Laparoscopic Laparoscopic Assisted Assisted
Anorectal Pull-Anorectal Pull-throughthroughKeith GeorgesonKeith Georgeson
Professor of SurgeryProfessor of Surgery
University of Alabama School of University of Alabama School of MedicineMedicine

Pre-operative EvaluationPre-operative Evaluation
Proximal sigmoid colostomyProximal sigmoid colostomy Careful perineal evaluationCareful perineal evaluation Distal colostogram under pressureDistal colostogram under pressure X-rays of spine and pelvisX-rays of spine and pelvis

Indications for SurgeryIndications for Surgery
All patients with high anorectal All patients with high anorectal malformationsmalformations
Some patients with intermediate Some patients with intermediate ARMsARMs
No patients with low ARMsNo patients with low ARMs Newborn patients if level can be Newborn patients if level can be
determineddetermined

Patient PositioningPatient Positioning
Supine Supine Cross tableCross table End of tableEnd of table Body but not head elevated on Body but not head elevated on
sheetssheets Firmly taped in positionFirmly taped in position

EquipmentEquipment One 5mm trocar, two 4mm trocarsOne 5mm trocar, two 4mm trocars Hook cautery-3mmHook cautery-3mm Bowel grasper-3mmBowel grasper-3mm Scissors-3mmScissors-3mm Needle driver-3mmNeedle driver-3mm Large monofilament sutureLarge monofilament suture Loop ligature-2Loop ligature-2 Sleeved, Varess needle trocars (inserts Sleeved, Varess needle trocars (inserts
5,10,12)5,10,12) Open minor instrument trayOpen minor instrument tray

LAARPLAARP
TechniqueTechnique

Goals of Lap-Assisted Goals of Lap-Assisted Anorectal Pull-ThroughAnorectal Pull-Through
Avoid dividing and weakening Avoid dividing and weakening external sphinctersexternal sphincters
Precise placement of rectum Precise placement of rectum through external sphinctersthrough external sphincters
Diminish perirectal scarringDiminish perirectal scarring Potential development of primary Potential development of primary
procedure avoiding colostomyprocedure avoiding colostomy

ColonColon
BladderBladder
Anorectal MalformationsAnorectal Malformations


VasVas
UreterUreter
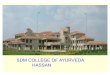
Laparoscopic Pull-throughLaparoscopic Pull-through


RectumRectum
BladderBladder
ClipClip
Laparoscopic Pull-throughLaparoscopic Pull-through
Recto-Urethral FistulaRecto-Urethral Fistula









Laparoscopic Pull-throughLaparoscopic Pull-through

Alternative ApproachesAlternative Approaches



Elements for Fecal Continence
Internal sphincter competenceInternal sphincter competence
Rectal reservoirRectal reservoir
Anorectal angleAnorectal angle
Rectosigmoid motilityRectosigmoid motility

Elements for Fecal Elements for Fecal ContinenceContinence
Sensation of rectal distentionSensation of rectal distention
Anoderm anal-lined canalAnoderm anal-lined canal
Anorectal reflexAnorectal reflex
External sphincter competenceExternal sphincter competence
Stool consistencyStool consistency

PSARPPSARP
PSARP does not provide superior PSARP does not provide superior fecal continence when compared to fecal continence when compared to other pull-through operations for high other pull-through operations for high imperforate anusimperforate anus
Nulder, et alNulder, et al EJPS EJPS19951995
Bliss, Tapper, et alBliss, Tapper, et al JPS JPS 19961996
ShandlingShandling JPSJPS 19961996

Anorectal Function after Anorectal Function after Posterior Sagital Posterior Sagital AnorectoplastyAnorectoplasty
Better anatomical positioning than Better anatomical positioning than older conventional operationsolder conventional operations
Increased constipationIncreased constipation Manometry is similarManometry is similar Long-term function is similarLong-term function is similar Most patients need bowel Most patients need bowel
managementmanagementTsuji et al, JPS Tsuji et al, JPS
37,200237,2002



Anorectal MalformationsAnorectal Malformations
Eventual continence is related to Eventual continence is related to a positive anorectal reflexa positive anorectal reflex
Tsuji et al, JPS 37,2002Tsuji et al, JPS 37,2002


Positive ARRPositive ARR
LARLAR PSARPPSARP
8/9 = 89%8/9 = 89% 4/13 = 30.8%4/13 = 30.8%
P = 0.0001P = 0.0001
Lin, et alLin, et al

Lap Assisted Pull-throughLap Assisted Pull-throughTime to Develop ARRTime to Develop ARR
LAPLAP PSARPPSARP4.9 4.9 ++ 1.2 months 1.2 months 10.1 10.1 ++ 2.5 months 2.5 months
Lin, et alLin, et al



Laparoscopic Primary Laparoscopic Primary Pullthrough for Pullthrough for
Hirschsprung’s diseaseHirschsprung’s disease
ConventionalConventional LaparoscopicLaparoscopicstaged pullthroughstaged pullthroughprimary pullthroughprimary pullthrough

Mid-term Analysis for High Mid-term Analysis for High Anorectal MalformationsAnorectal Malformations
No difference in centrality of pull-No difference in centrality of pull-through between Pena and through between Pena and GeorgesonGeorgeson
Muscle groups similarMuscle groups similar Continence somewhat better in G Continence somewhat better in G
groupgroup G=15, P=9G=15, P=9


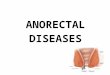
Laparoscopic Pull-throughLaparoscopic Pull-through
Surgical Anal CanalSurgical Anal Canal

Lap-Assisted Pull-ThroughLap-Assisted Pull-Through ComplicationsComplications
Urethral perforation Urethral perforation
Diverticulum around fistular clipDiverticulum around fistular clip
Rectal prolapseRectal prolapse
Missed muscle complexMissed muscle complex

Tips/TricksTips/Tricks
Hitch the bladder wall with a U-stitchHitch the bladder wall with a U-stitch Convergence of the vas deferens visually Convergence of the vas deferens visually
guides the surgeon to the prostateguides the surgeon to the prostate Don’t repair small nicks in the smooth muscleDon’t repair small nicks in the smooth muscle Open the rectal fistula to confirm it’s junction Open the rectal fistula to confirm it’s junction
with the urethrawith the urethra Push the plastic guide of the loop ligature to Push the plastic guide of the loop ligature to
the distal side of the rectourethral fistulathe distal side of the rectourethral fistula The anorectal angle is straight with the The anorectal angle is straight with the
thighs flexedthighs flexed

Fed on first or second post-operative Fed on first or second post-operative
dayday
Graduated anorectal dilation started Graduated anorectal dilation started
in two weeksin two weeks
Colostomy closure in three monthsColostomy closure in three months
Laparoscopic Pull-throughLaparoscopic Pull-through
Postoperative ManagementPostoperative Management

Goals of Lap-Assisted Goals of Lap-Assisted Anorectal Pull-ThroughAnorectal Pull-Through
Avoid dividing and weakening Avoid dividing and weakening external sphinctersexternal sphincters
Precise placement of rectum Precise placement of rectum through external sphinctersthrough external sphincters
Diminish perirectal scarringDiminish perirectal scarring Potential development of primary Potential development of primary
procedure avoiding colostomyprocedure avoiding colostomy

Lap Assisted Pull-throughLap Assisted Pull-through
Anatomically soundAnatomically sound
Leaves muscles intactLeaves muscles intact
Higher incidence of ARRHigher incidence of ARR
Better rectal complianceBetter rectal compliance
Needs long term follow-upNeeds long term follow-up

Recommended