I N T E R P R E T I N G C H E ST X- R AY SIllustrated with 100
CasesInterpreting chest X-rays can seem bafing and intimidating for
junior doctors. This highlyillustrated guide provides the ideal
introduction to chest radiology. It uses 100 clinical casesto
illuminate a wide range of common medical conditions, each
illustrated with a chest X-rayand a clear description of the
signicant diagnostic features and their clinical relevance.Where
appropriate, CT scans and bronchoscopic imaging are also included
as part of theinvestigation. Pulmonary medicine is largely based on
the strong foundation of the plain chest radio-graph. Indeed, chest
radiography is the single most common investigation carried out in
hos-pital practice. This collection of case studies will help make
the learning process easier, moreenjoyable, and less painful. As
well as offering enlightening pearls of core knowledge in
chestX-ray interpretation, it highlights some of the pitfalls that
might wrong-foot the inexperi-enced practitioner.Dr. Philip Eng is
Head of the Department of Respiratory and Critical Care Medicine at
theSingapore General Hospital, and Clinical Associate Professor of
Medicine at the NationalUniversity of Singapore.Dr. Foong-Koon
Cheah is Director of Body Imaging and Director of Teaching and
Education atthe Department of Radiology at the Singapore General
Hospital.
INTERPRETINGC H E ST X- R AY SIllustrated with 100 casesPhilip
EngandFoong-Koon CheahSingapore General Hospital
Cambridge, New York, Melbourne, Madrid, Cape Town, Singapore,
So PauloCambridge University PressThe Edinburgh Building, Cambridge
, UKPublished in the United States of America by Cambridge
University Press, New Yorkwww.cambridge.orgInformation on this
title: www.cambridge.org/9780521607322 P. Eng and F.-K. Cheah
2005This publication is in copyright. Subject to statutory
exception and to the provision ofrelevant collective licensing
agreements, no reproduction of any part may take placewithout the
written permission of Cambridge University Press.First published in
print format 2005- ---- eBook (NetLibrary)- --- eBook (NetLibrary)-
---- paperback- --- paperbackCambridge University Press has no
responsibility for the persistence or accuracy of sfor external or
third-party internet websites referred to in this publication, and
does notguarantee that any content on such websites is, or will
remain, accurate or appropriate.
CO N T E N T SPreface page viiCases 1 to 100 1Index 201
P R E FA C EThis book arose because of the huge amounts of
clinical material that pass throughthe Singapore General Hospital,
the largest tertiary care hospital in Singapore. Asignicant
proportion of our patients come to us for a second opinion from
theneighboring countries. Often they come to consult us for an
abnormality on achest radiograph. Pulmonary Medicine is largely
based on the strong foundation ofthe plain chest radiograph.
Indeed, chest radiography is the single most commoninvestigation
carried out in hospital practice. This book is targeted towards
nal-year medical students and residents in a medical training
program. We have givencountless tutorials to generations of medical
students, residents, and fellows andwe hope that this collection of
pearls can help make the learning process easier,more enjoyable,
and less painful. Readers are advised to read this book from cover
to cover as the cases are laidout in an increasing order of
complexity. The latter cases assume some fundamen-tal knowledge
which is laid out in the earlier cases. The authors have
intentionallymade the cases as clinically relevant as possible so
that interest is sustained andthe book will not be heavy going. P.
E N G F. K . C H EA H
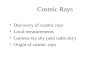
1 Interpreting Chest X-Rays CASE 1 Fig. 1.1 Case 1. A
35-year-old male presented with fever, cough, and purulent sputum
for one week. This was his CXR (Fig. 1.1). What is the
diagnosis?
CASE 1 Interpreting Chest X-Rays 2 Fig. 1.2 Ao SVC LA RA LVCASE
1 PNEUMONIAThe CXR shows a focal shadow in the right lower lobe
with air bronchograms sug-gestive of pneumonia. It is clearly in
the right lower lobe because the right hemidi-aphragm is eaced.
Right middle lobe shadows would eace the right heart border.The
presence of air bronchograms indicates pathology in the alveoli, as
the con-ducting airways remain patent with air. Water or blood can
also occupy the alveolias a result of pulmonary edema or pulmonary
hemorrhage respectively. Thereshould be other supporting signs such
as cardiomegaly, upper lobe diversion, andKerley B lines with
pulmonary edema. The dierential diagnoses of a focal shadowwith air
bronchograms include bronchoalveolar cell carcinoma and lymphoma.
Itis important to follow-up the CXR to ensure that total resolution
of infectionoccurs. This may take up to three months in the elderly
but generally someimprovement usually occurs within a week. The
borders of the heart on a PA CXRare shown in Fig. 1.2. SVC superior
vena cava, RA right atrium, Ao aorticknuckle, LA left atrium, LV
left ventricle
3 Interpreting Chest X-Rays CASE 2 Fig. 2.1 Case 2. This
25-year-old had sudden onset of left-sided chest pain. The CXR is
shown (Fig. 2.1).
CASE 2 Interpreting Chest X-Rays 4 Fig. 2.2C A S E 2 L E F T P
R I M A R Y S P O N TA N E O U S P N E U M OT H O R A XThe CXR
shows the visceral pleura (Fig. 2.2) separated from the parietal
pleura byair which now occupies the potential space in the pleural
cavity. The visceralpleura must not be mistaken for skin-fold
shadows which usually occur in supineor obese patient CXR. In
addition, the line from skin folds can be seen to cross thechest
wall. In the patient above, the lungs appear otherwise healthy and
this condi-tion is called primary spontaneous pneumothorax. It
occurs classically in youngmales. This is in contradistinction to
secondary pneumothorax which occurs indiseased lungs, e.g. chronic
obstructive pulmonary diseases (COPD).Pneumothorax in an erect lm
is usually seen at the apex. See Case 60.
5 Interpreting Chest X-Rays CASE 3 Fig. 3.1 Case 3. 50-year-old
male presented to the Emergency Room with shock and a four-day
history of a febrile illness. He required intubation and was
started on inotropes. This was his CXR (Fig. 3.1).
CASE 3 Interpreting Chest X-Rays 6 Fig. 3.2CASE 3 RUPTURED
LIVER ABSCESSIt is important to look at the blind areas of the CXR
in order not to miss impor-tant clues. These areas are under the
diaphragm, behind the heart, the hilum, andthe soft tissues. This
CXR shows a lucency over the liver density. The lucency doesnot
conform to the usual bowel conguration. In this clinical context,
an impor-tant dierential diagnosis to be considered is a ruptured
liver abscess. This can beconrmed either by bedside ultrasound or
CT (Fig. 3.2). Liver abscesses are usuallydue to organisms like
Klebsiella or Amoebiasis. All patients with Klebsiella bac-teremia
of unknown origin should have imaging studies of the abdomen to
ruleout a liver abscess.
7 Interpreting Chest X-Rays CASE 4 Fig. 4.1 Case 4. This
elderly male has exertional dyspnea, orthopnea, and parox- ysmal
nocturnal dyspnea. His CXR is shown (Fig. 4.1).
CASE 4 Interpreting Chest X-Rays 8 Fig. 4.2C A S E 4 CO N G E
ST I V E H E A R T FA I L U R EThe CXR shows classic evidence of
left ventricular failure, i.e. cardiomegaly (car-diothoracic ratio
50%), upper lobe pulmonary venous diversion, and Kerley Blines
(which indicate distension of lymphatics). In addition, there is
evidence ofsternotomy wires, suggesting previous coronary artery
bypass surgery (CABG).Following diuresis, the pulmonary inltrates
have cleared (Fig. 4.2). Only uid andblood on the chest radiograph
can clear rapidly (within days). This patient also hasa right
internal jugular central venous line.
9 Interpreting Chest X-Rays CASE 5 Fig. 5.1 Case 5. A
65-year-old male presented with cardiogenic shock. He had an
emergency CABG which was associated with a very stormy peri-opera-
tive period. This was his CXR (Fig. 5.1) taken upon arrival at the
Intensive Care Unit (ICU). What is the most significant
abnormality?
CASE 5 Interpreting Chest X-Rays 10 Fig. 5.2 Fig. 5.3C A S E 5
F O R E I G N B O DY R I G H T LO W E R ZO N EThe CXR shows an
opaque density in the region of the right lower zone (Fig.
5.2).Each lung eld on an erect CXR is divided into three zones. The
upper zone is anarea which lies above a horizontal line drawn from
the medial end of the secondrib anteriorly. The middle zone lies
below this and is bordered inferiorly by a linedrawn similarly from
the fourth rib. The lower zone lies below this. This opaquedensity
is similar in conguration to a tooth which was dislodged during
emer-gency intubation of this patient. Foreign bodies are not as
common in adults com-pared with children. It can occur silently in
patients with decreased consciouslevel. The typical site is in the
right main stem bronchus, as this has a more verticalcourse than
the left. An example is seen in this CT (Fig. 5.3).
Bronchoscopicremoval is the usual initial treatment of choice.
11 Interpreting Chest X-Rays CASE 6 Fig. 6.1 Case 6. This
patient was asymptomatic. Her CXR is shown (Fig. 6.1). Name the
anomaly.
CASE 6 Interpreting Chest X-Rays 12C A S E 6 C H I L A I D I T
I S S I G NChilaiditi described this normal variant in 1911 where
the transverse colon is inter-posed between the right hemidiaphragm
and the liver. Its prevalence is thought tobe 0.025%. Occasional
reports describe patients with Chilaiditis syndrome wherepatients
complain of intermittent abdominal pain requiring laparotomy to
rule outother causes of peritonism, e.g. perforated ulcer, ruptured
appendix. The recogni-tion of the haustrations (indicative of large
bowel origin) in the bowel shadows iscrucial to the diagnosis of
Chilaiditis sign.
13 Interpreting Chest X-Rays CASE 7 Fig. 7.1 Case 7. This
patient was asymptomatic. The CXR is shown (Fig. 7.1).
CASE 7 Interpreting Chest X-Rays 14 Fig. 7.2C A S E 7 A Z YG O
U S LO B EThere is a curvilinear density adjacent to the right
superior mediastinum with anovoid lower density at its lower end
(the azygous vein). The azygous lobe is thecommonest CXR normal
variant seen in up to 0.4% of individuals. This is anembryologic
variation which results in an accessory lobe at the right upper
lobe.The ssure (Fig. 7.2) is due to the invagination of the azygous
vein and the condi-tion is of no clinical signicance.
15 Interpreting Chest X-Rays CASE 8 Fig. 8.1 Case 8. This was
an 80-year-old male with fever, productive cough, hemoptysis, and
loss of weight. This was his CXR (Fig. 8.1). What is the
diagnosis?
CASE 8 Interpreting Chest X-Rays 16C A S E 8 A C T I V E P U L
M O N A R Y T U B E R C U LO S I SThe CXR shows bilateral upper
lobe inltrates with cavities, suggestive of activepulmonary
tuberculosis. In general, thin-walled cavities (5 mm) tend to be
infec-tive and, when thick-walled (10 mm), squamous cell carcinoma
of the lungenters into the dierential diagnosis. Tuberculosis tends
to aict the upper lobesand apical segment of the lower lobes.
However, within the upper lobe, anteriorsegment involvement is
rare. Diagnosis is conrmed by obtaining sputum andstaining with
uorochrome or Zeil Nielson and culturing with Lowenstein
Jansenmedia. Cavitary upper lobe disease has good correlation with
a sputum positivesmear and hence is extremely infectious. Other
dierential diagnoses of cavitarypulmonary lesions include
infections from Staphylococcus, Klebsiella, anaerobes,and
non-infectious causes like squamous cell carcinoma of the lung,
pulmonaryinfarcts, Wegeners granulomatosis, and rheumatoid
nodules.
17 Interpreting Chest X-Rays CASE 9 Fig. 9.1 Case 9. This
80-year-old male used to work in a sand quarry. He was
asymptomatic. His CXR is shown (Fig. 9.1). What is the
diagnosis?
CASE 9 Interpreting Chest X-Rays 18C A S E 9 S I L I CO S I
SThe CXR shows bilateral inltrates and calcied nodules in both
upper lobes.Dierential diagnoses of upper lobe inltrates include
silicosis, tuberculosis, andankylosing spondylitis. There is also
egg-shell calcication of the hilar lymphnodes. The egg-shell
calcication plus the upper lobe nodules are typical of silico-sis.
Dierential diagnoses of egg-shell calcication include sarcoidosis,
Hodgkinslymphoma following radiotherapy, and coal-workers
pneumoconiosis.
19 Interpreting Chest X-Rays CASE 10 Fig. 10.1 Case 10. This
80-year-old male presented with right-sided chest pain and
breathlessness. He gave a long history of exertional dyspnea. The
CXR is shown (Fig. 10.1).
CASE 10 Interpreting Chest X-Rays 20C A S E 1 0 S I L I CO S I
S W I T H P R O G R E S S I V E M A S S I V E F I B R O S I
S(PMF)This patients CXR shows a right pneumothorax. In addition,
there are bilateraldiuse nodules (10 mm but 2 mm) which could be
due to metastatic adenocar-cinoma, silicosis, disseminated
histoplasmosis, or varicella infection. In silicosis,some nodules
may coalesce to form conglomerate masses in the upper lobescalled
progressive massive brosis. Patients with silicosis are predisposed
to pul-monary tuberculosis and serial CXR comparison is
useful.
21 Interpreting Chest X-Rays CASE 11 Fig. 11.1 Case 11. This
40-year-old male of African origin was asymptomatic and had a
routine CXR (Fig. 11.1). What is the likely diagnosis?
CASE 11 Interpreting Chest X-Rays 22 Fig. 11.2C A S E 1 1 B I L
AT E R A L H I L A R A N D M E D I A ST I N A LA D E N O PAT H Y F
R O M S A R CO I D O S I SCXR shows bilateral symmetrically
enlarged hilar and mediastinal lymph nodes.CT (Fig. 11.2) conrms
this nding, typical of sarcoidosis. The main dierentialdiagnoses
would be lymphoma and tuberculosis, but the lymphadenopathy
wouldthen be asymmetrical. Bronchoscopy and transbronchial lung
biopsy are positivein 60% of cases, showing non-caseating
granulomas and culture negative fortuberculosis and fungus. Blind
endobronchial biopsies increase the yield byanother 20% but the
gold standard is mediastinoscopy. Incidence in people ofAfrican
origin is ten times higher than in Caucasians.
23 Interpreting Chest X-Rays CASE 12 Fig. 12.1 Case 12. A
60-year-old male presented at the Emergency Room with severe chest
pain of sudden onset. This was his CXR (Fig. 12.1). What is the
diagnosis?
CASE 12 Interpreting Chest X-Rays 24 Fig. 12.2CA SE 12
DISSECTING THORACIC ANEURYSMThe CXR shows widening of the superior
mediastinum and a well-dened massinferior and contiguous with the
arch of the aorta. In this clinical context, dissec-tion of the
arch of the aorta has to be excluded. CT Thorax in another
patientshows the presence of an aneurysm (Fig. 12.2) at the aortic
arch with thrombus.
25 Interpreting Chest X-Rays CASE 13 Fig. 13.1 Case 13. This
80-year-old male smoker is a known case of COPD. He pre- sented
with epigastric pain and worsening of shortness of breath. Arterial
blood gas showed acute metabolic acidosis. This was his CXR (Fig.
13.1). What is the most obvious abnormality?
CASE 13 Interpreting Chest X-Rays 26C A S E 1 3 P N E U M O P E
R I TO N E U M D U E TO P E R F O R AT E D P E P T I CU LC E RThe
CXR shows free air under the right hemidiaphragm, in addition to
features ofhyperination. The possibilities include perforated
peptic ulcer or GI malignancy,recent laparoscopy/laparotomy, and
peritoneal dialysis. It is important to do anerect CXR for the free
air to rise to the top of the abdomen. For patients with
anasogastric tube in place, instillation of 200 ml of free air
before the CXR may aidthe diagnosis.
27 Interpreting Chest X-Rays CASE 14 Fig. 14.1 Case 14. This
75-year-old male had a history of myocardial infarction and now
presented with recurrent Ventricular Tachycardia. These were his
CXR, PA and lateral (Figs. 14.1 and 14.2).
CASE 14 Interpreting Chest X-Rays 28 Fig. 14.2C A S E 1 4 C A
LC I F I E D L E F T V E N T R I C U L A R A N E U R Y S MThe PA
and lateral CXR conrm an arcuate density in the region of the left
ventri-cle. This is typical of calcication of a left ventricular
aneurysm, usually secondaryto previous myocardial infarction.
Surgical resection of the aneurysm is potentiallycurative.
29 Interpreting Chest X-Rays CASE 15 Fig. 15.1 Case 15. A
60-year-old male presented with exertional dyspnea, orthop- nea,
paroxysmal nocturnal dyspnea, and bilateral painless ankle
swelling. This was his CXR (Fig. 15.1). What is the abnormality and
sub- sequent management?
CASE 15 Interpreting Chest X-Rays 30 Fig. 15.2C A S E 1 5 P S E
U D OT U M O R D U E TO LO C U L AT E D R I G H T P L E U R A
LEFFUSIONThe CXR shows classic evidence of congestive heart failure
with cardiomegaly,upper lobe venous diversion, and bilateral
pleural eusions. In addition, there isan ovoid mass in the right
middle zone which seems to be related to the transversessure. This
is typical of a pseudotumor due to a loculated pleural eusion
dis-tending the transverse ssure. Appropriate management would
include diureticsand treatment of the cardiac failure. Repeat CXR a
week later showed the disap-pearance of the pseudotumor (Fig.
15.2).
31 Interpreting Chest X-Rays CASE 16 Fig. 16.1 Case 16. A
30-year-old male was seen in the Emergency Room for acute onset
chest pain. This was his CXR (Fig. 16.1). Name the most obvious
abnormality.
CASE 16 Interpreting Chest X-Rays 32 Fig. 16.2C A S E 1 6 M E D
I A ST I N A L E M P H Y S E M A ( P N E U M O M E D I A ST I N U M
)The CXR shows free air in the mediastinum and subcutaneous tissues
of the neck(Fig. 16.2). The mediastinal air could have come from
disruption of the integrity ofthe lung, major airways, or the
esophagus. A history of trauma (e.g. motor vehicleaccident with
blunt injury to the anterior chest wall by the steering wheel) or
iatro-genic instrumentation (e.g. recent endoscopy) is important.
Descending infectionsby gas-producing organisms from the oral
cavity and neck can cause severe medi-astinitis and result in a
similar appearance.
33 Interpreting Chest X-Rays CASE 17 Fig. 17.1 Case 17. An
80-year-old male presented with massive hemoptysis and was
intubated. This was his CXR (Fig. 17.1). He gave a past history of
being treated for tuberculosis many years ago.
CASE 17 Interpreting Chest X-Rays 34C A S E 1 7 MYC E TO M A R
I G H T U P P E R LO B EThe CXR shows a right upper lobe ball
within a cavity (air crescent sign) patho-gmonic of a mycetoma
(also called aspergilloma). A lateral decubitus X-ray
maydemonstrate the fungal ball shifting position. In this
condition, a preformed cavitybecomes colonized, usually by the
fungus Aspergillus fumigatus. Cavitary diseasemay be secondary to
brotic lung disease, e.g. previous tuberculosis, sarcoidosis,or
ankylosing spondylitis. Massive hemoptysis can result and bronchial
angiogramwith embolotherapy (using coils or gel foam) is
temporizing. Surgical resection isdenitive, but bronchopleural
stula may result. Unfortunately, most patientshave insucient
pulmonary reserve to allow surgical resection.
35 Interpreting Chest X-Rays CASE 18 Fig. 18.1 Case 18. This
68-year-old female had recurrent epistaxis. This was her CXR (Fig.
18.1). What is the diagnosis?
CASE 18 Interpreting Chest X-Rays 36 Fig. 18.2 Fig. 18.3C A S E
1 8 H E R E D I TA R Y H E M O R R H A G I C T E L A N G I E C TA S
I A O ROSLER WEBER RENDU DISEA SEThe CXR shows a mass in the right
lower zone. The mass has a sharp margin andtwo vessels (supplying
artery and draining vein) leading to the mass (Fig. 18.2). TheCT
(Fig. 18.3) shows marked enhancement of the mass with contrast
conrmingthe presence of pulmonary arteriovenous malformation
(pAVM). Of patients withpAVM, 60% have Oslers disease, and 10% of
patients with Oslers disease havepAVM. This condition is autosomal
dominant. Other sites of involvement includeskin, nose (epistaxis),
gastrointestinal (GI) system (bleeding GI and anemia).Paradoxical
embolism can occur resulting in cerebral vascular accidents or
brainabscess. Pulmonary angiogram and embolotherapy are recommended
if the pAVMis more than 2 mm.
37 Interpreting Chest X-Rays CASE 19 Fig. 19.1 Case 19. An
80-year-old female, 100-pack-a-year smoker with 5-year history of
dyspnea on exertion. Describe her CXR (Fig. 19.1). What is the
diagnosis?
CASE 19 Interpreting Chest X-Rays 38C A S E 1 9 C H R O N I C O
B ST R U C T I V E P U L M O N A R Y D I S E A S E( CO P D )The CXR
of COPD typically demonstrates evidence of air trapping. The signs
arehorizontality of the ribs, hyperinated lungs (normally the right
sixth rib bisectsthe right hemidiaphragm), hyperlucent lung elds,
bilateral symmetrical attenu-ated pulmonary vasculature, long
tubular heart, scalloping and attening of thediaphragm. The
commonest cause of COPD worldwide is tobacco smoking.However, it is
recognized that alpha-1-antitrypsin deciency can also
causeemphysema. One should look out for alpha-1-antitrypsin
deciency, especially ifthe COPD patient is young (< 45 years
old) or demonstrates basal predominanceon CXR.
39 Interpreting Chest X-Rays CASE 20 Fig 20.1 Case 20. This
55-year-old male was admitted in shock. He was recently diagnosed
with inoperable lung cancer. Clinical exam also showed dis- tended
neck veins and muffled heart sounds. This was his CXR (Fig. 20.1).
What is the diagnosis?
CASE 20 Interpreting Chest X-Rays 40C A S E 2 0 C A R D I A C
TA M P O N A D E F R O M M A S S I V E P E R I C A R D I A
LEFFUSIONBeck described a triad of hypotension, mued heart sounds,
and elevated jugularvenous pressure due to cardiac tamponade from
pericardial eusion. Immediatepericardiocentesis is life-saving. The
common causes of pericardial eusioninclude malignancy, congestive
heart failure, tuberculosis, systemic lupus erythe-matosus,
Dresslers syndrome, and uremia. This CXR shows a globular
enlarge-ment of the heart, typical of a large pericardial eusion.
In addition, there is a massin the right lung in keeping with the
primary lung cancer.
41 Interpreting Chest X-Rays CASE 21 Fig 21.1 Case 21. This
65-year-old male had a long history of dyspnea on exer- tion,
orthopnea, and bilateral ankle edema. This was his CXR (Fig. 21.1).
Should a thoracocentesis be done?
CASE 21 Interpreting Chest X-Rays 42 Fig. 21.2C A S E 2 1 S E V
E R E C A R D I O M E G A LY D U E TO E N D STA G EVA LV U L A R H
E A R T D I S E A S EThe CXR shows very severe cardiomegaly (the
normal cardiothoracic ratio isdened as less than 0.5). Both
costophrenic angles show lucency due to aeratedlung, making it
unlikely that the patient has massive pleural eusions. The carinais
also splayed indicating an enlarged left atrium due to severe
mitral valve disease.Hence, in this patient, thoracocentesis should
not be done. A simple way toconrm the presence of a pleural eusion
is to take a lateral decubitus CXR. A free-owing eusion will layer
out (Fig. 21.2). However, the absence of layering on alateral
decubitus CXR does not preclude the presence of a signicant
pleuraleusion as it may be loculated due to an empyema.
43 Interpreting Chest X-Rays CASE 22 Fig. 22.1 Case 22. This
75-year-old female presented with acute respiratory failure. She
had been sick for two weeks with fever, cough, and puru- lent
sputum. This was her CXR (Fig. 22.1). What is the diagnosis?
CASE 22 Interpreting Chest X-Rays 44CASE 22 SEVERE PNEUMONIASee
Case 1. The CXR shows opacities with air bronchograms involving
both lungelds. This is typical of severe pneumonia as evidenced by
multilobar involvement.Typical organisms include Streptococcus
pneumoniae, Legionella, and gram nega-tives like Klebsiella and
Pseudomonas aeroginosa. In South-East Asia, another pos-sible
etiologic agent is Burholderia pseudomallei (Meliodosis). Treatment
willrequire combination parenteral antibiotics, usually beta
lactams plus macrolide oruoroquinolone. The prognosis is dependent
not just upon the severity of presen-tation but also underlying age
and co-morbidities, e.g. cancer, heart, liver, or renaldisease, and
stroke. This patients pneumonia was conrmed to be due to
severeLegionellosis.
45 Interpreting Chest X-Rays CASE 23 Fig. 23.1 Case 23. A
30-year-old male presented with cough, shortness of breath and loss
of weight over four months. This was his CXR (Fig. 23.1). What is
the most likely diagnosis? What physical sign would be useful?
CASE 23 Interpreting Chest X-Rays 46CASE 23 PNEUMOCYSTIS
CARINII PNEUMONIA (PCP)The CXR shows bilateral inltrates and air
bronchograms with a perihilar distribu-tion. The heart size is
normal. There are no Kerley B lines or evidence of upper lobevenous
diversion. All these are typical features of PCP. PCP is the most
commonlife-threatening opportunistic infection in HIV disease.
Generally, the mostcommon opportunistic infection in HIV is oral
candidiasis. Oral candidiasis shouldbe looked for in any young
patient with pneumonia as it may be a sign of T-cellimmune
deciency. PCP can be diagnosed by sputum induction or
bronchoalveo-lar lavage. Note that 10% of PCP patients could have a
normal CXR.
47 Interpreting Chest X-Rays CASE 24 Fig. 24.1 Case 24. This
middle-aged female non-smoker was recently diagnosed and treated as
for asthma with little response. This was her CXR (Fig. 24.1). What
is the diagnosis?
CASE 24 Interpreting Chest X-Rays 48 Fig. 24.2 Fig. 24.3C A S E
2 4 T R A C H E A L T U M O R D U E TO A D E N O I D C Y ST I
CCARCINOMAAll patients diagnosed with asthma should have a CXR. In
addition to looking forpneumothorax and transient pulmonary
inltrates, one should pay attention tothe tracheal air column. Any
obstruction to the major airway can produce awheeze. If the
obstruction is high up, i.e. extrathoracic, the sound is described
asstridor, i.e. during inspiration. This is in contradistinction to
rhonchi which is clas-sically expiratory and due to small airway
obstruction. The CXR here shows a bulgein the lateral wall of the
mid-trachea (Fig. 24.2) due to a tumor. Possibilities
includesquamous cell carcinoma, metastases, mucoepidermoid
carcinoma, adenoidcystic carcinoma and carcinoid tumor. Flexible
bronchoscopy in this patientshowed a mid-tracheal tumor (Fig. 24.3)
and biopsy showed adenoid cystic carci-noma (a low-grade
malignancy).
49 Interpreting Chest X-Rays CASE 25 Fig. 25.1 Case 25. This
was a routine CXR (Fig. 25.1) in an ICU patient who was admitted
for aspiration pneumonia. Name the most obvious abnormality.
CASE 25 Interpreting Chest X-Rays 50 Fig. 25.2C A S E 2 5 M A L
P O S I T I O N E D N A S O G A ST R I C T U B EThe tip of the
nasogastric tube should be seen within the gastric bubble. In
thiscase, the tube has coiled at the esophageal cardia and ended up
in the mid-esophagus (Fig. 25.2). Feeding within the esophagus may
result in fatal aspiration.The CXR also shows evidence of right
lower lobe inltrates, a typical site for aspira-tion
pneumonia.
51 Interpreting Chest X-Rays CASE 26 Fig. 26.1 Case 26. This
was a routine CXR (Fig. 26.1) taken after placement of a subclavian
central venous catheter.
CASE 26 Interpreting Chest X-Rays 52C A S E 2 6 M A L P O S I T
I O N E D R I G H T C E N T R A L V E N O U S C AT H E T E RThe
most obvious abnormality is that the right subclavian central
venous cathetertip has curled upwards into the right internal
jugular vein instead of downwardsinto the superior vena cava. The
other nding is that of soft tissue swelling in theright neck and
superior mediastinal widening. This patient had severe
coagulop-athy and repeated attempts at the central venous catheter
insertion resulted in aneck hematoma which had also tracked
inferiorly causing a mediastinalhematoma. As a result, the patient
required intubation to secure the airway.
53 Interpreting Chest X-Rays CASE 27 Fig. 27.1 Case 27. This
patient was asymptomatic. Past history was significant for previous
thoracotomy. The CXR is shown (Fig. 27.1).
CASE 27 Interpreting Chest X-Rays 54 Fig. 27.2C A S E 2 7 P O
ST L E F T P N E U M O N E C TO MYThere is a homogenous whiteout of
the left hemithorax. The dierential diagnosesare complete left lung
collapse or post left pneumonectomy. The elevation of thegastric
bubble and leftward shift of mediastinum here rule out a massive
leftpleural eusion. The presence of surgical clips in the left
hemithorax in the vicinityof the left main-stem bronchus (Fig.
27.2) makes a left pneumonectomy very likely.
55 Interpreting Chest X-Rays CASE 28 Fig. 28.1 Case 28. This
patient presented with recent onset of dyspnea and streaky
hemoptysis. The CXR is shown (Fig. 28.1). What is the radiologi-
cal diagnosis?
CASE 28 Interpreting Chest X-Rays 56 Fig. 28.2C A S E 2 8 CO L
L A P S E / AT E L E C TA S I S O F T H E L E F T L U N GSee Case
27. There is a homogenous whiteout of the left hemithorax. As in
theprevious case, there is evidence of volume loss in the left lung
with shift of medi-astinum to the left, crowding of the left-sided
ribs and elevation of the left hemi-diaphragm. Flexible
bronchoscopy demonstrated near-total occlusion of the leftmain-stem
bronchus by a tumor (mucoepidermoid carcinoma, Fig. 28.2).
Laserresection of the tumor was then performed, resulting in
restoration of ventilationto the left lung.
57 Interpreting Chest X-Rays CASE 29 Fig. 29.1 Case 29. This
elderly male patient had recent loss of weight and bone pains. What
is the most obvious CXR abnormality (Fig. 29.1)? Name the
differential diagnoses?
CASE 29 Interpreting Chest X-Rays 58C A S E 2 9 I N C R E A S E
D B O N Y D E N S I T I E S D U E TOO ST E O S C L E R OT I C M E
TA STA S E SThe bones show patchy increased density due to
metastases from carcinoma of theprostate. The dierential diagnoses
are Pagets disease and Fluorosis. Cancer ofbreast or lymphoma may
also cause the same appearance. The CXR also showsright lower lobe
inltrates, suggesting aspiration pneumonia, common in the
laststages of patients debilitated with cancer.
59 Interpreting Chest X-Rays CASE 30 Fig. 30.1 Case 30. This
elderly male had recent onset of streaky hemoptysis. Name the
radiological sign (Fig. 30.1).
CASE 30 Interpreting Chest X-Rays 60 Fig. 30.2C A S E 3 0 G O L
D E N S S S I G N O F R I G H T U P P E R LO B E CO L L A P S
EThere is a homogeneous density in the right upper zone and
elevation of the trans-verse ssure. Instead of the transverse ssure
being straight, there is a bulge at themedial end (Fig. 30.2),
giving it an inverted S shape. Golden described this sign andthe
explanation for it is that the upper lobe collapse is due to a
right hilar masswhich accounts for the medial bulge.
61 Interpreting Chest X-Rays CASE 31 Fig. 31.1 Case 31. This
diabetic presented with prolonged pyrexia of uncertain origin
(PUO). Describe the CXR abnormality (Fig. 31.1).
CASE 31 Interpreting Chest X-Rays 62C A S E 3 1 D I F F U S E M
I L I A R Y S H A D O W S D U E TO M I L I A R YT U B E R C U LO S
I SCXR shows bilateral diuse miliary shadows (2 mm diameter) due to
miliarytuberculosis. The dierential diagnoses include previous
varicella infection, dis-seminated histoplasmosis, and silicosis. A
travel history to endemic countries or arelevant occupational
history is helpful to distinguish the various causes. Anothervery
rare cause of such a CXR pattern is pulmonary alveolar
microlithiasis.
63 Interpreting Chest X-Rays CASE 32 Fig. 32.1 Case 32. This
25-year-old female had tiredness and shortness of breath for the
past year. Describe the CXR (Fig. 32.1).
CASE 32 Interpreting Chest X-Rays 64CA SE 32 PRIMARY PULMONARY
HYPERTENSIONThis patient ts the typical clinical and radiological
prole of a patient withprimary pulmonary hypertension. The
pulmonary arteries are markedly enlargedwith the right atrial
chamber also enlarged. The normal right pulmonary descend-ing
artery diameter is less than 16 mm in males and 15 mm in females.
The lungelds are clear and the lung volumes normal making lung
disease causing pul-monary hypertension unlikely. Other causes to
be ruled out are congenital heartdisease and chronic pulmonary
thromboembolism.
65 Interpreting Chest X-Rays CASE 33 Fig. 33.1 Case 33. This
middle-aged male was involved in a motor vehicle acci- dent where
he was the driver and his vehicle was hit from behind resulting in
intense chest pain. His CXR is shown (Fig. 33.1).
CASE 33 Interpreting Chest X-Rays 66 Fig. 33.2C A S E 3 3 T R A
U M AT I C A O R T I C D I S R U P T I O NThis CXR shows evidence
of a widened superior mediastinum and loss of the aorticknuckle and
obliteration of the aorto-pulmonary window. There is left
apicalcapping as a result of mediastinal blood tracking to the
extrapleural region of theleft hemithorax. The trachea is deviated
to the right and the left main-stembronchus is depressed. The fth
and sixth ribs on the left side are fractured.Sometimes there is an
associated left hemothorax. All these are typical features
oftraumatic aortic disruption, which usually occurs just distal to
the ligamentumarteriosum (Fig. 33.2).
67 Interpreting Chest X-Rays CASE 34 Fig. 34.1 Case 34. This
middle-aged female had chronic productive cough for many years.
What is the diagnosis (Fig. 34.1)?
CASE 34 Interpreting Chest X-Rays 68 Fig. 34.2C A S E 3 4 B R O
N C H I E C TA S I S A F F E C T I N G B OT H LO W E RLO B E SThe
CXR shows inltrates especially in the right middle lobe and the
left lowerlobe. The ring shadows and tramlines indicate the
presence of dilated and thick-ened airways. The CXR ndings were
noted a few years previously indicating itschronicity. The accepted
modality for the diagnosis of bronchiectasis is a high-resolution
CT Thorax which demonstrates these dilated airways in the left
lowerlobe (Fig. 34.2) using very thin (12 mm) slices. Bronchography
is now seldomused.
69 Interpreting Chest X-Rays CASE 35 Fig. 35.1 Case 35. This
middle-aged female smoker was asymptomatic. Describe the CXR
abnormality (Fig. 35.1).
CASE 35 Interpreting Chest X-Rays 70 Fig. 35.2 Fig. 35.3C A S E
3 5 S O L I TA R Y P U L M O N A R Y N O D U L E ( S P N ) D U E
TOPRIMARY LUNG CANCERThe CXR shows a 1.5 cm solitary pulmonary
nodule in the left upper lobe (Fig.35.2). An SPN is described as a
single nodule (less than 4 cm) surrounded bynormal lung parenchyma.
The dierential diagnoses for SPN include pseudonodules (e.g. skin
tags, nipple shadows, and bone lesions), primary lung
cancer,solitary metastases, granulomas, arteriovenous
malformations, pseudo tumors,and hamartomas. In this patient, the
CXR a year ago did not demonstrate theshadow. CT (Fig. 35.3) also
demonstrates the nodule to be non-calcied and themargins show
spiculation making the nodule highly suspicious for
malignancy.Thoracotomy and lung biopsy showed primary Stage 1 lung
cancer (adenocarci-noma).
71 Interpreting Chest X-Rays CASE 36 Fig. 36.1 Case 36. This
middle-aged male had loss of weight and bilateral cervical
lymphadenopathy. His CXR is shown (Fig. 36.1).
CASE 36 Interpreting Chest X-Rays 72 Fig. 36.2C A S E 3 6 M E D
I A ST I N A L LYM P H A D E N O PAT H Y D U E TOLYM P H O M ASee
Case 11. The CXR shows asymmetric distortion of the mediastinal
contour bymarkedly enlarged lymph nodes overlying the left hilum.
This is described as thehilar overlay sign the normal left
pulmonary artery (Fig. 36.2) is seen through themass (lying at the
anterior mediastinum). Other dierential diagnoses includechronic
lymphocytic leukemia, sarcoidosis, Castlemans disease, and
granuloma-tous disease like tuberculosis or histoplasmosis. The
histology from medi-astinoscopy in this patient showed Non Hodgkins
lymphoma.
73 Interpreting Chest X-Rays CASE 37 Fig. 37.1 Case 37. This
elderly male was asymptomatic. What is the abnormality on his CXR
(Fig. 37.1)? What is the cause?
CASE 37 Interpreting Chest X-Rays 74 Fig. 37.2C A S E 3 7 B I L
AT E R A L C A LC I F I E D P L E U R A L P L A Q U E SD U E TO A S
B E STO S E X P O S U R EThe CXR shows bilateral calcied pleural
plaques, especially over the diaphrag-matic pleura. The mid-zones
show en face calcication (holly leaf sign). This istypical of
asbestos exposure. Previously asbestos was commonly used as an
insu-lating material. Asbestos exposure can also result in benign
pleural eusion, roundatelectasis, pulmonary brosis (asbestosis), or
malignant mesothelioma.Dierential diagnosis of pleural calcication
includes previous hemothorax,empyema, and tuberculosis. CT also
demonstrates the calcied pleural plaques(Fig. 37.2).
75 Interpreting Chest X-Rays CASE 38 Fig. 38.1 Case 38. This
elderly male was bed-bound because of a massive stroke. Over the
past week, he developed a low-grade fever and became tachypneic and
hypotensive, requiring resuscitation and mechanical ventilation.
What is the radiological sign (Fig. 38.1)? What is the
diagnosis?
CASE 38 Interpreting Chest X-Rays 76 Fig. 38.2C A S E 3 8 W E
ST E R M A R KS S I G N O F A C U T E P U L M O N A R YEMBOLISMThe
CXR shows an oligemic right upper lobe (Westermarks sign) due to
acute pul-monary embolism. Other causes of a hyperlucent lung
include a right pneumo-thorax or huge bullae. Other radiological
signs of pulmonary embolism arewedge-shaped infarct (Hamptons
hump), plate atelectasis, enlarged pulmonaryarteries, or small
pleural eusion. The CXR may also be normal. CT conrms theclot in
the right main pulmonary artery (Fig. 38.2).
77 Interpreting Chest X-Rays CASE 39 Fig. 39.1 Case 39. This
middle-aged male was asymptomatic. What is the CXR abnormality
(Fig. 39.1)?
CASE 39 Interpreting Chest X-Rays 78 Fig. 39.2C A S E 3 9 B A M
B O O S P I N E A P P E A R A N C E D U E TO A N K Y LO S I N GS P
O N DY L I T I SThe most obvious nding is calcication of the
interspinous ligaments causing abamboo spine appearance on CXR,
typical of ankylosing spondylitis. This disordertypically aects
young males with predominant involvement of the axial spine andthe
sacroiliac joints (Fig. 39.2). Upper lobe brosis may also result.
The lung func-tion abnormality that results is usually restrictive.
There is a very strong associa-tion with HLA-B27.
79 Interpreting Chest X-Rays CASE 40 Fig. 40.1 Case 40. This
middle-aged female smoker had hemoptysis and loss of weight. What
is the CXR abnormality (Fig. 40.1)?
CASE 40 Interpreting Chest X-Rays 80CA SE 40 MA SS IN RIGHT
LUNG ARISING FROM TRACHEA ANDRIGHT BRONCHIAL TREEThe CXR shows a
mass in the right upper zone with a pleural eusion, suggestiveof
advanced lung cancer. The lower end of the tracheal air column also
shows nar-rowing, indicating involvement by the cancer. Lung cancer
is the commonestcause of malignant pleural eusion and is usually
secondary to smoking.Squamous cell and small cell lung cancer tend
to involve the central airways, thelatter often associated with
mediastinal lymphadenopathy. Adenocarcinoma of thelung tends to
present as peripheral nodules.
81 Interpreting Chest X-Rays CASE 41 Fig. 41.1 Case 41. This
middle-aged male presented with fever, productive cough, and
shortness of breath of two weeks duration. This was his CXR (Fig.
41.1).
CASE 41 Interpreting Chest X-Rays 82 Fig. 41.2CASE 41 MASSIVE
LEFT PLEURAL EFFUSIONThe CXR shows a dense homogeneous whiteout of
almost the entire left hemi-thorax associated with a shift of
mediastinum to the right, consistent with amassive left pleural
eusion. Collapse and previous pneumonectomy may cause asimilar
appearance except that the mediastinum is shifted to the
ipsilateral side.All patients with unilateral pleural eusion should
be considered for thoracocente-sis to determine the cause of the
eusion. The commonest cause of a massivepleural eusion is
involvement from lung cancer. In this patient,
thoracocentesisyielded frank pus due to an empyema. CT thorax (Fig.
41.2) shows enhancement ofboth the parietal and visceral pleura,
also called the split pleura sign. This resultsfrom intense
inammation of the pleura.
83 Interpreting Chest X-Rays CASE 42 Fig. 42.1 Case 42. This
elderly male presented with left-sided persistent chest pain and
loss of weight for the past few months. He used to work as an
electrician on-board a ship for many years. This was his CXR (Fig.
42.1).
CASE 42 Interpreting Chest X-Rays 84 Fig. 42.2C A S E 4 2 M A L
I G N A N T M E S OT H E L I O M AThe CXR shows a small left
pleural eusion with blunting of the left costophrenicangle. The
left hemithorax is smaller than the right. The mediastinum is
alsowidened due to tumor creeping along the pleura. All these are
features of malig-nant mesothelioma, which is a primary malignancy
of the pleura and typicallyspreads along the pleura as demonstrated
on CT (Fig. 42.2).
85 Interpreting Chest X-Rays CASE 43 Fig. 43.1 Case 43. This
patient was asymptomatic. This was his CXR (Fig. 43.1).
CASE 43 Interpreting Chest X-Rays 86 Fig. 43.2C A S E 4 3 R I G
H T- S I D E D A O R T I C A R C HThe aortic knuckle, which is
usually on the left, is now on the right (Fig. 43.2). Thisis a
congenital abnormality. The commonest type is associated with an
aberrantanterior left common carotid artery and a retroesophageal
left subclavian artery.This is seen in about 1 in 2500 patients and
is not associated with any congenitalheart disease.
87 Interpreting Chest X-Rays CASE 44 Fig. 44.1 Case 44. This
patient was asymptomatic. The CXR is shown (Fig. 44.1).
CASE 44 Interpreting Chest X-Rays 88 Fig. 44.2 Fig. 44.3C A S E
4 4 A N O M A LO U S P U L M O N A R Y V E N O U S D R A I N A G E
S C I M I TA R S I G NThe curvilinear shadow in the right lower
zone is called a Scimitar sign. This is dueto aberrant drainage of
the right inferior pulmonary vein (Fig. 44.2) into the inferiorvena
cava. This is a congenital anomaly and is usually associated with a
small ipsi-lateral hemithorax and a small or hypoplastic pulmonary
artery. This condition isusually of no clinical signicance. The CT
scan shows the enhancing vein (Fig. 44.3).
89 Interpreting Chest X-Rays CASE 45 Fig. 45.1 Case 45. This
middle-aged female complained of hemoptysis and loss of weight of
two months duration. This was her CXR (Fig. 45.1).
CASE 45 Interpreting Chest X-Rays 90C A S E 4 5 L E F T U P P E
R LO B E CO L L A P S E D U E TO L U N G C A N C E RThe CXR shows
evidence of left upper lobe collapse. There is a hazy, veil-like
opaci-cation in the left upper lobe, which does not have a sharp
inferior margin unlikeright upper lobe collapse (see Case 30). This
is because there is usually no lefttransverse ssure and the lobe
collapses anteriorly. There is also volume loss in theleft
hemithorax as evidenced by an elevated left hemidiaphragm and
crowding ofthe left upper ribs. Sometimes the trachea may also be
deviated to the same sideand the aortic knuckle may be obscured by
the collapse.
91 Interpreting Chest X-Rays CASE 46 Fig. 46.1 Case 46. This
was a 48-year-old male with fever of one weeks duration. He was
extremely ill and hypotensive requiring inotrope therapy. His CXR
is shown (Fig. 46.1).
CASE 46 Interpreting Chest X-Rays 92 Fig. 46.2C A S E 4 6 D I F
F U S E N O D U L A R I N F I LT R AT E S S U G G E ST I N
GBACTEREMIA AND SEPTIC LUNG ABSCESSESThe CXR shows nodules in both
lungs (Fig. 46.2), which seem to be peripheral andof roughly equal
size. The dierential diagnosis would be cannon ball
metastasesthough these are typically basal and of unequal size.
This patient actually hasKlebsiella bacteremia. In parts of
South-East Asia, Burkolderia pseudomallei mayresult in the same CXR
appearance. The other important etiologic agent isStaphylococcus
aureus bacteremia.
93 Interpreting Chest X-Rays CASE 47 Fig. 47.1 Case 47. This
patient gave a history of a recent left thoracotomy for massive
hemoptysis. The CXR is shown (Fig. 47.1).
CASE 47 Interpreting Chest X-Rays 94C A S E 4 7 P R E V I O U S
L E F T U P P E R LO B E C TO MYThe CXR shows the left
hemidiaphragm higher than the right, indicating volumeloss of the
left lung. Normally the left hemidiaphragm is about 1 cm lower than
theright (at the height of the dome). The left main-stem bronchus
is also more hori-zontal than usual, indicating volume loss in the
left upper lobe. In addition, thereis subcutaneous emphysema on the
left chest wall.
95 Interpreting Chest X-Rays CASE 48 Fig. 48.1 Case 48. This
patient was asymptomatic. His CXR is shown (Fig. 48.1).
CASE 48 Interpreting Chest X-Rays 96 Fig. 48.2C A S E 4 8 P E R
I C A R D I A L C Y STThe CXR shows a homogeneous opacity in the
right cardio-phrenic angle. Thisopacity has a rounded border and
sharp margins. The right heart border and thediaphragm are
obliterated. CT (Fig. 48.2) shows the mass to be cystic with
low-density material. All these are features of a pericardial cyst
(also called spring watercyst).
97 Interpreting Chest X-Rays CASE 49 Fig. 49.1 Case 49. This
patient was asymptomatic. Her CXR is shown (Fig. 49.1).
CASE 49 Interpreting Chest X-Rays 98 Fig. 49.2 Fig. 49.3C A S E
4 9 P E R I C A R D I A L FAT PA DThe CXR shows opacity in the
right cardio-phrenic angle (Fig. 49.2). Again, theopacity has
obliterated the right heart margin and the diaphragm. CT (Fig.
49.3)shows the density to be fat making this a pericardial fat
pad.
99 Interpreting Chest X-Rays CASE 50 Fig. 50.1 Case 50. This
patient with a history of carcinoma of the colon presented with
chronic cough and loss of weight. The CXR is shown (Fig.
50.1).
CASE 50 Interpreting Chest X-Rays 100 Fig. 50.2C A S E 5 0 M E
TA STA S E S TO L U N G SSee Case 46. The CXR shows bilateral
peripheral lung nodules of varying sizes andthis is better
demonstrated on the CT (Fig. 50.2). This appearance is typical of
lungmetastases. The basal predominance is due to the greater blood
supply in the lungbases. Lung metastases can arise from cancers of
the breast, colon, rectum, andkidney.
101 Interpreting Chest X-Rays CASE 51 Fig. 51.1 Case 51. This
female patient was asymptomatic. Her CXR is shown (Fig. 51.1).
CASE 51 Interpreting Chest X-Rays 102 Fig. 51.2 Fig. 51.3C A S
E 5 1 P U L M O N A R Y P S E U D O - N O D U L E S D U E TO N I P
P L ESHADOWSThere are two nodules (Fig. 51.2), one in each lower
zone where the nipples aresupposed to be. These shadows are
typically homogeneous in appearance withsharp margins or sharp
lateral margins and an absent medial margin. For patientswith
asymmetric nipples, the diagnosis can be dicult but a repeat CXR
(Fig. 51.3)with nipple markers can help conrm that the opacity is
due to a nipple.
103 Interpreting Chest X-Rays CASE 52 Fig. 52.1 Case 52. This
young female had been coughing for the past few weeks. She also had
right-sided pleuritic chest pain. Describe the most obvious CXR
abnormality (Fig. 52.1).
CASE 52 Interpreting Chest X-Rays 104 Fig. 52.2C A S E 5 2 F R
A C T U R E D R I B S W I T H C A L L U S F O R M AT I O NThe CXR
shows densities along the anterolateral aspect of the right fth,
sixth, andseventh ribs (Fig. 52.2). This appearance is consistent
with callus formation alongthe ribs which could be due to cough
fractures. An alternate way to view the ribfracture more clearly is
a right lateral oblique lm.
105 Interpreting Chest X-Rays CASE 53 Fig. 53.1 Case 53. This
middle-aged female presented with a one-year history of exertional
dyspnea. Examination reveals clubbing, and chest ausculta- tion
revealed velcro-like crepitations. Her CXR is shown (Fig.
53.1).
CASE 53 Interpreting Chest X-Rays 106 Fig. 53.2C A S E 5 3 I D
I O PAT H I C P U L M O N A R Y F I B R O S I SThe CXR shows small
bilateral lung volumes. There are basal inltrates which
areperipheral and cystic in appearance, not unlike a honeycomb.
These changes arebetter demonstrated on the CT (Fig. 53.2). This is
the typical appearance ofIdiopathic Pulmonary Fibrosis (also known
as Cryptogenic Fibrosing Alveolitis).The typical prole is a
middle-aged female with shortness of breath over months.It can be
associated with connective tissue diseases like rheumatoid
arthritis andsystemic lupus erythematosis.
107 Interpreting Chest X-Rays CASE 54 Fig. 54.1 Case 54. This
middle-aged woman had symptoms of reflux. This was her CXR (Fig.
54.1).
CASE 54 Interpreting Chest X-Rays 108C A S E 5 4 H I AT U S H E
R N I AThe CXR shows a lucent shadow with an air uid level in the
lower mediastinum.This is typical of a hiatus hernia because of its
midline position with the stomachherniating through the esophageal
hiatus. Also the stomach bubble is not seen inits usual position. A
barium swallow or CT with oral contrast can be done in doubt-ful
cases.
109 Interpreting Chest X-Rays CASE 55 Fig. 55.1 Case 55. This
patient gave a history of tuberculosis in the 1950s for which
surgery was performed. The CXR is shown (Fig. 55.1).
CASE 55 Interpreting Chest X-Rays 110C A S E 5 5 P R E V I O U
S R I G H T T H O R A CO P L A ST YPrior to the advent of eective
anti-tuberculous drugs, surgery was the only treat-ment available
for patients with tuberculosis. The objective was to cause closure
ofthe upper lobe cavities and one option was thoracoplasty which
involves resectionof the upper ribs, resulting in lung collapse. In
this CXR, the right upper chest isdeformed and the pleural space is
calcied. Other procedures performed includearticial pneumothorax,
phrenic nerve crush, or plombage.
111 Interpreting Chest X-Rays CASE 56 Fig. 56.1 Case 56. This
middle-aged male was asymptomatic. His CXR (Fig. 56.1) remained
unchanged for many years.
CASE 56 Interpreting Chest X-Rays 112 Fig. 56.2 Fig. 56.3C A S
E 5 6 B R O N C H O G E N I C C Y STThe CXR shows a bulge at the
right paratracheal stripe (Fig. 56.2). The right para-tracheal
stripe on an erect CXR is normally up to 10 mm wide. Other causes
of awidened right paratracheal stripe include lymphoma, congestive
cardiac failure,vascular abnormalities, and superior mediastinal
masses. The CT (Fig. 56.3) showsa cystic (low-density) mass at the
right paratracheal area, likely to be due to a con-genital
bronchogenic cyst. Bronchogenic cysts can occur in any part of the
medi-astinum but typical sites include the carina, paratracheal,
retrocardiac areas, andadjacent to the esophagus in contact with
the trachea or main bronchi.
113 Interpreting Chest X-Rays CASE 57 Fig. 57.1 Case 57. This
patient gave a history of liver cirrhosis and ascites. The CXR is
shown (Fig. 57).
CASE 57 Interpreting Chest X-Rays 114CASE 57 RIGHT SUBPULMONIC
EFFUSIONThe CXR shows that the right costophrenic angle is blunted
suggestive of a smallpleural eusion. In addition, the right
hemidiaphragm has its highest point dis-placed laterally. Normally
the dome of the hemidiaphragm should have its highestpoint medial
to the midpoint between the midline and the chest wall. These
areclues to the fact that there is uid trapped in the space between
the right hemi-diaphragm and the inferior aspect of the lung.
115 Interpreting Chest X-Rays CASE 58 Fig. 58.1 Case 58. This
elderly patient is asymptomatic. He gave a history of a prolonged
severe viral illness previously. This is his CXR (Fig. 58.1).
CASE 58 Interpreting Chest X-Rays 116 Fig. 58.2C A S E 5 8 C H
R O N I C C A LC I F I C P E R I C A R D I T I SThe CXR shows
calcication of the pericardium (Fig. 58.2) indicative of
previouschronic pericarditis. Causes include previous viral
pericarditis, asbestos exposure,granulomatous disease like
tuberculosis or histoplasmosis, mediastinal irradia-tion, or
trauma. However, a signicant number of such cases have no
apparentcause.
117 Interpreting Chest X-Rays CASE 59 Fig. 59.1 Case 59. This
patient was asymptomatic. The CXR is shown (Fig. 59.1).
CASE 59 Interpreting Chest X-Rays 118 Fig. 59.2C A S E 5 9 R I
G H T U P P E R LO B E S P N D U E TO A C A LC I F I E DG R A N U
LO M AThe CXR shows a dense right upper lobe solitary pulmonary
nodule. The nodule isless than 1 cm (see Case 35) diameter and CT
conrms it to be dense and homoge-neously calcied (Fig. 59.2), a
characteristic of previous granulomatous diseaselike histoplasmosis
or tuberculosis.
119 Interpreting Chest X-Rays CASE 60 Fig. 60.1 Case 60. This
patient was admitted to the ICU for septic shock requiring
mechanical ventilation and inotropic support. This CXR was taken
after admission (Fig. 60.1).
CASE 60 Interpreting Chest X-Rays 120 Fig. 60.2C A S E 6 0 R I
G H T T E N S I O N P N E U M OT H O R A XSee Case 2. The CXR shows
that the endotracheal tube is too far down and the tip isnow
sitting at the origin of the right main-stem bronchus. The ideal
position is forthe tip of the tube to be at the level of the
clavicles. This patient also had a rightcentral venous catheter
inserted. The tip of the central venous catheter shouldideally lie
at the junction of the superior vena cava and the right atrium. The
otherimportant nding is that of a lucent area at the anterior
costophrenic recess on theright side with no lung markings. This is
the deep sulcus sign and is indicative of aright pneumothorax (Fig.
60.2). In addition, the right hemidiaphragm is depressedand the
mediastinum shifted away indicating a tension pneumothorax.
121 Interpreting Chest X-Rays CASE 61 Fig. 61.1 Case 61. This
middle-aged male was diagnosed as having asthma but has not
improved following inhaled steroids. His CXR is shown (Fig.
61.1).
CASE 61 Interpreting Chest X-Rays 122 Fig. 61.2 Fig. 61.3C A S
E 6 1 T R A C H E A L ST E N O S I S D U E TO T R A C H E O PAT H I
AO ST E O C H O N D R O P L A ST I C AThe CXR shows narrowing of
the tracheal air column (Fig. 61.2) with calcicationof the wall.
Tracheal narrowing can be due to malignant causes (lung cancer,
lym-phoma, metastases) or benign causes (post tuberculosis,
posttraumatic, amyloido-sis, sarcoidosis, Wegeners, Tracheopathia
Osteochondroplastica). TracheopathiaOsteochondroplastica (TO) is an
extremely rare condition, characterized by thepresence of multiple
osseous and/or cartilaginous submucosal nodules (Fig.
61.3)protruding into the lumen of the airway. Bronchoscopy is
diagnostic but treatmentis nonspecic and supportive.
123 Interpreting Chest X-Rays CASE 62 Fig. 62.1 Case 62. This
middle-aged male gave a history of lung cancer. Recently, he
complained of loss of weight and shortness of breath. His CXR is
shown (Fig. 62.1).
CASE 62 Interpreting Chest X-Rays 124 Fig. 62.2C A S E 6 2 L U
N G C A N C E R W I T H LYM P H A N G I T I SC A R C I N O M ATO S
I SThe CXR shows a left upper lobe mass and mid-zone inltrates with
a normal heartsize. In addition, there are Kerley B lines (Fig.
62.2) in the periphery of the left midzone, suggestive of lymphatic
distension. These features are consistent with theadvanced lung
cancer metastasizing to the lymphatics. The prognosis is
extremelypoor.
125 Interpreting Chest X-Rays CASE 63 Fig. 63.1 Case 63. This
24-year-old female was asymptomatic. Six months ago, she presented
with pneumonia-like symptoms of cough, fever, and purulent sputum.
Describe her CXR (Fig. 63.1).
CASE 63 Interpreting Chest X-Rays 126 Fig. 63.2CASE 63
BRONCHIOLITIS OBLITERANS ORGANIZINGPNEUMONIA (BOOP)The CXR shows a
right lower lobe inltrate which demonstrates some air bron-chograms
on CT (Fig. 63.2). In addition, there seems to be a beady
appearance tothe inltrates. Pneumonic changes on CXR typically
resolve within three months.She subsequently underwent a
bronchoscopy and transbronchial lung biopsywhich showed BOOP. This
is an idiosyncratic reaction sometimes seen in associa-tion with
drugs, chemical inhalation, connective tissue disease, and various
infec-tions. This is usually very steroid-responsive.
127 Interpreting Chest X-Rays CASE 64 Fig. 64.1 Case 64. This
elderly male had hemoptysis and loss of weight over the past three
months. His CXR is shown (Fig. 64.1).
CASE 64 Interpreting Chest X-Rays 128 Fig. 64.2CASE 64 MASS IN
THE BRONCHUS INTERMEDIUS WITHCO L L A P S E O F T H E M I D D L E A
N D LO W E R LO B EThe CXR shows a density in the right middle
zone. The density is demarcated supe-riorly by a horizontal line,
the transverse ssure, which is pulled down. The medialborder of the
mass has merged with the right heart border indicative of
rightmiddle lobe disease. The right hemidiaphragm is also obscured,
indicating rightlower lobe disease. These features are consistent
with a mass arising from thebronchus intermedius with resultant
collapse of the right middle and lower lobes(Fig. 64.2).
129 Interpreting Chest X-Rays CASE 65 Fig. 65.1 Case 65. This
young female had been breathless over the last two months. Her
symptoms are worse on lying down. Her CXR (Fig. 65.1) is
shown.
CASE 65 Interpreting Chest X-Rays 130 Fig. 65.2C A S E 6 5 A N
T E R I O R M E D I A ST I N A L M A S S D U E TOLYM P H O M AThe
PA CXR shows a mass adjacent to the left heart border. There is
hyperinationof both lung elds, suggesting obstructive airway
disease. The left cardiac marginis obscured, indicating an anterior
mediastinal mass as the heart is an anteriormediastinal structure.
CT (Fig. 65.2) conrms that there is a mass in the
anteriormediastinum and this mass is compressing the lower trachea
and main-stembronchi and right pulmonary artery. The dierential
diagnoses of masses in theanterior mediastinum include the 5 Ts:
thyroid masses, teratoma, thymicmasses, (terrible) lymphoma, and
thoracic aneurysm.
131 Interpreting Chest X-Rays CASE 66 Fig. 66.1 Case 66. This
47-year-old female had streaky hemoptysis for two years associated
with dyspnea on exertion. What does the CXR show (Fig. 66.1)?
CASE 66 Interpreting Chest X-Rays 132 Fig. 66.2 Fig. 66.3CASE
66 RIGHT LUNG OLIGEMIA CARCINOID TUMOR OFR I G H T M A I N ST E M B
R O N C H U SThe CXR shows a hyper-lucent right lung associated
with volume loss as indicatedby an elevated right hemidiaphragm. CT
conrms the presence of the mass in theright main-stem bronchus and
the oligemic right lung (Fig. 66.2). Air trapping maybe
demonstrated on an expiratory CXR showing an exaggeration of the
oligemiaand the shifting away of the mediastinum. In this patient,
bronchoscopy showed aslow-growing carcinoid tumor in the right
main-stem bronchus (Fig. 66.3). Thedierential diagnoses of a
hyper-lucent lung are bullae, acute pulmonaryembolism,
pneumothorax, Macleods syndrome, and a ball-valve-eect type
ofbronchial obstruction.
133 Interpreting Chest X-Rays CASE 67 Fig. 67.1 Case 67. This
patient presented with stridor due to thyroid goiter and was
intubated (Fig. 67.1). Repeat CXR was done six hours later (Fig.
67.2). What is the main radiological abnormality? What is the
cause?
CASE 67 Interpreting Chest X-Rays 134 Fig. 67.2 Fig. 67.3C A S
E 6 7 F L A S H P U L M O N A R Y E D E M A D U E TO U P P E R A I
R WAYO B ST R U C T I O NThe rst CXR shows a normal cardiac shadow
associated with bilateral perihilaralveolar inltrates suggestive of
acute pulmonary edema. The development of pul-monary edema with a
normal heart size is indicative of an acute event. The
rapidclearance of the pulmonary inltrates here indicates that the
process is rapidlycorrected by positive pressure. In this patient,
an important consideration is nega-tive pressure pulmonary edema
due to upper airway obstruction from the thyroidgoiter, which is
seen on the CT (Fig. 67.3).
135 Interpreting Chest X-Rays CASE 68 Fig. 68.1 Case 68. This
elderly female presented with left-sided chest pain of three months
duration. Name the CXR abnormalities (Fig. 68.1).
CASE 68 Interpreting Chest X-Rays 136 Fig. 68.2C A S E 6 8 L E
F T P L E U R A L E F F U S I O N A N D LY T I C L E S I O N I N T
H EL E F T T H I R D R I B S U G G E ST I V E O F M E TA STAT I C D
I S E A S EThe CXR shows a moderate-sized left pleural eusion,
which is loculated. There isalso globular cardiomegaly, suggesting
a pericardial eusion. Pleural tap showedmalignant cells consistent
with the diagnosis of adenocarcinoma of the lung. Inaddition, the
second, third, and fourth ribs on the left side (Fig. 68.2)
demonstratelytic lesions in keeping with bony metastases. Bone scan
would be helpful in con-rming the bone metastases. These are all
features of advanced lung cancer withmetastatic involvement.
137 Interpreting Chest X-Rays CASE 69 Fig. 69.1 Case 69. This
50-year-old female with a past history of tuberculosis had chronic
cough over the past year. Describe her CXR (Fig. 69.1).
CASE 69 Interpreting Chest X-Rays 138 Fig. 69.2C A S E 6 9 L E
F T LO W E R LO B E CO L L A P S EThere is volume loss in the left
lung as indicated by an elevation of the left hemi-diaphragm and
shift of mediastinum to the left. The left hemithorax is also
smallerthan the right. In addition, the left hemidiaphragm is
obscured indicating a leftlower lobe collapse. At bronchoscopy, she
was found to have a benign stricture ofthe left lower lobe orice
(Fig. 69.2) from previous tuberculosis.
139 Interpreting Chest X-Rays CASE 70 Fig. 70.1 Case 70. This
35-year-old female had a long history of chronic produc- tive
cough. Her CXR is shown (Fig. 70.1).
CASE 70 Interpreting Chest X-Rays 140 Fig. 70.2C A S E 7 0 D E
X T R O C A R D I A D U E TO K A R TA G E N E R S S Y N D R O M
EThis patient has obvious dextrocardia (the heart is on the right
side) and situsinversus (the stomach bubble is also on the right
side instead of the left). There isalso right lower lobe
bronchiectasis (Fig. 70.2) as evidenced by bronchial
wallthickening, bronchial opacication (bronchocele), and loss of
volume.Dextrocardia and situs inversus may be associated with
ciliary dysfunction causingsinusitis and bronchiectasis. This is
called Kartageners Syndrome.
141 Interpreting Chest X-Rays CASE 71 Fig. 71.1 Case 71. This
elderly male alcoholic had a binge and subsequently pre- sented
with alcoholic intoxication and vomiting. His CXR is shown (Fig.
71.1). What is the main abnormality?
CASE 71 Interpreting Chest X-Rays 142 Fig. 71.2 Fig. 71.3C A S
E 7 1 M E D I A ST I N I T I SThere is a right-sided pleural eusion
and, in addition, an air-uid level is notedbehind the right side of
the heart (Fig. 71.2). This is typical of a perforated esopha-gus
(Boerhaaves Syndrome due to a full thickness laceration leading to
media-stinitis from vomiting) resulting in free air in the
mediastinum and a pleuraleusion. This patient had food particles at
tube thoracostomy. CT scan shows theright hydropneumothorax due to
the resultant empyema (Fig. 71.3).
143 Interpreting Chest X-Rays CASE 72 Fig. 72.1 Case 72. This
elderly male was totally asymptomatic (Fig. 72.1). What does the
CXR show?