi/10.1002/jhm.68/full#fig1
P/T = process time W/T = wait time FTQ = first-time quality IR = interventional radiology

Identifying Ideas/Problems…the Starting
Point(s) Reducing admission hypothermia Reducing unplanned extubations Optimizing appropriate use of
oxygen through SpO2 targets Reducing procedural pain
PICC and Chose Carefully Reducing LOS for NAS Reducing time to 1st
administration of antibiotics Door-to-drug
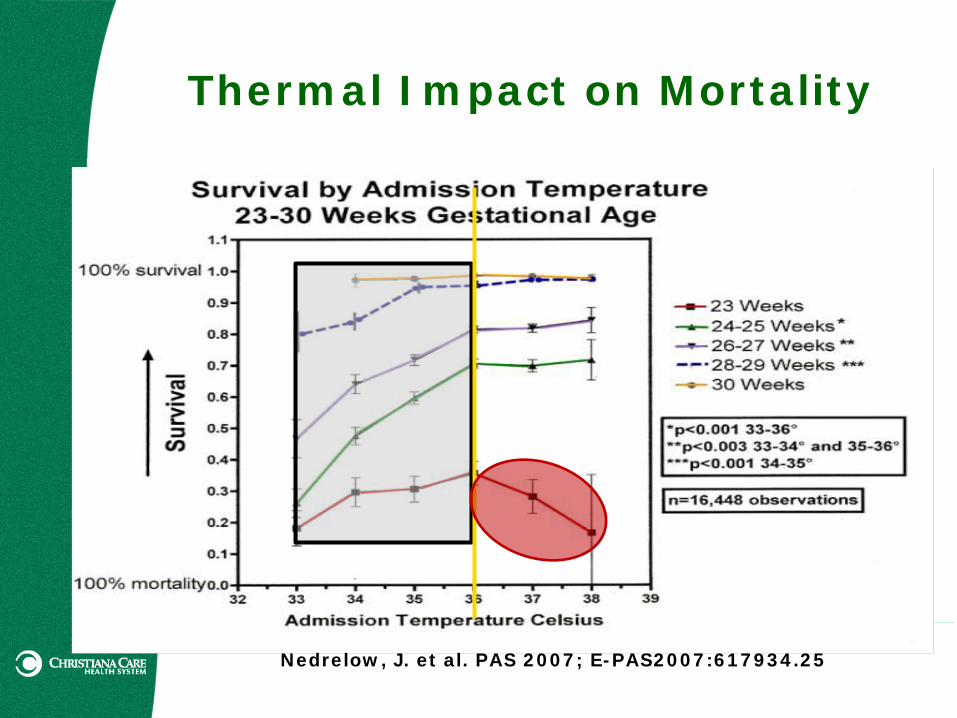
Thermal Impact on Mortality
Nedrelow, J. et al. PAS 2007; E-PAS2007:617934.25
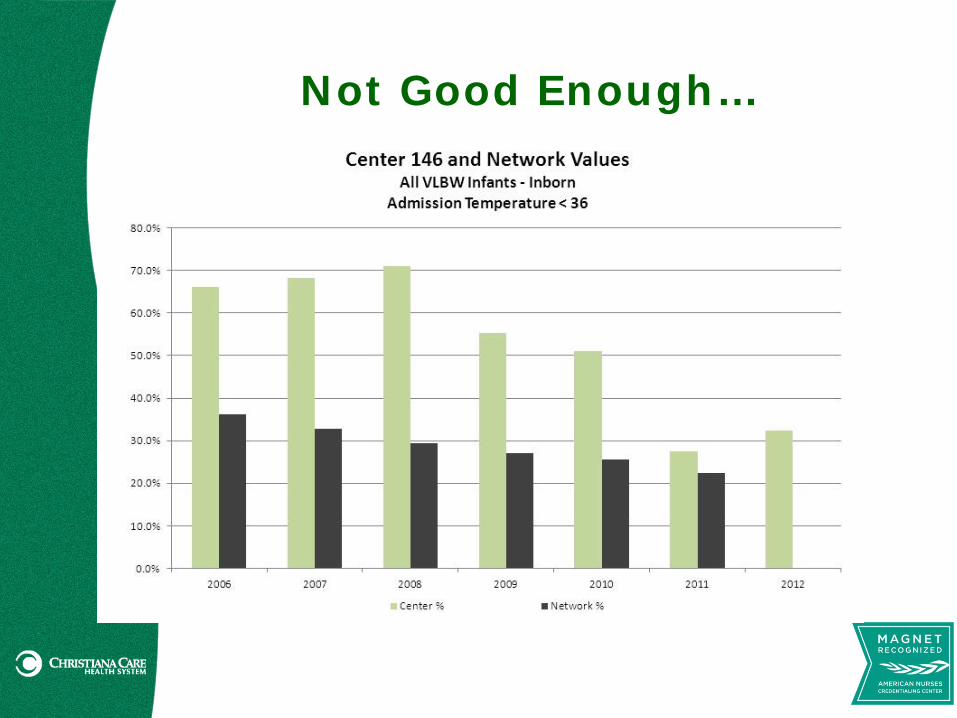
Not Good Enough…
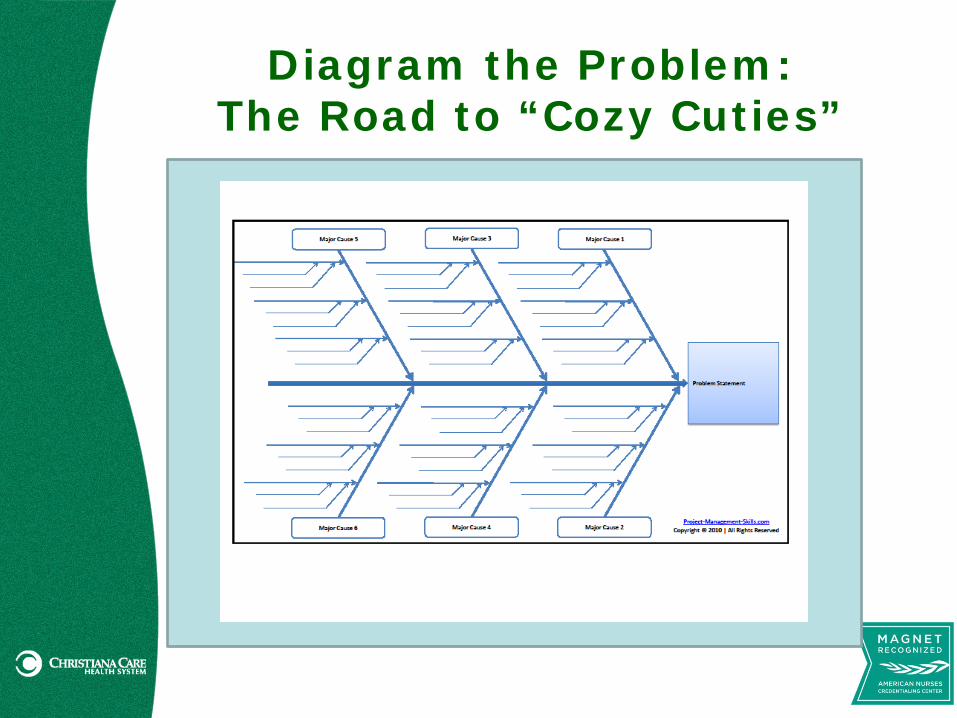
Diagram the Problem: The Road to “Cozy Cuties”
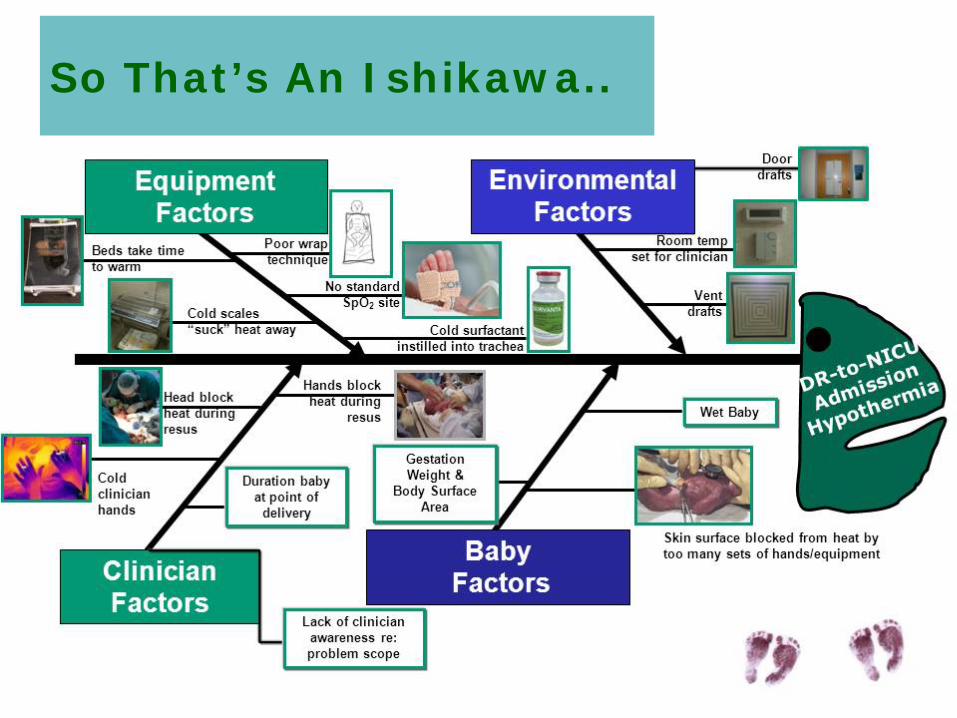
So That’s An Ishikawa..
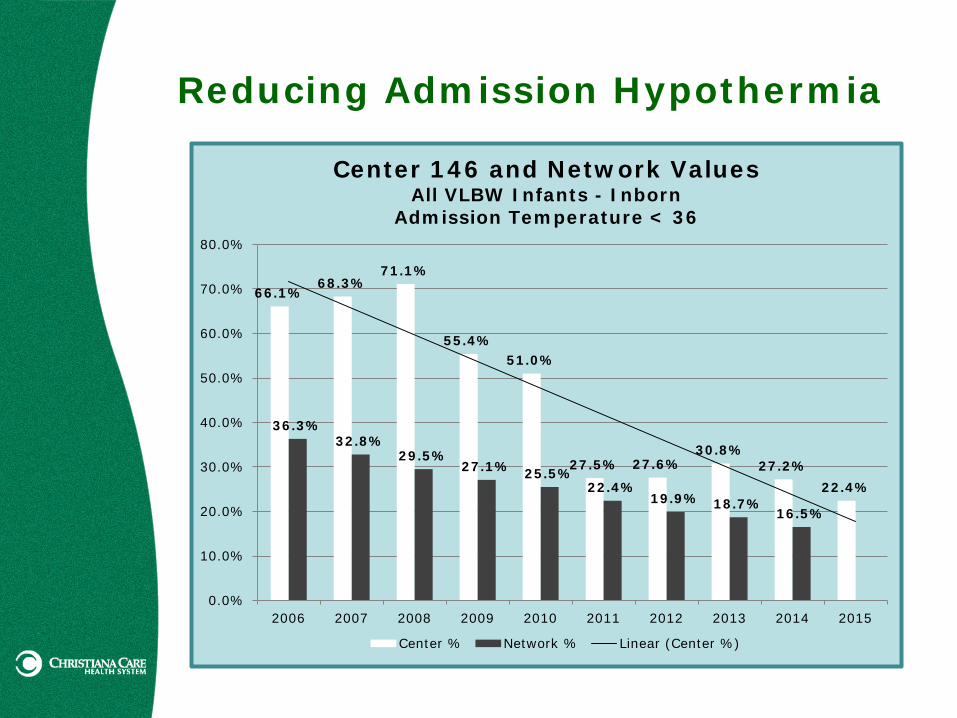
Reducing Admission Hypothermia
66.1% 68.3%
71.1%
55.4% 51.0%
27.5% 27.6% 30.8%
27.2% 22.4%
36.3% 32.8%
29.5% 27.1% 25.5%
22.4% 19.9% 18.7%
16.5%
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
80.0%
2006 2007 2008 2009 2010 2011 2012 2013 2014 2015
Center 146 and Network Values All VLBW Infants - Inborn
Admission Temperature < 36
Center % Network % Linear (Center %)
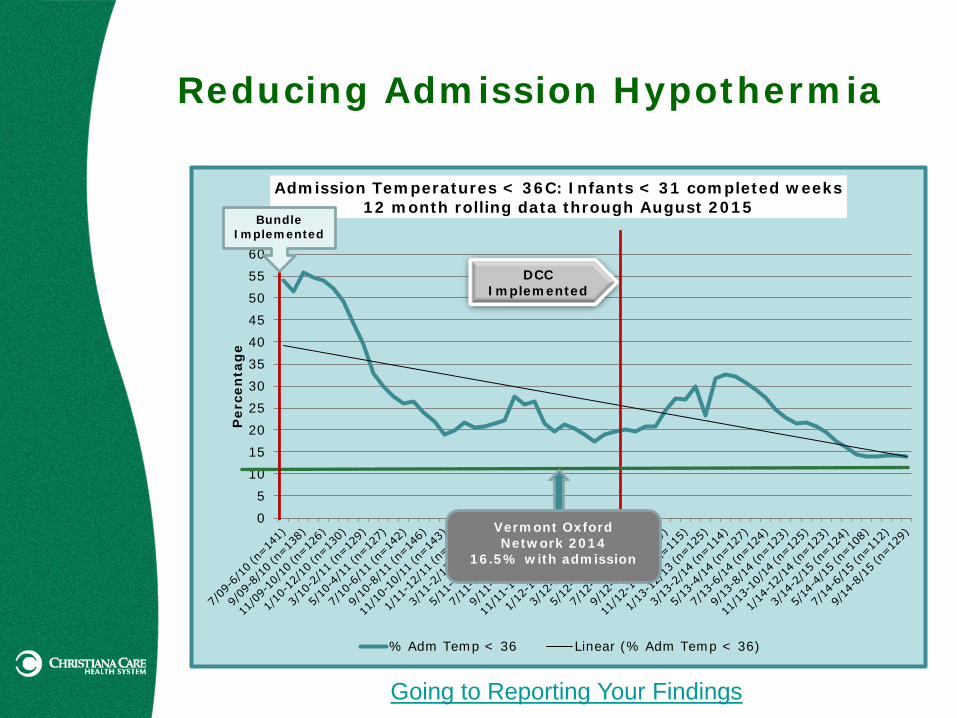
Reducing Admission Hypothermia
0 5
10 15 20 25 30 35 40 45 50 55 60
Per
cen
tag
e
Admission Temperatures < 36C: Infants < 31 completed weeks 12 month rolling data through August 2015
% Adm Temp < 36 Linear (% Adm Temp < 36)
DCC Implemented
Vermont Oxford Network 2014
16.5% with admission
Bundle Implemented
Going to Reporting Your Findings
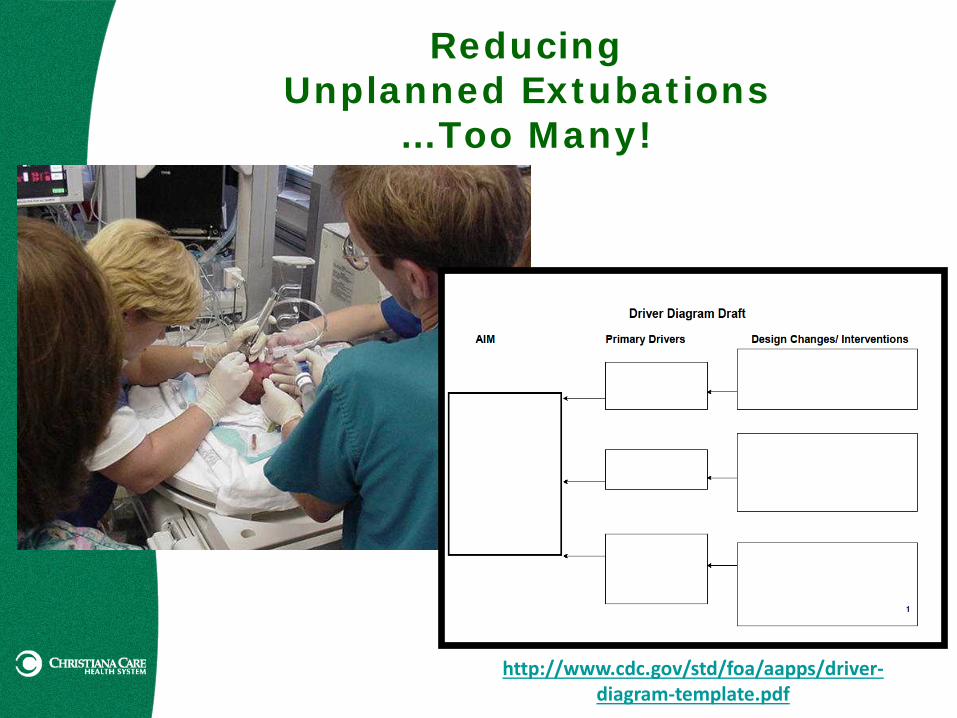
Reducing Unplanned Extubations
…Too Many!
http://www.cdc.gov/std/foa/aapps/driver-diagram-template.pdf
Data graphs pending; Findings shared at Hot Topics!
Going to Reporting Your Findings
Reducing Unplanned Extubations
…Too Many!
Optimizing Appropriate Use of O2 through SpO2 Target
Data graphs pending; Findings shared at Hot Topics!
Going to Reporting Your Findings
Reducing Procedural Pain …PICC & Choose Carefully
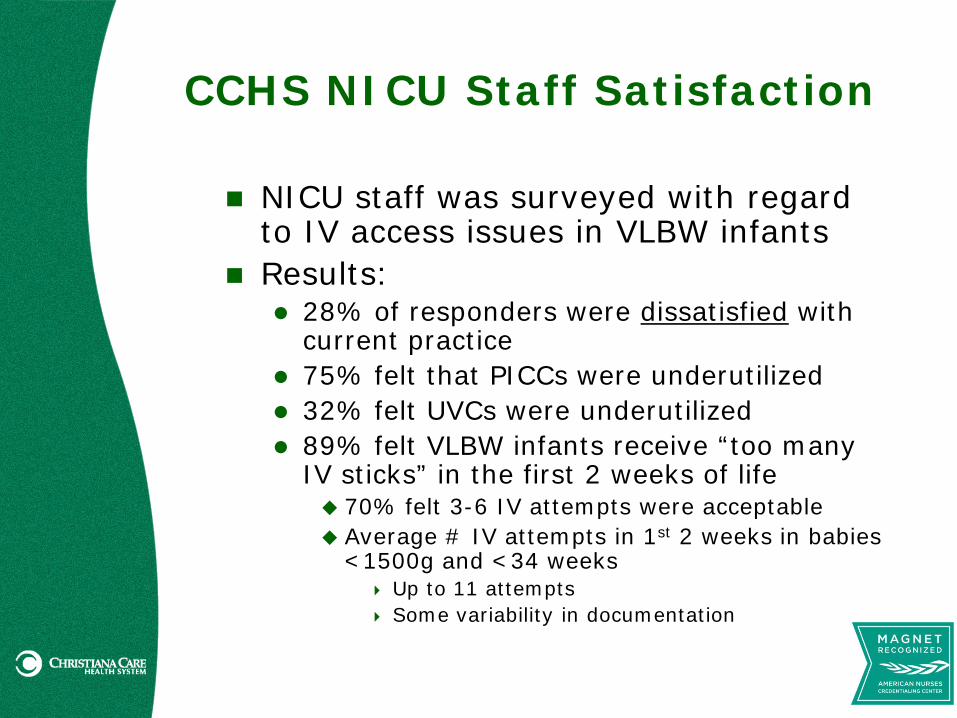
CCHS NICU Staff Satisfaction
NICU staff was surveyed with regard to IV access issues in VLBW infants
Results: 28% of responders were dissatisfied with
current practice 75% felt that PICCs were underutilized 32% felt UVCs were underutilized 89% felt VLBW infants receive “too many
IV sticks” in the first 2 weeks of life 70% felt 3-6 IV attempts were acceptable Average # IV attempts in 1st 2 weeks in babies
<1500g and <34 weeks Up to 11 attempts Some variability in documentation
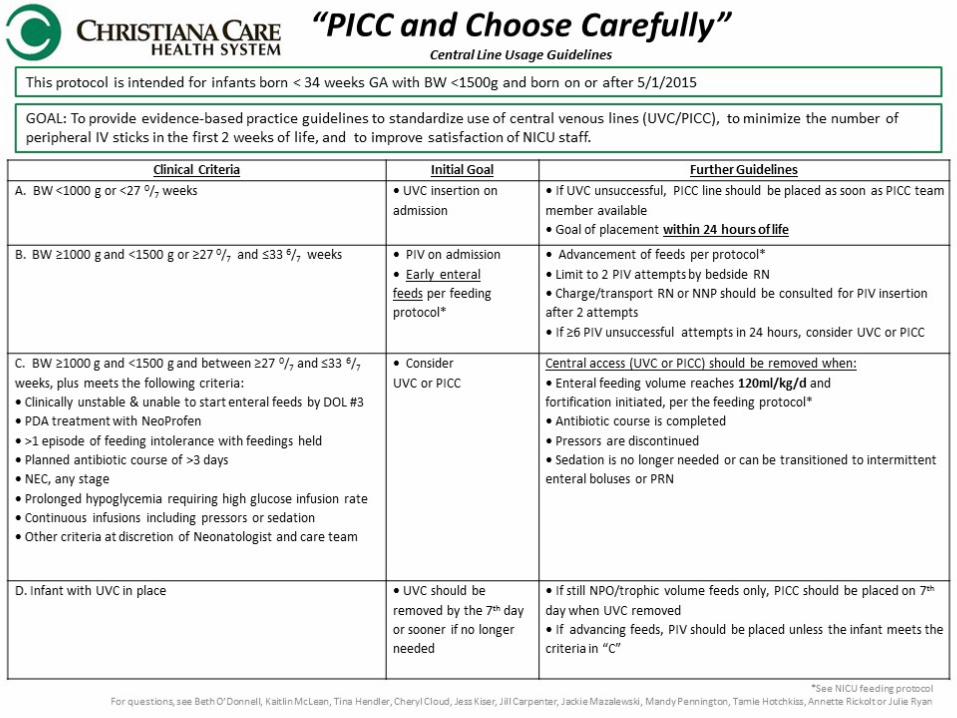
Reducing Procedural Pain …PICC & Choose Carefully
Going to Reporting Your Findings
Reducing LOS for NAS …Too Long!
Data graphs pending; Findings shared at Hot Topics!
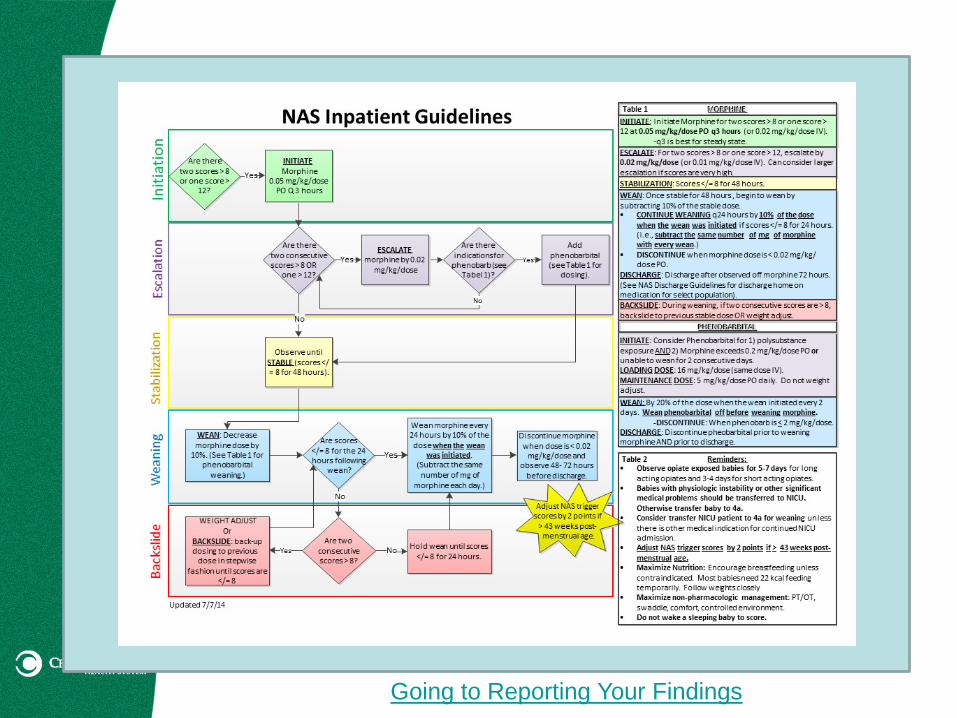
Going to Reporting Your Findings
Reducing Time to 1st Antibiotics
Data graphs pending; Findings shared at Hot Topics!
Going to Reporting Your Findings

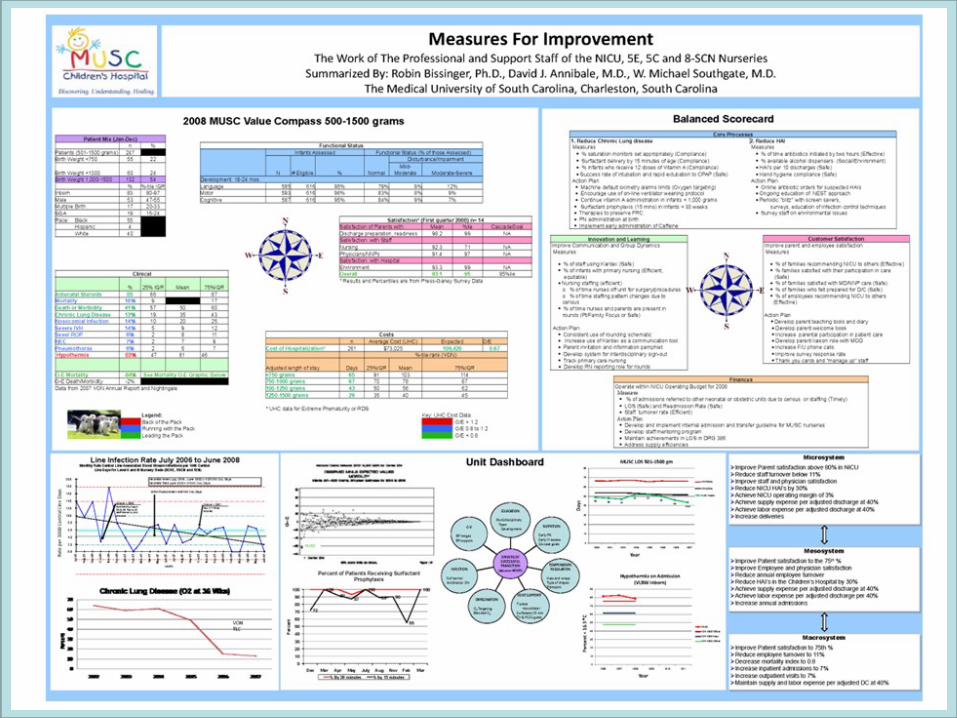
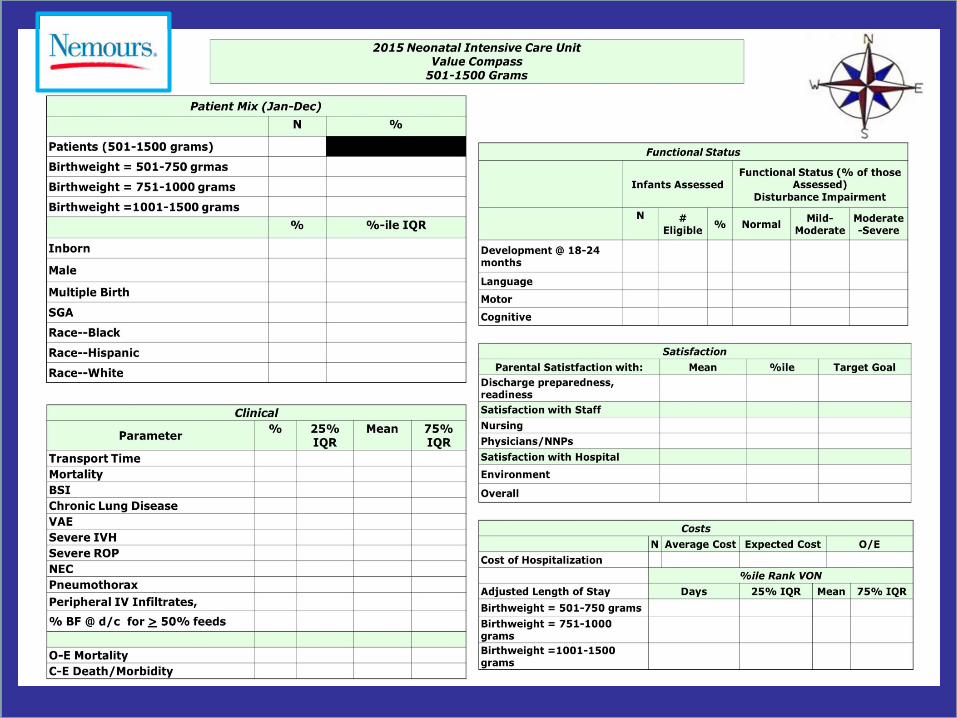
Reporting Your Findings Dashboards
Derived from airplane cockpits & automobile displays
Developed for business applications Display real-time or close to real-time data
Report cards Derived from education Display real-time or close to real-time data
Key qualities of a great dashboard/report card Contain meaningful outcomes and
measures Map to unit and/or organizational goals May be interdisciplinary or service line

Reporting Your Findings
Conclusion
Your journey starts today (if it hasn’t already started)!
Celebrate your successes Tweak where you can The line between research and
QI/PI is sometimes gray… So talk with your IRB!
..and never forget why we do what we do!

Permissions on file
References
Mateo, M.A. & Kirchoff, K.T. (1999). Using and Conducting Nursing Research in the Clinical Setting. Philadelphia, PA: WB Saunders Company.
Polit, D.F. & Beck C.T. (2010). Nursing Research Principles and Methods. Philadelphia, PA: Lippincott.
Doran, D.M. (2003). In Nursing Sensitive Outcomes: State of the Science. Sudbury, MA: Jones and Bartlett.
Albanese, M.P., Evans, D.A., Schantz, C.A., Bowen, M., Moffa, J.S., Piesieski, P., & Polomano, R.C. (2010). Engaging clinical nurses in quality and performance improvement activities. Nurs Admin Q, 34(3), pp. 226-245.
Recommended

















