J o i n t A n a t o m y & P h ys i o l o g y v 1 6. 0 5
JOINT ANATOMY & PHYSIOLOGY Student Manual
HLTM SG003 P ERFORM REM EDIAL M ASSAGE M U SCU LOSK ELETAL
ASSESSM ENTS

EVOLVE COLLEGE P age | 2
J o i n t A n a t o m y & P h ys i o l o g y © Ev o l v e Co l l e g e P t y L t d 2 0 1 6
© Ev olve College Pty Ltd, 2016 This document is copyright. This document may not, in whole or in part, and in any form or by any means (electronic, mechanical, micro copying, photocopying, recording or otherwise) be reproduced, stored in a retriev al system or transmitted without prior written permission
.

EVOLVE COLLEGE P age | 3
J o i n t A n a t o m y & P h ys i o l o g y © Ev o l v e Co l l e g e P t y L t d 2 0 1 6
CONTENT
MAJ OR J O INT ANAT OMY & PHYSI OLO GY ... . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4
S HOULD ER (GL ENO HUM ERAL) JOINT. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4
S ho u ld er J oi nt . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4
HIP (CO XAL ) JO INT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .5
H i p Joi nt . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5
S ACRO IL IAC JO INT. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .7 S acr oi l ia c Joi nt . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
KNEE JO INT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8 K n e e Joi nt . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8
JO INTS O F THE ANKLE & FOO T. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11
A n k le Joi nt . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1 1
JO INTS O F THE HAND & WR IST . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
J oi nt s o f t he H a n d & W r i s t . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1 3
E LBOW JO INT. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15
E l b o w J oi nt . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1 5
ACROM IOCL AV ICUL AR JO INT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16 T h e A cr o mio cl av ic ul ar J oi nt . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1 6
S TERNOCLAV ICULAR JO INT. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18 T h e S t er n ocl av ic ul a r J oi nt . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1 8
S TERNAL CO S TAL JO INTS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19
S t er n a l Cost al Joi nt s . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1 9
JO INTS O F THE VER TEBR AL COLUM N (S PINE) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20
J oi nt s o f t he S pi n e . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2 0
ATLANTO -OCC IPITAL JO INT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21
At la nt o - Oc ci pi t al J oi nt . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2 1
TEM POR OMANDIBUL AR JOINT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 22
T e m p or o m a n di b ul ar Jo i nt . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2 2
JO INT MO TIONS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24
A c ce ss or y / S e c o n da r y Joi nt M ot io n. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2 4
Co u p l e d J oi nt Mot i o n . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2 4
JO INT C APSUL AR PATTER NS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25
J oi nt Ca p s ul ar P at t e r ns . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2 5

EVOLVE COLLEGE P age | 4
J o i n t A n a t o m y & P h ys i o l o g y © Ev o l v e Co l l e g e P t y L t d 2 0 1 6
MAJOR JOINT ANATOMY & PHYSIOLOGY KNOWLEDGE EVIDENCE: K9: Detailed joint anatomy for each major joint (shoulder, hip, sacroiliac, knee,
ankle/foot, wrist, elbow, acromioclavicular, sternoclavicular, costal, spine, atlanto-occipital, temporomandibular) K9: Accessory/secondary coupled motions of joints K9: Capsular restrictions and patterns
SHOULDER (GLENOHUMERAL) JOINT
Shoulder Joint
In the shoulder joint stability has been sacrificed to provide the most freely
moveable joint in the body. Shoulder ligaments such as the coracohumeral,
glenohumeral and transverse humeral ligaments are located primarily on the
anterior aspect to reinforce the shoulder joint. Several bursae are associated with
the shoulder joint. The muscles that cross the shoulder are very important in
stabilising the shoulder as well as facilitat ing movements of the joint. These are
known as the rotator cuff group and encircle the joint and blending with the
art icular capsule. Shoulder dislocations are a common shoulder injury.

EVOLVE COLLEGE P age | 5
J o i n t A n a t o m y & P h ys i o l o g y © Ev o l v e Co l l e g e P t y L t d 2 0 1 6
HIP (COXAL) JOINT
Hip Joint
The hip joint, like the shoulder, is a ball and socket joint with very good movements
but not to the same range as the shoulder joint. Movements occur in all possible
planes but are limited by the deep socket and joint ligaments. The joint is formed
by the art iculat ion of the spherical head of the femur with the acetabulum or
socket. A circular rim of fibrocart ilage called the acetabular labrum lines the
socket. In contrast to the shoulder, the surfaces of the hip joint fit snugly together
such that hip dislocations are rare.
Several st rong ligaments reinforce the joint capsule including the iliofemoral,
pubofemoral and ischiofemoral ligaments. These ligaments are arranged in such a
way that they screw the femur head into the acetabulum. The ligamentum teres or
the ligament at the head of the femur appears to be of no importance in
stabilising the joint and its role is unclear. The arrangement of the muscles
ligaments and structural components of the hip supports standing and weight
bearing. The most common injury to the hip, usually as a result of a fall, is a fracture
to the neck of the femur, this area being the most vulnerable stress point in the
region.
See diagram on following page.

EVOLVE COLLEGE P age | 6
J o i n t A n a t o m y & P h ys i o l o g y © Ev o l v e Co l l e g e P t y L t d 2 0 1 6

EVOLVE COLLEGE P age | 7
J o i n t A n a t o m y & P h ys i o l o g y © Ev o l v e Co l l e g e P t y L t d 2 0 1 6
SACROILIAC JOINT
Sacroiliac Joint
The sacroiliac joint is located in the pelvis linking the lilac bone to the sacrum. This
joint t ransfers weight and forces between the upper body and legs and is an
essential component for shock absorpt ion to prevent impact from forces during
walking from reaching the spine. Stabilised by a network of ligaments and muscles
a normal sacroiliac joint has a small amount of movement approximately 2-4mm in
any direction. The ligaments are less st iff in women than in men to allow for mobility
during childbirth.

EVOLVE COLLEGE P age | 8
J o i n t A n a t o m y & P h ys i o l o g y © Ev o l v e Co l l e g e P t y L t d 2 0 1 6
KNEE JOINT
Knee Joint
The knee joint is the largest and most complex joint in the body. It allows flexion,
extension and some rotat ion. Despite its single joint cavity, the knee consists of
three joints in one.
Femoropatellar Joint
Between the patella and lower end of the femur. This is a plane joint, as the patella
glides over the distal end of the femur during knee movements.
Tibiofemoral Joint
Being the lateral and medial joints between the femoral condyles and the c -
shaped menisci (semi lunar) cart ilages, of the t ibia below. Besides deepening the
shallow t ibial art icular surfaces, the menisci help prevent side to side rocking of the
femur on the t ibia and absorb shock transmitted to the knee joint. A tear to the
menisci can occur frequently due to their light attachments only at the outer
edge. The t ibiofemoral joint acts primarily as a hinge, permitt ing flexion and
extension however it is st ructurally a bicondylar joint with some rotat ion possible
when the knee is part ly flexed. When extended any side to side movements and
rotat ion are strongly resisted by ligaments and the menisci. Three broad ligaments
run from the patella to the t ibia anteriorly. The patellar ligament and medial and
lateral patella ret inacula which merge into the art icular cart ilage on either side.
The patella ligament is actually a continuation of the quadriceps tendon. Doctors
test the knee jerk response by taping on the patellar ligament. At least a dozen
bursae are associated with the knee joint. Several ligaments are important in
stabilising and strengthening the knee joint:
Extra Capsular
Medial and Lateral collateral ligaments - crit ical to preventing medial and lateral
rotat ion when the knee is extended.
Oblique popliteal ligament - an extension of the semimembranous hamstring
muscle on the posterior aspect of the knee joint .
Arcuate popliteal ligament - acts inferiorly and reinforces the joint capsule
posteriorly.

EVOLVE COLLEGE P age | 9
J o i n t A n a t o m y & P h ys i o l o g y © Ev o l v e Co l l e g e P t y L t d 2 0 1 6
Intra Capsular
Anterior cruciate (cross) ligament
The anterior cruciate passes posteriorly, laterally and upward from the anterior
condyle to attach on the medial surface of the lateral femoral condyles. This
ligament prevents backward sliding of the femur on the t ibia and checks
hyperextension of the knee.
Posterior cruciate ligament
The stronger posterior cruciate ligament is attached to the posterior condylar t ibia
and passes anteriorly, medially and upward to attach to the lateral side of the
medial femoral condyle. This ligament prevents forward sliding of the femur or
backward displacement of the t ibia thus it helps prevent over flexion of the knee
joint.
The knee capsule is heavily reinforced by muscle tendons of the quadriceps and
the semimembranosus hamstring muscle posteriorly. Since the muscles associated
with the joint are major stabilisers of the knee, the greater their st rength and tone,
the less chance of knee injury. Of all the joints in the body the knees are the most
susceptible to sports injuries because of their high reliance on non-art icular factors
for stability and the fact that they carry the body’s weight. Most injuries result from
blows to the lateral side tearing the medial collateral ligament, the medial
meniscus and the anterior cruciate ligament.

EVOLVE COLLEGE P age | 10
J o i n t A n a t o m y & P h ys i o l o g y © Ev o l v e Co l l e g e P t y L t d 2 0 1 6

EVOLVE COLLEGE P age | 11
J o i n t A n a t o m y & P h ys i o l o g y © Ev o l v e Co l l e g e P t y L t d 2 0 1 6
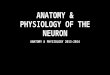
JOINTS OF THE ANKLE & FOOT
Ankle Joint
The ankle joint is a hinged synovial joint with primarily movements in one plane, up
and down, plantarflexion and dorsiflexion, however when the range of motion also
includes the subtalar joints (talocalcaneal and talocalcaneonavicular) together it
acts as a universal joint. Several ligaments support the ankle including the medial
(or deltoid) and lateral ligaments. The bony architecture of the ankle is most stable
in dorsiflexion hence a sprained ankle is more likely to occur in plantar flexion due
to stress on the ligament structures. The most common ankle sprain is an inversion
sprain involving the talofibular ligament (one of the lateral ligaments).

EVOLVE COLLEGE P age | 12
J o i n t A n a t o m y & P h ys i o l o g y © Ev o l v e Co l l e g e P t y L t d 2 0 1 6
Talonavicular Joint
Calcaneocuboidal
Joint
Tibiotalar Joint

EVOLVE COLLEGE P age | 13
J o i n t A n a t o m y & P h ys i o l o g y © Ev o l v e Co l l e g e P t y L t d 2 0 1 6
JOINTS OF THE HAND & WRIST
Joints of the Hand & Wrist
Radiocarpal (Wrist) Joint
Carpometacarpal Joints
Intercarpal Joints
Intermetacarpal Joints
The wrist joint, also known as the radiocarpal joint, is a synovial joint between the
forearm and hand distally formed by the proximal carpal bones and the distal end
of the radius. The ulna is not part of the wrist joint it art iculates with the radius at the
radioulnar joint. Joint capsules and four ligaments stabilise the wrist . Several
muscular tendons also cross the wrist joint. The wrist is an ellipsoid synovial joint
allowing for movement along two axes. This means that flexion, extension,
adduction and abduction can all occur.
A common injury to the wrist joint is a fracture to the scaphoid or radius bone also
known as a Colles’ fracture whilst the hand is outstretched. Scaphoid fractures are
more common in the younger populat ion as a result of a fall. Colles’ fracture is the
most commonly reported injury e.g. a fall from tripping whilst walking a dog.

EVOLVE COLLEGE P age | 14
J o i n t A n a t o m y & P h ys i o l o g y © Ev o l v e Co l l e g e P t y L t d 2 0 1 6

EVOLVE COLLEGE P age | 15
J o i n t A n a t o m y & P h ys i o l o g y © Ev o l v e Co l l e g e P t y L t d 2 0 1 6
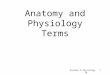
ELBOW JOINT
Elbow Joint
The most prominent joint in the upper limbs after the shoulder is the elbow joint . Its
st ructure provides a stable and smoothly operating hinge joint that allows flexion
and extension only. Within the joint both the radius and ulna art iculate with the
condyles (trochlea and capitulum) of the humerus but it is the close gripping of the
trochlea by the ulna t rochlea notch that const itutes the “hinge” and main
stabilising factor of this joint .
A relat ively lax art icular capsule allows for significant freedom for elbow flexion
and extension. However, side to side movements are restricted by two strong
ligaments, the ulnar/medial collateral ligament and the radial/lateral collateral
ligament. Addit ionally, tendons of several muscles, (the biceps, t riceps brachialis
and others cross the elbow joint and provide stability. Flexion of the elbow is limited
by the meeting of the soft t issues of the forearm and arm. Extension is checked by
tension in the medial ligament, tendons of the forearm flexors and the close fit of
the olecranon process into the olecranon fossa.
Lateral Mid Sagittal View Right Elbow

EVOLVE COLLEGE P age | 16
J o i n t A n a t o m y & P h ys i o l o g y © Ev o l v e Co l l e g e P t y L t d 2 0 1 6
ACROMIOCLAVICULAR JOINT
The Acromioclav icular Joint
The acromioclavicular (AC) joint is one of the three art iculat ions of the shoulder
girdle and links the clavicle to the scapula. The AC joint is a gliding or plane joint,
which is a type of synovial joint. Its function is to allow the scapula to rotate in three
dimensions during arm movements. It also allows forces to be transmitted from the
upper extremit ies to the clavicle. There is a limited degree of movement. Since
movements of the scapula and clavicle occur together lit tle relat ive movement
occurs at the joint itself and most occurs at the sternoclavicular joint. The distal end
of the clavicle is connected to the acromion by the medial and lateral divisions of
the AC ligament providing superior and inferior stability. A fall or blow to the
shoulder often results in sprains to the ac joint as commonly seen in contact sport
players.

EVOLVE COLLEGE P age | 17
J o i n t A n a t o m y & P h ys i o l o g y © Ev o l v e Co l l e g e P t y L t d 2 0 1 6
AC Joint Sprain/Separation Grade I-III

EVOLVE COLLEGE P age | 18
J o i n t A n a t o m y & P h ys i o l o g y © Ev o l v e Co l l e g e P t y L t d 2 0 1 6
STERNOCLAVICULAR JOINT
The Sternoclav icular Joint
The sternoclavicular joint (SC joint) is formed by the art iculat ion of the medial
aspect of the clavicle with the manubrium of the sternum. The SC joint is generally
classified as a plane joint with a fibro cart ilage joint disk. The inter clavicular,
anterior and posterior sternoclavicular and the costoclavicular ligaments
reinforcing this joint are very strong often result ing in a fracture to the clavicle
before a dislocation of the joint. Movements at this joint are associated with
motions of the scapula.
Intact sternoclavicular joint

EVOLVE COLLEGE P age | 19
J o i n t A n a t o m y & P h ys i o l o g y © Ev o l v e Co l l e g e P t y L t d 2 0 1 6
STERNAL COSTAL JOINTS
Sternal Costal Joints
The sternocostal joints are art iculat ions of cart ilage between the true ribs and the
sternum and are arthrodial (plane joint s) allowing gliding movements as required in
breathing. The joints are connected and supported by three ligaments, the
interart icular sternocostal, radiate sternocostal and the costoxiphoid ligaments.

EVOLVE COLLEGE P age | 20
J o i n t A n a t o m y & P h ys i o l o g y © Ev o l v e Co l l e g e P t y L t d 2 0 1 6
JOINTS OF THE VERTEBRAL COLUMN (SPINE)
Joints of the Spine
There are 2 joints between individual vertebrae:
1. Joints between bodies: Symphysis – intervertebral discs – the discs both
absorb shock and act as a flexible spacer that allows intervertebral
movement
2. Joints between superior and inferior art iculat ing processes (facets): synovial
joint – direct ion/orientat ion and shape of the art iculat ing processes defines
/determines what kind of movements are possible between vertebrae –
especially the degree of rotat ion possible

EVOLVE COLLEGE P age | 21
J o i n t A n a t o m y & P h ys i o l o g y © Ev o l v e Co l l e g e P t y L t d 2 0 1 6
ATLANTO-OCCIPITAL JOINT
Atlanto-Occipital Joint
The at lanto-occipital joint is the art iculat ion between the at las and the occipital
bone and consists of a pair of condyloid joints. The at lanto-occipital joints are
synovial socket type joints that are shallow in infancy and deepen with age.
Movements allowed include flexion/extension and lateral flexion with some
rotat ion. Muscles such as the anterior and posterior rectus capitus action
movements at this joint.

EVOLVE COLLEGE P age | 22
J o i n t A n a t o m y & P h ys i o l o g y © Ev o l v e Co l l e g e P t y L t d 2 0 1 6
TEMPOROMANDIBULAR JOINT
Temporomandibular Joint
The temporomandibular joint is the jaw joint frequently referred to as TMJ. The TMJ
is a bilateral synovial hinge joint that connects the mandible (jaw) to the temporal
bones of the skull allowing movements of the jaw up and down (elevation and
depression) and side to side such as in chewing, yawning, and talking.
There are six main components of the joint
Mandibular condyles
Art icular surface of the temporal bone
Capsule
Art icular disc
Ligaments – major - temporomandibular, minor - stylomandibular and
sphenomandibular
Lateral pterygoid muscle
The TMJ is classified as ginglymoarthrodial joint since it is both hinging (ginglymus)
and sliding (arthrodial). The art icular disc separates the TMJ into two dist inct parts
allowing for sliding and hinge movements. The mandible is moved mainly by four
muscles of mast ication: the masseter, medial and lateral pterygoid and the
temporalis allowing movement in different directions as experienced with
chewing. The most common injury to the TMJ is disc displacement , sometimes
called dislocation. TMJ pain or dysfunction however is far more common and
usually involves the muscles tendons and ligaments of mast ication.
See diagrams on following page.

EVOLVE COLLEGE P age | 23
J o i n t A n a t o m y & P h ys i o l o g y © Ev o l v e Co l l e g e P t y L t d 2 0 1 6

EVOLVE COLLEGE P age | 24
J o i n t A n a t o m y & P h ys i o l o g y © Ev o l v e Co l l e g e P t y L t d 2 0 1 6
JOINT MOTIONS
Accessory / Secondary Joint Motion
Accessory also called secondary joint movement
is joint movement that is necessary for a full range of motion at the joint but it
is not under direct voluntary control. Accessory movements cannot be performed
by the individual. These movements include roll, spin and slide and they naturally
accompany the physiological movements of a joint. Examples include movements
at the knee and wrist joints.
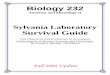
Coupled Joint Motion
In biomechanical terms, coupled motion is
the phenomenon of a consistent
associat ion of a motion along or about one
axis, whether it be a translat ion or a
rotat ion, with another motion about or
along a second axis; the principal motion
cannot be produced without the
associated motion occurring as well.
For example, in the cervical and upper
thoracic spine, side bending is coupled with
axial rotat ion in the same direction and in
the lumbar spine lateral bending is coupled
with axial rotat ion in the opposite direction.
The importance of coupling in the human
spine is that it allows for increase mobility without compromising stability.

EVOLVE COLLEGE P age | 25
J o i n t A n a t o m y & P h ys i o l o g y © Ev o l v e Co l l e g e P t y L t d 2 0 1 6
JOINT CAPSULAR PATTERNS
Joint Capsular Patterns
Capsular pattern is known as a series of limitat ions of joint movement when the
joint capsule is the limit ing structure. This pattern affects the whole joint. An
example is the range of movement in the shoulder or glenohumeral joint, from
flexion as the least limited movement to external rotat ion as the most limited
movement.
Knowledge of the capsular patterns improve diagnost ic ability and in the case of
massage therapists a general understanding may lead to client referral if
underlying condit ions are suspected.
There are two patterns of restrict ion in range of motion used in the interpretation of
joint motion:
A capsular pattern of restrict ion is a limitat ion of pain and movement in a joint
specific rat io, which usually occurs when there is arthritis, inflammation or following
prolonged immobilizat ion.
A non-capsular pattern of restrict ion is a limitat ion in a joint in any pattern other
than a capsular one, and may indicate the presence of either a derangement, a
restrict ion of one part of the joint capsule, or an extra-art icular lesion, that prevents
joint motion. In other words, the cause of the restrict ion is outside the joint itself.
Dr. James Cyriax was the first of many authors to extensively study soft t issue
lesions. When inflammation of a joint is present (known as synovit is or capsulit is), not
only does passive stretching of the joint capsule cause pain but there is a limitat ion
in range of motion of the involved joint in a specific pattern; this pattern is always
similar for that particular joint, although each joint has a different capsular pattern.
Capsular patterns are based on clinical findings rather than research which may
explain why there are some difference in the way they are reported.
Capsular patterns have shown to be extremely useful in determining arthritis and
capsular involvement.

EVOLVE COLLEGE P age | 26
J o i n t A n a t o m y & P h ys i o l o g y © Ev o l v e Co l l e g e P t y L t d 2 0 1 6
JOINT CAPSULAR PATTERN
Temporomandibular (Jaw) Increasing limitation of mouth opening
Occipitoatlanto Extension & side flexion equally limited
Cervical Spine Side flexion & rotations are equally limited,
extension equally limited and flexion is best movement
Glenohumeral (Shoulder) Limitation of Lateral rotation, abduction, less medial rotation
Sternoclavicular Pain at extreme range of movement
Acromioclavicular Pain at extreme range of movement
Humeroulnar (Elbow) Limitation of extension and more limitation of flexion
Radiohumeral Flexion, extension, supination, pronation
Proximal Radioulnar Pain on passive supination and pronation, no limitation
Distal Radioulnar Pain at extremes of rotation
Wrist Flexion & extension equally limited
Thoracic Spine Side flexion & rotation equally limited
Lumbar Spine Side flexion extension & rotation equally limited
SI, Symphysis Pubis, &
Sacrococcygeal Pain when joints stressed

EVOLVE COLLEGE P age | 27
J o i n t A n a t o m y & P h ys i o l o g y © Ev o l v e Co l l e g e P t y L t d 2 0 1 6
Hip Flexion more limited than extension, Gross limitation of abduction, medial rotation
(order varies)
Knee Limitation of flexion, extension
Tibiofibular Pain when joint stressed
Talocrural (Ankle) Limitation of dorsiflexion more limitation of plantar flexion
Subtalar (Talocalcaneal) Limitation of varus range of movement
For more information, visit these links.
https://sgphysio.wordpress.com/2013/06/02/cyriax-system-of-orthopaedic-medicine/
http://physicaltherapyweb.com/joint-capsular-patterns/
http://www.physio-pedia.com/Capsular_and_Noncapsular_Patterns
Recommended