June 3, 2009Palliative Care Team
Drs. St. Godard, Loiselle, Hohl and Pilkey

ObjectivesBy the end of the hour the learner will be
able to:Define neuropathic painList at least 2 types of Pain receptorsList at least 4 different types of adjuvant pain
medicationsList the mechanisms of action, benefits, and
side-effects of these 4 medicationsList 2 new/different adjuvant pain medications

Talk OutlineCase Study – Dr. Ted St. Godard & Dr. Joel Loiselle
Pathophysiology of Neuropathic Pain – Dr. Jana Pilkey
Adjuvant Medications – Dr. Chris Hohl
What’s new/different in Neuropathic Pain – Dr. Jana Pilkey

HistoryMs. G. D. 55 y.o with breast cancerMets to bonePain to left arm

History2 week hx of worsening painMid back – dull ache, PressureBurning to L hand and arm
Since 1997brachial plexus neuropathy
“Pins and needles”“Like dipped in acid”Morphine for 4 weeks not helping

Cancer HistoryBreast cancer dx 1997Lumpectomy, tamoxifen x 2 yrsMastectomy 1999 and LN dissectionOophorectomy 1999Multiple courses of chemo2008- mets to c-spine, ribs, sternum.Sept 2008 – Rx to spinePhx: PUD

Physical Exam & InvestigationsTemp 37.2Hr 100Rr 18Sao2 – 90% on RABP 150/88Lab work normal throughout

Course in HospitalAdmission orders:
Methadone 5mg bidDex 10mg bidPariet 20mg po odDilaudid 8 mg subcut q4h and q1prnFentanyl 50 per IPP

Course in HospitalDec 30
Myoclonus noticed – hydratedRotated to fentanyl patchMethadone increased
Jan 14CT head – mets to R cerebellum and R frontal
lobePain better- on methadone 40 bid, dex 8 bidStarts 12 rdtx to whole brain

Course in HospitalJan 27 Pain Crisis
Severe excruciating burning painFrom neck to top of R shoulderCrying, screamingBT HM ineffectiveSlept with 5mg versedMethadone increasedKetamine added 2.5 mg subcut tidPregabalin added 50mg bidLidocaine 2% gel to shoulder qid prn

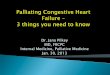
Potentially useful Peripheral Nerve Block in this Case
Interscalene block-Performed at root level -“Single shot” -only lasts 12 h.-Catheter techniques difficult to maintain (displacement).-Disease extent limits anesthetic flow.-Risk of bleeding /epidural hematoma is prohibitive in this case.

Neuraxial (Intraspinal) blocksEpidural:comparable to bilateral
peripheral nerve block catheter outside dura would be placed at C7/T1
Intrathecal = Spinal catheter enters CSF in
lumbar cisterncan be guided to high
thoracic level as required for upper limb pain

Contraindications to Neuraxial Analgesia in this Case- Extent of Disease involving C-spine:
- Risk of epidural hematoma if needle at C7-T1.- Poor CSF flow impedes spread of analgesics
- Brain Metastasis:- Posterior Fossa- increased risk of “coning”- Relative contraindication
Remember coagulopathy (Plt <100; INR >1.3) and need for ongoing anticoagulation are contraindications.

Course in HospitalConsult to Dr J. Loiselle
Nerve-block or epidural too risky given fragility of spine and cerebellar mets
Jan 28Pain continuesOn Methadone 60mg bidStarts fentanyl 50mcg/hr IVHM stopped – twitchingKetamine 5 mg subcut tid

Course in HospitalJan 28
Family concerned about sedation on fentanylJan 29
RR 7 - fentanyl stopped, Pain again severeFentanyl IV not restarted at family requestAtivan started
Jan 30 – Mini Case conferenceKetamine IV @ 2.5mg/hrGabapentin being lowered

Course in HospitalJan 31-Feb 5 – good pain controlFeb 6 – weepy and tired, pain with movementFeb 9 – increase in ketamine IV 3.52mg/hrFeb 13 – increase in ketamine IV 6mg/hrFeb 17 – decrease po intake – deteriorating –
ketamine 7.5mg/hr

Course in HospitalFeb 19 – pt wishes she could sleep until
death – tired of trying to “hold the pain in”
Feb 23 – unresponsiveFeb 26 – prognosis hrs to days/ discussed
sedationFeb 28 – difficulty maintaining sedationMar 4 – died sedated and comfortable

What is Neuropathic Pain?Pain initiated or caused by a primary lesion
or dysfunction in the nervous system
Characterized by :Burning, Tingling, Electric ,Shooting Pain

Pain ReceptorsA delta
Mechanical sensation eg. Cut, prick
C fibresDiffuse, respond to many stimuliBurning sensation
Sleeping receptorsActive in injured tissue onlyAcquire mechanical sensitivity
(Almeida 2004)


NociceptorsDamaged tissue releases:
Serotonin, Substance P, Bradykinin, Prostaglandin
Involved in acute & chronic pain
Influenced by endorphins

SensitizationCan be a tissue level (primary) orAt CNS level (secondary)
Results in: threshold of activation after injury intensity of a response to a noxious stimulus emergence of spontaneous activity
(Aguggia 2003)

SensitizationPrimary sensitization
Sympathetic activity and Inflammatory Mediators (Chong 2003)
Secondary sensitizationCNS changes in spinal cord and brainNMDA receptors activated“Wind-up” = increased amplitude and frequency
summation in neurons after prolonged stimulation (Chong 2003)
Blocked by NMDA antagonists, anti-inflammatories (McHugh 2000)

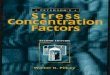
The Dorsal Root Ganglion


Tricyclic Antidepressants (TCAs)40-60% efficacy for partial relief (NNT~2.5-3)Start 10-25 mg/d and 10-25mg each week
Best effects: 50-150 mg/dayMechanism:
NE & 5HT reuptake blockade +/- NMDA antagonism, +/- Na channel blockade
Anticholinergic effectsSecondary amine better tolerated

Selective Serotonin-Norepinephrine Reuptake Inhibitors (SNRIs)
DuloxetineNNT ~4-5 (~7 for SSRI)Start & efficacious @
60mg/dayAntidepressant &
anxiolyticFavorable side effect
profileLimited long term data
VenlafaxineStart 37.5 mg/day Increase by 37.5 mg
weeklyEffective @ 150-225 mg/dLower doses – results
inconsistentShort vs XR preps

ά2-δ Ligands (Gabapentinoids)
GabapentinFew drug interactionsDizziness & sleepinessExacerbate cognitive
impairment Start 100-300mg TIDTitrate to 1800-3600 mg/dPeak effect in >2 weeks
PregabalinNo drug interactionsSimilar side effects to gabaStart 50-150mg divided Q8-
12HTitrate 50-150mg/day
weeklyGoal 300-600 mg/d in 1-2
weeksPeak effect in 2 weeks
Bind to ά2-δ subunit of voltage gated Ca channels glutamate, NE, substance P releaseNNT ~3.5-4.5

Opioids20-30% pain reduction, NNT
~2.5Provides rapid reliefRapid titration No ceiling effectMultiple forms & delivery
methodsMore side effects than 1st line
treatments Risk of misuse and abuse (5%)

Methadoneμ-receptor agonist + NMDA antagonist
Very long half-life, variable in individuals
Slow titration: start 2.5mg TID
Increase 50-100% every 48-72 hours
~5:1 to ~30:1 morphine equivalency (depending on
dose)
Little literature support, ++ practical support

NMDA AntagonistsKetamineStart 2.5-5mg PO TID Titrate by 50-100% dose to 1-2 mg/kg/dayStart IV infusion @ 0.05-0.1mg/kg/hr IV bolus @ 0.1-0.2 mg/kg/dose over 20 minutesNo NNT data
Poor performance in studies, good efficacy in practice
Topical or gargle preparations possible*opioid sparing effects

Other/New Things to TryIV Lidocaine And po Mexilitine
Cochrane Review 2005
Good quality evidence in neuropathic painBoth decrease VAS by 11 on 1-100 scale47% of people in trials had a 30% decrease in pain
(22% in placebo)35% had Side –effects
Numbness, dizziness, fatigue, metallic tasteAuthors conclude similar efficacy to other
adjuvants and good safety profile

Other/New Things to TryCapsaicin – High dose patch in PHN (640mcg/cm2)
1 – 60 min applicationLasts up to 12 weeksMean decrease in pain score of 29.6%Side-effects – Pain and erythema at site
(Backonja – Lancet Neurology, 2008)
Cannabis – Sativex - Neuropathic pain with AllodyniaImprovements of 1.43 on 10 point VASGood safety profile – SE include GI upset & drowsiness
(Nurmikko – Pain 2007)

Other/New Things to TryIntrathecal Ziconotide
N-type Ca Channel blocker (NCCB)Median dose 6.48mcg/dayImproved VASPI scores in 53.1%Decreased opioid usage in 9%Very expensiveSide Effects:
Memory loss, dizziness, nystagmus, somnolence, gait, CK rise
(Pommer - J Pain Symptom – 2009)

A Comparison of AdjuvantsDrug NNT Titratio
nNotes Side Effects
TCA 2.5-3 2-15 wks Antidepressant, cheap Anticholinergic
Duloxetine 4-5 none Anxiolytic, antidepressant
few
Venlafaxine 4-5 3-5 wks Antidepressant few
Gabapentin 3.5-4.5
1.5-6 mo Min drug interactions Dizzy/sleepy
Pregabalin 3.5-4.5
1-2 wks Min drug interactions Dizzy/sleepy
Methadone ? variable Opioid, cheap Opioid, drug interactions
Ketamine ? 1-4 wks Opioid sparing Hallucinations
Tramadol 3.8 4-8 wks For Diabetes, PHN Anticholinergic
Carbamezapine 1.7 1-4 wks For Trigeminal neuralgia
Drug interactions
Lidocaine/Mexilitine
4 none IV trial then po Cardiac, neurologic
Capsaicin ? none/days Topical Burning, redness
Cannabinoids ? none/days For MS, allodynia GI, drowsiness
Clonidine ? none/days Effective IT, topical Hypotension

Summary/ObjectivesBy the end of the hour the learner will be
able to:Define neuropathic painList at least 2 types of Pain receptorsList at least 4 different types of adjuvant pain
medicationsList the mechanisms of action, benefits, and
side-effects of these 4 medicationsList 2 new/different adjuvant pain medications

Recommended References1. Cruccum, G. Treatment of painful neuropathy.
Current Opions in Neurology. 2007; 20; 531-535.2. Dworkin, R. et al. Pharmacologic management of
neuropathic pain: evidence-based recommendations. Pain. 2007; 132; 237-251.
3. Gilron, I. et al. Neuropathic pain: a practical guide for the clinician. CMAJ. 2006; 175(3); 265-275.
Recommended