Integrating Family Planninginto PMTCT Services: Promising
Approaches from Tanzania’sIringa and Manyara Regions
Mwanga F; Paul Perchal; Motta W; Killian R; Kikumbih N; Nielsen-Bobbit J
Engenderheath ACQUIRE Tanzania Project

Outline
Background Integration model FP-PMTCT integration activities and results Challenges, lessons learnt, and recommendations

Background: Demographic Profile
Size945,087 sq. km Population of 43,187,823 (2010 projection)
FertilityTFR: 5.4 children per woman
Family PlanningCPR: 34% for any method; 27% modern methods Unmet need: 25% among married women (16% spacing and 9% limiting)
Maternal Health 96% received ANC from health professional51% deliveries assisted by health professionals
HIV/AIDSAdult prevalence rate 5.6% Prevalence among women attending ANC is 6.9%
Source Tanzania: TDHS 2010, THIV survey 2008

The ACQUIRE Tanzania Project (ATP)
Supports the Ministry of Health and Social Welfare to increase the quality of and access to: – Family planning services– Comprehensive post abortion care– PMTCT– Gender-based violence services
Supports integration of FP-PMTCT in Iringa and Manyara

Model of FP/PMTCT Integration
Antenatal Care
Labor andDelivery/Postnatal
Postnatal Care
Care and Treatment
FP Clinic(postpartum visit)

Activities to Strengthen FP-PMTCT Integration
Supply – Training and supportive supervision– Renovations /infrastructure – Procurement – Quality improvement
Enabling environment– Contribute to national guidelines– Build partnerships
Demand – Engage communities – Increase male involvement

How Do We Put This into Practice?
1,134 PMTCT service providers trained to offer FP counseling
HIV counseling and testing: HIV+ women who are and not eligible for ART are given ARV for prophylaxis
All pregnant women encouraged to deliver in health facilities and counseled on FP
All ANC clients are counseled on safer sex and given condoms for dual protection

How Do We Put This into Practice? cont’d.
After labor and delivery, mothers receive FP counseling and advice to attend FP clinic during their postpartum visit
At FP clinic, women with unknown status are offered HIV counseling and testing
If a woman chooses a LAPM and cannot get it at that facility, she receives a referral
Information on FP and PMTCT services also provided at mother and child health clinics (MCH)
FP data are collected using monthly PMTCT summary forms and register books

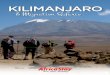
HIV-positive Women Receiving FP Methods atATP-Supported PMTCT Sites

Assessment of FP-PMTCT Integration
In collaboration with 12 districts in Iringa and Manyara
Priority areas for action identified included:– Additional provider training– Addressing stock-outs – Increased promotion of dual protection in both HIV and
FP services– Addressing loss to follow-up through strengthening
additional entry points for FP services

Ongoing Challenges
Shortage of FP commodities Human resource shortages Lack of adequate space for integrated services M&E tools are not designed to capture
integrated services Loss to follow-up of HIV-positive women Low male involvement

Recommendations
Let’s take it to scale! More research to prevent loss-to-follow-up Logistics and M&E systems need to better
integrated Coordinate and harmonize partnerships Government commitment in integration is high
but has not been translated to resource allocation

Client Perspectives
“A mother who has HIV should not be sent somewhere else. She should get everything at one table.”
– HIV+ woman at postnatal clinic
“We learnt of our HIV status when I escorted my wife to the antenatal clinic. We followed all the advise and thanks God, our child was born HIV negative. We were informed about FP during delivery we went back for an implant. We are very happy with this method.”
– HIV+ couple

ACKNOWLEDGEMENT
PEPFAR MOHSW Districts – Council Health Management Teams
(CHMTs) ATP supported facility management and staff EH HQ Engender health Partners
Recommended