Integrazione del profilo clinico-biologico con le nuove opzioni terapeutiche
Francesca R MauroDipartimento di Biotecnologie Cellulari ed EmatologiaUniversità “ La Sapienza” Roma


FCR the golden standard therapy for all patients?
AgeCytogenetic abnormalities &

CLL8: Genetic effect on PFS
FC FCR
17p-
17p-
13q-
normal
11q-
+12
11q-
+12
normal
13q-

Outcome of 11q- patients: FCR vs FC
p <.001 p <.05
PFS OS
FCR
FC
%CR
FCR FC
61.5 14
p< .001
FCR
FC
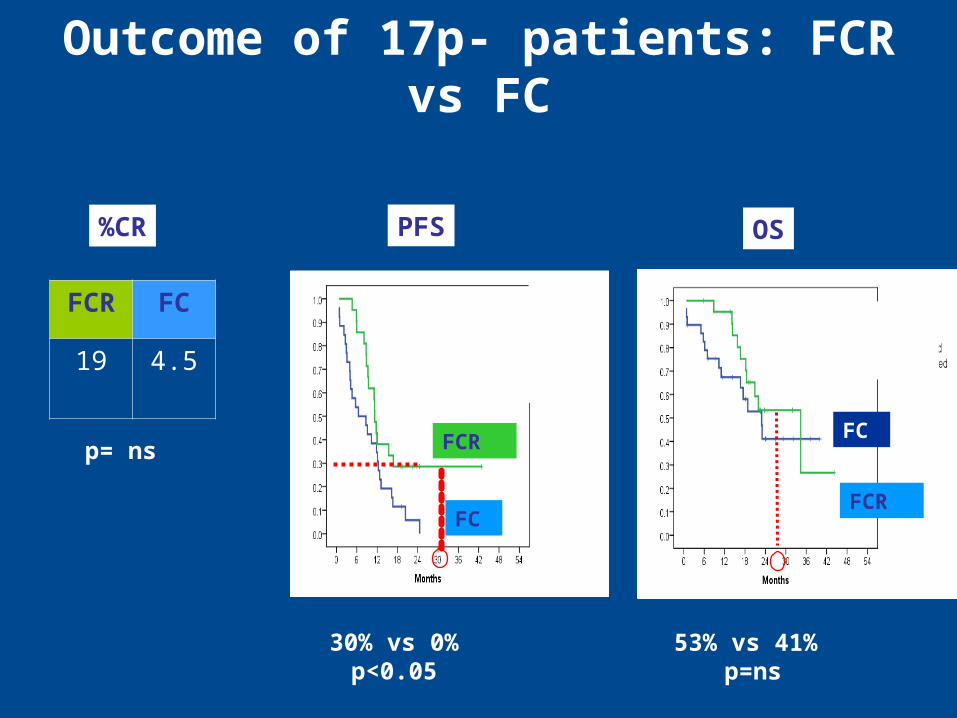
Outcome of 17p- patients: FCR vs FC
p <.001
PFS OS%CR
FCR FC
19 4.5
p= ns FCR
FC
53% vs 41% p=ns
30% vs 0%p<0.05
FCR
FC

FCM-R for Previously Untreated CLL
%
ORR 93
CR MRD - 46
CR MRD + 36
PR 11
Response
82%
MTX 6 mg/m2
FAMP 25 mg/m2
CTX 200 mg/m2
Rituximab 375 (1°)500mg/m2 (2°-6°)
R
D1 D2 D3
CR/PR
Rituximab 375mg/m2
every 3 months
%
CR
%
MRD-
CR
13q- 82 50
+12 100 50
11q- 87 62
17p- 26 0
Bosh, JCO 2009
Response
ORR 77%
CR 14.5%
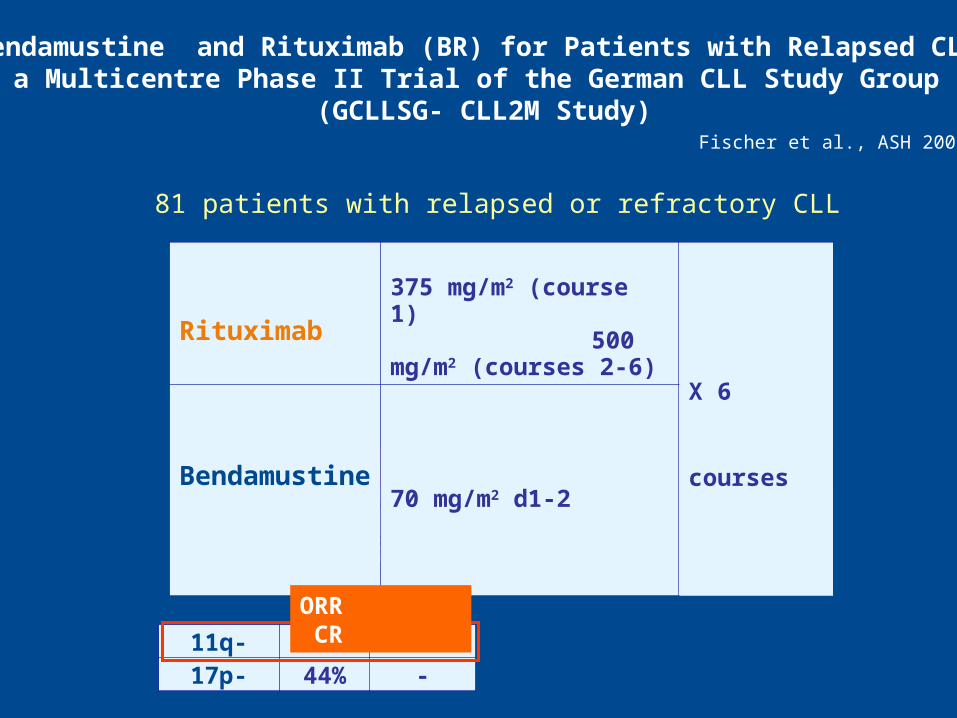
81 patients with relapsed or refractory CLL
Fischer et al., ASH 2008
Toxicity
Leucopenia 12%
Infections 5%
Rituximab375 mg/m2 (course 1) 500 mg/m2 (courses 2-6)
X 6 courses
Bendamustine 70 mg/m2 d1-2
11q- 92% 8%17p- 44% -
Bendamustine and Rituximab (BR) for Patients with Relapsed CLL: a Multicentre Phase II Trial of the German CLL Study Group
(GCLLSG- CLL2M Study)
ORR CR
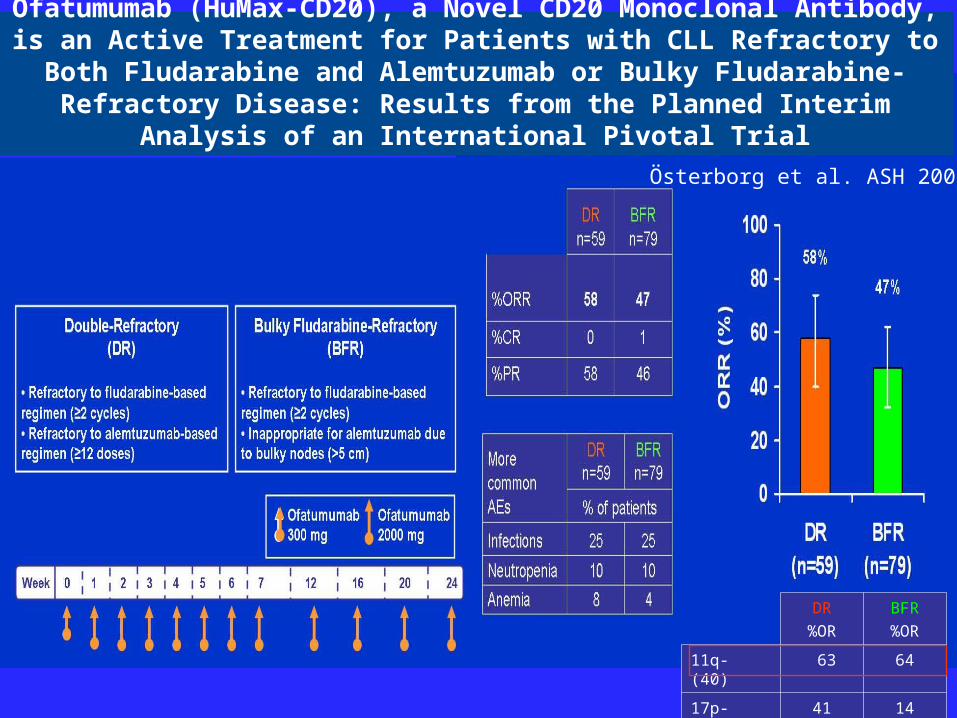
Ofatumumab (HuMax-CD20), a Novel CD20 Monoclonal Antibody, is an Active Treatment for Patients with CLL Refractory to Both Fludarabine
and Alemtuzumab or Bulky Fludarabine-Refractory Disease: Results from the Planned Interim Analysis of an International Pivotal Trial
Österborg et al. ASH 2008
DR
%OR
BFR
%OR
11q- (40) 63 64
17p- (31) 41 14

17p Deletion Predicts for Inferior Overall Survival after Fludarabine ± CTX First Analysis of Genetics in the CLL4 Trial of the GCLLSG
17p- significant adverse impact on:
Response (p=0.001)
PFS (P=0.001)
Survival (P<0.001)
17p-: 4.9% of CLL patients
Stilgenbauer et al., ASH 2005
no 17p-
17p-

CLL4 study: effect of FISH abnormalities
Survival Proportion of 17p-cells and response
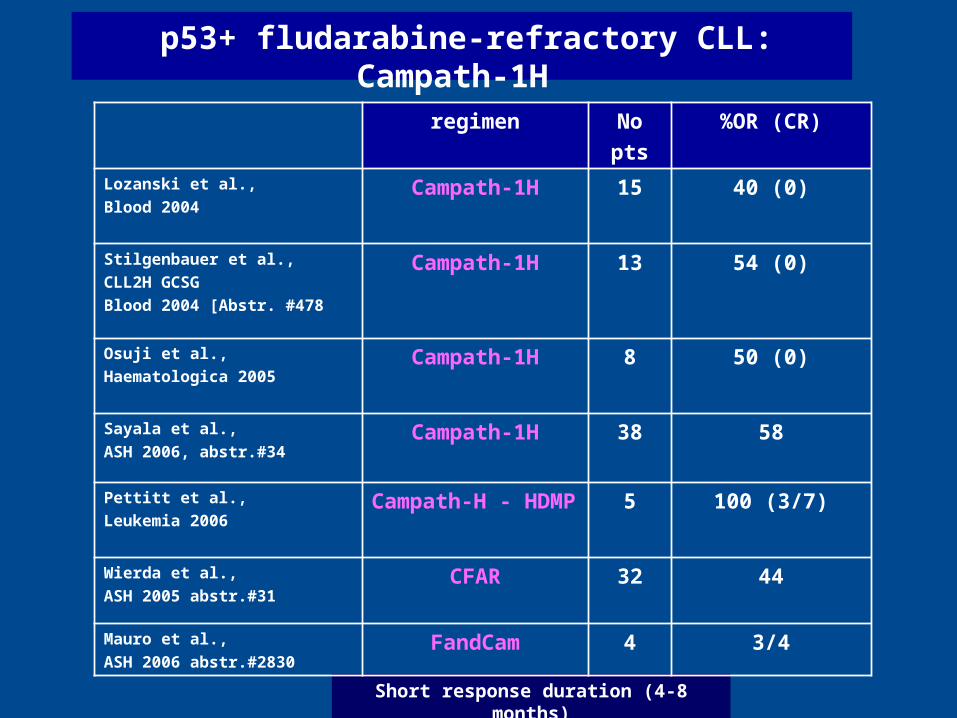
p53+ fludarabine-refractory CLL: Campath-1H
Short response duration (4-8 months)
regimen No
pts
%OR (CR)
Lozanski et al.,
Blood 2004Campath-1H 15 40 (0)
Stilgenbauer et al.,
CLL2H GCSG
Blood 2004 [Abstr. #478
Campath-1H 13 54 (0)
Osuji et al.,
Haematologica 2005Campath-1H 8 50 (0)
Sayala et al.,
ASH 2006, abstr.#34Campath-1H 38 58
Pettitt et al.,
Leukemia 2006Campath-H - HDMP 5 100 (3/7)
Wierda et al.,
ASH 2005 abstr.#31CFAR 32 44
Mauro et al.,
ASH 2006 abstr.#2830FandCam 4 3/4

Sc Campath-1H for fludarabine refractory CLL patientsGCLLSG-CLL2H study
Stilgenbauer et al., JCO 2009

NCRI- UKCLL206- CamPred regimen
PI: A Pettitt
– 50% ORR - Relapse post-remissional therapy
p53 deletion ≥ 20% of cells
HMP HMP HMP HMP

Campath T-cell depletion: the only significant adverse factor for PFS at multivariate analysis
EBMT transplant consensus: allogeneic SCT reasonable option for CLL patients with p53+ abnormalities requiring treatment
Allogeneic Hematopoietic SCT for CLL with 17p deletion: a retrospective analysis of the EBMT
Schetelig et al., JCO 2008
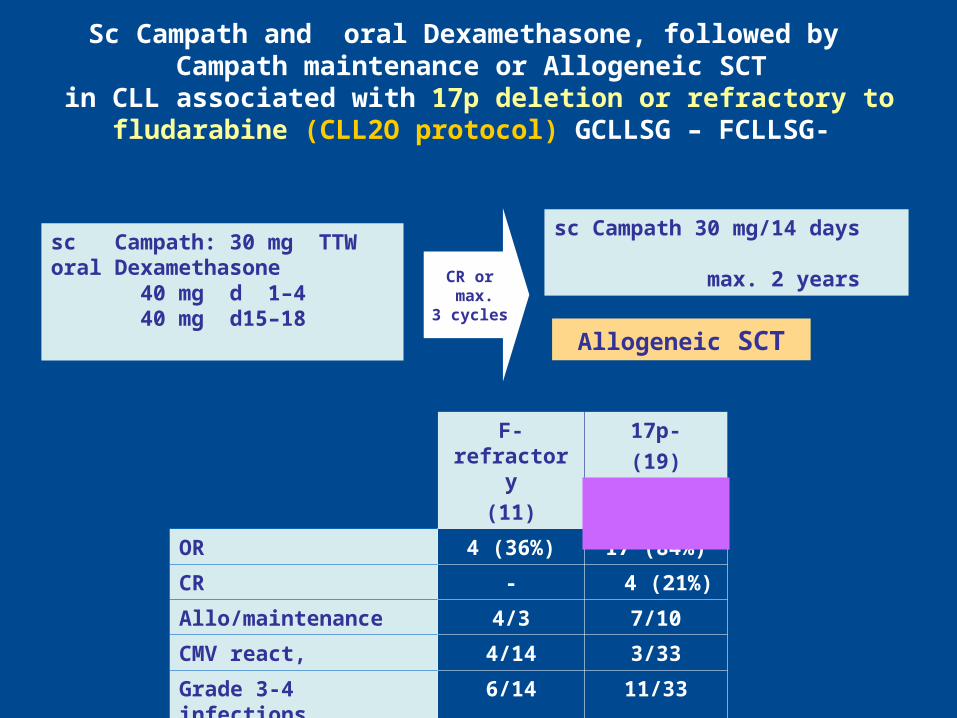
Sc Campath and oral Dexamethasone, followed by Campath maintenance or Allogeneic SCT
in CLL associated with 17p deletion or refractory to fludarabine (CLL2O protocol) GCLLSG – FCLLSG-
sc Campath: 30 mg TTWoral Dexamethasone 40 mg d 1–4 40 mg d15–18
sc Campath 30 mg/14 days max. 2 years
CR or max.
3 cycles
F-refractory
(11)
17p-
(19)
OR 4 (36%) 17 (84%)
CR - 4 (21%)
Allo/maintenance 4/3 7/10
CMV react, 4/14 3/33
Grade 3-4 infections 6/14 11/33
% DFS at 16 mos 60% 60%
Allogeneic SCT

NCRI- UKCLL210 - CamPred regimen
Lenalidomide
p53+ CLL
patients

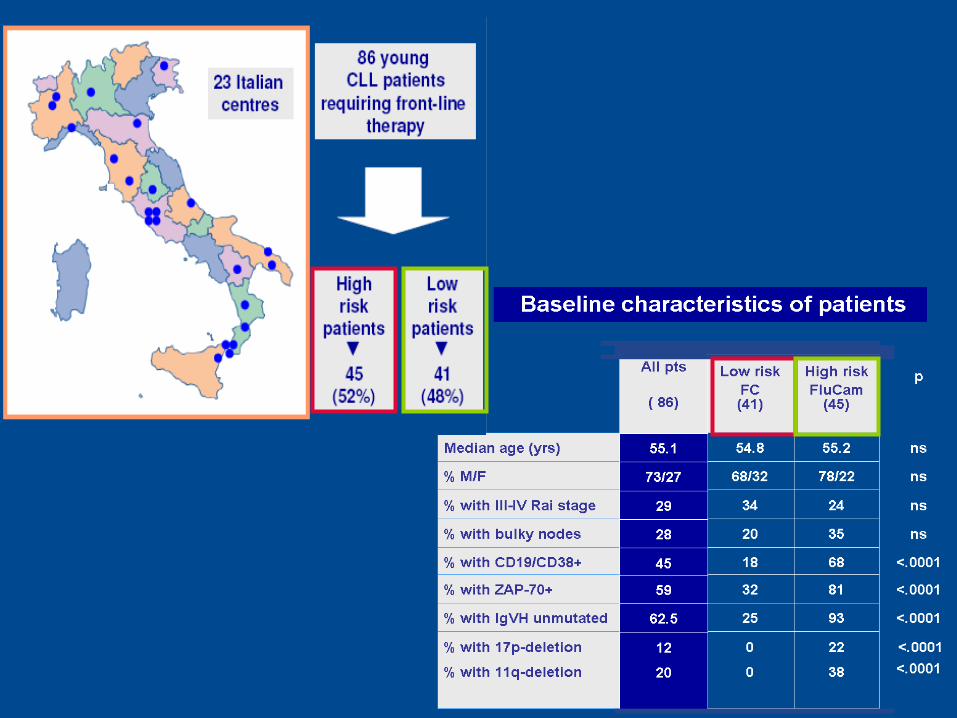
EFFICACY AND SAFETY OF A FIRST-LINE COMBINED THERAPEUTIC APPROACH FOR YOUNG CLL PATIENTS
STRATIFIED ACCORDING TO THE BIOLOGIC PROGNOSTIC FEATURES:
GIMEMA MULTICENTER LLC0405 STUDY

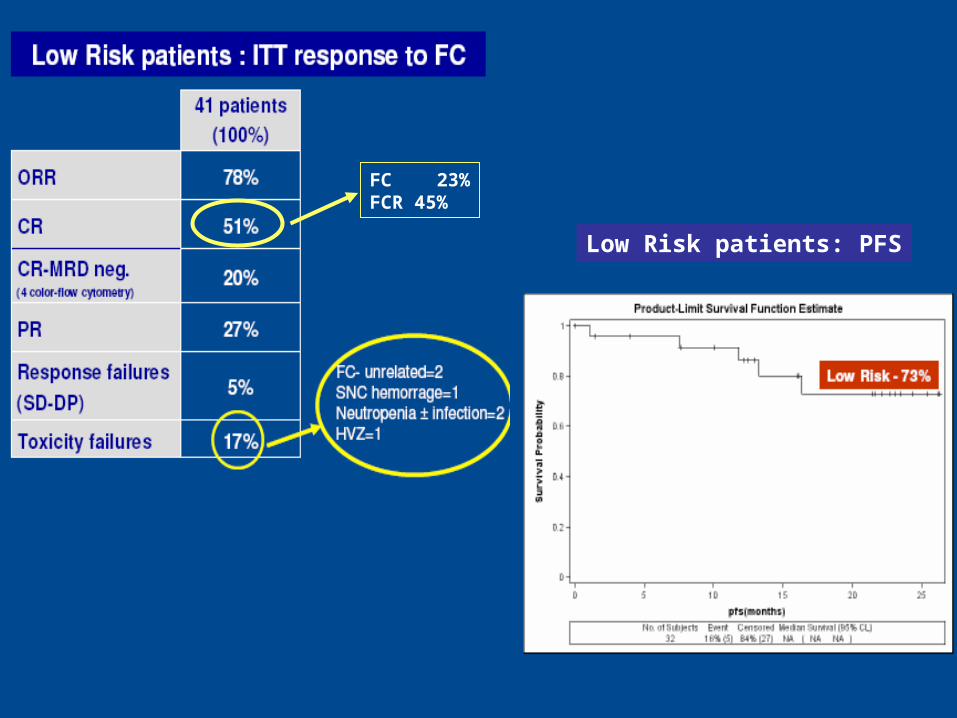
Low Risk patients: PFS
FC 23%FCR 45%
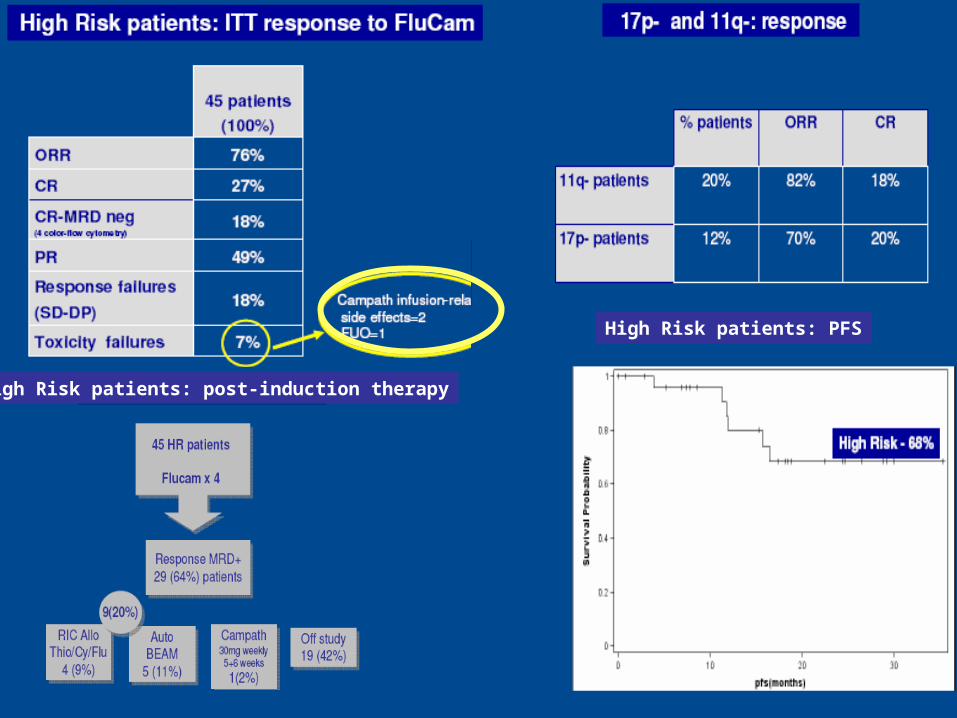
High Risk patients: PFS
High Risk patients: post-induction therapy

FCR: median age of patients•1st-line (CLL8) 61 yrs•2nd-line (REACH) 62 yrs
FCR and age

193 previously treated patients - median age 70 yrs 100 pts fludarabine 25 mg/m2 d1-d5 x 6 courses 93 pts chlorambucil 0.4 mg/kg d1-d15, 0.8 mg/kg increase every 15 days, x 12 months
Fludarabine
Chlorambucil
p= ns
Flu CB
OR 72% 52% <.01
CR 7% 0% <.05
mPFS 19 m 18 m
First-line fludarabine compared with chlorambucil does not result ina major benefit for elderly patients with advanced CLL
Eichhorst et al., Blood 2009
Multivariate analysis shorter PFS and OS: 1. elevated β2 microglobulin 2. ≥ 2 comorbidities R
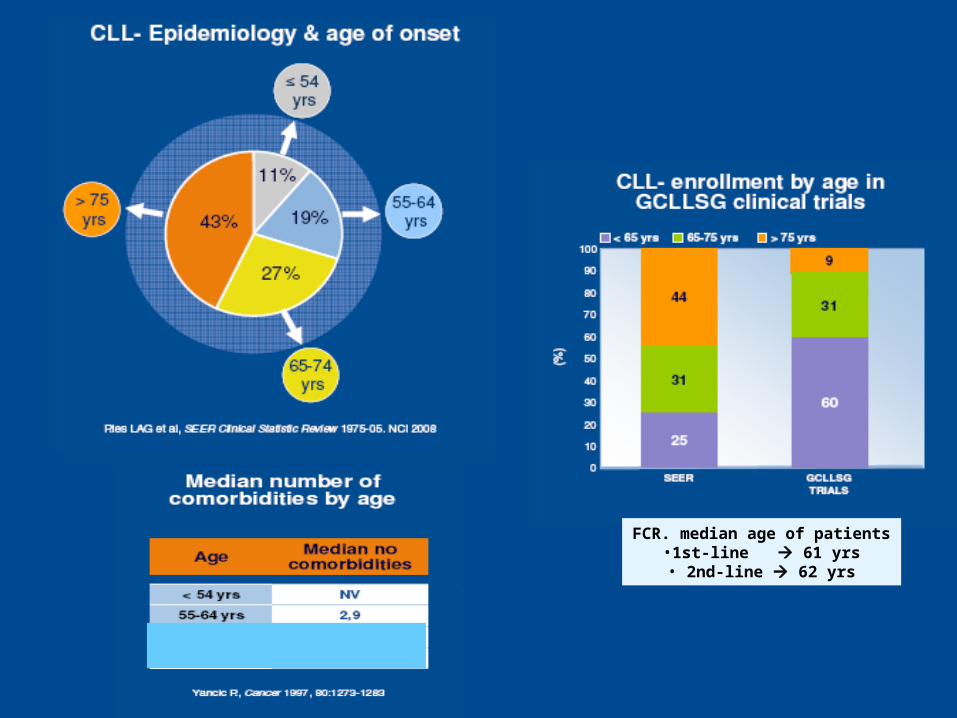
FCR. median age of patients•1st-line 61 yrs• 2nd-line 62 yrs
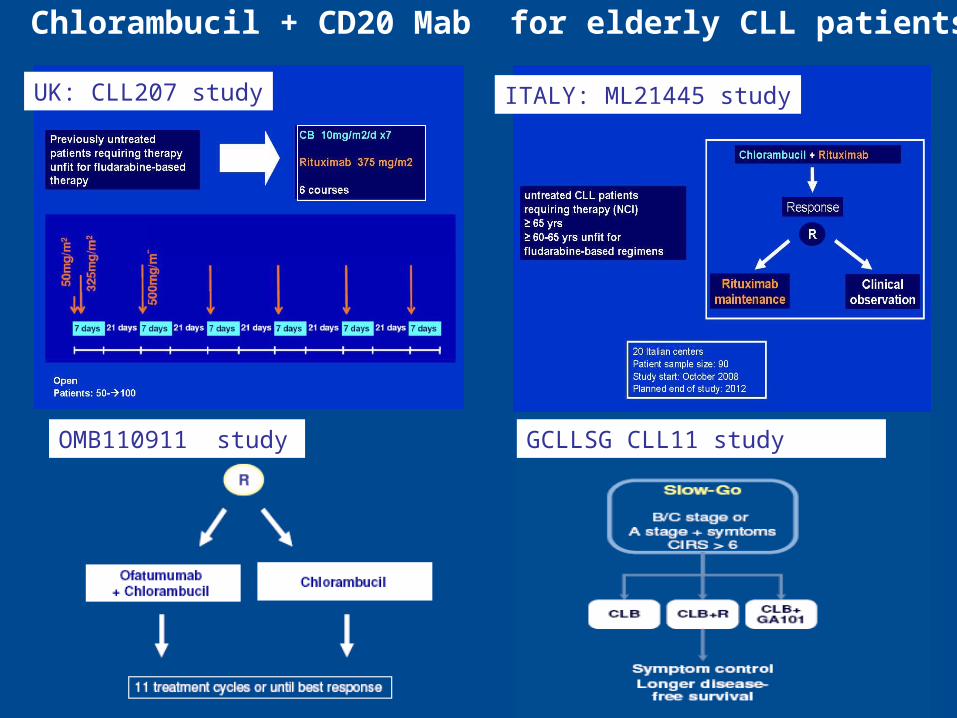
Chlorambucil + CD20 Mab for elderly CLL patients
UK: CLL207 study ITALY: ML21445 study
GCLLSG CLL11 studyOMB110911 study

Lenalidomide-based therapies for elderly CLL patients
>

FCR the new standard treatment for physically fit patients
Specific treatments for patients with selected cytogenetic entities.
Specific treatments for elderly patients under investigation
Conclusions
Recommended