Innovating for the future:
The Army Medical School at Netley and developments in infectious diseases
Introduction
British Science Week 2021 has the theme of 'Innovating
for the Future'. With this in mind, we have chosen to
celebrate the medical developments that came out of the
Army Medical School at Netley in the mid to late 19th
century, particularly in the field of infectious diseases. Not
only did these tackle some of the most serious problems
facing British forces stationed overseas at the time, but
they also paved the way for many future developments.
The Netley staff and students you will encounter over the
following pages really were 'innovating for the future' -
our present.
We would like to acknowledge the considerable contribution made by volunteer Tim Ford, whose extensive research forms the basis for this presentation.
We would also like to thank the University of Southampton for their generous sponsorship of our British Science Week activities.
Contents
Historical & Military Context 5
Scientific & Medical Context 15
Cholera 24
Malaria 36
Leishmaniasis 42
Brucellosis 50
Dysentery 59
Typhoid (Enteric) Fever 64
Trench Fever 72

Historical and Military Context
Return to Contents
Any consideration of the advances in medical science
pioneered at the Royal Victoria Hospital, or by those
associated with its Army Medical School, must start with
the military background.
It must take account of the following: Great Britain’s
global standing and international relationships in the mid-
nineteenth century; the reasons for the foundation of the
hospital; and the purpose of a military medical school.
Painting: The Founding of Australia 1787 by A. Talmage 1937.Creative Commons
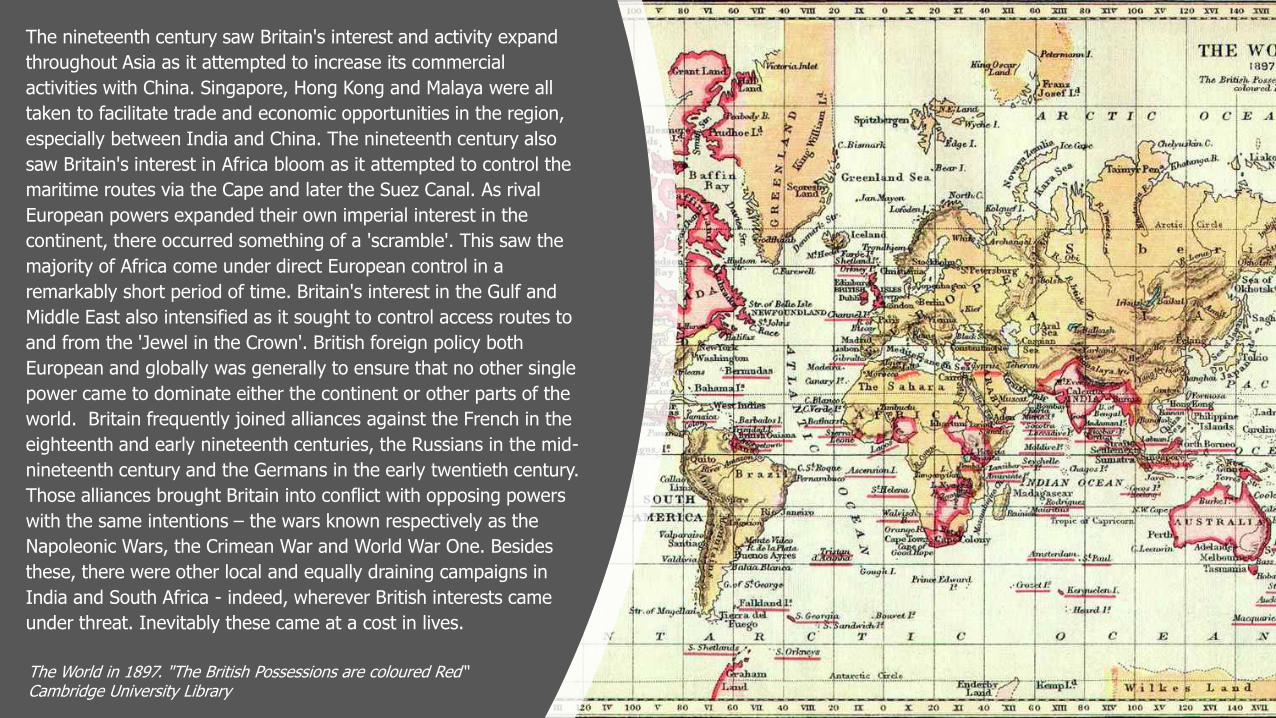
The nineteenth century saw Britain's interest and activity expand
throughout Asia as it attempted to increase its commercial
activities with China. Singapore, Hong Kong and Malaya were all
taken to facilitate trade and economic opportunities in the region,
especially between India and China. The nineteenth century also
saw Britain's interest in Africa bloom as it attempted to control the
maritime routes via the Cape and later the Suez Canal. As rival
European powers expanded their own imperial interest in the
continent, there occurred something of a 'scramble'. This saw the
majority of Africa come under direct European control in a
remarkably short period of time. Britain's interest in the Gulf and
Middle East also intensified as it sought to control access routes to
and from the 'Jewel in the Crown'. British foreign policy both
European and globally was generally to ensure that no other single
power came to dominate either the continent or other parts of the
world. Britain frequently joined alliances against the French in the
eighteenth and early nineteenth centuries, the Russians in the mid-
nineteenth century and the Germans in the early twentieth century.
Those alliances brought Britain into conflict with opposing powers
with the same intentions – the wars known respectively as the
Napoleonic Wars, the Crimean War and World War One. Besides
these, there were other local and equally draining campaigns in
India and South Africa - indeed, wherever British interests came
under threat. Inevitably these came at a cost in lives.
The World in 1897. "The British Possessions are coloured Red“Cambridge University Library
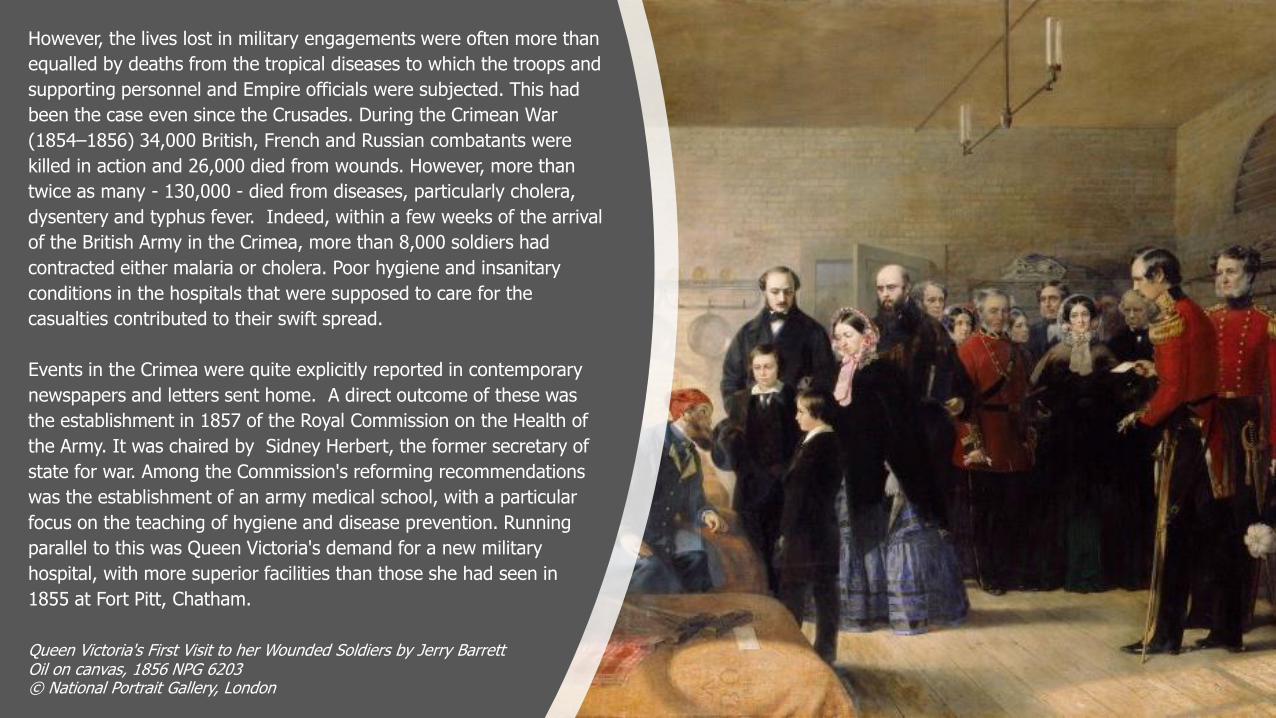
Queen Victoria's First Visit to her Wounded Soldiers by Jerry BarrettOil on canvas, 1856 NPG 6203© National Portrait Gallery, London
However, the lives lost in military engagements were often more than
equalled by deaths from the tropical diseases to which the troops and
supporting personnel and Empire officials were subjected. This had
been the case even since the Crusades. During the Crimean War
(1854–1856) 34,000 British, French and Russian combatants were
killed in action and 26,000 died from wounds. However, more than
twice as many - 130,000 - died from diseases, particularly cholera,
dysentery and typhus fever. Indeed, within a few weeks of the arrival
of the British Army in the Crimea, more than 8,000 soldiers had
contracted either malaria or cholera. Poor hygiene and insanitary
conditions in the hospitals that were supposed to care for the
casualties contributed to their swift spread.
Events in the Crimea were quite explicitly reported in contemporary
newspapers and letters sent home. A direct outcome of these was
the establishment in 1857 of the Royal Commission on the Health of
the Army. It was chaired by Sidney Herbert, the former secretary of
state for war. Among the Commission's reforming recommendations
was the establishment of an army medical school, with a particular
focus on the teaching of hygiene and disease prevention. Running
parallel to this was Queen Victoria's demand for a new military
hospital, with more superior facilities than those she had seen in
1855 at Fort Pitt, Chatham.
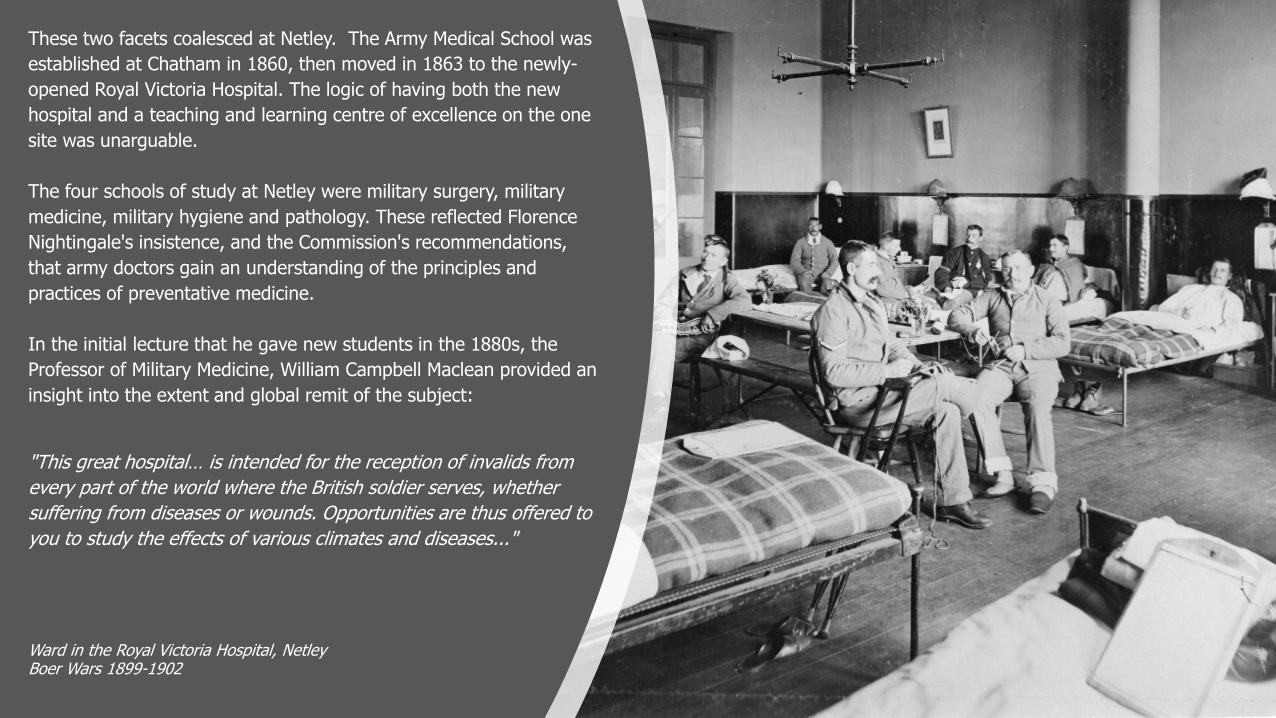
These two facets coalesced at Netley. The Army Medical School was
established at Chatham in 1860, then moved in 1863 to the newly-
opened Royal Victoria Hospital. The logic of having both the new
hospital and a teaching and learning centre of excellence on the one
site was unarguable.
The four schools of study at Netley were military surgery, military
medicine, military hygiene and pathology. These reflected Florence
Nightingale's insistence, and the Commission's recommendations,
that army doctors gain an understanding of the principles and
practices of preventative medicine.
In the initial lecture that he gave new students in the 1880s, the
Professor of Military Medicine, William Campbell Maclean provided an
insight into the extent and global remit of the subject:
"This great hospital… is intended for the reception of invalids from
every part of the world where the British soldier serves, whether
suffering from diseases or wounds. Opportunities are thus offered to
you to study the effects of various climates and diseases..."
Ward in the Royal Victoria Hospital, NetleyBoer Wars 1899-1902
Surgeon-Major William Campbell Maclean (1811-1898)
Maclean was equally explicit as to the need of such special
instruction for military medical personnel:
"above all because 60,000 British soldiers are always serving in
India, requiring a large staff of carefully instructed medical officers
for their care. Nor is this all. Side by side with those who devote
their lives to the service of the British army sit a body of gentlemen,
for whose benefit no less than theirs, this school was established.
For them the study of tropical medicine is of vital importance. All
their professional lives will be spent in India; on them the medical
charge of a large native army will devolve, without the aid of which
it would be impossible to hold India as a British possession... To
them will in the future be committed the care of the valuable lives of
those charged with the civil administration of India... From the ablest
of them, the selection of teachers will be made to fill the chairs of
the medical and allied sciences in the colleges established by an
enlightened Government, and to be advisers on all questions
affecting the health of the 200,000,000 people of the various races
of the Queen’s empire of Hindustan."
A group of hospital patients at Netley during World War One.
The importance of India and the medical care of both the British
armed forces and the civilian population is clear. This is reinforced by
the fact that for 15 years from 1865, students for the Indian Medical
Service were required to undertake the same training as their British
counterparts at Netley. However other parts of the Empire, and a
world in which British geo-political interests were paramount,
brought their own local medical challenges. The pages that follow
highlight the most significant diseases encountered by the military.
Although most prevalent in tropical areas, in a world where
sanitation was often still rudimentary, they could develop and blight
forces and the supporting civilians almost anywhere.
The campaigns fought in South Africa in the late nineteenth century
brought significant loss of life from typhoid. The strategic outpost of
Malta in the Mediterranean was frequently and significantly impacted
by brucellosis. British interests in India were severely affected by
outbreaks of malaria, leishmaniasis and cholera. Finally, even
fighting close to home on the Western Front in the early twentieth
century saw the emergence of a new debilitating condition, trench
fever, to be diagnosed, treated and overcome by those associated
with the Army Medical School.
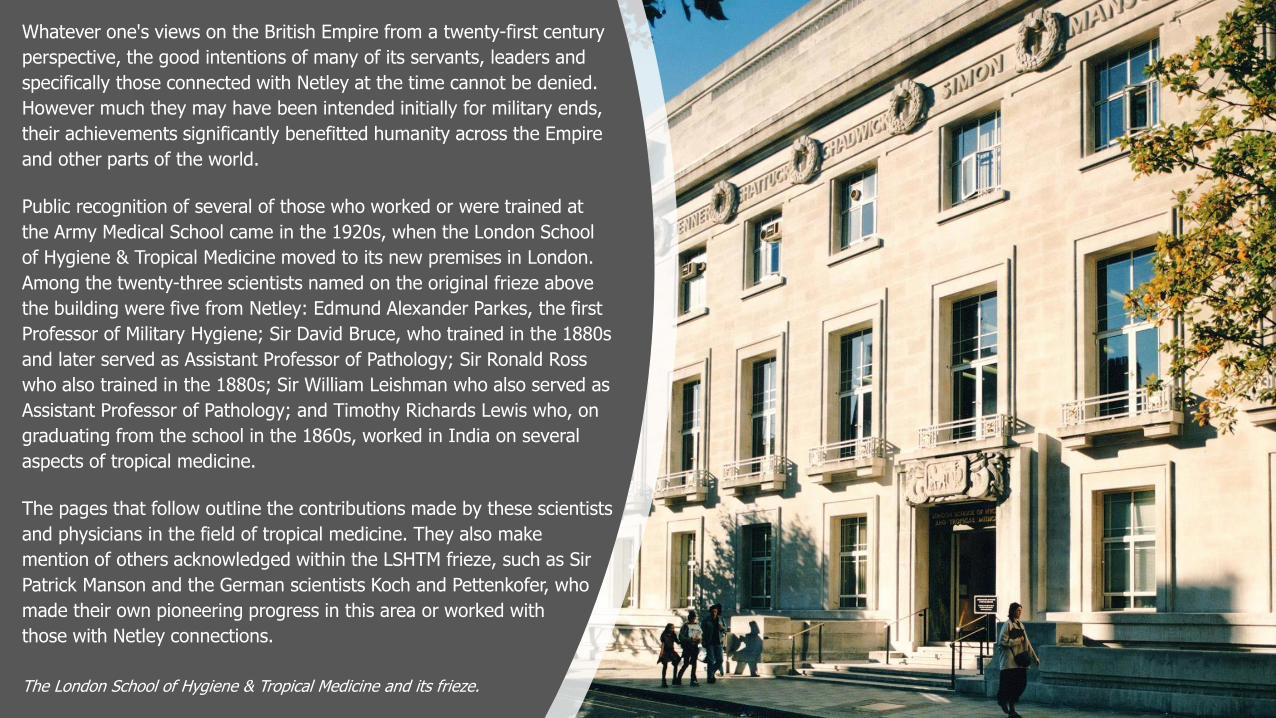
The London School of Hygiene & Tropical Medicine and its frieze.
Whatever one's views on the British Empire from a twenty-first century
perspective, the good intentions of many of its servants, leaders and
specifically those connected with Netley at the time cannot be denied.
However much they may have been intended initially for military ends,
their achievements significantly benefitted humanity across the Empire
and other parts of the world.
Public recognition of several of those who worked or were trained at
the Army Medical School came in the 1920s, when the London School
of Hygiene & Tropical Medicine moved to its new premises in London.
Among the twenty-three scientists named on the original frieze above
the building were five from Netley: Edmund Alexander Parkes, the first
Professor of Military Hygiene; Sir David Bruce, who trained in the 1880s
and later served as Assistant Professor of Pathology; Sir Ronald Ross
who also trained in the 1880s; Sir William Leishman who also served as
Assistant Professor of Pathology; and Timothy Richards Lewis who, on
graduating from the school in the 1860s, worked in India on several
aspects of tropical medicine.
The pages that follow outline the contributions made by these scientists
and physicians in the field of tropical medicine. They also make
mention of others acknowledged within the LSHTM frieze, such as Sir
Patrick Manson and the German scientists Koch and Pettenkofer, who
made their own pioneering progress in this area or worked with
those with Netley connections.
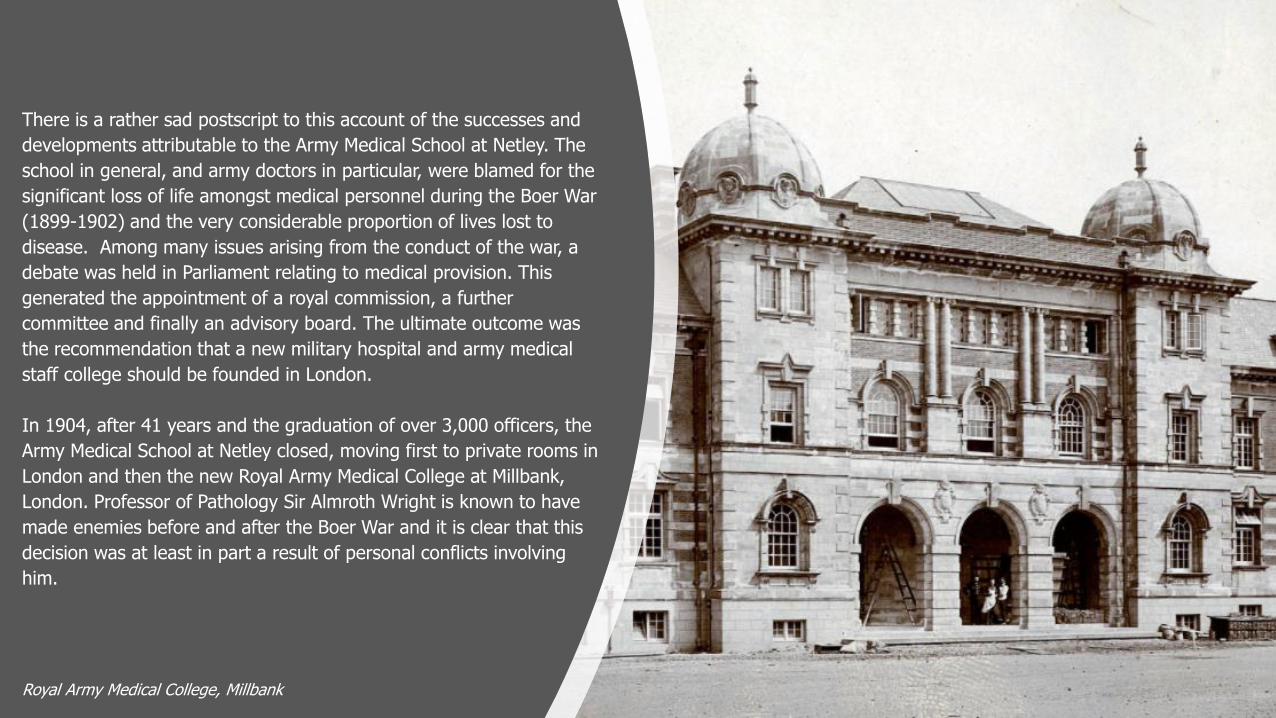
Royal Army Medical College, Millbank
There is a rather sad postscript to this account of the successes and
developments attributable to the Army Medical School at Netley. The
school in general, and army doctors in particular, were blamed for the
significant loss of life amongst medical personnel during the Boer War
(1899-1902) and the very considerable proportion of lives lost to
disease. Among many issues arising from the conduct of the war, a
debate was held in Parliament relating to medical provision. This
generated the appointment of a royal commission, a further
committee and finally an advisory board. The ultimate outcome was
the recommendation that a new military hospital and army medical
staff college should be founded in London.
In 1904, after 41 years and the graduation of over 3,000 officers, the
Army Medical School at Netley closed, moving first to private rooms in
London and then the new Royal Army Medical College at Millbank,
London. Professor of Pathology Sir Almroth Wright is known to have
made enemies before and after the Boer War and it is clear that this
decision was at least in part a result of personal conflicts involving
him.
Laboratory at the Army Medical School, Netley in the late 19th Century.
The decision was fiercely opposed by at least one writer to the
journal Nature. They predicted “a disastrous effect on the future
prospects of the development of scientific research in connection
with the Service”. The writer lamented that “clinical study in
tropical medicine has been eliminated from the programme of
instruction for officers entering the Army Medical Service” and how
“the transfer of the research laboratories must be detrimental to
the progress of research in tropical medicine”.
This letter was penned nearly 120 years ago. It is therefore
interesting, if disheartening, to recall the many enquiries in recent
years into the Science, Technology, Engineering and Maths (STEM)
skills gap in the UK. A 2018 report from STEM Learning noted that
the shortage of high level STEM skills is costing British businesses
£1.5 billion a year. Yvonne Baker, Chief Executive of STEM Learning
said: “We are heading towards a perfect storm for STEM
businesses in the UK - a very real skills crisis at a time of
uncertainty for the economy..."
What a pity it is that the words penned by the writer to the journal
Nature fell on deaf ears. With staggering foresight they concluded:
“the rulers of the Empire will some day understand what immense
loss the neglect of science entails, and until this is fully appreciated
it is the duty of all who know to explain on every occasion”.
Scientific and Medical Context
Return to Contents
The second half of the nineteenth century was an era of
very significant developments in medical science. The
achievements of those who trained or worked at the Royal
Victoria Hospital cannot be seen in isolation from (and
were in large part a product of) such progress made in
the Victorian age both in Great Britain and across Europe.
The list featured here of these milestones and other
significant events is set in the context of the
commissioning of a new military hospital in 1855 and its
opening at Netley in 1863. It is striking in the twenty-first
century to realise just how recent some of the innovations
are. However, it is also valuable to understand the level of
progress that had been made in medical science and how
standardised were treatments at the time the hospital
opened - the base from which its operations started.
Before the Hospital was commissioned
The first half of the nineteenth century may be termed the pre-sanitary
age. Medical treatments relied heavily on the following: a ‘change of
air’ (to the coast or mountains perhaps); the taking of emetic or
laxative substances; bleeding by cup or leeches to clear impurities; the
ingestion of mercury in small doses; and the power of prayer.
1796: Edward Jenner developed and pioneered the use of a vaccine
against smallpox, one of the great killer diseases. He believed that
vaccines should be free at the point of delivery, available to everyone,
no matter who they were or where they were from.
1847: James Simpson – pioneered the use of chloroform as the first
effective anaesthetic used during surgery. This notably helped women
in childbirth. In 1853 Queen Victoria’s eighth child was born with the
use of chloroform. This effectively silenced all opposition to Simpson
and his stance on pain-free childbirth. Simpson went on to work on
hospital infection and surgical sepsis. He advocated preventative
methods such as cleansing hands and instruments to avoid infection.
This reinforced the findings of the Hungarian Ignaz Semmelweis,
who insisted that doctors should disinfect their hands before
involvement in childbirth procedures.
Illustration of Edward Jenner vaccinating a child against smallpox.The New York Academy of Medicine Library
1848: the publication of Buchan’s Domestic Medicine. Listed
among the general causes of common illnesses were: night air,
sedentary habits, anger, wet feet and abrupt changes in temperature.
Cholera was said to be caused by rancid or putrid food, by ‘cold food’
such as cucumbers and melons and by passionate fear or rage.
Miasma or ‘bad air’ theory was borne out in contemporary views about
the spread of malaria and cholera. It was commonly believed, and
had been since ancient times, that diseases were the product of
environmental factors such as contaminated water, foul air, and poor
hygienic conditions. By this theory, diseases were not passed from
person to person, but would affect individuals within the locale that
gave rise to these foul smells.
1853: Scottish physician Alexander Wood added a plunger and
glass syringe to the hollow needle invented in 1844 by Francis Rynd,
creating the modern hypodermic needle. This allowed doctors to
estimate dosage based on the amount of liquid observed through the
glass. This gave a new and effective way of administering drugs into
the human body.
An 1831 colour lithograph by Robert Seymour depicts cholera as a robed, skeletal creature emanating a deadly black cloud.US National Library of Medicine photographic archive.
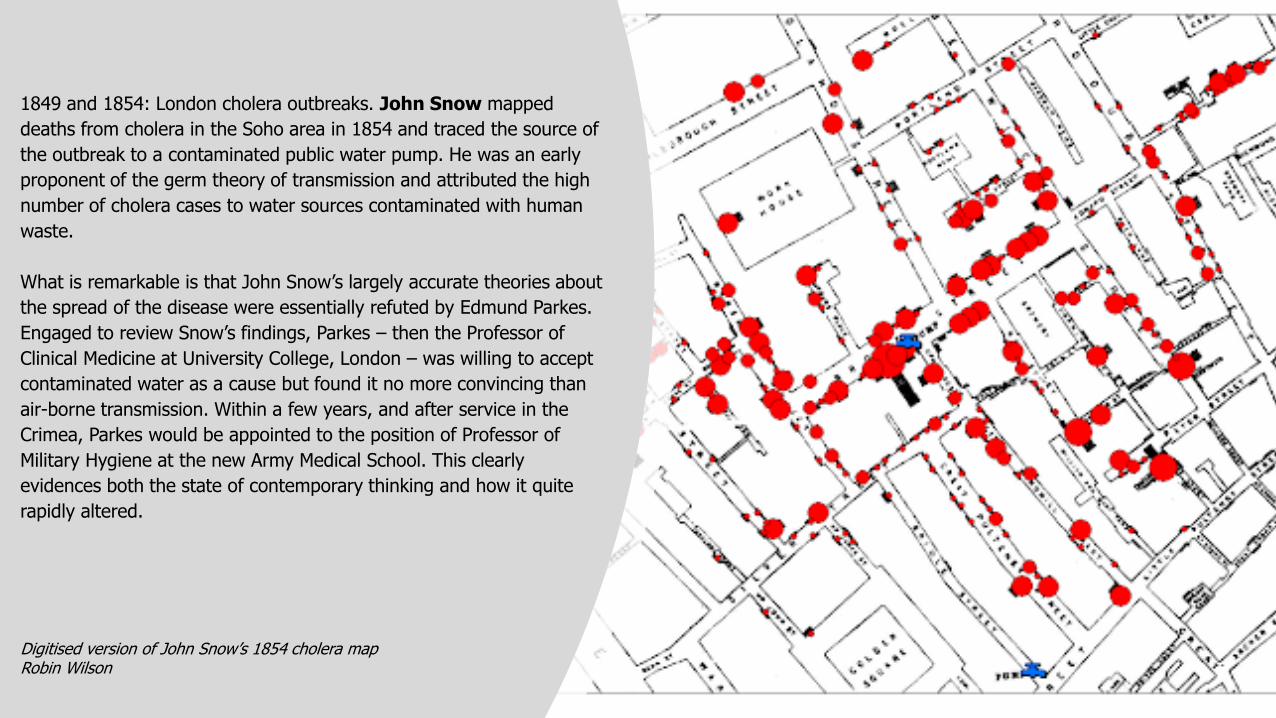
1849 and 1854: London cholera outbreaks. John Snow mapped
deaths from cholera in the Soho area in 1854 and traced the source of
the outbreak to a contaminated public water pump. He was an early
proponent of the germ theory of transmission and attributed the high
number of cholera cases to water sources contaminated with human
waste.
What is remarkable is that John Snow’s largely accurate theories about
the spread of the disease were essentially refuted by Edmund Parkes.
Engaged to review Snow’s findings, Parkes – then the Professor of
Clinical Medicine at University College, London – was willing to accept
contaminated water as a cause but found it no more convincing than
air-borne transmission. Within a few years, and after service in the
Crimea, Parkes would be appointed to the position of Professor of
Military Hygiene at the new Army Medical School. This clearly
evidences both the state of contemporary thinking and how it quite
rapidly altered.
Digitised version of John Snow’s 1854 cholera mapRobin Wilson
During the construction of the hospital
1858: the ‘Great Stink’. Hot weather in central London in July and
August 1858 exacerbated the smell of untreated human waste and
industrial effluent that was present on the banks of the River Thames.
The problem had been mounting for some years and was due to an
ageing and inadequate sewer system that emptied directly into the
Thames. The miasma from the effluent was thought to transmit
contagious diseases. The smell and fears of its possible effects
prompted action from the local and national administrators. They
accepted a proposal from the civil engineer Joseph Bazalgette to
move the effluent eastwards along a series of interconnecting sewers
that sloped towards outfalls beyond the metropolitan area.
1861: Louis Pasteur and ‘germ theory’. Pasteur published his theory
suggesting bacteria cause human diseases. He based his ideas on
experiments which proved that germs make milk go bad and cause
diseases in animals. Pasteur insisted that ‘germs’ could be spread by
human contact and even transmitted by medical instruments. Further
experiments convinced many doctors he was correct, however the
miasma ‘bad air’ theory persisted for some decades. Commentators
maintain that of all nineteenth century medical/scientific discoveries,
this was the one that was the most significant as it had the greatest
effect on future developments.
Studio portrait of Louis PasteurInstitut Pasteur
After the hospital opened
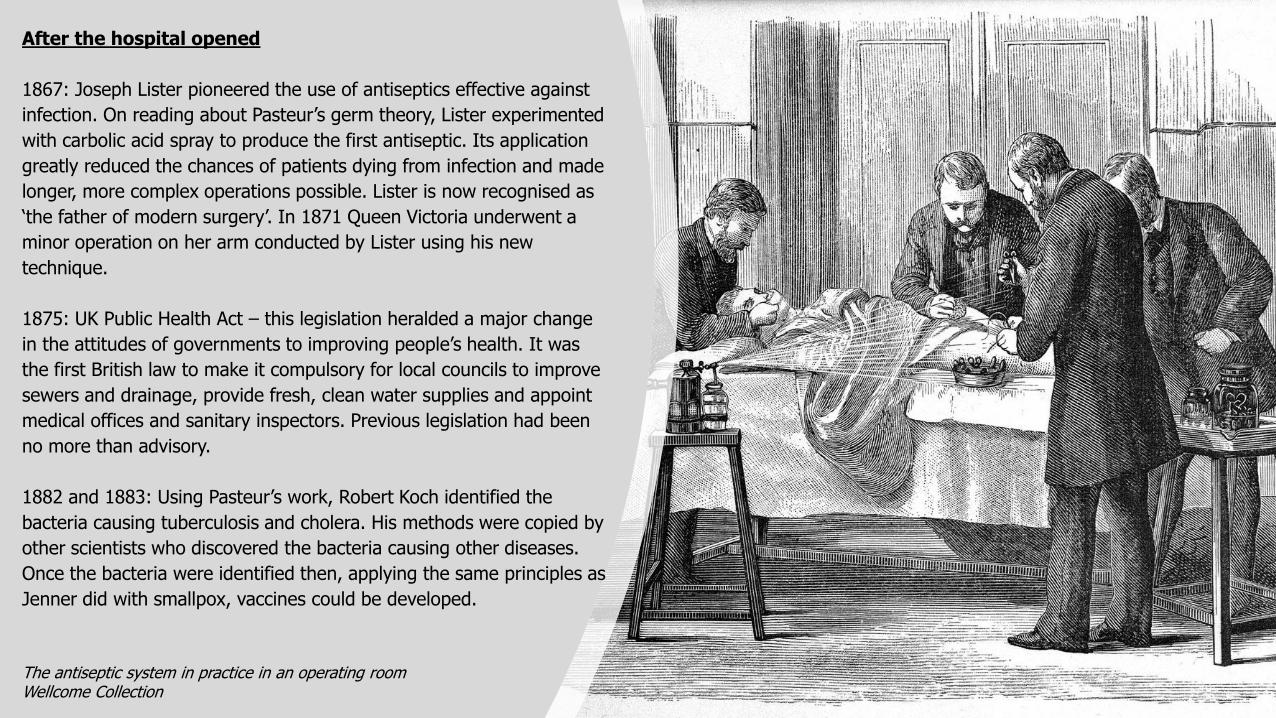
1867: Joseph Lister pioneered the use of antiseptics effective against
infection. On reading about Pasteur’s germ theory, Lister experimented
with carbolic acid spray to produce the first antiseptic. Its application
greatly reduced the chances of patients dying from infection and made
longer, more complex operations possible. Lister is now recognised as
‘the father of modern surgery’. In 1871 Queen Victoria underwent a
minor operation on her arm conducted by Lister using his new
technique.
1875: UK Public Health Act – this legislation heralded a major change
in the attitudes of governments to improving people’s health. It was
the first British law to make it compulsory for local councils to improve
sewers and drainage, provide fresh, clean water supplies and appoint
medical offices and sanitary inspectors. Previous legislation had been
no more than advisory.
1882 and 1883: Using Pasteur’s work, Robert Koch identified the
bacteria causing tuberculosis and cholera. His methods were copied by
other scientists who discovered the bacteria causing other diseases.
Once the bacteria were identified then, applying the same principles as
Jenner did with smallpox, vaccines could be developed.
The antiseptic system in practice in an operating roomWellcome Collection
This then was the background and context within which the Royal
Victoria Hospital and Army Medical School opened and operated, from
the spring of 1863.
In addition, medical publications such as The Lancet and Provincial
Medical and Surgical Journal (later the British Medical Journal), and
upon which professionals are so reliant, had been in existence since
the first half of the nineteenth century. However, for all that,
information technology and dissemination of new learning in late
nineteenth century Britain and Europe bore little resemblance to what
we experience and benefit from today. Whilst telegraph services
connected Britain to most of the empire for the whole of the period
under review, a telephone system was not operational until c.1900. In
short, the easy exchange of knowledge was problematic in Victorian
Britain. News of progress made by medical scientists in Europe or
especially in India (as with cholera) would have been slow to reach
Netley.
The great telegraphing room at the new offices of the Electric and International Telegraph Company, Bell Alley, Moorgate Street, LondonThe Illustrated London News, 31 December 1859.
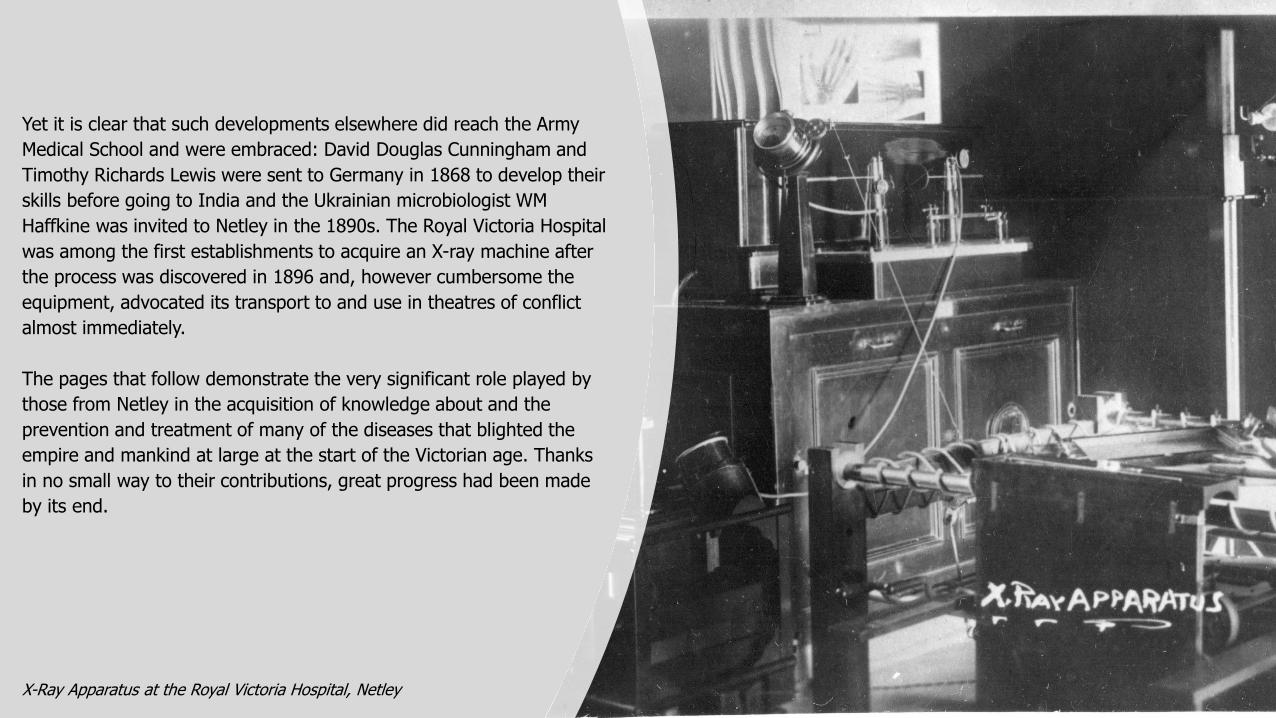
Yet it is clear that such developments elsewhere did reach the Army
Medical School and were embraced: David Douglas Cunningham and
Timothy Richards Lewis were sent to Germany in 1868 to develop their
skills before going to India and the Ukrainian microbiologist WM
Haffkine was invited to Netley in the 1890s. The Royal Victoria Hospital
was among the first establishments to acquire an X-ray machine after
the process was discovered in 1896 and, however cumbersome the
equipment, advocated its transport to and use in theatres of conflict
almost immediately.
The pages that follow demonstrate the very significant role played by
those from Netley in the acquisition of knowledge about and the
prevention and treatment of many of the diseases that blighted the
empire and mankind at large at the start of the Victorian age. Thanks
in no small way to their contributions, great progress had been made
by its end.
X-Ray Apparatus at the Royal Victoria Hospital, Netley
Cholera
Return to Contents
There were many infectious diseases prevalent in the 19th century. Of
these, cholera epitomises the impacts they all had in Great Britain and
parts of the Empire. It also shows the piecemeal and sometimes
confused efforts to analyse the cause and combat the effects of such
diseases.
In 1854, the year before the Royal Victoria Hospital was
commissioned, London suffered its fourth major cholera outbreak in
just over thirty years. The general view at the time was that the
disease was caused by poisonous vapours. These were thought to
come from the foul smelling air in areas with poor sanitation. This was
known as miasma theory. It suggested that diseases were not passed
from person to tperson, but would affect individuals in the area where
these foul smells were to be found. This was thought to explain why
diseases like cholera were epidemic in the 'undrained, filthy and
stinking areas' inhabited by the poor.
An 1831 colour lithograph by Robert Seymour depicts cholera as a robed, skeletal creature emanating a deadly black cloud.US National Library of Medicine photographic archive.
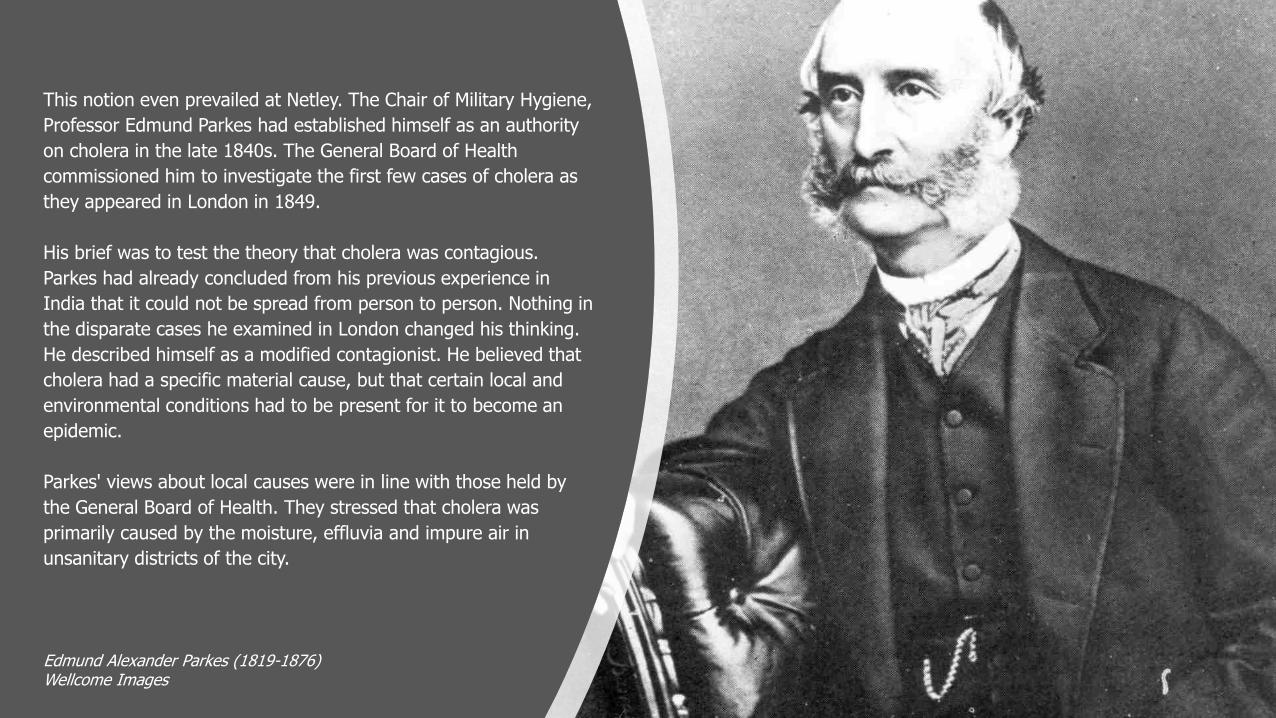
This notion even prevailed at Netley. The Chair of Military Hygiene,
Professor Edmund Parkes had established himself as an authority
on cholera in the late 1840s. The General Board of Health
commissioned him to investigate the first few cases of cholera as
they appeared in London in 1849.
His brief was to test the theory that cholera was contagious.
Parkes had already concluded from his previous experience in
India that it could not be spread from person to person. Nothing in
the disparate cases he examined in London changed his thinking.
He described himself as a modified contagionist. He believed that
cholera had a specific material cause, but that certain local and
environmental conditions had to be present for it to become an
epidemic.
Parkes' views about local causes were in line with those held by
the General Board of Health. They stressed that cholera was
primarily caused by the moisture, effluvia and impure air in
unsanitary districts of the city.
Edmund Alexander Parkes (1819-1876)Wellcome Images
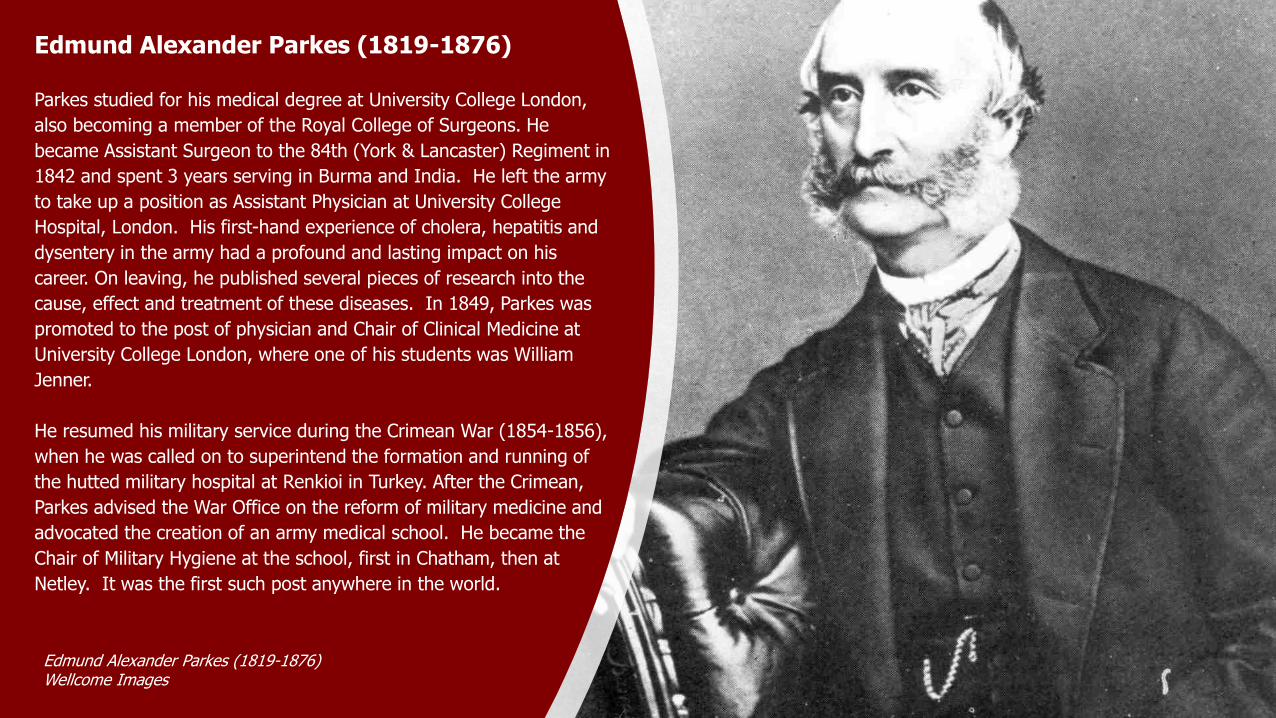
Edmund Alexander Parkes (1819-1876)
Parkes studied for his medical degree at University College London,
also becoming a member of the Royal College of Surgeons. He
became Assistant Surgeon to the 84th (York & Lancaster) Regiment in
1842 and spent 3 years serving in Burma and India. He left the army
to take up a position as Assistant Physician at University College
Hospital, London. His first-hand experience of cholera, hepatitis and
dysentery in the army had a profound and lasting impact on his
career. On leaving, he published several pieces of research into the
cause, effect and treatment of these diseases. In 1849, Parkes was
promoted to the post of physician and Chair of Clinical Medicine at
University College London, where one of his students was William
Jenner.
He resumed his military service during the Crimean War (1854-1856),
when he was called on to superintend the formation and running of
the hutted military hospital at Renkioi in Turkey. After the Crimean,
Parkes advised the War Office on the reform of military medicine and
advocated the creation of an army medical school. He became the
Chair of Military Hygiene at the school, first in Chatham, then at
Netley. It was the first such post anywhere in the world.
Edmund Alexander Parkes (1819-1876)Wellcome Images
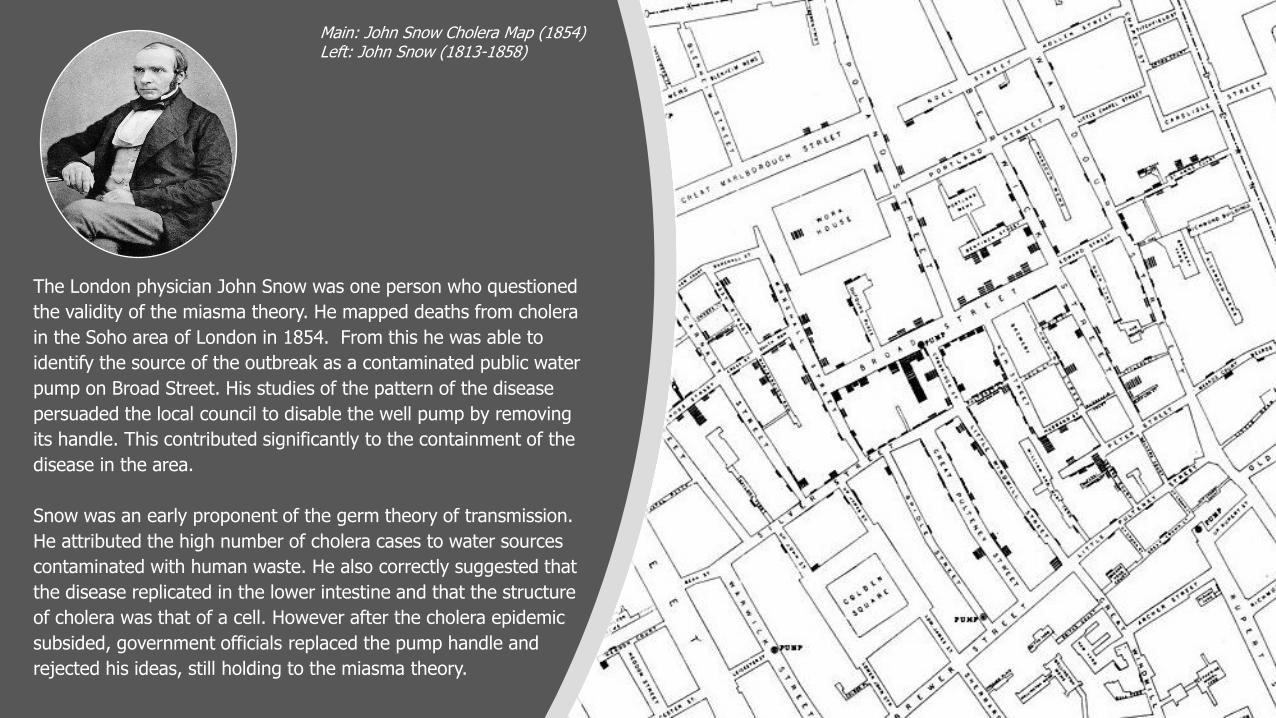
The London physician John Snow was one person who questioned
the validity of the miasma theory. He mapped deaths from cholera
in the Soho area of London in 1854. From this he was able to
identify the source of the outbreak as a contaminated public water
pump on Broad Street. His studies of the pattern of the disease
persuaded the local council to disable the well pump by removing
its handle. This contributed significantly to the containment of the
disease in the area.
Snow was an early proponent of the germ theory of transmission.
He attributed the high number of cholera cases to water sources
contaminated with human waste. He also correctly suggested that
the disease replicated in the lower intestine and that the structure
of cholera was that of a cell. However after the cholera epidemic
subsided, government officials replaced the pump handle and
rejected his ideas, still holding to the miasma theory.
Main: John Snow Cholera Map (1854)Left: John Snow (1813-1858)
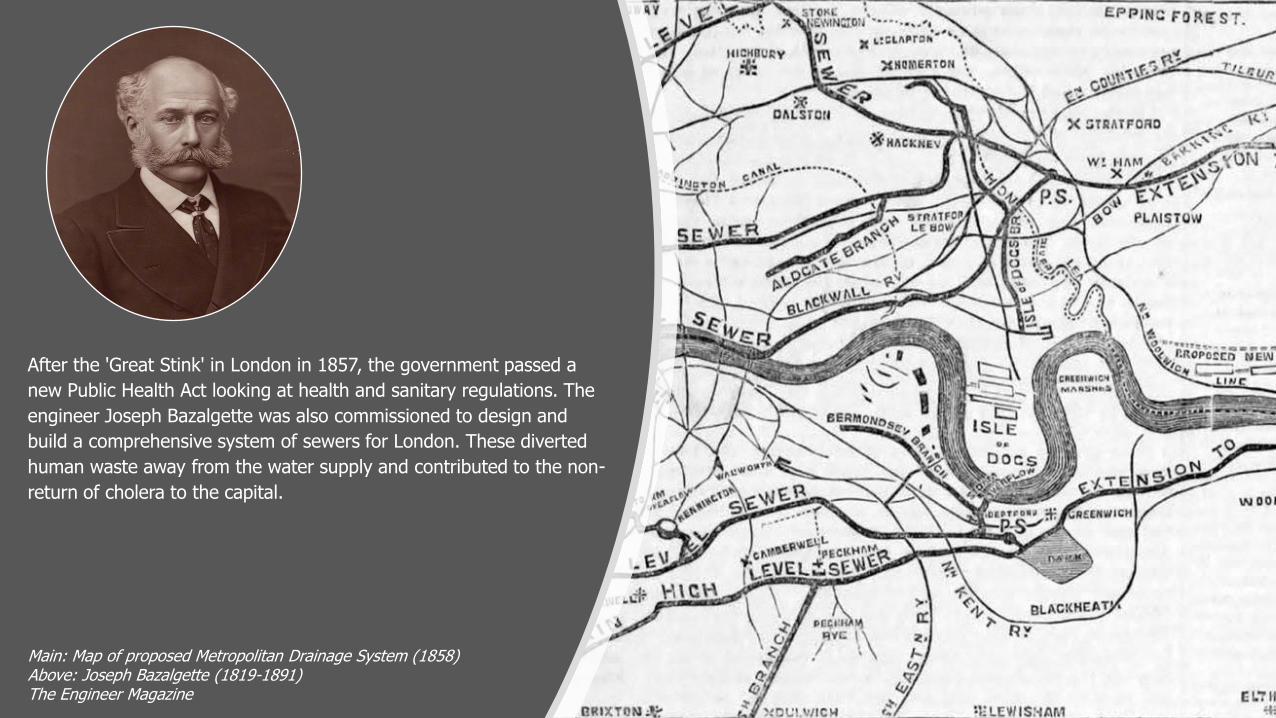
After the 'Great Stink' in London in 1857, the government passed a
new Public Health Act looking at health and sanitary regulations. The
engineer Joseph Bazalgette was also commissioned to design and
build a comprehensive system of sewers for London. These diverted
human waste away from the water supply and contributed to the non-
return of cholera to the capital.
Main: Map of proposed Metropolitan Drainage System (1858)Above: Joseph Bazalgette (1819-1891)The Engineer Magazine
Somewhat surprisingly, the links between cholera and sewage-
contaminated water do not seem to have been shared, or fully
grasped, across the wider British Empire.
The British Army in India had suffered considerably from a cholera
outbreak in 1817. More widely in India, epidemics in the 1830s, 1840s
and 1860s are thought to have killed anywhere between 10-15
million. These epidemics caused popular unrest in the country,
accentuating social conflict. Cholera was generally a disease of the
rural poor, but there were greater incidences at times of Hindu
pilgrimages and significant troop movements. The 1867 epidemic, for
example, was centred on the religious fair in Hardwar and killed more
than 100,000 people.
Even before the Hardwar outbreak, pressure was mounting on the
British to act to prevent cholera spreading from India to Europe. The
International Sanitary Conference met at Constantinople in 1866.
They demanded that the government in India take further measures
to control the disease on the sub-continent. Part of the British
response to this situation was to initiate a scientific study of the
causes of cholera. This was to be carried out under the direction of
James McNabb Cuningham, Sanitary Commissioner for the Bengal
Medical Service. Cuningham was a capable administrator and
pushed for improved sanitation across India. However he
doubted the value of bacteriological research.
James McNabb Cuningham (1829-1905) Wellcome Images
It was clear to the professors at Netley that no-one working in India
had the specialist skills needed to perform a study using microscopic
and botanical research. They therefore proposed that the two most
able doctors from the Netley 1868 cohorts be trained to undertake the
enquiry.
The top candidate from the Indian Medical Service exams was
Scotsman David Douglas Cunningham. Timothy Richards Lewis, a
Welsh doctor, obtained the highest mark in the Army Medical
Department exams. At the instigation of Professor Parkes,
Cunningham and Lewis travelled first to Germany. There they
received instruction from noted botanists looking at fungi as a
possible cause of the spread of disease.
David Douglas Cunningham (1843-1914)
David Douglas Cunningham obtained his medical degree
from Edinburgh in 1867. He passed the entry exam for the
Indian Medical Services in April 1868 and was sent to Netley
for the summer session. He completed the four month
course in military medicine, graduating top of his class. On
leaving Netley, Cunningham, along with fellow graduate
Timothy Richards Lewis, was posted to India to carry out
an enquiry into the causes of cholera.
David Douglas Cunningham (1843-1914)The Royal Society

Timothy Richards Lewis (1841-1886)The Royal Society
Timothy Richards Lewis (1841-1886)
Lewis was born in Wales and became a chemist and dispenser before
qualifying in medicine from the university of Aberdeen in 1867. The
following year he went to the Army Medical School at Netley,
qualifying top of his class.
He worked in India on several aspects of tropical medicine, including
cholera, leprosy, trypanosoma, and fungal infections. In 1883 Lewis
returned to Netley as Assistant Professor of Pathology, where he
introduced practical bacteriology to the curriculum.
Douglas David Cunningham and Timothy Richards Lewis arrived in
India in January 1869 to be supervised in their work by James
Cuningham. This is perhaps at the root of the difficulties they faced.
Although recruited by Parkes at Netley, they were under the direction
of the Sanitary Commission. Between them, Cunningham and Lewis
carried out considerable microscopic work, and investigated a vast
range of environmental and physical factors. However they did not
draw any conclusive, scientific answers for the causes of the
outbreaks of cholera. In fact, their research really served only to
validate British sanitary policy in India.
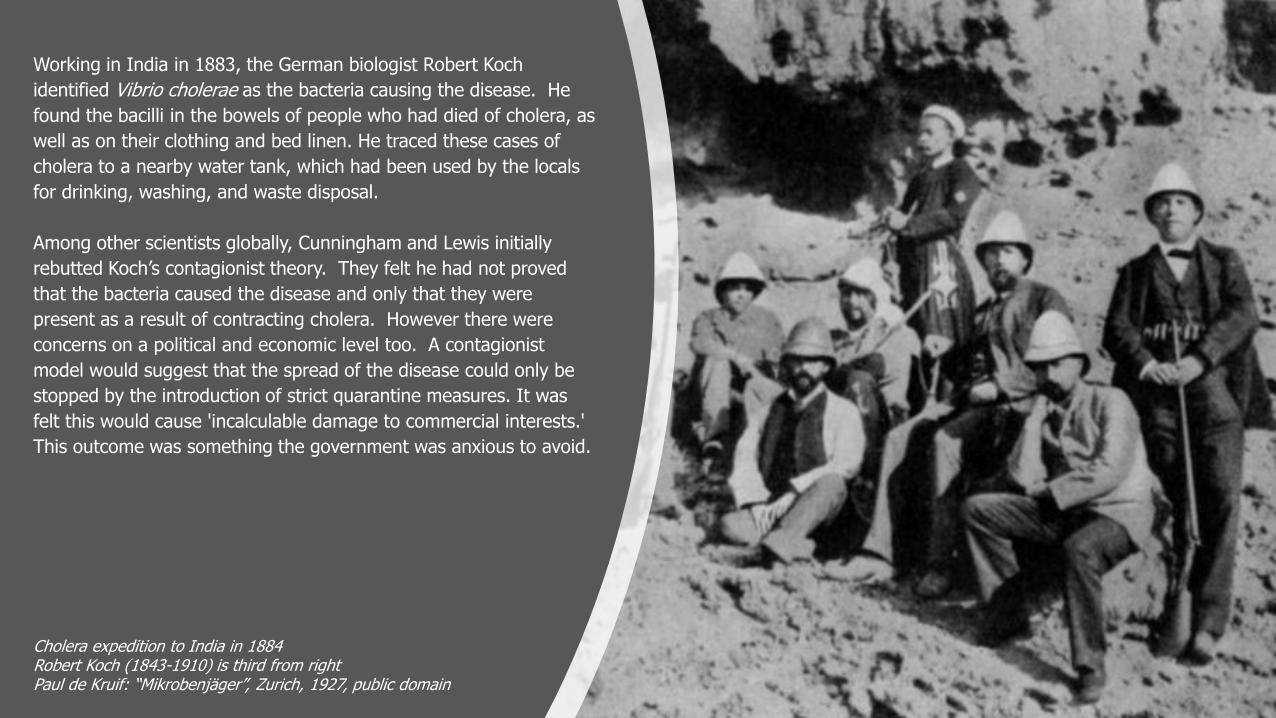
Working in India in 1883, the German biologist Robert Koch
identified Vibrio cholerae as the bacteria causing the disease. He
found the bacilli in the bowels of people who had died of cholera, as
well as on their clothing and bed linen. He traced these cases of
cholera to a nearby water tank, which had been used by the locals
for drinking, washing, and waste disposal.
Among other scientists globally, Cunningham and Lewis initially
rebutted Koch’s contagionist theory. They felt he had not proved
that the bacteria caused the disease and only that they were
present as a result of contracting cholera. However there were
concerns on a political and economic level too. A contagionist
model would suggest that the spread of the disease could only be
stopped by the introduction of strict quarantine measures. It was
felt this would cause 'incalculable damage to commercial interests.'
This outcome was something the government was anxious to avoid.
Cholera expedition to India in 1884Robert Koch (1843-1910) is third from rightPaul de Kruif: “Mikrobenjäger”, Zurich, 1927, public domain
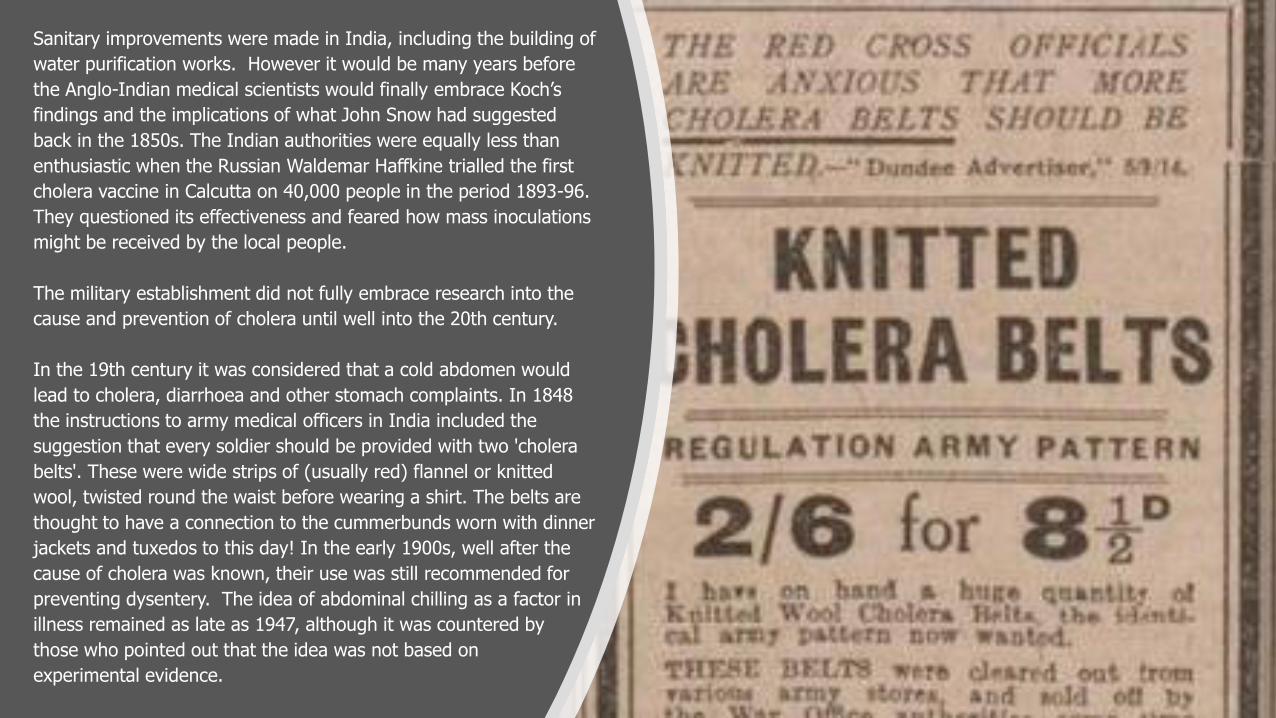
Sanitary improvements were made in India, including the building of
water purification works. However it would be many years before
the Anglo-Indian medical scientists would finally embrace Koch’s
findings and the implications of what John Snow had suggested
back in the 1850s. The Indian authorities were equally less than
enthusiastic when the Russian Waldemar Haffkine trialled the first
cholera vaccine in Calcutta on 40,000 people in the period 1893-96.
They questioned its effectiveness and feared how mass inoculations
might be received by the local people.
The military establishment did not fully embrace research into the
cause and prevention of cholera until well into the 20th century.
In the 19th century it was considered that a cold abdomen would
lead to cholera, diarrhoea and other stomach complaints. In 1848
the instructions to army medical officers in India included the
suggestion that every soldier should be provided with two 'cholera
belts'. These were wide strips of (usually red) flannel or knitted
wool, twisted round the waist before wearing a shirt. The belts are
thought to have a connection to the cummerbunds worn with dinner
jackets and tuxedos to this day! In the early 1900s, well after the
cause of cholera was known, their use was still recommended for
preventing dysentery. The idea of abdominal chilling as a factor in
illness remained as late as 1947, although it was countered by
those who pointed out that the idea was not based on
experimental evidence.
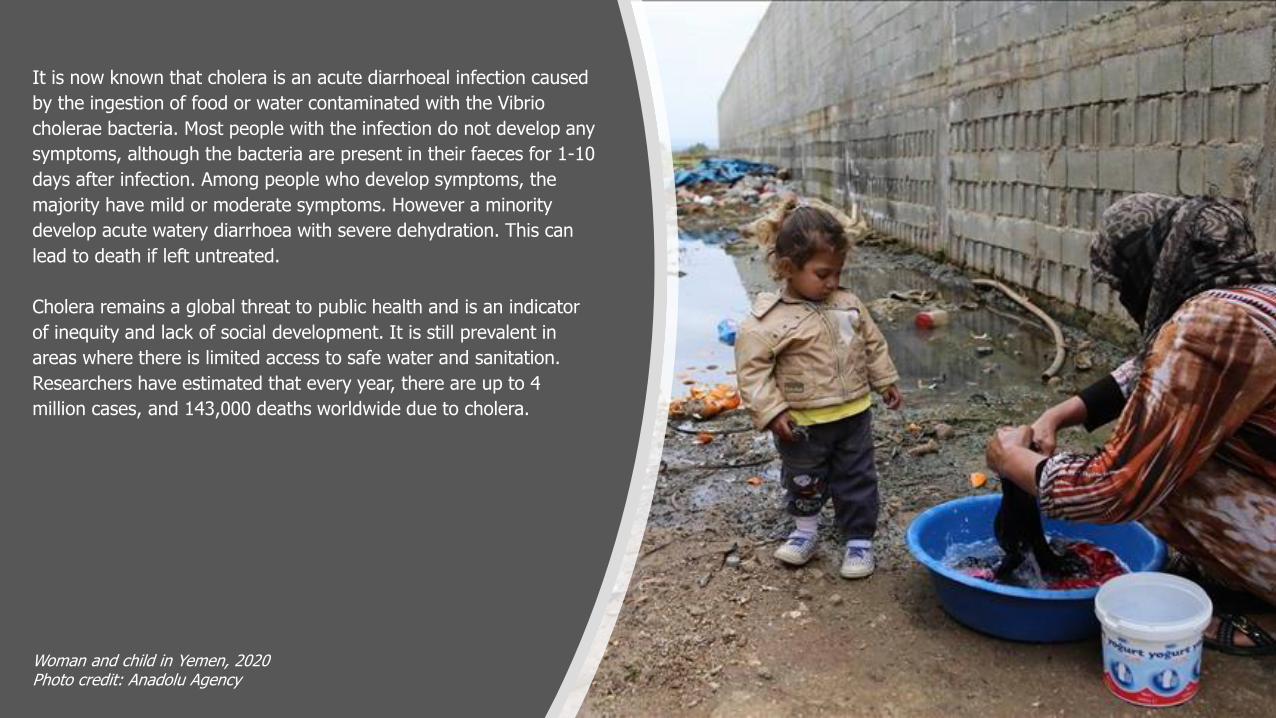
It is now known that cholera is an acute diarrhoeal infection caused
by the ingestion of food or water contaminated with the Vibrio
cholerae bacteria. Most people with the infection do not develop any
symptoms, although the bacteria are present in their faeces for 1-10
days after infection. Among people who develop symptoms, the
majority have mild or moderate symptoms. However a minority
develop acute watery diarrhoea with severe dehydration. This can
lead to death if left untreated.
Cholera remains a global threat to public health and is an indicator
of inequity and lack of social development. It is still prevalent in
areas where there is limited access to safe water and sanitation.
Researchers have estimated that every year, there are up to 4
million cases, and 143,000 deaths worldwide due to cholera.
Woman and child in Yemen, 2020Photo credit: Anadolu Agency
Malaria
Return to Contents
The term malaria dates to the mid-18th century, where it comes
from the Italian mala aria, meaning ‘bad air’. It was originally used
to describe the unwholesome atmosphere in marshlands, to which
the disease was attributed.
The idea that 'bad air' or 'marsh miasma' caused malarial infections
lingered as a misconception amongst scientists until the end of the
19th century. It persisted even as more scientific explanations
were established for the causes of other infectious diseases.
An insight into the impact of malaria on the British Army and other
forces can be gained from Professor William Maclean’s lecture
notes. These were published in 1886 in his book, Diseases of
Tropical Climates.
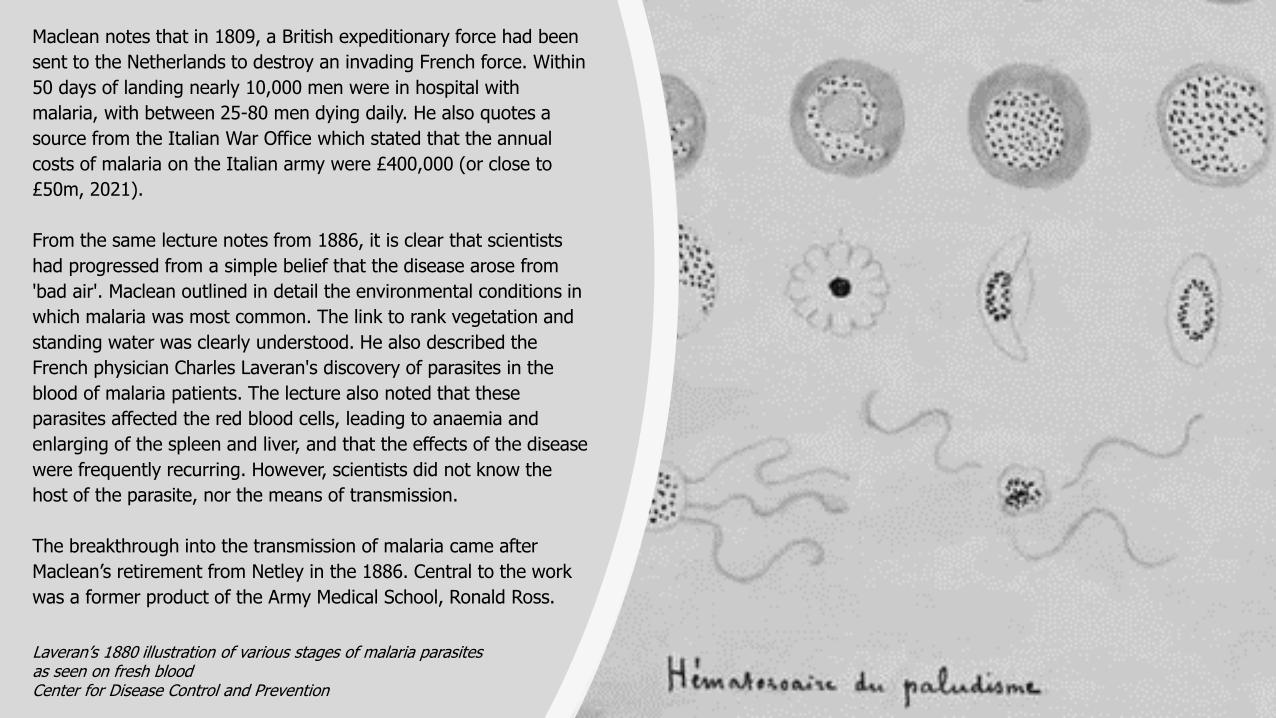
Maclean notes that in 1809, a British expeditionary force had been
sent to the Netherlands to destroy an invading French force. Within
50 days of landing nearly 10,000 men were in hospital with
malaria, with between 25-80 men dying daily. He also quotes a
source from the Italian War Office which stated that the annual
costs of malaria on the Italian army were £400,000 (or close to
£50m, 2021).
Surgeon-Major William Campbell Maclean (1811-1898)
William Campbell Maclean (1811-1898)
William Maclean was born in Ayr in 1811. He went to Edinburgh
Medical School, then at the height of its fame as the most
important in the world. He joined the Madras Army in 1838 and
worked exclusively in India as a medical officer. He held the post of
Residency Surgeon at the Court of Hyderabad from 1844-1845.
Here he organised a medical school where Indian people could be
instructed in Western medical science in their own languages.
In 1860, Maclean accepted the post of Professor of Military
Medicine at the new Army Medical School at Fort Pitt. He moved
with the school to Netley when the Royal Victoria Hospital opened
in 1863 and remained there until his retirement in 1886.
He was the army authority on malaria, enteric (typhoid) fever,
dengue fever, yellow fever, dysentery and cholera. He also
researched heart disease amongst soldiers and made
recommendations to redistribute the equipment they carried to
improve respiration and circulation.
Surgeon-Major William Campbell Maclean (1811-1898)
Maclean notes that in 1809, a British expeditionary force had been
sent to the Netherlands to destroy an invading French force. Within
50 days of landing nearly 10,000 men were in hospital with
malaria, with between 25-80 men dying daily. He also quotes a
source from the Italian War Office which stated that the annual
costs of malaria on the Italian army were £400,000 (or close to
£50m, 2021).
From the same lecture notes from 1886, it is clear that scientists
had progressed from a simple belief that the disease arose from
'bad air'. Maclean outlined in detail the environmental conditions in
which malaria was most common. The link to rank vegetation and
standing water was clearly understood. He also described the
French physician Charles Laveran's discovery of parasites in the
blood of malaria patients. The lecture also noted that these
parasites affected the red blood cells, leading to anaemia and
enlarging of the spleen and liver, and that the effects of the disease
were frequently recurring. However, scientists did not know the
host of the parasite, nor the means of transmission.
The breakthrough into the transmission of malaria came after
Maclean’s retirement from Netley in the 1886. Central to the work
was a former product of the Army Medical School, Ronald Ross.
Laveran’s 1880 illustration of various stages of malaria parasites as seen on fresh blood Center for Disease Control and Prevention
During his time in India, Ross took an increasing interest Malaria. It
was the cause of many of the fevers which he deemed to be his
biggest problem. About one third of the 300,000 men in the army
in India were admitted to hospital with malaria each year.
Ross knew of the French physician Charles Laveran’s 1880
discovery of malarial parasites in the blood. He carried out his own
microscopic research, but failed to find the parasites, which caused
him to question the whole theory.
On leave back in England in 1894, Ross was directed to physician
Patrick Manson, who demonstrated the parasites in specimens of
blood derived from a hospital patient. Manson had already
identified mosquitoes as important stages in the lifecycle of
another parasitic tropical disease. He raised with Ross the
possibility that mosquitoes might carry malaria.
Ronald Ross (1857-1932)Liverpool School of Tropical Medicine
Ronald Ross (1857-1932)
Ronald Ross completed his medical degree at St Bartholomew’s
Hospital Medical School. He graduated from Netley in 1880 and
entered the Madras Medical Service in 1881. He is best known for
his work on malaria, but also researched kālā āzār (now known as
Leishmaniasis) and dysentery.
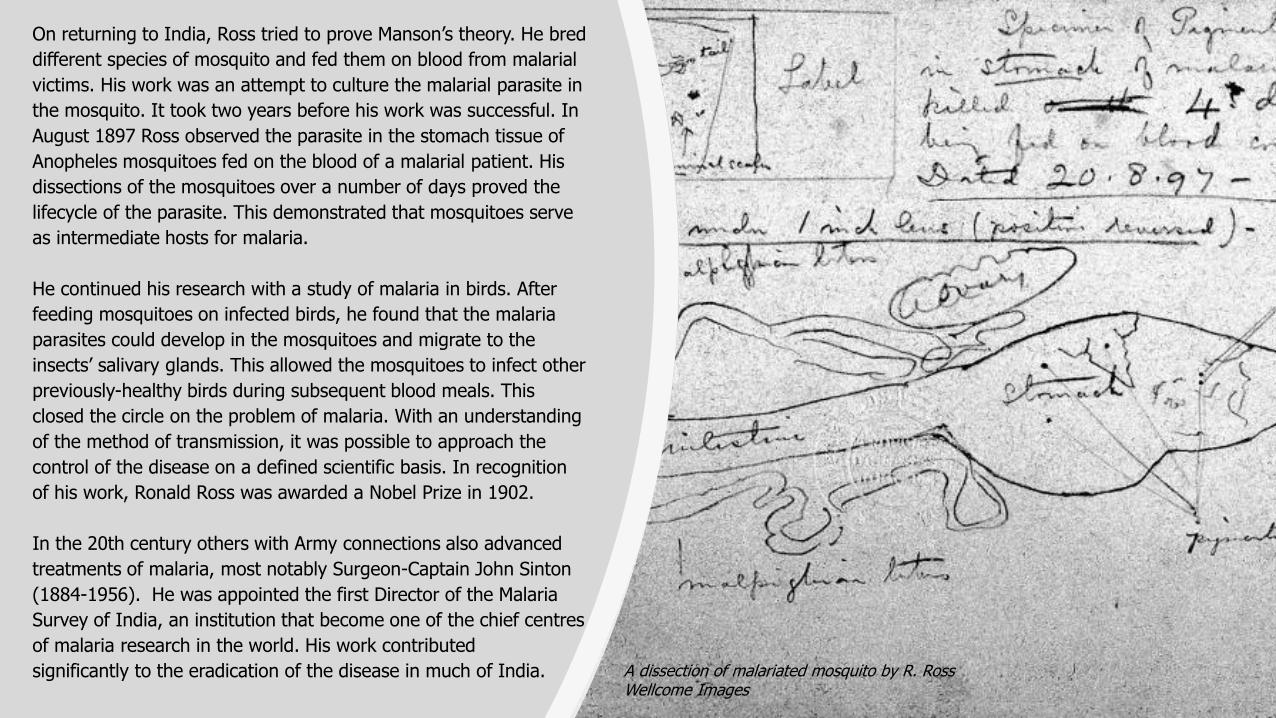
On returning to India, Ross tried to prove Manson’s theory. He bred
different species of mosquito and fed them on blood from malarial
victims. His work was an attempt to culture the malarial parasite in
the mosquito. It took two years before his work was successful. In
August 1897 Ross observed the parasite in the stomach tissue of
Anopheles mosquitoes fed on the blood of a malarial patient. His
dissections of the mosquitoes over a number of days proved the
lifecycle of the parasite. This demonstrated that mosquitoes serve
as intermediate hosts for malaria.
He continued his research with a study of malaria in birds. After
feeding mosquitoes on infected birds, he found that the malaria
parasites could develop in the mosquitoes and migrate to the
insects’ salivary glands. This allowed the mosquitoes to infect other
previously-healthy birds during subsequent blood meals. This
closed the circle on the problem of malaria. With an understanding
of the method of transmission, it was possible to approach the
control of the disease on a defined scientific basis. In recognition
of his work, Ronald Ross was awarded a Nobel Prize in 1902.
In the 20th century others with Army connections also advanced
treatments of malaria, most notably Surgeon-Captain John Sinton
(1884-1956). He was appointed the first Director of the Malaria
Survey of India, an institution that become one of the chief centres
of malaria research in the world. His work contributed
significantly to the eradication of the disease in much of India. A dissection of malariated mosquito by R. RossWellcome Images
Leishmaniasis
Return to Contents
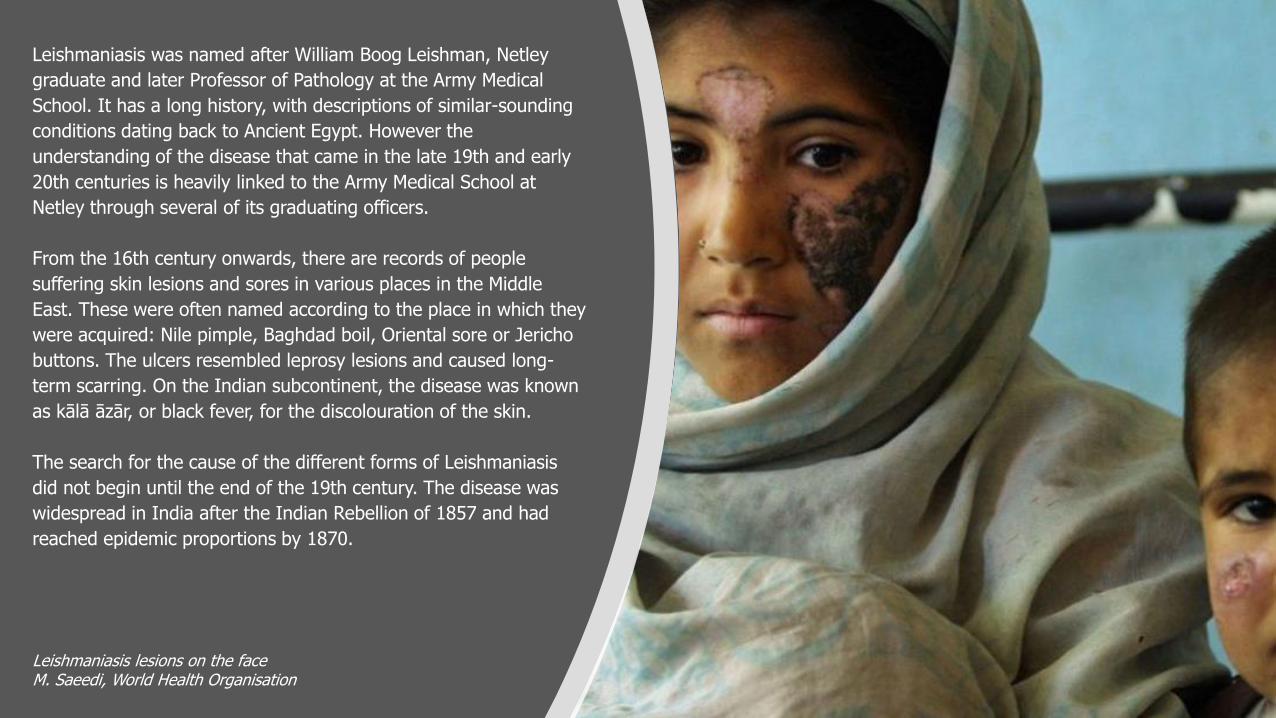
Leishmaniasis was named after William Boog Leishman, Netley
graduate and later Professor of Pathology at the Army Medical
School. It has a long history, with descriptions of similar-sounding
conditions dating back to Ancient Egypt. However the
understanding of the disease that came in the late 19th and early
20th centuries is heavily linked to the Army Medical School at
Netley through several of its graduating officers.
From the 16th century onwards, there are records of people
suffering skin lesions and sores in various places in the Middle
East. These were often named according to the place in which they
were acquired: Nile pimple, Baghdad boil, Oriental sore or Jericho
buttons. The ulcers resembled leprosy lesions and caused long-
term scarring. On the Indian subcontinent, the disease was known
as kālā āzār, or black fever, for the discolouration of the skin.
The search for the cause of the different forms of Leishmaniasis
did not begin until the end of the 19th century. The disease was
widespread in India after the Indian Rebellion of 1857 and had
reached epidemic proportions by 1870.
Leishmaniasis lesions on the faceM. Saeedi, World Health Organisation
The search for the cause of the different forms of Leishmaniasis did
not begin until the end of the 19th century. The disease was
widespread in India after the Indian Rebellion of 1857 and had
reached epidemic proportions by 1870.
In 1885, David Douglas Cunningham, Netley graduate and now
Surgeon Major of the British Indian Army, published a paper noting
the presence of “peculiar parasitic organisms in the tissue of a
specimen of Delhi boil.” However he did not realise what they were
or make the connection with kālā āzār.
In 1898 Peter Borovsky, a Russian military surgeon in Tashkent,
conducted research into the cause of ‘Oriental sore’. He published the
first accurate description of the causative agent – the bite of a
phlebotomine sandfly. However because his results were published in
Russian in a journal with low circulation, they were not then
internationally acknowledged. Instead the story is picked up later in
1898 by another Netley graduate, Ronald Ross.
David Douglas Cunningham (1843-1914)The Royal Society
In September 1898 Ross was invited by a local medical officer to
work in southern Assam (north east India) to study an epidemic of
kālā āzār. He had recently identified mosquitoes as the means of
transmission of malaria. This may account for him incorrectly
reaching the conclusion that kālā āzār was a quinine-resistant form
of the disease. He believed that the kālā āzār parasite was
transmitted by a mosquito, which he referred to as
Anopheles Rossi.
In 1900 there came a breakthrough when William Boog Leishman
discovered ovoid bodies in smears taken post-mortem from the
spleen of a soldier who had died from emaciation and splenomegaly.
The following year he developed a method of staining blood smears
to identify and differentiate between white blood cells, malaria
parasites and other protozoan parasites, called trypanosomes. He
used this to suggest that the ovoid bodies were degenerate
trypanosomes. He theorised that the soldier’s illness (which he called
‘Dum Dum fever’ from the town near Calcutta where the soldier had
been stationed) was a form of trypanosomiasis. He published his
findings in May 1903.
Sir William Boog Leishman (1865-1926)Wellcome Images
William Boog Leishman (1865-1926)
William Boog Leishman was just 20 when he qualified in medicine
in Glasgow. He completed the course at Netley in 1867 and was
posted to India. Here he began the research into the causes of
kālā āzār, for which he is best known.
On leaving India, Leishman returned to Netley, where he worked
with Almroth Wright on typhoid vaccine. In 1900 Leishman was
appointed Assistant Professor of Pathology at the Army Medical
School. He developed a method of staining blood samples, which
is known as Leishman’s stains and is still used today.
Leishman became Chair of Pathology when the Army Medical
School moved to London in 1904. He continued Almroth Wright’s
work on an anti-typhoid vaccine, which resulted in the successful
protection of British troops during the First World War.
Sir William Boog Leishman (1865-1926)Wellcome Images
A matter of weeks later, Lieutenant-Colonel Charles Donovan, yet
another graduate of Netley and now professor of physiology at the
Madras Medical College, published a paper with very similar
findings. He reported that he had found parasitic bodies in samples
taken from native Indian subjects with remittent fever and
enlarged spleens. He identified these parasites as the causative
agent of kālā āzār.
Charles Donovan (1863-1951)Wellcome Images
Charles Donovan (1863-1951)
Charles Donovan was born in India in 1863, son of an Irish judge
working in the Indian Civil Service. He studied medicine at Trinity
College Dublin and received his MD degree in 1889 from the Royal
University of Ireland. He graduated from the Army Medical School
at Netley in 1891 and was commissioned as Captain in the Indian
Medical Service. In 1898 he was posted to the Madras Medical
College and Government General Hospital, where he became
Chair of the Physiology Department.
There was some controversy as to whom should be credited with the
discovery, and confusion over the correct identity of the parasite.
It was Ronald Ross who resolved the conflict and linked the two
discoveries. He identified that the ovoid bodies were in fact a new
parasite species, which he named Leishman-Donovan bodies. They
were later formally named Leishmania donovani, equally crediting the
two scientists.
Donovan’s continued work on the biology of Leishmania donovani
established him as the leading authority on kālā āzār. He and Ronald
Ross coined the term leishmaniasis to cover all conditions associated
with this and closely allied parasites.
Leishmania donovani in bone marrow cellCenters for Disease Control and Prevention's Public Health Image Library

Despite work to discover its cause over a century ago, this infection
has never been eradicated. There are three main forms of
leishmaniasis – visceral, cutaneous and mucocutaneous. Of these,
visceral leishmaniasis (still also known as kālā āzār) is the most
serious. Leishmaniasis is caused by parasites which are transmitted
by the bite of infected female phlebotomine sandflies. The disease
affects some of the poorest people on earth. It is associated with
malnutrition, population displacement, poor housing and a weak
immune system.
According to the World Health Organisation, visceral leishmaniasis
infects 300,000 people annually, causing 20,000 deaths. It is the
second largest cause of parasitic death after malaria. To this day, the
WHO strives to prevent and mitigate its impacts in its most prevalent
areas.
Chepsera Limaru watches over her son Pturu Limaruk who suffers from kala-azar at the Amudat hospital in Uganda.Lameck Ododo/DNDi
Brucellosis
Return to Contents
Brucellosis was named after David Bruce, Assistant Professor of
Pathology at the Army Medical School, Netley. It was the second
disease, after leishmaniasis, to be named after a doctor with
associations to the Royal Victoria Hospital. This account, however, starts
before the discovery attributed to Bruce. It is, like others a complex one
of controversies, misunderstandings and slowly acquired knowledge.
There was considerable confusion in the Victorian era over the cause
and diagnosis of various fever-based diseases. These were prevalent in
the Mediterranean, but hard to distinguish due to the similarities of
their symptoms. One such disease came to be known by a variety of
regional names, including Malta, Gibraltar and Cyprus fever. It was also
common in the Crimean War theatre of the mid 1850s, where it was
locally labelled Crimea fever. Key symptoms, along with the fever, were
joint and muscle pain, night sweats and gastric irritation. However in
some cases it could also cause neurological disorders, including
agitation and confusion.
One of the most noted sufferers of Crimea fever was Florence
Nightingale, who was diagnosed with the condition in May 1855. She
spent several weeks in hospital, at times delirious, critically ill and
unable even to feed herself. Florence took months to recover from
the initial illness and suffered from poor health for the rest of her life.
Sir David Bruce (1855–1931)London School of Hygiene & Tropical Medicine

Sir David Bruce (1855–1931)
Bruce graduated in medicine from the University of Edinburgh and
joined the Army Medical Service in 1883. After graduating from Netley,
he was posted to Malta, where he researched the causes of Malta
Fever. It later came to be known as Brucellosis in his honour.
From 1889 to 1894, David Bruce served as Assistant Professor of
Pathology at the Army Medical School at Netley, where he introduced a
course in bacteriology.
Bruce was later posted to South Africa, where he researched African
trypanosomiasis (sleeping sickness in humans and nagana in animals),
identifying the tsetse fly as the means of transmission. His discovery of
the organism causing nagana led to it being named Trypanosoma
brucei. He was rewarded with a knighthood in 1908.
During the First World War Bruce was Commandant of the Royal Army
Medical College. He chaired the War Office Trench Fever Investigation
Commission to help identify the cause and means of transmission of
trench fever.
Sir David Bruce (1855–1931)London School of Hygiene & Tropical Medicine
The first clinical description of the disease was made in 1861 by the
army surgeon Dr Jeffery Allen Marston, stationed in Malta. He defined
the disease as Mediterranean gastric remittent fever, noting that
symptoms would worsen over time (relapse), followed by a period of
improvement (remission). Although Marston did not know the cause
of the disease, he made a clear distinction between it and other
Mediterranean fevers. He reported his findings to the army medical
department in 1861, but the report was only published in 1863.
There were no further developments for more than twenty years. In
1884 David Bruce, a young graduate of the Army Medical School at
Netley, was posted to Malta. This island, being in a strategic position
in the Mediterranean, was an important naval base with 25,000
permanent British soldiers and sailors. It was also used as a
temporary station for British troops to acclimatise to the change in
climate on the way from England to India. Malta fever had a big
impact on the health of the British troops stationed there and the
government was concerned about the large number of reported
cases. Doctors were sent from Great Britain to Malta to find out the
cause of this disease.
Bruce carried out the post-mortem examination of a soldier who died
fifteen days after developing an acute case of Malta fever.
Examination of tissue from the spleen revealed the bacteria that
caused the infection. Bruce called it ‘micrococcus melitensis’.
Dr Giuseppe Caruana Scicluna was a Maltese analytical chemist, who
collaborated with Bruce. He prepared the agar plates used for the
spleen smears in his laboratory in the Public Health Department.
Later he succeeded in culturing the bacteria from spleen samples of
four British soldiers dying of Malta Fever. However Bruce never
properly acknowledged Caruana Scicluna’s contributions to this
important research.
From 1889 to 1894, David Bruce served as Assistant Professor of
Pathology at the Army Medical School at Netley. Having previously
studied bacteriology under the German microbiologist Robert Koch in
Berlin, Bruce instituted the first systematic course on the subject to be
given in any British medical school. In his early years at Netley, Bruce
seems to have inspired an interest in Malta fever in his students.
Surgeon Matthew Louis Hughes passed out of Netley at the head of
the list in 1890 and was awarded the Parkes Memorial Prize. In
December 1890, he was posted to Malta. He wrote a book about the
disease, ‘Mediterranean, Malta, or Undulant Fever’, which was
published in 1897. This gave a clear and detailed description of the
signs and symptoms of the disease, as well as epidemiological
information about its distribution.
Dr G Caruana Scicluna, the First Maltese MicrobiologistJournal of Medical Biography, 2000
Another significant advance in 1897 was made by Professors Almroth
Wright and David Semple at the Army Medical School at Netley. They
developed a blood test which could distinguish typhoid fever from
Malta fever through the presence of specific antibodies. This made it
possible to make a clinical diagnosis of Malta fever for the first time.
However, despite these achievements, the source of the bacteria
remained unknown. Impure water in the Grand Harbour of Valletta
was thought by many to be the breeding place of the fever, though
bad air and drains were also considered likely. A Maltese scientist with
no connection to the military, Dr Themistocles Zammit, was also
working on the problem. In 1902, he carried out a survey of cases of
Malta fever, compared them with typhoid fever and concluded that the
disease might be spread by insects.
The British Government formed the Mediterranean Fever Commission
(MFC) in 1904 to identify the source and mode of transmission of the
disease. The Royal Society named David Bruce chairman of the
commission. Other members included Dr Themistocles Zammit and a
close associate of Bruce’s from Netley, Major William Horrocks.
Horrocks had graduated from the Army Medical School in 1887 and by
1904 had returned as Assistant Professor of Military Hygiene.
Some of the members of the Mediterranean Fever CommissionThemistocles Zammit: top row, far leftDavid Bruce: front row, centreWellcome Images
Members of the MFC conducted surveys to establish the prevalence of
Malta fever and identify the extent of the problem. They also carried
out microbiological investigations, including the experimental
transmission of the disease to laboratory animals. For this they used
goats, which were readily available locally. In carrying out blood tests
on the goats prior to experimentation, Zammit discovered that many
of them carried the micrococcus melitensis bacteria in their blood.
Thousands of goats were then examined in Malta and it was found
that nearly half of them were infected, even apparently healthy
animals. Further tests showed that around 10% of them had the
bacteria in their urine and milk. This gave a method of transmission
of the disease to humans through ingesting the infected milk.
This finding explained the hitherto baffling fact as to why patients and
medical staff in the military and naval hospitals were more likely to
contract Malta fever while there. At the time, the Maltese distributed
milk directly from goats at the door, where they were freshly milked.
In 1906, the use of goats’ milk by the British Armed Services was
prohibited and case numbers dropped dramatically. Between 1900 and
1906 there had been a total of 3,631 cases, but by 1907 there were
only 21. Condensed, evaporated and sterilised milks were used
instead.
Goats at St George’s Bay Malta with St George’s Barracks in the backgroundMalta RMC/QA Archives photo album 1914-1918
David Bruce had discouraged the experiments on goats being carried
out by Zammit and cast doubt on his ability as a microbiologist.
Between them, Bruce and Horrocks played down Zammit’s role and
Bruce took steps to take credit to himself. As editor of the Journal of
the Royal Army Medical Corps, he published frequent articles in the
journal about Malta fever. These articles emphasised the role of the
RAMC members of the Commission, but omitted or played down the
work by Zammit and the naval officer, Shaw.
To a certain extent, Bruce succeeded in claiming credit for the
discovery of both the bacteria and its source. The disease was later
named brucellosis in his honour. However, people outside the RAMC
also recognised Zammit’s contribution. He achieved an international
reputation both as a chemist and later as an archaeologist.
Themistocles Zammit was knighted in 1930 in recognition of his role in
helping eliminate undulant fever from Malta.
Portrait of Dr. Themistocles Zammit (1864-1935)painted by Edward Caruana DingliCulture Malta
It is now known that brucellosis is a highly contagious zoonosis - a
disease that can be transmitted from animals to humans. It is caused
by the ingestion of unpasteurised milk or undercooked meat from
infected animals, or close contact with their secretions. The most
common symptoms of brucellosis are fever, sweats, back and joint
pain, loss of appetite and extreme tiredness. However in severe cases,
the central nervous system and lining of the heart may be affected.
Brucellosis can also trigger an autoimmune response in some people,
causing inflammatory conditions such as arthritis, spondylitis and
meningitis. One form of the disease manifests itself in various
neurological conditions, including confusion, agitation, depression and
behavioural changes.
Florence Nightingale struggled with a chronic form of brucellosis,
which caused her many and varied health problems into old age. She
suffered heart palpitations, fainting fits, weakness, nausea and severe
spinal and joint pain. She also experienced persistent neurological
effects of the disease. These included depression, insomnia and
nervousness. Some historians say that these account for her ‘gloomy,
agitated and obsessive personality’ during her later life.
Florence Nightingale (1820-1910)Wellcome Images
Dysentery
Return to Contents
A close medical companion of cholera, dysentery is a type of
gastroenteritis that results in diarrhoea with blood. Other symptoms
may include fever, abdominal pain, and mucus or blood in the
faeces. Dysentery can be caused by bacterial infection, viral infection
or parasitic worms. It is one of the symptoms of cholera and, just as
in the nineteenth century, treatments today are similar. The English
word dysentery comes from two Greek words meaning 'ill' or 'bad'
and ‘intestine’. Prior to the Victorian age, it was known as ‘the
Bloodie Flux’.
One commentator of that age wrote: “Of the diseases incident to
Europeans in tropical climates, there is perhaps none of more
importance, whether we consider the amount of mortality arising
from it, or the permanently impaired health produced by alteration
of structure in those who have laboured under it. In the army this is
even more marked than in civil life, for the soldier … suffers
repeated relapses until the disease terminates either in death or in
organic alterations of such a character as to render him permanently
unfit for military service.”
A Dysentery ward of the General Hospital at Port Said© IWM Art.IWM ART 2941
This is borne out by some statistics: typhus and dysentery decimated
Napoleon's Grande Armée in Russia, while more than 80,000 Union
soldiers died of dysentery during the American Civil War. Critically
from a British perspective, during the Crimean War many more
soldiers died from cholera and dysentery than battle wounds.
In a lecture to students at the Army Medical School, the Professor of
Military Medicine, William Campbell Maclean told them that in the
1830s, roughly one third of British soldiers serving in India could be
expected to suffer from the disease - a rate eleven times higher than
local soldiers! Maclean left his students in no doubt as to the ravage
and suffering this disease brought.
Fortunately, treatment methods by the 1880s had advanced from the
bloodletting, blistering and ingesting of lead salts and emetics
common during the age of the Napoleonic wars. Instead, doses of
varying amounts of ipecacuanha, sometimes in association with
quinine, were favoured and are reported to have been successful. In
what Maclean referred to as the sanitary age, focus then appears to
have concentrated on improved hygienic practices to prevent its
occurrence and effective methods of successful treatment to
remediate the patient.
Hospital in Sebastopol – Dr Durgan attending the wounded from a sketch by EA GoodallWellcome Images
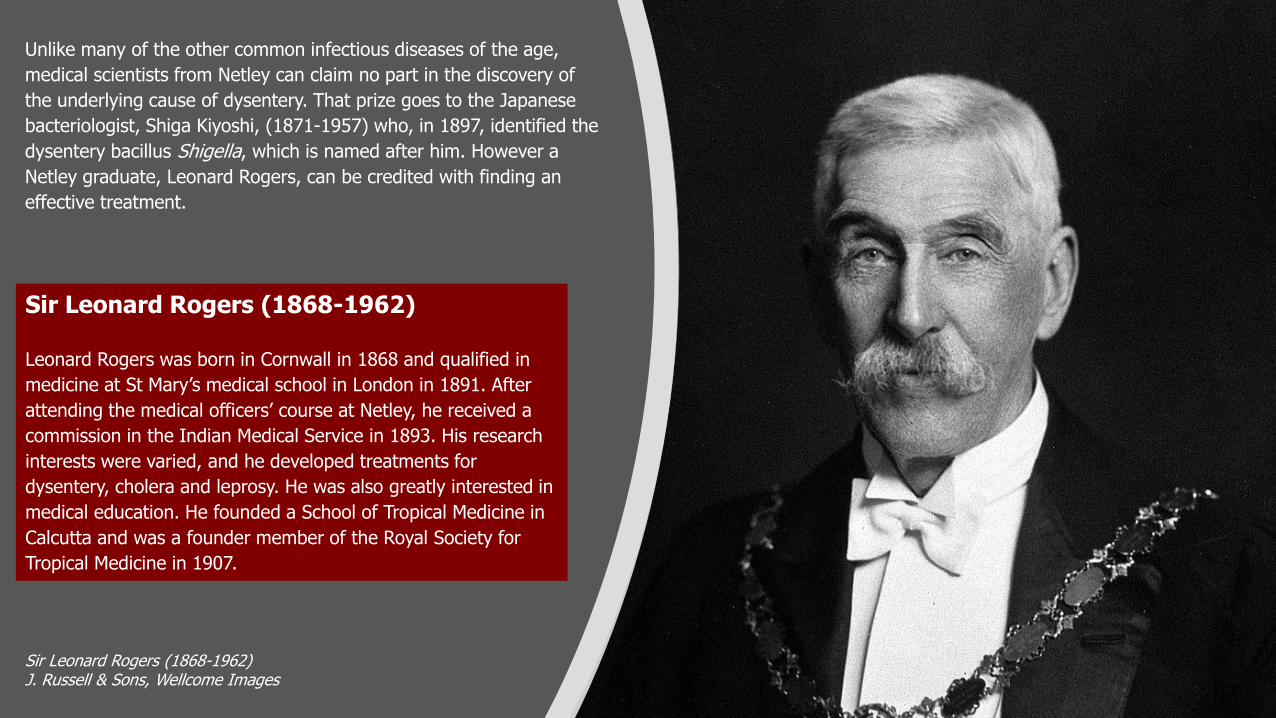
Unlike many of the other common infectious diseases of the age,
medical scientists from Netley can claim no part in the discovery of
the underlying cause of dysentery. That prize goes to the Japanese
bacteriologist, Shiga Kiyoshi, (1871-1957) who, in 1897, identified the
dysentery bacillus Shigella, which is named after him. However a
Netley graduate, Leonard Rogers, can be credited with finding an
effective treatment.
Sir Leonard Rogers (1868-1962)J. Russell & Sons, Wellcome Images
Sir Leonard Rogers (1868-1962)
Leonard Rogers was born in Cornwall in 1868 and qualified in
medicine at St Mary’s medical school in London in 1891. After
attending the medical officers’ course at Netley, he received a
commission in the Indian Medical Service in 1893. His research
interests were varied, and he developed treatments for
dysentery, cholera and leprosy. He was also greatly interested in
medical education. He founded a School of Tropical Medicine in
Calcutta and was a founder member of the Royal Society for
Tropical Medicine in 1907.
Posted to Calcutta in 1900, Rogers ultimately became Professor of
Pathology in the medical college. In fact, he spent much of his time in
the hospital wards. He differentiated between the symptoms of
bacillary dysentery (caused by the Shigella bacteria) and amoebic
dysentery (caused by a parasite called Entamoeba histolytica). In
1912, he developed a new treatment for the amoebic form, injecting
patients with emetine, a pure extract from the ipecacuanha root. Its
immediate success led to it becoming the accepted treatment.
Ronald Ross (Netley graduate whose work on Malaria is discussed
elsewhere in this collection) gave a lecture to the Royal Society of
Medicine in 1915. He made no mention of Shiga Kiyoshi's research
into the bacterial form of dysentery but did acknowledge Rogers'
work. Ross remarked: “as an immediately applicable routine
treatment, the hypodermic injection of emetine has certainly become
a great boon to humanity, for which we owe a debt to Sir Leonard
Rogers which can never be repaid.”
Rogers was recognised by the Royal Society for Tropical Medicine in
1938: “by his insistence on the value of emetine in amoebic dysentery
and by his introduction of the soluble salts of emetine, he very greatly
stimulated the use of this valuable drug in the treatment of amoebic
dysentery in all parts of the tropics.”
Entamoeba histolytica in the trophozoite stageJ. Craig Venter Institute

Typhoid Enteric Fever
Return to Contents
In a lecture to his students at Netley, the Professor of Military
Medicine William Maclean quoted his colleague Professor Aitken:
“enteric fever is the most treacherous of all diseases”.
Had he been alive just twenty years later and informed about ’Typhoid
Mary’, Maclean would probably have been unsurprised to learn how
such a ‘super-spreader’ could have existed, undetected, in the
community for so long. Mary Mallon’s story is synonymous with
typhoid but not one that can be told in the context of the Royal
Victoria Hospital and the Army Medical School.
Maclean was essentially referring to what we now know as typhoid,
but which was only specifically identified and labelled in the 1880s.
Before then there had been outbreaks of typhoid in England and it
had ravaged British troops serving overseas. This was particularly
notable during the Crimea War where it was prevalent with cholera
and dysentery.
Surgeon-Major William Campbell Maclean (1811-1898)
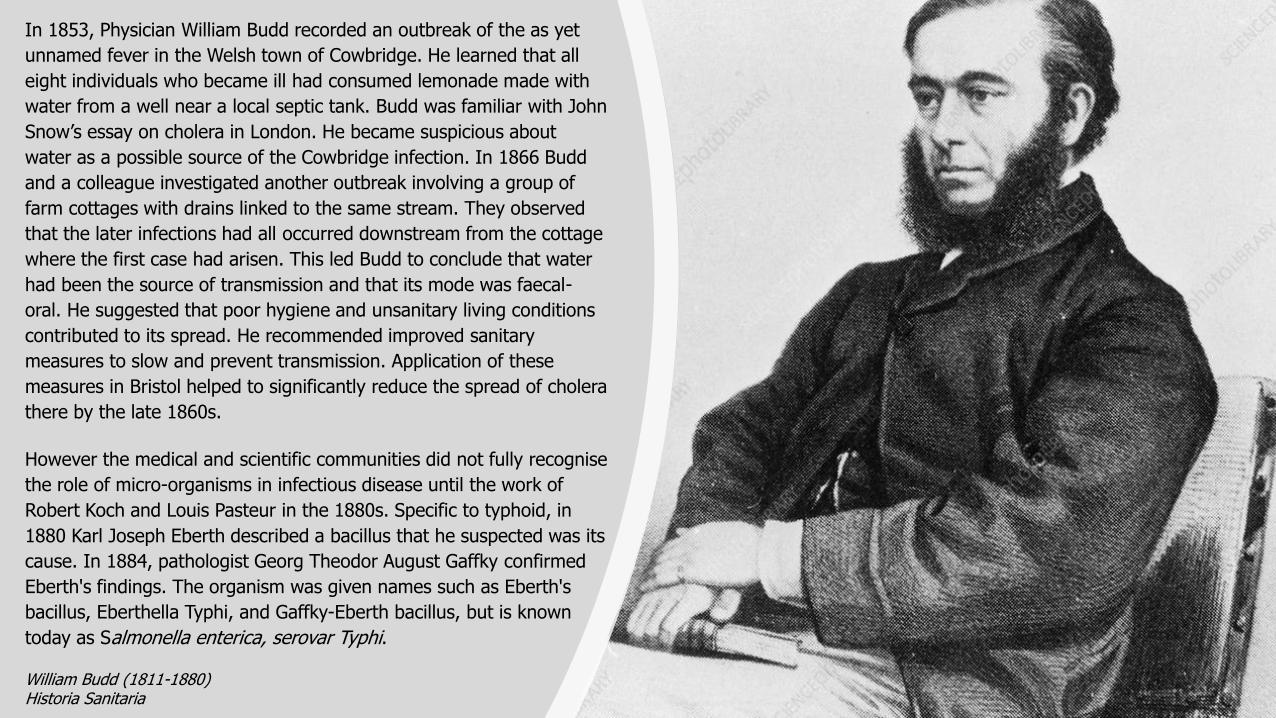
In 1853, Physician William Budd recorded an outbreak of the as yet
unnamed fever in the Welsh town of Cowbridge. He learned that all
eight individuals who became ill had consumed lemonade made with
water from a well near a local septic tank. Budd was familiar with John
Snow’s essay on cholera in London. He became suspicious about
water as a possible source of the Cowbridge infection. In 1866 Budd
and a colleague investigated another outbreak involving a group of
farm cottages with drains linked to the same stream. They observed
that the later infections had all occurred downstream from the cottage
where the first case had arisen. This led Budd to conclude that water
had been the source of transmission and that its mode was faecal-
oral. He suggested that poor hygiene and unsanitary living conditions
contributed to its spread. He recommended improved sanitary
measures to slow and prevent transmission. Application of these
measures in Bristol helped to significantly reduce the spread of cholera
there by the late 1860s.
However the medical and scientific communities did not fully recognise
the role of micro-organisms in infectious disease until the work of
Robert Koch and Louis Pasteur in the 1880s. Specific to typhoid, in
1880 Karl Joseph Eberth described a bacillus that he suspected was its
cause. In 1884, pathologist Georg Theodor August Gaffky confirmed
Eberth's findings. The organism was given names such as Eberth's
bacillus, Eberthella Typhi, and Gaffky-Eberth bacillus, but is known
today as Salmonella enterica, serovar Typhi.
William Budd (1811-1880)Historia Sanitaria
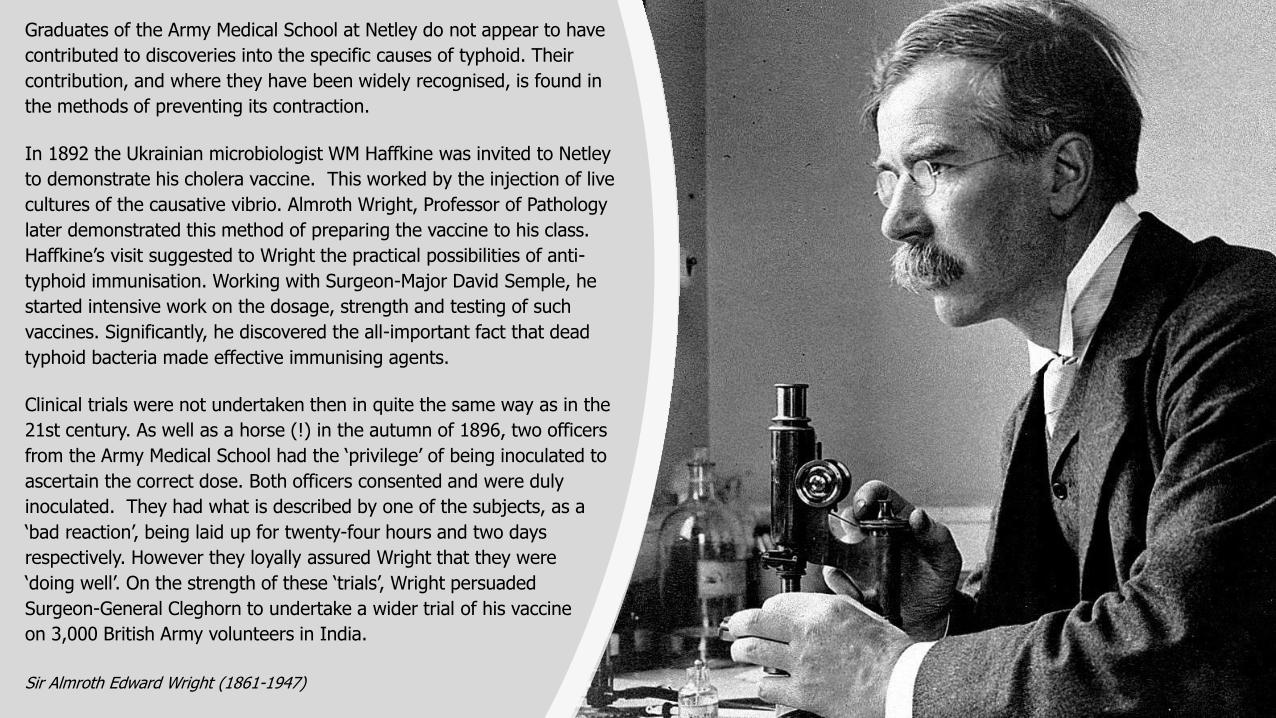
Graduates of the Army Medical School at Netley do not appear to have
contributed to discoveries into the specific causes of typhoid. Their
contribution, and where they have been widely recognised, is found in
the methods of preventing its contraction.
In 1892 the Ukrainian microbiologist WM Haffkine was invited to Netley
to demonstrate his cholera vaccine. This worked by the injection of live
cultures of the causative vibrio. Almroth Wright, Professor of Pathology
later demonstrated this method of preparing the vaccine to his class.
Haffkine’s visit suggested to Wright the practical possibilities of anti-
typhoid immunisation. Working with Surgeon-Major David Semple, he
started intensive work on the dosage, strength and testing of such
vaccines. Significantly, he discovered the all-important fact that dead
typhoid bacteria made effective immunising agents.
Clinical trials were not undertaken then in quite the same way as in the
21st century. As well as a horse (!) in the autumn of 1896, two officers
from the Army Medical School had the ‘privilege’ of being inoculated to
ascertain the correct dose. Both officers consented and were duly
inoculated. They had what is described by one of the subjects, as a
‘bad reaction’, being laid up for twenty-four hours and two days
respectively. However they loyally assured Wright that they were
‘doing well’. On the strength of these ‘trials’, Wright persuaded
Surgeon-General Cleghorn to undertake a wider trial of his vaccine
on 3,000 British Army volunteers in India.
Sir Almroth Edward Wright (1861-1947)
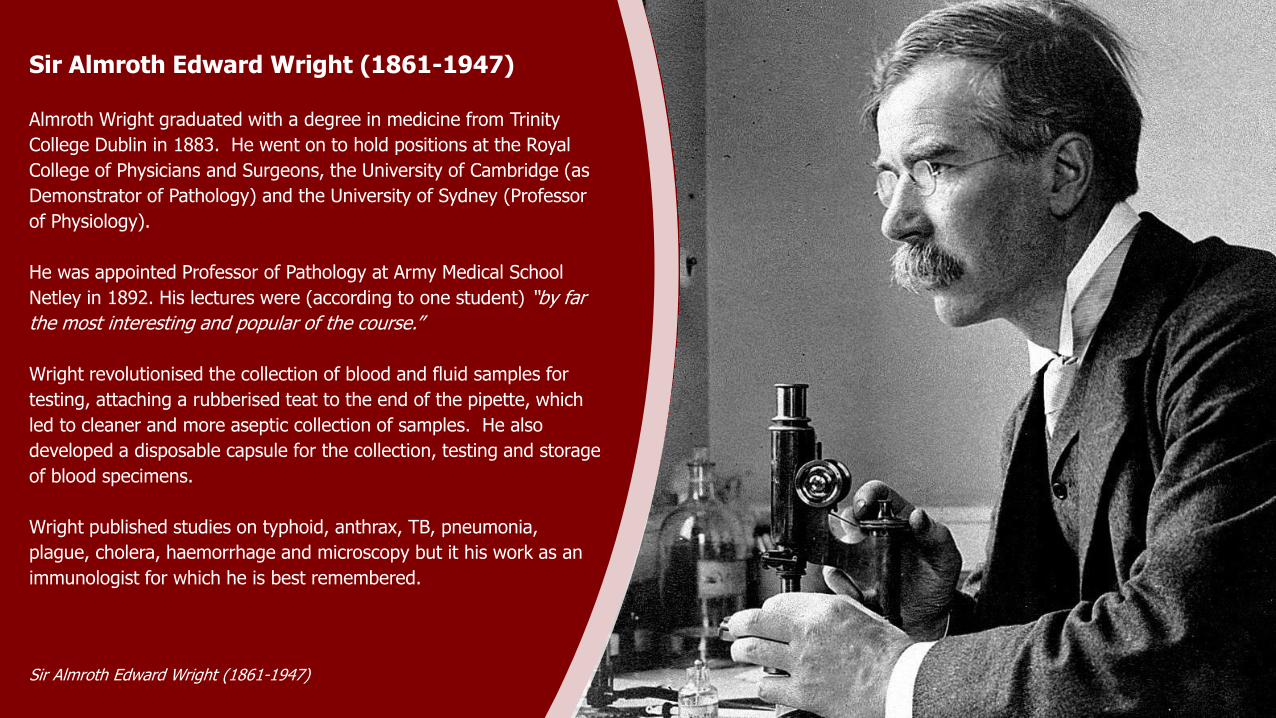
Sir Almroth Edward Wright (1861-1947)
Almroth Wright graduated with a degree in medicine from Trinity
College Dublin in 1883. He went on to hold positions at the Royal
College of Physicians and Surgeons, the University of Cambridge (as
Demonstrator of Pathology) and the University of Sydney (Professor
of Physiology).
He was appointed Professor of Pathology at Army Medical School
Netley in 1892. His lectures were (according to one student) “by far
the most interesting and popular of the course.”
Wright revolutionised the collection of blood and fluid samples for
testing, attaching a rubberised teat to the end of the pipette, which
led to cleaner and more aseptic collection of samples. He also
developed a disposable capsule for the collection, testing and storage
of blood specimens.
Wright published studies on typhoid, anthrax, TB, pneumonia,
plague, cholera, haemorrhage and microscopy but it his work as an
immunologist for which he is best remembered.
Sir Almroth Edward Wright (1861-1947)
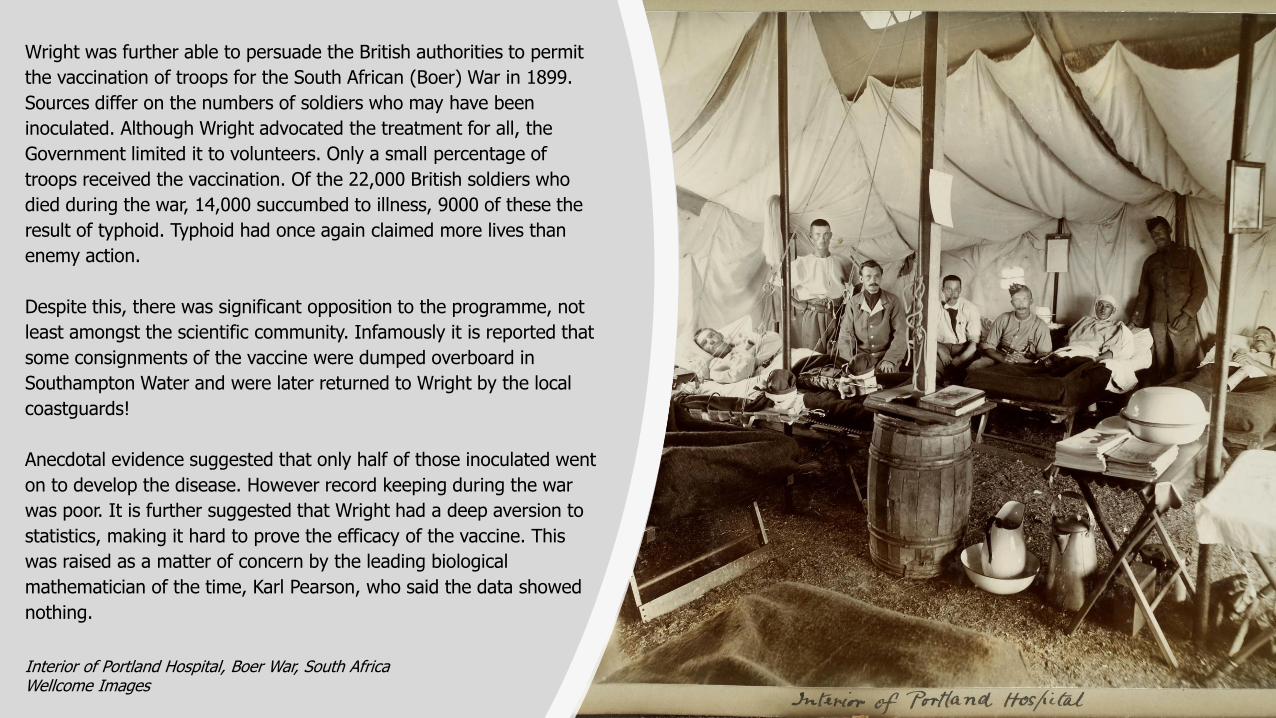
Wright was further able to persuade the British authorities to permit
the vaccination of troops for the South African (Boer) War in 1899.
Sources differ on the numbers of soldiers who may have been
inoculated. Although Wright advocated the treatment for all, the
Government limited it to volunteers. Only a small percentage of
troops received the vaccination. Of the 22,000 British soldiers who
died during the war, 14,000 succumbed to illness, 9000 of these the
result of typhoid. Typhoid had once again claimed more lives than
enemy action.
Despite this, there was significant opposition to the programme, not
least amongst the scientific community. Infamously it is reported that
some consignments of the vaccine were dumped overboard in
Southampton Water and were later returned to Wright by the local
coastguards!
Anecdotal evidence suggested that only half of those inoculated went
on to develop the disease. However record keeping during the war
was poor. It is further suggested that Wright had a deep aversion to
statistics, making it hard to prove the efficacy of the vaccine. This
was raised as a matter of concern by the leading biological
mathematician of the time, Karl Pearson, who said the data showed
nothing.
Interior of Portland Hospital, Boer War, South AfricaWellcome Images
At the end of the war, a Medical Advisory Board was established by
the British government to investigate the typhoid vaccine. The panel
included David Bruce, who had been Wright’s rival for the post of
Professor of Pathology at Netley back in 1892. They concluded that
the vaccine was ineffective, and the programme was suspended. The
immediate outcome of the committee’s investigation was the
resignation of Almroth Wright from the post at Netley. Longer term, it
also led to the Army Medical School's relocation to Millbank in
London.
With regard to typhoid, the committee recommended that inoculation
be resumed voluntarily in the British Army and that further
investigative work be undertaken. This was led by William Leishman,
who had succeeded Wright’s successor, David Semple, at Netley in
1900.
In 1910 Leishman concluded that the disappointing results during the
Boer War were almost entirely due to irregularities in the preparation
and standardisation of the vaccines. As a result of the lengthy trials
(including guinea pigs and rabbits as their subjects!) very specific
changes were made.
Sir William Boog Leishman (1865-1926)Wellcome Images
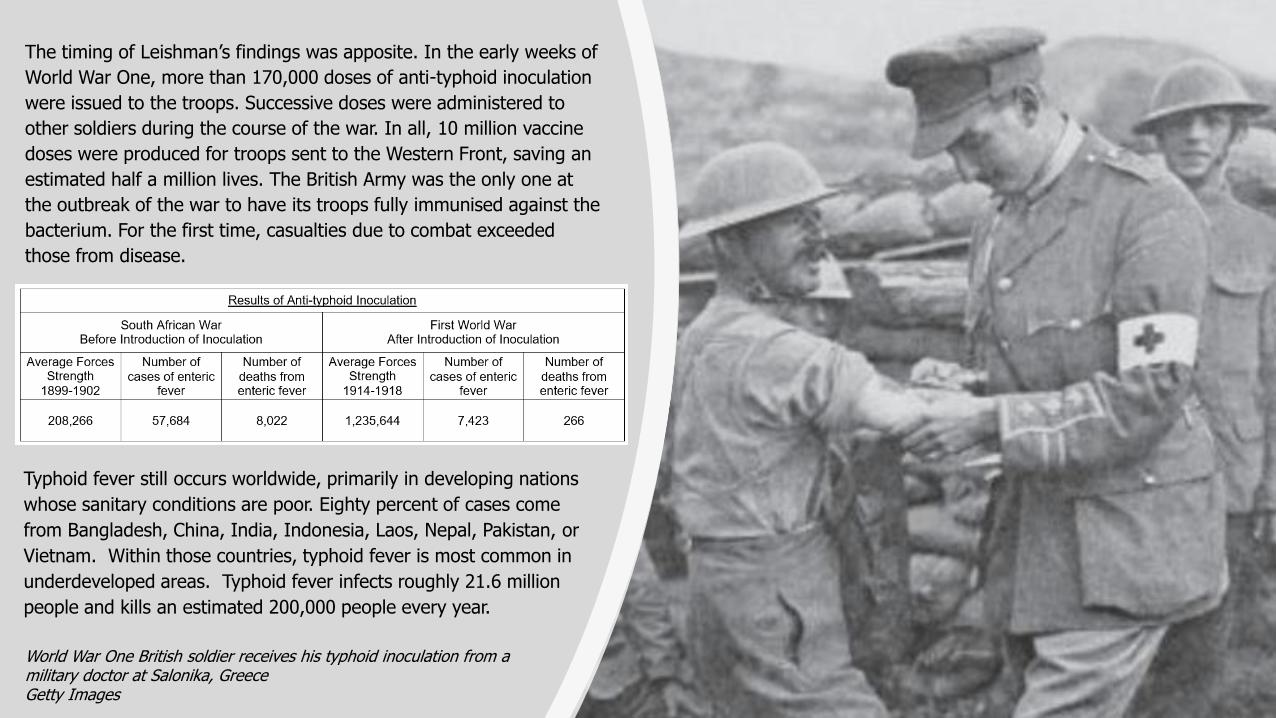
The timing of Leishman’s findings was apposite. In the early weeks of
World War One, more than 170,000 doses of anti-typhoid inoculation
were issued to the troops. Successive doses were administered to
other soldiers during the course of the war. In all, 10 million vaccine
doses were produced for troops sent to the Western Front, saving an
estimated half a million lives. The British Army was the only one at
the outbreak of the war to have its troops fully immunised against the
bacterium. For the first time, casualties due to combat exceeded
those from disease.
World War One British soldier receives his typhoid inoculation from a military doctor at Salonika, GreeceGetty Images
Typhoid fever still occurs worldwide, primarily in developing nations
whose sanitary conditions are poor. Eighty percent of cases come
from Bangladesh, China, India, Indonesia, Laos, Nepal, Pakistan, or
Vietnam. Within those countries, typhoid fever is most common in
underdeveloped areas. Typhoid fever infects roughly 21.6 million
people and kills an estimated 200,000 people every year.
Trench Fever
Return to Contents
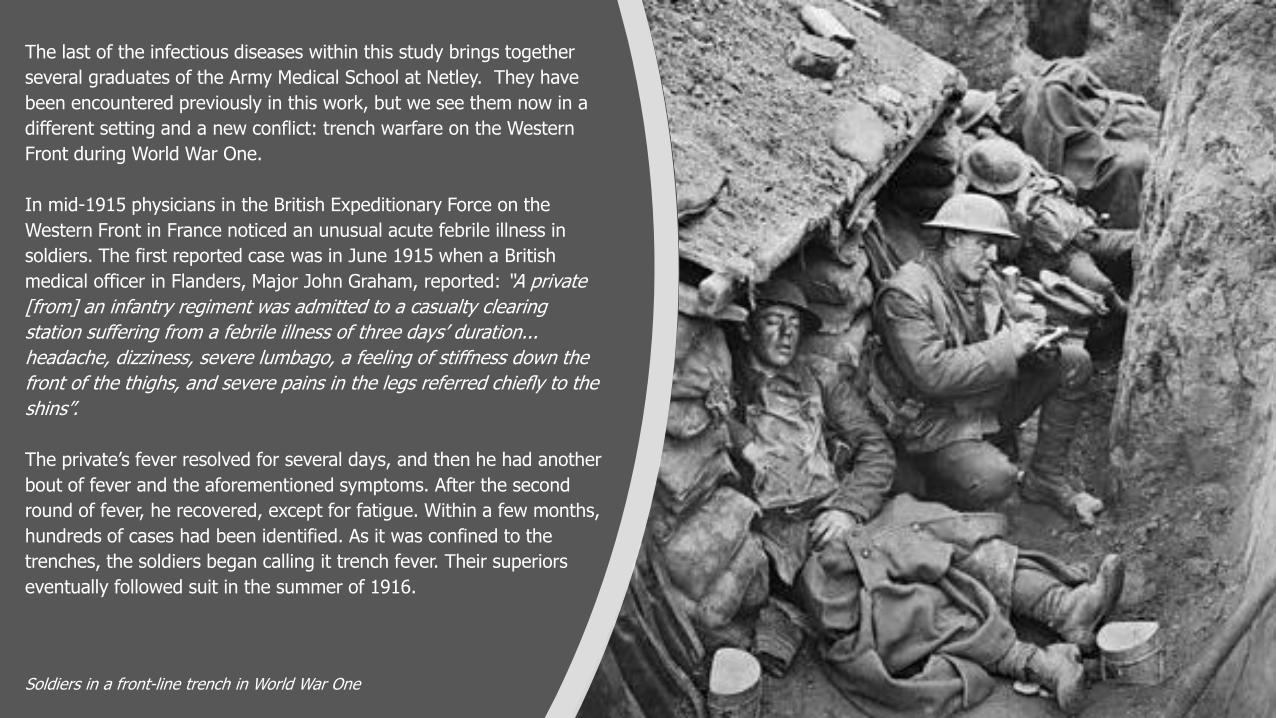
The last of the infectious diseases within this study brings together
several graduates of the Army Medical School at Netley. They have
been encountered previously in this work, but we see them now in a
different setting and a new conflict: trench warfare on the Western
Front during World War One.
In mid-1915 physicians in the British Expeditionary Force on the
Western Front in France noticed an unusual acute febrile illness in
soldiers. The first reported case was in June 1915 when a British
medical officer in Flanders, Major John Graham, reported: “A private
[from] an infantry regiment was admitted to a casualty clearing
station suffering from a febrile illness of three days’ duration...
headache, dizziness, severe lumbago, a feeling of stiffness down the
front of the thighs, and severe pains in the legs referred chiefly to the
shins”.
The private’s fever resolved for several days, and then he had another
bout of fever and the aforementioned symptoms. After the second
round of fever, he recovered, except for fatigue. Within a few months,
hundreds of cases had been identified. As it was confined to the
trenches, the soldiers began calling it trench fever. Their superiors
eventually followed suit in the summer of 1916.
Soldiers in a front-line trench in World War One
The British troops in France were not alone in suffering from this
disease. Their French, German, Austrian and American counterparts
also complained of it and there was even an outbreak in Greece near
Salonika. Estimates of the numbers infected vary from 500,000 to the
1 million that Sir David Bruce quoted in a report to the Trench Fever
Commission published in 1922. As a proportion of the fighting forces,
between one-fifth and one-third of all British troops who reported ill
had trench fever, while about one-fifth of ill German and Austrian
troops had the disease.
The cases described by Graham were brought to the attention of
Colonel Wilmot Herringham, consulting physician to the British First
Army and Colonel William Leishman, now advisor in pathology to the
British Expeditionary Force.
Initially Leishman wrote of the new ailment “I am doubtful whether it
deserves serious attention.” In a meeting with Lieutenant-General
Alfred Keogh, Director-General of the Army Medical Service (himself a
graduate from Netley in 1880) Leishman did not even mention the
illness. Nevertheless, when he returned to France, Leishman carried
out further investigations of the disease, visiting hospital patients and
reviewing case studies.
Sir William Boog Leishman (1865-1926)Wellcome Images
Initially few thought it could be anything other than an infection. The
intermittent nature of the fever meant that comparisons with malaria
and relapsing fever were commonly made. A seeming increase of
cases in summer and a corresponding decrease in winter also lent
credence to the possibility of it being spread by mosquitoes. Some
doctors hypothesized that the illness might be one of the enteric
group of fevers, modified by preventive inoculation, such as that
given for typhoid.
Other pathologists, including Captain GH Hunt and Major AC Rankin,
disagreed vehemently with this view. They, along with a growing
number of medical officers, believed that the cause was a specific
organism that had never previously been recognised.
Hundreds of cases were examined in laboratories before it was widely
accepted that the fever was not enteric. It was only in the summer of
1916 that authorities moved to officially recognise it as a novel clinical
syndrome.
But what caused this new, mysterious ailment? Attempts to culture
the causative organism from blood, faeces, urine and nasal mucous
were unsuccessful. Blood smears were unrevealing. Tests for virus
antigens and antibodies for typhoid, paratyphoid and brucellosis
were negative.
Pathological Laboratory, Royal Victoria Hospital, Netley

Throughout 1916 there was a vigorous debate about the causes of
trench fever. Malaria was known to be spread by the anopheles
mosquito. It was suggested that a similar transmission vector might
be responsible here too. A number of medics theorised that the
condition might be carried by one of the common flies or parasites
found in the trenches, most likely the human body louse. Notable
among them were Captain T Strethill Wright, Major JW McNee and
Major Arthur Hurst. Hurst, for instance, described a situation where a
‘lousy’ sergeant had transmitted the disease to six of his compatriots.
Sir Arthur Frederick Hurst (1879-1944)British Medical Journal
Sir Arthur Frederick Hurst (1879-1944)
Arthur Frederick Hurst graduated from Magdalen College, Oxford,
in 1904 and went on to join the staff of Guy's Hospital. In the
early part of World War One he was a consulting physician
stationed in Salonika (modern Thessaloniki), Greece. He led the
neurology department at Netley from 1916 to 1919 and is best
known for his work there treating patients with shell shock.
However he was also a pioneer in the use of x-rays, test meal
analysis, sigmoidoscopy, and the gastroscope. He was a
co-founder of the British Society of Gastroenterology.
Other agents were also proposed, including field voles and rats, which
were common in the trenches. There were even some commentators
who had not fully embraced “germ theory” and contended that
climatic conditions in the trenches were the cause of the new disease.
The process of identifying the cause and means of transmission of
trench fever was tortuous. Lieutenant-General Alfred Keogh
established the War Office Trench Fever Investigation Commission
(TFIC) to investigate the matter. The commission was chaired by
David Bruce (who had discovered the cause of brucellosis) and held
its first meeting in November 1917.
It took three years from the first cases of trench fever being
described by Graham for the cause of the disease to be confirmed. In
February 1918 the TFIC announced that the human body louse was
responsible for trench fever. Infected louse faeces entering the body
through the eyes or skin wounds were responsible for transmitting the
disease.
Sir David Bruce (1855–1931)London School of Hygiene & Tropical Medicine
In 1916, long before lice were identified as the cause of trench fever,
the entomologist Alexander Peacock and Major Arthur Hurst published
reports on louse infestation in the army. The War Office issued a
pamphlet on the louse problem. Schools of sanitation for medical
officers were established, with weekly lectures on louse infestation.
Treatment of the condition was not wholly effective. The more useful
weapon against trench fever was direct action against the parasitic
cause. Recommendations were made to minimise infestation including
baths, insecticides, and the use of steam-propelled disinfectors.
At the end of the war, the Allies implemented rigorous disinfestation
procedures at French ports to prevent lice from returning with the
troops. Within months of the armistice, trench fever disappeared from
the British Army on the continent. Far fewer cases of trench fever were
reported during World War Two. More effective lousicides, including
DDT, were used early in the war by most of the combatants.
Furthermore, the mobile nature of tactics in the war meant that soldiers
were not generally crowded closely together for long periods as they
had been in World War One.
Trench fever has not gone away, although now it is more commonly
seen in populations of the homeless. However, the body louse still
lies at the root of the problem, as it did in the trenches of World
War One.
Thresh Portable DisinfectorBeamish Transport Online

Research: Tim Ford – Heritage VolunteerEditing: Ursula Pearce, MA – Heritage & Education OfficerRoyal Victoria Chapel 2021
Recommended