CORRECTIONAL MEDICINE: A PUBLIC HEALTH APPROACH
Janet Mohle-Boetani, Deputy Medical Executive, Public Health ,CCHCS
Public Health in Corrections Public Health/Medicine comparison Why public health in corrections? Public Health Framework
Exercises on public health interventions Public Health in Corrections: challenges Public Health in CCHCS Exercises on public health and primary
care Summary
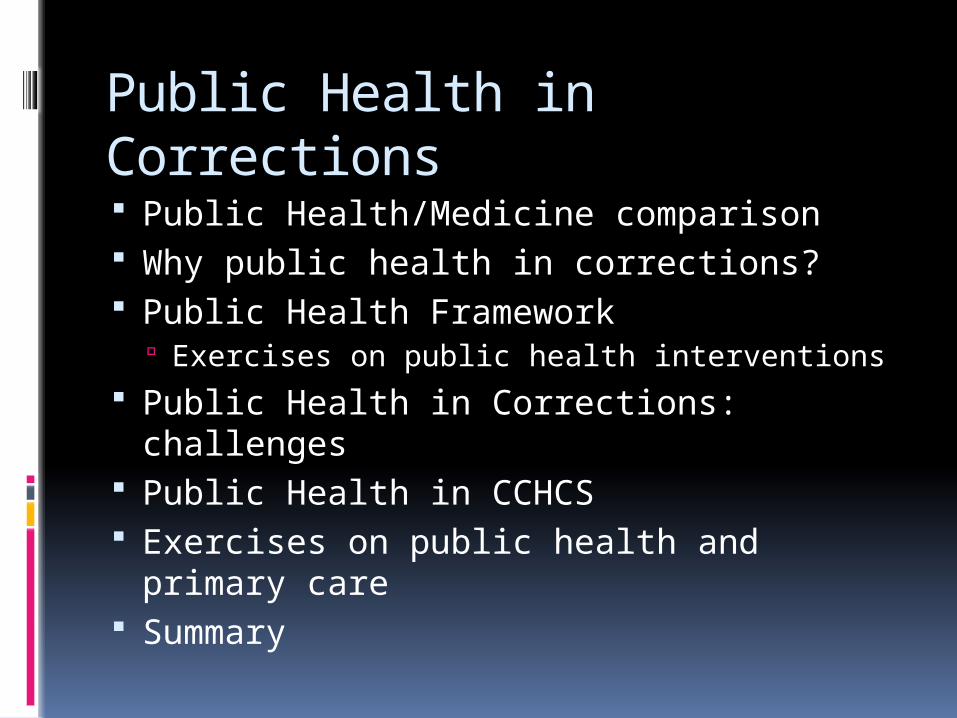
Medicine:Public Health Crosswalk
Medicine Public HealthFocus Patient Population
Intervention Treatment/disease management – prevent harm after disease (tertiary prevention)
Prevention- of exposure (primary prevention) or disease after infection (secondary prevention)
Constitutional Care/Not deliberate indifference
Access to Care Consulting Public Health to get access
Community Standard of Practice
Evidence-Based Guidelinesfor care/hospitalization
Evidence-Based Guidelinesfor outbreak control/prevention
Measurement Vital signs, individual labs
# of cases, % of pop, rate of disease
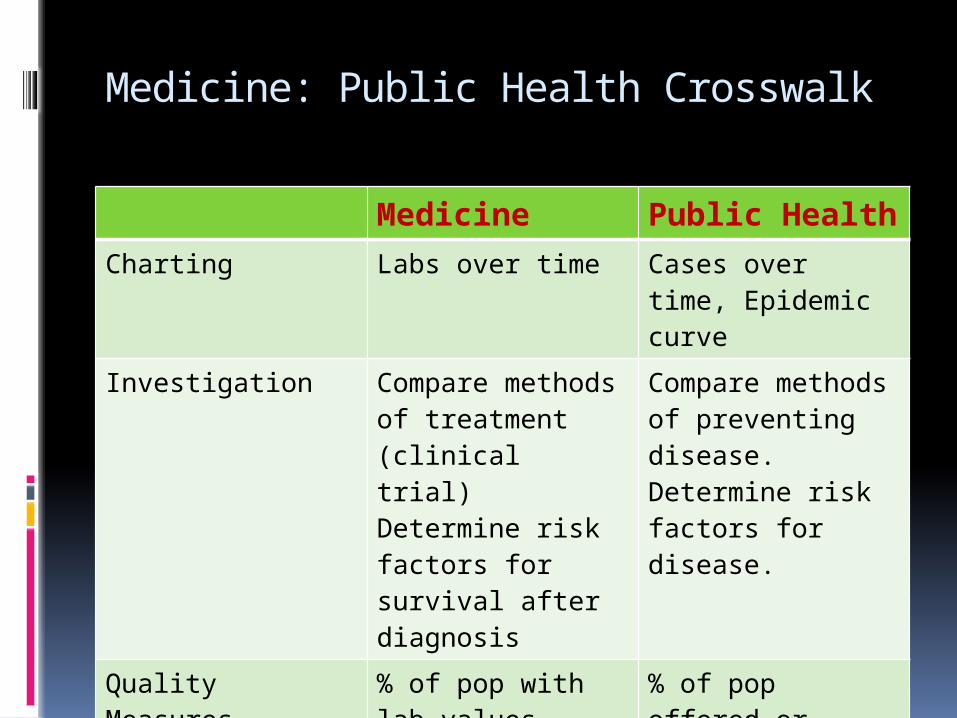
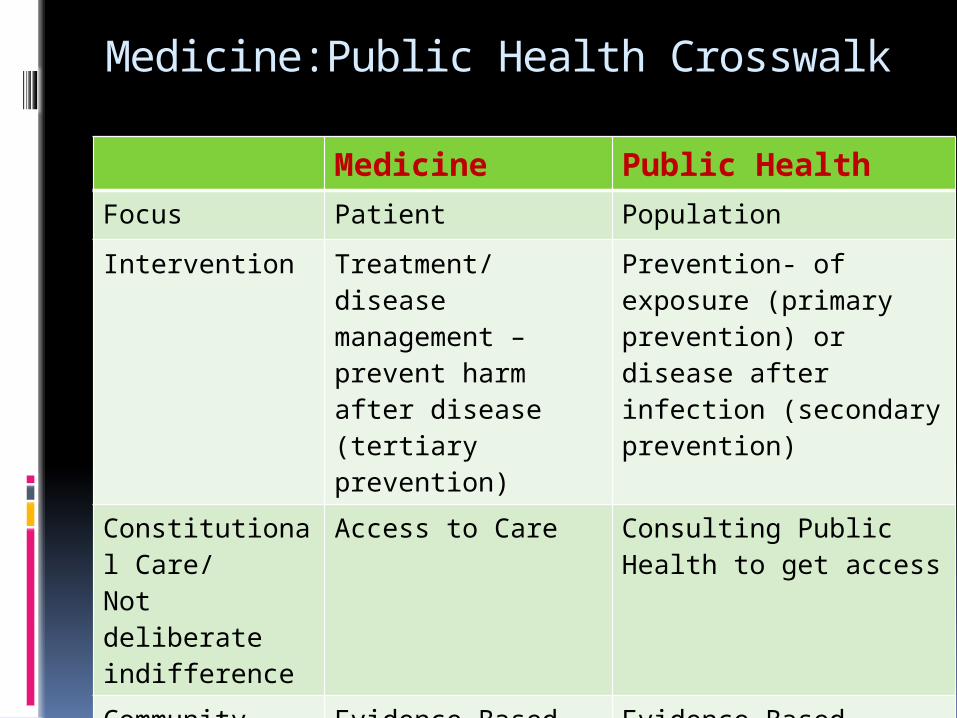
Medicine: Public Health Crosswalk
Medicine Public HealthCharting Labs over time Cases over time,
Epidemic curve
Investigation Compare methods of treatment (clinical trial)Determine risk factors for survival after diagnosis
Compare methods of preventing disease.Determine risk factors for disease.
Quality Measures % of pop with lab values indicating good control(e.g.,HbA1c)
% of pop offered or received preventive measure (HIV screen, flu vax)
Public Health In Corrections: the 7 Cs Risk for CDs– 3 Cs
Correctional staff, Concentrated Communicable Diseases, Crowded Environment
Why- 4 Cs Constitutional right, Control CDs,
Continuity of Care, Community public health impact
Risks for CDs in corrections- 3 Cs Correctional Staff
Introduce influenza, pertussis, tuberculosis May work while symptomatic No occupational health program
Concentrated communicable disease (high prevalence) TB (25%), Hepatitis (40%), STIs
Crowded Environment- 175% capacity High incidence of chicken pox (transmission
from shingles) TB transmission
Public Health in Corrections: Why? The 4 Cs
Constitutional care/civil right to no deliberate indifference
Control communicable diseases in prison Prevent exposure (Env. Mitigation/hand hygeine/ condoms?) Prevent infection (vaccinations [disease with higher rate
than gen pop vs other diseases) Detect disease/infection (screening/surveillance:
TB/varicella) Isolation (ill)and quarantine (exposed during incubation
period): influenza, norovirus Offer intervention to those exposed to communicable
diseases (contact investigation) Continuity of care with community for communicable
diseases- e.g., tuberculosis treatment on admit and after parole
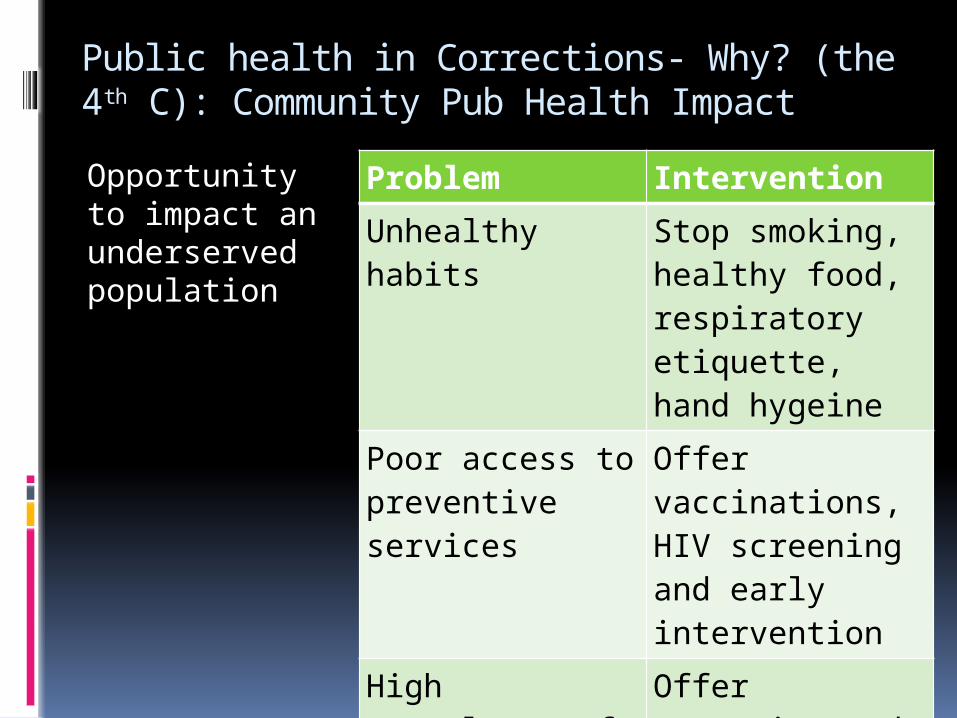
Public health in Corrections- Why? (the 4th C): Community Pub Health Impact
Opportunity to impact an underserved population
Problem Intervention
Unhealthy habits Stop smoking, healthy food, respiratory etiquette, hand hygeine
Poor access to preventive services
Offer vaccinations, HIV screening and early intervention
High prevalence of communicable diseases (TB and Hep C)
Offer screening and treatment
Community: Incarcerated Treatment inside: Impact outside
TB infection
10
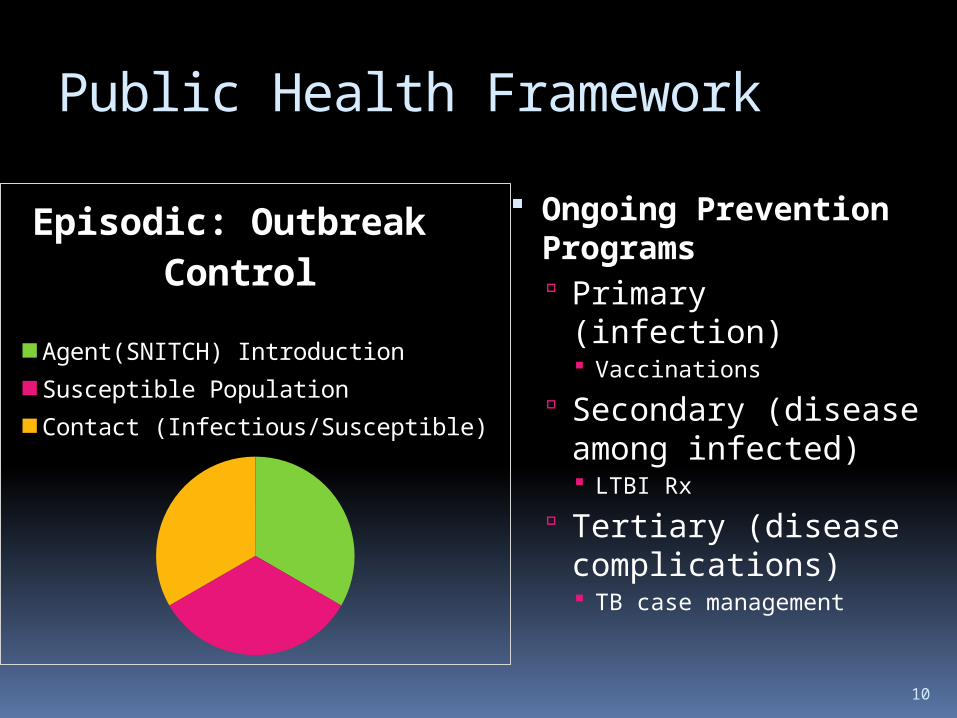
Public Health Framework
Ongoing Prevention Programs Primary (infection)
Vaccinations
Secondary (disease among infected) LTBI Rx
Tertiary (disease complications) TB case management
Episodic: Outbreak Control
Agent(SNITCH) IntroductionSusceptible PopulationContact (Infectious/Susceptible)
11
PH Diseases/Pathogens: CCHCS
S N I T C H
12
PH Disease/Pathogens: CCHCS
Shingles/Skin Diseases (MRSA)/STDs/Scabies
Norovirus infections Influenza Tuberculosis Chickenpox/Coccidioidomycosis HIV/Hepatitis
13
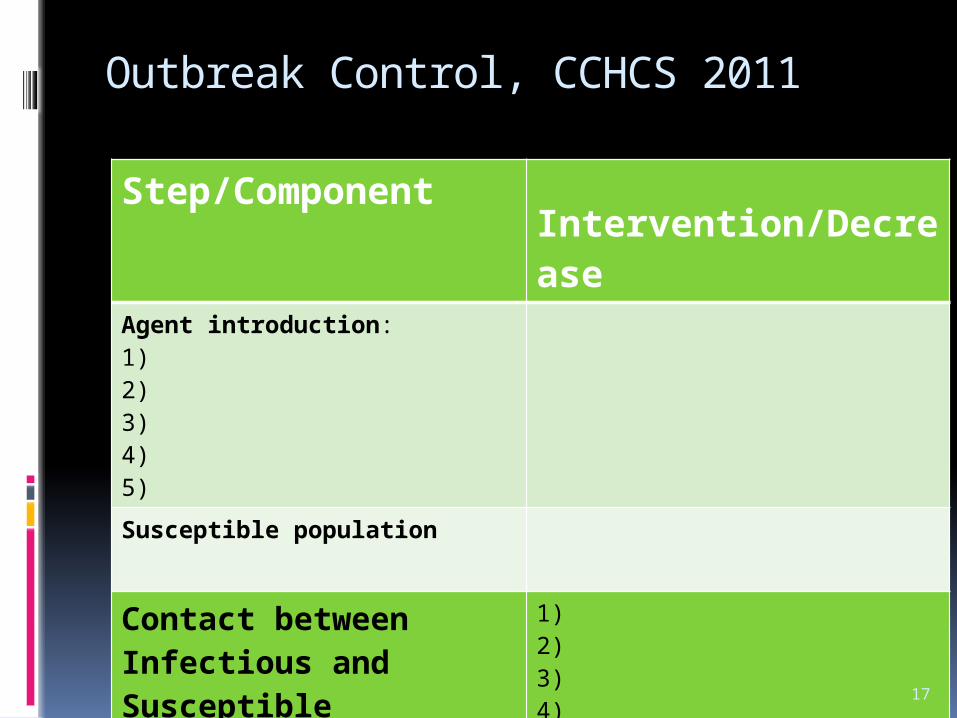
Outbreak Control, CCHCS 2011
Component Intervention/Decrease
Agent introduction method:1) 2) 3)4)5)
Susceptible population
Contact between Infectious and Susceptible
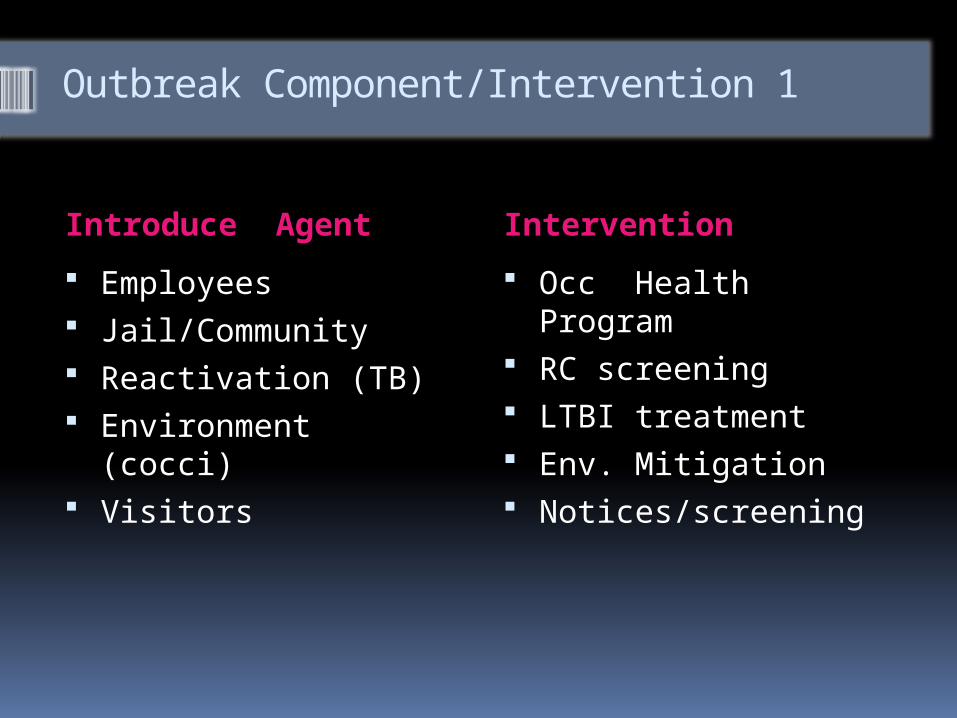
Outbreak Component/Intervention 1
Introduce Agent Intervention
Employees Jail/Community Reactivation (TB) Environment (cocci) Visitors
Occ Health Program RC screening LTBI treatment Env. Mitigation Notices/screening
15
Outbreak Control, CCHCS 2011
Step/Component
Intervention/Decrease
Agent introduction:1) 2) 3)4)5)
Susceptible population1)2)Contact between Infectious and Susceptible
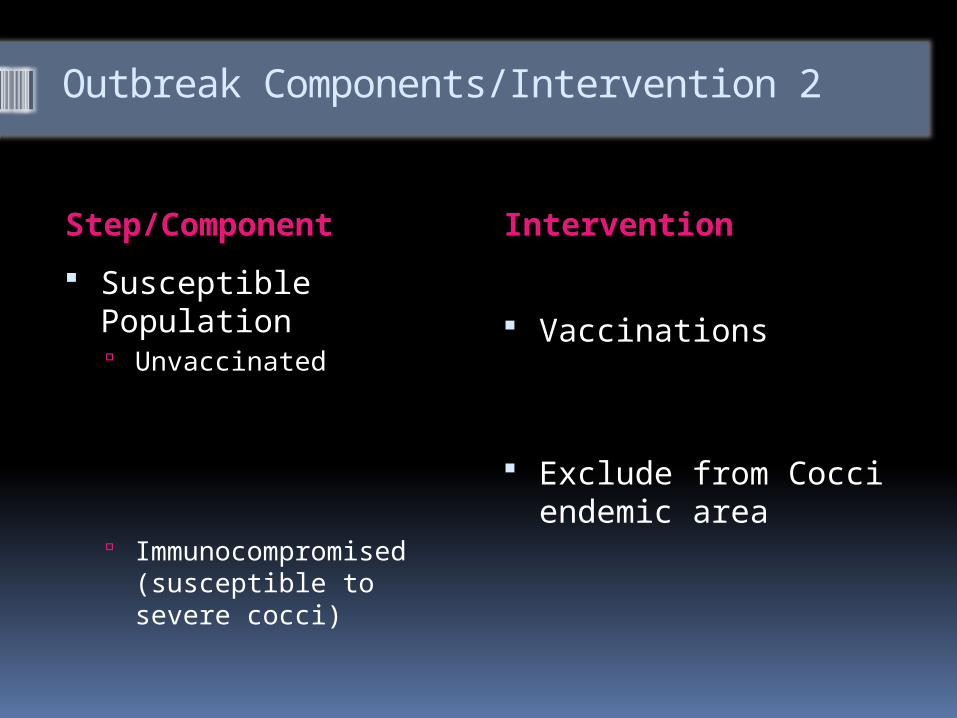
Outbreak Components/Intervention 2
Step/Component Intervention
Susceptible Population Unvaccinated
Immunocompromised (susceptible to severe cocci)
Vaccinations
Exclude from Cocci endemic area
17
Outbreak Control, CCHCS 2011
Step/Component
Intervention/Decrease
Agent introduction:1) 2) 3)4)5)
Susceptible population
Contact between Infectious and Susceptible
1)2)3)4)5)
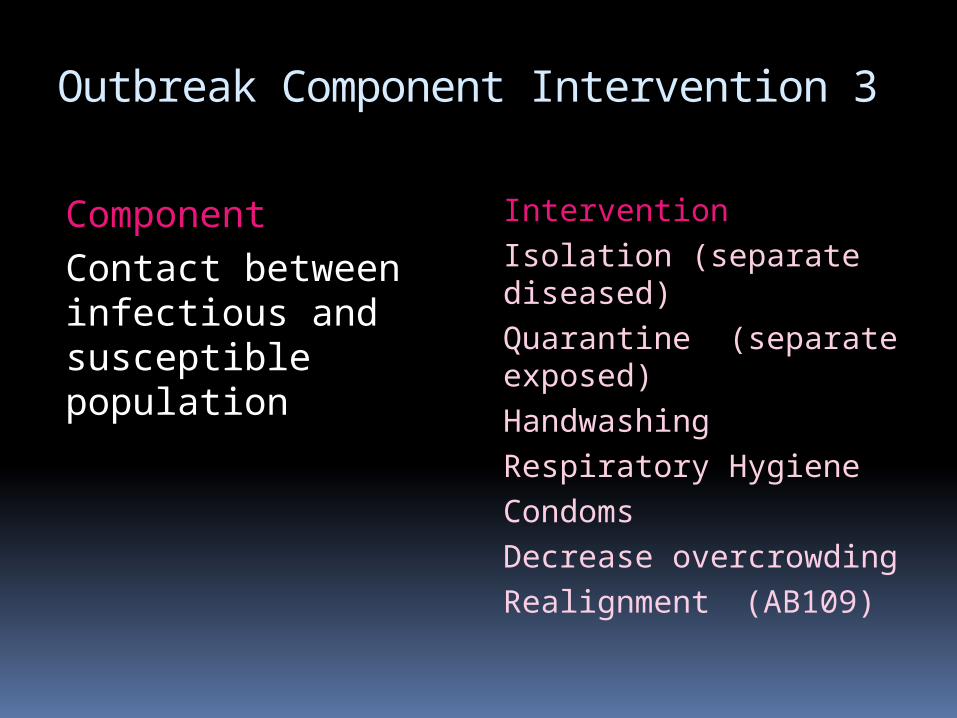
Outbreak Component Intervention 3
ComponentContact between infectious and susceptible population
InterventionIsolation (separate diseased)Quarantine (separate exposed)HandwashingRespiratory HygieneCondomsDecrease overcrowding
Realignment (AB109)
19
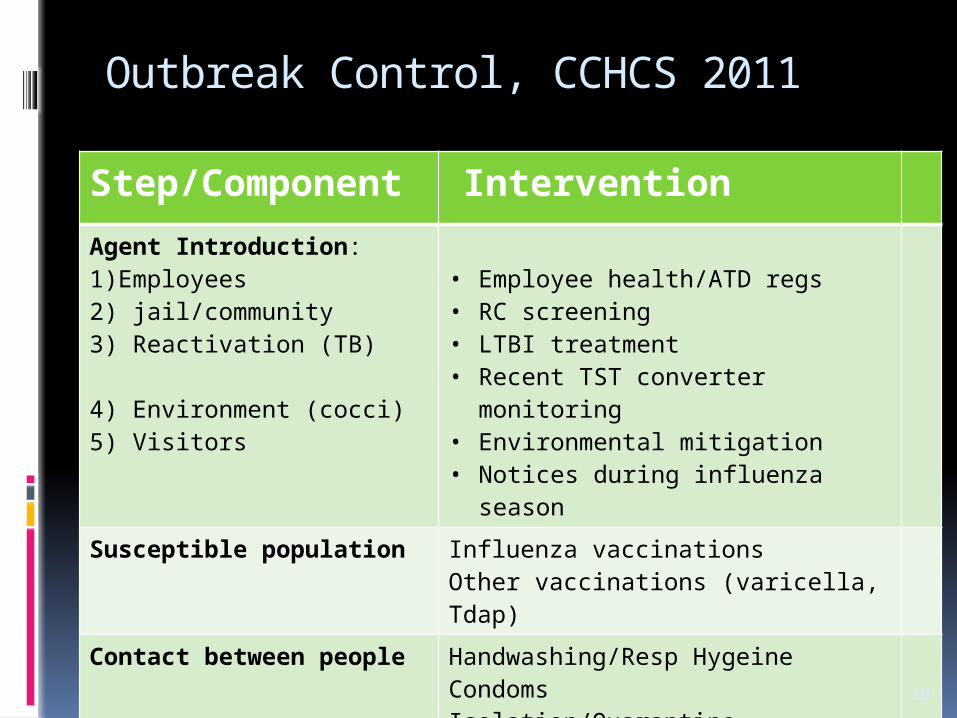
Outbreak Control, CCHCS 2011
Step/Component
Intervention
Agent Introduction:1)Employees2) jail/community3) Reactivation (TB)
4) Environment (cocci)5) Visitors
• Employee health/ATD regs• RC screening• LTBI treatment• Recent TST converter monitoring• Environmental mitigation• Notices during influenza season
Susceptible population Influenza vaccinationsOther vaccinations (varicella, Tdap)
Contact between people Handwashing/Resp HygeineCondomsIsolation/QuarantineAB109
Challenges of Public Health in Corrections
Isolation from mainstream public health Inmate vs occupational health issues : role of
healthcare in public health contact investigations
Personal medical care/public health overlap Disease management (HIV, TB, STDs, viral
hepatitis): chronic care vs public health clinics Prevention: public health campaigns vs public
health clinics vs incorporate into primary care Transfer of medical information: jail/prison,
prison/community Quality management: standard measures?
21
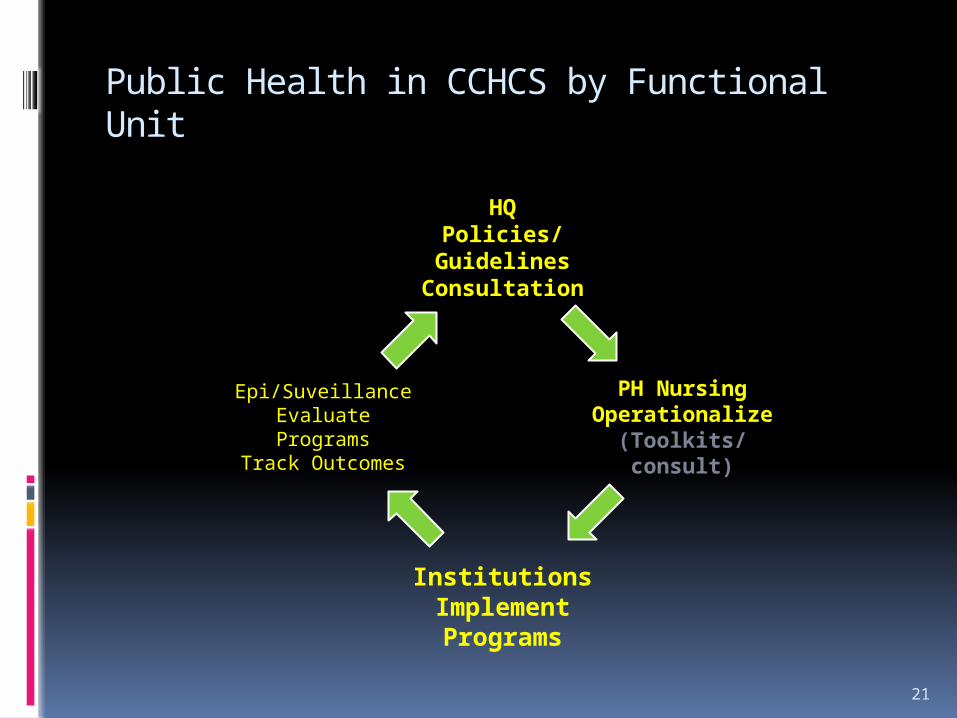
Public Health in CCHCS by Functional Unit
HQPolicies/
GuidelinesConsultation
PH NursingOperationalize
(Toolkits/consult)
InstitutionsImplement Programs
Epi/SuveillanceEvaluate Programs
Track Outcomes
22
Goal: Change in Public Health Practice in CCHCS
From To
Disjointed/Fragmented
Reactive Isolated Fear-based Thriftless/High
Cost
Systematic Proactive Integrated Evidence-based Saving resources
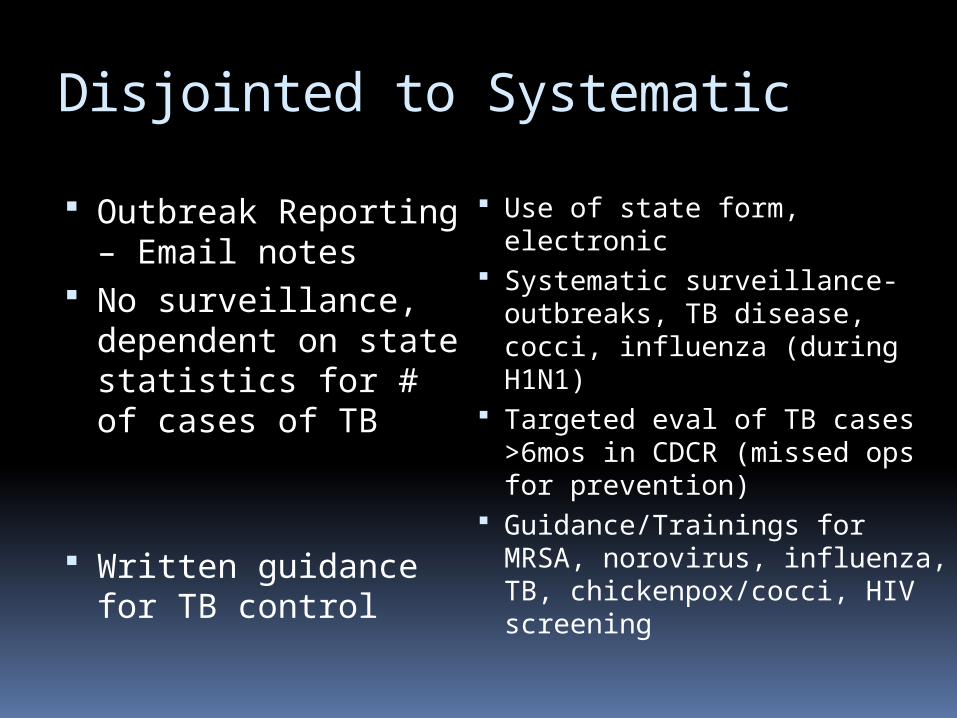
Disjointed to Systematic
Outbreak Reporting – Email notes
No surveillance, dependent on state statistics for # of cases of TB
Written guidance for TB control
Use of state form, electronic Systematic surveillance-
outbreaks, TB disease, cocci, influenza (during H1N1)
Targeted eval of TB cases >6mos in CDCR (missed ops for prevention)
Guidance/Trainings for MRSA, norovirus, influenza, TB, chickenpox/cocci, HIV screening
Reactive to Proactive
Norovirus: 200-500 cases and institutions shut down for weeks
Massive TB contact investigations- institution shut down for weeks, yards on med holds for months, incomplete investigations
Influenza Outbreaks- massive 200-500 cases, mass vaccinations after the outbreak was detected
Clusters of 10-20 cases, no shut downs
Targeted and complete investigations- usually 20 inmates/employees per CI
Most outbreaks are fewer than 10 cases, effective isolation/quarantine, vaccination in the fall
Isolated to Integrated
No statewide PH committee participation
Minimal regional PH committee participation
Isolated within CCHCS
Active participation in CCLHO-CD, CTCA, Cocci WG
Formal structured meetings by regional PHNs with hospitals and local health departments
Participation in HQ committees (eg, RC), collaborate with nursing, QM, IT, and UM
Fear-Based to Evidence-Based Laborious HIV
counseling for screening- backlogs
Massive TB contact investigations (e.g., all ees at an institution) Emphasis on testing
Respiratory isolation and massive contact investigations for shingles
No condoms: fear of use as contraband
HIV opt out screening- quality measure 85% screened at RCs
Targeted TB contact investigations (usually 20 inmates and 10 staff) Emphasis on LTBI Rx for
infected
Resp iso for chickenpox not localized shingles Limited CIs for shingles
Condom distribution feasibility study- no evidence of abuse
Thriftless/High Cost to Saving
Tuberculin Testing on Transfer between institutions
Reactive to chickenpox- screening and vaccination AFTER exposure
Coccidioidomycosis- Ongoing morbidity and high costs
Screen for TB disease not infection on transfer- Saves $2 million each
year
Varicella prevention- targeted screening and vaccination BEFORE exposure Saves $1.3 million/5 years
Environmental Mitigation ($200K) + evaluation
Exercise: Public Health and Primary Care
What options are there for increasing access to public health clinical services in corrections?
Should public health be integrated into primary care? Pros and cons of integration
How could public health be integrated into primary care?
29
Public Health and Primary Care – Level 1 (individual)
Free access to care for respiratory symptoms and rashes Problem list: TB disease, recent TB infection, LTBI
treatment PH clinical services in primary care (combine appts)
Immunizations (prim and tertiary prevention) LTBI treatment (sec prevention) STD treatment (prim, sec, tertiary prev)
TB case management (tertiary prev) primary care team Hospital discharge planning for suspect/confirmed TB
patients (team plans for DC when pt admitted) Continuity of medications when discharged from hospital Appropriate discharges to the general population
Community standard vs discharge into high risk population
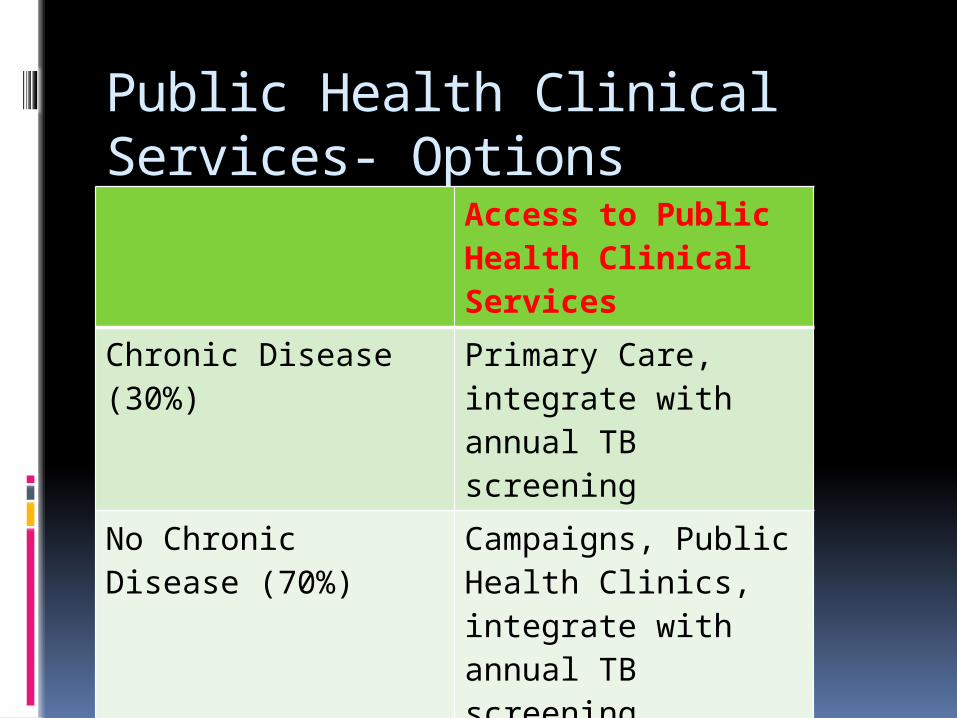
Public Health Clinical Services- Options
Access to Public Health Clinical Services
Chronic Disease (30%)
Primary Care, integrate with annual TB screening
No Chronic Disease (70%)
Campaigns, Public Health Clinics, integrate with annual TB screening
31
PH and Primary Care- Level II (registry based)
Registry of recent TB infections (within 2 years)
Registry of patients on LTBI treatment
Registry of patients with Hepatitis C
Exercise: Quality Measures What are some key public health
quality measures?
33
PH and Primary Care- Level III(pop based assessment)
Vaccination coverage by population Recent infections- monitoring for 2
years by population LTBI treatment- completion of 9 mos
in 1 year by population TB treatment-completion in 1 year by
population
Public Health In Corrections Summary: the 7 Cs Risk for CDs– 3 Cs
Correctional staff, Concentrated CDs, Crowded Environment
Why- 4 Cs Constitutional right, Control CDs,
Continuity of Care, Community public health impact
35
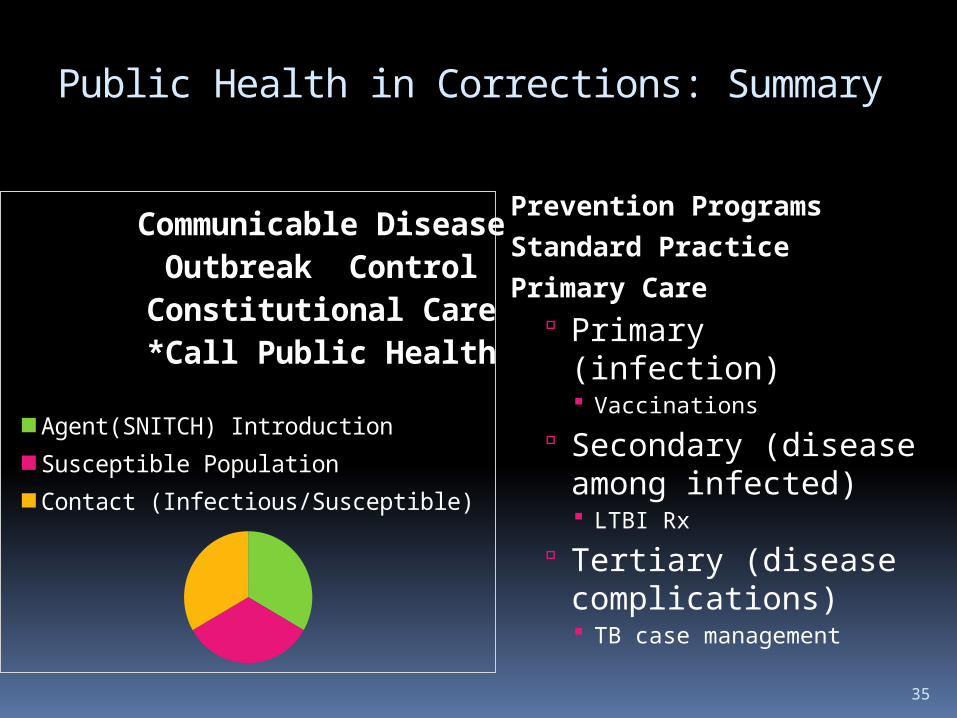
Public Health in Corrections: Summary
Prevention Programs
Standard Practice
Primary Care Primary (infection)
Vaccinations
Secondary (disease among infected) LTBI Rx
Tertiary (disease complications) TB case management
Communicable Disease
Outbreak ControlConstitutional Care*Call Public Health
Agent(SNITCH) IntroductionSusceptible PopulationContact (Infectious/Susceptible)
Public Health in Corrections in a nutshell
Control Communicable
Diseases Concentrated in
the incarcerated population
Crowded environment
Prevention programs
Primary care setting
Population-based assessments
Recommended